Getting Smart about Skin Infections and MRSA
|
|
|
- Lauren Dalton
- 6 years ago
- Views:
Transcription
1 Getting Smart about Skin Infections and MRSA Loren G. Miller, M.D., M.P.H. Associate Professor of Medicine David Geffen School of Medicine at UCLA Division of Infectious Diseases Director, Infection Control Program Harbor-UCLA Medical Center
2 Topics Clinical infections Epidemiology Treatment Prevention
3 Disclosures Pfizer: consultant, grant recipient Cubist Pharmaceuticals: grant recipient GSK: grant recipient NIH, CDC, AHRQ: grant recipient
4 Skin & Soft Tissue Infections associated with S. aureus Impetigo Folliculitis Cellulitis Erysipelas Furuncles (boils) Staphylococcal Scalded Skin Syndrome Toxic Shock Syndrome Swartz MN. In Mandell GL et al. Principals and Practice of Infect. Dis. 2000;
5 Other Syndromes associated with S. aureus Bacteremia and sepsis Arthritis, osteomyelitis, endocarditis, meningitis, lung abscess, empyema, pyomyositis, etc. Surgical site infections Pneumonia Nosocomial Community-acquired Catheter-associated infections Infections of prosthetic devices Food poisoning Waldvogel FA. In Mandell GL et al. Principals and Practice of Infect. Dis. 2000;
6 Methicillin-resistant S. aureus First described in 1961 Infections in hospitalized patients Strains typically R to commonly used antibiotics except vancomycin (& gentamicin, rifampin) Community infections first in IDU in Detroit, Australia, New Zealand in early 1990 s Community MRSA that was not MDR JH Jorgenson. Centers for Disease Control and Prevention




7 CA-MRSA Outbreaks

8 CA-MRSA Outbreaks Charlebois ED et al. Clin Infect Dis 2002; 34: Okuma K et al. J Clin Microbiol 2002;40: Salmenlinna S et al. Emerg Infect Dis 2002;8:602-7 Miller LG & Diep BA. Clin Infect Dis 2008;

9 Endemic CA-MRSA Moran GJ et al. New Engl J Med 2006;355:666-74
10 CA-MRSA Transmission The 5 C s of CA-MRSA Contact Crowding Contaminated items and environmental surfaces Compromised skin integrity Cleanliness J Hageman. Centers for Disease Control and Prevention
11 CA-MRSA Transmission The 5 C s of CA-MRSA Contact Crowding Contaminated items and environmental surfaces Compromised skin integrity Cleanliness J Hageman. Centers for Disease Control and Prevention

12 Kazakova SV et al. N Engl J Med 2005; 352:468-75
13 CA-MRSA Transmission The 5 C s of CA-MRSA Contact Crowding Contaminated items and environmental surfaces Compromised skin integrity Cleanliness J Hageman. Centers for Disease Control and Prevention

14
15 CA-MRSA Transmission The 5 C s of CA-MRSA Contact Crowding Contaminated items and environmental surfaces Compromised skin integrity Cleanliness J Hageman. Centers for Disease Control and Prevention

16
17 CA-MRSA Transmission The 5 C s of CA-MRSA Contact Crowding Contaminated items and environmental surfaces Compromised skin integrity Cleanliness J Hageman. Centers for Disease Control and Prevention

18 Kazakova SV et al. N Engl J Med 2005; 352:468-75
19 CA-MRSA Transmission The 5 C s of CA-MRSA Contact Crowding Contaminated items and environmental surfaces Compromised skin integrity Cleanliness J Hageman. Centers for Disease Control and Prevention

20

21
22 Risk Factors for CA-MRSA Among Persons w/ CA-S. aureus Infections MRSA MSSA OR P value (n=120) (N=82) [95% CI] PPV NPV Age (mean, in years) Charlson Co- Morbidity (mean) (per year) < Snorted/ 28% 12% 2.9 smoked drugs [ ] % 45% Jailed in past 12 mo Recent close contact w/ person w/ skin infection 20% 8% 2.8 [ ] 16% 7% 2.5 [ ] % 43% % 44% Miller LG et al. Clin Infect Dis. 2007; 44:471 82

23 MRSA Skin Infection

24 Spider bites and MRSA Vetter RJ. West J Med 2000;173:
25 Differences between HA- and CA-MRSA HA-MRSA Multi-drug R (clinda, gent, FQ) Contain SCCmec I, II, III Usually PVL- CA-MRSA Usu only R to eryth, + FQs Contain SCCmec IV Usually PVL + Appears: highly virulent (esp skin) highly transmissible to recur commonly Modified from JH Jorgenson. Centers for Disease Control and Prevention
26 SCCMec types in MRSA Type I Type IVa Type IVb Type II Type III Ma XX et al. Antimicrob Agents Chemother 2002;46:



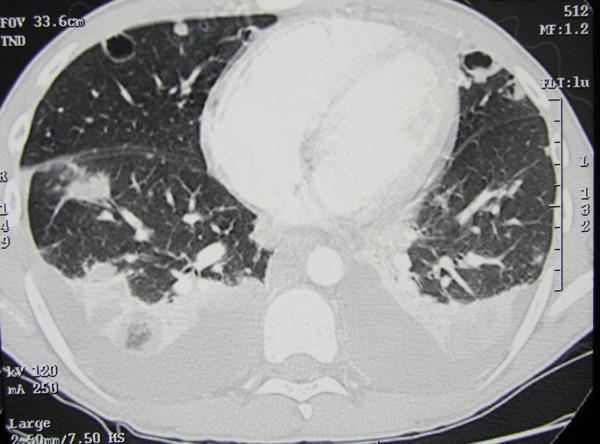
27 Severe CA-MRSA Syndromes Necrotizing fasciitis Necrotizing pneumonia Purpura fulminans Miller LG et al. N Eng J Med 2005; 352: Kravitz GR. Clinical Infect Dis 2005; 40:941 7 Francis JS et al. Clin Infect Dis 2005; 40:100 7

28 Severe CA-MRSA Sepsis in Adolescents 93% had bone/joint infections 57% had pyomyositis in neighboring muscles Gonzalez BE et al. Pediatrics 2005;115: Figure courtesy of Sheldon Kaplan MD
29
30 S. aureus treatment β-lactams oxacillin, nafcillin, dicloxacillin cephalexin, cefazolin ceftaroline Vancomycin Telavancin Erythromycin Clindamycin Tetracyclines (including doxy, mino) Tigecycline Trimethoprim-sulfamethoxazole Fluoroquinolones ciprofloxacin, levofloxacin, moxifloxacin Quinupristin/dalfopristin Linezolid Daptomycin
31
32 CA-MRSA & CA-MSSA susceptibility at Harbor-UCLA MRSA (n=120) MSSA (n=82) P value Pen G 0% 13% <0.001 Amp/Sul 0% 100% <0.001 Cefazolin/oxacillin 0% 100% <0.001 Erythromycin 7% 84% <0.001 Ciprofloxacin 15% 88% <0.001 Levofloxacin 88% 100% 0.01 Tetracycline 81% 94% 0.01 Clindamycin 95% 100% 0.11 TMP-SMX 100% 99% 0.94 Vancomycin 100% 100% 0.99 (Linezolid & daptomcyin) 100% 100% 0.99 Miller LG et al. Clin Infect Dis. 2007; 44:471 82
33
34
35 IDSA MRSA Guidelines Skin infections Recurrent MRSA skin infections Bloodstream infection Bacteremia and Endocarditis Pneumonia Bone and Joint Infections CNS infections Adjunctive Therapy Vancomycin dosing Persistent MRSA Bacteremia Vancomycin susceptibility testing Neonates Liu C et al. Clin Infect Dis 2011;52:
36 Treatment of Skin Infections
37 IDSA MRSA Guidelines: Skin Abscesses For cutaneous abscess, incision and drainage (I&D) is the primary treatment (A-II) For simple abscesses or boils, I&D alone is likely adequate additional data needed to further define role of antibiotics, if any Liu C et al. Clin Infect Dis 2011;52:
38 IDSA MRSA Guidelines: Skin Abscesses For abscesses or boils, Abx rec d for: (A-III) severe, extensive, rapidly progressive signs & sx s of systemic illness co-morbidities or immunosuppression extremes of age abscess in an area difficult to drain e.g., face, hand, and genitalia septic phlebitis lack of response to I&D alone Liu C et al. Clin Infect Dis 2011;52:

39 Treatment of Skin Infections
40 Purulent Cellulitis For outpatients w/ purulent cellulitis, empiric Rx for CA-MRSA rec d pending Cx results Empirical therapy for β-hemolytic streptococci likely unnecessary (A-II) Rx for 5-10 days of therapy Liu C et al. Clin Infect Dis 2011;52:
41 Outpatient Skin Infection Treatment Outpatient MRSA Outpatient betahemolytic Strep Clindamycin A II A II TMP-SMX Tetracycline A II A II Not rec d Must add B-lactam Not rec d Must add B-lactam Comments Perform D-test for severe cases Includes doxy, mino Linezolid A II A II Expensive Liu C et al. Clin Infect Dis 2011;52:

42 Treatment of Skin Infections
43 Non-Purulent Cellulitis Empirical therapy for infection due to β- hemolytic streptococci rec d (A-II) Role of CA-MRSA is unknown Empirical coverage for CA-MRSA rec d for patients who don t respond to β-lactam Rx Considered MRSA Rx if systemic toxicity Rx 5-10 days Liu C et al. Clin Infect Dis 2011;52:
44 Hospitalized Patients with Skin Infection Surgical debridement, if needed Vancomycin Linezolid (po or IV) Daptomycin 4 mg/kg/day Telavancin 10 mg/kg/day Clindamycin 600 mg po or IV (AI) (AI) (AI) (AI) (AIII) Liu C et al. Clin Infect Dis 2011;52:

45 The D-test Tests for inducible clinda resistance D test +: Clinda may not be useful D test -: Clinda prob. useful Siberry GK et al. Clin Infect Dis 2003; 37:
46 Hospitalized Patients with Skin Infection β-lactam antibiotic (e.g., cefazolin) (A-II) may be considered in patients w/ non-purulent cellulitis Use MRSA-active Rx if no clinical response Rx 7-14 days Liu C et al. Clin Infect Dis 2011;52:
47
48 Vancomycin Traditional Rx of choice for MRSA Bacteriocidal Inferior to β-lactams in difficult to treat infections Endocarditis Bacteremia Osteomyelitis Deresinski S. Clin Infect Dis 2005; 40: Tice AD et al. J Antimicrob Chemother 2003; 51,
49 Treatment Failure, % Vancomycin MIC & Treatment Failures in MRSA Infections MIC (ug/ml) Moise-Broder PA et al. Clin Infect Dis 2004;38:
50 MRSA Bacteremia Uncomplicated: exclusion of endocarditis no implanted prostheses follow-up blood Cx s 2 4 days after initial set negative for MRSA defervescence w/in 72 h of initiating effective Rx no evidence of metastatic sites of infection Otherwise complicated Liu C et al. Clin Infect Dis 2011;52:
51 MRSA Bacteremia Uncomplicated Bacteremia: Vancomycin (A-II) Daptomycin 6 mg/kg/day (AI) At least 2 weeks Complicated Bacteremia At least 4-6 weeks Consider daptomycin 8-10 mg/kg/day (BIII) Liu C et al. Clin Infect Dis 2011;52:
52
53 Linezolid for MRSA Pneumonia Secondary analysis of ventilator-assd MRSA pneumonia, linezolid superior to vancomycin in terms of: Clinical cure (59% vs. 26%, OR 3.3 [ ], p=0.01) Survival (80% vs. 64%, OR 2.2 [ ], p=0.05) Wunderink RG et al. Chest 2003; 124: Bauer TT. Chest 2003; 124: Kollef MF. Intensive Care Med 2004; 30:
54 MRSA Pneumonia Vancomycin (A-II) Linezolid po/iv 600 mg bid (A-II) or Clindamycin 600 mg PO/IV 3x day (B-III), if MRSA susceptible Liu C et al. Clin Infect Dis 2011;52:

55
56 Vancomycin Dosing mg/kg/dose (actual body weight) q8 12 h for pt s w/ normal renal function not to exceed 2 g per dose In seriously ill patients with suspected MRSA infection, consider mg/kg loading dose Liu C et al. Clin Infect Dis 2011;52:
57 Vancomycin Monitoring Monitor troughs only in: Severe infections Morbid obesity Renal dysfunction Fluctuating volumes of distribution Liu C et al. Clin Infect Dis 2011;52:
58 Vancomycin Monitoring Aim for trough of μg/ml for severe MRSA infections: bacteremia endocarditis osteomyelitis meningitis pneumonia severe SSTI (e.g., necrotizing fasciitis) Liu C et al. Clin Infect Dis 2011;52:
59 Vancomycin Guidelines Weight based dosing (AII) Consider loading dose mg/kg (BIII) Trough concentrations should be >10 mg/l (BIII) mg/l for complicated infections (BIII) E.g., bacteremia, endocarditis, osteomyelitis, pneumonia MIC > 2 mg/l with normal renal function Target AUC/MIC of >400 not achievable Rybak MJ et al. Clin Infect Dis 2009; 49: 325-7
60 S. aureus Treatment New Drugs/Pipeline Glycopeptides Telavancin (qd) Oritavancin (qd) Dalbavancin (q week) Ceftaroline, ceftobiprole, Cephalosporins with anti-mrsa activity Iclaprim selective dihydrofolate inhibitor Lopez S et al. J Antimicrob Chemother 2005, Suppl. S2, ii21 ii24 Raad I et al. Clin Infect Dis 2005; 40: Stryjewski ME et al. Clin Infect Dis 2005; 40: Ward KE et al. Expert Opin Investig Drugs 2006;15: Bogdanovich T. Antimicrob Agents Chemothe 2005;49: Talbot GF et al. Antimicrob Agents Chemothe 2007;51: Schneider P et al. Bioorganic & Medicinal Chemistry Letters 2003: 13:
61 Glygopeptide Telavancin Same class as vancomycin Approved for SSSI Non-inferior to vancomycin for VAP Dosing data poorly understood in peds None in CF patients Avoid treatment in pregnancy Rubenstein E et al. Clin Infect Dis 2011; 52:41-50 Stryjewski ME et al. Clin Infect Dis 2005; 40:1601 7
62 Ceftaroline β-lactam antibiotic with activity vs. MRSA 1,3-thiazole ring attached via a sulfur linker on the cephem ring high affinity for PBP2a on MRSA Active vs. gram negative pathogens Not Pseudomonas or ESBL+ GNB Safety profile similar to other cephalosporins Lim L et al. Am J Health Syst Pharm 2011; 68:491-8 Talbot GF et al. Antimicrob Agents Chemother 2007;51:
63 Tigecycline A glycecycline IV only minocycline derivative Broad spectrum, including S. aureus, MRSA Approved for Rx of SSSI Adverse effects: Gastrointestinal (N/V) Tooth discoloration Other Most MRSA appear S to tigecycline Livermore DM. J Antimicrobial Chemotherapy 2005; 56:
64 Rifampin Potent activity vs. S. aureus When used alone, R almost invariably develops Limitations: Drug interactions Hepatoxocity Colors tears, urine, sweat No compelling data synergistic Rx except where bioflim present (devices, ostemyelitis) Data for treatment in pneumonia, decolonization suggestive of benefit Lowy FD. New Engl J Med 1998; 3339: Perlroth JP et al. Arch Intern Med 2008; 168: Jung YJ et al. Crit Care Med 2010; 38: Falagas MF et al. Am J Infect Control 2007;35:106-14
65 Potential Mechanisms to Control CA-MRSA Search and Destroy Topical nasal antibiotics mupirocin others Body decolonization chlorhexidine hexachloraphene dilute bleach others Systemic antibiotics rifampin clindamycin others Environmental decolonization sprayable ethyl alcohol bleach solutions others
66 MRSA summary MRSA infections common community healthcare settings Skin infections typically MRSA Many older abx appropriate for MRSA Rx IDSA MRSA Guidelines can provide guidance Abx may not be needed after I&D for skin infxn
67
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Best Antimicrobials for Staphylococcus aureus Bacteremia
 Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Appropriate Antimicrobial Therapy for Treatment of
 Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections. Skin & Soft Tissue Infections (SSTI)
 Skin & Soft Tissue Infections. Skin & Soft Tissue Infections (SSTI)") Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections 2007 Abscess Cellulitis Bradley W Frazee, MD, FACEP Dept of Emergency Medicine Alameda County Medical Center - Highland Hospital Associate
Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections 2007 Abscess Cellulitis Bradley W Frazee, MD, FACEP Dept of Emergency Medicine Alameda County Medical Center - Highland Hospital Associate
Skin and Soft Tissue Infections Emerging Therapies and 5 things to know
 2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
Staph Cases. Case #1
 Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
IDSA GUIDELINES EXECUTIVE SUMMARY
 IDSA GUIDELINES Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin- Resistant Staphylococcus aureus Infections in Adults and Children Catherine
IDSA GUIDELINES Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin- Resistant Staphylococcus aureus Infections in Adults and Children Catherine
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust
 PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
STAPHYLOCOCCI: KEY AST CHALLENGES
 Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
S aureus infections: outpatient treatment. Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium
 S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
Ca-MRSA Update- Hand Infections. Washington Hand Society September 19, 2007
 Ca-MRSA Update- Hand Infections Washington Hand Society September 19, 2007 Resistant Staph. Aureus Late 1940 s -50% S.Aureus resistant to PCN 1957-80/81 strain- of S.A. highly virulent and easily transmissible
Ca-MRSA Update- Hand Infections Washington Hand Society September 19, 2007 Resistant Staph. Aureus Late 1940 s -50% S.Aureus resistant to PCN 1957-80/81 strain- of S.A. highly virulent and easily transmissible
Overview Management of Skin and Soft Tissue Infections in the MRSA Era
 Overview Management of Skin and Soft Tissue Infections in the MRSA Era April 2011 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Management of Recurrent SSTIs Necrotizing soft
Overview Management of Skin and Soft Tissue Infections in the MRSA Era April 2011 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Management of Recurrent SSTIs Necrotizing soft
MRSA Background. New Challenges From an Old Foe. MRSA Demographics. Comparison of Types of MRSA CA-MRSA HA-MRSA
 Winter Clinical 2017 : MRSA Update Whitney A. High, MD, JD, Meng whitney.high@ucdenver.edu Associate Professor, Dermatology & Pathology Director of Dermatopathology University of Colorado School of Medicine
Winter Clinical 2017 : MRSA Update Whitney A. High, MD, JD, Meng whitney.high@ucdenver.edu Associate Professor, Dermatology & Pathology Director of Dermatopathology University of Colorado School of Medicine
New Antibiotics & New Insights into Old Antibiotics
 New Antibiotics & New Insights into Old Antibiotics Louisiana Chapter of the American Academy of Pediatrics August 18, 2018 Baton Rouge, Louisiana John Bradley MD Rady Children s Hospital San Diego University
New Antibiotics & New Insights into Old Antibiotics Louisiana Chapter of the American Academy of Pediatrics August 18, 2018 Baton Rouge, Louisiana John Bradley MD Rady Children s Hospital San Diego University
5/17/2012 DISCLOSURES OBJECTIVES CONTEMPORARY PEDIATRICS
 CONTEMPORARY PEDIATRICS Surgical Management of MRSA Soft Tissue Infections John M. Draus, Jr., M.D. Assistant Professor of Surgery and Pediatrics Kentucky Children s Hospital University of Kentucky DISCLOSURES
CONTEMPORARY PEDIATRICS Surgical Management of MRSA Soft Tissue Infections John M. Draus, Jr., M.D. Assistant Professor of Surgery and Pediatrics Kentucky Children s Hospital University of Kentucky DISCLOSURES
New Antibiotics for MRSA
 New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Empiric therapy for severe suspected Staphylococcus aureus infection
 Empiric therapy for severe suspected Staphylococcus aureus infection Salman Qureshi, MD McGill University Faculty of Medicine Department of Critical Care Medicine McGill University Health Centre Relevant
Empiric therapy for severe suspected Staphylococcus aureus infection Salman Qureshi, MD McGill University Faculty of Medicine Department of Critical Care Medicine McGill University Health Centre Relevant
Infectious Disease Issues in the Intensive Care Unit
 Infectious Disease Issues in the Intensive Care Unit Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Overview Emerging antibiotic
Infectious Disease Issues in the Intensive Care Unit Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Overview Emerging antibiotic
IDSA GUIDELINES EXECUTIVE SUMMARY
 IDSA GUIDELINES Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus aureus Infections in Adults and Children: Executive
IDSA GUIDELINES Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus aureus Infections in Adults and Children: Executive
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Methicillin Resistant Staphylococcus Aureus (MRSA) The drug resistant `Superbug that won t die
 The drug resistant `Superbug that won t die") Methicillin Resistant Staphylococcus Aureus (MRSA) The drug resistant `Superbug that won t die Michael A. Miller, MD Assistant Professor of Pediatrics -Jacksonville OBJECTIVES 1. Understand the basic microbiology
Methicillin Resistant Staphylococcus Aureus (MRSA) The drug resistant `Superbug that won t die Michael A. Miller, MD Assistant Professor of Pediatrics -Jacksonville OBJECTIVES 1. Understand the basic microbiology
Discussion Points. Decisions in Selecting Antibiotics
 Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Sixth Plague of Egypt. Community MRSA. Epidemiology. Basic Features of Community MRSA. Populations with CA-MRSA
 Community MRSA Henry F. Chambers, M.D. University of California San Francisco San Francisco General Hospital Sixth Plague of Egypt (~ 1200 BCE) So they took soot from a kiln, and stood before Pharaoh;
Community MRSA Henry F. Chambers, M.D. University of California San Francisco San Francisco General Hospital Sixth Plague of Egypt (~ 1200 BCE) So they took soot from a kiln, and stood before Pharaoh;
MRSA What Are Our Treatment Options and How Do We Choose the Right One?
 MRSA What Are Our Treatment Options and How Do We Choose the Right One? Kristi Traugott, PharmD, BCPS Clinical Pharmacy Specialist Infectious Diseases University Health System San Antonio, TX October 25,
MRSA What Are Our Treatment Options and How Do We Choose the Right One? Kristi Traugott, PharmD, BCPS Clinical Pharmacy Specialist Infectious Diseases University Health System San Antonio, TX October 25,
Le infezioni di cute e tessuti molli
 Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Infections caused by Methicillin-Resistant Staphylococcus
 MRSA infections are no longer limited to hospitals. An infectious disease specialist offers insight on what this means for dermatologists. By Robert S. Jones, DO, Reading, PA Infections caused by Methicillin-Resistant
MRSA infections are no longer limited to hospitals. An infectious disease specialist offers insight on what this means for dermatologists. By Robert S. Jones, DO, Reading, PA Infections caused by Methicillin-Resistant
Antimicrobial Therapy
 Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Disclosure: Dr. Spach has no significant financial interest in any of the
Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Disclosure: Dr. Spach has no significant financial interest in any of the
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
GUIDE TO INFECTION CONTROL IN THE HOSPITAL
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key
SKIN AND SOFT TISSUE INFECTIONS OCTOBER 3-4, 2015
 SKIN AND SOFT TISSUE INFECTIONS OCTOBER 3-4, 2015 Disclosures I have no financial conflicts of interest to disclose or report. Steven Tran, PharmD NEFSHP Fall Meeting 2015 Objectives for Pharmacists Review
SKIN AND SOFT TISSUE INFECTIONS OCTOBER 3-4, 2015 Disclosures I have no financial conflicts of interest to disclose or report. Steven Tran, PharmD NEFSHP Fall Meeting 2015 Objectives for Pharmacists Review
LINEE GUIDA: VALORI E LIMITI
 Ferrara 28 novembre 2014 LINEE GUIDA: VALORI E LIMITI Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi EVIDENCE BIASED GERIATRIC MEDICINE Older patients with comorbid conditions
Ferrara 28 novembre 2014 LINEE GUIDA: VALORI E LIMITI Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi EVIDENCE BIASED GERIATRIC MEDICINE Older patients with comorbid conditions
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
A. Incision and drainage alone B. Incision and drainage plus oral anti-mrsa antimicrobial agent C. Oral anti-mrsa antimicrobial agent
 Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Necrotizing fasciitis Animal bites Other skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor
Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Necrotizing fasciitis Animal bites Other skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Staphylococcus Aureus
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
1/7/2012. Objectives. New Treatment Guidelines for Methicillin-Resistant Staphylococcus Aureus (MRSA) Classification. Definition
 Classification. Definition") New Treatment Guidelines for Methicillin-Resistant Staphylococcus Aureus (MRSA) Objectives Review the management of clinical syndromes associated with MRSA disease, including skin and soft tissue infections,
New Treatment Guidelines for Methicillin-Resistant Staphylococcus Aureus (MRSA) Objectives Review the management of clinical syndromes associated with MRSA disease, including skin and soft tissue infections,
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Infectious Disease Update 2017
 Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
TACKLING THE MRSA EPIDEMIC
 TACKLING THE MRSA EPIDEMIC Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine MRSA Trend (HA + CA) in US TSN Database USA (1993-2003) % of MRSA among S. aureus
TACKLING THE MRSA EPIDEMIC Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine MRSA Trend (HA + CA) in US TSN Database USA (1993-2003) % of MRSA among S. aureus
Source: Portland State University Population Research Center (
 Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Replaces:04/14/16. Formulated: 1997 SKIN AND SOFT TISSUE INFECTION
 Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
4/28/11. Update: 2011 IDSA MRSA Treatment Guidelines. Necrotizing fasciitis Animal bites Other skin and soft tissue infections
 Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs)
Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs)
Community Methicillin- Resistant Staphylococcus aureus. Sixth Plague of Egypt. Epidemiology
 Community Methicillin- Resistant Staphylococcus aureus Henry F. Chambers, M.D. University of California San Francisco San Francisco General Hospital Sixth Plague of Egypt (~ 1200 BCE) So they took soot
Community Methicillin- Resistant Staphylococcus aureus Henry F. Chambers, M.D. University of California San Francisco San Francisco General Hospital Sixth Plague of Egypt (~ 1200 BCE) So they took soot
STAPHYLOCOCCI: KEY AST CHALLENGES
 Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
* gender factor (male=1, female=0.85)
") Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
MRSA. ( Staphylococcus aureus; S. aureus ) ( community-associated )
 ( community-associated )") 005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
MRSA ventilatorassociated
 MRSA ventilatorassociated pneumonia Jean Chastre, M.D. www.reamedpitie.com Conflicts of interest Consulting or lecture fees: Medimmune/Astrazeneca, Bayer, Pfizer, Arsanis, Cubist/Merck, Basilea, Aridis,
MRSA ventilatorassociated pneumonia Jean Chastre, M.D. www.reamedpitie.com Conflicts of interest Consulting or lecture fees: Medimmune/Astrazeneca, Bayer, Pfizer, Arsanis, Cubist/Merck, Basilea, Aridis,
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections
 Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Annual U.S. ED Visits for Skin and Soft Tissue Infections,
 Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis Animal bites Unusual skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious
Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis Animal bites Unusual skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious
21 st Expert Committee on Selection and Use of Essential Medicines Peer Review Report Antibiotics Review
 (1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
(1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
Antibiotic Use in the Emergency Department
 Antibiotic Use in the Emergency Department Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
Antibiotic Use in the Emergency Department Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
In This Issue: Community-Associated MRSA Infection Surveillance in Washoe County Final Report For Health Care Providers
 EPI - NEWS Page 1 of 6 In This Issue: Community-Associated MRSA Infection Surveillance in Washoe County Final Report For Health Care Providers Please share this document with all physicians & staff in
EPI - NEWS Page 1 of 6 In This Issue: Community-Associated MRSA Infection Surveillance in Washoe County Final Report For Health Care Providers Please share this document with all physicians & staff in
Tropical infections caused by Staphylococcus aureus
 Tropical infections caused by Staphylococcus aureus Michael Ellis, MD Infectious Diseases Division Uniformed Services University of the Health Sciences February 2015 Introduction Tropical Pyomyositis Cutaneous
Tropical infections caused by Staphylococcus aureus Michael Ellis, MD Infectious Diseases Division Uniformed Services University of the Health Sciences February 2015 Introduction Tropical Pyomyositis Cutaneous
RESISTANT PATHOGENS. John E. Mazuski, MD, PhD Professor of Surgery
 RESISTANT PATHOGENS John E. Mazuski, MD, PhD Professor of Surgery Disclosures Contracted Research: AstraZeneca, Bayer, Merck. Advisory Boards/Consultant: Allergan (Actavis, Forest Laboratories), AstraZeneca,
RESISTANT PATHOGENS John E. Mazuski, MD, PhD Professor of Surgery Disclosures Contracted Research: AstraZeneca, Bayer, Merck. Advisory Boards/Consultant: Allergan (Actavis, Forest Laboratories), AstraZeneca,
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Oxazolidinone Antibiotics Table of Contents Coverage Policy... 1 General Background... 3 Coding/Billing Information... 5 References... 5 Effective Date...
Cigna Drug and Biologic Coverage Policy Subject Oxazolidinone Antibiotics Table of Contents Coverage Policy... 1 General Background... 3 Coding/Billing Information... 5 References... 5 Effective Date...
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
STAPHYLOCOCCI: KEY AST CHALLENGES
 Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate
 Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Doxycycline staph aureus
 Search Search Doxycycline staph aureus Mercer infection is the one of the colloquial terms given for MRSA (Methicillin-Resistant Staphylococcus Aureus ) infection. Initially, Staphylococcal resistance
Search Search Doxycycline staph aureus Mercer infection is the one of the colloquial terms given for MRSA (Methicillin-Resistant Staphylococcus Aureus ) infection. Initially, Staphylococcal resistance
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Methicillin Resistant Staphylococcus aureus:
 Methicillin Resistant Staphylococcus aureus: Action-Oriented Guidance for Community-Based Prevention Jackie Dawson, PhD Public Health Epidemiologist Chelan, Douglas, Grant, Kittitas, & Okanogan Counties
Methicillin Resistant Staphylococcus aureus: Action-Oriented Guidance for Community-Based Prevention Jackie Dawson, PhD Public Health Epidemiologist Chelan, Douglas, Grant, Kittitas, & Okanogan Counties
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Prevalence & Risk Factors For MRSA. For Vets
 For Vets General Information Staphylococcus aureus is a Gram-positive, aerobic commensal bacterium of humans that is carried in the anterior nares of approximately 30% of the general population. It is
For Vets General Information Staphylococcus aureus is a Gram-positive, aerobic commensal bacterium of humans that is carried in the anterior nares of approximately 30% of the general population. It is
New Antibiotics & New Insights into Old Antibiotics
 New Antibiotics & New Insights into Old Antibiotics Louisiana Chapter of the American Academy of Pediatrics August 18, 2018 Baton Rouge, Louisiana John Bradley MD Rady Children s Hospital San Diego University
New Antibiotics & New Insights into Old Antibiotics Louisiana Chapter of the American Academy of Pediatrics August 18, 2018 Baton Rouge, Louisiana John Bradley MD Rady Children s Hospital San Diego University
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process High Priority
 MEASURE TYPE: Process High Priority") Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Healthcare Associated
Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Healthcare Associated
What s New in MRSA? An Update on Legislative Mandates and MRSA in the Obstetrics/ Gynecology Patient
 What s New in MRSA? An Update on Legislative Mandates and MRSA in the Obstetrics/ Gynecology Patient Catherine Liu, M.D. Assistant Clinical Professor University of California, San Francisco Overview New
What s New in MRSA? An Update on Legislative Mandates and MRSA in the Obstetrics/ Gynecology Patient Catherine Liu, M.D. Assistant Clinical Professor University of California, San Francisco Overview New
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles
 Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
ANTIMICROBIAL SUSCEPTIBILITY DETECTION OF ELEVATED MICs TO PENICILLINS IN β- HAEMOLYTIC STREPTOCOCCI
 HAEMOLYTIC STREPTOCOCCI This specimen was designated as a sample from a skin wound that was to be cultured, identified to species level and susceptibility tested [1-3]. The culture contained a Streptococcus
HAEMOLYTIC STREPTOCOCCI This specimen was designated as a sample from a skin wound that was to be cultured, identified to species level and susceptibility tested [1-3]. The culture contained a Streptococcus
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Antimicrobials Update
 Antimicrobials Update Rosie Amini, PharmD. BCPS Antimicrobial Stewardship Program Coordinator Swedish Medical Center Disclosures: Dr. Amini has no significant financial interest in any of the products
Antimicrobials Update Rosie Amini, PharmD. BCPS Antimicrobial Stewardship Program Coordinator Swedish Medical Center Disclosures: Dr. Amini has no significant financial interest in any of the products
5/26/10. Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis Animal bites Unusual skin and soft tissue infections
 Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis
Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis
56 Clinical and Laboratory Standards Institute. All rights reserved.
 Table 2C 56 Clinical and Laboratory Standards Institute. All rights reserved. Table 2C. Zone Diameter and Minimal Inhibitory Concentration Breakpoints for Testing Conditions Medium: Inoculum: diffusion:
Table 2C 56 Clinical and Laboratory Standards Institute. All rights reserved. Table 2C. Zone Diameter and Minimal Inhibitory Concentration Breakpoints for Testing Conditions Medium: Inoculum: diffusion:
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia. Po-Ren Hsueh. National Taiwan University Hospital
 Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Antibacterials. Recent data on linezolid and daptomycin
 Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Mrsa abscess and cellulitis
 Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
Copyright 2012 Diabetes In Control, Inc. For permission to reprint, please contact Heather Moran, Production Editor, at
 Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Should we test Clostridium difficile for antimicrobial resistance? by author
 Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
High Risk Emergency Medicine. Antibiotic Pitfalls
 High Risk Emergency Medicine Antibiotic Pitfalls David, MD MS Assistant Professor Department of Emergency Medicine University of California, San Francisco I. Antibiotic Resistance Development of resistance
High Risk Emergency Medicine Antibiotic Pitfalls David, MD MS Assistant Professor Department of Emergency Medicine University of California, San Francisco I. Antibiotic Resistance Development of resistance
Antibiotic Duration for Common Infections
 Antibiotic Duration for Common Infections Emily Spivak, MD, MHS Division of Infectious Diseases Medical Director, Antimicrobial Stewardship Program University of Utah Hospitals and Clinics Learning Objectives
Antibiotic Duration for Common Infections Emily Spivak, MD, MHS Division of Infectious Diseases Medical Director, Antimicrobial Stewardship Program University of Utah Hospitals and Clinics Learning Objectives
Antibiotic Resistances Profile in Iran, Clinical Implication and Prospect for Antibiotic Stewardship Jafar Soltani
 Antibiotic Resistances Profile in Iran, Clinical Implication and Prospect for Antibiotic Stewardship Jafar Soltani Pediatrics Department, Faculty of Medicine, Kurdistan University of Medical Sciences,
Antibiotic Resistances Profile in Iran, Clinical Implication and Prospect for Antibiotic Stewardship Jafar Soltani Pediatrics Department, Faculty of Medicine, Kurdistan University of Medical Sciences,
CA-MRSA lesions: What works, what doesn t
 For mass reproduction, content licensing and permissions contact Dowden Health Media. FAMILY David McBride, MD University Student Health Services and the Department of Family Medicine, Boston University
For mass reproduction, content licensing and permissions contact Dowden Health Media. FAMILY David McBride, MD University Student Health Services and the Department of Family Medicine, Boston University
Infectious Disease: Drug Resistance Pattern in New Mexico
 Infectious Disease: Drug Resistance Pattern in New Mexico Are these the world's sexiest accents? Obi C. Okoli, MD.,MPH. Clinic for Infectious Diseases Las Cruces, NM. Are these the world's sexiest accents?
Infectious Disease: Drug Resistance Pattern in New Mexico Are these the world's sexiest accents? Obi C. Okoli, MD.,MPH. Clinic for Infectious Diseases Las Cruces, NM. Are these the world's sexiest accents?