DM seminar. Pulmonary diseases due to NTM & their management
|
|
|
- May Green
- 6 years ago
- Views:
Transcription
1 DM seminar Pulmonary diseases due to NTM & their management
2 Content 1. Introduction 2. Microbiology 3. Epidemiology 4. Diseases 5. Diagnosis 6. Treatment 7. Individual species
3 Introduction Genus Mycobacterium Mycolic acid containing genera Aerobic, non-spore forming, non motile Gram positive Rods Discovered for the first time in 1882 by Robert Koch More than 200 species NTM classification given by Runyon in 1959 Mycobacterium: General Characteristics, Laboratory Detection, and Staining Procedures. In: Manual of Clinical Microbiology. Canada: ASM, pp
4 Also known as Atypical Mycobacteria Mycobacteria other than Tuberculosis (MOTT) Potentially pathogenic environmental mycobacteria (PPEM) Anonymous Mycobacteria Non Tuberculous Mycobacteria The International Working Group on Mycobacterial Taxonomy
5 History 1868 Tuberculosis first described in Chicken 1890 Recognized in lab to be distinct from M. tuberculosis Identified as M. Avium 1943 First case of MAC lung disease 1950 Pulmonary disease due to NTM established
6 Mycobacterium Classification Mycobacterium tuberculosis complex Mycobacterium leprae Nontubercular Mycobacterium Slowly Growing Mycobacterium Rapidly Growing Mycobacterium Pigmented Mycobacterium Non Pigmented Mycobacterium Mycobacterium Tuberculosis. In: Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. New york: Elsevier, pp Scotochromogens Photochromogens Mycobacterium Avium Complex Non MAC
7 Content 1. Introduction 2. Microbiology 3. Epidemiology 4. Diseases 5. Diagnosis 6. Treatment 7. Individual species
8 Microbiology Staining: Ziehl- Neelsen staining, Auramine Rhodamine Culture methods: Sterile specimen can be inoculated directly Non Sterile specimen require chemical decontamination by NaLC-NaOH method Solid media: Middlebrook 7H11 and Lowenstein-Jensen Liquid media: BACTEC 12 B and MGIT Duration: one week for Rapidly growing and 2-3 weeks for slowly growing New techniques for species identification: Nucleic Acid probes, HPLC, PCR- RLPA, 16S Ribosomal DNA sequencing Susceptibility testing: Critical concentration method is used Woods, G. L., Susceptibility Testing of Mycobacteria, Nocardiae, and Other Aerobic Actinomycetes, Wayne : CLSI

9 Virulence Factors Mycobacterium: General Characteristics, Laboratory Detection, and Staining Procedures. In: Manual of Clinical Microbiology. Canada: ASM, pp
10 Microbiology: MAC Rapidly identified on HPLC Nucleic acid probes are also commercially available (Accuprobe, GenProbe) DST: single concentration DST do not correlate with in vivo responses Exception: Macrolides and Amikacin Clarithromycin sensitivity should be done in all clinical cases (IIA) In Macrolide resistant cases newer Quinolones and Linezolid sensitivity can be done J Infect Dis Jul 15; 186(2):
11 Microbiology: M. Kansasii Slowly growing Mycobacterium- Photochromogenic M. Kansasii found exclusively in treated water sources DST: In vitro Rifampicin sensitivity should be done in all cases (IIA) Sensitivity to Rifabutin, Clarithromycin, ethambutol, Fluoroquinolones and aminoglycosides should be done in Rifampicin resistant isolates Extremely virulent organism unlike other NTMs Clin Infect Dis May;18(5):736-43
12 Microbiology: RGM M. Abscessus, M. Fortuitum, M. Chelonae Can grow on Blood Agar as well as Chocolate Agar media Chemical decontamination should be avoided as they are susceptible Inherently resistant to Isoniazid, Ethambutol, Rifampicin Inducible macrolide resistance gene (erm) (50S RNA) Drug sensitivity test for Imipenem and Aminoglycosides should be done Abstr Annu Meet Am Soc Microbiol 2005;104.
13 Content 1. Introduction 2. Microbiology 3. Epidemiology 4. Diseases 5. Diagnosis 6. Treatment 7. Individual species
14 Epidemiology Soil and water sources (rinsing mouth with tap water) Spa, Showers and pools commonly have MAC isolates Resistant to conventional decontamination Not following manufacturers instructions for cleaning increases risk of growth M. xenopsi, M. mucogenicum, M. simiae and M. Lentiflavum are usually contaminants No evidence of animal to human or human to human transmission Centers for Disease Control and Prevention. Nontuberculous mycobacteria reported to the public health laboratory information system by state public health laboratories: United States,
15 Epidemiology Symptomatic disease is due to reinfection instead of reactivation MAC is the most common NTM Pulmonary disease is the most common manifestation Disease burden correlates with bacterial load Burden of NTM cases is increasing.
16 Reasons for increase burden Increased susceptibility of individuals Improved techniques for primary culture of NTM Detection of infection by direct DNA isolation and sequencing
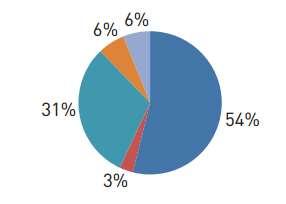
17 Distribution- Asia Total Eur Respir J Dec;42(6):
 Emg Inf Diseas J.")
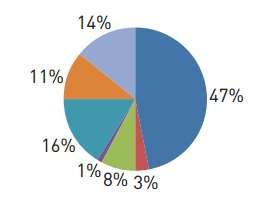
18 Asian countries 5 most prevalent NTM species found in respiratory specimens ( ) Emg Inf Diseas J Mar;17(3):
19 Indian epidemiology Prevalence- not exactly known NTM- not a reportable condition Lack of awareness among clinicians Lack of laboratory capacity to diagnose these infections
20 Indian scenario 133 isolates of NTM were studied to species levels Clinical aspects of the patients were considered 81% of the NTM were recovered from pulmonary and 19% from extra-pulmonary specimens. SGM: 40% were identified as M. Intracellulare, followed by M. Simiae (35%), M. kansasii (6%) RGM: M. fortuitum (41%) and M. abscessus (59%) 58 (46%) NTM met clinical, radiological and microbiological criteria. Int J Tuberc Lung Dis Aug;14(8):


21 CMC Vellore Indian J Med Microbiol Jul;23(3):172-5.

22 LRS Institute of TB & Respiratory Diseases (Indian J Tuberc 2013; 60: 71-76)
23 SGPGI Biomed Res Int. 2015; 2015:

24 PGIMER Indian J Med Res Mar;91:111-4.
25 Content 1. Introduction 2. Microbiology 3. Epidemiology 4. Diseases 5. Diagnosis 6. Treatment 7. Individual species
26 Diseases Pulmonary disease Hypersensitivity diseases Disseminated disease Lymphatic disease Skin, soft tissue and bone infections
27 Disease Spectrum Am J Respir Crit Care Med 2007 Feb 15;175(4):
28 Pulmonary manifestations Most common NTM manifestation Risk factors : o Age o Male o Low BMI o Prior lung disease o Exposure to soil o Working in water resources o GERD
29 Symptoms Chronic cough Sputum production Fatigue Malaise Dyspnea Fever Hemoptysis Weight loss
30 Radiographic changes 2 types: Fibrocavitatory: Can be evaluated only on Chest X ray basis Thin walled cavities with less parenchymal opacity Less bronchogenic but more contiguous spread Common pleural involvement Nodular/bronchiectatic: Need HRCT for evaluation Mid- and lower- lung fields Multifocal bronchiectasis Small (<5 mm) nodules Can even cause dense solitary pulmonary nodule

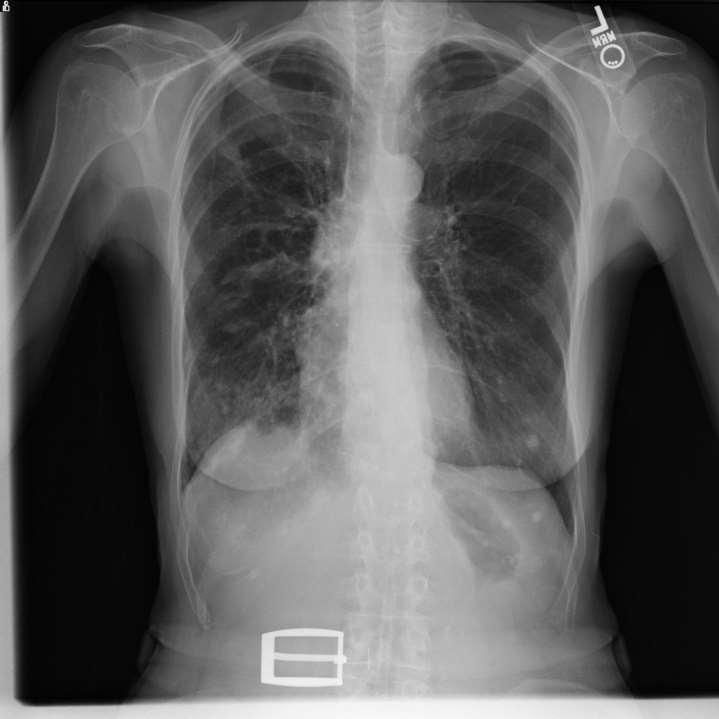
31 MAC MAC

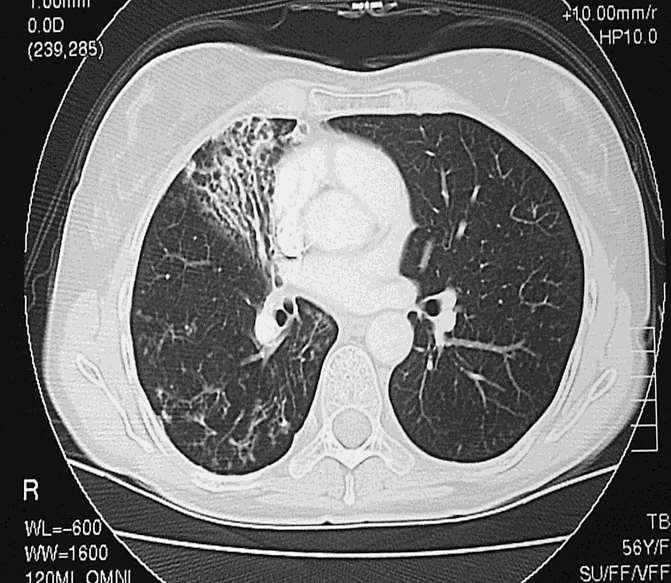
32 MAC MAC


33 M. Kansasii M. Abscessus
34 NTM pulmonary disease Fibrocavitatory disease Commonly occurs in patients with COPD & other structural lung diseases including silicosis, pneumoconiosis or prior TB infections Often older males H/O of heavy smoking & heavy alcohol consumption Predominant symptoms o Productive cough (occurring in >80% of patients) o Weight loss or weakness (in approximately half) o Fever or night sweats (each in 10% to 20% of patients) Am J Respir Crit Care Med 2007 Feb 15;175(4):
35 NTM pulmonary disease Nodular/Bronchiectatic disease In middle-aged to elderly women with no preexisting lung disease Referred to as the Lady Windermere syndrome Presents with a more indolent clinical picture Usually present with chronic cough Mild scoliosis and pectus excavatum Chest radiograph may show discrete pulmonary nodules in middle lobe or lingular regions Am J Respir Crit Care Med 2007 Feb 15;175(4):
36 NTM pulmonary disease Hypersensitivity pneumonitis Known as Hot-tub lung disease Occurs in persons exposed to pools of heated water containing MAC Associated with standing water source, showers and aeration systems NTM are resistant to common disinfectants Common in metal working fluids (M. immunogenum) Young non smoker population Am J Respir Crit Care Med 2007 Feb 15;175(4):
37 Hypersensitivity like disease Mild-to-moderate dyspnea Dry cough with or without fever Chest radiographs and CT scans :- o Centrilobular nodules o Ground-glass opacities MAC should be isolated form the respiratory specimens PFT can show mixed patterns Steroid with or without anti mycobacterial therapy
38 Radiology differences from Tuberculosis No imaging finding is sufficiently specific for diagnosis
39 NTM and Cystic Fibrosis 10,000-fold greater prevalence in respiratory cultures from patients with CF Reported prevalence varies dramatically even at single centres Largest studies (US & Europe): overall prevalence is 6% to 13% Most common: MAC and M.abscessus Concept of colonization Vs indolent disease is an untested hypothesis One hypothesis is that Bronchiectasis in cyctic fibrosis is a resultant of NTM disease Yearly screening Clin Chest Med 36 (2015)
40 Cystic fibrosis Other organisms should be considered and treated before initiating the therapy for NTM NTM should be ruled out before initiating macrolide monotherapy for CF Drug malabsorption due to pancreatic insufficiency adds to the enigma Surgical treatment should be reserved for severe, symptomatic and localized diseases NTM disease is not a concern in post transplant
41 Content 1. Introduction 2. Microbiology 3. Epidemiology 4. Diseases 5. Diagnosis 6. Treatment 7. Individual species
42 Specimen processing Samples from nonsterile body sites: Decontamination by-nalc-naoh method (MC used) Sterile body sites- Decontamination not required Tissues grounded aseptically in sterile physiological saline or bovine albumin & directly inoculated into media Smear microscopy Screened by fluorochrome (auramine) staining Confirmed by ZN staining
43 Cultures Isolation of NTM is must for initiation of therapy Contamination of the specimen can be confounding factor Uncommon species are usually contaminants Three sputum samples on separate days All samples should have an AFB staining Bronchial washing samples- more sensitive and less prone to contamination Histopathological specimen with demonstration of GI and AFB is diagnostic GI on biopsy + negative Biopsy culture= should have BAL/sputum positive for diagnosis
44 Culture ALL culture for NTM should include SOLID LIQUID AUTOMATED Lowenstein-Jensen agar Middlebrook 7H10 & 7H11 Middlebrook 7H9 broth MGIT 960 (Becton-Dickinson) BACTEC 9000 MB VersaTREK (Trek Diagnostics) Special supplementation: M. haemophilum (Hemin) Mycobacterium: General Characteristics, Laboratory Detection, and Staining Procedures. In: Manual of Clinical Microbiology. Canada: ASM, pp
45 NTM identification Phenotypic testing Biochemical Testing HPLC Mass spectrometry Nucleic acid based testing
46 Scheme for identification Growth obtained on culture Niacin test MTB complex NTM Rapid growers- growth on MacConkey Nitrate reductase M. fortuitum (+) M. chelonae (-)
47 Biochemical test TEST M.kansasii M.marinum M.simiae M.asiaticum MAC Nitrate reduction Catalase >45mm v Niacin - -/+ weak + (2-3%) Arylsulfatase 2 wk - - -/+ ++ -/+ +/- - Urease + + +/- - -
48 Chemotaxonomic Testing: HPLC Based on lipid composition analysis First saponification of mycobacterial cells Derivatization of mycolic acids to ester form Separation in columns and identification of patterns Highly sensitive and specific Limitation: time consuming and costly


49 MPT-64 MPT64, a 24 kda secretory protein one of the major antigens of MTb Simple and rapid Immunochromatographic test Using monoclonal anti-mpt64 antibody Able to discriminate between MTBC and NTM Indian J Tuberc 2012; 59: 92-96
50 Molecular methods FDA approved: Acridium ester labelled DNA probes specific for MAC, M. kansasii, and M. gordonae Currently used in many clinical laboratories (AccuProbe; Gen-Probe) Technique: based on release of target 16S rrna from organism Identification of the species can be achieved within 2 hrs Specificity 100% Sensitivity %
51 PRA (PCR restriction endonuclease assay) Based on coupling of PCR of a 441- bp sequence of gene hsp65 followed by restriction enzyme digestion Size of restriction fragments are generally species specific Relatively rapid Do not require viable organisms Identifies many NTM species that are not identifiable phenotypically
52 Molecular typing methods Pulsed-field gel electrophoresis (PFGE) Involves embedding the isolates in agarose gels, lysing the DNA, and digesting chromosomal DNA with specific restriction endonucleases Time-consuming procedure
53 Final Diagnosis Other lung disease must be ruled out ATT can be started empirically till the evaluation is complete if AFB is positive Single set of criteria may be inaccurate Pure Colonization without disease is uncommon and should be evaluated for tissue invasion NTM is an indolent disease hence confirmed diagnosis should be made in all cases M. Kansasii is an exception due to its virulent nature (single positive specimen) Low virulence NTM isolation should be kept under follow up
54 Diagnosis Clinical symptoms Isolation of the NTM: Sputum- at least 2 expectorated sputum samples should show growth At least one BAL sample positive Culture from biopsy specimen Histopathology: granulomatous inflammation with or without AFB positivity Chest X ray: Fibrocavitatory opacities HRCT chest: multifocal bronchiectasis with multiple nodules Am J Respir Crit Care Med 2007 Feb 15;175(4):
55 ATS/IDSA 2007
56 Content 1. Introduction 2. Microbiology 3. Epidemiology 4. Diseases 5. Diagnosis 6. Treatment 7. Individual species
57 Treatment Treatment duration: 12 to 24 months In vitro susceptibility might not correlate with in vivo effect Empiric therapy for NTM is not recommended Treatment is individualized as per pathogen Also in vitro DST is recommended for some species Drug toxicities also play role in decision making Immunosuppression changes treatment strategies.
58 Armentorium Macrolides Rifampicin Ethambutol Aminoglycosides Isoniazid Fluoroquinolones Surgery
59 Content 1. Introduction 2. Microbiology 3. Epidemiology 4. Diseases 5. Diagnosis 6. Treatment 7. Individual species
60 Mycobacterium Avium complex
61 Introduction Mycobacterium Avium: pulmonary disease and disseminated disease Mycobacterium intracellulare: pulmonary disease Found in water, soil, and in animals Most common NTM
62 MAC : Clinical Presentation Males Fibrocavitatory disease Smokers Alcohol users Apical regions Progressively causing respiratory failure over 1 to 2 years Nodular infiltrates Right middle lobe Postmenopausal Non smokers Lady Windermere syndrome Slower progression
63 MAC: Drug Treatment Macrolides: Clarithromycin > Azithromycin Only macrolide DST correlated with clinical response
64 Macrolide monotherapy (Wallace et al/texas) Prospective, non comparative trial, low dose, daily, single drug study for non HIV MAC patients DST done: clarithromycin sensitive were included Dose: 500 mg BD Finally 80 pt were evaluated 79 pt showed culture response with 58 % becoming negative No control no follow up less no of patients. Non uniform population Am J Respir Crit Care Med May;149(5):
65 Azithromycin vs clarithromycin (Ward et al/oregon) HIV positive Blood culture positive for MAC No previous treatment 600 mg azithromycin with 800 mg ethambutol vs 500mg BD clarithromycin with 800 mg ethambutol Follow up was done with blood cultures 59 subjects were enrolled Clin Infect Dis Nov;27(5):
66 Results Study was stopped prematurely in view of interim analysis showing significant difference in culture negativity Clearance of bacteremia was 37 % in azithromycin arm and 87 % in the clarithromycin arm Clinical symptom improvement was not difference at per significance Clin Infect Dis Nov;27(5):
67 Azithromycin vs clarithromycin (Dunne et al/ Texas) Randomized controlled trial 246 HIV Positive pt with disseminated MAC US, Brazil, Argentina, Chile: 55 centers DST was done on all isolates Azithromycin 600 mg + Ethambutol Vs Clarithromycin 500mg BD + Ethambutol Duration for 24 weeks and follow up for one year Clin Infect Dis Nov;31(5):
68 Outcomes Azithromycin group Clarithromycin group Culture negativity 46% 56% 0.24 Relapses 39% 27% 0.21 Adverse effects 63% 66% Clinical improvement at 12 weeks 68% 91% 0.02 Clinical improvement at 24 weeks 71% 73% 0.8 p Value Except for the early improvement in symptoms with clarithromycin group, the two drugs were similar
69 Intermittent therapy thrice weekly (Jeon et al/seoul) Retrospective comparative Non HIV 8 year period Criteria used for diagnosis: 2007 ATS/IDSA Patient excluded: Fibrocavitatory disease Previous macrolide use in one month Previous NTM treatment High lever Clarithromycin resistance on DST Treated with rifampicin, ethambutol and oral macrolide Am J Respir Crit Care Med Jan 1;191(1):96-103
70 Dosage Daily Intermittent Clarithromycin/Azithromycin 1000/ /500 Ethambutol 15mg/kg 25mg/kg Rifampicin Duration 24 Months 12 months of culture negativity (mean 18 months)

71 Outcomes
72 Risk factors for adverse response to intermittent therapy Old age AFB positivity Male
73 Factors predicting the success of intermittent regimen (Lam et al/san Diego) Comparative, prospective trial Cavitatory vs non Cavitatory disease 91 HIV negative patients were treated with TIW regimen Followed up for one year with cultures Am J Respir Crit Care Med.2006 Jun 1;173(11):1283-9
74 Outcomes Culture negative HRCT improved Symptom improved Cavitatory Non Cavitatory Total Am J Respir Crit Care Med.2006 Jun 1;173(11):1283-9
75 Discussion Non Cavitatory disease responded better than Cavitatory disease Older better than younger Previously non treated better than treated AFB negative responded well No history of COPD or bronchiectasis responded better HRCT response preceded symptom response and culture response Am J Respir Crit Care Med.2006 Jun 1;173(11):1283-9
76 3 Vs 2 drug regimens (Miwa et al/hamamatsu) Both types of MAC were included in the study 2007 ATS/IDSA criteria were used Immunosuppressed patients and clarithromycin resistant MAC population were excluded Treatment was given for 12 months Sputum conversion was defined as three sequential sputum culture to be negative Ann Am Thorac Soc 2014 Jan;11(1):23-9
77 Rationale: Rifampicin is the enzyme inducer hence decreasing the levels of clarithromycin (the most effective drug for MAC) Serum clarithromycin metabolite levels were estimated 2 weeks after the starting of treatment Drugs Dosage Clarithromycin 600 Ethambutol 750 Rifampicin 450 Ann Am Thorac Soc 2014 Jan;11(1):23-9
78 Outcomes 2 drug regimen was not inferior to 3 drugs regimen 2 drug regimen should not be used in HIV positive and disseminated MAC infections Limitation: small population, no follow up as per recommendation, no continuation of treatment for 12 months Ann Am Thorac Soc 2014 Jan;11(1):23-9
79 Use of fluoroquinolones (Fujita et al/fukuoka) Rifampicin + ethambutol + gatifloxacin Vs Rifampicin + ethambutol + Clarithromycin Rationale: Gatifloxacin has a low MIC value on DST of MAC HIV/ Diabetic/ CHF were excluded End point was eradication defined as three sequential culture specimens to be negative Treatment given for one year 27 patients Adverse effects were more with gatifloxacin but insignificant J Infect Chemother (2012) 18:
80 Outcomes Relapse rates were similar Eradication rates were similar This study also demonstrated the clinical and MIC correlation (in vivo and in vitro) Limitations: small, observational, no long term follow up, Can be considered as second line Moxifloxacin, Satifloxacin also have lower MAC J Infect Chemother (2012) 18:
81 Role of aminoglycosides (Kobashi et al/kurashiki) Streptomycin was used 15 mg /kg thrice weekly for three months Overall treatment constituted clarithromycin, ethambutol and rifampicin Duration of treatment was 24 months As per ATS IDSA guidelines patients were randomized Baseline clinical and demographical characteristics were matched HIV negative patients were included Respiratory Medicine (2007) 101,
82 Outcomes Sputum conversion rates were statistically more in SM group No difference in sputum relapse rates No statistically significant difference was there w.r.t. clinical efficacy or radiological efficacy Also there were no statistically significant difference in adverse effects Respiratory Medicine (2007) 101,
83 Role of interferon gamma (Virelles at al/havana) Eighteen patients Rational: IFN gamma plays an important role in activation Th1 response and macrophages Patients with contraindication to interferon therapy were excluded IGN gamma was given daily for 4 weeks and thrice weekly for 20 weeks Conventional treatment that was given to both arms was ciprofloxacin, azithromycin, rifampicin and ethambutol Only 6 months treatment was given and 12 months follow up period BMC Infect Dis Feb 11;8:17.
84 Outcomes Radiological improvement was statistically more significant in the IFN group General clinical status was significantly better and improved early in the IFN group Adverse effects like flu like symptoms, cytopenias were well tolerated Response of MAC was better than that of M fortuitum and M. Kansasii
85 A word about HIV + MAC Prophylaxis : if CD4 < 50 cells/mm 3 Drugs for prophylaxis: Clarithromycin > Azithromycin Drugs for treatment: Clarithromycin > Azithromycin + ethambutol ± Rifabutin Duration: 12 months after culture negativity ART: should be started after 2 weeks When to stop prophylaxis: CD4> 100 cells/mm 3 for 3 months CDC 2015/ WHO 2014/ NACO 2007
86 Summarizing Clarithromycin DST is a must Monotherapy is not recommended Clarithromycin + Ethambutol + Rifabutin Azithromycin can be used in case of adverse effects TIW regimen can be used in patients without any risk factor for adverse outcome Aminoglycosides can be used for Cavitatory or disseminated disease Fluoroquinolones can used in second line
87 Mycobacterium kansasii
88 Tap water is the most important source Second most common NTM in US Risk factor HIV Pneumoconiosis (silicosis) COPD Alcoholism Malignancy Symptoms and clinical features are identical to M. Tb
89 Treatment ATT drugs: Ethambutol, Streptomycin and Rifampicin have actions against M. kansasii DST might not correlate with in vivo response Other drugs that are effective in vitro are: clarithromycin, amikacin, sulfamethoxazole, fluoroquinolones and rifabutin Rifampicin is the critical component of any regimen against M. kansasii DST shows that resistance to isoniazid and pyrazinamide is common
90 Drugs that have activity Study Participants Methods Result Observational lab based study by Diaz et all 2003/Spain 108 isolates of NTM were studied (8 isolates of M. kansasii) DST of levofloxacin, moxifloxacin, gatifloxacin and linezolid were studied All the drugs were active against M kansasii. Gatifloxacin and moxifloxacin having the lowest MIC Comparative study of DST by Alcaidde et all Barcelona/ isolated of consecutive clinical specimen were tested for susceptibility Drugs used were INH, R, E, S, linezolid, Telithromycin, clarithromycin, levofloxacin and moxifloxacin All were resistant to M tuberculosis doses of INH, R, S and E. In vitro activity of other drugs was moxifloxacin> levofloxacin=clarithromycin = linezolid >>> telithromycin Int J Antimicrob Agents Jun;21(6): Antimicrob Agents Chemother Dec;48(12):
91 Era of Rifamycin Study Retrospective study, Banks et all (wales/1983) Prospective study, Ahn et all (Texas/1983) Participants Methods Result 35 patient with diagnosis of M kansasii on multiple sputum cultures and symptomatic disease were reviewed Cure was defined on the discretion of treating physician, repeated culture negativity and radiographic improvement. All regimens had rifampicin and ethambutol 66% had preexisting lung disease, 88% were smokers, all sputum samples were sensitive for Rifampicin, 90% had Cavitatory disease, 5 died during study, 100 % sputum conversion, no relapse for 5 ½ years 40 patients were included, diagnosis was made on Chest X ray findings of cavitation and multiple sputum cultures to be positive Treated with R, INH, E for 12 months, and streptomycin 1gm twice weekly for 3 months 70 % had underlying lung disease, after 12 months of chemotherapy and mean 31 months of follow up there was one relapse at 6 months. Culture negativity was achieved at mean on 5.5 weeks Thorax 1983 Apr; 38(4): Am Rev Respir Dis 1983 Dec;128(6):
92 Standardization of regimens Study Participants Retrospective study by Ahn et all (Texas/1981) Evaluation of chemotherapy of 256 patient with M. kansasii Prospective multicentric by Jenkins et all (BTS/Cardiff/ 1994) 173 patients with M. Kansasii in multiple sputum culture with Cavitatory disease on CXR were recruited Methods Records, cultures and DST were reviewed Given rifampicin and ethambutol for 9 months and followed up for 51 months Result Of regimens containing rifampicin 100% had sputum conversion at 4 months with none relapsing, but of regimens not containing rifampicin 90% had sputum conversion at 4 months with 7 % relapsing Duration of chemotherapy course was not analyzed. 50 % had pervious history of lung disease, 9 % relapsed, one patients never had culture negativity, radiographic improvement was noticed in 80%. 15 died during study (8 of respiratory failure only one of whom was having culture positivity) Thorax May; 49(5): Rev Infect Dis Sep-Oct;3(5):
93 R + E + M Study Participants Methods Result Prospective uncontrolled study by Griffith et all 2003/Texas 18 consecutive patients of M Kansasii lung disease (non pregnant, non HIV, no history of life threatening disease, no resistance to R or macrolides) Sputum samples were obtained monthly, pretreatment DST to R and clarithromycin was done. All patients received clarithromycin 500/1000mg, R 600mg, ethambutol 25 mg/kg thrice weekly. Therapeutic end point was 12 months of culture negativity 13 pt had bilateral upper lobe cavities, rest had nodulo-bronchiectatic disease. Time to sputum conversion was 1 ± 0.9 months. Duration of therapy 13.4 ± 0.9 months. No pt had relapsed after 4 years of follow up. Clin Infect Dis Nov 1;37(9):
94 Summarizing Highly virulent disease Presentation is similar to M. Tuberculosis Rifampicin is the most active drug Rifampicin DST should be done R, E, M and Streptomycin are active drugs
95 Mycobacterium abscessus
96 Clinical characteristics Nodular bronchiectasis is the main manifestation of M. Abscessus group lung disease Most common radiological feature is multiple micro-nodules, bronchiectasis, tree in bud. M. abscessus is the most common RGM Recently M Abscessus has been differentiated into M. abscessus sensu stricto, M. massiliense, and M. bolletii Treatment responses are better for M. massiliense compared to M Abscessus Zhonghua Jie He He Hu Xi Za Zhi Sep;36(9): Radiology Apr;263(1):
97 RGM introduction Study Participants/Methods Result Conclusion Retrospective study by Griffith et all (Texas/1993) 154 clinical isolates of RGM were identified who fulfilled ATS diagnostic criteria Predominant patients were white, female, non smokers Upper lobe infiltrates was the most common radiographic feature (88%)with 77% having bilateral disease Only 16% had cavities 8% had coexistent MAC isolation 82% were M abscessus and rest were M fortuitum 14 % died as a consequence of respiratory failure attributable to RGM Fortuitum isolate showed better response to antibiotic and M abscessus had better response to surgery Am Rev Respir Dis May;147(5):
98 Non Human studies Study Comparative lab based experimental study by Choi et all (Daejeon, Korea/ 2012) Participants Methods Result Conclusion 23 M. abscessus and 24 M. massiliense isolates were studies and followed up Clarithromycin and azithromycin sensitivity Was tested along with erm41 gene testing and gene knockout, Clarithromycin has lower MIC for M abscessus as well as M Massiliense Inducible resistance is more common in clarithromycin than azithromycin Clarithromycin induces erm gene more than azithromycin In lung model Azithromycin had significantly more decrease in bacterial load as compared to clarithromycin Serum and lung level distribution was equal for CLR and AZM Azithromycin has lower resistance rates against M Abscessus but response is equal in M Massiliense Am J Respir Crit Care Med Nov 1;186(9):
99 Preliminary studies Study Participants/Methods Result Conclusion Retrospective study by Huang et all (Taiwan/2010) 40 pt records who were diagnosed with M. abscessus were reviewed and with performing DST Only 22 pt met with the criteria of M. Abscessus pulmonary disease Cough, fever, hemoptysis were the most common symptoms Radiographically retico-nodular opacities, consolidation and cavities were most common All isolates were sensitive to antibiotics (full spectrum) Treatment failure by the end of 12 th month was 27% M Abscessus is naturally sensitive to clarithromycin and amikacin Variably sensitive to cefoxitin and amikacin Therapy require prolonged course with parenteral antibiotics Relapse rates are still high J Microbiol Immunol Infect Oct;43(5):401-6
100 One Parenteral Vs two Parenteral Study Retrospective study by Lyu et all (South Korea/ 2012) Participants/Methods Result Conclusion 41 Pt treated as per ATS guidelines for M abscessus were reviewed and follow up were taken 41 pt were treated with macrolide and one parenteral drug 58 % were treated with macrolides and two parenteral drugs Mean duration of parenteral drugs was 230 days and mean duration for total treatment was 511 days Treatment success, failure and relapse rate s were 80.5, 12.2, 7.3 % There was no significant difference between those receiving two or one parenteral drugs Combination antibiotic therapy, including long-term (minimum 2 4 months) parenteral drugs, as recommended by the ATS, resulted in successful treatment outcomes in 80.5% of patients with M. abscessus lung disease in Korea. Respir Med May;105(5):781-7
101 Differentiation into subspecies Study Retrospective study by Koh et all (Seol/ 2011) Participants/Methods Result Conclusion Molecular identification, along with comparison of clinical profile and treatment outcome were compared for 64 pt of M. abscessus and 81 pt M. Massiliense Clinical characteristics and radiographic abnormalities were similar in both groups Most of the pt in both groups received clarithromycin along with one month of parenteral cefoxitin and amikacin Sputum conversion and maintenance of negative sputum was 88 % in M. massiliense and 27% in M. abscessus All clinical isolates of M Abscessus had clarithromycin inducible resistance Treatment responses are higher in M Massiliense Inducible in vivo resistance might explain the lack of response in M. abscessus Am J Respir Crit Care Med Feb 1;183(3):
102 M. Abscessus and its subspecies Study Retrospective study by Harada et all (Sapporo/ 2013) Participants/Methods Result Molecular identification, clinical characteristic, treatment outcome comparison was done for 102 RGM isolates was done 72 were M Abscessus, 27 M Massiliense, 3 M Bollete Clinical characteristics were similar Among radiologic features bronchiectasis was significantly more common in M abscessus than other but rest of the findings were similar Streptomycin was uniformly ineffective, imipenem resistance was more in M. massiliense as compared to M abscessus All ATT were ineffective as were ciprofloxacin and moxifloxacin Sputum conversion rates were lower for M abscessus and relapse rates were higher Conclusion Treatment responses rates with CAM-based antibiotic therapy were higher for M. massiliense than in M. abscessus lung disease J Clin Microbiol Nov;50(11):
103 M. Abscessus Vs M. Massiliense Study Participants/Methods Retrospective study to compare the clinical outcomes of M Abscessus and M massiliense by Lyu et all (South Korea/2014) 59 pt with M. abscessus and 69 with M. massiliense were reviewed for treatment outcomes Result Most common regimen was Macrolide + amikacin + cefoxitin followed by M + A+ Imipenem Treatment duration for parenteral drugs was 7.4 month for M. Abscessus and 4.7 months for M Massiliense Total treatment duration was 16 months for M. Abscessus and 12.1 months for M Massiliense Relapse rate was 19% in M. massiliense and 27% in M. abscessus Conclusion Patients with M. massiliense pulmonary infection responded better to this antibiotic strategy than those with M. abscessus infection. Respir Med Nov;108(11):
104 In Cystic Fibrosis Study Prospective cohort study by Roux et all (Guyancourt France/ 2015) Participants/Methods Result Conclusion 16 pt with M Massiliense and 27 with M abscessus lung infection along with cystic fibrosis were followed up for 6 years M. Massiliense pt were significantly younger and had lower BMI as compared to the pt with M abscessus Transient colonization was more common with M. massiliense, eradication with antibiotic therapy was early and more prolonged with M. massiliense Particular link between M. massiliense and malnutrition specifically in CF patients Antibiotic response is better with M. massiliense J Cyst Fibros Jan;14(1):63-9
105 Newer therapies Study Retrospective analysis of Tigecycline containing regimens for M. Abscessus by Wallace (Texas/2014) Retrospective analysis of inhaled Amikacin for mycobacterium abscessus by Olivier (Boston/ 2013) Participants 52 patient records were reviewed Records reviewed from 2003 to 2010 Methods Result Conclusion Patients were reviewed on the basis of length of Tigecycline use 88 %had already received macrolide, amikacin and linezolid, 69% had pulmonary disease 58 %had underlying cystic fibrosis 61 % were considered improved. With the use of Tigecycline for M. abscessus for more than one month 60% patients result in improvement and 90% will have adverse effects Inhaled amikacin (n=20) Amikacin 250mg/ml was nebulized with 3 ml saline and was started at OD dose was titrated every 2 weekly to 500mg BD 9 had Cavitatory lung disease, mean duration of treatment was 60 months before Amikacin. Followed up for median of 19 months. 45 % showed improvement is symptoms and 25 %had persistent culture negativity. 35% required Amikacin discontinuance in view of adverse effects. Inhaled amikacin can be considered as salvage treatment in refractory cases of M. Abscessus J Antimiroc Chemother Jul;69(7): Ann Am Thorac Soc Jan;11(1):30-5
106 Surgery (for NTM) Study Participants Methods Result Retrospective analysis of pneumectomies for NTM by Shiraishi et all (Tokyo/2004) 53 patients infected with nontuberculous mycobacteria underwent 55 pulmonary resections Indications for pneumonectomy included multiple cavities in one lung and destruction of an entire lung. Predominant disease was MAC and M. abscessus No operative mortality, 3 pt developed BP fistula, two late deaths, No relapse, symptoms improvement in all Conclusion Despite bronchial stump protection, right pneumonectomy carries a risk for bronchopleural fistula. Nonetheless, pneumonectomy can result in high cure rates in patients with nontuberculous mycobacterial infections. Ann Thorac Surg Aug;78(2):
107 Surgery for M. Abscessus Study Participants Methods Result Conclusion Retrospective analysis of medical Vs surgical management in M abscessus by Jarand et all (Colorado/2010) 69 patients of known M abscessus pulmonary disease were reviewed Routine follow up data was collected apart from review of culture records 23 underwent surgery in addition to medical treatment and 46 received only medical treatment. 98% had nodulo-bronchiectatic disease and 44% had cavities. 92 % had bilateral multilobar disease Most common antibiotics given were Azithromycin, amikacin, imipenem, Clarithromycin, cefoxitin, ciprofloxacin. 25 lobectomies and 6 pneumectomies 39% became sputum negative in medical arm and 65 % in surgical arm 61% and 35% in medical arm and surgical arm respectively either never converted or relapsed Surgical resection offers a prolonged microbiologic response Clin Infect Dis Mar 1;52(5):565-71
108 Summarizing No antibiotic regimen has been proven to be superior to other Most of the effective antibiotics are parenteral except macrolides Commonly effective parenteral antibiotics are amikacin, imipenem, cefoxitin Newer antibiotics found to have in vitro activity but not studied are: linezolid, Tigecycline, Telithromycin Surgery is the only curative option for pt with limited disease Surgery should be early unlike in other NTM species Kekkaku Mar;90(3): Clin Chest Med Mar;36(1):67-78
109 Mycobacterium Fortuitum
110 Introduction RGM Pulmonary disease similar to M. Abscessus (though less common) Exception: pt with GERD and chronic vomitings with RGM pulmonary disease both occur in equal frequency Susceptible to most of the drugs erm38 gene is present- responsible for the inducible macrolide resistance Commonly found in heavy metal industries J Antimicrob Chemo. (2005) 55, Antimicrob Agents Chemother Oct;26(4):594-6.
111 RGM introduction Study Participants/Methods Result Conclusion Retrospective study by Griffith et all (Texas/1993) 154 clinical isolates of RGM were identified who fulfilled ATS diagnostic criteria Predominant patients were white, female, non smokers Upper lobe infiltrates was the most common radiographic feature (88%)with 77% having bilateral disease Only 16% had cavities 8% had coexistent MAC isolation 82% were M abscessus and rest were M fortuitum 14 % died as a consequence of respiratory failure attributable to RGM Fortuitum isolate showed better response to antibiotic and M abscessus had better response to surgery Am Rev Respir Dis May;147(5):
112 DST studies Study Participants/Methods Result Laboratory based study for DST to various drugs in M Fortuitum by Swenson et all (Texas/1985) 258 clinical isolates were tested for susceptibility with Broth microdilution test against Amikacin, Cefoxitin, Tobramycin, Doxycycline, Erythromycin & Ciprofloxacin DST to Amikacin, Cefoxitin showed susceptibility Uniformly resistant to erythromycin Variable resistant to Doxycycline and ciprofloxacin Conclusion In vitro susceptibility test should be performed for all clinical isolates of M. Fortuitum Antimicrob Agents Chemother Dec;28(6):
113 Summarizing Second most common RGM Lack of studies for standardization of protocols DST shows that most of the drugs are active M + R + E seems reasonable option
114 Finally
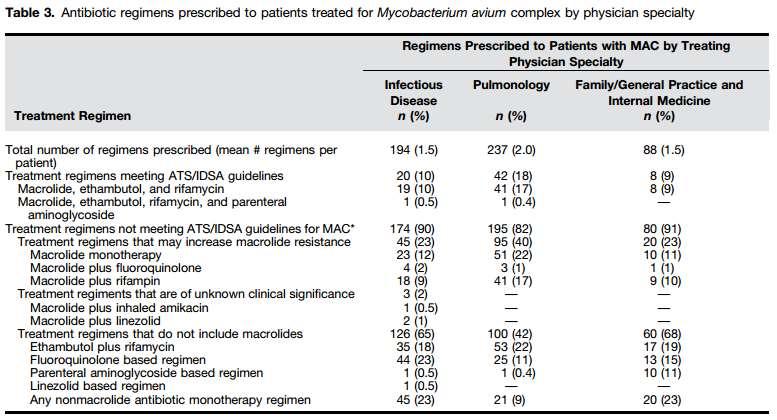
115 Lack of adherence to the guidelines (Adjemian et al/bethesda) 582 NTM treating physicians were contacted with a questionnaire Along with treatment record extracted for last 4 NTM patient they treated This data was compared with ATS/IDSA 2007 guidelines Ann Am Thorac Soc Jan; 11(1): 9 16.
116 Result 13 % antibiotic regimens met the criteria of ATS/IDSA 56 % did not contain a macrolide 16 % had macrolide monotherapy For M. abscessus 64 % did not contain macrolide Among Pulmonologists the adherence to the guidelines was 18%
117
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France
 Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
Treatment of Nontuberculous Mycobacterial Infections (NTM)
") Treatment of Nontuberculous Mycobacterial Infections (NTM) Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory
Treatment of Nontuberculous Mycobacterial Infections (NTM) Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory
Non-Tuberculous Mycobacterial Pulmonary Disease Diagnosis and Management Jakko van Ingen, MD, PhD
 Non-Tuberculous Mycobacterial Pulmonary Disease (NTM-PD) 1 Radbound University Nihmegen Medical Center Milestones in NTM research 1980s: Nodular bronchiectatic lung disease Lady Windermere syndrome 1882-1890
Non-Tuberculous Mycobacterial Pulmonary Disease (NTM-PD) 1 Radbound University Nihmegen Medical Center Milestones in NTM research 1980s: Nodular bronchiectatic lung disease Lady Windermere syndrome 1882-1890
Treatment of Slowly Growing NTM Infections
 Treatment of Slowly Growing NTM Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory Committee Insmed
Treatment of Slowly Growing NTM Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory Committee Insmed
Ting-Shu Wu, M.D. Infection Control Committee Infect Dis, Int Med, Chang Gung Memorial Hospital, Linkou Medical Center, Tao-Yuan, Taiwan
 Ting-Shu Wu, M.D. Infection Control Committee Infect Dis, Int Med, Chang Gung Memorial Hospital, Linkou Medical Center, Tao-Yuan, Taiwan NTM Other than M. tuberculosis, M. africanum, M. bovis, M. caprae,
Ting-Shu Wu, M.D. Infection Control Committee Infect Dis, Int Med, Chang Gung Memorial Hospital, Linkou Medical Center, Tao-Yuan, Taiwan NTM Other than M. tuberculosis, M. africanum, M. bovis, M. caprae,
Challenges to treat MDR TB
 Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
Dr Sharanjit Dhoot. Chelsea and Westminster Hospital, London. 18 th Annual Conference of the British HIV Association (BHIVA)
") 18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
TB Grand Rounds. MDR-TB: Management of Adverse Drug Reactions. Reynard J. McDonald, M.D. September 18, Patient History
 TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days
 Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Multidrug-resistant Tuberculosis. Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership
 Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
SENSITITRE. Broth Microdilution (MIC) Method:
 Method:") SENSITITRE Broth Microdilution (MIC) Method: For Rapidly Growing Mycobacteria (RGM), Slowly Growing Nontuberculosis Mycobacteria, Nocardia and other Aerobic Actinomycetes For Research Use Only For full
SENSITITRE Broth Microdilution (MIC) Method: For Rapidly Growing Mycobacteria (RGM), Slowly Growing Nontuberculosis Mycobacteria, Nocardia and other Aerobic Actinomycetes For Research Use Only For full
Treatment of Drug Resistant TB
 Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
Zyvox. Zyvox (linezolid) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.20 Subject: Zyvox Page: 1 of 7 Last Review Date: March 18, 2016 Zyvox Description Zyvox (linezolid)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.20 Subject: Zyvox Page: 1 of 7 Last Review Date: March 18, 2016 Zyvox Description Zyvox (linezolid)
Drug-resistant TB therapy: the future is now
 Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick
 Patrick") New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick Phillips Patrick.Phillips@ucsf.edu @PPJPhillips Outline Overview of regimen development strategies 1-3 year horizon: Ongoing phase
New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick Phillips Patrick.Phillips@ucsf.edu @PPJPhillips Outline Overview of regimen development strategies 1-3 year horizon: Ongoing phase
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Clinical Management : DR-TB
 Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION
 1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
Management of MDR and XDR TB Prof. Martin Boeree
 Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
Measure Information Form
 Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Period of study: 12 Nov 2002 to 08 Apr 2004 (first subject s first visit to last subject s last visit)
") Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Inappropriate Use of Antibiotics and Clostridium difficile Infection. Jocelyn Srigley, MD, FRCPC November 1, 2012
 Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
XDR TB: The Laboratory s Dilemma vs The Clinician s Dilemma
 XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
TB Intensive Houston, Texas. Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD
 TB Barbara Seaworth, MD") TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing - PRELIMINARY -
 Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
BRUCELLOSIS BRUCELLOSIS. CPMP/4048/01, rev. 3 1/7 EMEA 2002
 BRUCELLOSIS CPMP/4048/01, rev. 3 1/7 General points on treatment Four species are pathogenic to man: B. melitenis (acquired from goats), B. suis (pigs), B. abortus (cattle) and B. canis (dogs). The bacteria
BRUCELLOSIS CPMP/4048/01, rev. 3 1/7 General points on treatment Four species are pathogenic to man: B. melitenis (acquired from goats), B. suis (pigs), B. abortus (cattle) and B. canis (dogs). The bacteria
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
The New England Journal of Medicine THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY
 THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY KEMAL TAHAOĞLU, M.D., TÜLAY TÖRÜN, M.D., TÜLIN SEVIM, M.D., GÜLIZ ATAÇ, M.D., ALTAN KIR, M.D., LEVENT KARASULU, M.D., IPEK ÖZMEN, M.D., AND NILÜFER
THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY KEMAL TAHAOĞLU, M.D., TÜLAY TÖRÜN, M.D., TÜLIN SEVIM, M.D., GÜLIZ ATAÇ, M.D., ALTAN KIR, M.D., LEVENT KARASULU, M.D., IPEK ÖZMEN, M.D., AND NILÜFER
Bai-Yi Chen MD. FCCP
 Treatment strategies for hospitalized versus nonhospitalized CAP patients: Asian perspective Bai-Yi Chen MD. FCCP Professor of Medicine Division of Infectious Disease, Infection Control Team The First
Treatment strategies for hospitalized versus nonhospitalized CAP patients: Asian perspective Bai-Yi Chen MD. FCCP Professor of Medicine Division of Infectious Disease, Infection Control Team The First
Prevalence of Metallo-Beta-Lactamase Producing Pseudomonas aeruginosa and its antibiogram in a tertiary care centre
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 952-956 http://www.ijcmas.com Original Research Article Prevalence of Metallo-Beta-Lactamase
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 952-956 http://www.ijcmas.com Original Research Article Prevalence of Metallo-Beta-Lactamase
Subacute Adenitis. Ann M. Loeffler, MD
 Subacute Adenitis Ann M. Loeffler, MD Lymphadenitis Swelling and hyperplasia of sinusoidal lining cells Infiltration of leukocytes +/- abscess formation Granulomatous or non-granulomatous Pyogenic adenitis
Subacute Adenitis Ann M. Loeffler, MD Lymphadenitis Swelling and hyperplasia of sinusoidal lining cells Infiltration of leukocytes +/- abscess formation Granulomatous or non-granulomatous Pyogenic adenitis
Clinical Manifestations and Treatment of Plague Dr. Jacky Chan. Associate Consultant Infectious Disease Centre, PMH
 Clinical Manifestations and Treatment of Plague Dr. Jacky Chan Associate Consultant Infectious Disease Centre, PMH Update of plague outbreak situation in Madagascar A large outbreak since 1 Aug 2017 As
Clinical Manifestations and Treatment of Plague Dr. Jacky Chan Associate Consultant Infectious Disease Centre, PMH Update of plague outbreak situation in Madagascar A large outbreak since 1 Aug 2017 As
ANTHRAX. INHALATION, INTESTINAL and CUTANEOUS ANTHRAX
 INHALATION, INTESTINAL and CUTANEOUS ANTHRAX CPMP/4048/01, rev. 3 1/7 General points on treatment Anthrax is an acute infectious disease caused by Bacillus anthracis, that may be infecting man via cutaneous
INHALATION, INTESTINAL and CUTANEOUS ANTHRAX CPMP/4048/01, rev. 3 1/7 General points on treatment Anthrax is an acute infectious disease caused by Bacillus anthracis, that may be infecting man via cutaneous
What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa.
 Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
TB New Drugs, Shorter Courses
 TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
Multi-Drug and Extensively Drug Resistant Tuberculosis
 Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective
 : The Belgian perspective") ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective Antwerpen 8 november 2002 Yvan Valcke MD PhD AZ Maria Middelares Sint-Niklaas ACUTE EXACERBATIONS of COPD (AE-COPD) Treatment of AECB Role
ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective Antwerpen 8 november 2002 Yvan Valcke MD PhD AZ Maria Middelares Sint-Niklaas ACUTE EXACERBATIONS of COPD (AE-COPD) Treatment of AECB Role
Preliminary Results of Bedaquiline as Salvage Therapy for Patients With Nontuberculous Mycobacterial Lung Disease
 [ Original Research Chest Infections ] Preliminary Results of Bedaquiline as Salvage Therapy for Patients With Nontuberculous Mycobacterial Lung Disease Julie V. Philley, MD ; Richard J. Wallace Jr, MD,
[ Original Research Chest Infections ] Preliminary Results of Bedaquiline as Salvage Therapy for Patients With Nontuberculous Mycobacterial Lung Disease Julie V. Philley, MD ; Richard J. Wallace Jr, MD,
M5 MEQs 2016 Session 3: SOB 18/11/16
 M5 MEQs 2016 Session 3: SOB 18/11/16 http://tinyurl.com/hn7qzt3 Question 1 Ms Tan is a 52 year old female with no past medical history. She comes to the emergency department presenting with a fever for
M5 MEQs 2016 Session 3: SOB 18/11/16 http://tinyurl.com/hn7qzt3 Question 1 Ms Tan is a 52 year old female with no past medical history. She comes to the emergency department presenting with a fever for
Antibacterial Resistance: Research Efforts. Henry F. Chambers, MD Professor of Medicine University of California San Francisco
 Antibacterial Resistance: Research Efforts Henry F. Chambers, MD Professor of Medicine University of California San Francisco Resistance Resistance Dose-Response Curve Antibiotic Exposure Anti-Resistance
Antibacterial Resistance: Research Efforts Henry F. Chambers, MD Professor of Medicine University of California San Francisco Resistance Resistance Dose-Response Curve Antibiotic Exposure Anti-Resistance
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC
 Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings
 Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings Jasmanda H. Wu, Ph.D., 1 David H. Howard, Ph.D., 2 John E. McGowan, Jr.,
Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings Jasmanda H. Wu, Ph.D., 1 David H. Howard, Ph.D., 2 John E. McGowan, Jr.,
MDR/XDR TB. Barbara Seaworth, MD, FIDSA, FACP October 27, TB Intensive October 24 27, 2017 San Antonio, TX
 MDR/XDR TB Barbara Seaworth, MD, FIDSA, FACP October 27, 2017 TB Intensive October 24 27, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Barbara Seaworth, MD, FIDSA, FACP, has the following disclosures
MDR/XDR TB Barbara Seaworth, MD, FIDSA, FACP October 27, 2017 TB Intensive October 24 27, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Barbara Seaworth, MD, FIDSA, FACP, has the following disclosures
Cystic Fibrosis- management of Burkholderia. cepacia complex infections
 Guideline Cystic Fibrosis- management of Burkholderia cepacia complex infections Key messages Burkholderia cepacia infections are associated with significant adverse outcomes in Cystic Fibrosis patients
Guideline Cystic Fibrosis- management of Burkholderia cepacia complex infections Key messages Burkholderia cepacia infections are associated with significant adverse outcomes in Cystic Fibrosis patients
number Done by Corrected by Doctor Dr Hamed Al-Zoubi
 number 8 Done by Corrected by Doctor Dr Hamed Al-Zoubi 25 10/10/2017 Antibacterial therapy 2 د. حامد الزعبي Dr Hamed Al-Zoubi Antibacterial therapy Figure 2/ Antibiotics target Inhibition of microbial
number 8 Done by Corrected by Doctor Dr Hamed Al-Zoubi 25 10/10/2017 Antibacterial therapy 2 د. حامد الزعبي Dr Hamed Al-Zoubi Antibacterial therapy Figure 2/ Antibiotics target Inhibition of microbial
Chapter 51. Clinical Use of Antimicrobial Agents
 Chapter 51 Clinical Use of Antimicrobial Agents History of antimicrobial therapy Early 17 th century Cinchona bark was used as an important historical remedy against malaria. 1909 Paul Ehrlich sought a
Chapter 51 Clinical Use of Antimicrobial Agents History of antimicrobial therapy Early 17 th century Cinchona bark was used as an important historical remedy against malaria. 1909 Paul Ehrlich sought a
MDR treatment. Shanghai, May 2012 Arnaud Trébucq The Union
 MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
Treatment of Multidrug-resistant Tuberculosis (MDR-TB)
") Treatment of Multidrug-resistant Tuberculosis (MDR-TB) 2006 2008 2011 2013 2014 2016 2019 Charles L. Daley, MD National Jewish Health University of Colorado Disclosures Research grant Insmed: Phase II
Treatment of Multidrug-resistant Tuberculosis (MDR-TB) 2006 2008 2011 2013 2014 2016 2019 Charles L. Daley, MD National Jewish Health University of Colorado Disclosures Research grant Insmed: Phase II
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S.
 Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience
 MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience Dr Johan Van Wyk MB.Ch.B, M.Med (Clin Path) Clinical Pathologist ibhayi Region, Eastern Cape GWYNETH PALTROW SHAKESPEARE IN LOVE 1998 PORT
MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience Dr Johan Van Wyk MB.Ch.B, M.Med (Clin Path) Clinical Pathologist ibhayi Region, Eastern Cape GWYNETH PALTROW SHAKESPEARE IN LOVE 1998 PORT
Microbiology : antimicrobial drugs. Sheet 11. Ali abualhija
 Microbiology : antimicrobial drugs Sheet 11 Ali abualhija return to our topic antimicrobial drugs, we have finished major group of antimicrobial drugs which associated with inhibition of protein synthesis
Microbiology : antimicrobial drugs Sheet 11 Ali abualhija return to our topic antimicrobial drugs, we have finished major group of antimicrobial drugs which associated with inhibition of protein synthesis
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Coccidioidomycosis Nothing to disclose
 Coccidioidomycosis Nothing to disclose Disclosure Greg Melcher, M.D. Professor of Clinical Medicine Division of HIV, ID and Global Medicine Zuckerman San Francisco General Hospital University of California,
Coccidioidomycosis Nothing to disclose Disclosure Greg Melcher, M.D. Professor of Clinical Medicine Division of HIV, ID and Global Medicine Zuckerman San Francisco General Hospital University of California,
Control emergence of drug-resistant. Reduce costs
 ...PRESENTATIONS... Guidelines for the Management of Community-Acquired Pneumonia Richard E. Chaisson, MD Presentation Summary Guidelines for the treatment of community-acquired pneumonia (CAP) have been
...PRESENTATIONS... Guidelines for the Management of Community-Acquired Pneumonia Richard E. Chaisson, MD Presentation Summary Guidelines for the treatment of community-acquired pneumonia (CAP) have been
Int.J.Curr.Microbiol.App.Sci (2017) 6(3):
 6(3):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
Source: Portland State University Population Research Center (
 Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE. Measure Information Form
 Last Updated: Version 3.2a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form Organization Set Measure ID#
Last Updated: Version 3.2a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form Organization Set Measure ID#
Introduction to Chemotherapeutic Agents. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018
 Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
* gender factor (male=1, female=0.85)
") Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB)
") Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB) Session: Fanning the Flames of HIV and TB Cointeraction SA AIDS Conference-Durban ICC 13-15 June 2017
Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB) Session: Fanning the Flames of HIV and TB Cointeraction SA AIDS Conference-Durban ICC 13-15 June 2017
TOPICS. Continuing Education April 2014 Volume 16 Number 2. Journal of. Inside This Issue. Official publication of the American Medical Technologists
 Journal of TOPICS & ISSUES Official publication of the American Medical Technologists Continuing Education April 2014 Volume 16 Number 2 Inside This Issue Back to the Future with Urinalysis: Part 2 A Confusing,
Journal of TOPICS & ISSUES Official publication of the American Medical Technologists Continuing Education April 2014 Volume 16 Number 2 Inside This Issue Back to the Future with Urinalysis: Part 2 A Confusing,
Tularemia. Information for Health Care Providers. Physicians D Nurses D Laboratory Personnel D Infection Control Practitioners
 Tularemia Information for Health Care Providers Physicians D Nurses D Laboratory Personnel D Infection Control Practitioners Tularemia Caused by Francisella tularensis, a small, pleomorphic, gram-negative
Tularemia Information for Health Care Providers Physicians D Nurses D Laboratory Personnel D Infection Control Practitioners Tularemia Caused by Francisella tularensis, a small, pleomorphic, gram-negative
University of Groningen. Tuberculosis and its sequelae Akkerman, Onno
 University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani
 Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Bacterial whole genome sequencing in clinical microbiology, infection control and public health. Julian Parkhill. FIS, Birmingham, November 2013
 Bacterial whole genome sequencing in clinical microbiology, infection control and public health Julian Parkhill FIS, Birmingham, November 2013 Falling costs of genomics 2003 Cost/genome Throughput 60,000
Bacterial whole genome sequencing in clinical microbiology, infection control and public health Julian Parkhill FIS, Birmingham, November 2013 Falling costs of genomics 2003 Cost/genome Throughput 60,000
BRUCELLOSIS. Morning report 7/11/05 Andy Bomback
 BRUCELLOSIS Morning report 7/11/05 Andy Bomback Also called undulant, Mediterranean, or Mata fever, brucellosis is an acute and chronic infection of the reticuloendothelial system gram negative facultative
BRUCELLOSIS Morning report 7/11/05 Andy Bomback Also called undulant, Mediterranean, or Mata fever, brucellosis is an acute and chronic infection of the reticuloendothelial system gram negative facultative
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements
 Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007
 Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Principles of Antimicrobial therapy
 Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
Case Report Atypical Mycobacterial Infection after Abdominoplasty Overseas: A Case Report and Literature Review
 Case Reports in Infectious Diseases Volume 2016, Article ID 3642567, 4 pages http://dx.doi.org/10.1155/2016/3642567 Case Report Atypical Mycobacterial Infection after Abdominoplasty Overseas: A Case Report
Case Reports in Infectious Diseases Volume 2016, Article ID 3642567, 4 pages http://dx.doi.org/10.1155/2016/3642567 Case Report Atypical Mycobacterial Infection after Abdominoplasty Overseas: A Case Report
Should we test Clostridium difficile for antimicrobial resistance? by author
 Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
Case Presentations: Non Responding TB Dr. Manoj Yadav
 Case Presentations: Non Responding TB Dr. Manoj Yadav mbbs, dtcd, dnb (resp. dis.) Consultant Pulmonologist Kailash Hospital, Kailash Complex Near Mahadev Temple, Productivity Road Vadodara 390007 :: Phone:
Case Presentations: Non Responding TB Dr. Manoj Yadav mbbs, dtcd, dnb (resp. dis.) Consultant Pulmonologist Kailash Hospital, Kailash Complex Near Mahadev Temple, Productivity Road Vadodara 390007 :: Phone:
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Summary of unmet need guidance and statistical challenges
 Summary of unmet need guidance and statistical challenges Daniel B. Rubin, PhD Statistical Reviewer Division of Biometrics IV Office of Biostatistics, CDER, FDA 1 Disclaimer This presentation reflects
Summary of unmet need guidance and statistical challenges Daniel B. Rubin, PhD Statistical Reviewer Division of Biometrics IV Office of Biostatistics, CDER, FDA 1 Disclaimer This presentation reflects
Levofloxacin and moxifloxacin resistant Haemophilus influenzae in a patient with common variable immunodeficiency (CVID): a case report
: a case report") 46 Case Report Levofloxacin and moxifloxacin resistant Haemophilus influenzae in a patient with common variable immunodeficiency (CVID): a case report CT Hapuarachchi 1, GK Karunaratne 2, NR de Silva 3,
46 Case Report Levofloxacin and moxifloxacin resistant Haemophilus influenzae in a patient with common variable immunodeficiency (CVID): a case report CT Hapuarachchi 1, GK Karunaratne 2, NR de Silva 3,
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Le infezioni di cute e tessuti molli
 Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Surgical prophylaxis for Gram +ve & Gram ve infection
 Surgical prophylaxis for Gram +ve & Gram ve infection Professor Mark Wilcox Clinical l Director of Microbiology & Pathology Leeds Teaching Hospitals & University of Leeds, UK Heath Protection Agency Surveillance
Surgical prophylaxis for Gram +ve & Gram ve infection Professor Mark Wilcox Clinical l Director of Microbiology & Pathology Leeds Teaching Hospitals & University of Leeds, UK Heath Protection Agency Surveillance
Antibiotic therapy of acute gastroenteritis
 Antibiotic therapy of acute gastroenteritis Potential goals Clinical improvement (vs control) Fecal eradication of the pathogen and decrease infectivity Prevent complications Acute gastroenteritis viruses
Antibiotic therapy of acute gastroenteritis Potential goals Clinical improvement (vs control) Fecal eradication of the pathogen and decrease infectivity Prevent complications Acute gastroenteritis viruses
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis
 Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis Steve SM Wong Alice Ho Miu Ling Nethersole Hospital Background PD peritonitis is a major cause of PD
Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis Steve SM Wong Alice Ho Miu Ling Nethersole Hospital Background PD peritonitis is a major cause of PD
The impact on the routine laboratory of the introduction of an automated ELISA for the detection of Cryptosporidium and Giardia in stool samples
 The impact on the routine laboratory of the introduction of an automated ELISA for the detection of Cryptosporidium and Giardia in stool samples Nigel Stephenson BMS 3 Department of Medical Microbiology
The impact on the routine laboratory of the introduction of an automated ELISA for the detection of Cryptosporidium and Giardia in stool samples Nigel Stephenson BMS 3 Department of Medical Microbiology
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
DR-TB PATIENT IDENTITY CARD
 Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
مادة االدوية المرحلة الثالثة م. غدير حاتم محمد
 م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
In Vitro Activities of Linezolid against Clinical Isolates of ACCEPTED
 AAC Accepts, published online ahead of print on April 00 Antimicrob. Agents Chemother. doi:./aac.001-0 Copyright 00, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
AAC Accepts, published online ahead of print on April 00 Antimicrob. Agents Chemother. doi:./aac.001-0 Copyright 00, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
Critical Appraisal Topic. Antibiotic Duration in Acute Otitis Media in Children. Carissa Schatz, BSN, RN, FNP-s. University of Mary
 Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
Antibiotic Usage Guidelines in Hospital
 SUPPLEMENT TO JAPI december VOL. 58 51 Antibiotic Usage Guidelines in Hospital Camilla Rodrigues * Use of surveillance data information of Hospital antibiotic policy guidelines from Hinduja Hospital. The
SUPPLEMENT TO JAPI december VOL. 58 51 Antibiotic Usage Guidelines in Hospital Camilla Rodrigues * Use of surveillance data information of Hospital antibiotic policy guidelines from Hinduja Hospital. The
MDR Acinetobacter baumannii. Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta
 MDR Acinetobacter baumannii Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta 1 The Armageddon recipe Transmissible organism with prolonged environmental
MDR Acinetobacter baumannii Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta 1 The Armageddon recipe Transmissible organism with prolonged environmental
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES
 AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
Burn Infection & Laboratory Diagnosis
 Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die