Neurosurgical infections: New developments and outlook
|
|
|
- Noel Summers
- 5 years ago
- Views:
Transcription
1 IMPLANTS Neurosurgical infections: New developments and outlook Andrej Trampuz, MD Infectious Diseases Specialist Head, Center for Septic Surgery Mª Eugenia Portillo, PhD Microbiologist Head, Microbiology Laboratory Berlin, Germany Barcelona, Pamplona, Berlin Overview: What is new? Post-surgical infections Post-craniotomy infection Bacterial meningitis Brain abscess Shunt-, drain- and neurostimulator infections VP-shunts External ventricular drain Deep brain stimulation Spine infections Hematogenous Hardware infections 1






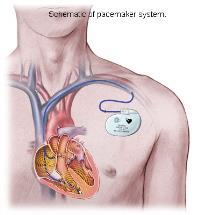

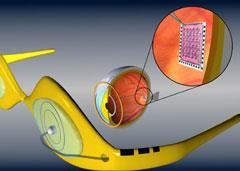

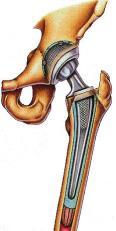

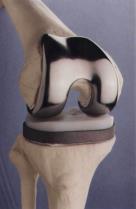



2 Implants improved life quality 2
3 Risk of implant-associated infection Device No. inserted in the US, per year Infection rate, % Fracture fixation devices 2,000, Dental implants 1,000, Joint prostheses 600, Neurosurgical implants 450, Cardiac pacemakers 300, Mammary implants 130, Mechanical heart valves 85, Penile implants 15, Heart assist devices Darouiche RO. Clin Infect Dis 2011;33: Pathogenesis of foreign-body infection References Foreign Min. infectious dose Pathogen (model) body (FB) no FB with FB Elek 1957 Sutures 5 x x 10 2 S. aureus (human) James 1961 Sutures 10 6 <10 3 S. aureus (mice) Zimmerli 1982 Cages > S. aureus (guinea pigs) Widmer 1988 Cages > S. epidermidis (guinea pigs) 3
4 Successful treatment concepts based on: 1. Biofilm 2. Diagnosis 3. Surgery 4. Antibiotics Against biofilms Cure rate >90% Infection is the best possible complication Key to success Interdisciplinary team Microbiologist Infectious diseases Surgeon 4




5 Diagnosis Normal microbiota of the skin bacteria/cm 2 - Staphylococci - Staphylococcus epidermidis - Staphylococcus aureus - Diphteroids - Corynebacterium spp. - Propionibacterium acnes 5

6 Classification Time after implantation <1 month 3 36 months Any time Type of infection Early postoperative Delayed (low grade) Late Route Perioperative Haematogenous Signs Acute: fever, effusion, warmth, dehiscence Chronic: Persistent pain, loosening, sinus tract Acute or subacute Pathogen Staph. aureus Streptococci Enterococci Staph. epidermidis Propionibacterium acnes S. aureus E. coli Biofilm 1 min 3 h 12 h 1 day 3 days Adherent to surface (min-h) Embedded in matrix (70%) Slowly replicating (stacionary-growth) 6








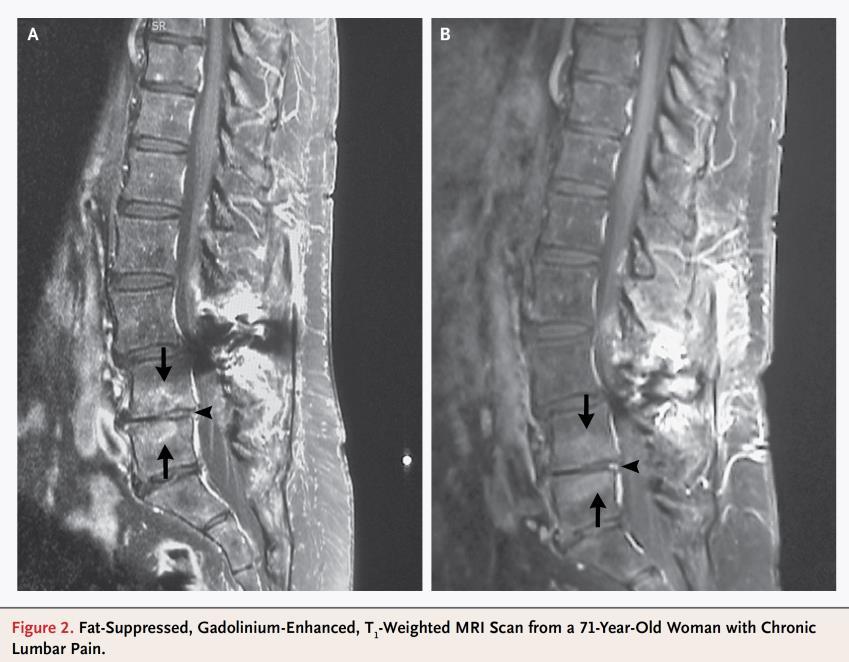
7 Sonication for implants Removed implants Vortex, 30 s Sonication, 1 min, 40 khz May 2005 Feb 2007 Standard method ( 3 tissue biopsies) Tissue Sonicate Trampuz A et al. N Engl J Med 2007;357: Principle of sonication Mechanical vibrations >20 khz Microbubbles (cavitation) 7
 Breast implants (Rieger UM et al. Aesth Plast Surg 2009) Electrophysiologic cardiac devices (Rohacek M et al.")
8 Better sensitivity (80-90%) Quantitative (more specific) Mixed infections (30%) Faster, less expensive Fluid for additional investigations Tissue biopsy Sonication fluid Sonication studies with implants Shoulder prosthesis (Piper KE et al. JCM 2009) Breast implants (Rieger UM et al. Aesth Plast Surg 2009) Electrophysiologic cardiac devices (Rohacek M et al. Circulation 2010) Spine implants (Sampedro M et al. Spine 2010) Ureteric catheters (Bonkat G et al. W J Urol 2010) Pacemaker (Mason PK et al. Pacing Clin Electrophysiol 2011) Joint prostheses (Portillo ME et al. J Clin Microbiol 2012) Osteosynthesis material (Portillo ME et al. J Clin Microbiol 2015) External ventricular drains (Walti L et al. J Infect 2013) 8
9 Antibiotics Antibiotics are not wonder drugs, but can produce wonders, if 1. the microorganism is known 2. given correctly (type, dose) 3. combined with correct surgery 9
10 Antibiotics Bacteriostatic Bactericidal Tigecycline OTHER Azithromycin Clindamycin TETRACYCLINE Minocycline Doxycycline Fusidic acid OXAZOLIDINONE Linezolid Oxytetracycline Teicoplanin LIPOGLYCOPEPTIDE Telavancin GLYCOPEPTIDE Dalbavancin Vancomycin Levofloxacin Ciprofloxacin Nalidixic acid QUINOLONES Moxifloxacin Cefazolin Oxacillin Ampicillin Co-amoxiclav Amoxicillin Flucloxacillin Nafcillin Methicillin Streptomycin BETA-LACTAMS Mupirocin AMINOGLYCOSIDE Amikacin Cephaloridine Ceftaroline Rifampin Gentamicin Daptomycin LIPOPEPTIDE OTHER Penicillin Rolinson GN. Int J Antimicrob Agents 2007;29:3 8 Error: oral drugs with poor bioavailability Drug Oral bioavailability Bone penetration Amoxicillin/clavulanic acid 15% 7% Cefuroxim, cefadroxil 10% 12% Levofloxacin 100% 77% Rifampin 80% 51% Cotrimoxazole 85% 55% Clindamycin 90% 45% Linezolid 100% 85% Sanford Guide to Antimicrobial Therapy nd ed. Lorian. Antibiotics in Laboratory Medicine. 5 th ed. 10


11 Foreign-body infection (FBI) model 4 Teflon cages implanted subcutaneously in guinea pigs Aspiration of cage fluid (planktonic bacteria) Cages removed 5 days after treatment (eradication) Zimmerli W et al. J Clin Invest 1984;73: Efficacy in the guinea pig model (MRSA) 11
12 Antibiotics with antibiofilm activity 1. Staphylococci: Rifampin (in combination) 2. Streptococci: Penicillin (ceftriaxon) 3. Gram-negative bacilli: Ciprofloxacin 4. Enterococci: Fosfomycin + gentamicin (?) 5. Candida: Caspofungin, anidulafungin (?) Surgery 12
13 Bacterial count (log) Postsurgical infections / implant Antibiotic Resistant strains No surgery Insufficient debridement Extensive debridement (+/- local antibiotics) Time Surgical and antibiotic treatment concepts Debridement and retention Onset of infection 2 3 weeks i.v. Explantation and implantation 9 10 weeks p.o. Debridement One stage Explantation Implantation Biofilm treatment (with rifampin) Two stage (short interval) Two stage (long interval) Explantation 6 weeks i.v. Implantation (2 weeks) Osteomyelitis treatment (no rifampin) Zimmerli W et al. N Engl J Med 2004 Borens O et al. Rev Med Suisse
14 Implant retention 1. No dysfunction or loosening 2. Known microorganism 3. Good soft tissue Biofilm eradication In all cases, debidement is needed (to achieve reduction of bacterial number)! Overview: What is new? Post-surgical infections Post-craniotomy infection Bacterial meningitis Brain abscess Shunt-, drain- and neurostimulator infections VP-shunts External ventricular drain Deep brain stimulation Spine infections Hematogenous Hardware-associated infections 14



 Requires surgical revision (debridement) to -")
15 Infection following craniotomy Infection rate: 1-5% Most common symptoms: - Change in mental status - Evidence of wound infection Cave: Bacterial meningitis! Dashti Neurosurg Focus 2008 Superficial and deep wound infections Distinction between superficial and deep wound infection is nonsense: Subgaleal and epidural compartments after craniotomy are in contiguity Any craniotomy infection should be considered a bone flap osteitis (for the treatment standpoint) Requires surgical revision (debridement) to - evacuate pus and infected tissue - remove infected bone flap 15
 Short interval of 2 weeks (2-stage) Bone flap reuse (sterilization, disinfection), acryl or other foreign material (impregnated with antibiotics?")
16 Infection following craniotomy Standard management of bone flap osteitis: Delayed cranioplasty (weeks to months) With foreign material once the infection is cleared New concept: Immediate cranioplasty in low-grade infection (1-stage) Short interval of 2 weeks (2-stage) Bone flap reuse (sterilization, disinfection), acryl or other foreign material (impregnated with antibiotics?) => Better cosmetic result, protect underlying brain Postoperative meningitis Incidence: <1% (recent series) to >8% (without prophylaxis) Life-threatening complication: mortality >20% Diagnosis difficult The clinical manifestations often mild and non-specific CSF characteristics modified by surgical procedure Direct bacteriological examination often negative Risk factors: Implantation of foreign body CSF leakage No antibiotic prophylaxis Duration of surgery >4 h Interventions involving nasal sinuses McClelland CID
17 Treatment: postoperative meningitis/abscess Postoperative meningitis Early empirical antibiotic therapy: Vancomycin 2 x 1 g + meropenem 3 x 2 g i.v. STAT Then targeted treatment, total 2-3 weeks If CSF cultures negative after 72 h, treatment stop Brain abscess Surgical revision or stereotactic puncture Treatment: same as for meningitis Duration: months, after 2 weeks oral (until MRI normal) Overview Post-surgical infections Post-craniotomy infection Bacterial meningitis Brain abscess Shunt-, drain- and neurostimulator infections VP-shunts External ventricular drain Deep brain stimulation Spine infections Hematogenous Hardware-associated infections 17



18 VP-shunt & external drain: Symptoms Infection VP-shunts External drains Risk 5-15% 10-15% (increase with time) VP-shunts: Symptoms Proximal shunt part: ventriculitis / meningitis Distal shunt part: peritonitis, abdominal abscess => Shunt dysfunction (increased ICP) 18
19 VP-shunt infection: CSF leukocyte & culture Suspicion of shunt-infection: lumbar puncture! VP-shunts: Therapy Success: 93% Retention of VP-shunt possible with antibiotics against biofilms 19

 and Microorganisms known Susceptible to antibiotics against")
20 VP-shunts: When retention? Shunt retention or immediate reinsertion possible, if: No ventriculitis / meningitis No dysfunction No abscess No erosion (intact skin and intestinum) and Microorganisms known Susceptible to antibiotics against biofilms EVD infection / meningitis: Symptoms 20

 If removed: optimal time of reimplantation?")
21 EVD infection: CSF leukocyte & culture Culture Deep Brain Stimulation: Infection rate 1-15% When retain the neurostimulator? Pocket infection: generator change (other site), keep the electrodes Electrode infection: no brain abscess, skin erosion covered (flap) If removed: optimal time of reimplantation? If organism known and susceptible to anti-biofilm antibiotics: - immediate (1-stage) or - delayed (after 2 weeks) 21

22 Overview Post-surgical infections Post-craniotomy infection Bacterial meningitis Brain abscess Shunt-, drain- and neurostimulator infections VP-shunts External vetricular drain Deep brain stimulation Spine infections Hematogenous Hardware-associated infections Osteoarticular infections Prosthetic joint infection CNS, S. aureus Streptococcus spp. Enterococcus spp. Propionibacterium acnes Septic arthritis S. aureus Streptococci Enterococci Post-traumatic infection S. aureus Polymicrobial Gramnegative bacilli Vertebral osteomyelitis S. aureus Gramnegative bacilli Streptococcus spp, Mycobacterium tuberculosis Diabetic foot infection S. aureus Streptococcus spp. Enterococcus spp. Gramnegative bacilli Anaerobes S. aureus is the most common pathogen of osteomyelitis 22


23 LWS
24 Vertebral osteomyelitis Hematogenous (urinary, respiratory, intestinal tract, endocarditis, dental): Staphylococcus aureus, streptococci, enterococci E. coli, other gram-negative (Candida albicans) Never surgery! Exogen (skin flora): Postoperative (1% after discectomy, 5% after stabilisation, 10% after revision) Postinterventional (infiltrations) Staphylococcus epidermidis (other coagulase-negative staphylococci), Propionibacterium acnes Always surgery! Hematogenous infection (no implant) Biopsy (percutaneous CT-guided, open): 1. Large needle (gauge) 2. Bone & discus (fluid/abscess) 3. Histology & microbiology 24
25 Antibiotic treatment Empiric (without meningitis): cover S. aureus & gram-neg. Cefepime 3 x 2 g i.v. or Piperacillin/tazobactam 3 x 4,5 g i.v. Empiric (with meningitis): cover everything Meropenem 3 x 2 g i.v. (or cefepime 3 x 2 g i.v.) and Vancomycin 3 x 1 g i.v. (for MRSA) Targeted therapy: switch to optimal antibiotic 2 weeks i.v., then oral Duration: 6 weeks (without implant), 12 weeks (with implant) 25




26 26
 Osteomyelitis treatment (no rifampin) Zimmerli W et al. N Engl J Med 2004 Borens O et al.")
27 Surgical and antibiotic treatment concepts Debridement and retention Onset of infection 2 3 weeks i.v. Explantation and implantation 9 10 weeks p.o. Debridement One stage Explantation Implantation Biofilm treatment (with rifampin) Two stage (short interval) Two stage (long interval) Explantation 6 weeks i.v. Implantation (2 weeks) Osteomyelitis treatment (no rifampin) Zimmerli W et al. N Engl J Med 2004 Borens O et al. Rev Med Suisse 2009 Outlook: diagnosis All removed implants should be sonicated Sonication fluid is usefull for further analysis 27


28 Outlook: New diagnostic methods Microcalorimetry Molecular methods (PCR) MALDI-TOF Corvec S, Portillo ME et al. IJAO 2012 Outlook: Staphylococcus aureus vaccine Adults undergoing elective posterior instrumented lumbar spinal fusion procedures A phase 2b, randomized, double-blind, placebo-controlled study Intervention Single dose: days before surgery 28



29 Conclusions 1. Improved diagnostic methods: sonication for implants, new faster and more accurate methods 2. Anti-biofilm antibiotics: retention, 1-stage exchange or short interval until reimplantation 3. Innovative prevention strategies: vaccination This will likely revolutionize implant surgery: efficient strategy to cure infections without implant removal. European Research Projects Workshops on Implant Infections Berlin, Germany: Patients will be recruited in university and nonuniversity institutions across Europe. Interactive sessions with international experts Educational activities: Books & Apps Observership & Hospitations Center for septic surgery at CMSC Charité Universitätsmedizin Berlin 29





30 Thank you Focus on implant, bone and joint-associated infections: Surgery: New concepts Diagnosis: Fast innovative methods Antibiotics: Active against biofilms 30
Treatment of PJI. Andrej Trampuz Charité University Medicine Berlin Germany
 Treatment of PJI Andrej Trampuz Charité University Medicine Berlin Germany Implants improved life quality Treatment Treatment concept To achieve high treatment success, a concerted surgical and antimicrobial
Treatment of PJI Andrej Trampuz Charité University Medicine Berlin Germany Implants improved life quality Treatment Treatment concept To achieve high treatment success, a concerted surgical and antimicrobial
Pocket Guide to Diagnosis & Treatment of Cardiovascular Implantable Electronic Device (CIED) Infections
 Infections") Pocket Guide to Diagsis & Treatment of Cardiovascular Implantable Electronic Device (CIED) Infections Draft Version : November 208 DEFINITION Pocket infection, if all 4 criteria are fulfilled: Investigation/sign
Pocket Guide to Diagsis & Treatment of Cardiovascular Implantable Electronic Device (CIED) Infections Draft Version : November 208 DEFINITION Pocket infection, if all 4 criteria are fulfilled: Investigation/sign
Who should read this document? 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version? 3
 Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Pocket Guide to Diagnosis & Treatment of Vascular Graft Infections (VGI)
") Pocket Guide to Diagsis & Treatment of Vascular Graft Infections (VGI) DEFINITION Investigation /sign Local signs of infection Histopathology Microbiology Definitive Criteria Purulent wound secretion sinus
Pocket Guide to Diagsis & Treatment of Vascular Graft Infections (VGI) DEFINITION Investigation /sign Local signs of infection Histopathology Microbiology Definitive Criteria Purulent wound secretion sinus
MANAGEMENT OF TOTAL JOINT ARTHROPLASTY INFECTIONS
 MANAGEMENT OF TOTAL JOINT ARTHROPLASTY INFECTIONS Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine TOTAL JOINT ARTHROPLASTIES In 2009: 1 million THA and TKA By 2030,
MANAGEMENT OF TOTAL JOINT ARTHROPLASTY INFECTIONS Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine TOTAL JOINT ARTHROPLASTIES In 2009: 1 million THA and TKA By 2030,
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Full Title of Guideline. Author: Contact Name and Job Title. Division & Speciality. Review date December 2020
 Full Title of Guideline Author: Contact Name and Job Title Division & Speciality Guideline for the treatment of prosthetic joint infections in adults Mr Peter James - Consultant Orthopaedic Surgeon Dr
Full Title of Guideline Author: Contact Name and Job Title Division & Speciality Guideline for the treatment of prosthetic joint infections in adults Mr Peter James - Consultant Orthopaedic Surgeon Dr
Pocket Guide to Diagnosis & Treatment of Ventricular Assist Device (VAD) Infections
 Infections") Pocket Guide to Diagnosis & Treatment of Ventricular Assist Device (VAD) Infections CLASSIFICATION OF VAD-INFECTIONS Draft Version 1: 1 November 2018 from Hannan M et al. Journal of Heart and Lung Transplantation,
Pocket Guide to Diagnosis & Treatment of Ventricular Assist Device (VAD) Infections CLASSIFICATION OF VAD-INFECTIONS Draft Version 1: 1 November 2018 from Hannan M et al. Journal of Heart and Lung Transplantation,
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how?
 Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Who should read this document 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version 3. Policy/Procedure/Guideline 3
 Antibiotic Prophylaxis in Cranial Neurosurgery Antibiotic Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Antibiotic Prophylaxis in Cranial Neurosurgery Antibiotic Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Management of Native Valve
 Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
21 st Expert Committee on Selection and Use of Essential Medicines Peer Review Report Antibiotics Review
 (1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
(1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Help with moving disc diffusion methods from BSAC to EUCAST. Media BSAC EUCAST
 Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE FOR HEALTHCARE ACQUIRED CEREBROSPINAL FLUID SHUNT ASSOCIATED INFECTIONS
 Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE FOR HEALTHCARE ACQUIRED CEREBROSPINAL FLUID SHUNT ASSOCIATED INFECTIONS FINAL November 29, 2017 Working Group: Joanne Langley (Chair),
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE FOR HEALTHCARE ACQUIRED CEREBROSPINAL FLUID SHUNT ASSOCIATED INFECTIONS FINAL November 29, 2017 Working Group: Joanne Langley (Chair),
Principles of Antimicrobial Therapy
 Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Neurosurgery Antibiotic Prophylaxis Guideline
 Neurosurgery Antibiotic Prophylaxis Guideline Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version
Neurosurgery Antibiotic Prophylaxis Guideline Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Introduction to Chemotherapeutic Agents. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018
 Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Le infezioni di cute e tessuti molli
 Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
MANAGEMENT STRATEGIES FOR ORTHOPEDIC IMPLANT-ASSOCIATED INFECTIONS. 5-6 March 2018 Berlin Germany. Endorsed by:
 MANAGEMENT STRATEGIES FOR ORTHOPEDIC IMPLANT-ASSOCIATED INFECTIONS 5-6 March 2018 Berlin Germany Endorsed by: Dear colleagues, It is our great pleasure to invite you to the first workshops on orthopedic
MANAGEMENT STRATEGIES FOR ORTHOPEDIC IMPLANT-ASSOCIATED INFECTIONS 5-6 March 2018 Berlin Germany Endorsed by: Dear colleagues, It is our great pleasure to invite you to the first workshops on orthopedic
Cefuroxime 1.5gm IV and Metronidazole 500mg IV. Metronidazole 500mg IV/Ampicillin-sulbactam e 3g/Ceftriaxone 2gm. +Metronidazole 500mg/Ertapenem 1gm
 SURGICAL ANTIBIOTIC PROPHYLAXIS GENERAL SURGERY* PROCEDURE RECOMMENDED AGENTS a,b Clean None None ALTERNATIVE AGENTS (If allergic to penicillin or colonized/infected with MRSA at any site) Clean with potential
SURGICAL ANTIBIOTIC PROPHYLAXIS GENERAL SURGERY* PROCEDURE RECOMMENDED AGENTS a,b Clean None None ALTERNATIVE AGENTS (If allergic to penicillin or colonized/infected with MRSA at any site) Clean with potential
GUIDELINE FOR ANTIMICROBIAL USE IN THE ORTHOPAEDIC AND TRAUMA DEPARTMENT
 GUIDELINE FOR ANTIMICROBIAL USE IN THE ORTHOPAEDIC AND TRAUMA DEPARTMENT Written by: Dr Ken. N. Agwuh, Consultant Microbiologist Mr Roger Helm, Consultant Orthopaedic Surgeon Mr T Kumar, Consultant Orthopaedic
GUIDELINE FOR ANTIMICROBIAL USE IN THE ORTHOPAEDIC AND TRAUMA DEPARTMENT Written by: Dr Ken. N. Agwuh, Consultant Microbiologist Mr Roger Helm, Consultant Orthopaedic Surgeon Mr T Kumar, Consultant Orthopaedic
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS
 VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Use And Misuse Of Antibiotics In Neurosurgery
 Use And Misuse Of Antibiotics In Neurosurgery CSF infection in the United States after neurosurgery from 1992 to 2003 0.86% to 2.32% * *National Nosocomial Infections Surveillance System: National Nosocomial
Use And Misuse Of Antibiotics In Neurosurgery CSF infection in the United States after neurosurgery from 1992 to 2003 0.86% to 2.32% * *National Nosocomial Infections Surveillance System: National Nosocomial
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Routine internal quality control as recommended by EUCAST Version 3.1, valid from
 Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
Introduction. n Ventricular catheter placement one of the most common neurosurgical procedures
 SHUNT INFECTION Introduction n Ventricular catheter placement one of the most common neurosurgical procedures n One of the most common complications associated is infection n Infection: positive CSF culture/
SHUNT INFECTION Introduction n Ventricular catheter placement one of the most common neurosurgical procedures n One of the most common complications associated is infection n Infection: positive CSF culture/
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS
 PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
Antimicrobial Prophylaxis in the Surgical Patient. M. J. Osgood
 Antimicrobial Prophylaxis in the Surgical Patient M. J. Osgood Outline Definitions surgical site infection (SSI) Risk factors Wound classification Microbiology of SSIs Strategies for prevention of SSIs
Antimicrobial Prophylaxis in the Surgical Patient M. J. Osgood Outline Definitions surgical site infection (SSI) Risk factors Wound classification Microbiology of SSIs Strategies for prevention of SSIs
Antibiotic Prophylaxis Update
 Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
National Clinical Guideline Centre Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults
 National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
ANTIBIOTICS USED FOR RESISTACE BACTERIA. 1. Vancomicin
 ANTIBIOTICS USED FOR RESISTACE BACTERIA 1. Vancomicin Vancomycin is used to treat infections caused by bacteria. It belongs to the family of medicines called antibiotics. Vancomycin works by killing bacteria
ANTIBIOTICS USED FOR RESISTACE BACTERIA 1. Vancomicin Vancomycin is used to treat infections caused by bacteria. It belongs to the family of medicines called antibiotics. Vancomycin works by killing bacteria
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Responders as percent of overall members in each category: Practice: Adult 490 (49% of 1009 members) 57 (54% of 106 members)
 57 (54% of 106 members)") Infectious Diseases Society of America Emerging Infections Network 6/2/10 Report for Query: Perioperative Staphylococcus aureus Screening and Decolonization Overall response rate: 674/1339 (50.3%) physicians
Infectious Diseases Society of America Emerging Infections Network 6/2/10 Report for Query: Perioperative Staphylococcus aureus Screening and Decolonization Overall response rate: 674/1339 (50.3%) physicians
Antimicrobial susceptibility
 Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Antimicrobial Susceptibility Testing: Advanced Course
 Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
EUCAST recommended strains for internal quality control
 EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
SURGICAL ANTIBIOTIC PROPHYLAXIS GUIDELINES WITHIN ORTHOPAEDIC SURGERY FOR ADULT PATIENTS
 SURGICAL ANTIBIOTIC PROPHYLAXIS GUIDELINES WITHIN ORTHOPAEDIC SURGERY FOR ADULT PATIENTS Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if
SURGICAL ANTIBIOTIC PROPHYLAXIS GUIDELINES WITHIN ORTHOPAEDIC SURGERY FOR ADULT PATIENTS Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS
 Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Compliance of manufacturers of AST materials and devices with EUCAST guidelines
 Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
S aureus infections: outpatient treatment. Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium
 S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
Surgical Site Infections (SSIs)
") Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Doxycycline staph aureus
 Search Search Doxycycline staph aureus Mercer infection is the one of the colloquial terms given for MRSA (Methicillin-Resistant Staphylococcus Aureus ) infection. Initially, Staphylococcal resistance
Search Search Doxycycline staph aureus Mercer infection is the one of the colloquial terms given for MRSA (Methicillin-Resistant Staphylococcus Aureus ) infection. Initially, Staphylococcal resistance
Enterococcal PJI. Miquel Ekkelenkamp
 Enterococcal PJI Miquel Ekkelenkamp Enterococci: Gram-positive and round Formerly streptococci (but really quite different) Main clinical species : E. faecalis and E. faecium Mostly opportunistic pathogen
Enterococcal PJI Miquel Ekkelenkamp Enterococci: Gram-positive and round Formerly streptococci (but really quite different) Main clinical species : E. faecalis and E. faecium Mostly opportunistic pathogen
2017 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Antibiotic prophylaxis guideline for colorectal, hepatobiliary and vascular surgery for adult patients.
 Antibiotic prophylaxis guideline for colorectal, hepatobiliary and vascular surgery for adult patients. Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience,
Antibiotic prophylaxis guideline for colorectal, hepatobiliary and vascular surgery for adult patients. Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience,
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings?
 An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali. Lec 1
 Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING TOTAL HIP AND KNEE ARTHROPLASTY
 Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING TOTAL HIP AND KNEE ARTHROPLASTY FINAL Working Group: E. Henderson, M. John, I. Davis, S. Dunford,
Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING TOTAL HIP AND KNEE ARTHROPLASTY FINAL Working Group: E. Henderson, M. John, I. Davis, S. Dunford,
January 2014 Vol. 34 No. 1
 January 2014 Vol. 34 No. 1. and Minimum Inhibitory Concentration (MIC) Interpretive Standards for Testing Conditions Medium: diffusion: Mueller-Hinton agar (MHA) Broth dilution: cation-adjusted Mueller-Hinton
January 2014 Vol. 34 No. 1. and Minimum Inhibitory Concentration (MIC) Interpretive Standards for Testing Conditions Medium: diffusion: Mueller-Hinton agar (MHA) Broth dilution: cation-adjusted Mueller-Hinton
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
2012 ANTIBIOGRAM. Central Zone Former DTHR Sites. Department of Pathology and Laboratory Medicine
 2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Compliance of manufacturers of AST materials and devices with EUCAST guidelines
 Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
THERAPY OF ANAEROBIC INFECTIONS LUNG ABSCESS BRAIN ABSCESS
 THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
DOI: /zenodo
 www.imiamn.org.ua /journal.htm 38 UDC 616-008.87:616-002:616-089.843 MICROBIOLOGICAL PARAMETERS IN PATIENTS WITH INFLAMMATORY COMPLICATIONS AFTER KNEE AND HIP JOINTS ENDOPROSTHESIS REPLACEMENT AND THEIR
www.imiamn.org.ua /journal.htm 38 UDC 616-008.87:616-002:616-089.843 MICROBIOLOGICAL PARAMETERS IN PATIENTS WITH INFLAMMATORY COMPLICATIONS AFTER KNEE AND HIP JOINTS ENDOPROSTHESIS REPLACEMENT AND THEIR
Aminoglycosides. Spectrum includes many aerobic Gram-negative and some Gram-positive bacteria.
 Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Scottish Medicines Consortium
 Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Management of CRBSI Leilani Paitoonpong MD MSc Chusana Suankratay MD PhD Division of Infectious Diseases Chulalongkorn University
 Management of CRBSI Leilani Paitoonpong MD MSc Chusana Suankratay MD PhD Division of Infectious Diseases Chulalongkorn University A 60-year-old man was admitted for CABG surgery due to triple-vessel disease.
Management of CRBSI Leilani Paitoonpong MD MSc Chusana Suankratay MD PhD Division of Infectious Diseases Chulalongkorn University A 60-year-old man was admitted for CABG surgery due to triple-vessel disease.
Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma
 Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma Lucio Petrizzi DVM DECVS Università degli Studi di Teramo Surgical site infections (SSI) Microbial contamination unavoidable Infection
Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma Lucio Petrizzi DVM DECVS Università degli Studi di Teramo Surgical site infections (SSI) Microbial contamination unavoidable Infection
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
What s new in EUCAST methods?
 What s new in EUCAST methods? Derek Brown EUCAST Scientific Secretary Interactive question 1 MIC determination MH-F broth for broth microdilution testing of fastidious microorganisms Gradient MIC tests
What s new in EUCAST methods? Derek Brown EUCAST Scientific Secretary Interactive question 1 MIC determination MH-F broth for broth microdilution testing of fastidious microorganisms Gradient MIC tests
Bacterial Pathogens in Urinary Tract Infection and Antibiotic Susceptibility Pattern from a Teaching Hospital, Bengaluru, India
 ISSN: 2319-7706 Volume 4 Number 11 (2015) pp. 731-736 http://www.ijcmas.com Original Research Article Bacterial Pathogens in Urinary Tract Infection and Antibiotic Susceptibility Pattern from a Teaching
ISSN: 2319-7706 Volume 4 Number 11 (2015) pp. 731-736 http://www.ijcmas.com Original Research Article Bacterial Pathogens in Urinary Tract Infection and Antibiotic Susceptibility Pattern from a Teaching
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance
 Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Microbiology ( Bacteriology) sheet # 7
 sheet # 7") Microbiology ( Bacteriology) sheet # 7 Revision of last lecture : Each type of antimicrobial drug normally targets a specific structure or component of the bacterial cell eg:( cell wall, cell membrane,
Microbiology ( Bacteriology) sheet # 7 Revision of last lecture : Each type of antimicrobial drug normally targets a specific structure or component of the bacterial cell eg:( cell wall, cell membrane,
Reducing Infections in Surgical Practice. Fred A Sweet, MD Rockford Spine Center Illinois, USA
 Reducing Infections in Surgical Practice Fred A Sweet, MD Rockford Spine Center Illinois, USA Introduction: How bacteria get in The Host The Surgeon The Procedure The STAFF Skin PREP Prophylactic Antibiotics
Reducing Infections in Surgical Practice Fred A Sweet, MD Rockford Spine Center Illinois, USA Introduction: How bacteria get in The Host The Surgeon The Procedure The STAFF Skin PREP Prophylactic Antibiotics
2016 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,