MDR/XDR TB. Barbara Seaworth, MD, FIDSA, FACP October 27, TB Intensive October 24 27, 2017 San Antonio, TX
|
|
|
- Penelope McCarthy
- 5 years ago
- Views:
Transcription
1 MDR/XDR TB Barbara Seaworth, MD, FIDSA, FACP October 27, 2017 TB Intensive October 24 27, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Barbara Seaworth, MD, FIDSA, FACP, has the following disclosures to make: No conflict of interests No relevant financial relationships with any commercial companies pertaining to this educational activity 1

2 Objective Improved Management of MDR/XDR TB Recognize which patients are at risk of MDR/XDR Discuss the recommendations for management of MDR/XDR TB Should I start treatment before I know the 2 nd line susceptibility results? How many drugs? Which ones? How long? How do I monitor for treatment response? Multiple Drug Resistant TB (MDR TB) TB resistant to both INH and Rifampin Extensively Drug Resistant TB (XDR TB) MDR TB plus resistance to: Any fluoroquinolone and Second line injectable Capreomycin Kanamycin Amikacin Pre XDR TB MDR TB plus resistance to: Any fluoroquinolone or Second line injectable Capreomycin Kanamycin Amikacin 2


3 CDC March 2014 WHO 2014 Report: TB Epidemic Even Bigger Than We Thought 9.0 million new cases of TB 500,000 more TB cases than previously estimated 1.5 million deaths (4000 each day) Estimated 480,000 new MDR TB cases in 2013 (9% are XDR) 3


4 10/27/2017 In 2015 estimated 10.4 million new TB Cases worldwide 1.8 Million died 300,000 more than a year earlier ~ 480,000 had a new diagnosis of MDR TB about half in India, China and Russian Federation only 125,000 (20%) enrolled in treatment ~ 100,000 additional people with rifampicin resistant TB Globally MDR treatment success rate was 52% and 28% for XDR TB in 2013 WHO Global Report 2016 WHO 2016 Global TB Report 4
5 CLASSIFICATION OF DRUG RESISTANCE PRIMARY DRUG RESISTENCE No previous treatment First isolate a person has is drug resistant ACQUIRED DRUG RESISTENCE Resistance develops during inadequate treatment Pathway to Drug Resistance Gandhi Lancet May
6 Why Do We Have Drug Resistant TB? Increase In Streptomycin Resistant Mutants During Monotherapy Weeks of treatment SM-resistant mutants SM-resistant mutants (%) 0 (before) 1 / 88, / 13, / / / Pyle M. Proc Mayo Clinic 1947;22:465 6
7 Isoniazid Resistance After 2 Months of Isoniazid Monotherapy Retrospective analysis from isoniazid treatment trial 1952 among patients with drug susceptible isolates before starting #Patients Cavities %Cult + % resistant % 22% % 40% % 61% % 87% Fox W, Sutherland I. Thorax 1955;10: /27/ WHO and National TB Program Policies Led to High Rates of MDR TB Global standard practice diagnosis by smear only No culture or susceptibility tests Drug resistance is not recognized Inadequate treatment is continued Standardized treatment regimens for those with failure This allows further AMPLIFICATION of resistance 7

8 DST Coverage Among New Cases and Enrolment on MDR TB Treatment Compared to Global Stop TB Targets WHO Global TB Report 2014 WHO Global TB Report



9 Countries that had reported at least one XDR TB case by Oct 2013 Countries with XDR TB 92 in in 2014 The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO All rights reserved 9
10 Risk of Acquired Drug Resistance During Treatment Does inadequate treatment of MDR XDR? PETTS Study n(%) Cure/Comp Failure Death Green Light 585 (65) 47 (5.2) 82 (9.1) Programatic 373 (52.7) 55 (7.8) 145 (20.5) Emergence of XDR GLC 21% non GLC 51% Emergence of FQN R GLC 10.1% non GLC 20.8% PETTS : Preserving Effective TB Treatment Study, Dalton et al. Lancet epub August 30, 2012 Predicting the Growth of XDR TB Inadequate treatment of MDR TB leads to more XDR TB! MDR Cases That Are XDR (%) Detected and Treated MDR Cases (%) Blower Lancet Inf Dis 2007;7:443 10

11 Cegielski CID 2014 Cegielski CID

12 Cegielski CID /27/


13 January 2012 CID Proposed definitions are ambiguous. No evidence that proposed totally resistant TB differs from XDR TB. Susceptibility tests for several drugs are poorly reproducible. Few laboratories can test all drugs. No consensus list of all anti TB drugs. Many drugs are used off label. New drugs would render the proposed category obsolete. Labeling TB strains as totally drug resistant might lead providers to think infected patients are untreatable. 13
14 Susceptibility Studies First Line Resistant INH Rifampin Rifabutin PZA Ethambutol Streptomycin Second Line Resistant Amikacin Kanamycin Capreomycin Ethionamide Ofloxacin PAS Susceptibility Studies Susceptible Linezolid < 0.4 Cycloserine Clofazimine < 0.06 mcg/ml 4 drugs Moxi? Moxifloxacin = 1.0 mcg/ml Usually has MIC < 0.5 MIC of 1.0 is intermediately resistant but drug may have some efficacy due to ability to get high blood levels 14
15 Treatment Outcomes for MDR Global Cohorts Treatment success overall % WHO 2014 Global TB Report How Can We Do Better? Management Strategies Must be Individualized by Patient and Drug Susceptibility 15
16 Early Recognition of Which Patients are at Risk of MDR/XDR TB Those who were: Born/reside in a country with high incidence of drug resistant TB Exposed to a patient with relapse or failure Those with a history of Prior treatment for TB Treatment failure Clinical deterioration during 4 drug therapy Bad Bugs Primary XDR TB 56 yr old male, born in US no history of TB TST positive, abnormal CXR, Cough, fever, sweats, weight loss Culture + M TB Resistant to: INH, Rifampin, Rifabutin PZA Ethambutol Streptomycin, Capreomycin, Amikacin Levofloxacin Ethionamide 16


17 Acquired XDR TB Contact to father who died with MDR TB in 1994 Father s culture resistant to: INH, Rifampin, Rifabutin PZA Ethambutol Streptomycin, Capreomycin, Amikacin Ofloxacin Ethionamide Father was drug susceptible at first diagnosis! XDR TB Extensively Drug Resistant Tuberculosis control Isoniazid Ethambutol Rifampin control control Streptomycin Ethionamide Ofloxacin control control control Rifabutin Kanamycin Capreomycin 17


18 INH and ethambutol resistant TB patient referred to Binational Project still smear + after 2 months INH and Ethambutol Resistant TB Initial culture resistant to: INH, ethambutol At 10 weeks of therapy patient remains ill and AFB + Providers ask to add moxifloxacin Best approach? Always plan treatment so that further resistance does not occur Know what the current resistance pattern is now Stop therapy if possible and wait 18
19 Never Treat Active TB With A Single Drug! Never Add a Single Drug to a Failing Treatment Regimen! Always Use At Least 2 Drugs To Which The TB Is Susceptible. PZA only works on slowly growing MTB; it should not be counted as a 2 nd drug to protect Rifampin INH and Ethambutol Resistant TB Initial culture resistant to: Streptomycin, kanamycin, amikacin, and capreomycin plus INH and ethambutol At 10 weeks of therapy patient is still quite sick cough, poor appetite, no energy and positive smears Best approach? Be aggressive but know where you are starting new treatment from Do Xpert, molecular testing now on new specimen as well as culture and susceptibility test Add Moxifloxacin? 19

20 After two months of RIPE treatment, 2 nd culture new Rifampin resistance Resistance to INH, ethambutol Streptomycin, kanamycin, amikacin, and capreomycin PRE XDR TB! Pre XDR TB Aggressive new treatment regimen needed Adding Moxifloxacin would have been adding a single drug to a failing regimen and created XDR! New Immigrant Sick on Plane Burmese teenager with prior history of TB 20
21 Case Study: New Immigrant Coughing during flight to U.S., weight 76 pounds History of prior treatment in country of origin Sputum smear and later culture was positive for M TB Treatment: INH, Rifampin, EMB, PZA plus Moxifloxacin Resistant : INH, Rifampin, EMB, PZA Susceptible : ethionamide, levofloxacin, amikacin Never treat with a single drug! A key drug has been compromised New Immigrant Patient improves clinically after MDR regimen starts Gains 25 pounds Cough, fever, and night sweats resolve Smears and cultures convert at 12 weeks Last positive culture Moxifloxacin resistant Moxifloxacin can t be the strong drug to anchor treatment Repeat sensitivity on last positive culture to look for further resistance to plan treatment based on effective drugs! 21

22 How Does Detection of Genetic Mutations Causing Resistance Fit Into Management of a New TB Case? 22
 On all before treatment most cost effective strategy to avert deaths and prevent additional resistance U.S. qualifies!")
23 2016 WHO Guidelines (Updated2016) Rapid drug susceptibility testing (DST) of at least Rifampin is recommended over conventional testing or not testing in adults and children at the time of diagnosis of TB (Strong recommendation, high certainty in evidence) On all before treatment most cost effective strategy to avert deaths and prevent additional resistance U.S. qualifies! Should provide a diagnosis within two days of testing Only molecular tests meet this criterion 23
 Identify additional drug resistance to help build new treatment regimen Global Approach: Regard and treat")
24 Detection of Rifampin Resistance on Gene Xpert United States Approach: Confirm resistance in all cases by referral to CDC laboratory for full Sanger sequencing Exclude false positive rifampin, usually associated with failure of probe B to bind (your lab may be able to tell you this) Identify additional drug resistance to help build new treatment regimen Global Approach: Regard and treat the same as MDR TB Additional molecular testing if plan to use Short Course treatment regimen CDC Molecular Detection of Drug Resistance (MDDR) Testing (Sanger sequencing) Drug Gene Sensitivity (%) Specificity (%) Rifampin rpob INH inha + katg FQ gyra gyrb Kanamycin rrs + eis Amikacin rrs Capreomycin rrs + tlya



25 When Should an Empiric Treatment Regimen for MDR TB Be Started? If patient is stable and no high risk contacts in the home, it is best to wait until molecular tests suggest a viable regimen or 2 nd line susceptibility tests are available. If patient is unstable or small children in home, start treatment Most experts would often start with an aggressive regimen using molecular testing to guide choices 38 year old woman admitted in respiratory failure along U.S./Mexico border 25


 but may be resistant on agar Significance of these")
26 rpob mutation GAC>GTC; Asp516Val Mutation predicts Rifampin resistance but Rifabutin susceptibility Low level Resistance to Rifampin Some rpob mutations can cause low level resistance to rifampin* Mutation Rifampin MIC 511 Leu Pro 0.5 ug/ml 516 Asp Tyr 0.25 ug/ml Strains with these 2 mutations may test as susceptible in MGIT broth (test concentration is 1ug/ml) but may be resistant on agar Significance of these mutations not yet clear *Williamson, DA, et al IJTLD 16(2):216 26
 3/3 with rpob mutation failed 2/49 without rpob mutation failed Van Deun looked at")
 will likely overcome some low level resistance *Williamson, DA, et al. 2012. IJTLD 16(2):216 **Van Deun et al. 2009. J.Clin. Microb.")
27 Low Level Resistance to Rifampin Do MICs from lead to treatment failure? Williamson article* cites 3 treatment failure cases Retrospective study of INH resistant patients (49 cases) 3/3 with rpob mutation failed 2/49 without rpob mutation failed Van Deun looked at difficult isolates in CDC performance tests Those with rpob mutations Failed in 6 of 14 instances Relapsed after initial cure in 5/14. Clinical information not available in 2, One cure. Increased rifampin exposure (20mg/kg/day) will likely overcome some low level resistance *Williamson, DA, et al IJTLD 16(2):216 **Van Deun et al J.Clin. Microb. 47(11): 3501 *** Molecular Detection of Drug Resistance Shows XDR TB 24 yr immigrant prior TB therapy PZA resistance detected suspected INH, rifampin, EMB 3 days later MDDR notes XDR Ofloxacin resistant Ala90Val Moxifloxacin? Resistant to all injectable drugs Case about to start graduate school at time of diagnosis Hospitalized in isolation 27
 Low level rifampin resistance may be missed (treatment failure) Rifabutin susceptible strains may be missed May help predict susceptibility or")

28 When Can DNA Sequencing Help Better Characterize Susceptibility of an Isolate? Resistance to rifampin (rpob) Low level rifampin resistance may be missed (treatment failure) Rifabutin susceptible strains may be missed May help predict susceptibility or resistance to moxifloxacin in cases of ofloxacin resistance PZA results on MGIT may give false resistance repeat susceptibility test and request molecular test (pnca) Confirm EMB susceptibility for INH Resistant cultures MGIT may give falsely susceptible ethambutol results MDR TB Reported After 2 Months of Treatment with INH, Rifampin, Ethambutol, and PZA January, 2011 at diagnosis March 29, 2011 after 2 mo RX Smear negative but culture quickly becomes positive 28


29 F/U of MDR TB 4 Years After Standardized First Line Therapy New and retreatment MDR TB cases managed by standard treatment all treated 3 x/week RIPE x 2, Rif/INH x 4 : for new cases 83% cure RIPES x 2, Rif/INH/EMB x 6 : for retreatment 66% cure 4 years later: Recurrence: 61% Death due to TB: 36% Treatment with FLD is highly ineffective in curing MDR TB even if the reported cure rate is high initially Patients were evaluated for cure with sputum smears only He GX et al, PloS ONE, May
30 2011 WHO Guidelines Recommendations on the number of drugs in the regimen, use of specific drugs, and duration of therapy were: Guided by a meta analysis from 32 studies with > 9000 treatment episodes using pooled individual patient data XDR TB patients excluded Many studies used DST results to adjust drug regimen 2016 Guidelines updated the initial individual patient data (ipd) analysis New patients added to the group of > 9000 Although newer studies had different outcomes, did not impact outcomes when added to 2011 ipd Quality of evidence was judged to be low or very low Only cohorts with new drugs were randomized controlled trials Bias likely to be substantial certain drugs used for sicker patients Ahuja et al; Plos Medicine WHO Guidelines In Rifampin Resistant (RR) or MDR TB, a regimen with at least five effective TB medicines during the intensive phase is recommended, including PZA and 4 core 2 nd line drugs one chosen from group A, one from group B, and at least 2 from group C (conditional recommendation, very low certainty in evidence). If the minimum number of effective TB medicines cannot be composed as above, an agent from group D2 and other agents from D 3 may be added to bring the total to 5. In patients with RR or MDR TB it is recommended that the regimen be further strengthened with high dose INH and/or ethambutol. (conditional recommendation, very low certainty in evidence) 30
 Ethionamide/ Prothionamide Cycloserine/ Terizidone Clofazimine Linezolid D1: Pyrazinamide Ethambutol High dose INH D2: Bedaquiline Delamanid D3: P aminosalicylic acid")
31 New Grouping of MDR-TB Drugs Group A Group B Group C Group D Fluoroquinolone Second line Other Core Add on agents injectable Second line Levofloxacin Moxifloxacin Gatifloxacin Amikacin Capreomycin Kanamycin (Streptomycin) Ethionamide/ Prothionamide Cycloserine/ Terizidone Clofazimine Linezolid D1: Pyrazinamide Ethambutol High dose INH D2: Bedaquiline Delamanid D3: P aminosalicylic acid Imipenem/meropenem Amoxacillin/Clavulanate (Thioacetazone) 2016 WHO Guidelines In Rifampin Resistant (RR) or MDR TB, a regimen with at least five effective TB medicines during the intensive phase is recommended, including PZA and 4 core 2 nd line drugs one chosen from group A, one from group B, and at least 2 from group C (conditional recommendation, very low certainty in evidence). If the minimum number of effective TB medicines cannot be composed as above, an agent from group D2 and other agents from D 3 may be added to bring the total to 5. In patients with RR or MDR TB it is recommended that the regimen be further strengthened with high dose INH and/or ethambutol. (conditional recommendation, very low certainty in evidence) 31

32 2016 WHO Guidelines In MDR TB, Group C drugs should usually be added in the noted order: ethionamide, cycloserine, linezolid 32
 Peak in cure was later for those with prior therapy 27.6 30.")
33 2016 WHO Guidelines In MDR TB, the intensive phase should last at least 8 months (recommendation stands unchanged from 2011) In MDR TB, the total treatment duration should be at least 20 months in those with no prior MDR TB treatment (recommendation stands unchanged from 2011) Peak in cure was later for those with prior therapy months WHO Policy Recommendation Shorter Course MDR-TB Regimen Recommendation: In patients with RR or MDR-TB who have not been treated with second-line drugs and in whom resistance to FQNs and SLI agents has been excluded or is considered to be highly unlikely a shorter MDR-TB regimen of 9-12 mo may be used instead of a conventional regimen (conditional recommendation, very low certainty in the evidence) WHO 2016 Update 33
34 Short, Highly Effective and Inexpensive Standardized Treatment of MDR TB Prospective cohorts treated in Bangladesh for minimum 9 months Cohort # patients, mean BMI 16.1 kg Relapse free cure 87.9% Intensive phase 4 (+) months High dose gatifloxacin (800 mg if 50 kg) Kanamycin 4 months or until sputum conversion (17% extended) Prothionamide, PZA, high dose INH (600mg), ethambutol, clofazamine Continuation phase 5 months Gatifloxacin, PZA, ethambutol, clofazamine ( mg) Van Deun, Int J Resp Crit Care Med, 2010 Proportion with Successful Outcomes Gatifloxacin Clofazamine throughout No INH Van Deun, Int J Resp Crit Care Med,
35 Short Course Standardized Regimen for MDR-TB Regimen Intensive Continuation Number Cum. % Treatment Success % 1 3KCOEHZP 12 OEHZP (+)KCOEHZP 12 OEHZP (4)KCOEZP 12 OEZP (+)KCOEHZP 12 OHEZ (+)KCOEHZP 12 OHEZC (+)KCGEHZP 5 GEZC C = clofazimine, E = ethambutol, G = gatifloxacin, H = isoniazid, K = kanamycin, O = ofloxacin, P = prothionamide, Z = pyrazinamide 3(4) = minimum of 3 mos, prolonged to 4 months if no conversion by end of 3 mos 3(+) = minimum of 3 mos, prolonged until conversion achieved 4(+) = minimum of 4 mos, prolonged until conversion achieved Van Deun, et al. Am J Respir Crit Care Med 2010;182: Short(er) Course Regimen for MDR-TB Initial Phase (7 drugs) Continuation Phase (4 drugs) Moxifloxacin* Ethambutol Pyrazinamide Clofazimine Prothionamide Isoniazid* Kanamycin *High dose months 35
36 Treatment Success* Shorter vs. Conventional Regimens Resistance pattern Shorter MDR TB Regimen (N=1116) Conventional MDR TB Regimen (N = 5850) All cases 90.3% 78.3% PZA susceptible; 96.8% 83.5% FQN susceptible PZA resistant; 88.8% 81.4% FQN susceptible PZA susceptible; 80.0% 64.4% FQN resistant PZA resistant; FQN resistant 67.9% 59.1% *Treatment success cure or completed Decreasing success WHO 2016 Update WHO Treatment Guidelines for Drug Resistant TB 2016 Update A= In patients with rifampicin resistant or multidrug resistant TB who have not been previously treated with second line drugs and in whom resistance to fluoroquinolones and second line injectable agents has been excluded or is considered highly unlikely, a shorter MDR TB regimen of 9 12 months may be used instead of a conventional regimen (conditional recommendations, very low certainty in the evidence) Based on treatment success from individual patient data (1116 patients) from 14 African countries Shorter regimen 90.3% success vs 78.3% conventional regimen (all) Shorter regimen 96.8% success vs 83.5% conventional regimen (PZA/FQN S) Shorter regimen 76.9% success vs 59.1% conventional regimen (PZA/FQN R) 36
 N = 130 MDR-TB (36% of MDR-TB) and 5 XDR-TB (56% of XDR-TB) 4 drugs 6 drugs 8 drugs 11")
37 Choosing the MDR-TB Regimen MDR/XDR TB in the U.S. ( ) N = 130 MDR-TB (36% of MDR-TB) and 5 XDR-TB (56% of XDR-TB) 4 drugs 6 drugs 8 drugs 11 drugs Median Marks SM, et al. EID 2014:20:812 37
 Unfavorable 46 (21.9%) 21 (19.4%) Stream for MDR Safety Results 38")
38 Stream Outcome STUDY CONTROL Total Assessed Favorable 164 (78%) 87 (80.6%) Unfavorable 46 (21.9%) 21 (19.4%) Stream for MDR Safety Results 38


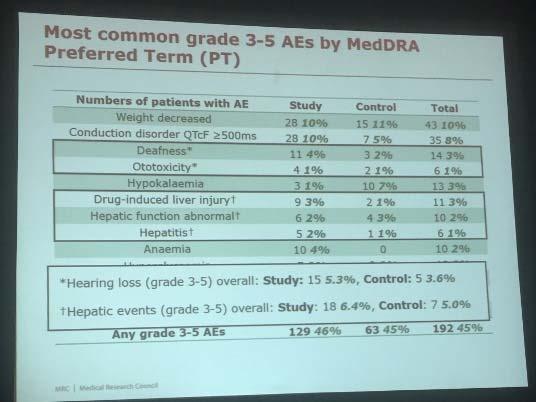
39 Stream for MDR Safety Results Stream for MDR Safety Results 39
 under operational research conditions.")
40 WHO Recommended Standardized Short Course Regimens and New Drugs At least 23 countries in African and Asia have introduced shorter regimen for treatment of MDR/RR TB Achieved high treatment success rates (87 90%) under operational research conditions. Intensive Phase: x 4 (to 6) months Moxifloxacin (H), Kanamycin, Prothionamide, Clofazimine, INH (H), PZA, and Ethambutol Injectable for 4 months, may extend to 6 if smear positive Continuation Phase x 5 months Moxifloxacin, Clofazimine, Ethambutol, PZA As part of efforts to improve outcomes for MDR/XDR TB, at least 70 countries had started using bedaquiline and 39 countries had used delamanid by the end of
41 WHO 2016 Update MDR TB Pediatric TB 2016 ipd of nearly 1000 children to inform recommendations In children with limited or culture negative MDR injectable dose not have to be included. High dose INH in children with low level INH resistance Linezolid 2016 Linezolid added as core drug Not addressed: XDR TB Chemoprophylaxis for contacts of MDR When Should Linezolid be Added? Core 2 nd line drug but often behind ethionamide and cycloserine in guidance. However with Extensive Drug Resistance, including XDR TB it should be used. Failed MDR TB therapy To make the strongest possible initial regimen? Patients on individualized therapy who have had 2 nd line drug susceptibility testing done Linezolid when included in a regimen was associated with culture conversion in most by 2 3 months and 81.8% were successfully treated Migliori ERJ 2012, 41
 of 38 patients had treatment failure: 2 patients in 300 mg group; 1 patient in 600 mg group 1 (3%) of 38 patients had treatment relapse")
42 Linezolid Added as Single Drug to Chronic MDR TB Culture Conversion Linezolid 600 mg daily added as only change in regimen at study start or after 4 months Lee NEJM Oct (89%) of 38 patients culture converted 6 months; median 75 days on Linezolid 3 (8%) of 38 patients had treatment failure: 2 patients in 300 mg group; 1 patient in 600 mg group 1 (3%) of 38 patients had treatment relapse 4 patients developed resistance Lee M, Lee J, Carrol MW, et al. N Engl J Med 2012;367(16):
43 Timing of Linezolid Toxicity Lee NEJM Oct 2012 Aggressive Regimen is Associated with Improved Outcomes Individualized based on 1 st /2 nd line susceptibility test results Use of drugs with proven or likely susceptibility, including 5 drugs including an injectable for 6 months after culture conversion 4 oral drugs including a FQN which should be given for months after culture conversion Mitnick, PLos One, March
44 Aggressive Regimen Outcomes Cure or completion in 66.1% of 669 patients Patients resistant to average of 5.4 drugs Only two had no prior therapy Such a regimen previously shown to decrease relapse (Frank, CID 2013) 87 Treatment Outcomes Among Patients with MDR TB: Systematic Review and Meta analysis Bayesian random effects meta analysis Successful treatment outcome was defined as cure or treatment completion. 34 clinical reports with a mean of 250 patients per report met the inclusion criteria. Our analysis shows that the proportion of patients treated successfully improved when treatment duration was at least 18 months, and if patients received directly observed therapy throughout treatment. Pooled success 69% if 18 months of treatment with DOT throughout Orenstein et al; Lancet Infect Dis 2009; 9:

45 Cegielski CID Feb


46 Cegielski CID Feb 2016 DO I REALLY HAVE TO USE AN INJECTABLE? Without a 2 nd Line Injectable (SLI) markedly poor outcomes much worse than with FQN resistance Cegielski CID Feb

47 DO I REALLY HAVE TO USE SO MANY DRUGS? MY PATIENT CAN T TOLERATE ALL OF THOSE Cegielski CID Feb 2016 Culture and Smear Outcomes in MDR TB Levofloxacin 750mg Vs Moxifloxacin 400mg Koh; AJRCCM

48 BDQ The Hard Facts! $23K for the 188 tablet/24 week course under 340B pricing. Non 340B will be more expensive CDC Recommendation # 1 Bedaquiline may be used in the initial 24 weeks of treatment in adults with laboratoryconfirmed pulmonary MDR TB when an effective treatment regimen cannot otherwise be provided. Quality of evidence: low 48
49 CDC Recommendation # 2 Bedaquiline may be used on a case by case basis in the populations listed below when an effective treatment regimen cannot otherwise be provided. Quality of evidence: insufficient expert opinion. Children HIV infected persons Pregnant women Persons with extrapulmonary TB Patients with co morbid conditions on concomitant medications CDC Recommendation # 3 Bedaquiline may be used on a case by case basis for durations longer than 24 weeks when an effective treatment regimen cannot otherwise be provided. Quality of evidence: insufficient expert opinion. 49







50 Clinical Features, Treatment History, Amplification of Drug Resistance, and Phenotypic Drug-Susceptibility Testing in the Patient. NEJM Nov 12,2015 Bloemberg GV et al. N Engl J Med 2015;373: Bacteriological Monitoring During MDR Therapy 2016 WHO Guidelines The use of sputum smear microscopy and culture rather than sputum smear alone Monthly sputum smear microscopy and culture performed best at identifying failures earlier Early identification of failure allows for institution of infection control measures and changes to drug regimen before resistance can be amplified. 50
51 Predictors of Poor Outcome for MDR Patients Treated at DOTS Plus Projects Independent predictors of death and failure: HIV positive, low BMI Prior treatment, more resistance Extensive disease, positive smear Positive culture after 3 months of treatment Consider augmenting treatment if possible Kurbatova et al. Tuberculosis, 2012 STREAM Trial for MDR TB All moxifloxacin (high dose), clofazimine, INH (high dose), PZA, EMB 9 Month Phase 3 Bedaquiline based completely oral regimen Prothionamide 6 Month Phase 3 Bedaquiline x 6 months Kanamycin x 2 months No prothionamide 51
52 Identification and Management of Contacts Transmission to household contacts similar to drug susceptible TB, active TB disease noted in: 3.6% in South Africa (all MDR or XDR) Mortality 14% if MDR, 52% if XDR Vella, Int J Tuberc Lung Dis % in Peru (80% MDR) Constant rate per year over three years Grandjean, 2011 Int J Tuberc Lung Dis Contacts with active disease identified early in South Africa but in Peru required follow up for at least 12 months Management of Contacts of MDR TB Evaluate possibility that source was MDR Discuss possible treatment with patient no studies to guide CDC recommends clinical and radiographic follow up for 24 months whether individuals with LTBI presumed due to an MDR/XDR isolate are treated or not 2 drugs to which source is susceptible for 6 12 months Levofloxacin or moxifloxacin and PZA or ethambutol and PZA Some experts use fluoroquinolone alone for 9 12 months Some experts use any two of the above that will work CDC. Targeted tuberculin testing and treatment of latent tuberculosis infection. MMWR 2000;49(No. RR 6):
 had HIV.")
 had died, 11 (10%)had failed treatment. 45 patients were discharged, of whom 26 (58%) had achieved sputum culture conversion and 19 (42%) had failed treatment.")
53 Long term outcomes of patients with XDR TB in South Africa: a cohort study Pietersen*, et al Lancet 2014; 383: Prospective F/U of 107 XDR patients treated from 3/2008, 8/2012, empirically as inpatients with a median of 8 drugs 44 patients (41%) had HIV. 36 (64%) of 56 isolates were resistant to at least eight drugs At 24 months of F/U, 17 (16%) had a favorable outcome, 49 (46%) had died At 60 months, 12 patients (11%) had a favorable outcome, 78 (73%) had died, 11 (10%)had failed treatment. 45 patients were discharged, of whom 26 (58%) had achieved sputum culture conversion and 19 (42%) had failed treatment. The medicine and syringes to treat one MDR TB patient for one year. Patients need to undergo treatment from months Staggering Medication Burden IDSA fact sheet

54 Only ~7 % of MDR is diagnosed with DST Only ~ 16% MDR is treated according to WHO standards 54
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S.
 Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 MDR/XDR TB Barbara J. Seaworth, MD October 16, 2013 Barbara J. Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
TB Intensive Houston, Texas October 15-17, 2013 MDR/XDR TB Barbara J. Seaworth, MD October 16, 2013 Barbara J. Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas May 6 9, 2014 MDR/XDR TB Barbara Seaworth, MD May 9, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial relationships
TB Intensive San Antonio, Texas May 6 9, 2014 MDR/XDR TB Barbara Seaworth, MD May 9, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial relationships
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
Multi-Drug and Extensively Drug Resistant Tuberculosis
 Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
Multidrug-resistant Tuberculosis. Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership
 Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
TB Intensive Houston, Texas. Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD
 TB Barbara Seaworth, MD") TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
Treatment of Multidrug-resistant Tuberculosis (MDR-TB)
") Treatment of Multidrug-resistant Tuberculosis (MDR-TB) 2006 2008 2011 2013 2014 2016 2019 Charles L. Daley, MD National Jewish Health University of Colorado Disclosures Research grant Insmed: Phase II
Treatment of Multidrug-resistant Tuberculosis (MDR-TB) 2006 2008 2011 2013 2014 2016 2019 Charles L. Daley, MD National Jewish Health University of Colorado Disclosures Research grant Insmed: Phase II
Treatment of MDR/XDR-TB. Short course chemotherapy for MDR-TB: practical issues. CHIANG Chen-Yuan MD, MPH, DrPhilos
 Treatment of MDR/XDR-TB Short course chemotherapy for MDR-TB: practical issues CHIANG Chen-Yuan MD, MPH, DrPhilos Treatment strategies for MDR-TB Standardized treatment: drug resistance survey data from
Treatment of MDR/XDR-TB Short course chemotherapy for MDR-TB: practical issues CHIANG Chen-Yuan MD, MPH, DrPhilos Treatment strategies for MDR-TB Standardized treatment: drug resistance survey data from
Clinical Management : DR-TB
 Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
Challenges to treat MDR TB
 Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION
 1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
Drug-resistant TB therapy: the future is now
 Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
MDR TB AND CASE STUDIES
 MDR TB AND CASE STUDIES Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Seattle, CITC Clinical Intensive June 15, 2018 Slide
MDR TB AND CASE STUDIES Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Seattle, CITC Clinical Intensive June 15, 2018 Slide
XDR TB: The Laboratory s Dilemma vs The Clinician s Dilemma
 XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
TB Grand Rounds. MDR-TB: Management of Adverse Drug Reactions. Reynard J. McDonald, M.D. September 18, Patient History
 TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
Drug resistant TB: The role of the laboratory
 Drug resistant TB: The role of the laboratory 26 Oct 2012 Andrew Whitelaw NHSLS / UCT TB lab functions: Outline Resistance testing Genotypic Phenotypic Which tests are done when, and why Reporting of
Drug resistant TB: The role of the laboratory 26 Oct 2012 Andrew Whitelaw NHSLS / UCT TB lab functions: Outline Resistance testing Genotypic Phenotypic Which tests are done when, and why Reporting of
Practical. Walk through New Survival Guide
 Many faces of TB: Drug resistant it ttbs Survival lgid Guide v3 P B L Ch G Sh t L T P. Barry, L. Chen, G. Schecter, L. True Curry International TB Center/CTCA April 20, 2016 Real case Practical Walk through
Many faces of TB: Drug resistant it ttbs Survival lgid Guide v3 P B L Ch G Sh t L T P. Barry, L. Chen, G. Schecter, L. True Curry International TB Center/CTCA April 20, 2016 Real case Practical Walk through
CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP)
 Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP)") CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP) Beverly Metchock, DrPH, D(ABMM) Mycobacteriology Laboratory Branch/Division
CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP) Beverly Metchock, DrPH, D(ABMM) Mycobacteriology Laboratory Branch/Division
MDR treatment. Shanghai, May 2012 Arnaud Trébucq The Union
 MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2
 1 MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2 1 India has the highest TB burden in the world 3 4 2 5 M. tuberculosis Resistance
1 MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2 1 India has the highest TB burden in the world 3 4 2 5 M. tuberculosis Resistance
Multidrug resistant Tuberculosis
 Multidrug resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive October 018 Objectives
Multidrug resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive October 018 Objectives
Management of MDR and XDR TB Prof. Martin Boeree
 Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
Treatment of Drug Resistant TB
 Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
Multidrug-resistant Tuberculosis
 Multidrug-resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive September 2016
Multidrug-resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive September 2016
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing - PRELIMINARY -
 Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France
 Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
MDR-TB drugs per WHO guidelines
 New antituberculous agents for drug-resistant resistant TB Symposium Belgian Society of Infectiology and Clinical Microbiology November 9 Jens Van Roey, MD - Tibotec Definitions MDR-TB multidrug resistance
New antituberculous agents for drug-resistant resistant TB Symposium Belgian Society of Infectiology and Clinical Microbiology November 9 Jens Van Roey, MD - Tibotec Definitions MDR-TB multidrug resistance
Quality of 2 nd line medicines for tuberculosis. Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products
 Quality of 2 nd line medicines for tuberculosis Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products Case studies in medicines for tuberculosis Outline: Statistics
Quality of 2 nd line medicines for tuberculosis Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products Case studies in medicines for tuberculosis Outline: Statistics
New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick
 Patrick") New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick Phillips Patrick.Phillips@ucsf.edu @PPJPhillips Outline Overview of regimen development strategies 1-3 year horizon: Ongoing phase
New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick Phillips Patrick.Phillips@ucsf.edu @PPJPhillips Outline Overview of regimen development strategies 1-3 year horizon: Ongoing phase
Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study
 Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study Julie Tans-Kersten, MS, BS-MT (ASCP) Tuberculosis Laboratory Program Coordinator Wisconsin
Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study Julie Tans-Kersten, MS, BS-MT (ASCP) Tuberculosis Laboratory Program Coordinator Wisconsin
DR-TB PATIENT IDENTITY CARD
 Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
TB New Drugs, Shorter Courses
 TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
Drug resistant TB: Lisa Chen, MD University of California, San Francisco Curry Interna:onal TB Center Sea=le, June 2016
 Drug resistant TB: Lisa Chen, MD University of California, San Francisco Curry Interna:onal TB Center Sea=le, June 2016 Drug- Resistant TB: De1initions Mono- resistant: Resistance to a single drug Poly-
Drug resistant TB: Lisa Chen, MD University of California, San Francisco Curry Interna:onal TB Center Sea=le, June 2016 Drug- Resistant TB: De1initions Mono- resistant: Resistance to a single drug Poly-
Treatment of Nontuberculous Mycobacterial Infections (NTM)
") Treatment of Nontuberculous Mycobacterial Infections (NTM) Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory
Treatment of Nontuberculous Mycobacterial Infections (NTM) Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory
Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB)
") Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB) Session: Fanning the Flames of HIV and TB Cointeraction SA AIDS Conference-Durban ICC 13-15 June 2017
Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB) Session: Fanning the Flames of HIV and TB Cointeraction SA AIDS Conference-Durban ICC 13-15 June 2017
Case 1 and Case 2. Case 1 3/23/2016
 Case 1 and Deidra D. Parrish, MD, MPH&TM Nashville Metro Public Health Dept TB Symposium March 30, 2016 Case 1 27 yo Indian woman came to the US to join her husband three months prior to clinic visit.
Case 1 and Deidra D. Parrish, MD, MPH&TM Nashville Metro Public Health Dept TB Symposium March 30, 2016 Case 1 27 yo Indian woman came to the US to join her husband three months prior to clinic visit.
Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool)
") Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool) DOTS + and LTBI New drugs for TB and the challenge of resistance talk plan 1. Epidemiology 2. Treatment 3. The MDRTB
Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool) DOTS + and LTBI New drugs for TB and the challenge of resistance talk plan 1. Epidemiology 2. Treatment 3. The MDRTB
Drug Resistant Tuberculosis:
 Drug Resistant Tuberculosis: Pearls and other Considerations John W. Wilson, MD Associate Professor of Medicine Division of Infectious Diseases Mayo Clinic, Rochester MN Mayo Clinic Center for Tuberculosis
Drug Resistant Tuberculosis: Pearls and other Considerations John W. Wilson, MD Associate Professor of Medicine Division of Infectious Diseases Mayo Clinic, Rochester MN Mayo Clinic Center for Tuberculosis
Linezolid: an effective, safe and cheap drug for patients failing multidrug-resistant tuberculosis treatment in India
 Eur Respir J 2012; 39: 956 962 DOI: 10.1183/09031936.00076811 CopyrightßERS 2012 Linezolid: an effective, safe and cheap drug for patients failing multidrug-resistant tuberculosis treatment in India R.
Eur Respir J 2012; 39: 956 962 DOI: 10.1183/09031936.00076811 CopyrightßERS 2012 Linezolid: an effective, safe and cheap drug for patients failing multidrug-resistant tuberculosis treatment in India R.
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 29 October 2014 GRANUPAS, gastro-resistant granules 30 sachets with a calibrated measuring spoon (CIP: 34009 278 801
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 29 October 2014 GRANUPAS, gastro-resistant granules 30 sachets with a calibrated measuring spoon (CIP: 34009 278 801
The New England Journal of Medicine THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY
 THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY KEMAL TAHAOĞLU, M.D., TÜLAY TÖRÜN, M.D., TÜLIN SEVIM, M.D., GÜLIZ ATAÇ, M.D., ALTAN KIR, M.D., LEVENT KARASULU, M.D., IPEK ÖZMEN, M.D., AND NILÜFER
THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY KEMAL TAHAOĞLU, M.D., TÜLAY TÖRÜN, M.D., TÜLIN SEVIM, M.D., GÜLIZ ATAÇ, M.D., ALTAN KIR, M.D., LEVENT KARASULU, M.D., IPEK ÖZMEN, M.D., AND NILÜFER
MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience
 MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience Dr Johan Van Wyk MB.Ch.B, M.Med (Clin Path) Clinical Pathologist ibhayi Region, Eastern Cape GWYNETH PALTROW SHAKESPEARE IN LOVE 1998 PORT
MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience Dr Johan Van Wyk MB.Ch.B, M.Med (Clin Path) Clinical Pathologist ibhayi Region, Eastern Cape GWYNETH PALTROW SHAKESPEARE IN LOVE 1998 PORT
Tb : Recent recommendation. Dr.Ketan Shah
 Tb : Recent recommendation Dr.Ketan Shah Tbc : Clinician If you think It is easy to diagnose : u r not good clinician It is difficult to diagnose :U r not alone doctor to think this 6/22/2015 Ketan Shah
Tb : Recent recommendation Dr.Ketan Shah Tbc : Clinician If you think It is easy to diagnose : u r not good clinician It is difficult to diagnose :U r not alone doctor to think this 6/22/2015 Ketan Shah
Tuberculosis in 2017: Searching for new solutions in the face of new challenges
 Tuberculosis in 2017: Searching for new solutions in the face of new challenges 6th TB Symposium Ministry of Health of the Republic of Belarus, Republican Scientific and Practical Center for Pulmonology
Tuberculosis in 2017: Searching for new solutions in the face of new challenges 6th TB Symposium Ministry of Health of the Republic of Belarus, Republican Scientific and Practical Center for Pulmonology
Introduction of Bedaquiline in the Philippines
 Introduction of Bedaquiline in the Philippines 24th PhilCAT Annual Convention Crown Plaza Hotel August 18,2107 Vivian S. Lofranco, MD., PHSAE National Clinical Coordinator, BDQ MDR-TB is highly contagious
Introduction of Bedaquiline in the Philippines 24th PhilCAT Annual Convention Crown Plaza Hotel August 18,2107 Vivian S. Lofranco, MD., PHSAE National Clinical Coordinator, BDQ MDR-TB is highly contagious
Dr Sharanjit Dhoot. Chelsea and Westminster Hospital, London. 18 th Annual Conference of the British HIV Association (BHIVA)
") 18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
University of Groningen. Tuberculosis and its sequelae Akkerman, Onno
 University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
In Vitro Activities of Linezolid against Clinical Isolates of ACCEPTED
 AAC Accepts, published online ahead of print on April 00 Antimicrob. Agents Chemother. doi:./aac.001-0 Copyright 00, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
AAC Accepts, published online ahead of print on April 00 Antimicrob. Agents Chemother. doi:./aac.001-0 Copyright 00, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
Dr Dean Shuey Team Leader Health Services Development WPRO. World Health Day Antimicrobial Resistance: The Global and Regional Situation
 Dr Dean Shuey Team Leader Health Services Development WPRO World Health Day 2011 Antimicrobial Resistance: The Global and Regional Situation 2 7 April 2011 World Health Day No action today, no cure tomorrow
Dr Dean Shuey Team Leader Health Services Development WPRO World Health Day 2011 Antimicrobial Resistance: The Global and Regional Situation 2 7 April 2011 World Health Day No action today, no cure tomorrow
Inappropriate Use of Antibiotics and Clostridium difficile Infection. Jocelyn Srigley, MD, FRCPC November 1, 2012
 Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
The challenge of managing extensively drug-resistant tuberculosis at a referral hospital in the state of São Paulo, Brazil: a report of three cases
 J Bras Pneumol. 2015;41(6):554-559 http://dx.doi.org/10.1590/s1806-37562015000000299 CASE REPORT The challenge of managing extensively drug-resistant tuberculosis at a referral hospital in the state of
J Bras Pneumol. 2015;41(6):554-559 http://dx.doi.org/10.1590/s1806-37562015000000299 CASE REPORT The challenge of managing extensively drug-resistant tuberculosis at a referral hospital in the state of
Extensively Drug-Resistant Tuberculosis in South Korea: Risk Factors and Treatment Outcomes among Patients at a Tertiary Referral Hospital
 MAJOR ARTICLE Extensively Drug-Resistant Tuberculosis in South Korea: Risk Factors and Treatment Outcomes among Patients at a Tertiary Referral Hospital Christie Y. Jeon, 1,2,a Soo Hee Hwang, 5,a Jin Hong
MAJOR ARTICLE Extensively Drug-Resistant Tuberculosis in South Korea: Risk Factors and Treatment Outcomes among Patients at a Tertiary Referral Hospital Christie Y. Jeon, 1,2,a Soo Hee Hwang, 5,a Jin Hong
Treatment of Slowly Growing NTM Infections
 Treatment of Slowly Growing NTM Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory Committee Insmed
Treatment of Slowly Growing NTM Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory Committee Insmed
Risk Factors for Poor Outcomes in Patients with Multi-Drug Resistant Tuberculosis in South Korea
 Hanyang Med Rev 2016;36:262-268 https://doi.org/10.7599/hmr.2016.36.4.262 pissn 1738-429X eissn 2234-4446 Original Article Risk Factors for Poor Outcomes in Patients with Multi-Drug Resistant Tuberculosis
Hanyang Med Rev 2016;36:262-268 https://doi.org/10.7599/hmr.2016.36.4.262 pissn 1738-429X eissn 2234-4446 Original Article Risk Factors for Poor Outcomes in Patients with Multi-Drug Resistant Tuberculosis
Title: Resistance to fluoroquinolones and second line injectable drugs: impact on MDR TB outcomes
 ERJ Express. Published on October 25, 2012 as doi: 10.1183/09031936.00134712 Title: Resistance to fluoroquinolones and second line injectable drugs: impact on MDR TB outcomes Authors: D. Falzon, N. Gandhi,
ERJ Express. Published on October 25, 2012 as doi: 10.1183/09031936.00134712 Title: Resistance to fluoroquinolones and second line injectable drugs: impact on MDR TB outcomes Authors: D. Falzon, N. Gandhi,
Eradiaction of Resistant Organisms:
 Eradiaction of Resistant Organisms: Can we do it and does it help? Noah Lechtzin, MD; MHS Director, Adult CF Program Outline Evidence resistant organisms are bad MRSA, B cepacia, Pseudomonas, Fungal infections
Eradiaction of Resistant Organisms: Can we do it and does it help? Noah Lechtzin, MD; MHS Director, Adult CF Program Outline Evidence resistant organisms are bad MRSA, B cepacia, Pseudomonas, Fungal infections
Current Status of Fluoroquinolone Use for Treatment of Tuberculosis in a Tertiary Care Hospital in Korea
 ORIGINAL ARTICLE https://doi.org/10.4046/trd.2017.80.2.143 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2017;80:143-152 Current Status of Fluoroquinolone Use for Treatment of Tuberculosis
ORIGINAL ARTICLE https://doi.org/10.4046/trd.2017.80.2.143 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2017;80:143-152 Current Status of Fluoroquinolone Use for Treatment of Tuberculosis
Online data supplement
 Online data supplement Title: Fluoroquinolone therapy for the prevention of multi-drug resistant tuberculosis in contacts: a cost-effectiveness analysis Authors: Gregory J Fox Olivia Oxlade Dick Menzies
Online data supplement Title: Fluoroquinolone therapy for the prevention of multi-drug resistant tuberculosis in contacts: a cost-effectiveness analysis Authors: Gregory J Fox Olivia Oxlade Dick Menzies
Creating a global community for clinical drug repurposing and development. Leonard Sacks Center for drug evaluation and research FDA
 Creating a global community for clinical drug repurposing and development Leonard Sacks Center for drug evaluation and research FDA Neglected tropical diseases 1) Repurposing and developing new drugs 2)
Creating a global community for clinical drug repurposing and development Leonard Sacks Center for drug evaluation and research FDA Neglected tropical diseases 1) Repurposing and developing new drugs 2)
Multidrug resistant tuberculosis treatment in the Indian private sector: Results from a tertiary referral private hospital in Mumbai
 Original Article Multidrug resistant tuberculosis treatment in the Indian private sector: Results from a tertiary referral private hospital in Mumbai Zarir F. Udwadia, Gautam Moharil Department of Pulmonology,
Original Article Multidrug resistant tuberculosis treatment in the Indian private sector: Results from a tertiary referral private hospital in Mumbai Zarir F. Udwadia, Gautam Moharil Department of Pulmonology,
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Non-Tuberculous Mycobacterial Pulmonary Disease Diagnosis and Management Jakko van Ingen, MD, PhD
 Non-Tuberculous Mycobacterial Pulmonary Disease (NTM-PD) 1 Radbound University Nihmegen Medical Center Milestones in NTM research 1980s: Nodular bronchiectatic lung disease Lady Windermere syndrome 1882-1890
Non-Tuberculous Mycobacterial Pulmonary Disease (NTM-PD) 1 Radbound University Nihmegen Medical Center Milestones in NTM research 1980s: Nodular bronchiectatic lung disease Lady Windermere syndrome 1882-1890
Section 6.2.4: Antituberculosis Medicines Application for moving streptomycin to complementary list
 Section 6.2.4: Antituberculosis Medicines Application for moving streptomycin to complementary list Stop TB Department World Health Organization Summary According to the recent guideline published in 2010
Section 6.2.4: Antituberculosis Medicines Application for moving streptomycin to complementary list Stop TB Department World Health Organization Summary According to the recent guideline published in 2010
Period of study: 12 Nov 2002 to 08 Apr 2004 (first subject s first visit to last subject s last visit)
") Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Tuberculosis (TB) is an infectious disease that is preventable, treatable
 is an infectious disease that is preventable, treatable") original article Multidrug-resistant tuberculosis: Treatment and outcomes of 93 patients Sarah K Brode MD FRCPC 1,2, Robert Varadi MDCM FRCPC 1,2, Jane McNamee RN(EC) 1, Nina Malek 1, Sharon Stewart MSW
original article Multidrug-resistant tuberculosis: Treatment and outcomes of 93 patients Sarah K Brode MD FRCPC 1,2, Robert Varadi MDCM FRCPC 1,2, Jane McNamee RN(EC) 1, Nina Malek 1, Sharon Stewart MSW
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days
 Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Duration of antibiotic therapy:
 Duration of antibiotic therapy: How low can you go? Thomas Holland, MD Hilton Head, SC July 2017 Disclosures Consulting: The Medicines Company, Basilea Pharmaceutica Adjudication committee: Achaogen Grant
Duration of antibiotic therapy: How low can you go? Thomas Holland, MD Hilton Head, SC July 2017 Disclosures Consulting: The Medicines Company, Basilea Pharmaceutica Adjudication committee: Achaogen Grant
INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS
 INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS 1 Research Associate, Drug Utilisation Research Unit, Nelson Mandela University 2 Human Sciences Research Council,
INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS 1 Research Associate, Drug Utilisation Research Unit, Nelson Mandela University 2 Human Sciences Research Council,
Critical Appraisal Topic. Antibiotic Duration in Acute Otitis Media in Children. Carissa Schatz, BSN, RN, FNP-s. University of Mary
 Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
ORIGINAL INVESTIGATION. Increasing Outpatient Fluoroquinolone Exposure Before Tuberculosis Diagnosis and Impact on Culture-Negative Disease
 ORIGINAL INVESTIGATION Increasing Outpatient Fluoroquinolone Exposure Before Tuberculosis Diagnosis and Impact on Culture-Negative Disease Pinky D. Gaba, MD; Connie Haley, MD, MPH; Marie R. Griffin, MD,
ORIGINAL INVESTIGATION Increasing Outpatient Fluoroquinolone Exposure Before Tuberculosis Diagnosis and Impact on Culture-Negative Disease Pinky D. Gaba, MD; Connie Haley, MD, MPH; Marie R. Griffin, MD,
New antituberculosis drugs and regimens
 New antituberculosis drugs: from clinical trial to programmatic use Gina Gualano, 1 Susanna Capone, 2 Alberto Matteelli, 2 Fabrizio Palmieri 1 1 Respiratory Infectious Diseases Unit, National Institute
New antituberculosis drugs: from clinical trial to programmatic use Gina Gualano, 1 Susanna Capone, 2 Alberto Matteelli, 2 Fabrizio Palmieri 1 1 Respiratory Infectious Diseases Unit, National Institute
Staph Cases. Case #1
 Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
ANTHRAX. INHALATION, INTESTINAL and CUTANEOUS ANTHRAX
 INHALATION, INTESTINAL and CUTANEOUS ANTHRAX CPMP/4048/01, rev. 3 1/7 General points on treatment Anthrax is an acute infectious disease caused by Bacillus anthracis, that may be infecting man via cutaneous
INHALATION, INTESTINAL and CUTANEOUS ANTHRAX CPMP/4048/01, rev. 3 1/7 General points on treatment Anthrax is an acute infectious disease caused by Bacillus anthracis, that may be infecting man via cutaneous
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship
 Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Tuberculosis infection in an Asian elephant at a Japanese Zoo and its first treatment in Japan
 Tuberculosis infection in an Asian elephant at a Japanese Zoo and its first treatment in Japan Satoshi Ishikawa, Satomi Suga, Yasuhiko Mukai Fukuyama Zoo, Hiroshima Fukuyama Zoo October 22th, 2017 Tuberculosis
Tuberculosis infection in an Asian elephant at a Japanese Zoo and its first treatment in Japan Satoshi Ishikawa, Satomi Suga, Yasuhiko Mukai Fukuyama Zoo, Hiroshima Fukuyama Zoo October 22th, 2017 Tuberculosis
Antimicrobial Stewardship in the Hospital Setting
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 12 Antimicrobial Stewardship in the Hospital Setting Authors Dan Markley, DO, MPH, Amy L. Pakyz, PharmD, PhD, Michael Stevens, MD, MPH Chapter Editor
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 12 Antimicrobial Stewardship in the Hospital Setting Authors Dan Markley, DO, MPH, Amy L. Pakyz, PharmD, PhD, Michael Stevens, MD, MPH Chapter Editor
Measure Information Form
 Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
ESCMID Online Lecture Library. by author
 Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Hosted by Dr. Benedetta Allegranzi, WHO Patient Safety Agency A Webber Training Teleclass
 The History of Medicine Antimicrobial Resistance Issues Worldwide and the WHO Approach to Combat It Carmem Lúcia Pessoa-Silva, MD, PhD Health Security and Environment Cluster, WHO HQ, Geneva Hosted by
The History of Medicine Antimicrobial Resistance Issues Worldwide and the WHO Approach to Combat It Carmem Lúcia Pessoa-Silva, MD, PhD Health Security and Environment Cluster, WHO HQ, Geneva Hosted by
MDR Acinetobacter baumannii. Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta
 MDR Acinetobacter baumannii Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta 1 The Armageddon recipe Transmissible organism with prolonged environmental
MDR Acinetobacter baumannii Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta 1 The Armageddon recipe Transmissible organism with prolonged environmental
Antimicrobial Stewardship 101
 Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
Infectious Disease Update 2017
 Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
POPULATION PHARMACOKINETICS AND PHARMACODYNAMICS OF OFLOXACIN IN SOUTH AFRICAN PATIENTS WITH DRUG- RESISTANT TUBERCULOSIS
 POPULATION PHARMACOKINETICS AND PHARMACODYNAMICS OF OFLOXACIN IN SOUTH AFRICAN PATIENTS WITH DRUG- RESISTANT TUBERCULOSIS Emmanuel Chigutsa 1, Sandra Meredith 1, Lubbe Wiesner 1, Nesri Padayatchi 2, Joe
POPULATION PHARMACOKINETICS AND PHARMACODYNAMICS OF OFLOXACIN IN SOUTH AFRICAN PATIENTS WITH DRUG- RESISTANT TUBERCULOSIS Emmanuel Chigutsa 1, Sandra Meredith 1, Lubbe Wiesner 1, Nesri Padayatchi 2, Joe
Can mutation detection accurately predict XDR- TB: study from a tertiary care centre India
 JCM Accepts, published online ahead of print on 2 February 2011 J. Clin. Microbiol. doi:10.1128/jcm.00113-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 2 February 2011 J. Clin. Microbiol. doi:10.1128/jcm.00113-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
Antibiotic Stewardship in the LTC Setting
 Antibiotic Stewardship in the LTC Setting Joe Litsey, Director of Consulting Services Pharm.D., Board Certified Geriatric Pharmacist Thrifty White Pharmacy Objectives Describe the Antibiotic Stewardship
Antibiotic Stewardship in the LTC Setting Joe Litsey, Director of Consulting Services Pharm.D., Board Certified Geriatric Pharmacist Thrifty White Pharmacy Objectives Describe the Antibiotic Stewardship
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
CLINICAL PROTOCOL FOR COMMUNITY ACQUIRED PNEUMONIA. SCOPE: Western Australia. CORB score equal or above 1. All criteria must be met:
 CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
BRUCELLOSIS BRUCELLOSIS. CPMP/4048/01, rev. 3 1/7 EMEA 2002
 BRUCELLOSIS CPMP/4048/01, rev. 3 1/7 General points on treatment Four species are pathogenic to man: B. melitenis (acquired from goats), B. suis (pigs), B. abortus (cattle) and B. canis (dogs). The bacteria
BRUCELLOSIS CPMP/4048/01, rev. 3 1/7 General points on treatment Four species are pathogenic to man: B. melitenis (acquired from goats), B. suis (pigs), B. abortus (cattle) and B. canis (dogs). The bacteria
The Threat of Multidrug Resistant Neisseria gonorrhoeae
 The Threat of Multidrug Resistant Neisseria gonorrhoeae Peel Public Health Symposium Sex, Drugs, and. Vanessa Allen, MD MPH October 16, 2012 The threat of multidrug resistant gonorrhea "We're sitting on
The Threat of Multidrug Resistant Neisseria gonorrhoeae Peel Public Health Symposium Sex, Drugs, and. Vanessa Allen, MD MPH October 16, 2012 The threat of multidrug resistant gonorrhea "We're sitting on
GUIDE TO INFECTION CONTROL IN THE HOSPITAL. Antibiotic Resistance
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 4: Antibiotic Resistance Author M.P. Stevens, MD, MPH S. Mehtar, MD R.P. Wenzel, MD, MSc Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 4: Antibiotic Resistance Author M.P. Stevens, MD, MPH S. Mehtar, MD R.P. Wenzel, MD, MSc Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017
 Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
Antibiotic Stewardship in the Neonatal Intensive Care Unit. Objectives. Background 4/20/2017. Natasha Nakra, MD April 28, 2017
 Antibiotic Stewardship in the Neonatal Intensive Care Unit Natasha Nakra, MD April 28, 2017 Objectives 1. Describe antibiotic use in the NICU 2. Explain the role of antibiotic stewardship in the NICU 3.
Antibiotic Stewardship in the Neonatal Intensive Care Unit Natasha Nakra, MD April 28, 2017 Objectives 1. Describe antibiotic use in the NICU 2. Explain the role of antibiotic stewardship in the NICU 3.
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
Case Presentations: Non Responding TB Dr. Manoj Yadav
 Case Presentations: Non Responding TB Dr. Manoj Yadav mbbs, dtcd, dnb (resp. dis.) Consultant Pulmonologist Kailash Hospital, Kailash Complex Near Mahadev Temple, Productivity Road Vadodara 390007 :: Phone:
Case Presentations: Non Responding TB Dr. Manoj Yadav mbbs, dtcd, dnb (resp. dis.) Consultant Pulmonologist Kailash Hospital, Kailash Complex Near Mahadev Temple, Productivity Road Vadodara 390007 :: Phone:
11/22/2016. Antimicrobial Stewardship Update Disclosures. Outline. No conflicts of interest to disclose
 Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University