Treatment of MDR/XDR-TB. Short course chemotherapy for MDR-TB: practical issues. CHIANG Chen-Yuan MD, MPH, DrPhilos
|
|
|
- Dortha Brown
- 5 years ago
- Views:
Transcription
1 Treatment of MDR/XDR-TB Short course chemotherapy for MDR-TB: practical issues CHIANG Chen-Yuan MD, MPH, DrPhilos
2 Treatment strategies for MDR-TB Standardized treatment: drug resistance survey data from representative patient populations are used to base regimen design in the absence of individual drug susceptibility testing result. Individualized treatment: Each regimen is designed based on the patient s past history of TB treatment and individual DST results.
3 Treatment of drug-resistant tuberculosis...the selection of anti-tb agents is based upon the history of previous therapy and the results of reliable DST. ATS. A Statement by the Committee on Therapy. Treatment Drug- Resistant TB. Am Rev Respir Dis 1966;94:125-7
4 Standardized treatment for MDR-TB much feasible under program condition for MDR-TB patients who has not been treated with second line drugs before, especially in settings where second-line drugs have not yet been widely used But, an inadequately designed standardized regimen not well matched to the general susceptibility pattern may perform poorly. Chiang C-Y, et al. Int J Tuberc Lung Dis 2010;14:
5 Essential components in individualized treatment for MDR-TB Ensure quality of drug susceptibility testing (DST). Short turn around time of DST (otherwise, the pattern of drug resistance may change). Detail history of previously anti-tuberculosis treatment, especially previous treatment with second line anti-tuberculosis drugs Well trained in interpreting DST results Well trained in designing a MDR-TB regimen Chiang C-Y, et al. Int J Tuberc Lung Dis 2010;14:
6 MDR-TB patient previously treated with second line drugs Individualized treatment is usually applied for MDR- TB patients previously treated with second-line drugs, taking into account history of drug use and quality assured drug susceptibility testing results Standardized approach might be feasible if rapid DST of fluoroquinolone and second line injectables is available
7 Previous WHO recommendations, 2008 should consist of at least 4 drugs with either certain or almost certain effectiveness, do not depend on DST in individual regimen design for ethambutol, pyrazinamide, and Group 4 and 5 drugs an injectable agent is used for a minimunm of 6 months and 4 months after culture conversion, the minimum duration of treatment is 18 months after culture conversion WHO/HTM/TB/ :1-247
8 MDR-TB: an Individual Patient Data (IPD) Meta-Analysis of 9153 patients three types of drug-exposure : 1. specific drugs administered 2. number of likely effective drugs used 3. duration of treatment regimen. PLoS Med 9(8): e doi: /journal.pmed
9 MDR-TB: an Individual Patient Data (IPD) Meta-Analysis of 9153 patients estimated odds of treatment success (defined as treatment cure or completion) compared to one of three alternate outcomes: [i] treatment failure and/or relapse; [ii] treatment failure, relapse and/or death; and [iii] treatment failure, relapse, death and/or default. PLoS Med 9(8): e doi: /journal.pmed
10 MDR-TB treatment regimens and patient outcomes: an Individual Patient Data (IPD) Meta-Analysis of 9153 patients Treatment success, compared to failure/relapse, was associted with use of: later generation quinolones ofloxacin ethionamide or prothionamide use of four or more likely effective drugs in the initial intensive phase three or more likely effective drugs in the continuation phase PLoS Med 9(8): e doi: /journal.pmed
11 MDR-TB treatment regimens and patient outcomes: an Individual Patient Data (IPD) Meta- Analysis of 9153 patients Among those who did not die, or default during treatment, the maximum odds of success was seen with duration of the initial intensive phase of months, and total treatment duration of months PLoS Med 9(8): e doi: /journal.pmed
12 3. Composition of second-line antituberculosis regimens 3.1 In the treatment of patients with MDR-TB, a fluoroquinolone should be used (strong recommendation, /very low quality evidence). 3.2 In the treatment of patients with MDR-TB, a latergeneration fluoroquinolone rather than an earlier-generation fluoroquinolone should be used (conditional recommendation, /very low quality evidence). 3.3 In the treatment of patients with MDR-TB, ethionamide (or prothionamide) should be used (strong recommendation, /very low quality evidence).
13 3. Composition of second-line antituberculosis regimens 3.4 In the treatment of patients with MDR-TB, four secondline anti-tuberculosis drugs likely to be effective (including a parenteral agent), as well as pyrazinamide, should be included in the intensive phase (conditional recommendation, /very low quality evidence). 3.5 In the treatment of patients with MDR-TB, regimens should include at least pyrazinamide, a fluoroquinolone, a parenteral agent, ethionamide (or prothionamide), and either cycloserine or PAS (p-aminosalicylic acid) if cycloserine cannot be used (conditional recommendation, /very low quality evidence).
14 4. Duration of second-line antituberculosis regimens 4.1 In the treatment of patients with MDR-TB, an intensive phase of at least 8 months duration is recommended (conditional recommendation, / very low quality evidence). 4.2 In the treatment of patients with MDR-TB, a total treatment duration of at least 20 months is recommended in patients without any previous MDR-TB treatment (conditional recommendation, /very low quality evidence).

15 Odds ratios of treatment success by duration of intensive phase and total treatment
16 the recommendation of at least Based on inadequate combination of : 1) the highest odds ratio in the duration analysis, 2) modification of duration according to response to treatment. Chiang C-Y, communication after 2 nd gglc meeting, Geneva, Feb 2012
17 Maximum duration of treatment? Duration of initial intensive phase (reference mo) PLoS Med 9(8): e doi: /journal.pmed
18 WHO recommendations, 2011 (revised) 4.1 In the treatment of patients with MDR-TB, an intensive phase of 8 months is suggested for most patients, and the duration may be modified according to the patient s response to therapy (conditional recommendation, /very low quality evidence). 4.2 In the treatment of patients newly diagnosed with MDR-TB (i.e. not previously treated for MDR-TB), a total treatment duration of 20 months is suggested for most patients, and the duration may be modified according to the patient s response to therapy (conditional recommendation, /very low quality evidence).

19 WHO Treatment Guidelines for drugresistant tuberculosis update
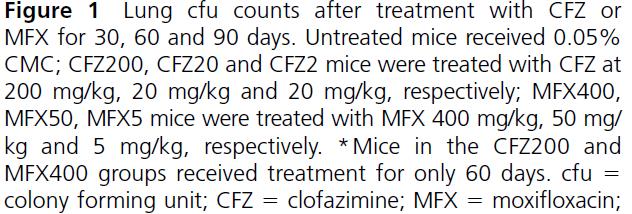
20 Medicines recommended for the treatment of rifampicin-resistant and multidrug-resistant TB A. Fluoroquinolones Levofloxacin Moxifloxacin Gatifloxacin B. Second-line injectable agents Amikacin Capreomycin Kanamycin (Streptomycin) C. Other core second-line agents Ethionamide / Prothionamide Cycloserine / Terizidone Linezolid Clofazimine * Medicines in Groups A and C are shown by decreasing order of usual preference for use
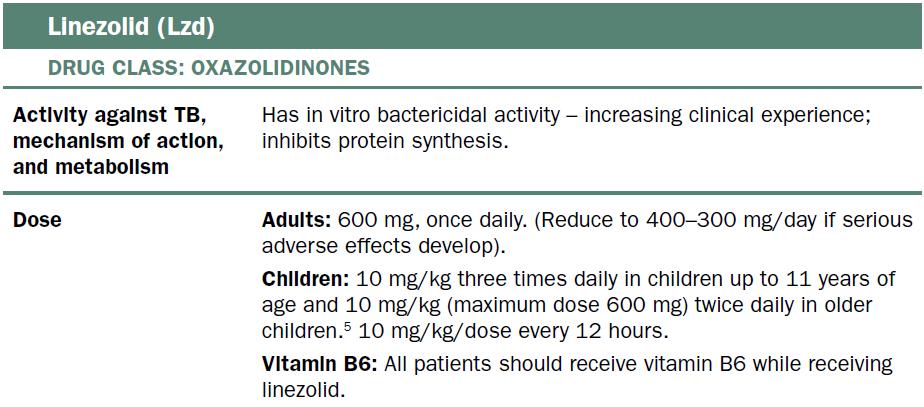
21 Medicines recommended for the treatment of rifampicin-resistant and multidrug-resistant TB D. Add-on agents (not part of the core MDR-TB regimen) 1 Pyrazinamide Ethambutol High-dose isoniazid 2 3 Bedaquiline Delamanid p-aminosalicylic acid Imipenem-Cilastatin Meropenem Amoxicillin-Clavulanate* (Thioacetazone)* *Carbapenems and clavulanate are meant to be used together; clavulanate is only available in formulations combined with amoxicillin; HIV-status must be tested and confirmed to be negative before thioacetazone is started
22 Emerging Infectious Diseases 2017
23 isoniazid (INH) 300 mg, levofloxacin 1000 mg, gatifloxacin 400 mg, or moxifloxacin 400 mg daily for 7 days Moxifloxacin, gatifloxacin, and high-dose levofloxacin have excellent EBA, only slightly less than for INH, and greater extended EBA.
24
25
26 The early bactericidal activity of antituberculosis drugs: a literature review In nearly all studies, whether over 0 2, 0 5 or 0 7 days, the fluoroquinolones have shown bactericidal activity close to, or equal to, that of INH. Despite being in vitro amongst the most bactericidal agents available, all the aminoglycosides have a relatively low EBA. Donald PR, et al. Tuberculosis 2008
27 Success Rates Levofloxacin Group Ofloxacin Group Overall 90% 79.7% Ofloxacin Susceptible 96,2% 87.5% Ofloxacin Resistant 78.6% 45.5% Levofloxacin was found to be more efficacious than ofloxacin when incorporated into multidrug regimens used for treatment of MDR-TB. Yew WW. Chest 2003; 124:
28 Comparison of Levofloxacin versus Moxifloxacin for Multidrug-Resistant Tuberculosis Comparison of time to culture (a) and smear (b) conversion between levofloxacin and moxifloxacin group adjusting for body mass index and pyrazinamide use Koh W-J, et al. Am J Respir Crit Care Med 2013
29 Fluoroquinolone-Containing Third-Line Regimen against M. tuberculosis In Vivo From 9 months onward, all of the organs of mice treated with the MXF-containing third-line regimen were culture negative. The majority of organs from mice treated with the OFX-containing regimen continued to be culture positive, and the mean CFU counts remained unchanged for as long as 12 months. The results for mice treated with the LVX-containing regimen fell between those for the groups receiving the MXF- and OFX containing regimens. Veziris N, et al. Antimicrob Agents Chemother 2003;47:
30 Phenotypic drug susceptibility testing for four fluoroquinolones in M. tuberculosis Coeck N, et al. J Antimicrob Chemother 2016; 71:
31 Correlation Between Type of gyra Mutation and Ofloxacin and Moxifloxacin MIC gyra mutations Ala90Val+Pro102Hi s No. of strains OFX 4 MOX 0.5 OFX 4 MOX OFX 8 MOX 1 Asp94Ala OFX 8 MOX 2 OFX 16 MOX 2 Ala90Val Ser91Pro 1 1 Ala126Arg Asp94His 1 1 Asp94Gly Asp94Tyr No specific mutation OFX 16 MOX 4 Total Kam KM, et al. Microb Drug Resistance 2006;12:7-11

32 Concordance of Mycobacterium tuberculosis fluoroquinolone resistance testing Farhat MR, et al. Int J Tuberc Lung Dis 2015;9:

33 Zignol M, et al Lancet Infect Dis 2016

34 Zignol M, et al Lancet Infect Dis 2016

35 Zignol M, et al Lancet Infect Dis 2016
36 Changes in treatment outcomes of MDR-TB, Korea The treatment success rate improved from 53.5% in to 68.8% in and 83.7% in (P<0.001). Improved outcomes were accompanied with more frequent use of later-generation fluoroquinolones and linezolid Kwak N, et al. Int J Tuberc Lung Dis 2015;19:


37 Aminoglycosides and Polypeptides Streptidine Streptomycin Deoxystreptamine Amikacin Kanamycin Polypeptides Capreomycin Viomycin
38 Cross-resistance between the aminoglycosides and/or the polypeptides Isolates that acquire resistance to streptomycin are usually susceptible to kanamycin, amikacin and capreomycin. rare strains with apparently single-step mutations that confer resistance to both streptomycin and kanamycin have been observed, although the molecular mechanism is not known World Health Organization. Policy guidance on drug-susceptibility testing (DST) of second-line antituberculosis drugs. 2008
39 Molecular Analysis of Cross-Resistance to Capreomycin, Kanamycin, Amikacin, and Viomycin in M. tuberculosis Maus CE, et al. Antimicrob Agents Chemother 2005
40 High Level of Cross-Resistance between Kanamycin, Amikacin, and Capreomycin among Mycobacterium tuberculosis Isolates from Georgia and a Close Relation with Mutations in the rrs Gene Of 78 kanamycin-resistant strains, 9 (11.5%) were susceptible to amikacin 16 (20.5%) were susceptible to capreomycin. Four strains were resistant to capreomycin but were susceptible to the other drugs, all amikacin-resistant isolates were resistant to kanamycin. Sequencing revealed six types of mutations in the rrs gene but no mutations in the tlya gene. Jugheli L, et al. Antimicrob Agents Chemother 2009;53:
 of the resistant isolates showed polymorphisms in the 16S ribosome components.")
41 Resistance and Cross-Resistance to Aminoglycosides and Capreomycin in M. tuberculosis Isolates, South Korea Most (33 of 36) of the resistant isolates showed polymorphisms in the 16S ribosome components. Three resistant strains (3 of 36) were identified that had no known polymorphisms in ribosomal constituents Via LE, et al. Antimicrob Agents Chemother 2010
42 Performance Assessment of the GenoType MTBDRsl Test and DNA Sequencing for Detection of Second-Line and Ethambutol Drug Resistance among MDR-TB Patients the sensitivities of resistance detection using the GenoType MTBDRsl test were kanamycin 43.2%, amikacin 84.2%, capreomycin 71.4% with the inclusion of an extra gene, eis, in sequencing, the sensitivity reached 70.3% for detection of KM resistance. Huang W-L. et al. 2011
43 Streptomycin for the treatment of second line injectable-resistant MDR-TB In cases where the strain is resistant to all the second-line injectable drugs (amikacin, kanamycin, and capreomycin), except streptomycin, streptomycin should be considered, as there is little cross-resistance between streptomycin and the other injectable agents. WHO Companion Handbook 2014

44 Hearing and balance functions of the inner ear The cochlea is the hearing part of the inner ear, The semicircular canals are part of our balance system Challenge TB. Audiometry in the Management of Drug-Resistant Tuberculosis 2017

45 Progressive damage to the organ of Corti. Scanning electron micrographs showing the progression of damage in the basal coil of the guinea pig organ of Corti after gentamicin treatment Loss of outer hair cells Initial loss of inner hair cells Complete loss of inner hair cells Organ of Corti replaced by squamous epithelium Forge A. Audiol Neurootol 2000;5:3 22

46 Challenge TB. Audiometry in the Management of Drug-Resistant Tuberculosis 2017

47 First synthesized in 1954.

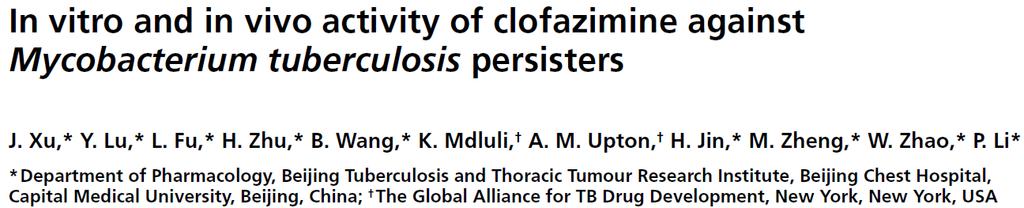
48 Comparative Intracellular Activities Against the Virulent H37Rv Strain in Human Macrophages Rastogi N, et al. Current Microbiology 1996;33:
49 49
50 Clofazimine Study designed and supervised by: Jacques Grosset, MD And conducted by: Sandeep Tyagi, BS, Si-yang Li, BS, Deepak Almeida, PhD, Paul Converse, PhD 50

51 Long-term outcomes of patients with extensively drug-resistant tuberculosis in South Africa: a cohort study Pietersen E, et al. Lancet 2014; 383:
52 Long-term outcomes of patients with extensively drug-resistant tuberculosis in South Africa: a cohort study predictors of net culture conversion no history of multidrug-resistant tuberculosis (p=0 0007) use of clofazimine (p=0 0069). predictors of survival net culture conversion (p<0 0001) treatment with clofazimine (p=0 021). Antiretroviral therapy in patients with HIV (p=0 003). Pietersen E, et al. Lancet 2014; 383:
53
54 Early and Extended Early Bactericidal Activity of Linezolid in Pulmonary Tuberculosis Am J Respir Crit Care Med 2008;178:
55 Linezolid for Treatment of Chronic XDR-TB N Engl J Med 2012;367:
56 Linezolid for Treatment of Chronic XDR-TB N Engl J Med 2012;367:

57 Linezolid :systematic review and metaanalysis Sotgiu G, et al. Eur Respir J 2012; 40:


58 Linezolid :systematic review and metaanalysis Sotgiu G, et al. Eur Respir J 2012; 40:
59 Isoniazid (INH):a prodrug that requires the activation of bacterial catalaseperoxidase enzyme (katg). katg mutation Reduce ability to activate the prodrug cause INH resistance (low or high level) Could be restored by transformation with a functional katg gene Zhang Y,et al. 1992, 1993, 2000
60 Isoniazid (INH) inha encodes the NADH-dependent enoyl ACP reductase ( an enzyme involved in synthesis of cell wall mycolic acid) Cause low level INH resistance Also confer resistance to the structurally related ethionamide Zhang Y, et al. ASM 2000
61 After adjustment for potential confounders, subjects who received high-dose INH became sputum negative 2.38 times (95%CI , P 0.001) more rapidly than those who did not receive it had a 2.37 times (95%CI , P 0.001) higher likelihood of being sputum-negative at 6 months.

62 Mycobacterium tuberculosis drug susceptibility testing Böttger EC. Clin Microbiol Infect 2011;17:
63

64 Meropenem-Clavulanate and XDR-TB (A) Aerobic growth (B) Nonreplicating anaerobic M. tuberculosis Science 2009;323:

65 Clinical use of the meropenem-clavulanate combination for XDR-TB Int J Tuberc Lung Dis 2012;16:
66 Clinical use of the meropenemclavulanate combination for XDR-TB Int J Tuberc Lung Dis 2012;16:

67 Efficacy and safety of meropenem clavulanate added to linezolid-containing regimens in the treatment of MDR-/XDR-TB De Lorenzo S, et al. Eur Respir J 2013;41:
68 Conventional treatment regimens for rifampicin-resistant TB In patients with rifampicin-resistant or multidrugresistant TB, a regimen with at least five effective TB medicines during the intensive phase is recommended, including pyrazinamide and four core second-line TB medicines - one chosen from group A, one from group B, and at least two from group C (conditional recommendation, very low certainty in the evidence). If the minimum of effective TB medicines cannot be composed as above, an agent from group D2 and other agents from D3 may be added to bring the total to five WHO Treatment Guidelines for drug-resistant tuberculosis update
69 In patients with rifampicin-resistant or multidrug-resistant TB, it is recommended that the regimen be further strengthened with high-dose isoniazid and/or ethambutol (conditional recommendation, very low certainty in the evidence). WHO Treatment Guidelines for drug-resistant tuberculosis update

70 Treatment outcomes for patients diagnosed with MDR- TB by WHO region, cohorts WHO. Global Tuberculosis Report
71 Predicting the future of XDR tuberculosis Blower S. Lancet Infect Dis 2007;7:443 71
72 Short Standardized Treatment of Multidrugresistant Tuberculosis Intensive phase: GEZC KHP 4 months, extended till sputum conversion Continuation phase: GEZC 5 months Kanamycin (K) Prothionamide (P) Isoniazid (H)* Gatifloxacin (G)* Clofazimine, C Ethambutol, E Pyrazinamide, P Gatifloxacin (G)* Clofazimine, C Ethambutol, E Pyrazinamide, P *high dose Van Deun A, et al. Am J Respir Crit Care Med 2010;182:
73 Regimens sequentially used in the treatment of multidrugresistant tuberculosis, Bangladesh Damien Foundation Projects K Kanamycin, C Clofazimine, O Ofloxacin, G Gatifloxacin, E Ethambutol, H Isoniazid Z Pyrazinamide, P Prothionamide Van Deun A, et al. Am J Respir Crit Care Med 2010;182:
74 Daily Drug Dosages Used For Standardized Multidrug-resistant Antituberculosis Treatment, Bangladesh Damien Foundation Projects *KM reduced by 25% for patients aged 45, later precisely as 15 mg/kg, 3 times weekly 4th month onward Gatifloxacin was used at a lower dosage for the first 50 patients enrolled The high dose of isoniazid was used with the gatifloxacin-based regimen, whereas the normal dose was given in all ofloxacin-based regimens Van Deun A, et al. Am J Respir Crit Care Med 2010;182:
75 Regimens sequentially used in the treatment of multidrugresistant tuberculosis, Bangladesh Damien Foundation Projects Van Deun A, et al. Am J Respir Crit Care Med 2010;182:
76 Van Deun A, et al. Am J Respir Crit Care Med 2010;182:
77 Outcome of treatment of multidrug-resistant tuberculosis, by grouped regimen category, Bangladesh Damien Foundation Projects. R1+2, 3KCOEHZP/12 OEHZP, few failures (5.8%), but 14.6% defaulted R3, 3(4) KCOEZP/12 OEZP, without H had a very low effectiveness (57.1% cure). R4, 3(+) KCOEHZP/12 OHEZ, problematic continuation phase, resulted in 13.3% failures R5, 3(+) KCOEHZP/12 OHEZC, no relapse with any of the five regimens during 2 years of follow-up, one reinfection Van Deun A, et al. Am J Respir Crit Care Med 2010;182:
78 Outcome of Treatment with the Gatifloxacin-based Regimen Of the 206 patients, 35 (17.0%) with a positive smear at 4 months required extension of the intensive phase. one treatment failure and 12 defaults(5.8%) Of the 182 patients who completed treatment, one had a relapse at 6 months. Van Deun A, et al. Am J Respir Crit Care Med 2010;182:

79 Treatment Antecedents and Initial Drug Resistance the gatifloxacin-based regimen, in contrast to the ofloxacin based regimens, did not lead to additional acquired resistance Van Deun A, et al. Am J Respir Crit Care Med 2010;182:
80 Dysglycemia 2/221 patients on ofloxacin 8/206 patients on gatifloxacin regimens No patient required permanent stopping of treatment due to adverse drug reactions, but 3 patients had gatifloxacin replaced by ofloxacin (and treatment prolonged accordingly) Van Deun A, et al. Am J Respir Crit Care Med 2010;182:
81 MDR-TB, Niger 12-month standardised regimen: 4 Km Gfx Pto H Cfz E Z / 8 Gfx Cfz E Z (Gfx, high dose) 65 MDR-TB patients Cure: 58 patients (89.2%, 95%CI ), died 6 Defaulted 1. No relapse at the 24-month follow-up after cure (49 patients) Piubello A, et al. Int J Tuberc Lung Dis 2014;18:

82 High effectiveness of a 12-month regimen for MDR-TB patients in Cameroon Kuaban C, et at. Int J Tuberc Lung Dis 2015; 19:
83 Kuaban C, et at. Int J Tuberc Lung Dis 2015; 19:
84 High effectiveness of a 12-month regimen for MDR-TB patients in Cameroon 150 MDR-TB patients (20% HIV-positive) 4 Km Gfx Pto H Cfz E Z / 8 Gfx Cfz Pto E Z (Gfx 400 mg) Kuaban C, et at. Int J Tuberc Lung Dis 2015; 19:
85 Bangladesh MDR-TB, Km Gfx Pto H Cfz E Z / 5 Gfx Cfz E Z relapse-free treatment success 84% (N = 515) cured 423 (82%) completed 12 (2%) defaulted 40 (8%) died 29 (6%) failed 7 (1%) relapsed 4 (0.8%) Aung KJM et al. Int J Tuberc Lung Dis 2014;18:
86 86
87 87
88 Successful 9-month Bangladesh regimen for MDR-TB patients Of the 515 patients 435 (84.4%) had a bacteriologically favorable outcome Eleven patients failed (n=7) or relapsed (n=4) Amplification of drug resistance occurred only once, in a patient strain that was initially only susceptible to kanamycin and clofazimine
89 Acquired Resistance to Fluoroquinolones Among 832 Adults With Pulmonary Multidrug-Resistant Tuberculosis Starting Treatment With Second-line Drugs, , in 9 Countries Of those without baseline resistance to specific secondline drugs, 68 (8.9%) acquired extensively drug-resistant (XDR) tuberculosis, 79 (11.2%) acquired fluoroquinolone (FQ) resistance, and 56 (7.8%) acquired resistance to second-line injectable drugs Cegielski JP, et al. Clin Infect Dis 2014;59:
90 Acquired Resistance to Fluoroquinolones Among 832 Adults With Pulmonary Multidrug-Resistant Tuberculosis Starting Treatment With Second-line Drugs, , in 9 Countries Baseline DST Ethambutol Resistance susceptible kanamycin Resistance susceptible Ethionamide Resistance susceptible Acquired FQ resistance 17.4% 7.9% 36.8% 6.0% 11.5% 12.1% RR (95% CI) 1.86 ( ) ( ) ( ) 1 Cegielski JP, et al. Clin Infect Dis 2014;59:
91 91

92 Characteristics of patients with a programmatically favorable outcome vs. those with an unfavorable treatment outcome Aung KJM et al. Int J Tuberc Lung Dis 2014;18:
93 Standardised regimens lasting up to 12 months for the treatment of patients with multidrug-resistant TB Recommendation: In patients with rifampicin-resistant or multidrugresistant TB who have not been previously treated with second-line drugs and in whom resistance to fluoroquinolones and second-line injectable agents has been excluded or is considered highly unlikely, a shorter MDR-TB regimen of 9-12 months may be used instead of a conventional regimen (conditional recommendation, very low certainty in the evidence) WHO Treatment Guidelines for drug-resistant tuberculosis update


94
95 Treatment success in patients treated with a shorter MDR-TB regimen versus conventional MDR-TB regimens Resistance pattern Shorter regimen Conventional regimen All cases (n=1116 vs 5850) 90.3% (87.8%- 92.4%) Pyrazinamide R; fluoroquinolone R (n=28 vs 137) Pyrazinamide R; fluoroquinolone S (n=100 vs 1075) Pyrazinamide S; fluoroquinolone R (n=15 vs 120) Pyrazinamide S; fluoroquinolone S (n=125 vs 1119) 67.9% (47.6%-84.1%) 88.8% (47.3%-98.6%) 80.0% (50.0%-94.1%) 96.8% (77.3%-99.6%) 78.3% (71.2%- 84%) 59.1% (50.6%-67.1%) 81.4% (71.6%-88.4%) 64.4% (49.6%-76.9%) 83.5% (75.7%-89.2%) treatment success (cured or treatment completed(14),(9)) versus failure/relapse/death in patients not previously treated with secondline TB medications
96 Subgroup considerations - RR-TB without MDR-TB All patients children or adult - with rifampicin-resistant TB in whom isoniazid resistance is not confirmed may be treated with the shorter MDR-TB treatment regimen WHO Treatment Guidelines for drug-resistant tuberculosis update
97 Subgroup considerations - Resistance additional to MDR-TB In patients infected with strains known or strongly suspected of being resistant to one or more drugs in the shorter MDR-TB treatment regimen (e.g. pyrazinamide) it is recommended not to use the shorter regimen until more evidence becomes available about its performance in such a situation.
98 The recommendations from the WHO on the use of shortened MDR-TB regimens controversially indicated that shortened MDR-TB regimens should not be used in patients who have documented or likely resistance to medicines in the regimen, leading to the concept that MDR-TB patients with additional resistance to not only fluoroquinolones (FQs) or second-line injectables (SLIs), but also ethambutol (EMB), prothionamide (Pto) and pyrazinamide (PZA) would not be eligible for the regimens. This is a highly conservative approach that will greatly limit the applicability of shortened MDR-TB regimens and deprive many MDR-TB patients in high-burden countries of short and highly effective regimens. Van Deun A, Chiang C-Y. Shortened multidrug-resistant tuberculosis regimens overcome low-level fluoroquinolone resistance. Eur Respir J 2017; 49: [ ].
99 Subgroup considerations - People living with HIV People living with HIV need to be given the same consideration for treatment with the shorter MDR-TB treatment regimen as people who are HIV seronegative.
100 Subgroup considerations - Children Children were generally excluded from studies of the shorter MDR-TB treatment regimens. However, there is no plausible biological reason to believe that these regimens are less effective in children than in adults. As a result, it is recommended that children with confirmed RR-/MDR-TB be given the same consideration for treatment with a shorter MDR-TB treatment regimen as adults
101 Subgroup considerations - Pregnant women Pregnancy was an exclusion criterion for the shorter MDR-TB treatment regimen studies. Two of the core components of the shorter MDR-TB regimens the injectable agent and ethionamide (or prothionamide) are usually contraindicated in pregnancy it is thus recommended that an individualised, conventional regimen is used which can allow the inclusion of four or more effective medicines with no known teratogenic properties
102 Subgroup considerations - Extrapulmonary disease The findings from studies of shorter MDR-TB regimen were limited to patients with pulmonary disease, and they cannot be extrapolated directly to extrapulmonary TB. No recommendation is thus possible at this stage to use the shorter regimen in patients with extrapulmonary MDR-TB.
103 Implementation considerations Patients are tested for susceptibility or resistance to fluoroquinolones and to the second-line injectable agent used in the regimen before being started on a shorter MDR-TB regimen: patients with strains resistant to any of the two groups of medicines are to be transferred to treatment with a conventional MDR-TB regimen. the Genotype MTBDRsl line probe assay may be used as an initial direct test, over phenotypic culture-based DST, to detect resistance to fluoroquinolones and to the second-line injectable drugs
104 Implementation considerations In settings in which laboratory capacity for DST to fluoroquinolones and injectable agents is not yet available, treatment decisions would need to be decided on the basis of the likelihood of resistance to these medicines, informed by the patient s clinical history and recent representative surveillance data.
MDR/XDR TB. Barbara Seaworth, MD, FIDSA, FACP October 27, TB Intensive October 24 27, 2017 San Antonio, TX
 MDR/XDR TB Barbara Seaworth, MD, FIDSA, FACP October 27, 2017 TB Intensive October 24 27, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Barbara Seaworth, MD, FIDSA, FACP, has the following disclosures
MDR/XDR TB Barbara Seaworth, MD, FIDSA, FACP October 27, 2017 TB Intensive October 24 27, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Barbara Seaworth, MD, FIDSA, FACP, has the following disclosures
Drug-resistant TB therapy: the future is now
 Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
Drug-resistant TB therapy: the future is now Gary Maartens Thanks to Francesca Conradie for sharing slides Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN
Multi-Drug and Extensively Drug Resistant Tuberculosis
 Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
Multi-Drug and Extensively Drug Resistant Tuberculosis Gwen A. Huitt, M.D., M.S. Professor, Department of Medicine Director, Adult Infectious Disease Care Unit National Jewish Health Disclosures None Tuberculosis
Clinical Management : DR-TB
 Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
Clinical Management : DR-TB Charoen Chuchottaworn MD., Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH. Tuberculosis Classification Drug susceptible TB
MDR treatment. Shanghai, May 2012 Arnaud Trébucq The Union
 MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
MDR treatment Shanghai, May 2012 Arnaud Trébucq The Union Why to diagnose MDR-TB? Outcome of SS+ new MDR-TB cases, treated with First Line TB (FLD) drugs Setting Success Died Fail LFFU Transf. Corea 20(56)
THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION
 1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
1 THE NEW DR-TB NATIONAL POLICY AND STATE OF IMPLEMENTATION Dr. Norbert Ndjeka MD, DHSM (Wits), MMed(Fam Med) (MED), Dip HIV Man (SA) Director Drug-Resistant TB, TB and HIV National Department of Health
Challenges to treat MDR TB
 Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
Challenges to treat MDR TB Manfred Danilovits Tartu University Hospital, Estonian NTP Program 2nd European Advanced Course in Clinical Tuberculosis 22-24 September 2014, Amsterdam MDR-TB control; WHO Europe,
Multidrug-resistant Tuberculosis. Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership
 Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
Multidrug-resistant Tuberculosis Charles L. Daley, MD National Jewish Health Chair, Global GLC, WHO and Stop TB Partnership Disclosures World Health Organization Chair, Global GLC Otsuka Chair, Data Monitoring
Treatment of Multidrug-resistant Tuberculosis (MDR-TB)
") Treatment of Multidrug-resistant Tuberculosis (MDR-TB) 2006 2008 2011 2013 2014 2016 2019 Charles L. Daley, MD National Jewish Health University of Colorado Disclosures Research grant Insmed: Phase II
Treatment of Multidrug-resistant Tuberculosis (MDR-TB) 2006 2008 2011 2013 2014 2016 2019 Charles L. Daley, MD National Jewish Health University of Colorado Disclosures Research grant Insmed: Phase II
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S.
 Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
Strategies for Successful Treatment of Drug Resistant Tuberculosis in the U.S. Barbara J. Seaworth, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Medical Director, Heartland
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing - PRELIMINARY -
 Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
Summary of outcomes from WHO Expert Group Meeting on Drug Susceptibility Testing PRELIMINARY 4 th Annual GLI meeting 17 April 2012 Fuad Mirzayev Laboratories, Diagnostics and Drug Resistance unit, Stop
Management of MDR and XDR TB Prof. Martin Boeree
 Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
Management of MDR and XDR TB 1, MD, PhD Associate Professor Consultant Respiratory Medicine Department of Lung Diseases Radboud University Nijmegen Medical Centre TB Referral Hospital Dekkerswald Nijmegen,
MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2
 1 MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2 1 India has the highest TB burden in the world 3 4 2 5 M. tuberculosis Resistance
1 MDR-TB is a manmade problem..it is costly, deadly, debilitating, and the biggest threat to our current TB control strategies 2 1 India has the highest TB burden in the world 3 4 2 5 M. tuberculosis Resistance
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 MDR/XDR TB Barbara J. Seaworth, MD October 16, 2013 Barbara J. Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
TB Intensive Houston, Texas October 15-17, 2013 MDR/XDR TB Barbara J. Seaworth, MD October 16, 2013 Barbara J. Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
Drug resistant TB: The role of the laboratory
 Drug resistant TB: The role of the laboratory 26 Oct 2012 Andrew Whitelaw NHSLS / UCT TB lab functions: Outline Resistance testing Genotypic Phenotypic Which tests are done when, and why Reporting of
Drug resistant TB: The role of the laboratory 26 Oct 2012 Andrew Whitelaw NHSLS / UCT TB lab functions: Outline Resistance testing Genotypic Phenotypic Which tests are done when, and why Reporting of
TB New Drugs, Shorter Courses
 TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
TB New Drugs, Shorter Courses Brian Chong John Hunter Hospital, Newcastle NSW Talk supervisor: Chris Coulter Disclosures Unfortunately none 1 Current Situation In 2013, Australia had: 1,263 notified TB
MDR-TB drugs per WHO guidelines
 New antituberculous agents for drug-resistant resistant TB Symposium Belgian Society of Infectiology and Clinical Microbiology November 9 Jens Van Roey, MD - Tibotec Definitions MDR-TB multidrug resistance
New antituberculous agents for drug-resistant resistant TB Symposium Belgian Society of Infectiology and Clinical Microbiology November 9 Jens Van Roey, MD - Tibotec Definitions MDR-TB multidrug resistance
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas May 6 9, 2014 MDR/XDR TB Barbara Seaworth, MD May 9, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial relationships
TB Intensive San Antonio, Texas May 6 9, 2014 MDR/XDR TB Barbara Seaworth, MD May 9, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial relationships
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
TB Intensive San Antonio, Texas April 6-8, 2011 Drug Resistant TB Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received research funding from
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France
 Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
Treatment for NTM: when how.and what next? Pr Claire Andréjak Respiratory and ICU Department University hospital, Amiens, France First step = To diagnose NTM disease One NTM positive sample NTM disease
DR-TB PATIENT IDENTITY CARD
 Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
Ministry of Health Community Development Gender Elderly and Children National Tuberculosis and Leprosy Programme DR-TB 02 DR-TB Treatment Unit: DR-TB PATIENT IDENTITY CARD DR-TB Reg. Number: Date of registration:
New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick
 Patrick") New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick Phillips Patrick.Phillips@ucsf.edu @PPJPhillips Outline Overview of regimen development strategies 1-3 year horizon: Ongoing phase
New drugs and regimens for treatment of drug-sensitive TB (DS-TB) Patrick Phillips Patrick.Phillips@ucsf.edu @PPJPhillips Outline Overview of regimen development strategies 1-3 year horizon: Ongoing phase
MDR TB AND CASE STUDIES
 MDR TB AND CASE STUDIES Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Seattle, CITC Clinical Intensive June 15, 2018 Slide
MDR TB AND CASE STUDIES Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Seattle, CITC Clinical Intensive June 15, 2018 Slide
Linezolid: an effective, safe and cheap drug for patients failing multidrug-resistant tuberculosis treatment in India
 Eur Respir J 2012; 39: 956 962 DOI: 10.1183/09031936.00076811 CopyrightßERS 2012 Linezolid: an effective, safe and cheap drug for patients failing multidrug-resistant tuberculosis treatment in India R.
Eur Respir J 2012; 39: 956 962 DOI: 10.1183/09031936.00076811 CopyrightßERS 2012 Linezolid: an effective, safe and cheap drug for patients failing multidrug-resistant tuberculosis treatment in India R.
Tuberculosis in 2017: Searching for new solutions in the face of new challenges
 Tuberculosis in 2017: Searching for new solutions in the face of new challenges 6th TB Symposium Ministry of Health of the Republic of Belarus, Republican Scientific and Practical Center for Pulmonology
Tuberculosis in 2017: Searching for new solutions in the face of new challenges 6th TB Symposium Ministry of Health of the Republic of Belarus, Republican Scientific and Practical Center for Pulmonology
Treatment of Drug Resistant TB
 Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
Treatment of Drug Resistant TB Diana M. Nilsen RN, MD Bureau of TB Control New York City Department of Health & Mental Hygiene Objectives Definition of other drug resistant (ODR), multiple drug resistant
TB Grand Rounds. MDR-TB: Management of Adverse Drug Reactions. Reynard J. McDonald, M.D. September 18, Patient History
 TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
TB Grand Rounds MDR-TB: Management of Adverse Drug Reactions Reynard J. McDonald, M.D. September 18, 2007 Patient History This 30 y/o H/M was born in Ecuador and immigrated to the US in 2001 On 11-22-05
The New England Journal of Medicine THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY
 THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY KEMAL TAHAOĞLU, M.D., TÜLAY TÖRÜN, M.D., TÜLIN SEVIM, M.D., GÜLIZ ATAÇ, M.D., ALTAN KIR, M.D., LEVENT KARASULU, M.D., IPEK ÖZMEN, M.D., AND NILÜFER
THE TREATMENT OF MULTIDRUG-RESISTANT TUBERCULOSIS IN TURKEY KEMAL TAHAOĞLU, M.D., TÜLAY TÖRÜN, M.D., TÜLIN SEVIM, M.D., GÜLIZ ATAÇ, M.D., ALTAN KIR, M.D., LEVENT KARASULU, M.D., IPEK ÖZMEN, M.D., AND NILÜFER
CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP)
 Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP)") CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP) Beverly Metchock, DrPH, D(ABMM) Mycobacteriology Laboratory Branch/Division
CDC s Molecular Detection of Drug Resistance (MDDR) Service and Mycobacterium tuberculosis DST Model Performance Evaluation Program (MPEP) Beverly Metchock, DrPH, D(ABMM) Mycobacteriology Laboratory Branch/Division
In Vitro Activities of Linezolid against Clinical Isolates of ACCEPTED
 AAC Accepts, published online ahead of print on April 00 Antimicrob. Agents Chemother. doi:./aac.001-0 Copyright 00, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
AAC Accepts, published online ahead of print on April 00 Antimicrob. Agents Chemother. doi:./aac.001-0 Copyright 00, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
University of Groningen. Tuberculosis and its sequelae Akkerman, Onno
 University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Tuberculosis and its sequelae Akkerman, Onno IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB)
") Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB) Session: Fanning the Flames of HIV and TB Cointeraction SA AIDS Conference-Durban ICC 13-15 June 2017
Effects of Moxifloxacin PK-PD and drug interactions on its use in the Treatment of Tuberculosis(TB) Session: Fanning the Flames of HIV and TB Cointeraction SA AIDS Conference-Durban ICC 13-15 June 2017
XDR TB: The Laboratory s Dilemma vs The Clinician s Dilemma
 XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
XD TB: The Laboratory s Dilemma vs The Clinician s Dilemma Barbara J. Seaworth, MD, FIDSA, FACP, Heartland National TB Center, San Antonio, TX Kenneth Jost, Jr., M(ASCP) Laboratory Services Section, Texas
TB Intensive Houston, Texas. Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD
 TB Barbara Seaworth, MD") TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
TB Intensive Houston, Texas November 10-12, 12 2009 Multi-Drug Resistant (MDR) TB Barbara Seaworth, MD November 12, 2009 Multi-Drug Resistant (MDR) TB Updates November 12, 2009 Barbara J. Seaworth Professor
Practical. Walk through New Survival Guide
 Many faces of TB: Drug resistant it ttbs Survival lgid Guide v3 P B L Ch G Sh t L T P. Barry, L. Chen, G. Schecter, L. True Curry International TB Center/CTCA April 20, 2016 Real case Practical Walk through
Many faces of TB: Drug resistant it ttbs Survival lgid Guide v3 P B L Ch G Sh t L T P. Barry, L. Chen, G. Schecter, L. True Curry International TB Center/CTCA April 20, 2016 Real case Practical Walk through
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Extensively Drug-Resistant Tuberculosis in South Korea: Risk Factors and Treatment Outcomes among Patients at a Tertiary Referral Hospital
 MAJOR ARTICLE Extensively Drug-Resistant Tuberculosis in South Korea: Risk Factors and Treatment Outcomes among Patients at a Tertiary Referral Hospital Christie Y. Jeon, 1,2,a Soo Hee Hwang, 5,a Jin Hong
MAJOR ARTICLE Extensively Drug-Resistant Tuberculosis in South Korea: Risk Factors and Treatment Outcomes among Patients at a Tertiary Referral Hospital Christie Y. Jeon, 1,2,a Soo Hee Hwang, 5,a Jin Hong
Multidrug resistant Tuberculosis
 Multidrug resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive October 018 Objectives
Multidrug resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive October 018 Objectives
Treatment of Nontuberculous Mycobacterial Infections (NTM)
") Treatment of Nontuberculous Mycobacterial Infections (NTM) Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory
Treatment of Nontuberculous Mycobacterial Infections (NTM) Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory
New antituberculosis drugs and regimens
 New antituberculosis drugs: from clinical trial to programmatic use Gina Gualano, 1 Susanna Capone, 2 Alberto Matteelli, 2 Fabrizio Palmieri 1 1 Respiratory Infectious Diseases Unit, National Institute
New antituberculosis drugs: from clinical trial to programmatic use Gina Gualano, 1 Susanna Capone, 2 Alberto Matteelli, 2 Fabrizio Palmieri 1 1 Respiratory Infectious Diseases Unit, National Institute
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 29 October 2014 GRANUPAS, gastro-resistant granules 30 sachets with a calibrated measuring spoon (CIP: 34009 278 801
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 29 October 2014 GRANUPAS, gastro-resistant granules 30 sachets with a calibrated measuring spoon (CIP: 34009 278 801
Multidrug-resistant Tuberculosis
 Multidrug-resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive September 2016
Multidrug-resistant Tuberculosis Pennan Barry, MD, MPH California MDR TB Consult Service Surveillance and Epidemiology Section Curry International Tuberculosis Center Clinical Intensive September 2016
Introduction of Bedaquiline in the Philippines
 Introduction of Bedaquiline in the Philippines 24th PhilCAT Annual Convention Crown Plaza Hotel August 18,2107 Vivian S. Lofranco, MD., PHSAE National Clinical Coordinator, BDQ MDR-TB is highly contagious
Introduction of Bedaquiline in the Philippines 24th PhilCAT Annual Convention Crown Plaza Hotel August 18,2107 Vivian S. Lofranco, MD., PHSAE National Clinical Coordinator, BDQ MDR-TB is highly contagious
Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool)
") Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool) DOTS + and LTBI New drugs for TB and the challenge of resistance talk plan 1. Epidemiology 2. Treatment 3. The MDRTB
Multidrug resistant tuberculosis. Where next? Professor Peter D O Davies (Liverpool) DOTS + and LTBI New drugs for TB and the challenge of resistance talk plan 1. Epidemiology 2. Treatment 3. The MDRTB
Quality of 2 nd line medicines for tuberculosis. Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products
 Quality of 2 nd line medicines for tuberculosis Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products Case studies in medicines for tuberculosis Outline: Statistics
Quality of 2 nd line medicines for tuberculosis Ms Lisa Hedman World Health Organization Department of Essential Medicines and Health Products Case studies in medicines for tuberculosis Outline: Statistics
Title: Resistance to fluoroquinolones and second line injectable drugs: impact on MDR TB outcomes
 ERJ Express. Published on October 25, 2012 as doi: 10.1183/09031936.00134712 Title: Resistance to fluoroquinolones and second line injectable drugs: impact on MDR TB outcomes Authors: D. Falzon, N. Gandhi,
ERJ Express. Published on October 25, 2012 as doi: 10.1183/09031936.00134712 Title: Resistance to fluoroquinolones and second line injectable drugs: impact on MDR TB outcomes Authors: D. Falzon, N. Gandhi,
INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS
 INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS 1 Research Associate, Drug Utilisation Research Unit, Nelson Mandela University 2 Human Sciences Research Council,
INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS 1 Research Associate, Drug Utilisation Research Unit, Nelson Mandela University 2 Human Sciences Research Council,
Case 1 and Case 2. Case 1 3/23/2016
 Case 1 and Deidra D. Parrish, MD, MPH&TM Nashville Metro Public Health Dept TB Symposium March 30, 2016 Case 1 27 yo Indian woman came to the US to join her husband three months prior to clinic visit.
Case 1 and Deidra D. Parrish, MD, MPH&TM Nashville Metro Public Health Dept TB Symposium March 30, 2016 Case 1 27 yo Indian woman came to the US to join her husband three months prior to clinic visit.
Drug resistant TB: Lisa Chen, MD University of California, San Francisco Curry Interna:onal TB Center Sea=le, June 2016
 Drug resistant TB: Lisa Chen, MD University of California, San Francisco Curry Interna:onal TB Center Sea=le, June 2016 Drug- Resistant TB: De1initions Mono- resistant: Resistance to a single drug Poly-
Drug resistant TB: Lisa Chen, MD University of California, San Francisco Curry Interna:onal TB Center Sea=le, June 2016 Drug- Resistant TB: De1initions Mono- resistant: Resistance to a single drug Poly-
Risk Factors for Poor Outcomes in Patients with Multi-Drug Resistant Tuberculosis in South Korea
 Hanyang Med Rev 2016;36:262-268 https://doi.org/10.7599/hmr.2016.36.4.262 pissn 1738-429X eissn 2234-4446 Original Article Risk Factors for Poor Outcomes in Patients with Multi-Drug Resistant Tuberculosis
Hanyang Med Rev 2016;36:262-268 https://doi.org/10.7599/hmr.2016.36.4.262 pissn 1738-429X eissn 2234-4446 Original Article Risk Factors for Poor Outcomes in Patients with Multi-Drug Resistant Tuberculosis
Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study
 Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study Julie Tans-Kersten, MS, BS-MT (ASCP) Tuberculosis Laboratory Program Coordinator Wisconsin
Exploring Novel Approaches to Shared TB Laboratory Services: California-Wisconsin Shared Services Pilot Study Julie Tans-Kersten, MS, BS-MT (ASCP) Tuberculosis Laboratory Program Coordinator Wisconsin
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections
 for the treatment of Acinetobacter baumannii infections") ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
Current Status of Fluoroquinolone Use for Treatment of Tuberculosis in a Tertiary Care Hospital in Korea
 ORIGINAL ARTICLE https://doi.org/10.4046/trd.2017.80.2.143 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2017;80:143-152 Current Status of Fluoroquinolone Use for Treatment of Tuberculosis
ORIGINAL ARTICLE https://doi.org/10.4046/trd.2017.80.2.143 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2017;80:143-152 Current Status of Fluoroquinolone Use for Treatment of Tuberculosis
The challenge of managing extensively drug-resistant tuberculosis at a referral hospital in the state of São Paulo, Brazil: a report of three cases
 J Bras Pneumol. 2015;41(6):554-559 http://dx.doi.org/10.1590/s1806-37562015000000299 CASE REPORT The challenge of managing extensively drug-resistant tuberculosis at a referral hospital in the state of
J Bras Pneumol. 2015;41(6):554-559 http://dx.doi.org/10.1590/s1806-37562015000000299 CASE REPORT The challenge of managing extensively drug-resistant tuberculosis at a referral hospital in the state of
MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience
 MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience Dr Johan Van Wyk MB.Ch.B, M.Med (Clin Path) Clinical Pathologist ibhayi Region, Eastern Cape GWYNETH PALTROW SHAKESPEARE IN LOVE 1998 PORT
MGIT 2 nd LINE DRUG SUSCEPTIBILITY TESTING A personal experience Dr Johan Van Wyk MB.Ch.B, M.Med (Clin Path) Clinical Pathologist ibhayi Region, Eastern Cape GWYNETH PALTROW SHAKESPEARE IN LOVE 1998 PORT
ORIGINAL INVESTIGATION. Increasing Outpatient Fluoroquinolone Exposure Before Tuberculosis Diagnosis and Impact on Culture-Negative Disease
 ORIGINAL INVESTIGATION Increasing Outpatient Fluoroquinolone Exposure Before Tuberculosis Diagnosis and Impact on Culture-Negative Disease Pinky D. Gaba, MD; Connie Haley, MD, MPH; Marie R. Griffin, MD,
ORIGINAL INVESTIGATION Increasing Outpatient Fluoroquinolone Exposure Before Tuberculosis Diagnosis and Impact on Culture-Negative Disease Pinky D. Gaba, MD; Connie Haley, MD, MPH; Marie R. Griffin, MD,
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens
 The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
Policy guidance on drug-susceptibility testing (DST) of second-line antituberculosis drugs World Health Organization Geneva 2008
 of second-line antituberculosis drugs World Health Organization Geneva 2008") Policy guidance on drugsusceptibility testing (DST) of secondline antituberculosis drugs World Health Organization Geneva 2008 WHO/HTM/TB/2008.392 1 World Health Organization 2008 All rights reserved.
Policy guidance on drugsusceptibility testing (DST) of secondline antituberculosis drugs World Health Organization Geneva 2008 WHO/HTM/TB/2008.392 1 World Health Organization 2008 All rights reserved.
Drug Resistant Tuberculosis:
 Drug Resistant Tuberculosis: Pearls and other Considerations John W. Wilson, MD Associate Professor of Medicine Division of Infectious Diseases Mayo Clinic, Rochester MN Mayo Clinic Center for Tuberculosis
Drug Resistant Tuberculosis: Pearls and other Considerations John W. Wilson, MD Associate Professor of Medicine Division of Infectious Diseases Mayo Clinic, Rochester MN Mayo Clinic Center for Tuberculosis
Can mutation detection accurately predict XDR- TB: study from a tertiary care centre India
 JCM Accepts, published online ahead of print on 2 February 2011 J. Clin. Microbiol. doi:10.1128/jcm.00113-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 2 February 2011 J. Clin. Microbiol. doi:10.1128/jcm.00113-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
Mono- versus Bitherapy for Management of HAP/VAP in the ICU
 Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
BRUCELLOSIS BRUCELLOSIS. CPMP/4048/01, rev. 3 1/7 EMEA 2002
 BRUCELLOSIS CPMP/4048/01, rev. 3 1/7 General points on treatment Four species are pathogenic to man: B. melitenis (acquired from goats), B. suis (pigs), B. abortus (cattle) and B. canis (dogs). The bacteria
BRUCELLOSIS CPMP/4048/01, rev. 3 1/7 General points on treatment Four species are pathogenic to man: B. melitenis (acquired from goats), B. suis (pigs), B. abortus (cattle) and B. canis (dogs). The bacteria
Sterilizing Activities of Fluoroquinolones against Rifampin-Tolerant Populations of Mycobacterium tuberculosis
 ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Feb. 2003, p. 653 657 Vol. 47, No. 2 0066-4804/03/$08.00 0 DOI: 10.1128/AAC.47.2.653 657.2003 Copyright 2003, American Society for Microbiology. All Rights Reserved.
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Feb. 2003, p. 653 657 Vol. 47, No. 2 0066-4804/03/$08.00 0 DOI: 10.1128/AAC.47.2.653 657.2003 Copyright 2003, American Society for Microbiology. All Rights Reserved.
Period of study: 12 Nov 2002 to 08 Apr 2004 (first subject s first visit to last subject s last visit)
") Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Non-Tuberculous Mycobacterial Pulmonary Disease Diagnosis and Management Jakko van Ingen, MD, PhD
 Non-Tuberculous Mycobacterial Pulmonary Disease (NTM-PD) 1 Radbound University Nihmegen Medical Center Milestones in NTM research 1980s: Nodular bronchiectatic lung disease Lady Windermere syndrome 1882-1890
Non-Tuberculous Mycobacterial Pulmonary Disease (NTM-PD) 1 Radbound University Nihmegen Medical Center Milestones in NTM research 1980s: Nodular bronchiectatic lung disease Lady Windermere syndrome 1882-1890
Tuberculosis (TB) is an infectious disease that is preventable, treatable
 is an infectious disease that is preventable, treatable") original article Multidrug-resistant tuberculosis: Treatment and outcomes of 93 patients Sarah K Brode MD FRCPC 1,2, Robert Varadi MDCM FRCPC 1,2, Jane McNamee RN(EC) 1, Nina Malek 1, Sharon Stewart MSW
original article Multidrug-resistant tuberculosis: Treatment and outcomes of 93 patients Sarah K Brode MD FRCPC 1,2, Robert Varadi MDCM FRCPC 1,2, Jane McNamee RN(EC) 1, Nina Malek 1, Sharon Stewart MSW
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia. Po-Ren Hsueh. National Taiwan University Hospital
 Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Fluoroquinolones for the treatment and prevention of multidrug-resistant tuberculosis
 INT J TUBERC LUNG DIS 20(12):S42 S47 Q 2016 The Union http://dx.doi.org/10.5588/ijtld.16.0117 MDR-TB TRIALS LANDSCAPE SUPPLEMENT Fluoroquinolones for the treatment and prevention of multidrug-resistant
INT J TUBERC LUNG DIS 20(12):S42 S47 Q 2016 The Union http://dx.doi.org/10.5588/ijtld.16.0117 MDR-TB TRIALS LANDSCAPE SUPPLEMENT Fluoroquinolones for the treatment and prevention of multidrug-resistant
Dr Sharanjit Dhoot. Chelsea and Westminster Hospital, London. 18 th Annual Conference of the British HIV Association (BHIVA)
") 18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
18 th Annual Conference of the British HIV Association (BHIVA) Dr Sharanjit Dhoot Chelsea and Westminster Hospital, London 18-20 April 2012, The International Convention Centre, Birmingham 18 th Annual
Treatment of Slowly Growing NTM Infections
 Treatment of Slowly Growing NTM Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory Committee Insmed
Treatment of Slowly Growing NTM Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Investigator Insmed (inhaled liposomal amikacin) Advisory Committee Insmed
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Section 6.2.4: Antituberculosis Medicines Application for moving streptomycin to complementary list
 Section 6.2.4: Antituberculosis Medicines Application for moving streptomycin to complementary list Stop TB Department World Health Organization Summary According to the recent guideline published in 2010
Section 6.2.4: Antituberculosis Medicines Application for moving streptomycin to complementary list Stop TB Department World Health Organization Summary According to the recent guideline published in 2010
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007
 Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
number Done by Corrected by Doctor Dr Hamed Al-Zoubi
 number 8 Done by Corrected by Doctor Dr Hamed Al-Zoubi 25 10/10/2017 Antibacterial therapy 2 د. حامد الزعبي Dr Hamed Al-Zoubi Antibacterial therapy Figure 2/ Antibiotics target Inhibition of microbial
number 8 Done by Corrected by Doctor Dr Hamed Al-Zoubi 25 10/10/2017 Antibacterial therapy 2 د. حامد الزعبي Dr Hamed Al-Zoubi Antibacterial therapy Figure 2/ Antibiotics target Inhibition of microbial
COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS
 The European Agency for the Evaluation of Medicinal Products Veterinary Medicines and Information Technology EMEA/MRL/728/00-FINAL April 2000 COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS STREPTOMYCIN AND
The European Agency for the Evaluation of Medicinal Products Veterinary Medicines and Information Technology EMEA/MRL/728/00-FINAL April 2000 COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS STREPTOMYCIN AND
Lefamulin: a novel pleuromutilin antibiotic class George Dimopoulos MD, PhD, FCCP, FCCM, FECMM
 : a novel pleuromutilin antibiotic class George Dimopoulos MD, PhD, FCCP, FCCM, FECMM Department of Critical Care, University Hospital ATTIKON National and Kapodistrian University of Athens, Medical School
: a novel pleuromutilin antibiotic class George Dimopoulos MD, PhD, FCCP, FCCM, FECMM Department of Critical Care, University Hospital ATTIKON National and Kapodistrian University of Athens, Medical School
COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE
 European Medicines Agency Veterinary Medicines and Inspections EMEA/CVMP/211249/2005-FINAL July 2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE DIHYDROSTREPTOMYCIN (Extrapolation to all ruminants)
European Medicines Agency Veterinary Medicines and Inspections EMEA/CVMP/211249/2005-FINAL July 2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE DIHYDROSTREPTOMYCIN (Extrapolation to all ruminants)
What does multiresistance actually mean? Yohei Doi, MD, PhD University of Pittsburgh
 What does multiresistance actually mean? Yohei Doi, MD, PhD University of Pittsburgh Disclosures Merck Research grant Clinical context of multiresistance Resistance to more classes of agents Less options
What does multiresistance actually mean? Yohei Doi, MD, PhD University of Pittsburgh Disclosures Merck Research grant Clinical context of multiresistance Resistance to more classes of agents Less options
GUIDE TO INFECTION CONTROL IN THE HOSPITAL. Antibiotic Resistance
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 4: Antibiotic Resistance Author M.P. Stevens, MD, MPH S. Mehtar, MD R.P. Wenzel, MD, MSc Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 4: Antibiotic Resistance Author M.P. Stevens, MD, MPH S. Mehtar, MD R.P. Wenzel, MD, MSc Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
ETX2514: Responding to the global threat of nosocomial multidrug and extremely drug resistant Gram-negative pathogens
 ETX2514: Responding to the global threat of nosocomial multidrug and extremely drug resistant Gram-negative pathogens Ruben Tommasi, PhD Chief Scientific Officer ECCMID 2017 April 24, 2017 Vienna, Austria
ETX2514: Responding to the global threat of nosocomial multidrug and extremely drug resistant Gram-negative pathogens Ruben Tommasi, PhD Chief Scientific Officer ECCMID 2017 April 24, 2017 Vienna, Austria
Summary of unmet need guidance and statistical challenges
 Summary of unmet need guidance and statistical challenges Daniel B. Rubin, PhD Statistical Reviewer Division of Biometrics IV Office of Biostatistics, CDER, FDA 1 Disclaimer This presentation reflects
Summary of unmet need guidance and statistical challenges Daniel B. Rubin, PhD Statistical Reviewer Division of Biometrics IV Office of Biostatistics, CDER, FDA 1 Disclaimer This presentation reflects
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Typhoid fever - priorities for research and development of new treatments
 Typhoid fever - priorities for research and development of new treatments Isabela Ribeiro, Manica Balasegaram, Christopher Parry October 2017 Enteric infections Enteric infections vary in symptoms and
Typhoid fever - priorities for research and development of new treatments Isabela Ribeiro, Manica Balasegaram, Christopher Parry October 2017 Enteric infections Enteric infections vary in symptoms and
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days
 Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
ANTHRAX. INHALATION, INTESTINAL and CUTANEOUS ANTHRAX
 INHALATION, INTESTINAL and CUTANEOUS ANTHRAX CPMP/4048/01, rev. 3 1/7 General points on treatment Anthrax is an acute infectious disease caused by Bacillus anthracis, that may be infecting man via cutaneous
INHALATION, INTESTINAL and CUTANEOUS ANTHRAX CPMP/4048/01, rev. 3 1/7 General points on treatment Anthrax is an acute infectious disease caused by Bacillus anthracis, that may be infecting man via cutaneous
Multidrug resistant tuberculosis treatment in the Indian private sector: Results from a tertiary referral private hospital in Mumbai
 Original Article Multidrug resistant tuberculosis treatment in the Indian private sector: Results from a tertiary referral private hospital in Mumbai Zarir F. Udwadia, Gautam Moharil Department of Pulmonology,
Original Article Multidrug resistant tuberculosis treatment in the Indian private sector: Results from a tertiary referral private hospital in Mumbai Zarir F. Udwadia, Gautam Moharil Department of Pulmonology,
ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective
 : The Belgian perspective") ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective Antwerpen 8 november 2002 Yvan Valcke MD PhD AZ Maria Middelares Sint-Niklaas ACUTE EXACERBATIONS of COPD (AE-COPD) Treatment of AECB Role
ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective Antwerpen 8 november 2002 Yvan Valcke MD PhD AZ Maria Middelares Sint-Niklaas ACUTE EXACERBATIONS of COPD (AE-COPD) Treatment of AECB Role
The role of moxifloxacin in tuberculosis therapy
 CLINICAL YEAR IN REVIEW TUBERCULOSIS The role of moxifloxacin in tuberculosis therapy Stephen H. Gillespie Affiliation: School of Medicine, University of St Andrews, St Andrews, UK. Correspondence: Stephen
CLINICAL YEAR IN REVIEW TUBERCULOSIS The role of moxifloxacin in tuberculosis therapy Stephen H. Gillespie Affiliation: School of Medicine, University of St Andrews, St Andrews, UK. Correspondence: Stephen
AMR Industry Alliance Antibiotic Discharge Targets
 AMR Industry Alliance Antibiotic Discharge Targets List of Predicted No-Effect Concentrations (PNECs) The members of the AMR Industry Alliance have developed a unified approach to establishing discharge
AMR Industry Alliance Antibiotic Discharge Targets List of Predicted No-Effect Concentrations (PNECs) The members of the AMR Industry Alliance have developed a unified approach to establishing discharge
DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY*
 44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
Outline. Antimicrobial resistance. Antimicrobial resistance in gram negative bacilli. % susceptibility 7/11/2010
 Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Palpasa Kansakar, Geeta Shakya, Nisha Rijal, Basudha Shrestha
 In-vitro resistance of Salmonella Typhi and Paratyphi A raises concern on the use of older fluroquinolones in the empiric treatment of enteric fever in Nepal Palpasa Kansakar, Geeta Shakya, Nisha Rijal,
In-vitro resistance of Salmonella Typhi and Paratyphi A raises concern on the use of older fluroquinolones in the empiric treatment of enteric fever in Nepal Palpasa Kansakar, Geeta Shakya, Nisha Rijal,
Antibacterials. Recent data on linezolid and daptomycin
 Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
ESCMID Online Lecture Library. by author
 Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS
 The European Agency for the Evaluation of Medicinal Products Veterinary Medicines and Inspections EMEA/CVMP/627/01-FINAL COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS GUIDELINE FOR THE DEMONSTRATION OF EFFICACY
The European Agency for the Evaluation of Medicinal Products Veterinary Medicines and Inspections EMEA/CVMP/627/01-FINAL COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS GUIDELINE FOR THE DEMONSTRATION OF EFFICACY
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Antimicrobial Cycling. Donald E Low University of Toronto
 Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Animal models and PK/PD. Examples with selected antibiotics
 Animal models and PK/PD PD Examples with selected antibiotics Examples of animal models Amoxicillin Amoxicillin-clavulanate Macrolides Quinolones Andes D, Craig WA. AAC 199, :375 Amoxicillin in mouse thigh
Animal models and PK/PD PD Examples with selected antibiotics Examples of animal models Amoxicillin Amoxicillin-clavulanate Macrolides Quinolones Andes D, Craig WA. AAC 199, :375 Amoxicillin in mouse thigh
Which agents should we use for the treatment of multidrug-resistant Mycobacterium tuberculosis? Giovanni Di Perri* and Stefano Bonora
 Journal of Antimicrobial Chemotherapy (2004) 54, 593 602 DOI: 10.1093/jac/dkh377 Advance Access publication 28 July 2004 Which agents should we use for the treatment of multidrug-resistant Mycobacterium
Journal of Antimicrobial Chemotherapy (2004) 54, 593 602 DOI: 10.1093/jac/dkh377 Advance Access publication 28 July 2004 Which agents should we use for the treatment of multidrug-resistant Mycobacterium
Creating a global community for clinical drug repurposing and development. Leonard Sacks Center for drug evaluation and research FDA
 Creating a global community for clinical drug repurposing and development Leonard Sacks Center for drug evaluation and research FDA Neglected tropical diseases 1) Repurposing and developing new drugs 2)
Creating a global community for clinical drug repurposing and development Leonard Sacks Center for drug evaluation and research FDA Neglected tropical diseases 1) Repurposing and developing new drugs 2)