Tropical infections caused by Staphylococcus aureus
|
|
|
- Lucinda Spencer
- 5 years ago
- Views:
Transcription
1 Tropical infections caused by Staphylococcus aureus Michael Ellis, MD Infectious Diseases Division Uniformed Services University of the Health Sciences February 2015



2 Introduction Tropical Pyomyositis Cutaneous infections Prevention Bites Tropical infections caused by S. aureus Outline


3 S. aureus Microbiology Gram-positive cocci Grape-like clusters on gram stain Catalase positive Coagulase positive β-hemolysis on sheep blood agar MRSA Identified based on oxacillin susceptibility Can be identified using chromogenic agar Rapid identification using PCR to detect meca


4
")
5 Hospital-associated MRSA Risk groups Zyvox (linezolid) advertisement.

6 Community-associated MRSA Risk groups Household contacts of CA-MRSA infected persons Athletes Children Prison inmates Soldiers MSM IVDA N Engl J Med. 2007;357: 380.
7 Epidemiological and clinical characteristics Occurs in the community or <48-72h after admission Absence of traditional risk factors for MRSA Primarily cause skin and soft tissue infection (SSTI) Molecular characteristics What is CA-MRSA? Methods of description Presence of resistance and virulence factors Staphylococcal cassette chromosome mec (SCCmec) type IV Panton-Valentine leukocidin (PVL) Pulsed-field types (PFTs) USA300 Predominant strain in U.S. Clin Infect Dis. 2008;46: S368.

8 Community-associated MRSA Molecular characteristics PFT Location SCCmec USA300 Community Type IV USA400 Community Type IV USA100 Hospital Type II USA200 Hospital Type II Adapted from J Clin Microbiol. 2003;41:5113.
9 Tropical Pyomyositis
10 Tropical pyomyositis Pathogenesis Pyomyositis is a primary infection of skeletal muscle Does not arise from contiguous site Result of transient hematogenous seeding Usually associated with abscess formation Pathogenesis is poorly understood Associated risk factors Trauma Immunodeficiency (but most are healthy) Injection drug use Concomitant parasitic infection (e.g., toxocara) S. aureus strain virulence
11 25%-50% of pyomyositis associated with trauma Includes strenuous exercise Normal skeletal muscle sequesters iron and is relatively resistant to infection Fewer than 1% of S. aureus bacteremia deaths reveal skeletal muscle abscesses Damaged muscle Increased perfusion Hematoma formation Provides binding site Provides iron for bacteria Tropical pyomyositis Pathogenesis-risk factors
12 HIV Tropical pyomyositis Pathogenesis- risk factors Noted in African studies as significant independent risk factor T-cell dysfunction HAART toxicity Primary HIV myopathy Increased S. aureus carriage Others- DM, sickle cell, cirrhosis Injection drug use Frequent S. aureus bacteremia Increased S. aureus carriage
13 Accounts for 1-4% of hospital admissions in tropical countries Increasingly reported in temperate regions Likely a reflection of the emergence of CA-MRSA More common in males (1.5:1) Peak age groups 2-5 years years Tropical pyomyositis Epidemiology Peak season in the tropics appears to be July-September
14 Tropical pyomyositis Microbiology Staphylococcus aureus- 90% CA-MRSA has emerged as an important pathogen Group A streptococcus- 1-5% Other pathogens Non-Group A strep Pneumococcus Gram negative enteric (e.g., E. coli) Mycobacterial (TB) Polymicrobial
15 Tropical pyomyositis Clinical manifestations Presents with fever and localized cramping muscle pain Usually single muscle group May be multiple in up to 20% of cases Lower extremities- but any muscle group possible Described in 3 clinical stages Stage 1 (invasive)- Stage 2 (suppurative) Most patients present during this stage Stage 3 (late)- systemic toxicity/infection
16 Stage 1 (invasive) Low-grade fever, mild leukocytosis Woody muscle induration Stage 2 (suppurative) days after initial symptoms Fever, high leukocytosis Exquisite muscle tenderness, edema, and often fluctuance Aspirate will yield purulent material Stage 3 (late)- systemic toxicity/infection Septic shock Endocarditis Pneumonia Abscesses Tropical pyomyositis Clinical manifestations
17 Stage 1 (invasive) Low-grade fever, mild leukocytosis Woody muscle induration Stage 2 (suppurative) days after initial symptoms Fever, high leukocytosis Exquisite muscle tenderness, edema, and often fluctuance Aspirate will yield purulent material Stage 3 (late)- systemic toxicity/infection Septic shock Endocarditis Pneumonia Abscesses Tropical pyomyositis Clinical manifestations

18 Left posterior thigh- stage 2 pyomyositis J Amer Acad Dermatol. 2004;51: 308.

19 CT fluid collection- stage 2 pyomyositis J Amer Acad Dermatol. 2004;51: 308.
20 Stage 1 (invasive) Low-grade fever, mild leukocytosis Woody muscle induration Stage 2 (suppurative) days after initial symptoms Fever, high leukocytosis Exquisite muscle tenderness, edema, and often fluctuance Aspirate will yield purulent material Stage 3 (late)- systemic toxicity/infection Septic shock Endocarditis Pneumonia Abscesses Tropical pyomyositis Clinical manifestations

21 Necrotizing pneumonia Clin Infect Dis. 2005;40: 100.
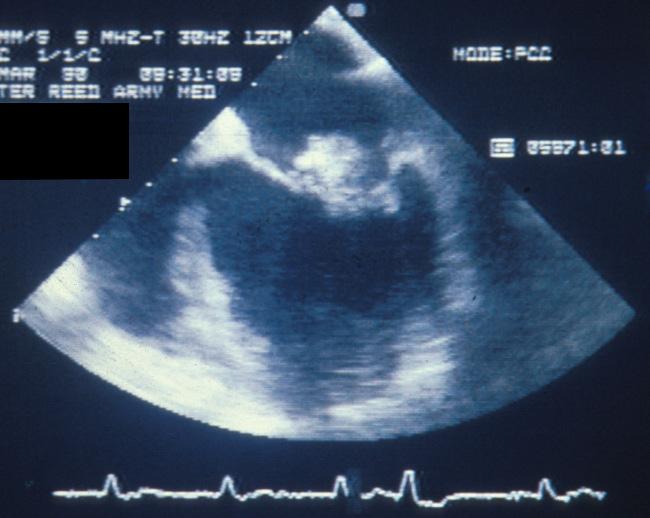
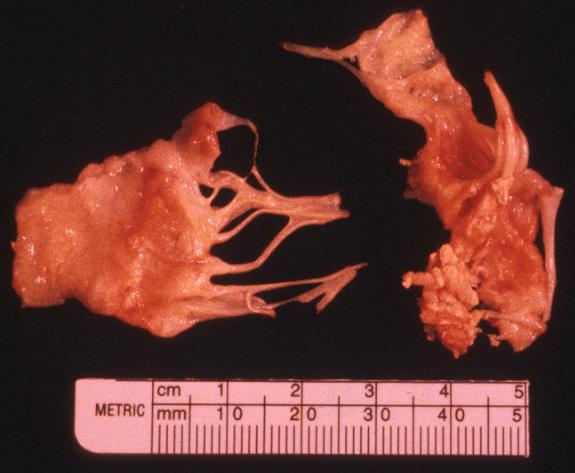
22 Endocarditis

23 Septic emboli Clin Infect Dis. 2005;40: 100.
24 Tropical pyomyositis Differential diagnosis Muscle contusion Cellulitis DVT Osteomyelitis Septic arthritis Neoplasm (osteosarcoma) Clostridial myonecrosis Necrotizing fasciitis Trichinosis Cysticercosis
25 All patients should be evaluated for endocarditis Radiography MRI (preferred), US, CT Diagnostic guided drainage prior to antibiotics Labs Leukocytosis Elevated ESR/CRP CPK usually normal Cultures Tropical pyomyositis Diagnosis Blood cultures positive in at least 10% of cases Positive in 30% of temperate pyomyositis (due to technique)

26 Coronal CT image of psoas abscess Infect Dis Clin NA. 2005;19: 981.
27 Stage 1 (invasive)- antibiotics alone may be effective Stage 2 and 3 Drainage- percutaneous or surgical Antibiotics (at least 2-3 weeks duration) Vancomycin Oxacillin Cefazolin Tropical pyomyositis Treatment Add Gram-negative and anaerobic coverage for immunocompromised

28 Left hip- stage 2 pyomyositis J Amer Acad Dermatol. 2004;51: 308.

29 Left hip- stage 2 pyomyositis- post drainage J Amer Acad Dermatol. 2004;51: 308.
30 Cutaneous S. aureus infections

31 Folliculitis Furuncles (abscesses) May be multiple Recurrence is common Outbreak settings/families Purulent cellulitis Associated with abscess/ulcer Nonpurulent cellulitis Cutaneous S. aureus infections Manifestations Contribution is unknown

32 Folliculitis- leg 32

33 Cellulitis- knee 33

34 Abscess-foot

35 Abscess- knee

36 Abscess- axilla
37 Int J Infect Dis. 2008; 12: 593.
38 Dermatologic conditions in travelers Epidemiology GeoSentinel Surveillance Network data encounters for dermatological complaints 18% of all encounters Skin lesions in returning travelers Cutaneous larvae migrans (9.8%) Insect bite (8.2%) Skin abscess (7.7%) Infected insect bite (6.8%) Int J Infect Dis. 2008; 12: 593.

39 Infect Dis Clin Pract. 2005;13:139.
40 65-year-old man who had returned from 4 wks in DRC Developed R leg swelling and pain during return trip CA-MRSA leg abscess CA-MRSA bacteremia CA-MRSA genotype, PVL+, SCCmec IV Infect Dis Clin Pract. 2005;13: 139.
41 Military treatment facility-baghdad SSTI abscesses 26 abscesses cultured 22/26 S. aureus 70% MRSA Mil Med. 2009;174: 408.
42 J Trauma. 2010;69: S1.
43 Treatment
44 Clin Infect Dis. 2014; epub.
45

46 SSTI management Furunculosis
47 Incision and drainage- most important intervention Antimicrobial therapy recommended for: Severe or extensive disease Signs/symptoms of systemic illness (Fever, tachy, leukocytosis) Rapid progression Extremes of age Comorbid conditions/immunosuppression Abscess on face, hand, groin Send specimen for culture Duration-5 days therapy SSTI management Furunculosis-outpatient Timely follow-up (24-72 hours) Clin Infect Dis. 2014; epub.

48 Study: 161 Pediatric patients (80% MRSA) I&D + TMP/SMX vs. I&D + placebo for 10 days Placebo cure: 95% TMP/SMX cure: 96% difference NS Ann Emerg Med
49 Nonpurulent cellulitis SSTI management Cellulitis Etiology- β-hemolytic streptococci (less likely S. aureus) Empirical coverage for MRSA: Evidence of MRSA MRSA colonization Penetrating trauma Immune-compromised Systemic toxicity Timely follow-up (24-72 hours) Clin Infect Dis. 2014; epub.
50 Adjunctive measures Elevate and rest affected limb Treated tinea pedis Address pre-disposing conditions Extremity edema Dermatological conditions SSTI management Cellulitis Clin Infect Dis. 2014; epub.
51 Study: 153 patients (children and adults) nonpurulent cellulitis Cephalexin + TMP/SMX vs. Cephalexin + placebo 14d Placebo cure: 82% TMP/SMX cure: 85% difference NS No benefit to MRSA coverage Clin Infect Dis. 2013;69:
52 S. aureus prevention
53
54
55 Adhesive bandages Gauze Adhesive tape Elastic bandage Antiseptic Cotton swabs Antibacterial ointment 1% hyrocortisone cream Moleskin Thermometer SSTI Prevention Basic First Aid kit CDC Yellow Book. 2010, pg 233.
56 Bites Human Microbiology Aeorobic & anaerobic bacteria (oral and skin flora) Eikenella corrodens must be covered Management/prophylaxis Surgical evaluation (consider primary closure for face- specialist) Emobilize/splint Amox/clav or TMP-SMX + clindamycin Tetanus consideration Treatment of infection Obtain cultures IV antibiotics (Amp-sulbactam, Pip-taz, FQN+clinda)
57 Bites Dog Microbiology- 5% become infected Pasteurella spp, staph, strep, anaerobes Capnocytophaga canimorsus (asplenic, immune suppressed) Management/prophylaxis Surgical evaluation (consider form of closure) Emobilize/splint Severe- face, genitals, immune suppressed, crush Amox/clav or TMP-SMX + clindamycin (1 st dose IV) Tetanus and rabies consideration Treatment of infection Obtain cultures IV antibiotics (Amp-sulbactam, Pip-taz)
58 Bites Cat Microbiology- 80% become infected Pasteurella multocida, staph, strep, anaerobes Develop infection within 24 hours Management/prophylaxis- all get antibiotics! Surgical evaluation (consider form of closure) X-ray Emobilize/splint Amox/clav or doxycycline, cefuroxime (1 st dose IV) Tetanus and rabies consideration Treatment of infection (high risk for bone/joint) Obtain cultures IV antibiotics (Amp-sulbactam, FQN + metro, carbapenem)
59 Questions Michael Ellis, MD LTC, MC Department of Medicine Infectious Diseases Division Uniformed Services University of the Health Sciences 4301 Jones Bridge Road Bethesda, MD (301)
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust
 PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections. Skin & Soft Tissue Infections (SSTI)
 Skin & Soft Tissue Infections. Skin & Soft Tissue Infections (SSTI)") Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections 2007 Abscess Cellulitis Bradley W Frazee, MD, FACEP Dept of Emergency Medicine Alameda County Medical Center - Highland Hospital Associate
Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections 2007 Abscess Cellulitis Bradley W Frazee, MD, FACEP Dept of Emergency Medicine Alameda County Medical Center - Highland Hospital Associate
Skin and Soft Tissue Infections Emerging Therapies and 5 things to know
 2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections
 Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Methicillin-Resistant Staphylococcus aureus
 Methicillin-Resistant Staphylococcus aureus By Karla Givens Means of Transmission and Usual Reservoirs Staphylococcus aureus is part of normal flora and can be found on the skin and in the noses of one
Methicillin-Resistant Staphylococcus aureus By Karla Givens Means of Transmission and Usual Reservoirs Staphylococcus aureus is part of normal flora and can be found on the skin and in the noses of one
MRSA Outbreak in Firefighters
 MRSA Outbreak in Firefighters Angie Carranza Munger, MD Resident, Occupational and Environmental Medicine The University of Colorado, Denver and National Jewish Health Candidate, Masters of Public Health
MRSA Outbreak in Firefighters Angie Carranza Munger, MD Resident, Occupational and Environmental Medicine The University of Colorado, Denver and National Jewish Health Candidate, Masters of Public Health
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Infections caused by Methicillin-Resistant Staphylococcus
 MRSA infections are no longer limited to hospitals. An infectious disease specialist offers insight on what this means for dermatologists. By Robert S. Jones, DO, Reading, PA Infections caused by Methicillin-Resistant
MRSA infections are no longer limited to hospitals. An infectious disease specialist offers insight on what this means for dermatologists. By Robert S. Jones, DO, Reading, PA Infections caused by Methicillin-Resistant
Ca-MRSA Update- Hand Infections. Washington Hand Society September 19, 2007
 Ca-MRSA Update- Hand Infections Washington Hand Society September 19, 2007 Resistant Staph. Aureus Late 1940 s -50% S.Aureus resistant to PCN 1957-80/81 strain- of S.A. highly virulent and easily transmissible
Ca-MRSA Update- Hand Infections Washington Hand Society September 19, 2007 Resistant Staph. Aureus Late 1940 s -50% S.Aureus resistant to PCN 1957-80/81 strain- of S.A. highly virulent and easily transmissible
5/17/2012 DISCLOSURES OBJECTIVES CONTEMPORARY PEDIATRICS
 CONTEMPORARY PEDIATRICS Surgical Management of MRSA Soft Tissue Infections John M. Draus, Jr., M.D. Assistant Professor of Surgery and Pediatrics Kentucky Children s Hospital University of Kentucky DISCLOSURES
CONTEMPORARY PEDIATRICS Surgical Management of MRSA Soft Tissue Infections John M. Draus, Jr., M.D. Assistant Professor of Surgery and Pediatrics Kentucky Children s Hospital University of Kentucky DISCLOSURES
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Mrsa abscess and cellulitis
 Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
S aureus infections: outpatient treatment. Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium
 S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
Prevalence & Risk Factors For MRSA. For Vets
 For Vets General Information Staphylococcus aureus is a Gram-positive, aerobic commensal bacterium of humans that is carried in the anterior nares of approximately 30% of the general population. It is
For Vets General Information Staphylococcus aureus is a Gram-positive, aerobic commensal bacterium of humans that is carried in the anterior nares of approximately 30% of the general population. It is
Disclosures. Consider This Case. Objectives. Consequences of Bites. Animal Bites: What to Do and What to Avoid. Animal Bites: Epidemiology
 Animal Bites: What to Do and What to Avoid Meg Fisher, MD Medical Director Disclosures I have no disclosures I do not plan to discuss off label uses of drugs Objectives Manage a child who is bitten Discuss
Animal Bites: What to Do and What to Avoid Meg Fisher, MD Medical Director Disclosures I have no disclosures I do not plan to discuss off label uses of drugs Objectives Manage a child who is bitten Discuss
Cellulitis. Assoc Prof Mark Thomas. Conference for General Practice Auckland Saturday 28 July 2018
 Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
M R S A. Methicillin-Resistant Staphylococcus aureus. The Facts
 M R S A Methicillin-Resistant Staphylococcus aureus The Facts Michael Parry, M.D. Director of Infectious Diseases and Microbiology Stamford Hospital January 24, 2008 Introduction to Staph aureus Staphylococcus
M R S A Methicillin-Resistant Staphylococcus aureus The Facts Michael Parry, M.D. Director of Infectious Diseases and Microbiology Stamford Hospital January 24, 2008 Introduction to Staph aureus Staphylococcus
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Source: Portland State University Population Research Center (
 Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Risk factors? Insect bites? Hygiene? Household crowding Health literacy
 Recurrent boils Commonest sites face, neck, armpits, shoulders, and buttocks (bottom) infection of the hair root or sweat pore Occur in otherwise healthy people (higher rates in diabetics, eczema, iron
Recurrent boils Commonest sites face, neck, armpits, shoulders, and buttocks (bottom) infection of the hair root or sweat pore Occur in otherwise healthy people (higher rates in diabetics, eczema, iron
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Methicillin Resistant Staphylococcus Aureus (MRSA) The drug resistant `Superbug that won t die
 The drug resistant `Superbug that won t die") Methicillin Resistant Staphylococcus Aureus (MRSA) The drug resistant `Superbug that won t die Michael A. Miller, MD Assistant Professor of Pediatrics -Jacksonville OBJECTIVES 1. Understand the basic microbiology
Methicillin Resistant Staphylococcus Aureus (MRSA) The drug resistant `Superbug that won t die Michael A. Miller, MD Assistant Professor of Pediatrics -Jacksonville OBJECTIVES 1. Understand the basic microbiology
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Overview Management of Skin and Soft Tissue Infections in the MRSA Era
 Overview Management of Skin and Soft Tissue Infections in the MRSA Era April 2011 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Management of Recurrent SSTIs Necrotizing soft
Overview Management of Skin and Soft Tissue Infections in the MRSA Era April 2011 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Management of Recurrent SSTIs Necrotizing soft
Replaces:04/14/16. Formulated: 1997 SKIN AND SOFT TISSUE INFECTION
 Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
CHAPTER 18 THE COCCI OF MEDICAL IMPORTANCE. Learning Objectives
 CHAPTER 18 THE COCCI OF MEDICAL IMPORTANCE Gram-positive and gram-negative cocci that cause infection are presented. The difference between commensal and pathogenic strains is explained, because many of
CHAPTER 18 THE COCCI OF MEDICAL IMPORTANCE Gram-positive and gram-negative cocci that cause infection are presented. The difference between commensal and pathogenic strains is explained, because many of
22/09/2010. Laboratory 2a + b Staphylococci and Streptococci
 Laboratory 2a + b Staphylococci and Streptococci 1 Hamster: To be or not to be..!? (a play on Ham-let!) Summary on Exercise 1 (Lab 2a) Big colony heavy growth, color? Double-zone hly CAT and Tube Coag
Laboratory 2a + b Staphylococci and Streptococci 1 Hamster: To be or not to be..!? (a play on Ham-let!) Summary on Exercise 1 (Lab 2a) Big colony heavy growth, color? Double-zone hly CAT and Tube Coag
Diagnosis and Management of Skin and Soft-tissue Infections
 Diagnosis and Management of Skin and Soft-tissue Infections Skin and soft tissue infections (SSTIs), are referred as skin and skin structure infections. These infections also represent a group of infections
Diagnosis and Management of Skin and Soft-tissue Infections Skin and soft tissue infections (SSTIs), are referred as skin and skin structure infections. These infections also represent a group of infections
MRSA Background. New Challenges From an Old Foe. MRSA Demographics. Comparison of Types of MRSA CA-MRSA HA-MRSA
 Winter Clinical 2017 : MRSA Update Whitney A. High, MD, JD, Meng whitney.high@ucdenver.edu Associate Professor, Dermatology & Pathology Director of Dermatopathology University of Colorado School of Medicine
Winter Clinical 2017 : MRSA Update Whitney A. High, MD, JD, Meng whitney.high@ucdenver.edu Associate Professor, Dermatology & Pathology Director of Dermatopathology University of Colorado School of Medicine
CA-MRSA lesions: What works, what doesn t
 For mass reproduction, content licensing and permissions contact Dowden Health Media. FAMILY David McBride, MD University Student Health Services and the Department of Family Medicine, Boston University
For mass reproduction, content licensing and permissions contact Dowden Health Media. FAMILY David McBride, MD University Student Health Services and the Department of Family Medicine, Boston University
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Methicillin Resistant Staphylococcus aureus:
 Methicillin Resistant Staphylococcus aureus: Action-Oriented Guidance for Community-Based Prevention Jackie Dawson, PhD Public Health Epidemiologist Chelan, Douglas, Grant, Kittitas, & Okanogan Counties
Methicillin Resistant Staphylococcus aureus: Action-Oriented Guidance for Community-Based Prevention Jackie Dawson, PhD Public Health Epidemiologist Chelan, Douglas, Grant, Kittitas, & Okanogan Counties
Development of Drugs for Skin Infections
 EFPIA - Skin Infection comments 1 Development of Drugs for Skin Infections John H Rex, MD EFPIA - Skin Infection comments 2 Skin Infections Significant recent debate: Acceptable forms: A focus on fever
EFPIA - Skin Infection comments 1 Development of Drugs for Skin Infections John H Rex, MD EFPIA - Skin Infection comments 2 Skin Infections Significant recent debate: Acceptable forms: A focus on fever
Bacterial skin infection
 D i v i s i o n o f P e d i a t r i c E m e r g e n c y M e d i c i n e P a g e 1 Bacterial skin infection Cellulitis w/o abscess Abscess Deep tissue involvement Multiple abscesses Perirectal Anterior
D i v i s i o n o f P e d i a t r i c E m e r g e n c y M e d i c i n e P a g e 1 Bacterial skin infection Cellulitis w/o abscess Abscess Deep tissue involvement Multiple abscesses Perirectal Anterior
Burn Infection & Laboratory Diagnosis
 Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
Staph Cases. Case #1
 Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Dirty Wounds. Christopher M. Ziebell, MD, FACEP
 Dirty Wounds Christopher M. Ziebell, MD, FACEP Types Fresh Water Salt Water Bites Cats Humans Dogs and other mammals Freshwater Trauma Recognize this finger? Lindsey Lohan Microbiology Usual suspects:
Dirty Wounds Christopher M. Ziebell, MD, FACEP Types Fresh Water Salt Water Bites Cats Humans Dogs and other mammals Freshwater Trauma Recognize this finger? Lindsey Lohan Microbiology Usual suspects:
MRSA. ( Staphylococcus aureus; S. aureus ) ( community-associated )
 ( community-associated )") 005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
Meropenem for all? Midge Asogan ICU Fellow (also ID AT)
") Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Skin & Soft Tissue Infections: It's More Than Just MRSA
 28 Osteopathic Family Physician Volume 11, No. 1 January/February, 2019 Osteopathic Family Physician (2019) 28-32 REVIEW ARTICLE Skin & Soft Tissue Infections: It's More Than Just Matthew J. Hadfield,
28 Osteopathic Family Physician Volume 11, No. 1 January/February, 2019 Osteopathic Family Physician (2019) 28-32 REVIEW ARTICLE Skin & Soft Tissue Infections: It's More Than Just Matthew J. Hadfield,
Skin & Soft Tissue Infections (SSTIs)
") Skin & Soft Tissue Infections (SSTIs) Marnie Peterson, Pharm.D., Ph.D. College of Pharmacy peter377@umn.edu (612) 626-4388 SSTIs Objectives To classify types of skin infections To present a case of cellulitis
Skin & Soft Tissue Infections (SSTIs) Marnie Peterson, Pharm.D., Ph.D. College of Pharmacy peter377@umn.edu (612) 626-4388 SSTIs Objectives To classify types of skin infections To present a case of cellulitis
Staphylococcus aureus
 Staphylococcus aureus Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins Quintessential Pathogen? Nizet
Staphylococcus aureus Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins Quintessential Pathogen? Nizet
Antibiotic Stewardship
 Antibiotic Stewardship Nick Zaksek Pharm D., BCPS AQ-ID Infectious Disease POMA 2019 1 Disclosures None 2 Objectives Practice good Antibiotic stewardship and foster the notion of antibiotic stewardship
Antibiotic Stewardship Nick Zaksek Pharm D., BCPS AQ-ID Infectious Disease POMA 2019 1 Disclosures None 2 Objectives Practice good Antibiotic stewardship and foster the notion of antibiotic stewardship
Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins
 Staphylococcus aureus Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins Quintessential Pathogen? Nizet
Staphylococcus aureus Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins Quintessential Pathogen? Nizet
CLPNA Pressure Ulcers ecourse: Module 5.6 Quiz II page 1
 CLPNA Pressure Ulcers ecourse: Module 5.6 Quiz II 1. What are the symptoms of an infected wound? a. Fever b. Edema c. Erythema d. Local pain and tenderness e. Induration of wound edge 2. A person with
CLPNA Pressure Ulcers ecourse: Module 5.6 Quiz II 1. What are the symptoms of an infected wound? a. Fever b. Edema c. Erythema d. Local pain and tenderness e. Induration of wound edge 2. A person with
Principles of Antimicrobial Therapy
 Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Clindamycin coverage streptococcus
 Clindamycin coverage streptococcus Oct 12, 2017. While clindamycin and erythromycin were at one time uniformly active against group B streptococci, resistance has been increasing. One large. We assessed
Clindamycin coverage streptococcus Oct 12, 2017. While clindamycin and erythromycin were at one time uniformly active against group B streptococci, resistance has been increasing. One large. We assessed
Community-Associated Methicillin-Resistant Staphylococcus aureus: Review of an Emerging Public Health Concern
 Community-Associated Methicillin-Resistant Staphylococcus aureus: Review of an Emerging Public Health Concern Timothy D. Drews, MD; Jonathan L. Temte, MD, PhD; Barry C. Fox, MD ABSTRACT Methicillin-resistant
Community-Associated Methicillin-Resistant Staphylococcus aureus: Review of an Emerging Public Health Concern Timothy D. Drews, MD; Jonathan L. Temte, MD, PhD; Barry C. Fox, MD ABSTRACT Methicillin-resistant
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how?
 Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
GUIDE TO INFECTION CONTROL IN THE HOSPITAL
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key
TACKLING THE MRSA EPIDEMIC
 TACKLING THE MRSA EPIDEMIC Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine MRSA Trend (HA + CA) in US TSN Database USA (1993-2003) % of MRSA among S. aureus
TACKLING THE MRSA EPIDEMIC Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine MRSA Trend (HA + CA) in US TSN Database USA (1993-2003) % of MRSA among S. aureus
Staphylococcus Aureus
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key
Management of Skin and Soft-Tissue Infection
 Clinical Decisions Interactive at www.nejm.org Management of Skin and Soft-Tissue Infection This interactive feature addresses the diagnosis or management of a clinical case. A case vignette is followed
Clinical Decisions Interactive at www.nejm.org Management of Skin and Soft-Tissue Infection This interactive feature addresses the diagnosis or management of a clinical case. A case vignette is followed
Antimicrobial Resistance and Molecular Epidemiology of Staphylococcus aureus in Ghana
 Antimicrobial Resistance and Molecular Epidemiology of Staphylococcus aureus in Ghana Beverly Egyir, PhD Noguchi Memorial Institute for Medical Research Bacteriology Department, University of Ghana Background
Antimicrobial Resistance and Molecular Epidemiology of Staphylococcus aureus in Ghana Beverly Egyir, PhD Noguchi Memorial Institute for Medical Research Bacteriology Department, University of Ghana Background
Objectives. Basic Microbiology. Patient related. Environment related. Organism related 10/12/2017
 Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
Antibacterials. Recent data on linezolid and daptomycin
 Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Sixth Plague of Egypt. Community MRSA. Epidemiology. Basic Features of Community MRSA. Populations with CA-MRSA
 Community MRSA Henry F. Chambers, M.D. University of California San Francisco San Francisco General Hospital Sixth Plague of Egypt (~ 1200 BCE) So they took soot from a kiln, and stood before Pharaoh;
Community MRSA Henry F. Chambers, M.D. University of California San Francisco San Francisco General Hospital Sixth Plague of Egypt (~ 1200 BCE) So they took soot from a kiln, and stood before Pharaoh;
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate
 Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship
 Curriculum for Antimicrobial Stewardship") General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Copyright 2012 Diabetes In Control, Inc. For permission to reprint, please contact Heather Moran, Production Editor, at
 Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
ISPUB.COM. Animal Bites And Reconstruction. S Saraf INTRODUCTION PATIENTS AND METHODS
 ISPUB.COM The Internet Journal of Plastic Surgery Volume 3 Number 1 S Saraf Citation S Saraf.. The Internet Journal of Plastic Surgery. 2006 Volume 3 Number 1. Abstract Animal bites resulting in significant
ISPUB.COM The Internet Journal of Plastic Surgery Volume 3 Number 1 S Saraf Citation S Saraf.. The Internet Journal of Plastic Surgery. 2006 Volume 3 Number 1. Abstract Animal bites resulting in significant
Symptoms of cellulitis (n=396) %
 %") Cellulitis and lymphoedema Vaughan Keeley May 2012 What is cellulitis? - also called erysipelas, acute inflammatory episodes etc. - bacterial infection of skin + subcutaneous tissues - more common in people
Cellulitis and lymphoedema Vaughan Keeley May 2012 What is cellulitis? - also called erysipelas, acute inflammatory episodes etc. - bacterial infection of skin + subcutaneous tissues - more common in people
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Excerpts Bare Minimum Microbiology Review. Staph aureus
 Excerpts Bare Minimum Microbiology Review Staph aureus 9. Northwestern Medical Review, Bare Minimum Microbiology, 2012 Staphylococcus aureus Gram-positive cocci, grape-like clusters, facultative anaerobic,
Excerpts Bare Minimum Microbiology Review Staph aureus 9. Northwestern Medical Review, Bare Minimum Microbiology, 2012 Staphylococcus aureus Gram-positive cocci, grape-like clusters, facultative anaerobic,
ASSIST. PROF. Dr. Abdulameer Abdullah University of Basra, College of Nursing
 ASSIST. PROF. Dr. Abdulameer Abdullah University of Basra, College of Nursing 2017-2108 Gram Positive Cocci Pyogenic Opportunists (normal flora) Staphylococcus, Streptococcus, Enterococcus Contagious Pathogens
ASSIST. PROF. Dr. Abdulameer Abdullah University of Basra, College of Nursing 2017-2108 Gram Positive Cocci Pyogenic Opportunists (normal flora) Staphylococcus, Streptococcus, Enterococcus Contagious Pathogens
Impact of a Standardized Protocol to Address Outbreak of Methicillin-resistant
 Impact of a Standardized Protocol to Address Outbreak of Methicillin-resistant Staphylococcus Aureus Skin Infections at a large, urban County Jail System Earl J. Goldstein, MD* Gladys Hradecky, RN* Gary
Impact of a Standardized Protocol to Address Outbreak of Methicillin-resistant Staphylococcus Aureus Skin Infections at a large, urban County Jail System Earl J. Goldstein, MD* Gladys Hradecky, RN* Gary
Antibiotic guidelines for SKIN AND SOFT TISSUE INFECTIONS
 CLINICAL USEFUL INFORMATION RECOMMENDATIONS ALTERNATIVE Impetigo erythematous papules vesicles and pustules honey-colored crusts on an erythematous base Gram stain and culture of the pus or exudates from
CLINICAL USEFUL INFORMATION RECOMMENDATIONS ALTERNATIVE Impetigo erythematous papules vesicles and pustules honey-colored crusts on an erythematous base Gram stain and culture of the pus or exudates from
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
5/26/10. Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis Animal bites Unusual skin and soft tissue infections
 Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis
Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis
Infectious Disease Update 2017
 Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
"What's new in Infectious skin diseases"
 "What's new in Infectious skin diseases" Prof. Dr. med. Kathrin Mühlemann Dep. of Infectious Diseases, Inselspital Institute for Infectious Diseases, University of Bern Disclosure Educational Grant with
"What's new in Infectious skin diseases" Prof. Dr. med. Kathrin Mühlemann Dep. of Infectious Diseases, Inselspital Institute for Infectious Diseases, University of Bern Disclosure Educational Grant with
Cellulitis and Abscess: ED Phase v 1.1
 Cellulitis and Abscess: ED Phase v 1.1 Executive Summary Test Your Knowledge PHASE I (E.D.) Explanation of Evidence Ratings Summary of Version Changes! Labs if systemic illness or necrotizing fasciitis
Cellulitis and Abscess: ED Phase v 1.1 Executive Summary Test Your Knowledge PHASE I (E.D.) Explanation of Evidence Ratings Summary of Version Changes! Labs if systemic illness or necrotizing fasciitis
Wound Infections Lecture 20 - Dr. Gary Mumaugh
 Wound Infections Lecture 20 - Dr. Gary Mumaugh Wound Infections Disease production in infected wounds depends on o How virulent infecting organisms are o How many organisms infect the wound o Is the host
Wound Infections Lecture 20 - Dr. Gary Mumaugh Wound Infections Disease production in infected wounds depends on o How virulent infecting organisms are o How many organisms infect the wound o Is the host
CA-MRSA: How Should We Respond to Outbreaks?
 CA-MRSA: How Should We Respond to Outbreaks? Robert B. Stroube, MD, MPH Medscape Infectious Diseases. 2008; 2008 Medscape Posted 11/05/2008 Introduction to MRSA Methicillin-resistant Staphylococcus aureus
CA-MRSA: How Should We Respond to Outbreaks? Robert B. Stroube, MD, MPH Medscape Infectious Diseases. 2008; 2008 Medscape Posted 11/05/2008 Introduction to MRSA Methicillin-resistant Staphylococcus aureus
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles
 Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
A. Incision and drainage alone B. Incision and drainage plus oral anti-mrsa antimicrobial agent C. Oral anti-mrsa antimicrobial agent
 Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Necrotizing fasciitis Animal bites Other skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor
Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Necrotizing fasciitis Animal bites Other skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor
COMMUNITY ASSOCIATED METHICILLIN-RESISTANT STAPHLOCOCCUS AUREUS A PRACTICAL GUIDE FOR PRIMARY CARE PRACTITIONERS
 COMMUNITY ASSOCIATED METHICILLIN-RESISTANT STAPHLOCOCCUS AUREUS A PRACTICAL GUIDE FOR PRIMARY CARE PRACTITIONERS December 21, 2010 Background Since it was first described in 1961 methicillin resistant
COMMUNITY ASSOCIATED METHICILLIN-RESISTANT STAPHLOCOCCUS AUREUS A PRACTICAL GUIDE FOR PRIMARY CARE PRACTITIONERS December 21, 2010 Background Since it was first described in 1961 methicillin resistant
Responders as percent of overall members in each category: Practice: Adult 490 (49% of 1009 members) 57 (54% of 106 members)
 57 (54% of 106 members)") Infectious Diseases Society of America Emerging Infections Network 6/2/10 Report for Query: Perioperative Staphylococcus aureus Screening and Decolonization Overall response rate: 674/1339 (50.3%) physicians
Infectious Diseases Society of America Emerging Infections Network 6/2/10 Report for Query: Perioperative Staphylococcus aureus Screening and Decolonization Overall response rate: 674/1339 (50.3%) physicians
Surgical Site Infections (SSIs)
") Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa.
 Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
Scottish Medicines Consortium
 Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Prophylactic antibiotic timing and dosage. Dr. Sanjeev Singh AIMS, Kochi
 Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Objectives. Impetigo 8/6/2013
 Bacterial Infections E.J. Mayeaux, Jr., M.D. Professor of Family Medicine Professor of Obstetrics & Gynecology Louisiana State University Health Sciences Center Shreveport, LA No disclosures to report.
Bacterial Infections E.J. Mayeaux, Jr., M.D. Professor of Family Medicine Professor of Obstetrics & Gynecology Louisiana State University Health Sciences Center Shreveport, LA No disclosures to report.