Case Presentations: Non Responding TB Dr. Manoj Yadav
|
|
|
- Lynette Elinor Carroll
- 5 years ago
- Views:
Transcription
 Consultant Pulmonologist Kailash Hospital, Kailash Complex Near Mahadev Temple, Productivity Road Vadodara 390007 ::")
1 Case Presentations: Non Responding TB Dr. Manoj Yadav mbbs, dtcd, dnb (resp. dis.) Consultant Pulmonologist Kailash Hospital, Kailash Complex Near Mahadev Temple, Productivity Road Vadodara :: Phone: /63
2 Disclaimer The information, including but not limited to, text, graphics, images and other material contained in any presentation on this website are for informational purposes only. The case presentation are meant for qualified health professionals only. Since the uploaded presentation is converted from a ppt presentation, some of the points/aspects that are verbally communicated during ppt presentation will be missing. The clinical approach and treatment are tailored to individual patient. So it is not intended to be a substitute for one s own professional medical advice, diagnostic approach or treatment. Any questions/queries if any can be posted on my . Kindly give adequate time to reply to the same.
3 World TB Day 24 March 2016
4 What we all know Firm diagnosis of TB, esp. pulmonary TB, once suspected clinically is not difficult using common modalities like Radiology Chest X ray HRCT Chest Microbiology Smear and Culture PCR, Genexpert etc.
5 Common understanding TB not responding to 1 st line AKT = Drug resistant TB 2 nd Line drugs are usually started Though microbiological diagnosis should be attempted before labelling a case as MDR TB, it is not done by some doctors
6 Todays Talk 2 cases of Pulmonary TB Both started on treatment of MDR TB Without basic investigations
7 Case year old married lady 8 months gravida Dry Cough for 2 months Given symptomatic treatment at health center Post delivery had severe cough and breathlessness and went to SSGH
 Wt : 33 kg Sputum : AFB")
8 Reports Consulted private chest physician Admitted for 5 days (March 2014) Wt : 33 kg Sputum : AFB Negative
9 On discharge Tab Omnacortil 10 mg 1 bd Tab Akurit-4 : 1 tds Tab Moxiflox 400 mg 1 od Tab Ethionamide 250 mg 1 bd Tab Linezolid 600 mg 1 od Tab Clarithromycin 250 mg 1 bd Tab MV, Antacid etc
10 On follow up 18/04/2014 Wt : 31 kg / SpO2 : 86% Tab Akurit-4 : 1 bd Tab Moxiflox 400 mg 1 od Tab Ethionamide 250 mg ½ Tab Linezolid 600 mg 1 od Tab Clarithromycin 250 mg 1 bd Tab DAN-P / Antacid / MV/ powder 28/04/2014 Cough and fever Tab Akurit-4 : 1 bd Tab Omnacortil 10 mg 1BD Cough Suppresant Syp Tab DAN-P / Antacid / MV/ powder
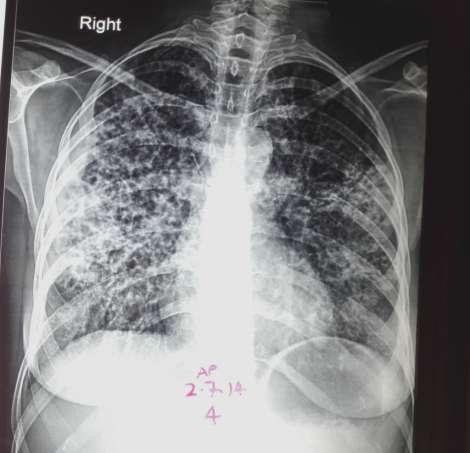
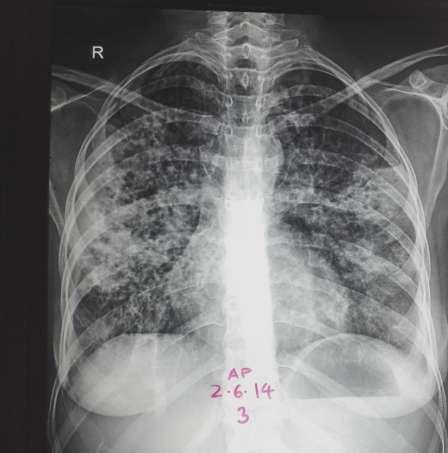
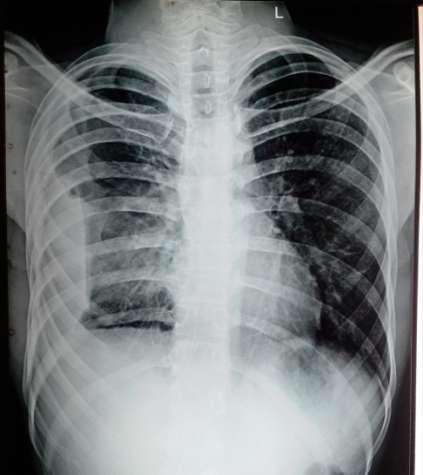
11 27 April 2014 Had giddiness at social function Admitted in ICU with altered sensorium Chest X ray : bilateral consolidation and pleural effusion Deranged LFT CT head s/o early communicating hydrocephalus CSF : Non conclusive

12
13 Sputum report (3 rd May 2014) AFB 3 day NEGATIVE AFB Culture put up Line probe assay Mycobacterium Tuberculosis complex DETECTED ISONIAZID : SUSCEPTIBLE RIFAMPICIN : SUSCEPTIBLE

14 Sputum G/S and C/S
15 Discharged on 7 May 2014 Inj Streptomycin 750 mg IM alternate day Tab Isoniazid 200 mg Tab Etambutol 800 mg Tab Moxiflox 400 mg 1 od Eustochol / Levarecetam / Hepamerz/ Duphalac
16 AFB Culture and Sensitivity Report (In 3 weeks) Culture Positive for MTB Complex 2 weeks later (after culture positive) AFB Sensitivity report AFB Sensitive to ISONIZID STREMPTOMYCIN RIFAMPICIN EHTAMBUTOL
17 OPD follow up : June- July 2014 Wt : 29 kg INH : 300 & 150 alt day EMB : 600 mg RFM : 300 mg 1 od Moxi 400 mg 1 od Inj. SM.75 IM alt day Livfit/ Livogen/ Betonin/ Rabifine-D/ B-long SM omitted No weight gain
18


19 First week of Aug 2014 Sputum for AFB 3 days report G/S and C/S report
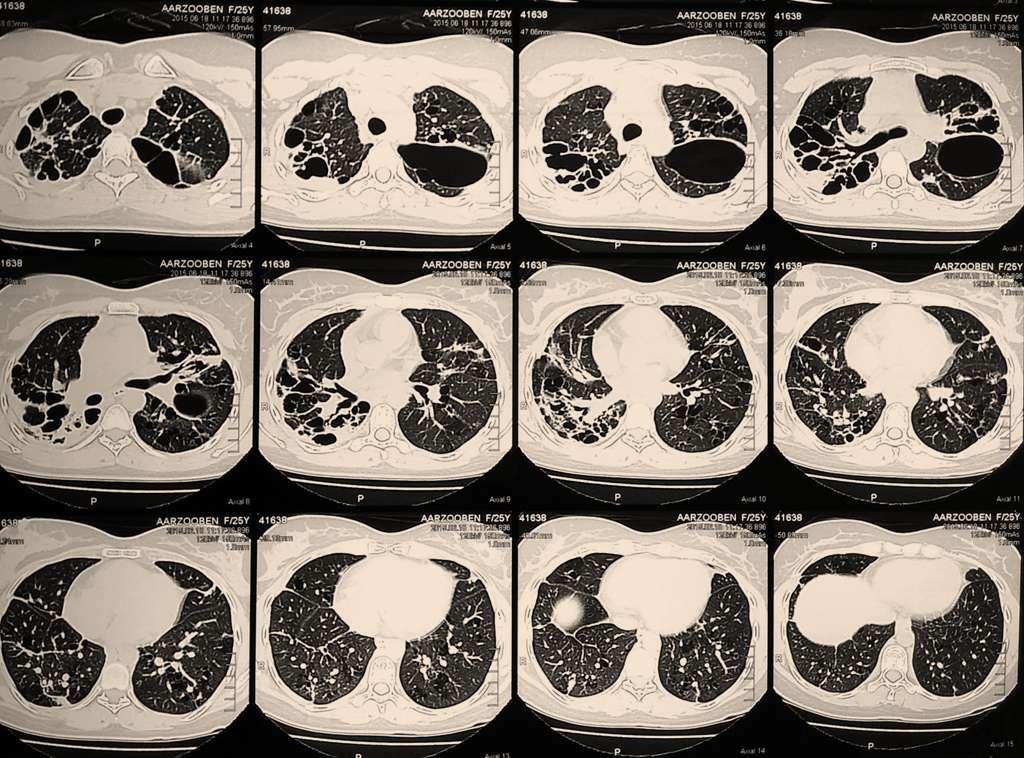
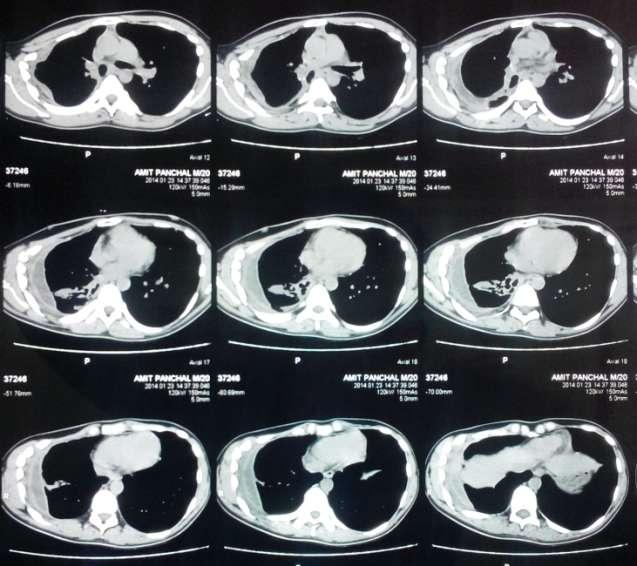
20 Last week of August 2014 By Now No weight gain AFB Positive Gram negative bacilli persist HRCT Chest Advice and patient referred to me

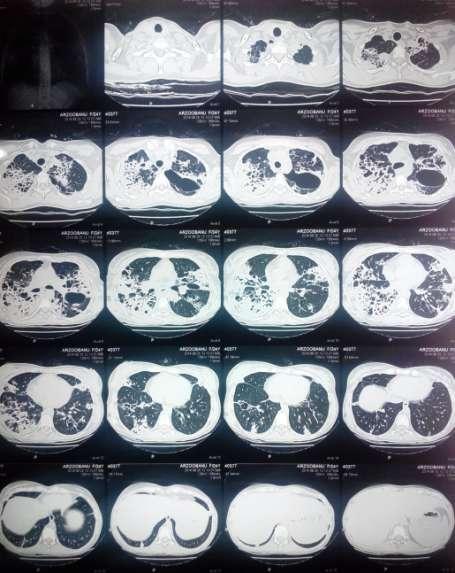
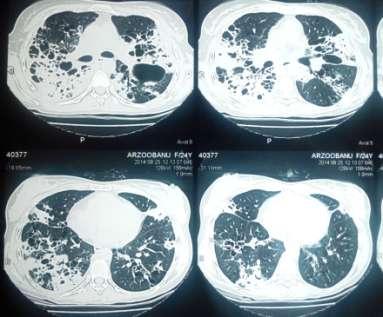
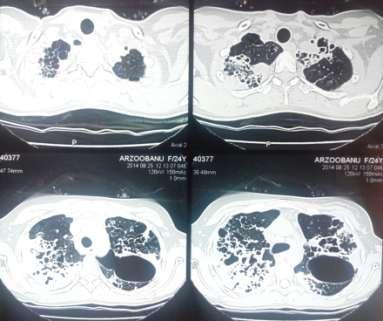
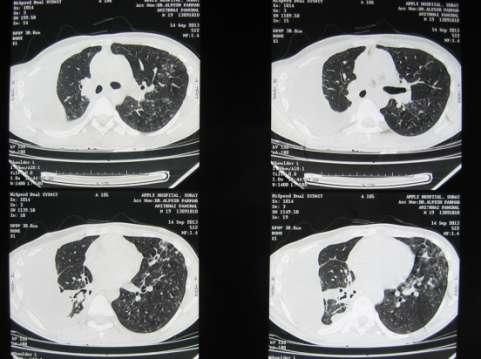
21 HRCT Chest 25-Aug-2014

22 Seen the patient with all reports and reassessed Adviced routine hemogram and Ix for Immunodeficiency Also did Bronchoscopy
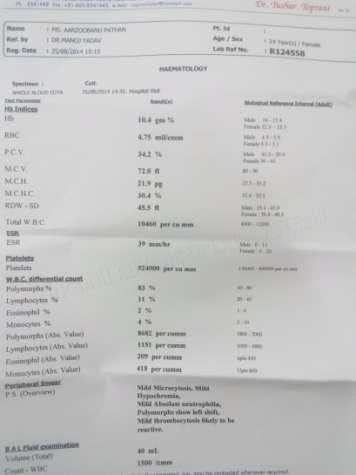
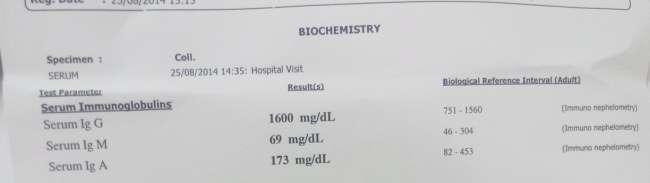
23 Investigated



24 Fiberoptic Bronchoscopy and lavage

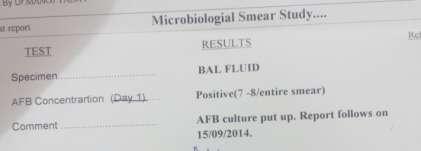
25 BAL fluid sent
26 ANTI TB drugs given for 17 months as patient had possible TBME also apart from extensive PTB. Faropenem given for persistent E.Coli infection To months to months to months Weight INH INH 300 INH 300 INH 300 RFM RFM 300 RFM 450 RFM 450 EMB EMB 600 EMB 800 EMB 800 Moxi Moxi 400 Moxi Faropenem Faropenem
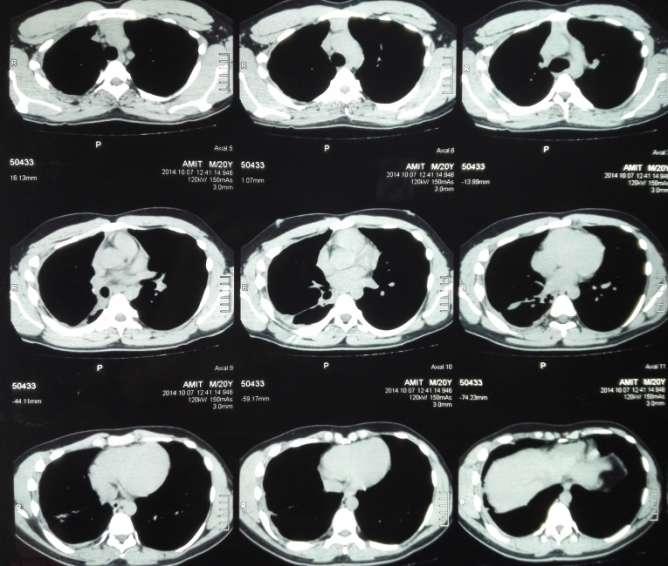
27 AFB Culture : No growth HRCT chest advised in June 2015
28 HRCT

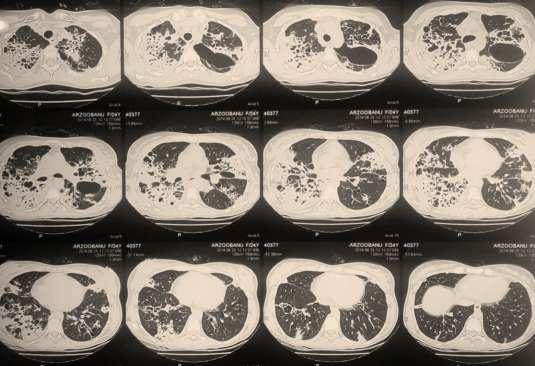
29 HRCT HRCT
30 ANTI TB drugs given for 17 months as patient had possible TBME also apart from extensive PTB. Faropenem given for persistent E.Coli infection To to to to months 3 months 7 months 5 months Weight INH INH 300 INH 300 INH 300 INH 300 STOP AKT RFM RFM 300 RFM 450 RFM 450 RFM 450 EMB EMB 600 EMB 800 EMB 800 EMB 800 Moxi Moxi 400 Moxi Faropenem Faropenem
31 Case 2
32 Case 2: 18 year old boy Dry Cough for 2 months Associated Fever Chest pain while coughing On treatment from GP for last 25 days, for RTI with raised TC Consulted Physician Pulse : 114 BP : 130/80 Weight : 54 kg R/S : AEBE Chest X ray advised

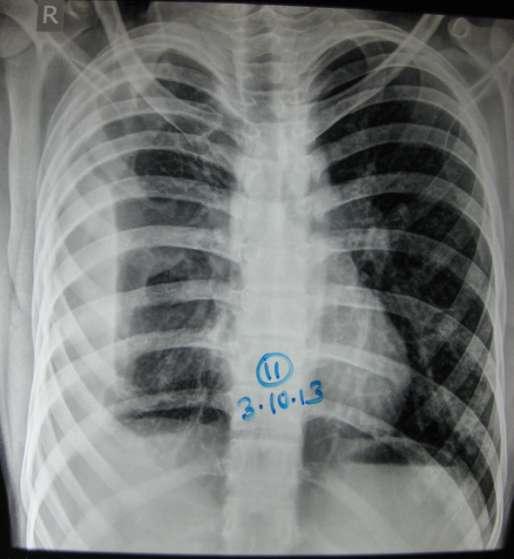
33 Prescribed (Day 1) Tab Tetracox : Tab Levofloxacin Tab PCM 500 : Tab Izra 20 : Liq Phensedyl :
34 2 nd Visit (Day 7) : : PR : 134 ; SpO2 : 94%, BP : 120/80, Wt.: 52.7 kg Tab Tetracox : 1 BD for 15 days Levoflox OMITTED 3 rd Visit (Day 18) : : Fever with rigors, Wt : 51 kg Stopped Tetracox, Started AKT-3 : for 15 days Tab Ranidom, Liq. Elixir : for 15 days Inj. Kanamycin.75 mg alternate day for 7 days Tab Moxifloxacin 400 mg 1 od for 5 days
35 4 th Visit (Day 28) 11-04: Wt. 50 kg AKT-3 : for 20 days Inj. Kanamycin 0.5 mg alt day for 7 doses 5 th Visit (Day 46) : Wt : 49 kg AKT-3 Inj. Kanamycin 0.5 mg alt day Tab Levofloxacin 250 mg 1 BD Tab Ranidom, Tab PCM, Liq Elixir Referred to DTC for possible MDR TB
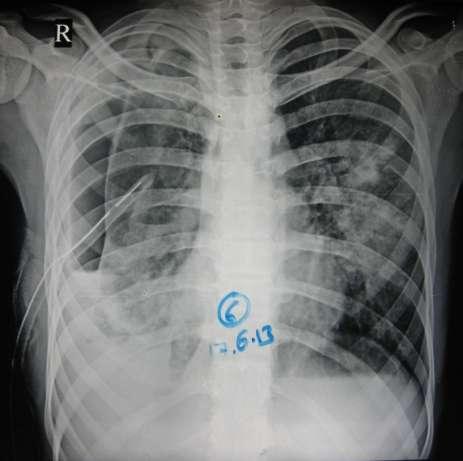
36 June 2013

37 (Day 60) Wt : 43.9 kg Acute onset right side chest pain and breathlessness Chest X ray : : Right HPT Adv: DTC reference and admission Patient went to Surat :

38 Serial Chest X ray at Surat Admitted from 14 Jun to 20 Jun in Surat ICD Tube was inserted and AKT and antibiotics given : Labelled as MDR TB

39


40 Discharged on 6 th day with ICD Tube in situ

41 Follow up at 7 days ICD Tube removed




42 40 days after tube removal Chest X ray in September 2013 Lab Reports done Hb : 12.7 WBC : 11,500 P-64; L-27; E-04; M-05 Platelet : 4,33,000 HRCT Chest advised
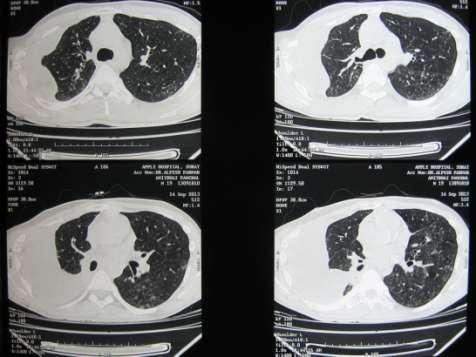
43
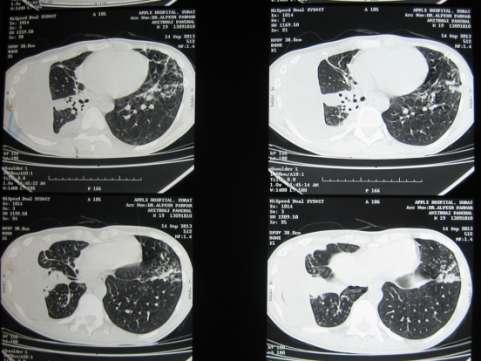
44 CT chest Moderate amount of free fluid noted in rt. Costophrenic recess with thickened visceral and parietal pleura, p/o loculated pleural effusion Ill defined branching centrilobular nodelurs in apicopost and ant seg of LUL, apical, anterobasal, lateral basal seg of LLL and post seg of RUL and apical and poster basal seg of RLL Collapse consolidated lateralbasal seg of RLL Few small LN in both axilla

45 ICD Tube Inserted : 14 Sep 2013 Pleural Fluid : Turbid Protein: 5.4 Cells : Suppurative debris No organisms detected AFB Not detected
46 ICD Tube removed on 4 th Day Treatment on Discharge (17 th Sept 2013) Inj. Kanamac 750 mg IM daily Tab Linezolid 600 mg 1 od Tab Ethionamide 250 mg 1 tds Tab Levofloxacin 750 mg 1 od Tab Coxerin 250 mg 1 bd Tab Pantoprazole 20 mg
47
48 Nov 2013

49 Inj. Kanamac 750 mg IM daily Tab Linezolid 600 mg 1 od Tab Ethionamide 250 mg 1 tds Tab Levofloxacin 750 mg 1 od Tab Coxerin 250 mg 1 bd CVTS Opinion for decortication adviced
50 Hb : 10.3 WBC : 8,300 P-73; L-19; E-03; M-05 Platelet : 4,34,000 Pleural Fluid : No Organism No AFB Debris Predominantely Polymorphs Protein 5.9 Sugar 13.6 Few RBC

51 5 days later ICD Tube removed On Discharge Inj. Kanamycin 750m mg IM od Tab Linezolid 600 mg 1 od Tab Ethionamid 250 mg 1 tds Tab Moxifloxacin 400 mg 1 od Tab Ranitidine 1 bd Tab Esomeprazole 1bd Tab Dan P 1 sos
52 By Now 9 months of AKT In 2 nd month: Diagnosed as MDR TB with empyema (No report available for labelling MDR TB) Second line AKT for 7 months Kanamycin, Ethionamide, Cycloserine, PAS, Quinolone ICD Tube inserted : 3 times AFB never was positive Pleural fluid : inconclusive Patient had severe gastritis and also depression with phobias of being attacked Advised CVTS opinion decortication Weight loss from 54 kg to 49 kg

53 Consulted me in Nov 2013 Cough Epigastric tenderness Anorexia Fever Wt.: 49 kg




54 Got admitted from 19 to 24 Dec 2013 Fiberoptic Bronchoscopy and bronchial lavage done Copious secretions in RLL, esp. apical segment


55 Bronchial Lavage
56 Pleural Fluid Report Next day : Pleural fluid aspirated 80 ml turbid No organisms No AFB by ZN stain No growth on culture



57
58 Discharged on 6 th day Treated with HERZ Inj. Amikacin Inj. Piperacillin+Tazo Switched to Inj. Tigycycline for 3 days supportive treatment for gastritis On Discharge HERZ Tab Chloramphenicol 500 mg tds Supportive MV/BC

59 06-Jan-2014 Follow up

60 15 days later HRCT Chest done again
61





62 Fiberoptic Bronchoscopy repeated Apart from usual lavage, a catheter was inserted into the lower lobe segment and fluid aspirated



63
64 Continued treatment on OPD HERZ Tab Immumod Tab Esomeprazole Nutritious diet Rapid weight gain and good clinical improvement noted.


65

66 CT Chest in Oct 2014
67


68 October 2104 January 2014 Pleural thickening GONE

69 Chest X ray taken before stopping AKT No pleural thickening No decortication was required. 16 Nov 2014
70 Remarks Both cases were labelled as MDR TB without most basic investigations Both cases were complicated with gram negative bacilli. Both patients responded well to the first line AKT and other medications
71 Learning Points A patient of Kochs not responding to AKT is not always MDR TB Try to rule out common pathogens Common pathogens too can be multidrug resistant Timely and Judicious use of interventional modalities can change the course of disease and patients life
72
73
74 Thank you for viewing Your valuable comments can be ed to or click on
M5 MEQs 2016 Session 3: SOB 18/11/16
 M5 MEQs 2016 Session 3: SOB 18/11/16 http://tinyurl.com/hn7qzt3 Question 1 Ms Tan is a 52 year old female with no past medical history. She comes to the emergency department presenting with a fever for
M5 MEQs 2016 Session 3: SOB 18/11/16 http://tinyurl.com/hn7qzt3 Question 1 Ms Tan is a 52 year old female with no past medical history. She comes to the emergency department presenting with a fever for
Dr Sharanjit Dhoot. Chelsea and Westminster Hospital, London. 18 th Annual Conference of the British HIV Association (BHIVA)
") 18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
TB Grand Rounds. MDR-TB: Management of Adverse Drug Reactions. Reynard J. McDonald, M.D. September 18, Patient History
 TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION
 1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
Clinical Management : DR-TB
 Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC
 Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Tb : Recent recommendation. Dr.Ketan Shah
 Tb : Recent recommendation Dr.Ketan Shah Tbc : Clinician If you think It is easy to diagnose : u r not good clinician It is difficult to diagnose :U r not alone doctor to think this 6/22/2015 Ketan Shah
Tb : Recent recommendation Dr.Ketan Shah Tbc : Clinician If you think It is easy to diagnose : u r not good clinician It is difficult to diagnose :U r not alone doctor to think this 6/22/2015 Ketan Shah
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
TB Intensive Houston, Texas. Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD
 TB Barbara Seaworth, MD") TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
Drug resistant TB: The role of the laboratory
 Drug resistant TB: The role of the laboratory 26 Oct 2012 Andrew Whitelaw NHSLS / UCT TB lab functions: Outline Resistance testing Genotypic Phenotypic Which tests are done when, and why Reporting of
Drug resistant TB: The role of the laboratory 26 Oct 2012 Andrew Whitelaw NHSLS / UCT TB lab functions: Outline Resistance testing Genotypic Phenotypic Which tests are done when, and why Reporting of
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
Community Acquired Pneumonia (CAP)
") Community Acquired Pneumonia (CAP) The following guidelines have been developed to aid clinicians in the investigation and management of patients with CAP at the Royal Liverpool University Hospital (RLUH).
Community Acquired Pneumonia (CAP) The following guidelines have been developed to aid clinicians in the investigation and management of patients with CAP at the Royal Liverpool University Hospital (RLUH).
Absolutely fragilis - A case discussion
 Absolutely fragilis - A case discussion Rohma Ghani 1 Giovanni Satta 1 Harriet Hughes 2 James Hatcher 1 1 Imperial College Healthcare NHS Trust 2 UK Anaerobe Reference Unit 64F Kuwaiti national Metastatic
Absolutely fragilis - A case discussion Rohma Ghani 1 Giovanni Satta 1 Harriet Hughes 2 James Hatcher 1 1 Imperial College Healthcare NHS Trust 2 UK Anaerobe Reference Unit 64F Kuwaiti national Metastatic
Challenges to treat MDR TB
 Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
CLINICAL PROTOCOL FOR COMMUNITY ACQUIRED PNEUMONIA. SCOPE: Western Australia. CORB score equal or above 1. All criteria must be met:
 CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
Case 1 and Case 2. Case 1 3/23/2016
 Case 1 and Deidra D. Parrish, MD, MPH&TM Nashville Metro Public Health Dept TB Symposium March 30, 2016 Case 1 27 yo Indian woman came to the US to join her husband three months prior to clinic visit.
Case 1 and Deidra D. Parrish, MD, MPH&TM Nashville Metro Public Health Dept TB Symposium March 30, 2016 Case 1 27 yo Indian woman came to the US to join her husband three months prior to clinic visit.
Treatment of Drug Resistant TB
 Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
Outlines. Introduction Prevalence Resistance Clinical presentation Diagnosis Management Prevention Case presentation Achievements
 Amal Meas Al-Anizi, PharmD Candidate KSU, Infectious Disease Rotation 2014 Outlines Introduction Prevalence Resistance Clinical presentation Diagnosis Management Prevention Case presentation Achievements
Amal Meas Al-Anizi, PharmD Candidate KSU, Infectious Disease Rotation 2014 Outlines Introduction Prevalence Resistance Clinical presentation Diagnosis Management Prevention Case presentation Achievements
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France
 Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
DR-TB PATIENT IDENTITY CARD
 Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
Acute Pyelonephritis POAC Guideline
 Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
MDR treatment. Shanghai, May 2012 Arnaud Trébucq The Union
 MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
XDR TB: The Laboratory s Dilemma vs The Clinician s Dilemma
 XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
Quality of 2 nd line medicines for tuberculosis. Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products
 Quality of 2 nd line medicines for tuberculosis Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products Case studies in medicines for tuberculosis Outline: Statistics
Quality of 2 nd line medicines for tuberculosis Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products Case studies in medicines for tuberculosis Outline: Statistics
Tuberculosis infection in an Asian elephant at a Japanese Zoo and its first treatment in Japan
 Tuberculosis infection in an Asian elephant at a Japanese Zoo and its first treatment in Japan Satoshi Ishikawa, Satomi Suga, Yasuhiko Mukai Fukuyama Zoo, Hiroshima Fukuyama Zoo October 22th, 2017 Tuberculosis
Tuberculosis infection in an Asian elephant at a Japanese Zoo and its first treatment in Japan Satoshi Ishikawa, Satomi Suga, Yasuhiko Mukai Fukuyama Zoo, Hiroshima Fukuyama Zoo October 22th, 2017 Tuberculosis
Multidrug-resistant Tuberculosis. Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership
 Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
Management of MDR and XDR TB Prof. Martin Boeree
 Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
Antimicrobial Stewardship in Continuing Care. Urinary Tract Infections Clinical Checklist
 Antimicrobial Stewardship in Continuing Care Urinary Tract Infections Clinical Checklist December 2014 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis at the
Antimicrobial Stewardship in Continuing Care Urinary Tract Infections Clinical Checklist December 2014 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis at the
MDR TB AND CASE STUDIES
 MDR TB AND CASE STUDIES Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Seattle, CITC Clinical Intensive June 15, 2018 Slide
MDR TB AND CASE STUDIES Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Seattle, CITC Clinical Intensive June 15, 2018 Slide
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
Survey of Wisconsin Primary Care Clinicians
 ... for our health Clinical Approach to Nonresponsive Pneumonia: A Survey of Wisconsin Primary Care Clinicians Hannah A. Louks, 1,3 Jared M. Fixmer, MD 2, and Dennis J. Baumgardner, MD 1,2,3 1 Wisconsin
... for our health Clinical Approach to Nonresponsive Pneumonia: A Survey of Wisconsin Primary Care Clinicians Hannah A. Louks, 1,3 Jared M. Fixmer, MD 2, and Dennis J. Baumgardner, MD 1,2,3 1 Wisconsin
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing - PRELIMINARY -
 Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
Multi-Drug and Extensively Drug Resistant Tuberculosis
 Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2
 1 MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2 1 India has the highest TB burden in the world 3 4 2 5 M. tuberculosis Resistance
1 MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2 1 India has the highest TB burden in the world 3 4 2 5 M. tuberculosis Resistance
MDR/XDR TB. Barbara Seaworth, MD, FIDSA, FACP October 27, TB Intensive October 24 27, 2017 San Antonio, TX
 MDR/XDR TB Barbara Seaworth, MD, FIDSA, FACP October 27, 2017 TB Intensive October 24 27, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Barbara Seaworth, MD, FIDSA, FACP, has the following disclosures
MDR/XDR TB Barbara Seaworth, MD, FIDSA, FACP October 27, 2017 TB Intensive October 24 27, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Barbara Seaworth, MD, FIDSA, FACP, has the following disclosures
Drug-resistant TB therapy: the future is now
 Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
BRUCELLOSIS. Morning report 7/11/05 Andy Bomback
 BRUCELLOSIS Morning report 7/11/05 Andy Bomback Also called undulant, Mediterranean, or Mata fever, brucellosis is an acute and chronic infection of the reticuloendothelial system gram negative facultative
BRUCELLOSIS Morning report 7/11/05 Andy Bomback Also called undulant, Mediterranean, or Mata fever, brucellosis is an acute and chronic infection of the reticuloendothelial system gram negative facultative
Content. In the beginning Antimicrobial Stewardship 2. Antimicrobial Prescribing with cases to cover
 Content Safe & Effective Prescribing of Antimicrobials: Whistle-stop update for non-medical prescribers Elaine Roberts Lead Pharmacist, Antimicrobials BCUHB East 1. Antimicrobial Stewardship 2. Antimicrobial
Content Safe & Effective Prescribing of Antimicrobials: Whistle-stop update for non-medical prescribers Elaine Roberts Lead Pharmacist, Antimicrobials BCUHB East 1. Antimicrobial Stewardship 2. Antimicrobial
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance
 Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Antimicrobial susceptibility
 Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Coccidioidomycosis Nothing to disclose
 Coccidioidomycosis Nothing to disclose Disclosure Greg Melcher, M.D. Professor of Clinical Medicine Division of HIV, ID and Global Medicine Zuckerman San Francisco General Hospital University of California,
Coccidioidomycosis Nothing to disclose Disclosure Greg Melcher, M.D. Professor of Clinical Medicine Division of HIV, ID and Global Medicine Zuckerman San Francisco General Hospital University of California,
Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy
 biopsy") Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy Dr. Fidelma Fitzpatrick Consultant Microbiologist, Co-chair, NCCP Prostate Bx Infection Project Board Fidelma.fitzpatrick@hse.ie
Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy Dr. Fidelma Fitzpatrick Consultant Microbiologist, Co-chair, NCCP Prostate Bx Infection Project Board Fidelma.fitzpatrick@hse.ie
Suitability of Antibiotic Treatment for CAP (CAPTIME) The duration of antibiotic treatment in community acquired pneumonia (CAP)
 The duration of antibiotic treatment in community acquired pneumonia (CAP)") STUDY PROTOCOL Suitability of Antibiotic Treatment for CAP (CAPTIME) Purpose The duration of antibiotic treatment in community acquired pneumonia (CAP) lasts about 9 10 days, and is determined empirically.
STUDY PROTOCOL Suitability of Antibiotic Treatment for CAP (CAPTIME) Purpose The duration of antibiotic treatment in community acquired pneumonia (CAP) lasts about 9 10 days, and is determined empirically.
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
University of Groningen. Tuberculosis and its sequelae Akkerman, Onno
 University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
DATA COLLECTION SECTION BY FRONTLINE TEAM. Patient Identifier/ Medical Record number (for facility use only)
") Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Safety of an Out-Patient Intravenous Antibiotics Programme
 Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Principles of Antimicrobial Therapy
 Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool)
") Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool) DOTS + and LTBI New drugs for TB and the challenge of resistance talk plan 1. Epidemiology 2. Treatment 3. The MDRTB
Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool) DOTS + and LTBI New drugs for TB and the challenge of resistance talk plan 1. Epidemiology 2. Treatment 3. The MDRTB
MDR-TB drugs per WHO guidelines
 New antituberculous agents for drug-resistant resistant TB Symposium Belgian Society of Infectiology and Clinical Microbiology November 9 Jens Van Roey, MD - Tibotec Definitions MDR-TB multidrug resistance
New antituberculous agents for drug-resistant resistant TB Symposium Belgian Society of Infectiology and Clinical Microbiology November 9 Jens Van Roey, MD - Tibotec Definitions MDR-TB multidrug resistance
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S.
 Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
To guide safe and appropriate selection of antibiotic therapy for Peritoneal Dialysis patients.
 Nephrology Directorate Subject: Objective: Prepared by: Aintree Antibiotic Guidelines for Peritoneal Dialysis (PD): Catheter Insertion, and the Diagnosis and Treatment of PD Peritonitis and Exit-Site Infections.
Nephrology Directorate Subject: Objective: Prepared by: Aintree Antibiotic Guidelines for Peritoneal Dialysis (PD): Catheter Insertion, and the Diagnosis and Treatment of PD Peritonitis and Exit-Site Infections.
Volume. December Infection. Notes. length of. cases as 90% 1 week. tonsillitis. First Line. sore throat / daily for 5 days. quinsy >4000.
 Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
NEW ATS/IDSA VAP-HAP GUIDELINES
 NEW ATS/IDSA VAP-HAP GUIDELINES MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the University
NEW ATS/IDSA VAP-HAP GUIDELINES MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the University
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements
 Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
Management of Hospital-acquired Pneumonia
 Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Protocol for exit-site care and treatment of exit-site infections in peritoneal dialysis CONTROLLED DOCUMENT
 CONTROLLED DOCUMENT Protocol for exit-site care and treatment of exit-site infections in peritoneal dialysis CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Guideline Clinical The purpose
CONTROLLED DOCUMENT Protocol for exit-site care and treatment of exit-site infections in peritoneal dialysis CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Guideline Clinical The purpose
UPDATE ON PARASITE DIAGNOSIS
 NORTH CANTERBURY DEER INDUSTRY FOCUS FARM PROJECT DEER PARASITE WORKSHOP TUESDAY 29 TH JANUARY 213 UPDATE ON PARASITE DIAGNOSIS COLIN MACKINTOSH VETERINARY SCIENTIST, INVERMAY SOME QUESTIONS FARMERS ASK
NORTH CANTERBURY DEER INDUSTRY FOCUS FARM PROJECT DEER PARASITE WORKSHOP TUESDAY 29 TH JANUARY 213 UPDATE ON PARASITE DIAGNOSIS COLIN MACKINTOSH VETERINARY SCIENTIST, INVERMAY SOME QUESTIONS FARMERS ASK
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Reducing Time to Initial Antibiotic Dose in Pneumonia Patients
 Intermountain Health Care Institute for Health Care Delivery Research ATP Project Report April 2005 Reducing Time to Initial Antibiotic Dose in Pneumonia Patients Susan Bukunt RN MPA Chris Hunter RN MPH
Intermountain Health Care Institute for Health Care Delivery Research ATP Project Report April 2005 Reducing Time to Initial Antibiotic Dose in Pneumonia Patients Susan Bukunt RN MPA Chris Hunter RN MPH
Practical. Walk through New Survival Guide
 Many faces of TB: Drug resistant it ttbs Survival lgid Guide v3 P B L Ch G Sh t L T P. Barry, L. Chen, G. Schecter, L. True Curry International TB Center/CTCA April 20, 2016 Real case Practical Walk through
Many faces of TB: Drug resistant it ttbs Survival lgid Guide v3 P B L Ch G Sh t L T P. Barry, L. Chen, G. Schecter, L. True Curry International TB Center/CTCA April 20, 2016 Real case Practical Walk through
MANAGEMENT OF PELVIC INFLAMMATORY DISEASE
 GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 29 October 2014 GRANUPAS, gastro-resistant granules 30 sachets with a calibrated measuring spoon (CIP: 34009 278 801
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 29 October 2014 GRANUPAS, gastro-resistant granules 30 sachets with a calibrated measuring spoon (CIP: 34009 278 801
How to get in senior hospital and clinical engagement?
 How to get in senior hospital and clinical engagement? G. C. Khilnani M.D. FCCP(USA), MNAMS, FNCCP, FICP Professor Pulmonary Medicine & Sleep Disorders All India Institute of Medical Sciences New-Delhi
How to get in senior hospital and clinical engagement? G. C. Khilnani M.D. FCCP(USA), MNAMS, FNCCP, FICP Professor Pulmonary Medicine & Sleep Disorders All India Institute of Medical Sciences New-Delhi
VIET NAM Percentage below / above median
 National 1983-84 0. - 4.99 11809 47.0 64.1 8.5 Converted estimates 00336 National 1987-89 0. - 4.99 7044 40.7 61.3 11.1 Converted estimates 00349 National SEP-OCT 1992-93 0. - 5.00 2833 9.7 36.9 29.5 61.4
National 1983-84 0. - 4.99 11809 47.0 64.1 8.5 Converted estimates 00336 National 1987-89 0. - 4.99 7044 40.7 61.3 11.1 Converted estimates 00349 National SEP-OCT 1992-93 0. - 5.00 2833 9.7 36.9 29.5 61.4
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children
 Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Promoting Appropriate Antimicrobial Prescribing in Secondary Care
 Promoting Appropriate Antimicrobial Prescribing in Secondary Care Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2015 Introduction Background ESPAUR
Promoting Appropriate Antimicrobial Prescribing in Secondary Care Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2015 Introduction Background ESPAUR
2010 ARO/CDI Prevalence Survey. MRSA [ ] VRE [ ] Clostridium difficile [ ]
![2010 ARO/CDI Prevalence Survey. MRSA [ ] VRE [ ] Clostridium difficile [ ]](/thumbs/89/98738029.jpg "2010 ARO/CDI Prevalence Survey. MRSA [ ] VRE [ ] Clostridium difficile [ ]") 2010 ARO/CDI Prevalence Survey 1) Patient identifier: 2) Hospital number: 3) Is the patient currently (day of survey) infected or colonized with (check all that apply): MRSA [ ] VRE [ ] Clostridium difficile
2010 ARO/CDI Prevalence Survey 1) Patient identifier: 2) Hospital number: 3) Is the patient currently (day of survey) infected or colonized with (check all that apply): MRSA [ ] VRE [ ] Clostridium difficile
Infection Comments First Line Agents Penicillin Allergy History of multiresistant. line treatment: persist for >7 days they may be
 Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
SPECIMEN COLLECTION FOR CULTURE OF BACTERIAL PATHOLOGENS QUICK REFERENCE
 1 Policy #: Subject: 611 (PLH-611-02) Effective Date: NA Reviewed Date: 2/1/2008 SPECIMEN COLLECTION FOR CULTURE OF BACTERIAL PATHOGENS QUICK REFERENCE Approved by: Laboratory Executive Director, Ed Hughes
1 Policy #: Subject: 611 (PLH-611-02) Effective Date: NA Reviewed Date: 2/1/2008 SPECIMEN COLLECTION FOR CULTURE OF BACTERIAL PATHOGENS QUICK REFERENCE Approved by: Laboratory Executive Director, Ed Hughes
CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP)
 Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP)") CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP) Beverly Metchock, DrPH, D(ABMM) Mycobacteriology Laboratory Branch/Division
CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP) Beverly Metchock, DrPH, D(ABMM) Mycobacteriology Laboratory Branch/Division
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
These recommendations were approved for use by the Pharmaceutical and Therapeutics Committee, RCWMCH on 1 February 2017.
 Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE
 ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE Version 1.0 Date ratified June 2009 Review date June 2011 Ratified by Authors Consultation Nottingham Antibiotic Guidelines Committee
ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE Version 1.0 Date ratified June 2009 Review date June 2011 Ratified by Authors Consultation Nottingham Antibiotic Guidelines Committee
TB New Drugs, Shorter Courses
 TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 MDR/XDR TB Barbara J. Seaworth, MD October 16, 2013 Barbara J. Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
TB Intensive Houston, Texas October 15-17, 2013 MDR/XDR TB Barbara J. Seaworth, MD October 16, 2013 Barbara J. Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
Clinical Manifestations and Treatment of Plague Dr. Jacky Chan. Associate Consultant Infectious Disease Centre, PMH
 Clinical Manifestations and Treatment of Plague Dr. Jacky Chan Associate Consultant Infectious Disease Centre, PMH Update of plague outbreak situation in Madagascar A large outbreak since 1 Aug 2017 As
Clinical Manifestations and Treatment of Plague Dr. Jacky Chan Associate Consultant Infectious Disease Centre, PMH Update of plague outbreak situation in Madagascar A large outbreak since 1 Aug 2017 As
Measure Information Form
 Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Septicaemia Definitions 1
 Septicaemia Definitions 1 Term Definition Bacteraemia Systemic Inflammatory response (SIRS) Sepsis Bacteria that can be cultured from the blood stream The systemic response to a wide range of stresses.
Septicaemia Definitions 1 Term Definition Bacteraemia Systemic Inflammatory response (SIRS) Sepsis Bacteria that can be cultured from the blood stream The systemic response to a wide range of stresses.
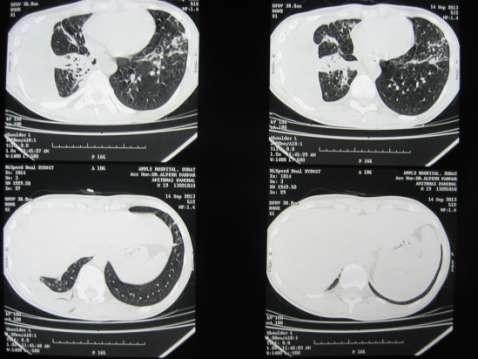
"Serpent" Sign, "Double Arch" Sign and "Air-Bubble"Sign in a case of Ruptured Hydatid Cyst-A Case Report
 Article ID: WMC004602 ISSN 2046-1690 "Serpent" Sign, "Double Arch" Sign and "Air-Bubble"Sign in a case of Ruptured Hydatid Cyst-A Case Report Peer review status: No Corresponding Author: Dr. Dipti Gothi,
Article ID: WMC004602 ISSN 2046-1690 "Serpent" Sign, "Double Arch" Sign and "Air-Bubble"Sign in a case of Ruptured Hydatid Cyst-A Case Report Peer review status: No Corresponding Author: Dr. Dipti Gothi,
Dr.Asad A. Khan FRCPC Consultant, Division of Infectious Diseases Tawam Hospital Al Ain, UAE
 MDR Enterobacteriaceae in community acquired infections Dr.Asad A. Khan FRCPC Consultant, Division of Infectious Diseases Tawam Hospital Al Ain, UAE Introduction Case presentation Epidemiology Objectives
MDR Enterobacteriaceae in community acquired infections Dr.Asad A. Khan FRCPC Consultant, Division of Infectious Diseases Tawam Hospital Al Ain, UAE Introduction Case presentation Epidemiology Objectives
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Antibiotic treatment and monitoring for suspected or confirmed early-onset neonatal infection bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to
Antibiotic treatment and monitoring for suspected or confirmed early-onset neonatal infection bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT
 INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
Women s Antimicrobial Guidelines Summary
 Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
Guidelines for Antimicrobial treatment for treatment of confirmed infections adults
 Guidelines for Antimicrobial treatment for treatment of confirmed infections adults This guideline gives recommendations for treatment of confirmed infections in adults for children please see the Paediatric
Guidelines for Antimicrobial treatment for treatment of confirmed infections adults This guideline gives recommendations for treatment of confirmed infections in adults for children please see the Paediatric
Role of the nurse in diagnosing infection: The right sample, every time
 BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
FOLLOWING BUNDLE ADMINISTERED WITHIN ONE HOUR.
 Patient label DATE and TIME: 1 REVIEW BY Emergency Department SENIOR REGISTRAR (ED BLEEP 5999) +/-Leave Proforma 2 FOLLOWING BUNDLE ADMINISTERED WITHIN ONE HOUR. Bloods for FBC, U+E, CRP, LFT s, Clotting
Patient label DATE and TIME: 1 REVIEW BY Emergency Department SENIOR REGISTRAR (ED BLEEP 5999) +/-Leave Proforma 2 FOLLOWING BUNDLE ADMINISTERED WITHIN ONE HOUR. Bloods for FBC, U+E, CRP, LFT s, Clotting
DRAFT DRAFT. Paediatric Antibiotic Prescribing Guideline. May
 Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Antibiotic stewardship in long term care
 Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
References and supporting documents 5 Roles and responsibilities 5
 Antibiotic Therapy for Patients with Antibody Deficiency Guidelines for Classification: guidelines Lead Author: Dr Archana Herwadkar, Paul Chadwick Additional author(s): Dr Hana Alachkar Authors Division:
Antibiotic Therapy for Patients with Antibody Deficiency Guidelines for Classification: guidelines Lead Author: Dr Archana Herwadkar, Paul Chadwick Additional author(s): Dr Hana Alachkar Authors Division:
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study
 Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study Julie Tans-Kersten, MS, BS-MT (ASCP) Tuberculosis Laboratory Program Coordinator Wisconsin
Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study Julie Tans-Kersten, MS, BS-MT (ASCP) Tuberculosis Laboratory Program Coordinator Wisconsin
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT DRAFT AS CURRENTLY OUT FOR CONSULTATION BUT CAN BE UTILISED IN PRESENT FORMAT Name & Title Of Author: Date Revised: Approved by Committee/Group:
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT DRAFT AS CURRENTLY OUT FOR CONSULTATION BUT CAN BE UTILISED IN PRESENT FORMAT Name & Title Of Author: Date Revised: Approved by Committee/Group:
Antimicrobial Stewardship Programs The Same, but Different. Sara Nausheen, MD Kevin Kern, PharmD
 Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Telephone Clindamycin iv to oral conversion P.O. Box 189 Navan, ON, K4B 1J4 Canada. Sitemap
 Telephone 613-835-9490 Clindamycin iv to oral conversion P.O. Box 189 Navan, ON, K4B 1J4 Canada Sitemap 12-3-2018 Healthy people commonly aspirate small amounts of oral secretions, but normal defense mechanisms
Telephone 613-835-9490 Clindamycin iv to oral conversion P.O. Box 189 Navan, ON, K4B 1J4 Canada Sitemap 12-3-2018 Healthy people commonly aspirate small amounts of oral secretions, but normal defense mechanisms