Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
|
|
|
- Jordan Skinner
- 5 years ago
- Views:
Transcription
1 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe

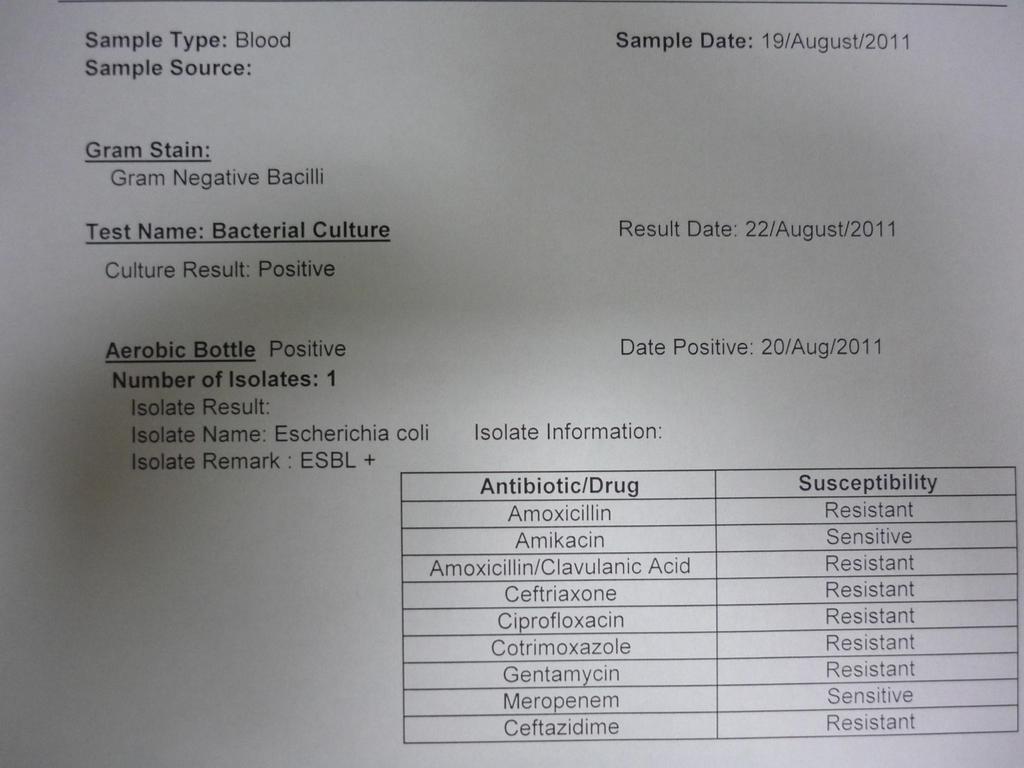
2 Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic treatment: ceftriaxone +/- amikacin RISK FACTORS FOR ESBL+ E coli Older age History of UTI Presence of urinary catheter History of recent urological surgery Recent intake of antibiotics
3 Another 2 d later Blood culture: Escherichia coli Urine culture: Escherichia coli Antibiogram: Amoxicillin R Amoxicillin/clavulanic acid S Amikacin S Ceftriaxone S Ceftazidime S Cotrimoxazole R Ciprofloxacin S Gentamicin R Meropenem S
4 Which treatment will you give now? PO amoxycillin IV amoxycillin PO amoxycillin-clavulanic acid IV ciprofloxacin PO ciprofloxacin IV ceftriaxone IV ceftriaxone + amikacin IV meropenem
5 Another 2 d later Antibiogram: Amoxicillin R Amoxicillin/clavulanic acid S Amikacin S Ceftriaxone S Ceftazidime S Cotrimoxazole R Ciprofloxacin S Gentamicin R Meropenem S IV ceftriaxone 2 g qd or IV ciprofloxacin 500 mg q12 If no more fever 48 h: PO ciprofloxacin 500 mg q12 Total duration 7-10 days
6 But imagine another patient Another antibiogram: Amoxicillin R Amoxicillin/clavulanic acid S Amikacin S Ceftriaxone R Ceftazidime R Cotrimoxazole R Ciprofloxacin R Gentamicin R Meropenem S
7 Which treatment will you give now? PO amoxycillin IV amoxycillin PO amoxycillin-clavulanic acid IV ciprofloxacin PO ciprofloxacin IV ceftriaxone IV ceftriaxone + amikacin IV meropenem
8 Amoxicillin R Amoxicillin/clavulanic acid S Amikacin S Ceftriaxone R Ceftazidime R Cotrimoxazole R Ciprofloxacin R Gentamicin R Meropenem S Ceftriaxone R suggest presence of ESBL = resistance for all beta-lactam drugs (exc. Carbapenem, cefepime) =often co-resistance to ciprofloxacin, gentamicin, cotrimoxazole Here you need to use Meropenem 1 g q8 x 10 d


9 Case 3 15 year old female student 10 d high fever, abdominal pain BP 82/43 mmhg RR 24/, O2 Sat 97%, temp 39.3 C Hb 11.9 g/dl WBC 7200/µl sgot/sgpt 91/28 Malaria smear negative CXR negative


10 2 days later Persisting high fever and abdominal pain Blood cultures show Gram negative bacilli
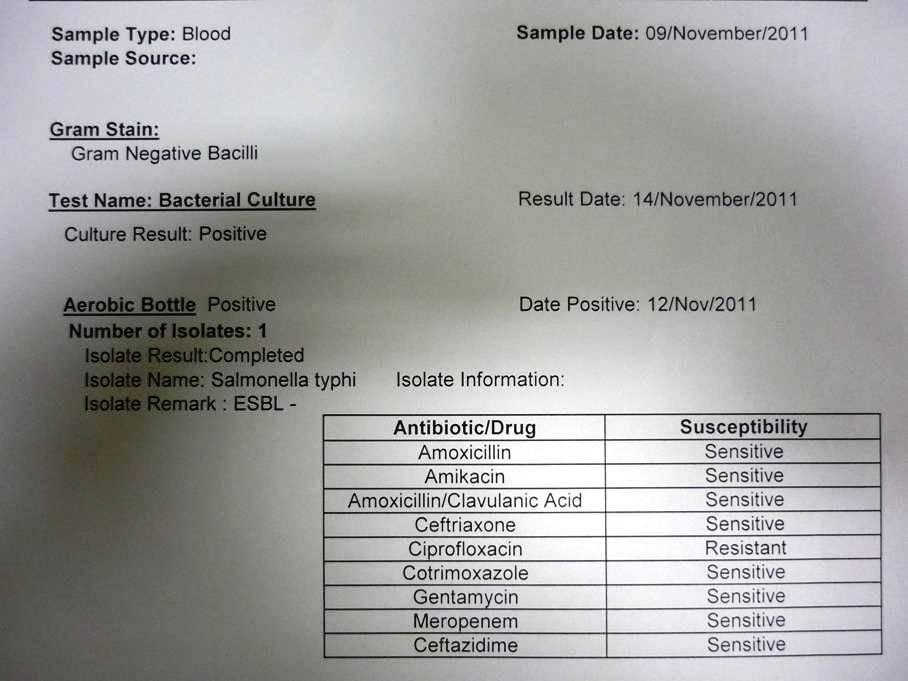
11 Another 2 days later Blood cultures Salmonella Typhi Antibiogram Ampicillin R Amoxycillin-clavulanic acid I Cotrimoxazole R Chloramphenicol R Ciprofloxacin R Ceftriaxone S
12 Which treatment do you give? PO amoxycillin PO Augmentin PO ciprofloxacin IV ceftriaxone IV imipenem IV vancomycin
13 Which treatment do you give? PO amoxycillin PO Augmentin PO ciprofloxacin IV ceftriaxone IV imipenem IV vancomycin
14 But imagine another typhoid patient: Blood cultures Salmonella Typhi Antibiogram Ampicillin R Amoxycillin-clavulanic acid I Cotrimoxazole R Chloramphenicol R Nalidixic acid S Ciprofloxacin S Ceftriaxone S
15 Which treatment do you give? PO amoxycillin PO Augmentin PO ciprofloxacin IV ceftriaxone IV imipenem IV vancomycin
16 Which treatment do you give? PO amoxycillin PO Augmentin PO ciprofloxacin IV ceftriaxone IV imipenem IV vancomycin
17 Salmonella Typhi If possible, treat with ciprofloxacin If nalidixic acid R cipro R Then: IV ceftriaxone 2 g qd x 10 d Or PO azithromycin 1000 mg d1, then 500 mg/d x 7 d

18 Case 4 40 y/o man Prey Veng History DMII (3years) Malaria in 1980 Liver abscess (4 & 2 months ago) Medication: herbal medicine Amoxicillin Diamicron. No known allergy His wife and 3 children are healthy
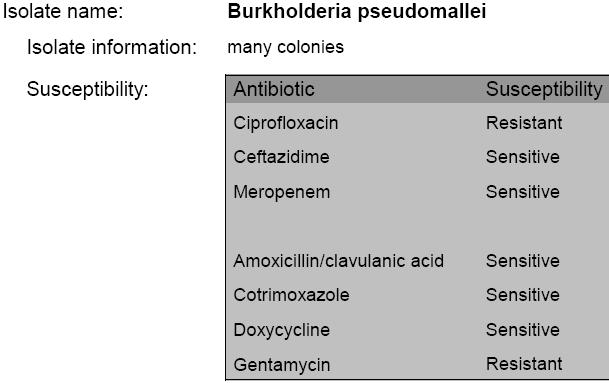
19 Evolution amoxycillin (2 w) no improvement Ceftriaxone + metronidazole (5d) no improvement Blood cultures: Burkholderia pseudomallei
20
21 How to treat? Continue IV ceftriaxone + metronidazole Switch to IV Augmentin Switch to IV ceftazidime Switch to IV cotrimoxazole Switch to IV chloramphenicol + amikacin other
22 How to treat? Continue IV ceftriaxone + metronidazole Switch to IV Augmentin Switch to IV ceftazidime Switch to IV cotrimoxazole Switch to IV chloramphenicol + amikacin other
23 Melioidosis: intensive phase IV ceftazidime 50mg/kg up to 2g q6 x minimum 10 days IF NO CEFTAZIDIME: IV Augmentin 20/5 mg/kg q4 at least 10 days OR IV/PO cotrimoxazole (IV or PO 8/40mg/kg q12 up to 320/1600mg q12) +/- doxycycline 2.5 mg/kg up to 100mg q12 (dose) OR IV ceftriaxone (at larger doses than usual 50mg/kg up to 2g qd) at least 10 days + cotrimoxazole (IV or PO 8/40mg/kg q12 up to 320/1600mg q12)
24 Melioidosis: continuation phase Cotrimoxazole 8/40mg/kg up to 320/1600mg q12 x at least 3 months (= 12 weeks) OR For children and pregnant women: Augmentin 20/5mg/kg up to 1500/375mg q8 x at least 3 months (=12 weeks) may need treatment for 6 months
25 Evolution Clinical improvement, no more fever on 08/06/ : switch to Cotrimoxazole with Doxycyclin and discharge home Ambulatory follow up for Melioidosis treatment and diabetes: he was ok at followup on 26/07/10.

26 Interpretation of antibiograms
27 Step by step 1. Look for the name of the bacteria 2. Look for the first choice antibiotic 3. If S prescribe this 4. If R second choice antibiotic 5. If possible, de-escalate
28 1. Look for the name of the bacteria Is this a true pathogen (causing the disease) e.g. Staphylococcus aureus Choose antibiotics! E coli and other Gram negative bacilli Or is this more likely a contaminant e.g. Coagulase negative Staphylococci Bacillus Corynebacterium No antibiotics needed!!
29 2. Look for the first choice antibiotic Each bacterium has first choice antibiotics Best activity, smallest spectrum, Should be written in treatment guideline Staphylococcus aureus cloxacillin Pneumococ penicillin G Salmonella species ciprofloxacin E. coli ciprofloxacin, ampicillin, Augmentin
30 3. If the first choice AB shows S Then you prescribe the first choice AB! According to your local guidelines & availability With the smallest spectrum possible Dose according to the disease severity e.g. S aureus causing skin infection» Cloxacillin PO 500 mg q6 S aureus causing blood stream infection/sepsis» Cloxacillin IV 1-2 g q4-6
31
32 4. If the first choice shows R Use the second choice antibiotic As listed in guidelines Or: with known good activity against this bacterium AND with the smallest spectrum possible
33
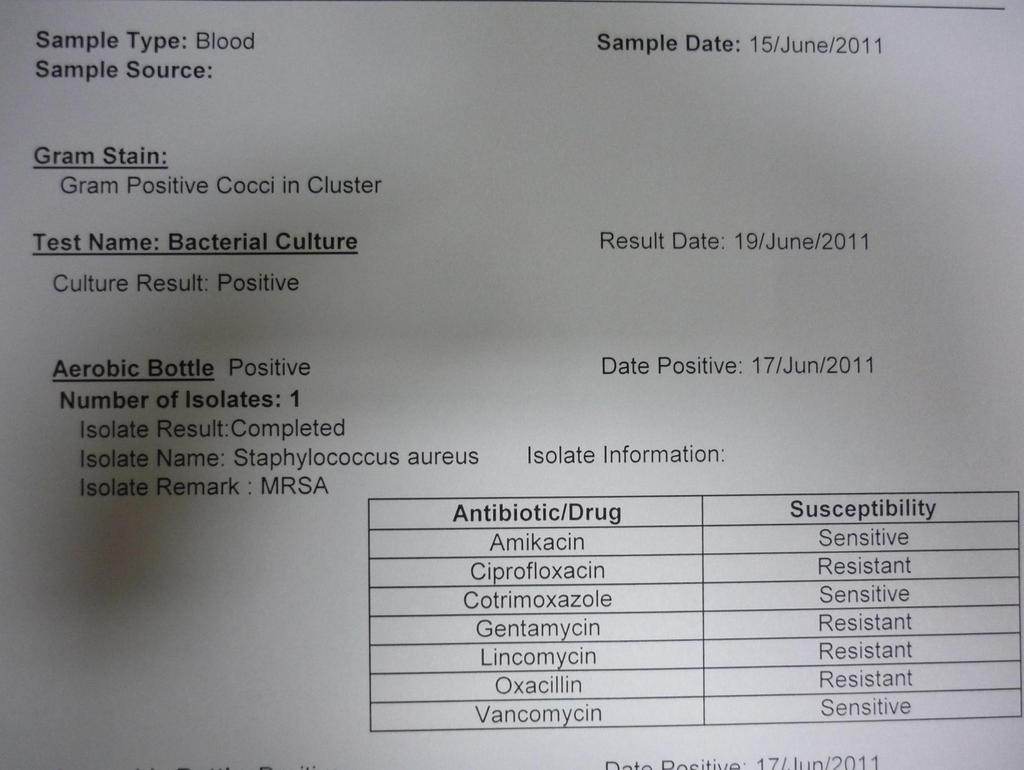
34 Example1: Staphylococcus aureus Cloxacillin R (MRSA) Serious infection use vancomycin if possible Mild infection use cotrimoxazole (or lincomycin) if S
35
36 Example 2: E. coli Ampicillin R use Augmentin or ciprofloxacin Ciprofloxacin R use Augmentin (if S) or Ceftriaxone Augmentin R check if also Ceftriaxone R (likely ESBL+) use ciprofloxacin, cotrimoxazole (if S) if all other AB R: use meropenem (if available) Ceftriaxone R serious infections: use meropenem (if available) mild infections: use cotrimoxazole, ciprofloxacin (if S) UTI: use nitrofurantoin (if S) Use only meropenem if serious and if you have no other possibility
37



38 Beta-lactamases
39 ESBL Extended spectrum beta-lactamase Treatment options: Severe disease: carbapenem( meropenem or imipenem) amikacin (use ALWAYS in combination) Moderate disease: Is treatment necessary, is I&D alone enough, Check if you can use cotrimoxazole or ciprofloxacin Only if no other option use carbapenem UTI: nitrofurantoin (if S )

40 4. If possible, de-escalate: Treatment simplification/narrowing of microbiological spectrum Narrowing the spectrum Kill the bacteria as selectively as possible Use the least toxic, easiest and most affordable drug BROAD SPECTRUM ANTIBIOTIC NARROW SPECTRUM ANTIBIOTIC
41 Broad spectrum AB Ceftriaxone Amoxyclavulanate Piperacillin-tazobactam Meropenem Examples Narrow spectrum AB Cloxacillin (for Staphylococci) Ampicillin, penicillin (for Streptococci) Temocillin (for E. coli)
42 Examples of de-escalation Staphylococcus aureus, methicillin sensitive (MSSA) IV/PO flucloxacilline (Floxapen ) Streptococcus pneumoniae, penicillin susceptible S) IV Penicilline/amoxycilline Salmonella Typhi, ciprofloxacin sensitive ciprofloxacin, (azithromycin) E. coli: more difficult. Depends on antibiogram IV temocillin, PO ciprofloxacine, (IV/PO amoxyclavulanate)
43 Usual duration of treatment Bacteremia (blood stream infection): days Typhoid fever: 7-10 days Community acquired pneumonia: 7 days UTI: 3-5 days 7 d if nitrofurantoin used Skin and soft tissue infection: 7 days Meningitis: days 21 d if Streptococcus suis, S. aureus, Listeria, Pseudomonas) Osteomyelitis/septic arthritis: 4-6 weeks
44 Usual doses (1) Ampicillin For (suspected) endocarditis: 1-2 g q4-6 IV For mild/local infections: 1 g q8 PO Augmentin For respiratory tract: 1 g q8 PO For urinary/abdominal: 500 mg q6-8 PO For melioidosis: 1 g q4-6 IV Azithromycin For typhoid fever mg qd PO Cloxacillin For bacteremia/endocarditis: 1-2 g q4-6 IV For skin/soft tissue infection: 500 mg q6 PO
45 Usual doses (2) Ciprofloxacin: 500 mg q12 Cotrimoxazole For MRSA and Gram-negative infections: 5/25 mg/kg q12 For melioidosis: 8/40 mg/kg q12 Ceftriaxone For meningitis 2 g q12 For other indications 2 g qd Ceftazidime For melioidosis: 1 g q8 Meropenem: 1 g q8 (ONLY FOR SEVERE INFECTIONS) Nitrofurantoin: 100 mg q8 x 7 days (UTI ONLY)
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
2012 ANTIBIOGRAM. Central Zone Former DTHR Sites. Department of Pathology and Laboratory Medicine
 2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
21 st Expert Committee on Selection and Use of Essential Medicines Peer Review Report Antibiotics Review
 (1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
(1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS
 PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient
 1 Chapter 79, Self-Assessment Questions 1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient with normal renal function is: A. Trimethoprim-sulfamethoxazole B. Cefuroxime
1 Chapter 79, Self-Assessment Questions 1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient with normal renal function is: A. Trimethoprim-sulfamethoxazole B. Cefuroxime
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Antimicrobial Susceptibility Testing: Advanced Course
 Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Help with moving disc diffusion methods from BSAC to EUCAST. Media BSAC EUCAST
 Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
2015 Antibiogram. Red Deer Regional Hospital. Central Zone. Alberta Health Services
 2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
Antimicrobial susceptibility
 Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
2017 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
QUICK REFERENCE. Pseudomonas aeruginosa. (Pseudomonas sp. Xantomonas maltophilia, Acinetobacter sp. & Flavomonas sp.)
") Pseudomonas aeruginosa (Pseudomonas sp. Xantomonas maltophilia, Acinetobacter sp. & Flavomonas sp.) Description: Greenish gray colonies with some beta-hemolysis around each colony on blood agar (BAP),
Pseudomonas aeruginosa (Pseudomonas sp. Xantomonas maltophilia, Acinetobacter sp. & Flavomonas sp.) Description: Greenish gray colonies with some beta-hemolysis around each colony on blood agar (BAP),
RCH antibiotic susceptibility data
 RCH antibiotic susceptibility data The following represent RCH antibiotic susceptibility data from 2008. This data is used to inform antibiotic guidelines used at RCH. The data includes all microbiological
RCH antibiotic susceptibility data The following represent RCH antibiotic susceptibility data from 2008. This data is used to inform antibiotic guidelines used at RCH. The data includes all microbiological
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
EUCAST recommended strains for internal quality control
 EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
2016 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Rational use of antibiotics
 Rational use of antibiotics Uga Dumpis MD, PhD,, DTM Stradins University Hospital Riga, Latvia ugadumpis@stradini.lv BALTICCARE CONFERENCE, PSKOV, 16-18.03, 18.03, 2006 Why to use antibiotics? Prophylaxis
Rational use of antibiotics Uga Dumpis MD, PhD,, DTM Stradins University Hospital Riga, Latvia ugadumpis@stradini.lv BALTICCARE CONFERENCE, PSKOV, 16-18.03, 18.03, 2006 Why to use antibiotics? Prophylaxis
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
National Surveillance of Antimicrobial Resistance
 National Surveillance of Antimicrobial Resistance Report to Ministry of Health by Sri Lanka College of Microbiologists SLCM ARSP & NLBSA Technical Committees December 2014 National Surveillance of Antimicrobial
National Surveillance of Antimicrobial Resistance Report to Ministry of Health by Sri Lanka College of Microbiologists SLCM ARSP & NLBSA Technical Committees December 2014 National Surveillance of Antimicrobial
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Antimicrobial Stewardship Strategy: Antibiograms
 Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Routine internal quality control as recommended by EUCAST Version 3.1, valid from
 Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
Antibiotic Usage Guidelines in Hospital
 SUPPLEMENT TO JAPI december VOL. 58 51 Antibiotic Usage Guidelines in Hospital Camilla Rodrigues * Use of surveillance data information of Hospital antibiotic policy guidelines from Hinduja Hospital. The
SUPPLEMENT TO JAPI december VOL. 58 51 Antibiotic Usage Guidelines in Hospital Camilla Rodrigues * Use of surveillance data information of Hospital antibiotic policy guidelines from Hinduja Hospital. The
Dr. Shaiful Azam Sazzad. MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College
 Critical Care Medicine Dhaka Medical College") Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
number Done by Corrected by Doctor Dr.Malik
 number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
CUMULATIVE ANTIBIOGRAM
 BC Children s Hospital and BC Women s Hospital & Health Centre CUMULATIVE ANTIBIOGRAM 2017 Division of Medical Microbiology Department of Pathology and Laboratory Medicine Page 1 of 5 GRAM-POSITIVE BACTERIA
BC Children s Hospital and BC Women s Hospital & Health Centre CUMULATIVE ANTIBIOGRAM 2017 Division of Medical Microbiology Department of Pathology and Laboratory Medicine Page 1 of 5 GRAM-POSITIVE BACTERIA
Intro Who should read this document 2 Key practice points 2 Background 2
 Antibiotic Guidelines: Obstetric Anti-Infective Prescribing Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Kelly Alexander / Frances Garraghan
Antibiotic Guidelines: Obstetric Anti-Infective Prescribing Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Kelly Alexander / Frances Garraghan
Antimicrobial Chemotherapy
 2016 edition by Claudine El-Beyrouty, PharmD, BCPS Department of Pharmacy Thomas Jefferson University Hospital Brian Roslund, PharmD, BCPS, AQ-ID Department of Pharmacy Thomas Jefferson University Hospital
2016 edition by Claudine El-Beyrouty, PharmD, BCPS Department of Pharmacy Thomas Jefferson University Hospital Brian Roslund, PharmD, BCPS, AQ-ID Department of Pharmacy Thomas Jefferson University Hospital
FOLLOWING BUNDLE ADMINISTERED WITHIN ONE HOUR.
 Patient label DATE and TIME: 1 REVIEW BY Emergency Department SENIOR REGISTRAR (ED BLEEP 5999) +/-Leave Proforma 2 FOLLOWING BUNDLE ADMINISTERED WITHIN ONE HOUR. Bloods for FBC, U+E, CRP, LFT s, Clotting
Patient label DATE and TIME: 1 REVIEW BY Emergency Department SENIOR REGISTRAR (ED BLEEP 5999) +/-Leave Proforma 2 FOLLOWING BUNDLE ADMINISTERED WITHIN ONE HOUR. Bloods for FBC, U+E, CRP, LFT s, Clotting
Cipro for gram positive cocci in urine
 Buscar... Cipro for gram positive cocci in urine 20-6-2017 Pneumonia can be generally defined as an infection of the lung parenchyma, in which consolidation of the affected part and a filling of the alveolar
Buscar... Cipro for gram positive cocci in urine 20-6-2017 Pneumonia can be generally defined as an infection of the lung parenchyma, in which consolidation of the affected part and a filling of the alveolar
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
ß-lactams. Sub-families. Penicillins. Cephalosporins. Monobactams. Carbapenems
 β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
2010 ANTIBIOGRAM. University of Alberta Hospital and the Stollery Children s Hospital
 2010 ANTIBIOGRAM University of Alberta Hospital and the Stollery Children s Hospital Medical Microbiology Department of Laboratory Medicine and Pathology Table of Contents Page Introduction..... 2 Antibiogram
2010 ANTIBIOGRAM University of Alberta Hospital and the Stollery Children s Hospital Medical Microbiology Department of Laboratory Medicine and Pathology Table of Contents Page Introduction..... 2 Antibiogram
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles
 Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
National Clinical Guideline Centre Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults
 National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
3/20/2011. Code 215 of Hammurabi: If a physician performed a major operation on
 The Good Antibiotics: the Good, the Bad and the Ugly John P. Cello, MD Professor of Medicine and Surgery, University of California, San Francisco Most organisms can be readily identified by culture, special
The Good Antibiotics: the Good, the Bad and the Ugly John P. Cello, MD Professor of Medicine and Surgery, University of California, San Francisco Most organisms can be readily identified by culture, special
These recommendations were approved for use by the Pharmaceutical and Therapeutics Committee, RCWMCH on 1 February 2017.
 Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
2009 ANTIBIOGRAM. University of Alberta Hospital and the Stollery Childrens Hospital
 2009 ANTIBIOGRAM University of Alberta Hospital and the Stollery Childrens Hospital Division of Medical Microbiology Department of Laboratory Medicine and Pathology 2 Table of Contents Page Introduction.....
2009 ANTIBIOGRAM University of Alberta Hospital and the Stollery Childrens Hospital Division of Medical Microbiology Department of Laboratory Medicine and Pathology 2 Table of Contents Page Introduction.....
EAGAR Importance Rating and Summary of Antibiotic Uses in Humans in Australia
 EAGAR Importance Rating and Summary of Antibiotic Uses in Humans in Australia Background The Expert Advisory Group on Antimicrobial Resistance of the NH&MRC provides advice to Australian governments and
EAGAR Importance Rating and Summary of Antibiotic Uses in Humans in Australia Background The Expert Advisory Group on Antimicrobial Resistance of the NH&MRC provides advice to Australian governments and
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Bacterial Pathogens in Urinary Tract Infection and Antibiotic Susceptibility Pattern from a Teaching Hospital, Bengaluru, India
 ISSN: 2319-7706 Volume 4 Number 11 (2015) pp. 731-736 http://www.ijcmas.com Original Research Article Bacterial Pathogens in Urinary Tract Infection and Antibiotic Susceptibility Pattern from a Teaching
ISSN: 2319-7706 Volume 4 Number 11 (2015) pp. 731-736 http://www.ijcmas.com Original Research Article Bacterial Pathogens in Urinary Tract Infection and Antibiotic Susceptibility Pattern from a Teaching
جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی
 جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی ویرایش دوم بر اساس ed., 2017 CLSI M100 27 th تابستان ۶۹۳۱ تهیه
جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی ویرایش دوم بر اساس ed., 2017 CLSI M100 27 th تابستان ۶۹۳۱ تهیه
Responsible use of antibiotics
 Responsible use of antibiotics Uga Dumpis MD, PhD Department of Infectious Diseases and Infection Control Pauls Stradiņs Clinical University Hospital Challenges in the hospitals Antibiotics are still effective
Responsible use of antibiotics Uga Dumpis MD, PhD Department of Infectious Diseases and Infection Control Pauls Stradiņs Clinical University Hospital Challenges in the hospitals Antibiotics are still effective
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
a. 379 laboratories provided quantitative results, e.g (DD method) to 35.4% (MIC method) of all participants; see Table 2.
 to 35.4% (MIC method) of all participants; see Table 2.") AND QUANTITATIVE PRECISION (SAMPLE UR-01, 2017) Background and Plan of Analysis Sample UR-01 (2017) was sent to API participants as a simulated urine culture for recognition of a significant pathogen colony
AND QUANTITATIVE PRECISION (SAMPLE UR-01, 2017) Background and Plan of Analysis Sample UR-01 (2017) was sent to API participants as a simulated urine culture for recognition of a significant pathogen colony
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE FOR HEALTHCARE ACQUIRED CEREBROSPINAL FLUID SHUNT ASSOCIATED INFECTIONS
 Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE FOR HEALTHCARE ACQUIRED CEREBROSPINAL FLUID SHUNT ASSOCIATED INFECTIONS FINAL November 29, 2017 Working Group: Joanne Langley (Chair),
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE FOR HEALTHCARE ACQUIRED CEREBROSPINAL FLUID SHUNT ASSOCIATED INFECTIONS FINAL November 29, 2017 Working Group: Joanne Langley (Chair),
number Done by Corrected by Doctor
 number 28 Done by Dina Yaseen Corrected by حسام أبو عوض Doctor مالك الزحلف Cephalosporins -Cephalosporins are β-lactam antibiotics isolated from a strain of Streptomyces. -They are bactericidal and work
number 28 Done by Dina Yaseen Corrected by حسام أبو عوض Doctor مالك الزحلف Cephalosporins -Cephalosporins are β-lactam antibiotics isolated from a strain of Streptomyces. -They are bactericidal and work
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
** the doctor start the lecture with revising some information from the last one:
 Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Antimicrobial Susceptibility Testing: The Basics
 Antimicrobial Susceptibility Testing: The Basics Susan E. Sharp, Ph.D., DABMM, FAAM Director, Airport Way Regional Laboratory Director, Regional Microbiology and Molecular Infectious Diseases Laboratories
Antimicrobial Susceptibility Testing: The Basics Susan E. Sharp, Ph.D., DABMM, FAAM Director, Airport Way Regional Laboratory Director, Regional Microbiology and Molecular Infectious Diseases Laboratories
Medicinal Chemistry 561P. 2 st hour Examination. May 6, 2013 NAME: KEY. Good Luck!
 Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Cell Wall Weakeners. Antimicrobials: Drugs that Weaken the Cell Wall. Bacterial Cell Wall. Bacterial Resistance to PCNs. PCN Classification
 Cell Wall Weakeners Antimicrobials: Drugs that Weaken the Cell Wall Beta Lactams Penicillins Cephalosporins Carbapenems Aztreonam Vancomycin Teicoplanin Bacterial Cell Wall Bacterial cytoplasm is hypertonic
Cell Wall Weakeners Antimicrobials: Drugs that Weaken the Cell Wall Beta Lactams Penicillins Cephalosporins Carbapenems Aztreonam Vancomycin Teicoplanin Bacterial Cell Wall Bacterial cytoplasm is hypertonic
DRAFT DRAFT. Paediatric Antibiotic Prescribing Guideline. May
 Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Detection of ESBL Producing Gram Negative Uropathogens and their Antibiotic Resistance Pattern from a Tertiary Care Centre, Bengaluru, India
 ISSN: 2319-7706 Volume 4 Number 12 (2015) pp. 578-583 http://www.ijcmas.com Original Research Article Detection of ESBL Producing Gram Negative Uropathogens and their Antibiotic Resistance Pattern from
ISSN: 2319-7706 Volume 4 Number 12 (2015) pp. 578-583 http://www.ijcmas.com Original Research Article Detection of ESBL Producing Gram Negative Uropathogens and their Antibiotic Resistance Pattern from
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Septicaemia Definitions 1
 Septicaemia Definitions 1 Term Definition Bacteraemia Systemic Inflammatory response (SIRS) Sepsis Bacteria that can be cultured from the blood stream The systemic response to a wide range of stresses.
Septicaemia Definitions 1 Term Definition Bacteraemia Systemic Inflammatory response (SIRS) Sepsis Bacteria that can be cultured from the blood stream The systemic response to a wide range of stresses.
ESBL Positive E. coli and K. pneumoneae are Emerging as Major Pathogens for Urinary Tract Infection
 ESBL Positive E. coli and K. pneumoneae are Emerging as Major Pathogens for Urinary Tract Infection Muhammad Abdur Rahim*, Palash Mitra*. Tabassum Samad*. Tufayel Ahmed Chowdhury*. Mehruba Alam Ananna*.
ESBL Positive E. coli and K. pneumoneae are Emerging as Major Pathogens for Urinary Tract Infection Muhammad Abdur Rahim*, Palash Mitra*. Tabassum Samad*. Tufayel Ahmed Chowdhury*. Mehruba Alam Ananna*.
National Antimicrobial Prescribing Survey
 Indication documented Surgical prophylaxis >24 hrs Allergy mismatch Microbiology mismatch Incorrect route Incorrect dose/frequency Incorrect duration Therapeutic Guidelines Local guidelines * Non-compliant
Indication documented Surgical prophylaxis >24 hrs Allergy mismatch Microbiology mismatch Incorrect route Incorrect dose/frequency Incorrect duration Therapeutic Guidelines Local guidelines * Non-compliant
Acute Pyelonephritis POAC Guideline
 Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
Understanding the Hospital Antibiogram
 Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how?
 Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Guidelines for the Empirical Treatment of Sepsis in Adults (excluding Neutropenic Sepsis)
") Guidelines for the Empirical Treatment of Sepsis in Adults (excluding Neutropenic Sepsis) Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state
Guidelines for the Empirical Treatment of Sepsis in Adults (excluding Neutropenic Sepsis) Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance
 Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
BACTERIAL SUSCEPTIBILITY REPORT: 2016 (January 2016 December 2016)
") BACTERIAL SUSCEPTIBILITY REPORT: 2016 (January 2016 December 2016) VA Palo Alto Health Care System April 14, 2017 Trisha Nakasone, PharmD, Pharmacy Service Russell Ryono, PharmD, Public Health Surveillance
BACTERIAL SUSCEPTIBILITY REPORT: 2016 (January 2016 December 2016) VA Palo Alto Health Care System April 14, 2017 Trisha Nakasone, PharmD, Pharmacy Service Russell Ryono, PharmD, Public Health Surveillance
Optimizing Selection of Empirical Antimicrobial Therapy in the Era of Precision Medicine
 Optimizing Selection of Empirical Antimicrobial Therapy in the Era of Precision Medicine Majdi Al-Hasan, MBBS Associate Professor of Medicine University of South Carolina School of Medicine Disclosure
Optimizing Selection of Empirical Antimicrobial Therapy in the Era of Precision Medicine Majdi Al-Hasan, MBBS Associate Professor of Medicine University of South Carolina School of Medicine Disclosure
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIII NUMBER 1 July 2008 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell, SM (ASCP), Marti Roe SM (ASCP), Ann-Christine Nyquist MD, MSPH Are the bugs winning? The 2007
VOLUME XXIII NUMBER 1 July 2008 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell, SM (ASCP), Marti Roe SM (ASCP), Ann-Christine Nyquist MD, MSPH Are the bugs winning? The 2007
Meropenem for all? Midge Asogan ICU Fellow (also ID AT)
") Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Cellulitis. Assoc Prof Mark Thomas. Conference for General Practice Auckland Saturday 28 July 2018
 Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cipro for klebsiella uti
 Cipro for klebsiella uti Search Can UTI be an effective treatment for Klebsiella Pneumoniae? It is safe or dangerous to use UTI while suffering from Klebsiella Pneumoniae? 87 discussions on Treato. instock
Cipro for klebsiella uti Search Can UTI be an effective treatment for Klebsiella Pneumoniae? It is safe or dangerous to use UTI while suffering from Klebsiella Pneumoniae? 87 discussions on Treato. instock
your hospitals, your health, our priority PARC (Policy Approval and Ratification Committee) STANDARD OPERATING PROCEDURE:
 STANDARD OPERATING PROCEDURE:") STANDARD OPERATING PROCEDURE: TRUST ANTIBIOTIC TREATMENT SOP SOP NO: TW10/136 SOP 1 VERSION NO: VERSION 6.1 (JANUARY 2013) APPROVING COMMITTEE: INFECTION PREVENTION AND CONTROL COMMITTEE DATE THIS VERSION
STANDARD OPERATING PROCEDURE: TRUST ANTIBIOTIC TREATMENT SOP SOP NO: TW10/136 SOP 1 VERSION NO: VERSION 6.1 (JANUARY 2013) APPROVING COMMITTEE: INFECTION PREVENTION AND CONTROL COMMITTEE DATE THIS VERSION
Super Bugs and Wonder Drugs: Protecting the One While Respecting the Many
 Super Bugs and Wonder Drugs: Protecting the One While Respecting the Many Vicki Stringfellow, MSN, CPNP-AC/PC Werner Division of Pediatric Critical Care University of Kentucky Lexington, KY Disclosure
Super Bugs and Wonder Drugs: Protecting the One While Respecting the Many Vicki Stringfellow, MSN, CPNP-AC/PC Werner Division of Pediatric Critical Care University of Kentucky Lexington, KY Disclosure
ADC 2016 Report on Bacterial Resistance in Cultures from SEHOS and General Practitioners in Curaçao
 ADC 216 Report on Bacterial Resistance in Cultures from SEHOS and General Practitioners in Curaçao Willemstad, November 217 Authors: Radjin Steingrover clinical microbiologist, head dpt. Microbiology ADC
ADC 216 Report on Bacterial Resistance in Cultures from SEHOS and General Practitioners in Curaçao Willemstad, November 217 Authors: Radjin Steingrover clinical microbiologist, head dpt. Microbiology ADC
INFECTIOUS DISEASES DIAGNOSTIC LABORATORY NEWSLETTER
 INFECTIOUS DISEASES DIAGNOSTIC LABORATORY NEWSLETTER University of Minnesota Health University of Minnesota Medical Center University of Minnesota Masonic Children s Hospital May 2017 Printed herein are
INFECTIOUS DISEASES DIAGNOSTIC LABORATORY NEWSLETTER University of Minnesota Health University of Minnesota Medical Center University of Minnesota Masonic Children s Hospital May 2017 Printed herein are
Doxycycline for enterococcus
 Doxycycline for enterococcus Antibiotic Options for Enterococcus Faecalis Infections. Farhan E. Abdulla 1, Essa M. Abdulla 2. ABSTRACT. Objective: Escalating resistance of enterococci to many. Linezolid
Doxycycline for enterococcus Antibiotic Options for Enterococcus Faecalis Infections. Farhan E. Abdulla 1, Essa M. Abdulla 2. ABSTRACT. Objective: Escalating resistance of enterococci to many. Linezolid