Cellulitis and Abscess: ED Phase v 1.1
|
|
|
- April Stokes
- 6 years ago
- Views:
Transcription

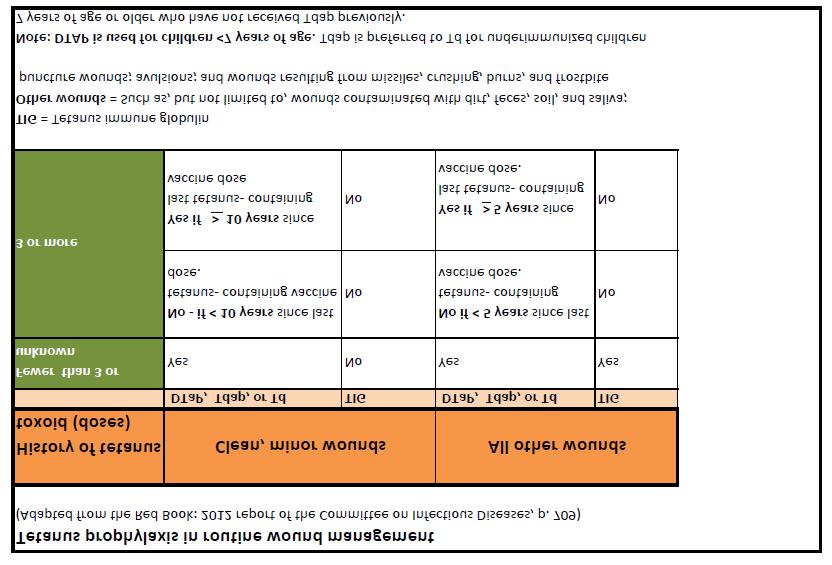
1 Cellulitis and Abscess: ED Phase v 1.1 Executive Summary Test Your Knowledge PHASE I (E.D.) Explanation of Evidence Ratings Summary of Version Changes! Labs if systemic illness or necrotizing fasciitis suspected Inclusion Criteria Suspected skin/soft tissue infection in children > 44 weeks CGA Exclusion Criteria Hospital-acquired, surgical site & device-associated infections Presumed necrotizing fasciitis Orbital/periorbital cellulitis Immunodeficiency Pressure ulcers Solitary dental! Consider tetanus immunization status as necessary If referral call from PMD, request perimeter line be drawn and make patient NPO. Provider Assessment Determine if special situation present. Concern for: Deep extremity infection (e.g., tenosynovitis, septic arthritis, osteomyelitis) Deep puncture wound of hand/fingers/feet Yes Order labs, then Involve Orthopedics No Concern for: Peri-anal (within 1cm of anal verge) Breast Perineal Pilonidal cyst Large or complex Yes Involve General Surgery No Concern for: Neck Yes Involve ENT No Concern for: Facial cellulitis of dental origin Yes Involve Dental; See antibiotic table Determine with consultant if suitable for pathway No Yes No Go to Simple Cellulitis / Abscess Phase Off Pathway For questions concerning this pathway, contact: CellulitisandAbscess@seattlechildrens.org 2013 Seattle Children s Hospital, all rights reserved, Medical Disclaimer Last Updated: 08/15/2013 Valid until:08/15/2016
2 Cellulitis and Abscess: ED simple cellulitis / v.1 Executive Summary Test Your Knowledge PHASE I (E.D.) Explanation of Evidence Ratings Summary of Version Changes! Labs if systemic illness or necrotizing fasciitis suspected Inclusion Criteria Suspected skin/soft tissue infection in children > 44 weeks CGA Exclusion Criteria Hospital-acquired, surgical site & device-associated infections Presumed necrotizing fasciitis Orbital/periorbital cellulitis Immunodeficiency Pressure ulcers Solitary dental! Alter antibiotic selection if >48h of prior antibiotics given Simple cellulitis / Non-purulent Perform bedside ultrasound unless clearly fluctuant or draining Purulent No routine labs Fluctuant or 1cm on ultrasound: Sedation / pain control I&D and culture wound Determine Disposition Low Risk Criteria Simple Adequate I&D Age 1 year No fever Well-appearing No significant comorbidities Follow up assured Inpatient Admit Criteria (any one of the following) Systemic illness Not tolerating PO Treatment failure on >48h of appropriate antibiotics Rapidly progressive lesion Pain control / wound care All < 2 mo; consider if <6 mo Inadequate F/U Purulent Definition Actively draining pus History of drainage Abscess present Non-purulent Discharged patients Purulent! Antibiotic selection by condition Non-purulent Admitted patients Purulent Medical Treatment Oral cephalexin Clindamycin if failed outpatient treatment, cephalosporin allergic or if MRSA risks Medical Treatment No systemic antibiotics after I&D if low risk Oral clinda if not low risk TMP/SMX (or doxycycline if >8 years) if presumed clindamycin-resistant MRSA Medical Treatment IV cefazolin Clindamycin if failed outpatient treatment, cephalosporin allergic or if MRSA risks Consider vancomycin if systemic toxicity Medical Treatment IV clindamycin Vancomycin if presumed clindamycin-resistant MRSA Consider vancomycin if systemic toxicity, failed outpatient clindamycin Discharge Instructions 7-10 days total treatment PMD f/u within hours Go to For questions concerning this pathway, contact: CellulitisandAbscess@seattlechildrens.org 2013 Seattle Children s Hospital, all rights reserved, Medical Disclaimer Last Updated: 08/15/2013 Valid until:08/15/2016
3 Cellulitis and Abscess: v.1 Executive Summary Test Your Knowledge PHASE II (INPATIENT) Explanation of Evidence Ratings Summary of Version Changes! Labs if systemic illness or necrotizing fasciitis suspected Inclusion Criteria Suspected skin/soft tissue infection in children > 44 weeks CGA INPATIENT Exclusion Criteria Hospital-acquired, surgical site & device-associated infections Peri-anal or pilonidal es Presumed necrotizing fasciitis Orbital/periorbital cellulitis Pts admitted to surgical service Immunodeficiency Deep structure infections Pressure ulcers! Antibiotic selection by condition Improving Daily re-evaluation Clinical exam Culture data Not Improving Tailor antibiotics if culture results are available Use narrowest-spectrum agent possible Tailor antibiotics if culture results are available If rapid progression at any time or no improvement on empiric antibiotics at 48 hours, consider empiric change in antibiotics If no improvement on adequate antibiotics, image (U/S preferred) to rule out formation If fluctuance develops or 1 cm on imaging, consult gen. surgery Consult ID as necessary Discharge Criteria (Meets all) Lesion(s) show signs of improvement Tolerating PO Pain controlled Afebrile >24 hours F/U assured within 48 hours Discharge Instructions 7-10 days total treatment PMD f/u within 48 hours For questions concerning this pathway, contact: CellulitisandAbscess@seattlechildrens.org 2013 Seattle Children s Hospital, all rights reserved, Medical Disclaimer Last Updated: 08/15/2013 Valid until:08/15/2016
4 Cellulitis and Abscess: Antibiotic Table Executive Summary Test Your Knowledge Explanation of Evidence Ratings Summary of Version Changes Cellulitis and Abscess Antibiotic Table Condition Non-purulent cellulitis Purulent SSTI/ Bite wounds Facial cellulitis of dental origin IV choice Cefazolin Clindamycin Ampicillin/sulbactam Penicillin OR Ampicillin/sulbactam IV Alternatives Clindamycin if cephalosporin allergic Consider vancomycin if rapidly progressive lesion; hemodynamic instability; illappearing Vancomycin if presumed clindamycin resistant MRSA; rapidly progressive lesion; hemodynamic instability; illappearing; failed oral clindamycin as outpatient; in an area difficult to drain completely such as face/hand/genitals Call ID if linezolid desired Cefoxitin (transition to clindamycin AND ciprofloxacin at discharge) if penicillin allergic Clindamycin if penicillin allergic PO choice Cephalexin No antibiotics if low risk criteria* met and adequately drained Amoxicillin/clavulanate Penicillin OR Amoxicillin/clavulanate Clindamycin otherwise PO Alternatives Clindamycin if cephalosporin allergic TMP/SMX if presumed clindamycin resistant MRSA Doxycycline if age >8 years and prior clindamycin and TMP/SMX resistant MRSA OR presumed clindamycin resistance and sulfa allergy Call ID if linezolid desired Doxycycline if age >8 years and penicillin allergy Clindamycin AND ciprofloxacin for penicillin allergic patients Call ID for other scenarios Clindamycin if penicillin allergic *Low risk criteria: Age 1 year; no fever; well-appearing; adequate I&D; no significant comorbidities Low Risk Criteria* Simple Adequate I&D Age 1 year No fever Well-appearing No significant comorbidities Follow up assured Alternate antibiotic choices If fresh or saltwater contact, or other special circumstance, discuss with ID * For use in determining the need for PO antibiotics for purulent infection post I&D, outpatient treatment (see above) Return Return to ED Simple Cellulitis / Abscess Phase Return to For questions concerning this pathway, contact: CellulitisandAbscess@seattlechildrens.org 2013 Seattle Children s Hospital, all rights reserved, Medical Disclaimer Last Updated: 08/15/2013 Valid until:08/15/2016
5
6 Bibliography Literature SearchSearch Methods, Soft Tissue Infections Cellulitis, Clinical Standard Work Studies were identified by searching electronic databases using search strategies developed and executed by a medical librarian, Susan Klawansky. Searches were performed in November 2012 in the following databases on the Ovid platform: Medline and Cochrane Database of Systematic Reviews; elsewhere: Embase, Clinical Evidence, National Guideline Clearinghouse and TRIP. Retrieval was limited to 2004 to current, humans, and English language. In Medline and Embase, appropriate Medical Subject Headings (MeSH) and Emtree headings were used respectively, along with text words, and the search strategy was adapted for other databases as appropriate. Concepts searched were soft tissue infections, cellulitis and many other related conditions, some of which are skin, bites and stings, impetigo, carbuncle, infectious skin diseases and penetrating wounds. All retrieval was further limited to certain publication types representing high order evidence. Susan Klawansky, MLS, AHIP April 9, 2013 Identification 383 records identified through database searching 13 additional records identified through other sources Screening 396 records after duplicates removed 396 records screened 340 records excluded Elgibility 55 full-text articles assessed for eligibility 11 full-text articles excluded, did not answer clinical question did not meet quality threshold Included 44 studies included in pathway Flow diagram adapted from Moher D et al. BMJ 2009;339:bmj.b2535 To Bibliography, Pg 1
7 Bibliography 1) Kilburn SA, Featherstone P, Higgins B, Brindle R. Interventions for cellulitis and erysipelas. Cochrane Database of Systematic Reviews 2010 (6). DOI: / CD pub2. 2) Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BE, Rybak MJ, Talan DA, Chambers HF. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant staphylococcus aureus infections in adults and children. Clin Infect Dis 2011 Feb;52: ) JL Robinson, MI Salvadori; Canadian Paediatric Society Infectious Diseases and Immunization Committee, Management of community associated methicillin-resistant Staphylococcus aureus skin es in children. Paediatr Child Health 2011; 16(2): ) May A et al. Treatment of complicated skin and soft tissues infections, Surgical Infection Society Guidelines. Surgical Infections 2009 Vol 10, Number 5, ) Paydar, K Z, Hansen, SL, Charlebois, ED, Harris, HW, Young, DL. Inappropriate antibiotic use in soft tissue infections. Archives of Surgery 2006; 141(9), ) Elliott DJ, Zaoutis TE, Troxel AB, Loh A, Keren R. Empiric antimicrobial therapy for pediatric skin and soft-tissue infections in the era of methicillin-resistant Staphylococcus aureus. Pediatrics 2009; 123(6), e ) Duong et al, Randomized Controlled Trial of Antibiotics in the Management of Community- Acquired Skin Abscesses in the Pediatric Patient. Ann Emerg Med 2010;55(5): ) Stevens DL et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections. Clin Infect Dis 2005;41: ) Williams DJ et al. Comparative effectiveness of antibiotic treatment strategies for pediatric skin and soft-tissue infections. Pediatrics 2011;128(3) e1-e9. 10) Chen AE et al. Randomized Controlled Trial of Cephalexin Versus Clindamycin for Uncomplicated Pediatric Skin Infections. Pediatrics 2011;127(3);e ) Squire et al. ABSCESS: Applied Bedside Sonography for Convenient Evaluation of Superficial Soft Tissue Infections. Acad Emerg Med 2005 Vol. 12, No. 7, ) Tayal, VS, Hasan, N, Norton, HJ et al, The effect of soft-tissue ultrasound on the management of cellulitis in the emergency department. Acad Emerg Med 2006, 13, 4,
8 Executive Summary Objective To improve the quality and safety of care for uncomplicated community acquired soft tissue infections in children older than 30 days of life, specifically: Reduce use of broader spectrum, inappropriate, or more toxic antibiotics for cellulitis and Reduce the use of systemic antibiotics for children with simple who meet low risk criteria Decrease unnecessary laboratory testing Increase the use of laboratory testing that will allow for targeted antimicrobial therapy Decrease unnecessary hospital days Recommendations 1. Use bedside ultrasound where available to improve the accuracy in diagnosis of subcutaneous es. 2. Obtain wound cultures when possible. 3. Do NOT obtain routine blood testing (CBC, CRP, blood culture) for most children with cellulitis or. 4. No incision and drainage is needed for es <1 cm on bedside ultrasound; these patients may be discharged home on antibiotics alone. 5. Do NOT prescribe oral antibiotics for simple es that have been incised and drained completely, if the patient is >1 year of age, afebrile, well-appearing, with no significant comorbidities and adequate follow up assured. 6. Prescribe oral clindamycin for outpatient treatment of es that could not have an adequate I&D, or do not meet low-risk criteria. 7. Prescribe cephalexin for outpatient treatment of simple cellulitis without an, drainage, history of drainage, or failure of outpatient antibiotic course (>48 h on appropriate antibiotics). 8. Prescribe oral clindamycin for outpatient treatment of purulent cellulitis or cellulitis that has not responded to anti-mssa therapy (beta lactam, >48 hours). 9. Prescribe cefazolin for inpatient treatment of simple cellulitis without an, drainage, history of drainage, or failure of outpatient antibiotic course (>48 h on appropriate antibiotic). 10. Prescribe IV clindamycin for inpatient treatment of purulent cellulitis or cellulitis that has not responded to anti-mssa therapy (beta lactam, >48 hours). 11. Prescribe IV vancomycin for inpatient treatment of cellulitis in patients who are systemically ill (fever >38, tachycardia, vomiting) or have failed antibiotic therapy that covers MRSA. 12. Obtain general surgery, orthopedics, ENT, or dental consultation for the appropriate special clinical scenarios. Implementation Items Created three care algorithms (two for the Emergency Department, and one for inpatients) as well as an antibiotic table to address common clinical scenarios Developed a Learning Center training module for the management of community acquired cellulitis and Developed a multi-phase PowerPlan, with ED, inpatient, and discharge phases Metrics Plan Cellulitis Process Metrics Antibiotic Change/Vancomycin Rate AIM : fewer than 10% of eligible population should change from clindamycin or cefazolin to vancomycin. ED Antibiotics for Home Rate AIM: reduce antibiotic prescription rate to 15% among patients undergoing I&D for who are discharged from the ED PDCA Plan Quarterly Review of Metrics, Literature Review, E-Feedback, and Audit Reports will inform Improvement efforts Revision History Date Approved: August, 2013 Next Review Date: August, 2016
9 Executive Summary
10 Self-Assessment Completion qualifies you for 1 hour of Category II CME credit. If you are taking this self-assessment as a part of required departmental training at Seattle Children s Hospital, you MUST logon to Learning Center (for SCH only) Cellulitis and Abscess: Test your knowledge! 1. When evaluating a patient for SSTI, blood cultures should be drawn: a) From all patients with suspected SSTI b) From patients with cellulitis only c) From patients with only d) From patients with systemic toxicity or suspected necrotizing fasciitis. 2. Abscesses that have been adequately drained may be discharged home without antibiotics if a) >1 year old b) Well appearing c) Reliable followup within 2 days d) All of the above Test Your Knowledge 2 Answer Key
11 Self-Assessment Completion qualifies you for 1 hour of Category II CME credit. If you are taking this self-assessment as a part of required departmental training at Seattle Children s Hospital, you MUST logon to Learning Center (for SCH only) Cellulitis and Abscess: Test your knowledge! 3. A patient has an uncomplicated non-suppurative cellulitis. The patient should be discharged home with: a) Cephalexin b) Trimethoprim-Sulfamethoxazole c) Clindamycin d) No antibiotics. 4. A patient presents to the ED for evaluation of a suspected pilonidal. You should consult: a) Plastic surgery b) General surgery c) Orthopedic surgery d) All of the above Test Your Knowledge 3 Answer Key
12 Self-Assessment Completion qualifies you for 1 hour of Category II CME credit. If you are taking this self-assessment as a part of required departmental training at Seattle Children s Hospital, you MUST logon to Learning Center (for SCH only) Cellulitis and Abscess: Test your knowledge! 5. A patient is admitted after an I&D of a buttock with significant surrounding cellulitis. You would treat initially start treatment with: a) Vancomycin b) Clindamycin c) Cefazolin d) Trimethoprim-sulfamethoxazole e) Cephalexin Test Your Knowledge Test Your Knowledge 2 Answer Key
13 Cellulitis and Abscess: Answer Key! Answers: 1. d 2. d 3. a 4. b 5. b Test Your Knowledge Test Your Knowledge 2 Test Your Knowledge 3
14 Evidence Ratings We used the GRADE method of rating evidence quality. Evidence is first assessed as to whether it is from randomized trial, or observational studies. The rating is then adjusted in the following manner: Quality ratings are downgraded if studies: Have serious limitations Have inconsistent results If evidence does not directly address clinical questions If estimates are imprecise OR If it is felt that there is substantial publication bias Quality ratings can be upgraded if it is felt that: The effect size is large If studies are designed in a way that confounding would likely underreport the magnitude of the effect OR If a dose-response gradient is evident Quality of Evidence: High quality Moderate quality Low quality Very low quality Expert Opinion (E) Reference: Guyatt G et al. J Clin Epi 2011: To Bibliography
15 Summary of Version Changes Version 1 (08/15/2013): Go live Version 1.1 (11/6/2013): Clarified which patients should receive Orthopedic consultation in the ED; recommended laboratory studies to be performed prior to Orthopedic consultation; excluded patients with solitary dental from the ED phase
16 Medical Disclaimer Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor Seattle Children s Healthcare System nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from the use of such information. Readers should confirm the information contained herein with other sources and are encouraged to consult with their health care provider before making any health care decision.
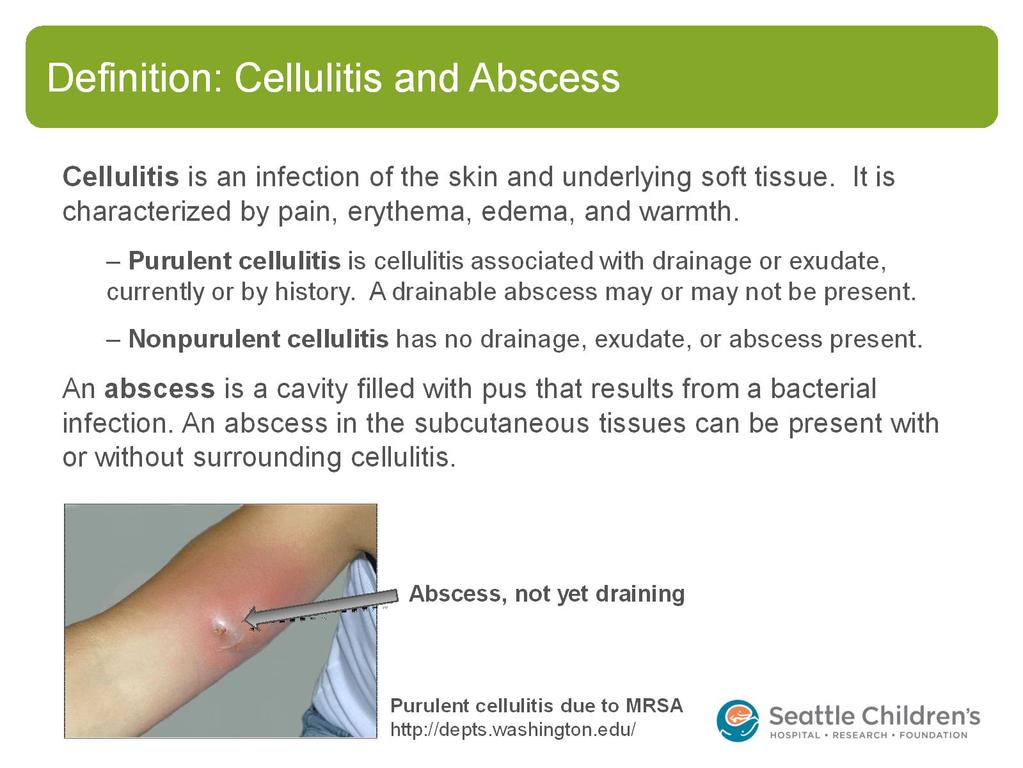
17 Background Many patients present to their health care providers, urgent care clinics, or the emergency department for evaluation and treatment of soft tissue infections. Some have a simple cellulitis that is often easily treated with antibiotics, while others have more complicated infections that require extensive incision and drainage or hospitalization. In addition to Streptococcus pyogenes and methicillin-sensitive Staphylococcus aureus (MSSA), methicillin-resistant Staphylococcus aureus (MRSA) has also become a real consideration in these types of infections. This pathway s intent is to standardize to the extent possible the diagnosis and management of such soft tissue infections at Seattle Children s.
18 Introduction Cellulitis and Abscess This clinical standard work pathway is meant to guide the diagnosis and management of patients with cellulitis and/or. Inclusion criteria: Suspected community-acquired skin and soft tissue infection in a child > 44 weeks CGA Exclusion criteria: o Hospital-acquired, surgical site and device-associated infections o Pressure ulcers o Orbital/periorbital cellulitis o Immunodeficiency o Presumed necrotizing fasciitis o Solitary dental es o Note: For the inpatient phase, we additionally exclude peri-anal es, pilonidal es, deep structure infections, and patients admitted to surgical services. Initial ED management is provided in the ED phase, however.
19
. Approximately 27% of S aureus isolates from wounds are MRSA at Seattle Children s (2012-13 data) S. pyogenes (GAS) http://textbookofbacteriology.")
20 Microbiology Nonpurulent cellulitis is usually due to group A streptococci (although studies are limited due to the difficulty culturing from these infections) Purulent cellulitis may be caused by MSSA, MRSA, or group A streptococci (GAS). Approximately 27% of S aureus isolates from wounds are MRSA at Seattle Children s ( data) S. pyogenes (GAS)
21 Risk factors for MRSA History in the last 6 months of: MRSA in the patient MRSA in the family Recurrent boils, pustules, spider bites, etc. that required antibiotics, in patient or family
22 Examining a soft tissue infection Erythema, warmth, edema universally present Induration or fluctuance (the latter diagnostic of fluid collection) may be present Signs of possible necrotizing infection: Very rapid spread Bluish discoloration, blistering, pain out of proportion or beyond the edges of the lesion, skin anesthesia, rapid progression, or gas in the tissue These signs sometimes appear late in course When first examining, draw a line (mark date/time) around lesion s borders, if not already present
23 Diagnostic testing Use bedside ultrasound where available to improve the accuracy in diagnosis of subcutaneous es (Squire, Tayal ) Obtain wound cultures when possible; i.e., in patients who have spontaneously draining lesions and in patients who undergo I&D procedures (Liu, local consensus [LC]) Routine blood testing (CBC, CRP, blood culture) is not necessary for most children with SSTI (Stevens, LC) Obtain a CBC, CRP, and blood cultures in children with signs of systemic toxicity, including ill-appearance, rapidly spreading lesions, persistent fevers, and age <1yo (Liu, Stevens, LC)
24 Surgical consultation Specific locations of cellulitis/ warrant subspecialist consultation to evaluate for deeper and more serious/complicated extension of infection. Orthopedics: Infections over joints, infections of hand/fingers/feet General surgery: Peri-anal (within 1 cm of anal verge), pilonidal, perineal, breast ENT: Neck Dental: Facial cellulitis of dental origin (LC) Note: Also consult General Surgery if an inpatient develops any requiring drainage (LC)
25 Laboratory studies prior to Orthopedic consultation Prior to consulting Orthopedics, obtain the following: Blood work: Complete blood count with differential, C-reactive protein, and erythrocyte sedimentation rate. Consider blood culture for ill-appearing or febrile patients. Radiographs: Obtain appropriate films of the affected area; typically more than one view is required (LC) Note: The above studies will need to be ordered as needed from outside the Cellulitis and Abscess PowerPlan.
26 Incision and drainage (I&D) No drainage is needed for es <1 cm on bedside ultrasound; these patients may be discharged home on antibiotics alone with close PCP follow-up (Tayal, LC) Larger es require thorough I&D of purulent material with adequate sedation and analgesia Ketamine sedation is frequently needed in pediatric patients, though local anesthesia will also provide some pain relief Consider surgical consultation for very large or complicated es that may require extensive exploration or prolonged sedation time All patients who have had an I&D procedure should have reliable follow-up for re-evaluation with their PCP in hours Incision and drainage (continued) Correct incision and drainage technique is the cornerstone of treating es. If you perform I&D, the following video is a good reminder of proper techniques: Return to Home
27 Incision and drainage (continued) Correct incision and drainage technique is the cornerstone of treating es. If you perform I&D, the following video is a good reminder of proper techniques:
28 Antibiotics for post I&D No oral antibiotics are needed for simple es that have been incised and drained completely, (Duong, Chen, Paydar, and Hankin ) unless the patient has one of the following: Severe or extensive disease Rapid progression in presence of associated cellulitis Signs and symptoms of systemic illness Associated comorbidities or immunosuppression Extremes of age (<1 year old) Abscess in area difficult to drain (face, hand, and genitalia) Associated septic phlebitis Lack of response to I &D alone (Liu )

29 Antibiotics for (continued) Prescribe oral clindamycin for outpatient treatment of es that could not have an adequate I&D, or do not meet low-risk criteria as summarized below (Liu )
30 Antibiotics for nonpurulent cellulitis Prescribe an oral beta lactam (cephalexin) for outpatient treatment of simple cellulitis without an, drainage, history of drainage, or failure of outpatient antibiotic course (>48 h on appropriate antibiotics) (Liu, Stevens, Elliott, and Williams ) Prescribe an IV beta lactam (cefazolin) for inpatient treatment of simple cellulitis without an, drainage, history of drainage, or failure of outpatient antibiotic course (>48 h on appropriate antibiotic) (Liu and Stevens ) Prescribe oral clindamycin for cellulitis that has not responded to anti- MSSA therapy (beta lactam, >48 hours) (Liu, LC) Consider IV vancomycin for inpatient treatment of cellulitis in patients who are systemically ill (fever >38, tachycardia, vomiting) or have failed an outpatient antibiotic course that covers MRSA (Liu ) Antibiotics for purulent cellulitis Prescribe oral clindamycin for outpatient treatment of purulent cellulitis or cellulitis that has not responded to anti-mssa therapy (beta lactam, >48 hours) (Liu, LC) Prescribe IV clindamycin for inpatient treatment of purulent cellulitis or cellulitis that has not responded to anti-mssa therapy (beta lactam, >48 hours) (Liu, LC) Prescribe IV vancomycin for inpatient treatment of cellulitis in patients who are systemically ill (fever >38, tachycardia, vomiting) or have failed antibiotic therapy that covers MRSA (Liu )

31 ED Cellulitis / Abscess pathway Antibiotic selection
32 Empiric antibiotic selection Non-purulent cellulitis Purulent SSTI/ Bite wounds IV choice Cefazolin Clindamycin Ampicillin/sulbactam Facial cellulitis of dental origin Penicillin OR Ampicillin/sulbactam IV Alternatives Clindamycin if cephalosporin allergic Consider vancomycin if rapidly progressive lesion; hemodynamic instability; illappearing Vancomycin if presumed clindamycin resistant MRSA; rapidly progressive lesion; hemodynamic instability; illappearing; failed oral clindamycin as outpatient; in an area difficult to drain completely such as face/hand/genitals Call ID if linezolid desired Cefoxitin (transition to clindamycin AND ciprofloxacin at discharge) if penicillin allergic Clindamycin if penicillin allergic PO choice PO Alternatives Cephalexin Clindamycin if cephalosporin allergic No antibiotics if low risk criteria met and adequately drained Clindamycin otherwise TMP/SMX if presumed clindamycin resistant MRSA Doxycycline if age >8 years and prior clindamycin and TMP/SMX resistant MRSA OR presumed clindamycin resistance and sulfa allergy Call ID if linezolid desired Amoxicillin/clavulanate Doxycycline if age >8 years and penicillin allergy Clindamycin AND ciprofloxacin for penicillin allergic patients Call ID for other scenarios Penicillin OR Amoxicillin/clavulanate Clindamycin if penicillin allergic
33 Admission criteria Patients who should be admitted: Are systemically ill (ill-appearance, persistent fevers, hemodynamic instability etc.) Are unable to tolerate oral therapy Fail appropriate outpatient therapy (48 hours of treatment and not showing signs of improvement) Have rapidly progressive lesions Need pain control or wound care Consider if < 6 months of age Adequate follow up not available (LC)

34 Inpatient pathway daily flow Reevaluate lesion daily or with significant changes Follow microbiology cultures, and change to the narrowest spectrum antibiotic once sensitivities are available Consult general surgery if an develops that necessitates drainage
35 Treatment failure Treatment failure occurs if there is: Significant or rapid expansion of cellulitis at any point in the course of treatment (i.e. more than just one or two centimeters beyond margins), or Cellulitis is not showing improvement after 48 hours of effective antibiotic treatment (LC) The development of a new within an area of previous infection while on antibiotics does not in and of itself constitute treatment failure Note: Referring physicians will be asked to outline lesions with permanent marker if possible before sending patients to the ED and make the patient NPO; lesions will be outlined in ED triage if not already done
36 Switching to oral antibiotics Conversion from an IV to oral antibiotic prior to discharge is not necessary (LC) If worries about palatability or concerns about administration exist, a single oral antibiotic dose may be given prior to discharge (LC)
37 Discharge criteria A patient is ready for discharge when: Lesion(s) show signs of improvement Tolerating PO Pain well controlled No fever > 24 hours Follow up assured within 48 hours (LC) Patients should complete 7-10 total days of antibiotic treatment. (LC, Liu ). Antibiotic treatment can be extended by the PCP if the lesion is not completely resolved at the end of this course.
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
S aureus infections: outpatient treatment. Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium
 S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
Skin and Soft Tissue Infections Emerging Therapies and 5 things to know
 2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
Mrsa abscess and cellulitis
 Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Le infezioni di cute e tessuti molli
 Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections. Skin & Soft Tissue Infections (SSTI)
 Skin & Soft Tissue Infections. Skin & Soft Tissue Infections (SSTI)") Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections 2007 Abscess Cellulitis Bradley W Frazee, MD, FACEP Dept of Emergency Medicine Alameda County Medical Center - Highland Hospital Associate
Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections 2007 Abscess Cellulitis Bradley W Frazee, MD, FACEP Dept of Emergency Medicine Alameda County Medical Center - Highland Hospital Associate
Quality Improvement Case Study Don Buckingham, MBOE Senior Quality Improvement Service Line Coordinator
 Quality Improvement Case Study Don Buckingham, MBOE Senior Quality Improvement Service Line Coordinator Began my QI Journey not quite 10 years ago Capstone Project as EVP Marketing Distribution Submitted
Quality Improvement Case Study Don Buckingham, MBOE Senior Quality Improvement Service Line Coordinator Began my QI Journey not quite 10 years ago Capstone Project as EVP Marketing Distribution Submitted
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections
 Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust
 PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
Clinical Practice Standard
 Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Diagnosis and Management of Skin and Soft-tissue Infections
 Diagnosis and Management of Skin and Soft-tissue Infections Skin and soft tissue infections (SSTIs), are referred as skin and skin structure infections. These infections also represent a group of infections
Diagnosis and Management of Skin and Soft-tissue Infections Skin and soft tissue infections (SSTIs), are referred as skin and skin structure infections. These infections also represent a group of infections
This survey was sent only to EIN members with a pediatric infectious diseases practice.
 Infectious Diseases Society of America Emerging Infections Network Report for Query: Pediatric Outpatient Parenteral Antibiotic Therapy (OPAT) Overall response rate: 188/281 (66.9%) physicians responded
Infectious Diseases Society of America Emerging Infections Network Report for Query: Pediatric Outpatient Parenteral Antibiotic Therapy (OPAT) Overall response rate: 188/281 (66.9%) physicians responded
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES:
CELLULITIS / SKIN INFECTIONS
 Skin Infections Assessment Investigations Cellulitis Management Abscess Management Infection Control Antibiotic Choice Education Recurrent Infections Referral to Community Nursing References Skin Infections
Skin Infections Assessment Investigations Cellulitis Management Abscess Management Infection Control Antibiotic Choice Education Recurrent Infections Referral to Community Nursing References Skin Infections
5/17/2012 DISCLOSURES OBJECTIVES CONTEMPORARY PEDIATRICS
 CONTEMPORARY PEDIATRICS Surgical Management of MRSA Soft Tissue Infections John M. Draus, Jr., M.D. Assistant Professor of Surgery and Pediatrics Kentucky Children s Hospital University of Kentucky DISCLOSURES
CONTEMPORARY PEDIATRICS Surgical Management of MRSA Soft Tissue Infections John M. Draus, Jr., M.D. Assistant Professor of Surgery and Pediatrics Kentucky Children s Hospital University of Kentucky DISCLOSURES
Clinical Management of Skin and Soft Tissue Infections in the U.S. Emergency Departments
 Original Research Clinical Management of Skin and Soft Tissue Infections in the U.S. Emergency Departments Rakesh D. Mistry, MD, MS* Daniel J. Shapiro, BA Monika K. Goyal, MD Theoklis E. Zaoutis Jeffrey
Original Research Clinical Management of Skin and Soft Tissue Infections in the U.S. Emergency Departments Rakesh D. Mistry, MD, MS* Daniel J. Shapiro, BA Monika K. Goyal, MD Theoklis E. Zaoutis Jeffrey
Skin Infections and Antibiotic Stewardship: Analysis of Emergency Department Prescribing Practices,
 Original Research Skin Infections and Antibiotic Stewardship: Analysis of Emergency Department Prescribing Practices, 2007-2010 Daniel J. Pallin, MD, MPH Carlos A. Camargo Jr, MD, DrPH Jeremiah D. Schuur,
Original Research Skin Infections and Antibiotic Stewardship: Analysis of Emergency Department Prescribing Practices, 2007-2010 Daniel J. Pallin, MD, MPH Carlos A. Camargo Jr, MD, DrPH Jeremiah D. Schuur,
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process High Priority
 MEASURE TYPE: Process High Priority") Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Healthcare Associated
Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Healthcare Associated
Cellulitis. Assoc Prof Mark Thomas. Conference for General Practice Auckland Saturday 28 July 2018
 Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Bacterial skin infection
 D i v i s i o n o f P e d i a t r i c E m e r g e n c y M e d i c i n e P a g e 1 Bacterial skin infection Cellulitis w/o abscess Abscess Deep tissue involvement Multiple abscesses Perirectal Anterior
D i v i s i o n o f P e d i a t r i c E m e r g e n c y M e d i c i n e P a g e 1 Bacterial skin infection Cellulitis w/o abscess Abscess Deep tissue involvement Multiple abscesses Perirectal Anterior
Acute Pyelonephritis POAC Guideline
 Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
11/22/2016. Antimicrobial Stewardship Update Disclosures. Outline. No conflicts of interest to disclose
 Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
The Three R s Rethink..Reduce..Rocephin
 The Three R s Rethink..Reduce..Rocephin By: Alisa Cuff RN,BN,CIC and John Bautista B.Sc. (Chem), B.Sc.Pharm, M.Sc.Pharm IPAC National Conference 2017 Newfoundland and Labrador Regional Health Authorities
The Three R s Rethink..Reduce..Rocephin By: Alisa Cuff RN,BN,CIC and John Bautista B.Sc. (Chem), B.Sc.Pharm, M.Sc.Pharm IPAC National Conference 2017 Newfoundland and Labrador Regional Health Authorities
Replaces:04/14/16. Formulated: 1997 SKIN AND SOFT TISSUE INFECTION
 Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
Staph Cases. Case #1
 Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Approval Signature: Original signed by Dr. Michel Tetreault Date of Approval: July Review Date: July 2017
 WRHA Infection Prevention and Control Program Operational Directives Admission Screening for Antibiotic Resistant Organisms (AROs): Methicillin Resistant Staphylococcus aureus (MRSA) and Vancomycin Resistant
WRHA Infection Prevention and Control Program Operational Directives Admission Screening for Antibiotic Resistant Organisms (AROs): Methicillin Resistant Staphylococcus aureus (MRSA) and Vancomycin Resistant
Overview Management of Skin and Soft Tissue Infections in the MRSA Era
 Overview Management of Skin and Soft Tissue Infections in the MRSA Era April 2011 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Management of Recurrent SSTIs Necrotizing soft
Overview Management of Skin and Soft Tissue Infections in the MRSA Era April 2011 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Management of Recurrent SSTIs Necrotizing soft
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING HIP AND KNEE ARTHROPLASTY
 Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING HIP AND KNEE ARTHROPLASTY FINAL Working Group: Dominik Mertz (Chair) Elizabeth Henderson, Johan
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING HIP AND KNEE ARTHROPLASTY FINAL Working Group: Dominik Mertz (Chair) Elizabeth Henderson, Johan
Antibiotic Prophylaxis in Spinal Surgery Antibiotic Guidelines. Contents
 Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Infectious Disease Update 2017
 Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
FM - Male, 38YO. MRSA nasal swab (+) Due to positive MRSA nasal swab test, patient will be continued on Vancomycin 1500mg IV q12 for MRSA treatment...
 Due to positive MRSA nasal swab test, patient will be continued on Vancomycin 1500mg IV q12 for MRSA treatment...") Jillian O Keefe Doctor of Pharmacy Candidate 2016 September 15, 2015 FM - Male, 38YO HPI: Previously healthy male presents to ED febrile (102F) and in moderate distress ~2 weeks after getting a tattoo
Jillian O Keefe Doctor of Pharmacy Candidate 2016 September 15, 2015 FM - Male, 38YO HPI: Previously healthy male presents to ED febrile (102F) and in moderate distress ~2 weeks after getting a tattoo
Surgical Site Infections (SSIs)
") Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Methicillin Resistant Staphylococcus aureus:
 Methicillin Resistant Staphylococcus aureus: Action-Oriented Guidance for Community-Based Prevention Jackie Dawson, PhD Public Health Epidemiologist Chelan, Douglas, Grant, Kittitas, & Okanogan Counties
Methicillin Resistant Staphylococcus aureus: Action-Oriented Guidance for Community-Based Prevention Jackie Dawson, PhD Public Health Epidemiologist Chelan, Douglas, Grant, Kittitas, & Okanogan Counties
Risk factors? Insect bites? Hygiene? Household crowding Health literacy
 Recurrent boils Commonest sites face, neck, armpits, shoulders, and buttocks (bottom) infection of the hair root or sweat pore Occur in otherwise healthy people (higher rates in diabetics, eczema, iron
Recurrent boils Commonest sites face, neck, armpits, shoulders, and buttocks (bottom) infection of the hair root or sweat pore Occur in otherwise healthy people (higher rates in diabetics, eczema, iron
Optimizing Antibiotic Stewardship in the ED
 Optimizing Antibiotic Stewardship in the ED Michael Pulia, MD MS FAAEM FACEP Director, UW EM Antibiotic Stewardship Research Program Chair, AAEM Antimicrobial Stewardship Task Force @DrMichaelPulia Learning
Optimizing Antibiotic Stewardship in the ED Michael Pulia, MD MS FAAEM FACEP Director, UW EM Antibiotic Stewardship Research Program Chair, AAEM Antimicrobial Stewardship Task Force @DrMichaelPulia Learning
DRAFT DRAFT. Paediatric Antibiotic Prescribing Guideline. May
 Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Burden of disease of antibiotic resistance The example of MRSA. Eva Melander Clinical Microbiology, Lund University Hospital
 Burden of disease of antibiotic resistance The example of MRSA Eva Melander Clinical Microbiology, Lund University Hospital Discovery of antibiotics Enormous medical gains Significantly reduced morbidity
Burden of disease of antibiotic resistance The example of MRSA Eva Melander Clinical Microbiology, Lund University Hospital Discovery of antibiotics Enormous medical gains Significantly reduced morbidity
Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction
 Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Treatment of septic peritonitis
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Executive Summary: A Point Prevalence Survey of Antimicrobial Use: Benchmarking and Patterns of Use to Support Antimicrobial Stewardship Efforts
 Executive Summary: A Point Prevalence Survey of Antimicrobial Use: Benchmarking and Patterns of Use to Support Antimicrobial Stewardship Efforts Investigational Team: Diane Brideau-Laughlin BSc(Pharm),
Executive Summary: A Point Prevalence Survey of Antimicrobial Use: Benchmarking and Patterns of Use to Support Antimicrobial Stewardship Efforts Investigational Team: Diane Brideau-Laughlin BSc(Pharm),
Breastfeeding Challenges - Mastitis & Breast Abscess -
 CLINICAL PRACTICE GUIDELINE Breastfeeding Challenges - Mastitis & Breast Abscess - SCOPE (Area): Maternity Unit, Emergency Department, Paediatrics SCOPE (Staff): Medical, Midwifery & Nursing DESIRED OUTCOME/OBJECTIVE
CLINICAL PRACTICE GUIDELINE Breastfeeding Challenges - Mastitis & Breast Abscess - SCOPE (Area): Maternity Unit, Emergency Department, Paediatrics SCOPE (Staff): Medical, Midwifery & Nursing DESIRED OUTCOME/OBJECTIVE
Infections caused by Methicillin-Resistant Staphylococcus
 MRSA infections are no longer limited to hospitals. An infectious disease specialist offers insight on what this means for dermatologists. By Robert S. Jones, DO, Reading, PA Infections caused by Methicillin-Resistant
MRSA infections are no longer limited to hospitals. An infectious disease specialist offers insight on what this means for dermatologists. By Robert S. Jones, DO, Reading, PA Infections caused by Methicillin-Resistant
Who should read this document? 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version? 3
 Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process High Priority
 MEASURE TYPE: Process High Priority") Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction Meaningful Measure Area: Appropriate Use of Healthcare 2019 COLLECTION
Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction Meaningful Measure Area: Appropriate Use of Healthcare 2019 COLLECTION
Responders as percent of overall members in each category: Practice: Adult 490 (49% of 1009 members) 57 (54% of 106 members)
 57 (54% of 106 members)") Infectious Diseases Society of America Emerging Infections Network 6/2/10 Report for Query: Perioperative Staphylococcus aureus Screening and Decolonization Overall response rate: 674/1339 (50.3%) physicians
Infectious Diseases Society of America Emerging Infections Network 6/2/10 Report for Query: Perioperative Staphylococcus aureus Screening and Decolonization Overall response rate: 674/1339 (50.3%) physicians
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Oxazolidinone Antibiotics Table of Contents Coverage Policy... 1 General Background... 3 Coding/Billing Information... 5 References... 5 Effective Date...
Cigna Drug and Biologic Coverage Policy Subject Oxazolidinone Antibiotics Table of Contents Coverage Policy... 1 General Background... 3 Coding/Billing Information... 5 References... 5 Effective Date...
Randomized, Controlled Trial of Antibiotics in the Management of Community-Acquired Skin Abscesses in the Pediatric Patient
 PEDIATRICS/ORIGINAL RESEARCH Randomized, Controlled Trial of Antibiotics in the Management of Community-Acquired Skin Abscesses in the Pediatric Patient Myto Duong, MD, MS Stephen Markwell, MA John Peter,
PEDIATRICS/ORIGINAL RESEARCH Randomized, Controlled Trial of Antibiotics in the Management of Community-Acquired Skin Abscesses in the Pediatric Patient Myto Duong, MD, MS Stephen Markwell, MA John Peter,
Development of Drugs for Skin Infections
 EFPIA - Skin Infection comments 1 Development of Drugs for Skin Infections John H Rex, MD EFPIA - Skin Infection comments 2 Skin Infections Significant recent debate: Acceptable forms: A focus on fever
EFPIA - Skin Infection comments 1 Development of Drugs for Skin Infections John H Rex, MD EFPIA - Skin Infection comments 2 Skin Infections Significant recent debate: Acceptable forms: A focus on fever
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING TOTAL HIP AND KNEE ARTHROPLASTY
 Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING TOTAL HIP AND KNEE ARTHROPLASTY FINAL Working Group: E. Henderson, M. John, I. Davis, S. Dunford,
Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING TOTAL HIP AND KNEE ARTHROPLASTY FINAL Working Group: E. Henderson, M. John, I. Davis, S. Dunford,
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
Impact of a Standardized Protocol to Address Outbreak of Methicillin-resistant
 Impact of a Standardized Protocol to Address Outbreak of Methicillin-resistant Staphylococcus Aureus Skin Infections at a large, urban County Jail System Earl J. Goldstein, MD* Gladys Hradecky, RN* Gary
Impact of a Standardized Protocol to Address Outbreak of Methicillin-resistant Staphylococcus Aureus Skin Infections at a large, urban County Jail System Earl J. Goldstein, MD* Gladys Hradecky, RN* Gary
CA-MRSA lesions: What works, what doesn t
 For mass reproduction, content licensing and permissions contact Dowden Health Media. FAMILY David McBride, MD University Student Health Services and the Department of Family Medicine, Boston University
For mass reproduction, content licensing and permissions contact Dowden Health Media. FAMILY David McBride, MD University Student Health Services and the Department of Family Medicine, Boston University
Scottish Surveillance of Healthcare Infection Programme (SSHAIP) Health Protection Scotland SSI Surveillance Protocol 7th Edition 2017 Question &
 Health Protection Scotland SSI Surveillance Protocol 7th Edition 2017 Question &") Contents General... 4 Pre-op... 4 Peri-op... 5 Post-op... 8 Caesarean Section... 12 Orthopaedics... 14 Large Bowel:... 15 Vascular... 17 General Pre-op Q: If a patient is an emergency admission is the
Contents General... 4 Pre-op... 4 Peri-op... 5 Post-op... 8 Caesarean Section... 12 Orthopaedics... 14 Large Bowel:... 15 Vascular... 17 General Pre-op Q: If a patient is an emergency admission is the
Who should read this document 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version 3. Policy/Procedure/Guideline 3
 Antibiotic Prophylaxis in Cranial Neurosurgery Antibiotic Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Antibiotic Prophylaxis in Cranial Neurosurgery Antibiotic Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
SASKATCHEWAN REGISTERED NURSES ASSOCIATION. RNs WITH ADDITIONAL AUTHORIZED PRACTICE CLINICAL DECISION TOOL DECEMBER 1, 2016 MASTITIS ADULT & PEDIATRIC
 DEFINITION An inflammatory condition of the breast, possibly accompanied by infection and usually associated with lactation. Can be seen in non-lactating clients. IMMEDIATE CONSULTATION REQUIRED IN THE
DEFINITION An inflammatory condition of the breast, possibly accompanied by infection and usually associated with lactation. Can be seen in non-lactating clients. IMMEDIATE CONSULTATION REQUIRED IN THE
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
IAEM Clinical Guideline 6 Bite Wound Management in Adults and Children Version 1 July 2016
 IAEM Clinical Guideline 6 Bite Wound Management in Adults and Children Version 1 July 2016 Authors: Dr Sinead Ni Bhraonain, Dr Jessica Pflipsen, Dr Éanna Mac Suibhne Guideline lead: Dr Termizi Hassan,
IAEM Clinical Guideline 6 Bite Wound Management in Adults and Children Version 1 July 2016 Authors: Dr Sinead Ni Bhraonain, Dr Jessica Pflipsen, Dr Éanna Mac Suibhne Guideline lead: Dr Termizi Hassan,
Antimicrobial Stewardship 101
 Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship
 Curriculum for Antimicrobial Stewardship") General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
Skin & Soft Tissue Infections (SSTIs)
") Skin & Soft Tissue Infections (SSTIs) Marnie Peterson, Pharm.D., Ph.D. College of Pharmacy peter377@umn.edu (612) 626-4388 SSTIs Objectives To classify types of skin infections To present a case of cellulitis
Skin & Soft Tissue Infections (SSTIs) Marnie Peterson, Pharm.D., Ph.D. College of Pharmacy peter377@umn.edu (612) 626-4388 SSTIs Objectives To classify types of skin infections To present a case of cellulitis
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings. Carlos Reyes Sacin, MD, AAHIVS
 Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
For analyst certification and disclosures please see page 7
 Physician Survey Survey of Healthcare Professionals on Community-Acquired Bacterial Pneumonia We conducted a survey on prescribing habits for community-acquired bacterial pneumonia (CABP) in order to better
Physician Survey Survey of Healthcare Professionals on Community-Acquired Bacterial Pneumonia We conducted a survey on prescribing habits for community-acquired bacterial pneumonia (CABP) in order to better
Clinical Guideline. District Infectious Diseases Management. Go to Guideline. District Infectious Diseases Management CG 18_24
 Clinical Guideline District Infectious Diseases Management Sites where Clinical Guideline applies All facilities This Clinical Guideline applies to: 1. Adults Yes 2. Children up to 16 years Yes 3. Neonates
Clinical Guideline District Infectious Diseases Management Sites where Clinical Guideline applies All facilities This Clinical Guideline applies to: 1. Adults Yes 2. Children up to 16 years Yes 3. Neonates
A review of in-patient hand infections
 Archives of Emergency Medicine, 1992, 9, 299-305 A review of in-patient hand infections A. R. PHIPPS & J. BLANSHARD Department of Plastic and Reconstructive Surgery, Queen Mary's University Hospital, Roehampton
Archives of Emergency Medicine, 1992, 9, 299-305 A review of in-patient hand infections A. R. PHIPPS & J. BLANSHARD Department of Plastic and Reconstructive Surgery, Queen Mary's University Hospital, Roehampton
CLPNA Pressure Ulcers ecourse: Module 5.6 Quiz II page 1
 CLPNA Pressure Ulcers ecourse: Module 5.6 Quiz II 1. What are the symptoms of an infected wound? a. Fever b. Edema c. Erythema d. Local pain and tenderness e. Induration of wound edge 2. A person with
CLPNA Pressure Ulcers ecourse: Module 5.6 Quiz II 1. What are the symptoms of an infected wound? a. Fever b. Edema c. Erythema d. Local pain and tenderness e. Induration of wound edge 2. A person with
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children
 Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prophylactic antibiotic timing and dosage. Dr. Sanjeev Singh AIMS, Kochi
 Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Pharmacist Coordinated Antimicrobial Therapy: OPAT and Transitions of Care
 Pharmacist Coordinated Antimicrobial Therapy: OPAT and Transitions of Care Jennifer McCann, PharmD, BCCCP State Director of Clinical Pharmacy Services St. Vincent Health Indiana Conflicts of Interest No
Pharmacist Coordinated Antimicrobial Therapy: OPAT and Transitions of Care Jennifer McCann, PharmD, BCCCP State Director of Clinical Pharmacy Services St. Vincent Health Indiana Conflicts of Interest No
ANTIBIOTICS IN THE ER:
 ANTIBIOTICS IN THE ER: EXPLORING THE ROLE OF ANTIMICROBIAL STEWARDSHIP IN THE EMERGENCY DEPARTMENT ANGELINA DAVIS, PHARMD, MS, BCPS (AQ-ID) LIAISON CLINICAL PHARMACIST DUKE ANTIMICROBIAL STEWARDSHIP OUTREACH
ANTIBIOTICS IN THE ER: EXPLORING THE ROLE OF ANTIMICROBIAL STEWARDSHIP IN THE EMERGENCY DEPARTMENT ANGELINA DAVIS, PHARMD, MS, BCPS (AQ-ID) LIAISON CLINICAL PHARMACIST DUKE ANTIMICROBIAL STEWARDSHIP OUTREACH
Antimicrobial Stewardship Strategy: Antibiograms
 Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Antimicrobial Stewardship Strategy:
 Antimicrobial Stewardship Strategy: Prospective audit with intervention and feedback Formal assessment of antimicrobial therapy by trained individuals, who make recommendations to the prescribing service
Antimicrobial Stewardship Strategy: Prospective audit with intervention and feedback Formal assessment of antimicrobial therapy by trained individuals, who make recommendations to the prescribing service
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
COMMUNITY ASSOCIATED METHICILLIN-RESISTANT STAPHLOCOCCUS AUREUS A PRACTICAL GUIDE FOR PRIMARY CARE PRACTITIONERS
 COMMUNITY ASSOCIATED METHICILLIN-RESISTANT STAPHLOCOCCUS AUREUS A PRACTICAL GUIDE FOR PRIMARY CARE PRACTITIONERS December 21, 2010 Background Since it was first described in 1961 methicillin resistant
COMMUNITY ASSOCIATED METHICILLIN-RESISTANT STAPHLOCOCCUS AUREUS A PRACTICAL GUIDE FOR PRIMARY CARE PRACTITIONERS December 21, 2010 Background Since it was first described in 1961 methicillin resistant
Study population The target population for the model were hospitalised patients with cellulitis.
 Comparison of linezolid with oxacillin or vancomycin in the empiric treatment of cellulitis in US hospitals Vinken A G, Li J Z, Balan D A, Rittenhouse B E, Willke R J, Goodman C Record Status This is a
Comparison of linezolid with oxacillin or vancomycin in the empiric treatment of cellulitis in US hospitals Vinken A G, Li J Z, Balan D A, Rittenhouse B E, Willke R J, Goodman C Record Status This is a
$100 $200 $300 $400 $500
 Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Antimicrobial Stewardship in the Hospital Setting
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 12 Antimicrobial Stewardship in the Hospital Setting Authors Dan Markley, DO, MPH, Amy L. Pakyz, PharmD, PhD, Michael Stevens, MD, MPH Chapter Editor
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 12 Antimicrobial Stewardship in the Hospital Setting Authors Dan Markley, DO, MPH, Amy L. Pakyz, PharmD, PhD, Michael Stevens, MD, MPH Chapter Editor
Impact of Antimicrobial Stewardship Program
 Impact of Antimicrobial Stewardship Program Ripal Joshi, Pharm.D. AAHIVP Tampa General Hospital January 28, 2016 Objectives Provide an overview on antimicrobial stewardship programs (ASP) Describe the
Impact of Antimicrobial Stewardship Program Ripal Joshi, Pharm.D. AAHIVP Tampa General Hospital January 28, 2016 Objectives Provide an overview on antimicrobial stewardship programs (ASP) Describe the
Can you treat mrsa with amoxicillin
 Can you treat mrsa with amoxicillin 15-8-2017 Community-associated MRSA You can pick up MRSA outside the hospital, especially if you :. (a related drug developed to treat these germs). Amoxicillin and
Can you treat mrsa with amoxicillin 15-8-2017 Community-associated MRSA You can pick up MRSA outside the hospital, especially if you :. (a related drug developed to treat these germs). Amoxicillin and
Inappropriate Use of Antibiotics and Clostridium difficile Infection. Jocelyn Srigley, MD, FRCPC November 1, 2012
 Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Peri-operative Antibiotic Prophylaxis. 2 nd QI Cycle results Compiled by: Dr Stella Sasha
 Peri-operative Antibiotic Prophylaxis 2 nd QI Cycle results Compiled by: Dr Stella Sasha 2 nd QI cycle 4 weeks (11 April 8 May) Elective MIS cases Hysterectomy +/- salpingo-oophorectomy Myomectomy Oophorectomy
Peri-operative Antibiotic Prophylaxis 2 nd QI Cycle results Compiled by: Dr Stella Sasha 2 nd QI cycle 4 weeks (11 April 8 May) Elective MIS cases Hysterectomy +/- salpingo-oophorectomy Myomectomy Oophorectomy
DATA COLLECTION SECTION BY FRONTLINE TEAM. Patient Identifier/ Medical Record number (for facility use only)
") Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Safety of an Out-Patient Intravenous Antibiotics Programme
 Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial