Fever in returning travellers: clinical cases
|
|
|
- Everett Bennett
- 6 years ago
- Views:
Transcription

1 Fever in returning travellers: clinical cases Nick Beeching Senior Lecturer in Infectious Diseases Tropical & Infectious Disease Unit Royal Liverpool University Hospital Liverpool School of Tropical Medicine
2 Nil commercial Frequent traveller Declarations One of clinical coordinators of UK Imported Fever Service Member of GeoSentinel network Member of ESGITM Partially supported by NIHR HPRU grant in Emerging Infections & Zoonoses
3 Plan Focus on recently returned travellers Brief epidemiology Bedside approach Interactive cases Conclusions
4 1. Caribbean 2. Egypt Where is your next holiday? (choose one) 3. Mediterranean 4. South Asia 5. South America 6. Too dangerous to travel
5 1. Caribbean 2. Egypt Where is your next holiday? (choose one) 3. Mediterranean 4. South Asia 5. South America 6. Too dangerous to travel


6 Club ESCMID traveller
7 Club ESCMID traveller What has he caught?

8 Unde venis? 1963
9 Unde venis? Where have you come from? 1963
10 Clinical approach to fever History patient geography symptoms Signs Diagnosis Hospitalise/not Treatment Prevention
11 Clinical approach to fever Is it malaria? Is it dangerous? Is it new? Is it resistant? Is it reportable? Local & national public health ProMED, TropNet Europe, GeoSentinel Is it worth writing up?
12 Travel history Where travelled, exact location When travelled, exact dates Why What travelled, work / leisure specific exposures Which immunisations, malaria prophylaxis, anti-mosquito measures? compliance
13 English units centres 390/421 adult travel admissions infectious cause 93% UK domiciled 2918 bed days (21 ITU) Malaria (29% all cases) 20% bed days & 80% ITU stay Median length of stay 4 days W Africa 39/65 (59%) malaria OR 5.22 E Africa 44/72 (61%) malaria OR 5.82 S Asia 8/82 (10%) malaria OR 0.21 Harling R et al. J Infect 2004; 48:
 28% of 24,920")

14 GeoSentinel fever (n=6957) 28% of 24,920 travellers Wilson M et al. CID 2007;44:1560-8
15 GeoSentinel fever study n=6957 Fever Mal DEN No diag Resp Diarrh Oceania SS Africa SE Asia SC Asia N Asia N Africa All Figures are % of travellers returning from each region Wilson M et al. CID 2007;44:1560-8
16 Raw foods enterococci, trichinosis Untreated water, milk hepatitis, brucellosis, shigella Fresh water contact schistosomiasis, leptospirosis Sex HIV, syphilis, GC Insect bites malaria, arbovirus, rickettsiae trypanosomes Animals rabies, Q fever, brucellosis, People Exposure and infection plague VHF, hepatitis, meningococcal
17 Incubation period < 10 days Arbovirus including dengue Enteric bacterial Typhus (louse borne, flea borne) Plague Typhoid Haemorrhagic fevers
18 Fever and localizing signs Rash - dengue, typhoid, HIV, syphilis Jaundice Lymphadenopathy Hepatomegaly Splenomegaly Eschar Haemorrhage - malaria, hepatitis, leptospirosis - HIV, rickettsial infections - amoebic liver abscess, leptospirosis - malaria, typhoid, brucella - typhus, CCHF - VHF, rickettsial infection
19 Investigations Thick and thin films (antigen detection) Full blood count, biochemistry Blood cultures Save serum for serology Urine analysis and culture Stool microscopy and culture Chest X ray Scans only as indicated
20 Common sense Establish the presence of fever before investigation Retrospective investigation of fever that has settled is usually pointless Bryceson A 1988

21 Dr Nick BEECHING Liverpool School of Tropical Medicine 23 year old woman with fever and headache for 4 days in March 2007

22 Case year old woman Candolim & Dudhsagar falls with husband 4-18 Nov 2006 Bed & breakfast Both: Used DEET Full CQ/P prophylaxis She had few mosquito bites, he had many Fever end of March 2007
 AST 43 U/L (<40) Blood")
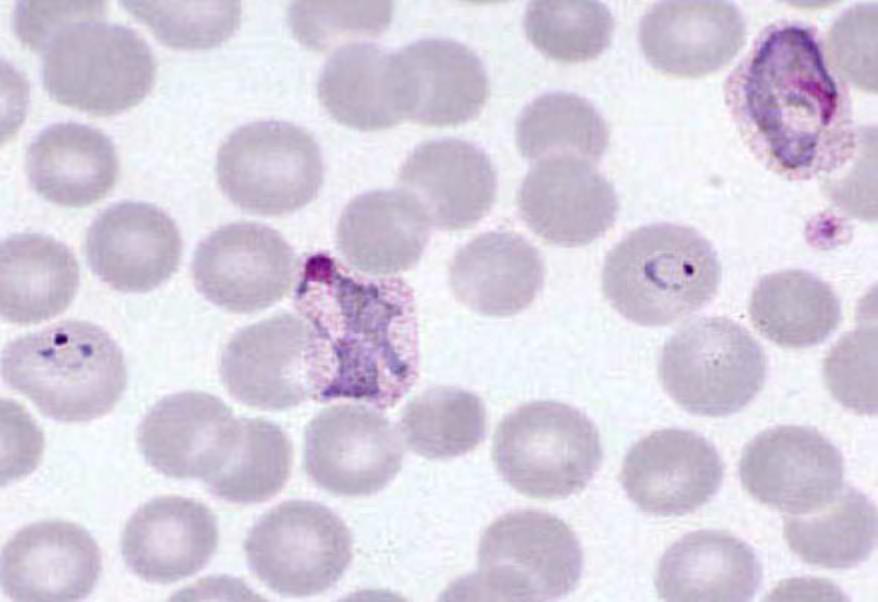
23 Progress Hospital after 4 days Temp 39.5 o C Nil else Hb 12.5 g/dl WBC 4.5 x 10 9 /L Platelets 105 x 10 9 /L Bilirubin 25 mmol/l (<18) AST 43 U/L (<40) Blood film shows:
24 What is the most likely 1. Dengue 2. Enteric fever 3. Falciparum malaria 4. Leptospirosis 5. Scrub typhus 6. Vivax malaria diagnosis?
25 What is the most likely 1. Dengue 2. Enteric fever 3. Falciparum malaria 4. Leptospirosis 5. Scrub typhus 6. Vivax malaria diagnosis?
26 GeoSentinel update travellers 53 units 23.3% fever SSA Pf malaria Rickettsial Latin Am/Carib DEN Pv malaria SEA DEN Pf malaria SCA Enteric DEN MENA HAV Pf malaria Brucella EUR HIV HAV N AM Cocci Rickettsial AUS/NZ/OC Pv malaria DEN Leder K et al. Ann Intern Med 2013; 158:456-68

27 What is the diagnosis? (choose one but vote in a minute) 1. Dengue 2. Falciparum malaria 3. Vivax malaria 4. Ovale malaria 5. Ehrlichiosis
28 1. Dengue What is the diagnosis? (choose one - vote now) 2. Falciparum malaria 3. Vivax malaria 4. Ovale malaria 5. Ehrlichiosis
29 1. Dengue What is the diagnosis? (choose one answer) 2. Falciparum malaria 3. Vivax malaria 4. Ovale malaria 5. Ehrlichiosis

30 Common in India Points in favour of vivax Long incubation period No complications Parasitology Scanty parasitaemia Younger, larger RBC Single chromatin Schüffner s dots Rest of film shows various stages & amoeboid forms
31
32 Progress Treated with chloroquine 1.5 g over 3 days Rapidly improved Glucose 6 phosphate dehydrogenase normal Primaquine considered Weight 65kg
33 What primaquine regimen would you use? (choose one) 1. 15mg per day for 2 weeks after CQ finished mg per day for 2 weeks at same time as CQ mg per day for 2 weeks after CQ finished mg per day for 2 weeks at same time as CQ 5. None
34 What primaquine regimen would you use? (choose one) 1. 15mg per day for 2 weeks after CQ finished mg per day for 2 weeks at same time as CQ mg per day for 2 weeks after CQ finished mg per day for 2 weeks at same time as CQ 5. None

35 Mueller I et al. Lancet Infect Dis 2009; 9:
36 Case year old husband Had been admitted to another hospital in late January (two weeks of symptoms) Quite ill with vivax malaria Treated with full dose chloroquine and primaquine 30mg/day for 14 days Readmitted May 2007 with confirmed vivax malaria (1 day of symptoms) Weight 92 kg
37 How would you treat him now? (choose one) 1. CQ 1.5 g and PQ 30 mg/day for 14 days 2. CQ 1.5 g and PQ 30 mg/day for 21 days 3. CQ 1.5 g and PQ 45 mg/day for 14 days 4. Malarone alone 5. Malarone plus PQ
38 How would you treat him now? (choose one) 1. CQ 1.5 g and PQ 30 mg/day for 14 days 2. CQ 1.5 g and PQ 30 mg/day for 21 days 3. CQ 1.5 g and PQ 45 mg/day for 14 days 4. Malarone alone 5. Malarone plus PQ

 www.")
39 Guidelines Immediate diagnosis & management of malaria in emergency room British Infection Society Advisory Committee on Malaria Prophylaxis (HPA)
40 Previously endemic Malaria in Goa Risk assessment last 10 years low risk for tourists so chemoprophylaxis not usually advised Heavy rains Oct 2006 Falciparum cases in European travellers especially from Candolim area north of capital Panaji Expect more cases of vivax Chemoprophylaxis now advised

41 Jelinek T et al. Euro Surveill Jan 2008;13(5):pii=8028
42 Lessons Epidemiology of infection continually changing Pretravel health advice needs to keep up with this Chemoprophylaxis does not always prevent malaria Especially vivax/ovale Use higher dose primaquine for vivax (and ovale?) Give primaquine with chloroquine (not after) Clinical chloroquine resistance not yet a major problem with vivax Lalloo DG et al. (UK guidelines) J Infect 2007; 54(2): Hill DR et al. Primaquine. Am J Trop Med 2006; 75(3): Griffith KS et al. (US guidelines) JAMA 2007; 297:
43 Dr Nick BEECHING Liverpool School of Tropical Medicine 50 year old woman with fever, rash and chest pain from Mauritius in March week holiday in Mauritius returned 4 days ago Injured leg and admitted to hospital on day 9 for antibiotics Many patients on ward with fever No mosquito bites remembered 4 days later fever and headache for 3 days Improved as flew back to UK Full immunisations, no malaria chemoprophylaxis

44 Now has 2 days of Fever to 39 o C Migratory joint pains Headache Photophobia Rash Pleuritic chest pain Temp 38.9 o C P100 BP 120/85 RR 12 Discrete rash on legs Chest clear No neck stiffness Joints normal
 Mono 0.2 (0.2-0.")
 Plt 270 x 10 9 /L (>150) ESR 12 mm/hr Malaria")
45 Investigations Hb 11.0 g/dl (>11.5) WBC 6.1 x 10 9 /L Lymph 0.6 (1.5-4) Mono 0.2 ( ) Neut 5.2 (2-7.5) Plt 270 x 10 9 /L (>150) ESR 12 mm/hr Malaria smears neg Liver function normal CXR normal
46 1. Dengue 2. Malaria What is your diagnosis? (choose one) 3. Meningococcal meningitis 4. O nyong-nyong 5. Something else
47 1. Dengue 2. Malaria What is your diagnosis? (choose one) 3. Meningococcal meningitis 4. O nyong-nyong 5. Something else
48 Initial diagnosis & progress Concern about meningococcal disease CT of head normal Given ceftriaxone No lumbar puncture Transferred to Liverpool Diagnosis presumed chikungunya Pulmonary embolus excluded by VQ scan Pialoux G et al. Lancet Inf Dis May 2007; 7:

49 Clinical features chikungunya Pialoux G et al. LID 2007; 7:

50 Oveall Suhrbier A et al. Arthritogenic alphaviruses--an overview Nat Rev Rheumatol 2012; 8: 420-9

51 Dengue Main differential diagnosis Dengue from Vietnam Jan 2008
52 Fever & exanthems: differences Hochedez P et al. Am J Trop Med Hyg 2008; 78(5): 710 3
53 Fever & exanthems: differences Hochedez P et al. Am J Trop Med Hyg 2008; 78(5): 710 3
54 Which of these is not a vector for chikungunya? (choose one) 1. Aedes aegypti 2. Aedes albopictus 3. Aedes vittatus 4. Anopheles gambiense 5. Culex annulorostris
55 Which of these is not a vector for chikungunya? (choose one) 1. Aedes aegypti 2. Aedes albopictus 3. Aedes vittatus 4. Anopheles gambiense 5. Culex annulorostris

56 Vectors Pialoux G et al. Lancet Inf Dis May 2007; 7:
57 How would you treat her? 1. Symptomatic treatment 2. Chloroquine 3. Interferon 4. Ribavirin 5. Aciclovir (choose one)
58 How would you treat her? 1. Symptomatic treatment 2. Chloroquine 3. Interferon 4. Ribavirin 5. Aciclovir (choose one)
59 Progress 6 weeks later Severe fatigue Mild joint pain Sore leg wound osteomyelitis excluded 3 months later Improving Compensated by travel health insurance Serology Positive IgM & IgG for Chikungunya

60 Tanzania 1953 Asia West Africa Réunion, Mauritius etc from M visitors in 2004 UK importations >130 in 2006 Epidemiology

61 France

62 11 Sep 2007
 Index case Foreigner arrived Italy June 21 2007 Travel history - Indian sub Continent Developed symptoms 2-3 days later Castiglione di Cervia,")
63 Chikungunya - Italy September cases reported (Ravenna Province) 1-95 yr old; 52% female; 36 laboratory confirmed 31 being investigated 11 cases required hospital admission (incl. 83yr old man multiple morbid chronic disease who died) Index case Foreigner arrived Italy June Travel history - Indian sub Continent Developed symptoms 2-3 days later Castiglione di Cervia, Ravenna Province C/o Graham Lloyd HPA Porton

64 CMI papers CMI 2013; 19: (series)

65 Suhrbier A et al. Nat Rev Rheumatol 2012; 8: 420-9
66 Where is the new epidemic occurring? 1. Brazil 2. Guadeloupe 3. Rwanda 4. South Carolina 5. Syria (choose one)
67 Where is the new epidemic occurring? 1. Brazil 2. Guadeloupe 3. Rwanda 4. South Carolina 5. Syria (choose one)

68 INVS Point Sanitaire No. 14, 7-13 Apr /version/61/file/pe_chikungunya_antilles_ pdf
69 Points Differential diagnosis of fever and rash from tropics is wide Case of probable nosocomial chikungunya infection As part of current large epidemic More severe and prolonged sequelae than dengue, especially joint disease Aedes vectors spreading and climate change may exacerbate this Pialoux G et al. Lancet Inf Dis 2007; 7: Suhrbier A et al. Nat Rev Rheumatol 2012; 8: 420-9
70
71 Dr Nick Beeching LSTM 42 year old British teacher with a sore leg after travel to South Africa Two week holiday with husband in South Africa Fully immunised Took Malarone Visited towns & game parks 4 days after return sees family doctor with painful groin
72 Complaint: Progress dullness in left thigh -exquisitely tender lump left groin GP diagnosis:?? Incarcerated hernia Referred to local hospital Surgeons agree: explore left groin enlarged lymph nodes Histology: marked non-specific hyperplasia with suppurative granulomas
73 What is your diagnosis? (choose one) 1. Glandular fever (EBV) 2. Toxoplasmosis 3. Plague 4. Cat scratch fever 5. Lymphadenopathy draining infected insect bite 6. Something else
74 What is your diagnosis? (choose one) 1. Glandular fever (EBV) 2. Toxoplasmosis 3. Plague 4. Cat scratch fever 5. Lymphadenopathy draining infected insect bite 6. Something else
75 Sent home Progress Feels increasingly unwell Headache Fever Lethargy and anorexia Sore throat (? post anaesthesia) Swollen painful left neck 2 days later (day 7 of illness) develops rash D8+ Referred to Liverpool

76 Examination Ambulant Looks unwell T 38.0ºC, BP 105/70 HR 80 Left neck node + Chest & throat clear Generalised rash
77 What is your diagnosis now? (choose one) 1. Tularaemia 2. Dengue 3. Crimean Congo haemorrhagic fever 4. Malarone allergy 5. Measles 6. Something else
78 What is your diagnosis now? (choose one) 1. Tularaemia 2. Dengue 3. Crimean Congo haemorrhagic fever 4. Malarone allergy 5. Measles 6. Something else


79 Further history Anaesthetist found lesion in hair Husband saw lesion under breast Patient found other lesions x 4
 Other biochem")
80 Hb 14.5, Plt 185 WBC 3.4, Neut 1.6, Lymph 1.5 ESR 35 CRP 21 ALT 100 U/L (<40) Other biochem normal Results
81 Diagnosis?

82 Outcome Clinical diagnosis African tick typhus Treated with doxycycline Better within 2 days Fully recovered Fame in women s magazine


83 Family Circle Aug 2006

84 Rickettsia africae in sport 8 th Raid Gauloise multi-sport event in rural Lesotho & Natal /331 French participants hospitalised 12 more symptomatic Fournier PE et al. Clin Infect Dis 1998; 27:
 Eschar 100% Adenopathy 100% Rash")
85 Features Tick bite noticed by 8/13 (61.5%) Eschar 100% Adenopathy 100% Rash 15%


86 Hers Eschar under bra strap Rash on legs
87 Tick bite fever Mediterranean Africa Rickettsia R conorii R africae Affects tourists Rare Common Fever Yes Yes Rash Common Less Eschar Single Multiple Regional nodes Yes Common Mortality ~2% Rare
88 Diagnosis & management History of tick exposure -?? Clinical - non specific symptoms Serology - only positive after 7-10 days Biochem/haem - non specific: acute phase, Hb, plt, WBC normal LFT, LDH, CK Culture - feasible, but not readily available Immunohistology/PCR of skin biopsy (rash, eschar) Treat on suspicion
89 Summary Consider African tick typhus in tourists with fever from Africa Symptoms non specific Headache often prominent Rash often absent Careful search for eschars eg hairline Lymph nodes Tick bites often not noticed Presumptive treatment with doxycycline Jensenius M et al. Clin Inf Dis 2004; 39:
90 Conclusions Travel history is essential Details of risk activity And preventive measures Examination Knowledge of epidemiology Simple tests Usually leads to diagnosis Epidemiology of pathogen resistance Guides empirical therapy
91

92

93 Travel Safe
Three patients with fever and rash after a stay in Morocco: infection with Rickettsia conorii
 Three patients with fever and rash after a stay in Morocco: infection with Rickettsia conorii Stylemans D 1, Mertens R 1, Seyler L 1, Piérard D 2, Lacor P 1 1. Department of Internal Medicine, UZ Brussel
Three patients with fever and rash after a stay in Morocco: infection with Rickettsia conorii Stylemans D 1, Mertens R 1, Seyler L 1, Piérard D 2, Lacor P 1 1. Department of Internal Medicine, UZ Brussel
Malaria & Dengue Global Health Lecture Series
 Malaria & Dengue Global Health Lecture Series Julie Gutman, MD MSc Pediatric Infectious Disease 5/13/2011 What would be the most appropriate treatment for a patient presenting with malaria acquired in
Malaria & Dengue Global Health Lecture Series Julie Gutman, MD MSc Pediatric Infectious Disease 5/13/2011 What would be the most appropriate treatment for a patient presenting with malaria acquired in
Outlines. Introduction Prevalence Resistance Clinical presentation Diagnosis Management Prevention Case presentation Achievements
 Amal Meas Al-Anizi, PharmD Candidate KSU, Infectious Disease Rotation 2014 Outlines Introduction Prevalence Resistance Clinical presentation Diagnosis Management Prevention Case presentation Achievements
Amal Meas Al-Anizi, PharmD Candidate KSU, Infectious Disease Rotation 2014 Outlines Introduction Prevalence Resistance Clinical presentation Diagnosis Management Prevention Case presentation Achievements
Clinical Manifestations and Treatment of Plague Dr. Jacky Chan. Associate Consultant Infectious Disease Centre, PMH
 Clinical Manifestations and Treatment of Plague Dr. Jacky Chan Associate Consultant Infectious Disease Centre, PMH Update of plague outbreak situation in Madagascar A large outbreak since 1 Aug 2017 As
Clinical Manifestations and Treatment of Plague Dr. Jacky Chan Associate Consultant Infectious Disease Centre, PMH Update of plague outbreak situation in Madagascar A large outbreak since 1 Aug 2017 As
Clinical manifestations of brucellosis and leptospirosis
 Clinical manifestations of brucellosis and leptospirosis Department of Internal Medicine Division of Infectious Diseases Medical University of Vienna Fever after sexual intercourse admissional status 25-year
Clinical manifestations of brucellosis and leptospirosis Department of Internal Medicine Division of Infectious Diseases Medical University of Vienna Fever after sexual intercourse admissional status 25-year
Beware the black spot BELINDA LIN ID/MICROBIOLOGY REGISTRAR BARWON HEALTH
 Beware the black spot BELINDA LIN ID/MICROBIOLOGY REGISTRAR BARWON HEALTH Mr MG, 61 Presents unwell 1 week following trekking the Kokoda Headache, arthralgias High fevers to 40 C, drenching sweats Delirium
Beware the black spot BELINDA LIN ID/MICROBIOLOGY REGISTRAR BARWON HEALTH Mr MG, 61 Presents unwell 1 week following trekking the Kokoda Headache, arthralgias High fevers to 40 C, drenching sweats Delirium
 Kraichat.tan@mahidol.ac.th 1 Outline Vector Borne Disease The linkage of CC&VBD VBD Climate Change and VBD Adaptation for risk minimization Adaptation Acknowledgement: data supported from WHO//www.who.org
Kraichat.tan@mahidol.ac.th 1 Outline Vector Borne Disease The linkage of CC&VBD VBD Climate Change and VBD Adaptation for risk minimization Adaptation Acknowledgement: data supported from WHO//www.who.org
Biology and Control of Insects and Rodents Workshop Vector Borne Diseases of Public Health Importance
 Vector-Borne Diseases of Public Health Importance Rudy Bueno, Jr., Ph.D. Director Components in the Disease Transmission Cycle Pathogen Agent that is responsible for disease Vector An arthropod that transmits
Vector-Borne Diseases of Public Health Importance Rudy Bueno, Jr., Ph.D. Director Components in the Disease Transmission Cycle Pathogen Agent that is responsible for disease Vector An arthropod that transmits
Mosquito Control Matters
 Mosquito Control Matters Community Presentation: FIGHT THE BITE Mosquitoes and West Nile Virus Prevention Luz Maria Robles Public Information Officer Sacramento Yolo Mosquito & Vector Control District
Mosquito Control Matters Community Presentation: FIGHT THE BITE Mosquitoes and West Nile Virus Prevention Luz Maria Robles Public Information Officer Sacramento Yolo Mosquito & Vector Control District
Medical Section, TIFR
 Overview It is nicknamed as Break-bone fever About 390 million dengue infections occur every year world- wide Dengue fever is caused by Aedes aegypti mosquitoes It gets under your skin and into your blood
Overview It is nicknamed as Break-bone fever About 390 million dengue infections occur every year world- wide Dengue fever is caused by Aedes aegypti mosquitoes It gets under your skin and into your blood
Welcome to Pathogen Group 9
 Welcome to Pathogen Group 9 Yersinia pestis Francisella tularensis Borrelia burgdorferi Rickettsia rickettsii Rickettsia prowazekii Acinetobacter baumannii Yersinia pestis: Plague gram negative oval bacillus,
Welcome to Pathogen Group 9 Yersinia pestis Francisella tularensis Borrelia burgdorferi Rickettsia rickettsii Rickettsia prowazekii Acinetobacter baumannii Yersinia pestis: Plague gram negative oval bacillus,
Subacute Adenitis. Ann M. Loeffler, MD
 Subacute Adenitis Ann M. Loeffler, MD Lymphadenitis Swelling and hyperplasia of sinusoidal lining cells Infiltration of leukocytes +/- abscess formation Granulomatous or non-granulomatous Pyogenic adenitis
Subacute Adenitis Ann M. Loeffler, MD Lymphadenitis Swelling and hyperplasia of sinusoidal lining cells Infiltration of leukocytes +/- abscess formation Granulomatous or non-granulomatous Pyogenic adenitis
Blood protozoan: Plasmodium
 Blood protozoan: Plasmodium The causative agent of including Plasmodium vivax P. falciparum P. malariae P. ovale. malaria in humans:four species are associated The Plasmodium spp. life cycle can be divided
Blood protozoan: Plasmodium The causative agent of including Plasmodium vivax P. falciparum P. malariae P. ovale. malaria in humans:four species are associated The Plasmodium spp. life cycle can be divided
Tularemia. Information for Health Care Providers. Physicians D Nurses D Laboratory Personnel D Infection Control Practitioners
 Tularemia Information for Health Care Providers Physicians D Nurses D Laboratory Personnel D Infection Control Practitioners Tularemia Caused by Francisella tularensis, a small, pleomorphic, gram-negative
Tularemia Information for Health Care Providers Physicians D Nurses D Laboratory Personnel D Infection Control Practitioners Tularemia Caused by Francisella tularensis, a small, pleomorphic, gram-negative
BIO Parasitology Spring 2009
 BIO 475 - Parasitology Spring 2009 Stephen M. Shuster Northern Arizona University http://www4.nau.edu/isopod Lecture 10 Malaria-Life Cycle a. Micro and macrogametocytes in mosquito stomach. b. Ookinete
BIO 475 - Parasitology Spring 2009 Stephen M. Shuster Northern Arizona University http://www4.nau.edu/isopod Lecture 10 Malaria-Life Cycle a. Micro and macrogametocytes in mosquito stomach. b. Ookinete
Dave D. Chadee. Novel dengue surveillance and control strategies developed at UWI, St Augustine, Trinidad
 Novel dengue surveillance and control strategies developed at UWI, St Augustine, Trinidad Dave D. Chadee Department of Life Sciences, Faculty of Science and Technology, University of the West Indies, St.
Novel dengue surveillance and control strategies developed at UWI, St Augustine, Trinidad Dave D. Chadee Department of Life Sciences, Faculty of Science and Technology, University of the West Indies, St.
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Coccidioidomycosis Nothing to disclose
 Coccidioidomycosis Nothing to disclose Disclosure Greg Melcher, M.D. Professor of Clinical Medicine Division of HIV, ID and Global Medicine Zuckerman San Francisco General Hospital University of California,
Coccidioidomycosis Nothing to disclose Disclosure Greg Melcher, M.D. Professor of Clinical Medicine Division of HIV, ID and Global Medicine Zuckerman San Francisco General Hospital University of California,
A:Malaria (Plasmodium species) Plasmodium falciparum causes malignant tertian malaria P. malariae: causes Quartan malaria P. vivax: causes benign
 Plasmodium falciparum causes malignant tertian malaria P. malariae: causes Quartan malaria P. vivax: causes benign") A:Malaria (Plasmodium species) Plasmodium falciparum causes malignant tertian malaria P. malariae: causes Quartan malaria P. vivax: causes benign tertian malaria P. ovale: causes benign tertian malaria
A:Malaria (Plasmodium species) Plasmodium falciparum causes malignant tertian malaria P. malariae: causes Quartan malaria P. vivax: causes benign tertian malaria P. ovale: causes benign tertian malaria
Top End Souvenirs: Infectious Diseases. Dr Anna Ralph
 Top End Souvenirs: Infectious Diseases Dr Anna Ralph Infectious Diseases Staff Specialist, Royal Darwin Hospital Clinical Researcher, Menzies School of Health Research Souvenir 1 Triage note says: 32 year
Top End Souvenirs: Infectious Diseases Dr Anna Ralph Infectious Diseases Staff Specialist, Royal Darwin Hospital Clinical Researcher, Menzies School of Health Research Souvenir 1 Triage note says: 32 year
Treatment of Dangerous Illnesses
 Treatment of Dangerous Illnesses Preventative Healthcare Workbook Name: Ó1995 Sommer Haven International Read section I on page 2 of the Training Pac Fill in the blanks 1. List five signs of dangerous
Treatment of Dangerous Illnesses Preventative Healthcare Workbook Name: Ó1995 Sommer Haven International Read section I on page 2 of the Training Pac Fill in the blanks 1. List five signs of dangerous
Australian and New Zealand College of Veterinary Scientists. Membership Examination. Medicine of Cats Paper 1
 Australian and New Zealand College of Veterinary Scientists Membership Examination June 2016 Medicine of Cats Paper 1 Perusal time: Fifteen (15) minutes Time allowed: Two (2) hours after perusal Answer
Australian and New Zealand College of Veterinary Scientists Membership Examination June 2016 Medicine of Cats Paper 1 Perusal time: Fifteen (15) minutes Time allowed: Two (2) hours after perusal Answer
Role of the general physician in the management of sepsis and antibiotic stewardship
 Role of the general physician in the management of sepsis and antibiotic stewardship Prof Martin Wiselka Dept of Infection and Tropical Medicine University Hospitals of Leicester Sepsis and antibiotic
Role of the general physician in the management of sepsis and antibiotic stewardship Prof Martin Wiselka Dept of Infection and Tropical Medicine University Hospitals of Leicester Sepsis and antibiotic
Natural Outbreaks and Bioterrorism: Giovanni Rezza Department of Infectious Diseases Istituto Superiore di Sanità
 Natural Outbreaks and Bioterrorism: Giovanni Rezza Department of Infectious Diseases Istituto Superiore di Sanità Chikungunya In Italy An unusual natural outbreak Chikungunya Castiglione di Ravenna Castiglione
Natural Outbreaks and Bioterrorism: Giovanni Rezza Department of Infectious Diseases Istituto Superiore di Sanità Chikungunya In Italy An unusual natural outbreak Chikungunya Castiglione di Ravenna Castiglione
Survey of Wisconsin Primary Care Clinicians
 ... for our health Clinical Approach to Nonresponsive Pneumonia: A Survey of Wisconsin Primary Care Clinicians Hannah A. Louks, 1,3 Jared M. Fixmer, MD 2, and Dennis J. Baumgardner, MD 1,2,3 1 Wisconsin
... for our health Clinical Approach to Nonresponsive Pneumonia: A Survey of Wisconsin Primary Care Clinicians Hannah A. Louks, 1,3 Jared M. Fixmer, MD 2, and Dennis J. Baumgardner, MD 1,2,3 1 Wisconsin
Zoonotic Diseases. Risks of working with wildlife. Maria Baron Palamar, Wildlife Veterinarian
 Zoonotic Diseases Risks of working with wildlife www.cdc.gov Definition Zoonoses: infectious diseases of vertebrate animals that can be naturally transmitted to humans Health vs. Disease Transmission -
Zoonotic Diseases Risks of working with wildlife www.cdc.gov Definition Zoonoses: infectious diseases of vertebrate animals that can be naturally transmitted to humans Health vs. Disease Transmission -
Diagnosis and management of zoonoses a tool for general practice
 clinical Praveena Gunaratnam Peter Massey Keith Eastwood David Durrhein Stephen Graves Diana Coote Louise Fisher Diagnosis and management of zoonoses a tool for general practice Background Zoonotic infections
clinical Praveena Gunaratnam Peter Massey Keith Eastwood David Durrhein Stephen Graves Diana Coote Louise Fisher Diagnosis and management of zoonoses a tool for general practice Background Zoonotic infections
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Blood protozoan: Plasmodium
 Blood protozoan: Plasmodium Dr. Hala Al Daghistani The causative agent of including Plasmodium vivax P. falciparum P. malariae P. ovale. malaria in humans: four species are associated The Plasmodium spp.
Blood protozoan: Plasmodium Dr. Hala Al Daghistani The causative agent of including Plasmodium vivax P. falciparum P. malariae P. ovale. malaria in humans: four species are associated The Plasmodium spp.
PLASMODIUM MODULE 39.1 INTRODUCTION OBJECTIVES 39.2 MALARIAL PARASITE. Notes
 Plasmodium MODULE 39 PLASMODIUM 39.1 INTRODUCTION Malaria is characterized by intermittent fever associated with chills and rigors in the patient. There may be enlargement of the liver and spleen in the
Plasmodium MODULE 39 PLASMODIUM 39.1 INTRODUCTION Malaria is characterized by intermittent fever associated with chills and rigors in the patient. There may be enlargement of the liver and spleen in the
Pan European maps of Vector Borne diseases
 Pan European maps of Vector Borne diseases Marieta Braks On behalf of WP4 2 Vbornet AGM 2012, Riga European Network for Arthropod Vector Surveillance for Human Public Health http://www.vbornet.eu/ Project
Pan European maps of Vector Borne diseases Marieta Braks On behalf of WP4 2 Vbornet AGM 2012, Riga European Network for Arthropod Vector Surveillance for Human Public Health http://www.vbornet.eu/ Project
Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy
 biopsy") Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy Dr. Fidelma Fitzpatrick Consultant Microbiologist, Co-chair, NCCP Prostate Bx Infection Project Board Fidelma.fitzpatrick@hse.ie
Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy Dr. Fidelma Fitzpatrick Consultant Microbiologist, Co-chair, NCCP Prostate Bx Infection Project Board Fidelma.fitzpatrick@hse.ie
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
BRUCELLOSIS. Morning report 7/11/05 Andy Bomback
 BRUCELLOSIS Morning report 7/11/05 Andy Bomback Also called undulant, Mediterranean, or Mata fever, brucellosis is an acute and chronic infection of the reticuloendothelial system gram negative facultative
BRUCELLOSIS Morning report 7/11/05 Andy Bomback Also called undulant, Mediterranean, or Mata fever, brucellosis is an acute and chronic infection of the reticuloendothelial system gram negative facultative
Medical Bacteriology- Lecture 14. Gram negative coccobacilli. Zoonosis. Brucella. Yersinia. Francesiella
 Medical Bacteriology- Lecture 14 Gram negative coccobacilli Zoonosis Brucella Yersinia Francesiella 1 Zoonosis: A disease, primarily of animals, which is transmitted to humans as a result of direct or
Medical Bacteriology- Lecture 14 Gram negative coccobacilli Zoonosis Brucella Yersinia Francesiella 1 Zoonosis: A disease, primarily of animals, which is transmitted to humans as a result of direct or
Medical and Veterinary Entomology
 Medical and Veterinary Entomology An eastern treehole mosquito, Aedes triseriatus, takes a blood meal. Urbana, Illinois, USA Alexander Wild Photography Problems associated with arthropods 1) Psychological
Medical and Veterinary Entomology An eastern treehole mosquito, Aedes triseriatus, takes a blood meal. Urbana, Illinois, USA Alexander Wild Photography Problems associated with arthropods 1) Psychological
Symptoms of cellulitis (n=396) %
 %") Cellulitis and lymphoedema Vaughan Keeley May 2012 What is cellulitis? - also called erysipelas, acute inflammatory episodes etc. - bacterial infection of skin + subcutaneous tissues - more common in people
Cellulitis and lymphoedema Vaughan Keeley May 2012 What is cellulitis? - also called erysipelas, acute inflammatory episodes etc. - bacterial infection of skin + subcutaneous tissues - more common in people
Feline zoonoses. Institutional Animal Care and Use Committee 12/09
 Feline zoonoses Institutional Animal Care and Use Committee 12/09 Cat scratch disease Bacterial infection caused by Bartonella henselae Associated with a cat bite or scratch Infection at point of injury,
Feline zoonoses Institutional Animal Care and Use Committee 12/09 Cat scratch disease Bacterial infection caused by Bartonella henselae Associated with a cat bite or scratch Infection at point of injury,
Guidelines for Antimicrobial treatment for treatment of confirmed infections adults
 Guidelines for Antimicrobial treatment for treatment of confirmed infections adults This guideline gives recommendations for treatment of confirmed infections in adults for children please see the Paediatric
Guidelines for Antimicrobial treatment for treatment of confirmed infections adults This guideline gives recommendations for treatment of confirmed infections in adults for children please see the Paediatric
Mosquitoes & Diseases. Maxwell Lea, Jr. DVM State Veterinarian Louisiana Dept. of Agriculture and Forestry Department of Animal Health Services
 Mosquitoes & Diseases Maxwell Lea, Jr. DVM State Veterinarian Louisiana Dept. of Agriculture and Forestry Department of Animal Health Services Canine Heartworm Disease Eastern Equine Encephalomyelitis
Mosquitoes & Diseases Maxwell Lea, Jr. DVM State Veterinarian Louisiana Dept. of Agriculture and Forestry Department of Animal Health Services Canine Heartworm Disease Eastern Equine Encephalomyelitis
BRUCELLOSIS BRUCELLOSIS. CPMP/4048/01, rev. 3 1/7 EMEA 2002
 BRUCELLOSIS CPMP/4048/01, rev. 3 1/7 General points on treatment Four species are pathogenic to man: B. melitenis (acquired from goats), B. suis (pigs), B. abortus (cattle) and B. canis (dogs). The bacteria
BRUCELLOSIS CPMP/4048/01, rev. 3 1/7 General points on treatment Four species are pathogenic to man: B. melitenis (acquired from goats), B. suis (pigs), B. abortus (cattle) and B. canis (dogs). The bacteria
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Their Biology and Ecology. Jeannine Dorothy, Entomologist Maryland Department of Agriculture, Mosquito Control Section
 Their Biology and Ecology Jeannine Dorothy, Entomologist Maryland Department of Agriculture, Mosquito Control Section Mosquito Biology 60+ species in Maryland in 10 genera 14 or more can vector disease
Their Biology and Ecology Jeannine Dorothy, Entomologist Maryland Department of Agriculture, Mosquito Control Section Mosquito Biology 60+ species in Maryland in 10 genera 14 or more can vector disease
What s Your Diagnosis? By Sohaila Jafarian, Class of 2018
 Signalment: Greeley, 3 yo MC DSH Presenting Complaint: ADR History: What s Your Diagnosis? By Sohaila Jafarian, Class of 2018 Patient is an indoor/outdoor cat. Previously healthy and up to date on vaccines
Signalment: Greeley, 3 yo MC DSH Presenting Complaint: ADR History: What s Your Diagnosis? By Sohaila Jafarian, Class of 2018 Patient is an indoor/outdoor cat. Previously healthy and up to date on vaccines
Saturday Clinics. Every Saturday morning we hold an open clinic for the local community.
 Saturday Clinics Every Saturday morning we hold an open clinic for the local community. We see a variety of animals ranging from livestock, dogs, cats and even rabbits and monkeys! The majority of our
Saturday Clinics Every Saturday morning we hold an open clinic for the local community. We see a variety of animals ranging from livestock, dogs, cats and even rabbits and monkeys! The majority of our
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Vector Control in emergencies
 OBJECTIVE Kenya WASH Cluster Training for Emergencies Oct 2008 3.06 - Vector Control in emergencies To provide practical guidance and an overview of vector control in emergency situations It will introduce
OBJECTIVE Kenya WASH Cluster Training for Emergencies Oct 2008 3.06 - Vector Control in emergencies To provide practical guidance and an overview of vector control in emergency situations It will introduce
Tick-borne Disease Testing in Shelters What Does that Blue Dot Really Mean?
 Tick-borne Disease Testing in Shelters What Does that Blue Dot Really Mean? 2017 ASPCA. All Rights Reserved. Your Presenter Stephanie Janeczko, DVM, MS, DABVP, CAWA Senior Director of Shelter Medical Programs
Tick-borne Disease Testing in Shelters What Does that Blue Dot Really Mean? 2017 ASPCA. All Rights Reserved. Your Presenter Stephanie Janeczko, DVM, MS, DABVP, CAWA Senior Director of Shelter Medical Programs
Breastfeeding Challenges - Mastitis & Breast Abscess -
 CLINICAL PRACTICE GUIDELINE Breastfeeding Challenges - Mastitis & Breast Abscess - SCOPE (Area): Maternity Unit, Emergency Department, Paediatrics SCOPE (Staff): Medical, Midwifery & Nursing DESIRED OUTCOME/OBJECTIVE
CLINICAL PRACTICE GUIDELINE Breastfeeding Challenges - Mastitis & Breast Abscess - SCOPE (Area): Maternity Unit, Emergency Department, Paediatrics SCOPE (Staff): Medical, Midwifery & Nursing DESIRED OUTCOME/OBJECTIVE
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance
 Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Pathogenesis of E. canis
 Tick-born disease Rhipicephalus sanguineus brown dog tick Rickettsia Ehrlichia canis Ehrlichia platys Anaplasma platys Pathogenesis of E. canis Incubation period: 8 20 days Mononuclear cells Liver, spleen,
Tick-born disease Rhipicephalus sanguineus brown dog tick Rickettsia Ehrlichia canis Ehrlichia platys Anaplasma platys Pathogenesis of E. canis Incubation period: 8 20 days Mononuclear cells Liver, spleen,
2. What you need to know before you take Doxycycline capsule
 PACKAGE LEAFLET: INFORMATION FOR THE USER Doxycycline 100 mg capsules Doxycycline (as hyclate) Read all of this leaflet carefully before you start taking this medicine because it contains important information
PACKAGE LEAFLET: INFORMATION FOR THE USER Doxycycline 100 mg capsules Doxycycline (as hyclate) Read all of this leaflet carefully before you start taking this medicine because it contains important information
Taking your pets abroad
 Taking your pets abroad Your guide to diseases encountered abroad Produced by the BVA Animal Welfare Foundation www.bva-awf.org.uk BVA AWF is a registered charity (287118) Prevention is better than cure!
Taking your pets abroad Your guide to diseases encountered abroad Produced by the BVA Animal Welfare Foundation www.bva-awf.org.uk BVA AWF is a registered charity (287118) Prevention is better than cure!
Adopting a dog from Spain comes with some risks of which you should be aware.
 LHB Galgo Rescue Information for your Vet Adopting a dog from Spain comes with some risks of which you should be aware. Nearly all Spanish shelters test for Babesia, Ehrlichia, Leishmania and heartworm
LHB Galgo Rescue Information for your Vet Adopting a dog from Spain comes with some risks of which you should be aware. Nearly all Spanish shelters test for Babesia, Ehrlichia, Leishmania and heartworm
Chikungunya. A mosquito-borne disease
 A mosquito-borne disease Chikungunya is a disease caused by a virus transmitted by mosquitoes It is also called contorted fever and that which bends up The virus is called Chikungunya Virus The virus is
A mosquito-borne disease Chikungunya is a disease caused by a virus transmitted by mosquitoes It is also called contorted fever and that which bends up The virus is called Chikungunya Virus The virus is
Some of your patients have Valley Fever: Do you know which ones?
 Some of your patients have : Do you know which ones? ACP-Az Meeting, Nov 13, 2015 John N Galgiani MD University of Arizona Problem in Arizona Alone Total Infections Seek Medical Attention Diagnosed/Reported
Some of your patients have : Do you know which ones? ACP-Az Meeting, Nov 13, 2015 John N Galgiani MD University of Arizona Problem in Arizona Alone Total Infections Seek Medical Attention Diagnosed/Reported
Introduction- Rickettsia felis
 Cat flea-borne spotted fever in humans is the dog to blame? Rebecca J Traub Assoc. Prof. in Parasitology Faculty of Veterinary and Agricultural Sciences Introduction- Rickettsia felis Emerging zoonoses
Cat flea-borne spotted fever in humans is the dog to blame? Rebecca J Traub Assoc. Prof. in Parasitology Faculty of Veterinary and Agricultural Sciences Introduction- Rickettsia felis Emerging zoonoses
Brucellosis in Kyrgyzstan
 Centers for Disease Control and Prevention Case Studies in Applied Epidemiology No. 053-D11 Brucellosis in Kyrgyzstan Participant's Guide Learning Objectives After completing this case study, the participant
Centers for Disease Control and Prevention Case Studies in Applied Epidemiology No. 053-D11 Brucellosis in Kyrgyzstan Participant's Guide Learning Objectives After completing this case study, the participant
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
Tick-Borne Infections Council
 Tick-Borne Infections Council of North Carolina, Inc. 919-215-5418 The Tick-Borne Infections Council of North Carolina, Inc. (TIC-NC), a 501(c)(3) non-profit organization, was formed in 2005 to help educate
Tick-Borne Infections Council of North Carolina, Inc. 919-215-5418 The Tick-Borne Infections Council of North Carolina, Inc. (TIC-NC), a 501(c)(3) non-profit organization, was formed in 2005 to help educate
Infection Comments First Line Agents Penicillin Allergy History of multiresistant. line treatment: persist for >7 days they may be
 Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
Medical Conditions Questionnaire
 Medical Conditions Questionnaire (to be completed by the member) Member Full Name.Date of birth. Policy number or scheme name. Please complete the appropriate section(s) only after completing the Member
Medical Conditions Questionnaire (to be completed by the member) Member Full Name.Date of birth. Policy number or scheme name. Please complete the appropriate section(s) only after completing the Member
With Proper Prevention and Cure Victory over Malaria is Sure! Flipbook on Malaria Prevention and control
 With Proper Prevention and Cure Victory over Malaria is Sure! Flipbook on Malaria Prevention and control Malaria Malaria is a public health problem in several parts of the country. About 80% cases of
With Proper Prevention and Cure Victory over Malaria is Sure! Flipbook on Malaria Prevention and control Malaria Malaria is a public health problem in several parts of the country. About 80% cases of
Urbani School Health Kit. A Dengue-Free Me. Urbani School Health Kit TEACHER'S RESOURCE BOOK
 Urbani School Health Kit TEACHER'S RESOURCE BOOK A Dengue-Free Me A Campaign on the Prevention and Control of Dengue for Health Promoting Schools Urbani School Health Kit World Health Organization Western
Urbani School Health Kit TEACHER'S RESOURCE BOOK A Dengue-Free Me A Campaign on the Prevention and Control of Dengue for Health Promoting Schools Urbani School Health Kit World Health Organization Western
h e a l t h l i n e ISSN X Volume 1 Issue 1 July-December 2010 Pages 16-20
 h e a l t h l i n e ISSN 2229-337X Volume 1 Issue 1 July-December 2010 Pages 16-20 Original Article Awareness and practice about preventive method against mosquito bite in Gujarat Niraj Pandit 1, Yogesh
h e a l t h l i n e ISSN 2229-337X Volume 1 Issue 1 July-December 2010 Pages 16-20 Original Article Awareness and practice about preventive method against mosquito bite in Gujarat Niraj Pandit 1, Yogesh
Zoonoses - Current & Emerging Issues
 Zoonoses - Current & Emerging Issues HUMAN HEALTH & MEDICINE VETERINARY HEALTH & MEDICINE Martin Shakespeare RD MRPharmS MCGI Scope Zoonotic Disease What is it? Why is it significant? Current Issues &
Zoonoses - Current & Emerging Issues HUMAN HEALTH & MEDICINE VETERINARY HEALTH & MEDICINE Martin Shakespeare RD MRPharmS MCGI Scope Zoonotic Disease What is it? Why is it significant? Current Issues &
 Page 1 of 5 Medical Summary OTHER TICK-BORNE DISEASES This article covers babesiosis, anaplasmosis, and ehrlichiosis. See Rickettsial Infections (tick-borne rickettsia), Lyme Disease, and Tick-Borne Encephalitis
Page 1 of 5 Medical Summary OTHER TICK-BORNE DISEASES This article covers babesiosis, anaplasmosis, and ehrlichiosis. See Rickettsial Infections (tick-borne rickettsia), Lyme Disease, and Tick-Borne Encephalitis
Community Acquired Pneumonia (CAP)
") Community Acquired Pneumonia (CAP) The following guidelines have been developed to aid clinicians in the investigation and management of patients with CAP at the Royal Liverpool University Hospital (RLUH).
Community Acquired Pneumonia (CAP) The following guidelines have been developed to aid clinicians in the investigation and management of patients with CAP at the Royal Liverpool University Hospital (RLUH).
AUSTRALIAN AND NEW ZEALAND COLLEGE OF VETERINARY SCIENTISTS. Sample Exam Questions. Veterinary Practice (Small Animal)
") AUSTRALIAN AND NEW ZEALAND COLLEGE OF VETERINARY SCIENTISTS Sample Exam Questions Veterinary Practice (Small Animal) Written Examination (Component 1) Written Paper 1 (two hours): Principles of Veterinary
AUSTRALIAN AND NEW ZEALAND COLLEGE OF VETERINARY SCIENTISTS Sample Exam Questions Veterinary Practice (Small Animal) Written Examination (Component 1) Written Paper 1 (two hours): Principles of Veterinary
Ticks and tick-borne diseases
 Occupational Diseases Ticks and tick-borne diseases Ticks Ticks are small, blood sucking arthropods related to spiders, mites and scorpions. Ticks are only about one to two millimetres long before they
Occupational Diseases Ticks and tick-borne diseases Ticks Ticks are small, blood sucking arthropods related to spiders, mites and scorpions. Ticks are only about one to two millimetres long before they
The Invasive Mosquito Project
 The Invasive Mosquito Project Master of Public Health Capstone Project and Field Experience Presentation Ashley Thackrah Trotter Hall 104C Kansas State University November 19, 2015 8:30 a.m. My Bio B.S.
The Invasive Mosquito Project Master of Public Health Capstone Project and Field Experience Presentation Ashley Thackrah Trotter Hall 104C Kansas State University November 19, 2015 8:30 a.m. My Bio B.S.
Update on Fluoroquinolones. Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO
 Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings. Carlos Reyes Sacin, MD, AAHIVS
 Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Delayed Prescribing for Minor Infections Resource Pack for Prescribers
 Delayed Prescribing for Minor Infections Resource Pack for Prescribers Background: Antibiotic resistance is an alarming threat to modern healthcare, and infectious illness remains a major global threat
Delayed Prescribing for Minor Infections Resource Pack for Prescribers Background: Antibiotic resistance is an alarming threat to modern healthcare, and infectious illness remains a major global threat
DENGUE: Dengue is caused by the bite of an infected Aedes aegypti
 DENGUE: Dengue is caused by the bite of an infected Aedes aegypti mosquito. Aedes is a day biter i.e. it bites during the day time. These mosquitoes usually breed in clean water collections in containers,
DENGUE: Dengue is caused by the bite of an infected Aedes aegypti mosquito. Aedes is a day biter i.e. it bites during the day time. These mosquitoes usually breed in clean water collections in containers,
Canine Anaplasmosis Anaplasma phagocytophilum Anaplasma platys
 Canine Anaplasmosis Anaplasma phagocytophilum Anaplasma platys It takes just hours for an infected tick to transmit Anaplasma organisms to a dog. What is canine anaplasmosis? Canine anaplasmosis is a disease
Canine Anaplasmosis Anaplasma phagocytophilum Anaplasma platys It takes just hours for an infected tick to transmit Anaplasma organisms to a dog. What is canine anaplasmosis? Canine anaplasmosis is a disease
GP Small Group education April/May 2015 Antibiotics Resistance is futile
 GP Small Group education April/May 2015 Antibiotics Resistance is futile Acknowledgements This material was prepared by the Clinical Quality and Education team with help gratefully received from: Topic
GP Small Group education April/May 2015 Antibiotics Resistance is futile Acknowledgements This material was prepared by the Clinical Quality and Education team with help gratefully received from: Topic
Package leaflet: Information for the patient. FLUCLOXACILLIN 250MG/5ML ORAL SOLUTION Flucloxacillin
 Package leaflet: Information for the patient FLUCLOXACILLIN 250MG/5ML ORAL SOLUTION Flucloxacillin Read all of this leaflet carefully before you start taking this medicine because it contains important
Package leaflet: Information for the patient FLUCLOXACILLIN 250MG/5ML ORAL SOLUTION Flucloxacillin Read all of this leaflet carefully before you start taking this medicine because it contains important
Prepared: August Review: July Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide.
 Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
Life Cycle of Malaria for Primary Schools
 Life Cycle of Malaria for Primary Schools This lesson provides the teacher with material to teach the life cycle of malaria in a basic way. It may therefore be appropriate for primary school classes, or
Life Cycle of Malaria for Primary Schools This lesson provides the teacher with material to teach the life cycle of malaria in a basic way. It may therefore be appropriate for primary school classes, or
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT
 INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
Situation update of dengue in the SEA Region, 2010
 Situation update of dengue in the SEA Region, 21 The global situation of Dengue It is estimated that nearly 5 million dengue infections occur annually in the world. Although dengue has a global distribution,
Situation update of dengue in the SEA Region, 21 The global situation of Dengue It is estimated that nearly 5 million dengue infections occur annually in the world. Although dengue has a global distribution,
Early warning for Lyme disease: Lessons learned from Canada
 Early warning for Lyme disease: Lessons learned from Canada Nick Hume Ogden, National Microbiology Laboratory @ Saint-Hyacinthe Talk outline The biology of Lyme disease emergence in the context of climate
Early warning for Lyme disease: Lessons learned from Canada Nick Hume Ogden, National Microbiology Laboratory @ Saint-Hyacinthe Talk outline The biology of Lyme disease emergence in the context of climate
B09 Breast Uplift. Will my bra size change? Your bra size will not usually change. However, your cup size and shape of bra you need may be different.
 B09 Breast Uplift What is a breast uplift? A breast uplift (mastoplexy) is a cosmetic operation to remove excess skin from your breasts to improve their shape. Your surgeon will assess you and let you
B09 Breast Uplift What is a breast uplift? A breast uplift (mastoplexy) is a cosmetic operation to remove excess skin from your breasts to improve their shape. Your surgeon will assess you and let you
Australian and New Zealand College of Veterinary Scientists. Membership Examination. Veterinary Emergency and Critical Care Paper 1
 Australian and New Zealand College of Veterinary Scientists Membership Examination June 2014 Veterinary Emergency and Critical Care Paper 1 Perusal time: Fifteen (15) minutes Time allowed: Two (2) hours
Australian and New Zealand College of Veterinary Scientists Membership Examination June 2014 Veterinary Emergency and Critical Care Paper 1 Perusal time: Fifteen (15) minutes Time allowed: Two (2) hours
Economic Impact of Dengue in LAC and the World
 Economic Impact of Dengue in LAC and the World Matheus Takatu Barros Donald S. Shepard, PhD Heller School for Social Policy and Management Brandeis University, Waltham, MA USA mtakatu@brandeis.edu shepard@brandeis.edu
Economic Impact of Dengue in LAC and the World Matheus Takatu Barros Donald S. Shepard, PhD Heller School for Social Policy and Management Brandeis University, Waltham, MA USA mtakatu@brandeis.edu shepard@brandeis.edu
Allergy patient with organism. Mike Cooper Consultant Microbiologist New Cross Hospital, Wolverhampton
 Allergy patient with organism Mike Cooper Consultant Microbiologist New Cross Hospital, Wolverhampton 60 year old male Referred to hospital by GP?IE 3/52 history of feeling generally unwell with malaise,
Allergy patient with organism Mike Cooper Consultant Microbiologist New Cross Hospital, Wolverhampton 60 year old male Referred to hospital by GP?IE 3/52 history of feeling generally unwell with malaise,
Knowledge Aptitude and Perspective Study Regarding Awareness of Dengue Fever among 4th Year Students of Nishtar Medical College, Multan-Pakistan
 Knowledge Aptitude and Perspective Study Regarding Awareness of Dengue Fever among 4th Year Students of Nishtar Medical College, Multan-Pakistan Dr. Sana Ahmad Khan Dr. Hajrah Ahsan Dr. Talha Kareem Post
Knowledge Aptitude and Perspective Study Regarding Awareness of Dengue Fever among 4th Year Students of Nishtar Medical College, Multan-Pakistan Dr. Sana Ahmad Khan Dr. Hajrah Ahsan Dr. Talha Kareem Post
Dr Steve Holden Consultant Microbiologist Nottingham University Hospitals NHS Trust
 Dr Steve Holden Consultant Microbiologist Nottingham University Hospitals NHS Trust Clinical Case 38 yrold man Renal replacement (CAPD) since 2011 Unexplained ESRF Visited Pakistan for 3 months end of
Dr Steve Holden Consultant Microbiologist Nottingham University Hospitals NHS Trust Clinical Case 38 yrold man Renal replacement (CAPD) since 2011 Unexplained ESRF Visited Pakistan for 3 months end of
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT DRAFT AS CURRENTLY OUT FOR CONSULTATION BUT CAN BE UTILISED IN PRESENT FORMAT Name & Title Of Author: Date Revised: Approved by Committee/Group:
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT DRAFT AS CURRENTLY OUT FOR CONSULTATION BUT CAN BE UTILISED IN PRESENT FORMAT Name & Title Of Author: Date Revised: Approved by Committee/Group:
Drug therapy of Filariasis. Dr. Shareef sm Asst. professor pharmacology
 Drug therapy of Filariasis Dr. Shareef sm Asst. professor pharmacology Signs and symptoms Lymphatic filariasis Fever Inguinal or axillary lymphadenopathy Testicular and/or inguinal pain Skin exfoliation
Drug therapy of Filariasis Dr. Shareef sm Asst. professor pharmacology Signs and symptoms Lymphatic filariasis Fever Inguinal or axillary lymphadenopathy Testicular and/or inguinal pain Skin exfoliation
PACKAGE LEAFLET: INFORMATION FOR THE USER. AMOXICILLIN 250mg and 500mg CAPSULES BP Amoxicillin (as amoxicillin trihydrate)
") PACKAGE LEAFLET: INFORMATION FOR THE USER AMOXICILLIN 250mg and 500mg CAPSULES BP Amoxicillin (as amoxicillin trihydrate) Read all of this leaflet carefully before you start taking this medicine because
PACKAGE LEAFLET: INFORMATION FOR THE USER AMOXICILLIN 250mg and 500mg CAPSULES BP Amoxicillin (as amoxicillin trihydrate) Read all of this leaflet carefully before you start taking this medicine because
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus
 Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
TANZANIA March 2016 Arrival at Kilimanjaro International Airport (JRO) 1. Day: Sunday Transfer to the Karama Lodge, Arusha (30 km)
 1. Day: Sunday Transfer to the Karama Lodge, Arusha (30 km)") TANZANIA 2016 13 March 2016 Arrival at Kilimanjaro International Airport (JRO) 1. Day: Sunday Transfer to the Karama Lodge, Arusha (30 km) 23.00 Briefing of the medical program (Dr. Schaefer) Meeting point:
TANZANIA 2016 13 March 2016 Arrival at Kilimanjaro International Airport (JRO) 1. Day: Sunday Transfer to the Karama Lodge, Arusha (30 km) 23.00 Briefing of the medical program (Dr. Schaefer) Meeting point:
sanguineus, in a population of
 BVA Student Travel Grant Final Report Prevalence of the Brown Dog tick, Rhipicephalus sanguineus, in a population of dogs in Zanzibar, and its role as a vector of canine tickborne disease. Bethan Warner
BVA Student Travel Grant Final Report Prevalence of the Brown Dog tick, Rhipicephalus sanguineus, in a population of dogs in Zanzibar, and its role as a vector of canine tickborne disease. Bethan Warner
Malaria. This sheet is from both sections recording and includes all slides and diagrams.
 Malaria This sheet is from both sections recording and includes all slides and diagrams. Malaria is caused by protozoa family called plasmodium (Genus) mainly affect blood system specially RBCs and each
Malaria This sheet is from both sections recording and includes all slides and diagrams. Malaria is caused by protozoa family called plasmodium (Genus) mainly affect blood system specially RBCs and each
Volume 2; Number 16 October 2008
 Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Traveling (resistant) bacteria
 bacteria") Traveling resistant bacteria Erika Vlieghe Institute of Tropical Medicine, Antwerp University Hospital Antwerp Traveling (resistant) bacteria Colonisation - carriership rectal flora, skin Infection: mild-moderate
Traveling resistant bacteria Erika Vlieghe Institute of Tropical Medicine, Antwerp University Hospital Antwerp Traveling (resistant) bacteria Colonisation - carriership rectal flora, skin Infection: mild-moderate
FOLLOWING BUNDLE ADMINISTERED WITHIN ONE HOUR.
 Patient label DATE and TIME: 1 REVIEW BY Emergency Department SENIOR REGISTRAR (ED BLEEP 5999) +/-Leave Proforma 2 FOLLOWING BUNDLE ADMINISTERED WITHIN ONE HOUR. Bloods for FBC, U+E, CRP, LFT s, Clotting
Patient label DATE and TIME: 1 REVIEW BY Emergency Department SENIOR REGISTRAR (ED BLEEP 5999) +/-Leave Proforma 2 FOLLOWING BUNDLE ADMINISTERED WITHIN ONE HOUR. Bloods for FBC, U+E, CRP, LFT s, Clotting
Cracking open or keeping a lid on? The Pandora s Box of human infectious disease risks associated with (intact) forests
 forests") Cracking open or keeping a lid on? The Pandora s Box of human infectious disease risks associated with (intact) forests Kris Murray kris.murray@imperial.ac.uk @earthfluenza Hiral Shah Arran Hamlet Elizabeth
Cracking open or keeping a lid on? The Pandora s Box of human infectious disease risks associated with (intact) forests Kris Murray kris.murray@imperial.ac.uk @earthfluenza Hiral Shah Arran Hamlet Elizabeth