Multidrug-resistant Tuberculosis
|
|
|
- Joan Logan
- 6 years ago
- Views:
Transcription
1 Multidrug-resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive September 2016
2 Objectives Describe the national and global epidemiology of MDR and XDR-TB Recognize who is at higher risk for MDR TB Discuss interpretation of molecular tests for drug resistance List the general principles of MDR/XDR-TB treatment Discuss the challenges in managing contacts of MDR/XDR-TB Identify resources for education, training, and expert consultation 1
3 Terminology Mono-resistant: resistant to only one drug Poly-resistant: resistant to more than one drug, but not the combination of INH and RIF Multidrug-resistant (MDR): resistant to at least INH and RIF Pre-extensively drug-resistant (Pre-XDR): MDR plus resistance to fluoroquinolone (FQ) or a second-line injectable (Amikacin, Kanamycin, or Capreomycin) Extensively drug-resistant (XDR): MDR-TB plus resistance to a FQ and at least one second line injectable
4 Global MDR Burden 2014 Estimate: 480,000 incident cases Half from China, India and Russia Surveillance varies by country and region Resistance surveys vs continuous surveillance National vs subnational 2015: Data from 79% of countries since 1994 WHO Global Tuberculosis Control Report 2014 WHO. M/XDR TB: 2010 Global Report on Surveillance and Response


5 Percentage of New TB Cases with MDR TB Overall: 3.3% WHO, Global tuberculosis report

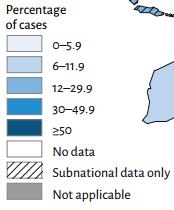
6 Percent of Previously treated cases with MDR-TB Overall: 20% WHO, Global tuberculosis report
7 XDR TB 9.7% of MDR TB cases 105 countries have reported at least 1 case TDR reports from Iran and India 6
 is defined as resistance")
8 Primary Anti-TB Drug Resistance, United States, * Resistant (%) Year * As of June 9, Note: Based on initial isolates from persons with no prior history of TB; multidrug-resistant TB (MDR-TB) is defined as resistance to at least isoniazid and rifampin.
 * As of June 9, 2016.")
9 Primary Isoniazid Resistance Among U.S.-Born versus Foreign-Born Persons, United States, * Resistant (%) * As of June 9, Note: Based on initial isolates from persons with no prior history of TB.
 defined as resistance to at least")
10 Primary MDR-TB Among U.S.-Born versus Foreign- Born Persons, United States, * Resistant (%) * As of June 9, Note: Based on initial isolates from persons with no prior history of TB; multidrug resistant TB (MDR-TB) defined as resistance to at least isoniazid and rifampin.

11 XDR-TB* Case Count, Defined on Initial DST, by Year, Case count Year of diagnosis * XDR-TB, extensively drug-resistant TB. DST, drug susceptibility test. As of June 9, Note: XDR-TB is defined as resistance to isoniazid and rifampin, plus resistance to any fluoroquinolone and at least one of three injectable second-line anti-tb drugs.
12 Multidrug-resistant TB Cases California, Number of MDR cases Percent of culture pos cases MDR cases Pct MDR 11
13 Recognition: Who Is At Higher Risk of MDR-TB? History of previous TB treatment, particularly if recent Known exposure to MDR-TB case HIV (+) Higher incidence of Rifampin mono resistance Poor response to standard 4-drug treatment Culture remains (+) after 2 months treatment
14 Recognition: Who Is At Higher Risk of MDR-TB? NonUS-born arrived in U.S. within last 2 years Immigration from or recent extended travel to country with > 2% MDR among cases from that country diagnosed in California/U.S. These countries* are: India Laos Russia and other former Soviet states Korea Peru Central America Burma Ecuador Dominican Republic Other state or locally identified risk groups, including: Hmong refugees Persons of Tibetan origin *California data from and U.S. data from Current U.S. data are available from the CDC, Division of TB Elimination (DTBE) ( 13
15 High-risk for MDR: Action Steps Obtain molecular test for drug resistance Xpert MTB/RIF, (pyro)sequencing, Hain line-probe test, or other Consider initiation of expanded regimen (rare in era of molecular testing) Contact of MDR-TB case with active TB Immigrant with history of extensive treatment for TB in the past and again has active TB Extended time to resistance information
16 Molecular Testing for Drug Resistance 15
17 Antimicrobial agent Isoniazid (INH) INH and Ethionamide Molecular Testing: Drugs/Loci Gene/locus katg inha promoter Sensitivity (Sequencing) Specificity (Sequencing) Assays Hain, PSQ, MDDR INH ahpc promoter PSQ INH fabg1 PSQ, MDDR Rifampin (RIF) rpob Xpert, Hain, PSQ, MDDR Ethambutol (EMB) embb Hain, MDDR Pyrazinamide (PZA) pnca MDDR Fluoroquinolones gyra Hain, PSQ, MDDR Amikacin (AMK) rrs Hain, PSQ, MDDR Capreomycin (CAP) rrs tlya MDDR Lin, et al., Clin Lab Med Jun;34(2): doi: /j.cll Lin, et al., J Clin Micro. 2014;52:475 16
18 Types of mutations Silent (synonymous) Nucleic acid change No amino acid change Not associated with drug resistance generally 514 (TTC TTT) mutation in rpob is the most common silent mutation Missense (nonsynonymous) Nucleic acid change Amino acid change Some are associated with resistance 17
19 Molecular Testing for Rifampin (rpob) Rifampin cornerstone of TB treatment Resistance requires a longer duration of therapy Rif resistance without INH resistance rare Rif resistance MDR
20 Xpert Probes: Coverage of rpob Codon # Most common silent mutation (514 TTT) Most common resistance mutation (531 TTG) Location of silent mutation Location of missense mutation

21 20
22 Steingart 2014 Cochrane Review ( 21 Library-Updated-Xpert-SR.pdf) Xpert Performance Rifampin Resistance Pooled median sensitivity: 95% (95% CrI: 90, 97) Pooled median specificity: 98% (95% CrI: 97, 99)
23 Number and Proportion MDR TB by Country/Region of Origin, CA Country/Region No. % PPV PPV (99% spec) (98% spec) Former Soviet Republics % 87% Laos % 72% Burma % 63% Japan % 61% India % 60% Guatemala % 60% Korea (N&S) % 59% Peru % 56% Ethiopia % 50% Philippines % 45% Vietnam % 40% China (incl Taiwan) % 37% United States % 28% Cambodia % 25% Mexico % 22% Countries with >20 cases tested for MDR 22
24 MDR TB Cases by Country/Region of Origin and Years in the US, CA Country/Region Total MDR TB cases 2 years in US No. (%) >2 years in US No. (%) All Countries (excl US)* (3.7) 71 (1.2) Former Soviet Republics 5 2 (33.3) 3 (8.6) Vietnam* 13 9 (7.9) 3 (0.4) China (incl Taiwan)* 7 5 (8.8) 2 (0.4) Philippines* 27 8 (4.0) 19 (1.4) Guatemala 5 1 (3.9) 4 (2.9) India 12 3 (3.3) 9 (3.2) All Other Countries 10 2 (1.1) 8 (0.9) Mexico 11 0 (0.0) 11 (0.7) Korea, North and South 7 0 (0.0) 7 (3.2) Laos 6 0 (0.0) 5 (4.6) * Difference is statistically significant 23
25 Number and % MDR among foreign-born TB patients in the U.S., Country of(top origin 15 Total countries) TB cases* No. % Ukraine Laos Peru Dominican Republic Ecuador Republic of Korea Burma / Myanmar India 2, Vietnam 2, China 1, Haiti Philippines 3, Ethiopia Guatemala Mexico 5, Source: Centers for Disease Control and Prevention, Division of Tuberculosis Elimination, National Tuberculosis Surveillance System, Bob Pratt 24
26 How to interpret results of molecular tests for resistance 25
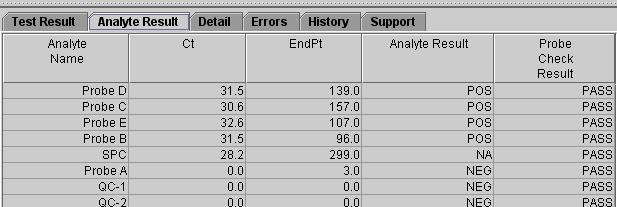
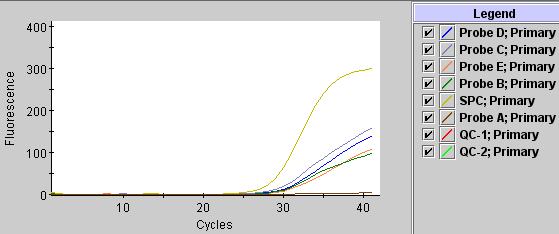
27 Case 1 70 yo asymptomatic man from India with abnormal preimmigration CXR, no TB history Domestic CXR with multifocal infiltrates Sputum smear positive x 3 Xpert positive: rifampin resistant What do you do next? Start MDR treatment Order pyrosequencing or MDDR Start RIPE Repeat Xpert on another specimen Start treatment for monorif resistance 26
28 Case 1 Treatment held; PSQ available within 2 days and clinically stable Pyrosequencing: katg mutation: INH R rpob 531TTG mutation: RIF R gyra (FQ): no mutations rrs (amikacin): no mutations What do you do next? Start MDR treatment Order MDDR Start RIPE Repeat Xpert on another specimen Order second line DSTs Cancel DSTs (already have molecular results) 27
29 Case 2 70 yo man from Mexico in US x 25 years with 4 weeks of cough, no TB history CXR with multifocal infiltrates Sputum smear positive x 3 Xpert positive, rifampin resistant What do you do next? Start MDR treatment Order pyrosequencing or MDDR Start RIPE Repeat Xpert on another specimen Start treatment for monorif resistance 28
30 Case 2 RIPE started PSQ: katg/inha: no mutation INH Sens rpob: 514TTT silent mutation: RIF Sens 29
31 How to interpret molecular test for resistance Put into clinical and epidemiologic context! Confirm non-sequencing tests (e.g., Xpert) with sequencing test Consider Rif resistance on Xpert to be MDR (not just rifampin monoresistant) Can usually treat based on sequencing test results; follow the growth based DST results 30
32 Limitations / Areas for Caution Molecular tests vs. DST discordance Undescribed mutations outside of loci in current molecular tests resistance Emerging resistance in mixed populations may not be detected Disputed mutations DSTs show susceptible but associated with clinical treatment failure 31
33 An example of an expanded regimen is: 1. I, R, E, Z, Moxi 2. I, R, E, Z, Strep 3. I, R, E, Z, Levo, Strep 4. I, R, E, Z, Moxi, Amik 5. All of the above 0% 0% 0% 0% 0%
 regimen for MDR: 4 first-line + FQ + injectable (+ consider additional second-line")
34 Basic steps: Choosing a regimen Decision: Begin empiric MDR regimen Ask for help: Expert consultation Empiric (expanded) regimen for MDR: 4 first-line + FQ + injectable (+ consider additional second-line drug)
35 How many drugs for MDR? Goal: 4-6 likely effective drugs optimally at least 5 Recent studies suggest better outcomes with at least 5 drugs Expert input: Consider more if extensive disease and/or resistance Four may be sufficient with limited disease and/or limited resistance [WHO 2011 at least 4 likely effective drugs ]
36 Building an Individualized Regimen for MDR-TB STEP 1 Begin with any First-line agents to which the isolate is susceptible Add a fluoroquinolone and an injectable drug based on susceptibilities Use any available First-line drugs Pyrazinamide Ethambutol* One of these Fluoroquinolones Levofloxacin Moxifloxacin One of these Injectable agents Amikacin Capreomycin Kanamycin 1 Streptomycin 2 1. Not available in U.S. 2. SM: use only if not previously used and if documented susceptibility *WHO 2016 Guidelines put EMB in a lower group
37 Building a Regimen for MDR-TB (2) STEP 2 Add second-line drugs until you have 4-6 drugs (optimally at least 5) to which the isolate is susceptible (and preferably which have not been used to treat the patient previously) Pick one or more of these Oral second-line drugs Cycloserine Ethionamide Linezolid PAS* * 2016 WHO Guidelines put PAS lower
38 Building a Regimen for MDR-TB (3) STEP 3 If there are not 4-6 drugs available in the above categories, consider third-line drugs in consultation with an MDR-TB expert Bedaquiline Delamanid 4 Clofazimine* Imipenem Consider use of these Third-line drugs Meropenem/ Clavulanate Amoxicillin/ Clavulanate High-dose INH* 4. Awaiting FDA approval *WHO Guidelines have these higher
39 Step 1 Step 2 Step 3 Step 4 Building a Treatment Regimen Group A (one) Levofloxacin Gatifloxaxin Group B (one) Kanamycin Amikacin WHO 2016 Update Moxifloxacin Capreomycin Group C (two) Ethionamide/Prothionamide Cycloserine/Terizidone Clofazimine Linezolid Group D1 Pyrazinamide (include) Ethambutol* High-dose INH* Group D2 Bedaquiline Delamanid Group D3 Imipemen/Meropenem Amoxacillin/Clavulanate P-aminosalicylic acid 5 drugs, incl. PZA Demoted: PAS and EMB Promoted: Clofazimine, linezolid, INH high-dose
40 Bangladesh Regimen Short course treatment for MDR Recommended by WHO 2016 Observational data impressive (85-90% cure) RCTs ongoing Contraindications: resistance to any drug in regimen, extrapulmonary disease, pregnancy Should this be used in the U.S.? WHO,
41 Short(er) Course Regimen for MDR-TB Initial Phase (7 drugs) Continuation Phase (4 drugs) Moxifloxacin* Ethambutol Pyrazinamide Clofazimine Prothionamide Isoniazid* Kanamycin *High dose months
42 Eligibility for Short Course Regimen in California, n=171 with full DSTs H (any) H (high) H (low) Drug resistance (%) Eligible for shorter regimen Alternate eligibility for shorter regimen * R SLID 1 FQ 2 Eto E Z No.(%) No.(%) (15%) 35(21%) *allow for resistance to ETO if INH resistance is low-level Clofazimine not tested Analysis by Phil Lowenthal
43 Barriers to Implementing Clofazimine availability Full DST info few qualify by strict criteria How to substitute for adverse events or resistance Why does it work?
 Avoid drugs used previously Side")
44 Other considerations when choosing drugs Beyond susceptibility results, consider: Cross-resistance (table page 76) Avoid drugs used previously Side effect profile
45 Treatment Duration Survival Guide Expert consensus for U.S. Setting: Use culture conversion to guide minimum duration Intensive phase: at least 6 mo beyond culture conversion for use of injectable agent Total duration: at least 18 months beyond culture conversion WHO 2011 and 2016 Guideline: Intensive phase at least 8 months Total duration at least 20 months (if no prior rx for MDR; if prior MDR rx at least 24 months) 2003 ATS/CDC/IDSA guidelines: mo

46 Treatment regimens Suggestions based on pattern of drug resistance Pre-XDR and XDR recommend longer duration (at least 24 mo. post culture conversion) Chapter 4, page 80

47 Medication Fact Sheets Drug class/trade name Activity against TB Cross-resistance Dose (adult, peds, renal) Route of administration Preparation/storage Pharmacokinetics Oral absorbtion/metabolism CSF penetration Special circumstances Adverse reactions/contraindications Monitoring Costs/patient education
48 Regimens for XDR-TB Treatment choices are limited Bedaquiline, Linezolid and any remaining injectable become the mainstay of treatment Add whatever oral medications are left to which there is in vitro susceptibility Surgery if disease is localized Nearly all patients are treatable and curable
49 Surgery? No hard and fast rules; WHO: Surgery may be used Metaanalysis suggests success Consider if: Very extensive resistance Residual large cavity Predominantly one-sided disease Previous MDR treatment failure Marrone MT, et al. Surgical interventions for drug-resistant tuberculosis: a systematic review and meta-analysis. Int J Tuberc Lung Dis 2013;17(1):6-16.
50 MDR-TB Clinical Case Management Seek consultation with MDR-TB expert as soon as multidrug resistance known Use daily DOT throughout entire treatment course No intermittent therapy for drug resistance!! Use case management tools (drug-o-gram) to follow serial changes in drugs, bacteriology, CXR, toxicities Optimize management of underlying medical conditions and nutritional status (i.e. diabetes)
51
52
53 Cycloserine: Therapeutic Drug Monitoring absorption highly variable therapeutic and toxic levels are very close drug levels are highly recommended Draw 2 hours after dose Injectables: if renal compromise, significantly over or under weight, or elderly Some experts recommend obtaining levels routinely peak and/or trough levels
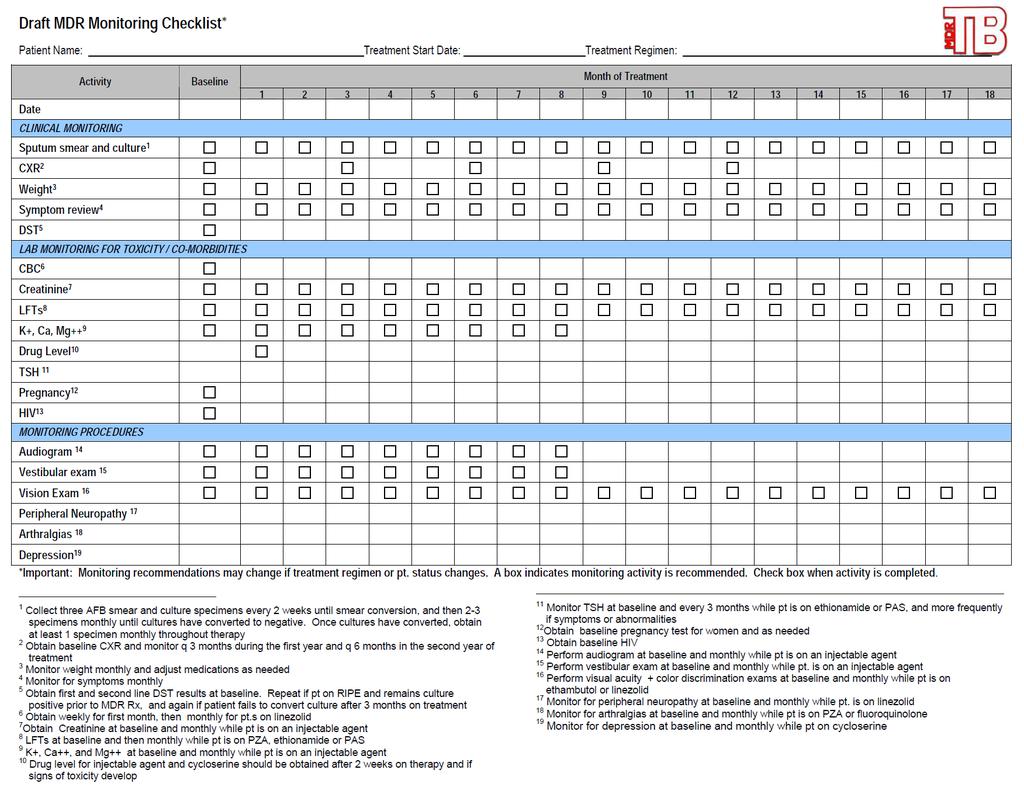
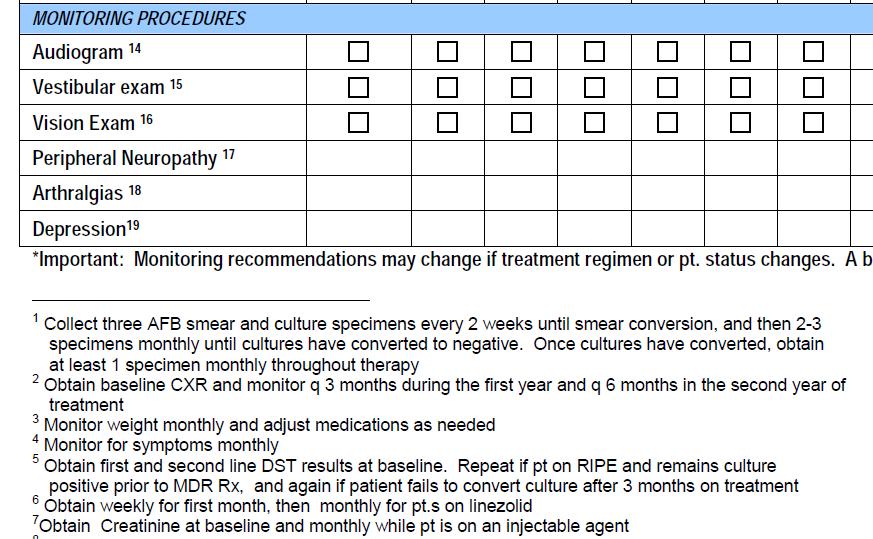
54 Recommended MDR-TB Monitoring for Efficacy Collect sputum monthly throughout End-of-treatment sputum for smear and culture CXR quarterly and at end of treatment Monitor for 2 years after treatment Quarterly: first year, Q6 months: second year)
55 MDR-TB Laboratory Monitoring Second-line drug susceptibilities Repeat susceptibilities on cultures that remain positive after 2-3 months Repeat susceptibility for EMB/PZA if susceptible at baseline and 4 weeks of first-line treatment
56
57
58 California MDR Outcomes All MDR Cases n=195 Off Treatment 132 On Treatment 52 Moved 11 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% Failure (micro)=1 Death=4 Failure(ADR)=4 Default/LTFU=5 Off Treatment n=132 Cure/Complete 118 0% 20% 40% 60% 80% 100% Includes consult and nonconsult cases by year of MDR Service notification MDR by MDR Service definition: includes molecular susceptibility tests and clinical cases
59 Common Side Effects G.I. complaints Hearing loss, vestibular toxicity Renal insufficiency/electrolyte Abn Hepatotoxicity Peripheral neuropathy Neuropsychiatric: depression, agitation, psychosis, difficulty concentrating, insomnia Rash Visual changes Hypothyroidism Headache Ethionamide, PAS, Quinolones, Clofazimine, Rifabutin, Linezolid Injectables Injectables PZA, PAS, Rifabutin, Ethionamide, Quinolones Linezolid, INH, Quinolones, Ethionamide, Cycloserine Cycloserine, Quinolones, Ethionamide All EMB, Rifabutin, Linezolid Ethionamide, PAS Quinolones, Cycloserine, Ethionamide, EMB Chapter 9
60 Prevention Preventing acquired drug resistance DOT and daily therapy as appropriate Preventing transmission of MDR-TB to contacts Effective treatment, Isolation until noninfectious Preventing progression to active disease in infected MDR- TB contacts MDR LTBI treatment and monitoring
61 Isolation (CDPH/CTCA Guidelines) Patients with pulmonary MDR-TB should be considered infectious until: An appropriate MDR regimen has been initiated and tolerated for 2 weeks AND A favorable clinical response has occurred AND 3 consecutive sputum smears are documented AFB negative Guidelines for the Assessment of Tuberculosis Patient Infectiousness and Placement into High and Lower Risk Settings, 2009:
62 Preventing Progression to Active TB Little published data on LTBI treatment for MDR-TB contacts; No randomized trials CDC guidance last in 1992 Contact investigation and management principles same as drug susceptible: Drug resistant TB is not more infectious, but duration can be longer and consequences are greater Consider infectiousness of index case, duration/intensity of contact, immune status of contact, LTBI test results Rule out active disease prior to starting LTBI treatment
63 Treatment Regimens for MDR-TB Contacts FQ monotherapy FQ + EMB Monitor for 2 years only acceptable FQ + PZA very poorly tolerated PZA + EMB Other combinations? Duration?
64 Fluoroquinolones for MDR Contacts Published data from 2 MDR outbreaks in Chuuk: 104 of 119 received LTBI treatment x 12 months Adults: MFX + EMB (n=24) or MFX/LFX alone (n=51) Children: LFX + EMB (N=17) or LFX + Ethionamide (n=12) 11 stopped early; 6 received >6 mos 0 cases in treated vs 3 among 15 refused (36 mo f/u) Bamrah et al, Int J Tuberculosis Lung Dis
65 Resources 64
66 Resources: RTMCCs Francis J. Curry International Tuberculosis Center NOTB or Heartland National Tuberculosis Center TEX-LUNG or New Jersey Medical School Global Tuberculosis Institute TB-DOCS or Southeastern National Tuberculosis Center TB-INFO or Mayo Clinic Center for Tuberculosis
67 MDR Resources Partners in Health Guide (2013): WHO MDR Guides: Companion Guide (2014): Guideline (2016): International Union Guide (2013): CDC Bedaquiline Guideline (2013): 66

68 California Resources MDR-TB Service Provides clinical consultation, case management, CI assistance CA Microbial Diseases Lab pyrosequencing for drug resistance phenotypic DST for first-line drugs and amikacin, moxifloxacin, capreomycin, and ethionamide
 Lisa True Janice Westenhouse Jenny Flood Neha Shah Kristen Wendorf Christy Pak (Ret) Not pictured: Shereen")
69 Acknowledgments Lisa True Lisa Chen Neha Shah Grace Lin Gisela Schecter Leslie Henry Phil Lowenthal Pennan Barry Gayle Schack (Ret) Lisa True Janice Westenhouse Jenny Flood Neha Shah Kristen Wendorf Christy Pak (Ret) Not pictured: Shereen Katrak 68
Multidrug resistant Tuberculosis
 Multidrug resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive October 018 Objectives
Multidrug resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive October 018 Objectives
Practical. Walk through New Survival Guide
 Many faces of TB: Drug resistant it ttbs Survival lgid Guide v3 P B L Ch G Sh t L T P. Barry, L. Chen, G. Schecter, L. True Curry International TB Center/CTCA April 20, 2016 Real case Practical Walk through
Many faces of TB: Drug resistant it ttbs Survival lgid Guide v3 P B L Ch G Sh t L T P. Barry, L. Chen, G. Schecter, L. True Curry International TB Center/CTCA April 20, 2016 Real case Practical Walk through
Clinical Management : DR-TB
 Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
MDR TB AND CASE STUDIES
 MDR TB AND CASE STUDIES Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Seattle, CITC Clinical Intensive June 15, 2018 Slide
MDR TB AND CASE STUDIES Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Seattle, CITC Clinical Intensive June 15, 2018 Slide
Multidrug-resistant Tuberculosis. Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership
 Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
Challenges to treat MDR TB
 Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
MDR/XDR TB. Barbara Seaworth, MD, FIDSA, FACP October 27, TB Intensive October 24 27, 2017 San Antonio, TX
 MDR/XDR TB Barbara Seaworth, MD, FIDSA, FACP October 27, 2017 TB Intensive October 24 27, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Barbara Seaworth, MD, FIDSA, FACP, has the following disclosures
MDR/XDR TB Barbara Seaworth, MD, FIDSA, FACP October 27, 2017 TB Intensive October 24 27, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Barbara Seaworth, MD, FIDSA, FACP, has the following disclosures
TB Intensive Houston, Texas. Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD
 TB Barbara Seaworth, MD") TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
TB Grand Rounds. MDR-TB: Management of Adverse Drug Reactions. Reynard J. McDonald, M.D. September 18, Patient History
 TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S.
 Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
Drug-resistant TB therapy: the future is now
 Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 MDR/XDR TB Barbara J. Seaworth, MD October 16, 2013 Barbara J. Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
TB Intensive Houston, Texas October 15-17, 2013 MDR/XDR TB Barbara J. Seaworth, MD October 16, 2013 Barbara J. Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
Drug resistant TB: Lisa Chen, MD University of California, San Francisco Curry Interna:onal TB Center Sea=le, June 2016
 Drug resistant TB: Lisa Chen, MD University of California, San Francisco Curry Interna:onal TB Center Sea=le, June 2016 Drug- Resistant TB: De1initions Mono- resistant: Resistance to a single drug Poly-
Drug resistant TB: Lisa Chen, MD University of California, San Francisco Curry Interna:onal TB Center Sea=le, June 2016 Drug- Resistant TB: De1initions Mono- resistant: Resistance to a single drug Poly-
Treatment of Multidrug-resistant Tuberculosis (MDR-TB)
") Treatment of Multidrug-resistant Tuberculosis (MDR-TB) 2006 2008 2011 2013 2014 2016 2019 Charles L. Daley, MD National Jewish Health University of Colorado Disclosures Research grant Insmed: Phase II
Treatment of Multidrug-resistant Tuberculosis (MDR-TB) 2006 2008 2011 2013 2014 2016 2019 Charles L. Daley, MD National Jewish Health University of Colorado Disclosures Research grant Insmed: Phase II
THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION
 1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
Treatment of Drug Resistant TB
 Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
Drug resistant TB: The role of the laboratory
 Drug resistant TB: The role of the laboratory 26 Oct 2012 Andrew Whitelaw NHSLS / UCT TB lab functions: Outline Resistance testing Genotypic Phenotypic Which tests are done when, and why Reporting of
Drug resistant TB: The role of the laboratory 26 Oct 2012 Andrew Whitelaw NHSLS / UCT TB lab functions: Outline Resistance testing Genotypic Phenotypic Which tests are done when, and why Reporting of
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas May 6 9, 2014 MDR/XDR TB Barbara Seaworth, MD May 9, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial relationships
TB Intensive San Antonio, Texas May 6 9, 2014 MDR/XDR TB Barbara Seaworth, MD May 9, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial relationships
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing - PRELIMINARY -
 Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2
 1 MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2 1 India has the highest TB burden in the world 3 4 2 5 M. tuberculosis Resistance
1 MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2 1 India has the highest TB burden in the world 3 4 2 5 M. tuberculosis Resistance
Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study
 Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study Julie Tans-Kersten, MS, BS-MT (ASCP) Tuberculosis Laboratory Program Coordinator Wisconsin
Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study Julie Tans-Kersten, MS, BS-MT (ASCP) Tuberculosis Laboratory Program Coordinator Wisconsin
DR-TB PATIENT IDENTITY CARD
 Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
XDR TB: The Laboratory s Dilemma vs The Clinician s Dilemma
 XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
Multi-Drug and Extensively Drug Resistant Tuberculosis
 Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
Management of MDR and XDR TB Prof. Martin Boeree
 Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
Treatment of MDR/XDR-TB. Short course chemotherapy for MDR-TB: practical issues. CHIANG Chen-Yuan MD, MPH, DrPhilos
 Treatment of MDR/XDR-TB Short course chemotherapy for MDR-TB: practical issues CHIANG Chen-Yuan MD, MPH, DrPhilos Treatment strategies for MDR-TB Standardized treatment: drug resistance survey data from
Treatment of MDR/XDR-TB Short course chemotherapy for MDR-TB: practical issues CHIANG Chen-Yuan MD, MPH, DrPhilos Treatment strategies for MDR-TB Standardized treatment: drug resistance survey data from
CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP)
 Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP)") CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP) Beverly Metchock, DrPH, D(ABMM) Mycobacteriology Laboratory Branch/Division
CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP) Beverly Metchock, DrPH, D(ABMM) Mycobacteriology Laboratory Branch/Division
MDR treatment. Shanghai, May 2012 Arnaud Trébucq The Union
 MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
Drug Resistant Tuberculosis:
 Drug Resistant Tuberculosis: Pearls and other Considerations John W. Wilson, MD Associate Professor of Medicine Division of Infectious Diseases Mayo Clinic, Rochester MN Mayo Clinic Center for Tuberculosis
Drug Resistant Tuberculosis: Pearls and other Considerations John W. Wilson, MD Associate Professor of Medicine Division of Infectious Diseases Mayo Clinic, Rochester MN Mayo Clinic Center for Tuberculosis
Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool)
") Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool) DOTS + and LTBI New drugs for TB and the challenge of resistance talk plan 1. Epidemiology 2. Treatment 3. The MDRTB
Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool) DOTS + and LTBI New drugs for TB and the challenge of resistance talk plan 1. Epidemiology 2. Treatment 3. The MDRTB
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France
 Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
TB New Drugs, Shorter Courses
 TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
MDR-TB drugs per WHO guidelines
 New antituberculous agents for drug-resistant resistant TB Symposium Belgian Society of Infectiology and Clinical Microbiology November 9 Jens Van Roey, MD - Tibotec Definitions MDR-TB multidrug resistance
New antituberculous agents for drug-resistant resistant TB Symposium Belgian Society of Infectiology and Clinical Microbiology November 9 Jens Van Roey, MD - Tibotec Definitions MDR-TB multidrug resistance
The New England Journal of Medicine THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY
 THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY KEMAL TAHAOĞLU, M.D., TÜLAY TÖRÜN, M.D., TÜLIN SEVIM, M.D., GÜLIZ ATAÇ, M.D., ALTAN KIR, M.D., LEVENT KARASULU, M.D., IPEK ÖZMEN, M.D., AND NILÜFER
THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY KEMAL TAHAOĞLU, M.D., TÜLAY TÖRÜN, M.D., TÜLIN SEVIM, M.D., GÜLIZ ATAÇ, M.D., ALTAN KIR, M.D., LEVENT KARASULU, M.D., IPEK ÖZMEN, M.D., AND NILÜFER
Case 1 and Case 2. Case 1 3/23/2016
 Case 1 and Deidra D. Parrish, MD, MPH&TM Nashville Metro Public Health Dept TB Symposium March 30, 2016 Case 1 27 yo Indian woman came to the US to join her husband three months prior to clinic visit.
Case 1 and Deidra D. Parrish, MD, MPH&TM Nashville Metro Public Health Dept TB Symposium March 30, 2016 Case 1 27 yo Indian woman came to the US to join her husband three months prior to clinic visit.
University of Groningen. Tuberculosis and its sequelae Akkerman, Onno
 University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick
 Patrick") New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick Phillips Patrick.Phillips@ucsf.edu @PPJPhillips Outline Overview of regimen development strategies 1-3 year horizon: Ongoing phase
New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick Phillips Patrick.Phillips@ucsf.edu @PPJPhillips Outline Overview of regimen development strategies 1-3 year horizon: Ongoing phase
Linezolid: an effective, safe and cheap drug for patients failing multidrug-resistant tuberculosis treatment in India
 Eur Respir J 2012; 39: 956 962 DOI: 10.1183/09031936.00076811 CopyrightßERS 2012 Linezolid: an effective, safe and cheap drug for patients failing multidrug-resistant tuberculosis treatment in India R.
Eur Respir J 2012; 39: 956 962 DOI: 10.1183/09031936.00076811 CopyrightßERS 2012 Linezolid: an effective, safe and cheap drug for patients failing multidrug-resistant tuberculosis treatment in India R.
Introduction of Bedaquiline in the Philippines
 Introduction of Bedaquiline in the Philippines 24th PhilCAT Annual Convention Crown Plaza Hotel August 18,2107 Vivian S. Lofranco, MD., PHSAE National Clinical Coordinator, BDQ MDR-TB is highly contagious
Introduction of Bedaquiline in the Philippines 24th PhilCAT Annual Convention Crown Plaza Hotel August 18,2107 Vivian S. Lofranco, MD., PHSAE National Clinical Coordinator, BDQ MDR-TB is highly contagious
Quality of 2 nd line medicines for tuberculosis. Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products
 Quality of 2 nd line medicines for tuberculosis Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products Case studies in medicines for tuberculosis Outline: Statistics
Quality of 2 nd line medicines for tuberculosis Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products Case studies in medicines for tuberculosis Outline: Statistics
MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience
 MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience Dr Johan Van Wyk MB.Ch.B, M.Med (Clin Path) Clinical Pathologist ibhayi Region, Eastern Cape GWYNETH PALTROW SHAKESPEARE IN LOVE 1998 PORT
MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience Dr Johan Van Wyk MB.Ch.B, M.Med (Clin Path) Clinical Pathologist ibhayi Region, Eastern Cape GWYNETH PALTROW SHAKESPEARE IN LOVE 1998 PORT
Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB)
") Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB) Session: Fanning the Flames of HIV and TB Cointeraction SA AIDS Conference-Durban ICC 13-15 June 2017
Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB) Session: Fanning the Flames of HIV and TB Cointeraction SA AIDS Conference-Durban ICC 13-15 June 2017
Tuberculosis in 2017: Searching for new solutions in the face of new challenges
 Tuberculosis in 2017: Searching for new solutions in the face of new challenges 6th TB Symposium Ministry of Health of the Republic of Belarus, Republican Scientific and Practical Center for Pulmonology
Tuberculosis in 2017: Searching for new solutions in the face of new challenges 6th TB Symposium Ministry of Health of the Republic of Belarus, Republican Scientific and Practical Center for Pulmonology
Treatment of Nontuberculous Mycobacterial Infections (NTM)
") Treatment of Nontuberculous Mycobacterial Infections (NTM) Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory
Treatment of Nontuberculous Mycobacterial Infections (NTM) Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory
ECHO: Management of URIs. Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018
 ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 29 October 2014 GRANUPAS, gastro-resistant granules 30 sachets with a calibrated measuring spoon (CIP: 34009 278 801
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 29 October 2014 GRANUPAS, gastro-resistant granules 30 sachets with a calibrated measuring spoon (CIP: 34009 278 801
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Dr Sharanjit Dhoot. Chelsea and Westminster Hospital, London. 18 th Annual Conference of the British HIV Association (BHIVA)
") 18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
Risk Factors for Poor Outcomes in Patients with Multi-Drug Resistant Tuberculosis in South Korea
 Hanyang Med Rev 2016;36:262-268 https://doi.org/10.7599/hmr.2016.36.4.262 pissn 1738-429X eissn 2234-4446 Original Article Risk Factors for Poor Outcomes in Patients with Multi-Drug Resistant Tuberculosis
Hanyang Med Rev 2016;36:262-268 https://doi.org/10.7599/hmr.2016.36.4.262 pissn 1738-429X eissn 2234-4446 Original Article Risk Factors for Poor Outcomes in Patients with Multi-Drug Resistant Tuberculosis
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Dr Dean Shuey Team Leader Health Services Development WPRO. World Health Day Antimicrobial Resistance: The Global and Regional Situation
 Dr Dean Shuey Team Leader Health Services Development WPRO World Health Day 2011 Antimicrobial Resistance: The Global and Regional Situation 2 7 April 2011 World Health Day No action today, no cure tomorrow
Dr Dean Shuey Team Leader Health Services Development WPRO World Health Day 2011 Antimicrobial Resistance: The Global and Regional Situation 2 7 April 2011 World Health Day No action today, no cure tomorrow
Section 6.2.4: Antituberculosis Medicines Application for moving streptomycin to complementary list
 Section 6.2.4: Antituberculosis Medicines Application for moving streptomycin to complementary list Stop TB Department World Health Organization Summary According to the recent guideline published in 2010
Section 6.2.4: Antituberculosis Medicines Application for moving streptomycin to complementary list Stop TB Department World Health Organization Summary According to the recent guideline published in 2010
Creating a global community for clinical drug repurposing and development. Leonard Sacks Center for drug evaluation and research FDA
 Creating a global community for clinical drug repurposing and development Leonard Sacks Center for drug evaluation and research FDA Neglected tropical diseases 1) Repurposing and developing new drugs 2)
Creating a global community for clinical drug repurposing and development Leonard Sacks Center for drug evaluation and research FDA Neglected tropical diseases 1) Repurposing and developing new drugs 2)
In Vitro Activities of Linezolid against Clinical Isolates of ACCEPTED
 AAC Accepts, published online ahead of print on April 00 Antimicrob. Agents Chemother. doi:./aac.001-0 Copyright 00, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
AAC Accepts, published online ahead of print on April 00 Antimicrob. Agents Chemother. doi:./aac.001-0 Copyright 00, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS
 INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS 1 Research Associate, Drug Utilisation Research Unit, Nelson Mandela University 2 Human Sciences Research Council,
INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS 1 Research Associate, Drug Utilisation Research Unit, Nelson Mandela University 2 Human Sciences Research Council,
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Title: Resistance to fluoroquinolones and second line injectable drugs: impact on MDR TB outcomes
 ERJ Express. Published on October 25, 2012 as doi: 10.1183/09031936.00134712 Title: Resistance to fluoroquinolones and second line injectable drugs: impact on MDR TB outcomes Authors: D. Falzon, N. Gandhi,
ERJ Express. Published on October 25, 2012 as doi: 10.1183/09031936.00134712 Title: Resistance to fluoroquinolones and second line injectable drugs: impact on MDR TB outcomes Authors: D. Falzon, N. Gandhi,
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
Curricular Components for Infectious Diseases EPA
 Curricular Components for Infectious Diseases EPA 1. EPA Title Promoting antimicrobial stewardship based on microbiological principles 2. Description of the A key role for subspecialists is to utilize
Curricular Components for Infectious Diseases EPA 1. EPA Title Promoting antimicrobial stewardship based on microbiological principles 2. Description of the A key role for subspecialists is to utilize
Extensively Drug-Resistant Tuberculosis in South Korea: Risk Factors and Treatment Outcomes among Patients at a Tertiary Referral Hospital
 MAJOR ARTICLE Extensively Drug-Resistant Tuberculosis in South Korea: Risk Factors and Treatment Outcomes among Patients at a Tertiary Referral Hospital Christie Y. Jeon, 1,2,a Soo Hee Hwang, 5,a Jin Hong
MAJOR ARTICLE Extensively Drug-Resistant Tuberculosis in South Korea: Risk Factors and Treatment Outcomes among Patients at a Tertiary Referral Hospital Christie Y. Jeon, 1,2,a Soo Hee Hwang, 5,a Jin Hong
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Current Status of Fluoroquinolone Use for Treatment of Tuberculosis in a Tertiary Care Hospital in Korea
 ORIGINAL ARTICLE https://doi.org/10.4046/trd.2017.80.2.143 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2017;80:143-152 Current Status of Fluoroquinolone Use for Treatment of Tuberculosis
ORIGINAL ARTICLE https://doi.org/10.4046/trd.2017.80.2.143 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2017;80:143-152 Current Status of Fluoroquinolone Use for Treatment of Tuberculosis
Treatment of Slowly Growing NTM Infections
 Treatment of Slowly Growing NTM Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory Committee Insmed
Treatment of Slowly Growing NTM Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory Committee Insmed
Tb : Recent recommendation. Dr.Ketan Shah
 Tb : Recent recommendation Dr.Ketan Shah Tbc : Clinician If you think It is easy to diagnose : u r not good clinician It is difficult to diagnose :U r not alone doctor to think this 6/22/2015 Ketan Shah
Tb : Recent recommendation Dr.Ketan Shah Tbc : Clinician If you think It is easy to diagnose : u r not good clinician It is difficult to diagnose :U r not alone doctor to think this 6/22/2015 Ketan Shah
Antimicrobial Stewardship in the Hospital Setting
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 12 Antimicrobial Stewardship in the Hospital Setting Authors Dan Markley, DO, MPH, Amy L. Pakyz, PharmD, PhD, Michael Stevens, MD, MPH Chapter Editor
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 12 Antimicrobial Stewardship in the Hospital Setting Authors Dan Markley, DO, MPH, Amy L. Pakyz, PharmD, PhD, Michael Stevens, MD, MPH Chapter Editor
11/22/2016. Antimicrobial Stewardship Update Disclosures. Outline. No conflicts of interest to disclose
 Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Antimicrobial stewardship
 Antimicrobial stewardship Magali Dodemont, Pharm. with the support of Wallonie-Bruxelles International WHY IMPLEMENT ANTIMICROBIAL STEWARDSHIP IN HOSPITALS? Optimization of antimicrobial use To limit the
Antimicrobial stewardship Magali Dodemont, Pharm. with the support of Wallonie-Bruxelles International WHY IMPLEMENT ANTIMICROBIAL STEWARDSHIP IN HOSPITALS? Optimization of antimicrobial use To limit the
Council Conclusions on Antimicrobial Resistance (AMR) 2876th EMPLOYMENT, SOCIAL POLICY, HEALTH AND CONSUMER AFFAIRS Council meeting
 2876th EMPLOYMENT, SOCIAL POLICY, HEALTH AND CONSUMER AFFAIRS Council meeting") COUNCIL OF THE EUROPEAN UNION Council Conclusions on Antimicrobial Resistance (AMR) 2876th EMPLOYMT, SOCIAL POLICY, HEALTH AND CONSUMER AFFAIRS Council meeting Luxembourg, 10 June 2008 The Council adopted
COUNCIL OF THE EUROPEAN UNION Council Conclusions on Antimicrobial Resistance (AMR) 2876th EMPLOYMT, SOCIAL POLICY, HEALTH AND CONSUMER AFFAIRS Council meeting Luxembourg, 10 June 2008 The Council adopted
The Threat of Multidrug Resistant Neisseria gonorrhoeae
 The Threat of Multidrug Resistant Neisseria gonorrhoeae Peel Public Health Symposium Sex, Drugs, and. Vanessa Allen, MD MPH October 16, 2012 The threat of multidrug resistant gonorrhea "We're sitting on
The Threat of Multidrug Resistant Neisseria gonorrhoeae Peel Public Health Symposium Sex, Drugs, and. Vanessa Allen, MD MPH October 16, 2012 The threat of multidrug resistant gonorrhea "We're sitting on
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days
 Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources
 Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources Andrew Hunter, PharmD, BCPS Infectious Diseases Clinical Pharmacy Specialist Michael E. DeBakey VA Medical Center Andrew.hunter@va.gov
Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources Andrew Hunter, PharmD, BCPS Infectious Diseases Clinical Pharmacy Specialist Michael E. DeBakey VA Medical Center Andrew.hunter@va.gov
CLINICAL USE OF AMINOGLYCOSIDES AND FLUOROQUINOLONES THE AMINOGLYCOSIDES:
 CLINICAL USE OF AMINOGLYCOSIDES AND FLUOROQUINOLONES Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu THE AMINOGLYCOSIDES: 1944-1975 Drug
CLINICAL USE OF AMINOGLYCOSIDES AND FLUOROQUINOLONES Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu THE AMINOGLYCOSIDES: 1944-1975 Drug
New antituberculosis drugs and regimens
 New antituberculosis drugs: from clinical trial to programmatic use Gina Gualano, 1 Susanna Capone, 2 Alberto Matteelli, 2 Fabrizio Palmieri 1 1 Respiratory Infectious Diseases Unit, National Institute
New antituberculosis drugs: from clinical trial to programmatic use Gina Gualano, 1 Susanna Capone, 2 Alberto Matteelli, 2 Fabrizio Palmieri 1 1 Respiratory Infectious Diseases Unit, National Institute
Critical Appraisal Topic. Antibiotic Duration in Acute Otitis Media in Children. Carissa Schatz, BSN, RN, FNP-s. University of Mary
 Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
The challenge of managing extensively drug-resistant tuberculosis at a referral hospital in the state of São Paulo, Brazil: a report of three cases
 J Bras Pneumol. 2015;41(6):554-559 http://dx.doi.org/10.1590/s1806-37562015000000299 CASE REPORT The challenge of managing extensively drug-resistant tuberculosis at a referral hospital in the state of
J Bras Pneumol. 2015;41(6):554-559 http://dx.doi.org/10.1590/s1806-37562015000000299 CASE REPORT The challenge of managing extensively drug-resistant tuberculosis at a referral hospital in the state of
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
DATA COLLECTION SECTION BY FRONTLINE TEAM. Patient Identifier/ Medical Record number (for facility use only)
") Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali. Lec 1
 Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP)
") IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
Global response to antibiotic access and resistance: Stuart B. Levy, M.D. Tufts University School of Medicine Alliance for Prudent Use of Antibiotics
 Global response to antibiotic access and resistance: Stuart B. Levy, M.D. Tufts University School of Medicine Alliance for Prudent Use of Antibiotics Established in 1981 APUA s Mission To improve control
Global response to antibiotic access and resistance: Stuart B. Levy, M.D. Tufts University School of Medicine Alliance for Prudent Use of Antibiotics Established in 1981 APUA s Mission To improve control
Chapter 51. Clinical Use of Antimicrobial Agents
 Chapter 51 Clinical Use of Antimicrobial Agents History of antimicrobial therapy Early 17 th century Cinchona bark was used as an important historical remedy against malaria. 1909 Paul Ehrlich sought a
Chapter 51 Clinical Use of Antimicrobial Agents History of antimicrobial therapy Early 17 th century Cinchona bark was used as an important historical remedy against malaria. 1909 Paul Ehrlich sought a
GUIDE TO INFECTION CONTROL IN THE HOSPITAL. Antibiotic Resistance
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 4: Antibiotic Resistance Author M.P. Stevens, MD, MPH S. Mehtar, MD R.P. Wenzel, MD, MSc Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 4: Antibiotic Resistance Author M.P. Stevens, MD, MPH S. Mehtar, MD R.P. Wenzel, MD, MSc Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
Measure Information Form
 Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Antibiotic Stewardship in the Neonatal Intensive Care Unit. Objectives. Background 4/20/2017. Natasha Nakra, MD April 28, 2017
 Antibiotic Stewardship in the Neonatal Intensive Care Unit Natasha Nakra, MD April 28, 2017 Objectives 1. Describe antibiotic use in the NICU 2. Explain the role of antibiotic stewardship in the NICU 3.
Antibiotic Stewardship in the Neonatal Intensive Care Unit Natasha Nakra, MD April 28, 2017 Objectives 1. Describe antibiotic use in the NICU 2. Explain the role of antibiotic stewardship in the NICU 3.
Antimicrobial Stewardship 101
 Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
Objectives 4/26/2017. Co-Investigators Sadie Giuliani, PharmD, BCPS Claude Tonnerre, MD Jayme Hartzell, PharmD, MS, BCPS
 IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
Antimicrobial Susceptibility Patterns of Salmonella Typhi From Kigali,
 In the name of God Shiraz E-Medical Journal Vol. 11, No. 3, July 2010 http://semj.sums.ac.ir/vol11/jul2010/88030.htm Antimicrobial Susceptibility Patterns of Salmonella Typhi From Kigali, Rwanda. Ashok
In the name of God Shiraz E-Medical Journal Vol. 11, No. 3, July 2010 http://semj.sums.ac.ir/vol11/jul2010/88030.htm Antimicrobial Susceptibility Patterns of Salmonella Typhi From Kigali, Rwanda. Ashok
Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring. Janis Chan Pharmacist, UCH 2008
 and their Monitoring. Janis Chan Pharmacist, UCH 2008") Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring Janis Chan Pharmacist, UCH 25-4-2008 2008 Aminoglycosides (AG) 1. Gentamicin 2. Amikacin 3. Streptomycin 4. Neomycin
Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring Janis Chan Pharmacist, UCH 25-4-2008 2008 Aminoglycosides (AG) 1. Gentamicin 2. Amikacin 3. Streptomycin 4. Neomycin
Antibiotic stewardship in long term care
 Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Impact of Antimicrobial Stewardship Program
 Impact of Antimicrobial Stewardship Program Ripal Joshi, Pharm.D. AAHIVP Tampa General Hospital January 28, 2016 Objectives Provide an overview on antimicrobial stewardship programs (ASP) Describe the
Impact of Antimicrobial Stewardship Program Ripal Joshi, Pharm.D. AAHIVP Tampa General Hospital January 28, 2016 Objectives Provide an overview on antimicrobial stewardship programs (ASP) Describe the
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings
 Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings Jasmanda H. Wu, Ph.D., 1 David H. Howard, Ph.D., 2 John E. McGowan, Jr.,
Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings Jasmanda H. Wu, Ph.D., 1 David H. Howard, Ph.D., 2 John E. McGowan, Jr.,
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens
 The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
Period of study: 12 Nov 2002 to 08 Apr 2004 (first subject s first visit to last subject s last visit)
") Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Cost high. acceptable. worst. best. acceptable. Cost low
 Key words I Effect low worst acceptable Cost high Cost low acceptable best Effect high Fig. 1. Cost-Effectiveness. The best case is low cost and high efficacy. The acceptable cases are low cost and efficacy
Key words I Effect low worst acceptable Cost high Cost low acceptable best Effect high Fig. 1. Cost-Effectiveness. The best case is low cost and high efficacy. The acceptable cases are low cost and efficacy
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings. Carlos Reyes Sacin, MD, AAHIVS
 Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Outline. Antimicrobial resistance. Antimicrobial resistance in gram negative bacilli. % susceptibility 7/11/2010
 Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities
 Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities Introduction As the problem of antibiotic resistance continues to worsen in all healthcare setting, we
Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities Introduction As the problem of antibiotic resistance continues to worsen in all healthcare setting, we