CLINICAL DECISION MAKING IN MICROBIAL KERATITIS. Gregory M. Schultz, O.D.,F.A.A.O. Eye Center of Virginia Williamsburg and Gloucester Virginia
|
|
|
- Suzan Johnston
- 5 years ago
- Views:
Transcription

1 CLINICAL DECISION MAKING IN MICROBIAL KERATITIS Gregory M. Schultz, O.D.,F.A.A.O. Eye Center of Virginia Williamsburg and Gloucester Virginia
2 :
3 GOALS OF THIS COURSE: QUESTIONS WE WILL ANSWER Do I have an infectious corneal ulcer? How do I determine if this infiltrate/ulcer is sterile vs. infection? Do I have to culture? How do I maximize my yield if I culture? How aggressive must I be with my treatment? When do I modify my treatment plan?
4 QUESTIONS WE WILL ANSWER: The Standard of Care: What is my liability here? Is a fourth generation Fluoroquinolone enough? What is the recommended dosing regimen? Do I keep my patient up through the night? Should I use drops, ointments or both? When or should I employ a steroid?
5 GOALS OF THIS COURSE When would I use fortified antibiotics? If I treat with commercially available AB, do I use a 2 nd, 3 rd, or a fourth generation fluoroqinolone What about besifloxacin, is it the best? New treatments of bacterial keratitis
6 INFECTIOUS KERATITIS Infectious keratitis is a potentially blinding eye disease 30,000 cases each year Bacterial,fungal, Acanthamoeba (Pepose,JS et al AJO 1992) If Appropriate antimicrobial treatment is delayed only 50% of eyes gain reasonably good visual recovery * AAO Preferred Practice Patterns for bacterial keratitis
7 PREDISPOSING FACTORS: BACTERIAL KERATITIS Contact lens wear/ EW, homemade soln. /use of tap water DW 1 case / 2,500 per year EW 1 case / / year Ocular surface disease ( MGD, DES) Previous HSK Corneal anesthesia Exposure/ lagophthalmus Bullous Keratopathy trauma
8 PREDISPOSING FACTORS: BACTERIAL KERATITIS Immuno-compromised host Debilitating illness ( DM, Cancer/chemo) Recent ocular surgery LASIK / LASEK, PK, PRK Dry eye/ OSID Lid deformities/ trichiasis, entropion/ectropion Chronic use of topical steroids Contact lens wear and or abuse

9 Virtually anything that will put a chink in the armor!
10 HOWEVER THERE ARE A FEW BUGS THAT CAN PENETRATE AN INTACT CORNEAL EPITHELIUM Neisseria species Cornybacterium diphtheriae Haemophilus species, Aegyptius Listeria species
11 SYSTEMIC CONDITIONS THAT PREDISPOSE TO BACTERIAL KERATITIS Diabetes Vitamin A deficiency Collagen vascular diseases Gonococcal infection with conjunctivitis
12 INFECTIOUS KERATITIS The hallmark of Corneal infection is Corneal Leukocytic infiltration!
13 BACTERIAL KERATITIS: SIGNS/ SYMPTOMS Mild to severe ocular pain Photophobia Decreased vision Tearing with discharge Mild to severe conjunctival inflammation Focal white opacity in the stroma (infiltrative lesion) Stromal edema Corneal ectasia Liquifactive necrosis Mild to severe hypopyon, A/C reaction Lid edema


14 PSEUDOMONAS INFECTION
15 DIFFERENTIATING INFECTIOUS FROM STERILE KERATITIS Characteristic Infectious Sterile Pain Significant Little to none Onset Acute onset/ 24 hours or < More indolent course Location Central / para-central Peripheral/mid-periph Injection Significant: grade 3-4+ Trace to 1+ Discharge excessive Minimal to none Visual Acuity Typically reduced Often unaffected A/C reaction 2-4+ trace

16 THE RULE OF 2 A corneal ulcer is less likely to be infectious when: It is < 2 mm in diameter There is < 2+ cells in the anterior chamber The lesion is > 2mm from the visual axis

17

18
19 DISTRIBUTION OF CAUSATIVE ORGANISMS IN MONOMICROBIAL KERATITIS LEVY SB ET AL CORNEA. 1997; 16: H. INFLUENZA, MORAXELLA Organism Staphylococcus epidermidis Percent of infections 47% Pseudomonas Aeruginosa 21% Staphylococcus aureus 13.2% Serratia 5.3% Gram+/ Streptococcus pneumonia** 5.3% +
20 BACTERIAL FLORA IN THE NORMAL EYE Staph epidermidis % Diptheroida 20-33% Staphylococcus aureus 20-25% Hemophilus influenza. 3% or > Streptococcus pneumoniae 1-3 % Gram negative rods 1% Psuedomonas 0-5%
21 GRAM (+) COCCI (EYE PATHOGENS) Staphylococcus Aureus/ epidermidis Micrococcus Species Streptococcus pneumonia Streptococcus pyogenese Streptococcus viridans
22 GRAM (+) BACILLI (EYE PATHOGENS) Cornybacterium Propionibacterium Acnes ( P. Acnes) Clostidium Listeria
23 GRAM (-) COCCI (EYE PATHOGENS) Neisseria gonorrhoeae Moraxella Proteus Serratia Marcesens
24 GRAM (-) BACILLI (EYE PATHOGENS) Pseudomonas aeruginosa H. influenza Moraxella lacunata Proteus Serratia Marcescens
25 PSEUDOMONAS AERUGINOSA Ubiquitous gram (-) rod Most virulent corneal pathogen Can not penetrate an intact corneal epithelium Can perforate a cornea in 24 hours
26 THESE BACTERIA CAUSE RAPID TISSUE DESTRUCTION Pseudomonas Streptococcus pneumoniae gonococcus
27 RESULTS OF BACTERIAL KERATITIS Corneal scarring Visual morbidity Corneal perforation Endophthalmitis
28 RETROSPECTIVE CASE SERIES WILL S EYE HOSPITAL ( MAH-SADORRA JH ET AL CORNEA 2005) In , 12% of all cases were related to CL wear In , 30% of all cases were related to CL use 43 % of CL related infections related to daily wear, frequent replacement soft CL s
29 BACTERIA, FUNGI, PROTOZOA AND VIRUSES CAN ALL INFECT THE CORNEA How do we know what we are dealing with?
30 DIFFERENTIAL DIAGNOSIS Must differentiate from: Herpetic ulcers Hypoesthesia, geographic lesions, dendritic lesions Disciform lesions of stroma / ring immune infiltrate Fungal ulcers Characteristic feathery appearance Poor response to antibiotic therapy History of vegetative trauma

31 HSK Geographic ulcer Dendritic ulcer

32 EPITHELIAL WITH STROMAL DISEASE

33 FUNGAL KERATITIS
34 DIAGNOSIS Clinical suspicion, corneal scraping, superficial keratectomy Diagnostic stains: Gram stain, Giemsa stain, PAS, acridine orange, calcofluor white Culture media: Sabouraud s dextrose agar, blood agar Confocal microscopy
35 MOST COMMON FUNGAL KERATITIS Aspergillus, filamentous fungi Fusarium, filamentous fungi, Yeast ( candida albicans) There are 40 different genera that cause keratomycoses Nation wide about 300 cases per year Treatment: Natamycin 5% (Natacyn) Amphotericin B 0.15%
36 TREATMENT OF FUNGAL KERATITIS Topical : natamycin 5 % suspension Q1h for hrs Amphotericin-B % Q minutes for hours Miconazole 1%- very toxic Q1h Oral therapy Ketoconazole (Nizoral) or Fluconizole ( Diflucan) mg /day


37 FUNGAL KERATITIS

38 FUNGAL KERATITIS
39 DIFFERENTIAL DIAGNOSIS Endophthalmitis does not follow bacterial keratitis without corneal perforation Unlike fungal keratitis Therefore A/C and vitreous taps are not necessary when perforation is absent in bacterial keratitis!
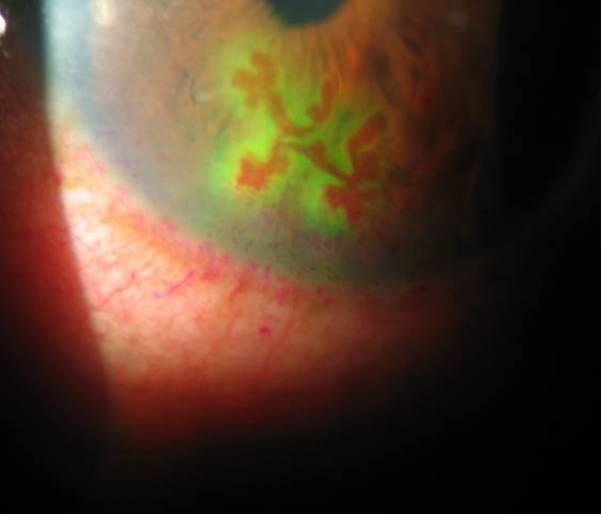
40 ACANTHAMOEBA KERATITIS: COURSE Pain, photophobia, and tearing that is out of proportion with the clinical picture Often starts as non-specific keratitis Epithelial micro-erosions, micro-cystic edema and perineural infiltrates in radial pattern Proceeding to a classic ring infiltrate
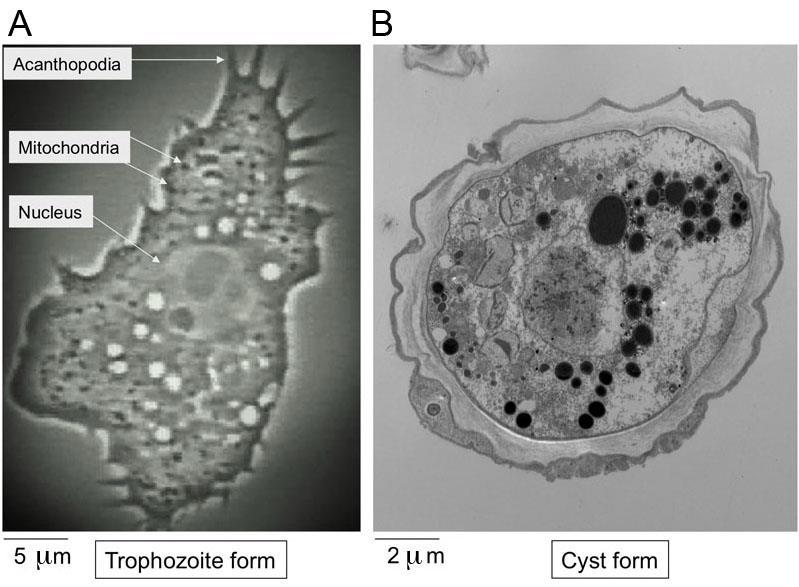
41 ACANTHAMOEBA KERATITIS: PROTOZOAN A ubiquitous protozoan feeds on other microbes not human tissue Seven species infect the eye Explains indolent course Has the ability to encyst when food supply is low Most have a history of CL wear with bad hygiene habits Unsanitary water conditions; lakes pools hot-tubs 10% are not CL wearers

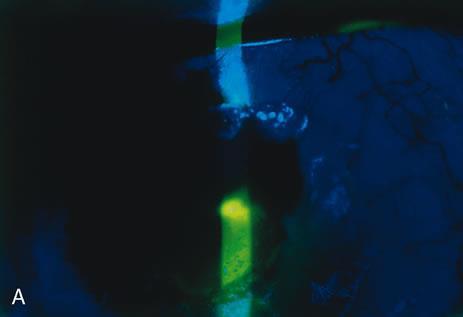
42 ACANTHAMOEBA KERATITIS
43

44 ENCYSTED ORGANISM : ACANTHAMOEBA

45 ACANTHAMOEBA KERATITIS: TREATMENT Brolene 0.1% Polyhexamethylene Biguanide (PHMB) 0.2% DESTROYS cysts and trophozoites Alternate therapies include; Neomycin Clotrimazole Chlorhexidine Baquacil
46 TREATMENT OF ACANTHAMOEBA USE ONE FROM THE BIOCIDE/CATIONIC ANTISEPTIC GROUP PLUS ONE OR MORE OF THE FOLLOWING Polyhexamethylene biguanide (PHMB, Baquasil, Cosmocil) chlorhexidine digluconate
47 TREATMENT OF ACANTHAMOEBA Antibiotic / Aminoglycoside Paromomycin ( Humatin)/ neomycin Antifungal Clotrimazole,ketoconazole, itraconazole, miconazole,fluconazole ( Diflucan) Anti-parasitic Propamidine isethionate (Brolene)
48 DIFFERENTIAL DIAGNOSIS Non-infectious stromal inflammation may be associated with CL wear (EWCL) Systemic diseases such as collagen vascular disorders ( RA, SLE) Vasculitic disorders polyarteritis nodosa Wegener s granulomatosis Sarcoid Severe rosacea Atopy/ limbal vernal
49 CORNEAL PERFORATIONS
50 CORNEAL CULTURING AND SCRAPINGS A must in severe bacterial keratitis!
51 INDICATIONS FOR CORNEAL CULTURING CORNEAL SCRAPING IS A MUST IN SEVERE/SERIOUS INFECTIOUS KERATITIS Central location Large lesions (>2mm) Painful lesions Post-op corneal infections Suspected fungal infection
52 WHEN YOU NEED TO CULTURE Depth of infiltrate middle to deep stroma Simultaneous presence of significant A/C reaction, fibrin or hypopyon Poor vision Presence of corneal abscess Unresponsive to broad spectrum therapy!
53 HOW TO CULTURE AND OBTAIN RELIABLE RESULTS MAXIMIZING YOUR YIELD
54 CULTURING: WHAT IS OUR GOAL The culture guided approach to managing bacterial keratitis involves taking a sample of corneal tissue ( by scraping) and performing microbiological tests to determine the type of bacterial organisms and their sensitivities Avoiding contamination and false positives!
55 WHAT YOU WILL NEED: SUPPLIES Kimura Spatula Heat sterilization method Culture media Blood agar Chocolate agar Thioglycolate broth Sabaraud s dextrose agar Access to calcofluor white
56 STANDARD CULTURE MEDIA Culture media Blood agar Chocolate Agar Thioglycolate broth Sabaraud's dextrose agar Growth of Isolates Aerobic and facultative anaerobic bacteria P. aeruginosa, S. aureus, S.epidermidis, S.pneumonia H. influenza, N. Gonorrhea, bartonella species Aerobic and facultative anaerobic bacteria Fungi
57 SUPPLEMENTAL CULTURE MEDIA Culture media Anaerobic Blood agar Lowenstein-Jensen Middlebrook agar Thayer- Martin Agar Growth of Isolates P. Acnes, streptococcus Mycobacterium species Mycobacterium species Pathogenic Neisseria
58 WHAT YOU WILL NEED: SUPPLIES Sterile cotton swabs Glass microscopic slides for gram staining and smears

59 CULTURING SUPPLIES
60 KIMURA SPATULA
61 HOW TO CULTURE: TECHNIQUE Instill topical anesthetic! (better if preservative free) This helps with patient cooperation Yield may improve if PF anesthetics are used Culturing only the purulent material often yields inadequate sample Grab stroma! Inoculate directly onto culture media Consider the CL case, the CL and solutions!
62 HOW TO CULTURE: TECHNIQUE Consider culturing when ulcer presents with features that are suggestive of fungal, amoebic or mycobacterial keratitis Culture when the history is suspicious Trauma Vegetative injury CL hx. In lakes, pools, or hot tubs Post LASIK
63 SPECIALIZED CULTURES Fungal Acanthamoeba Moraxella Proteus

64 CULTURING TECHNIQUES

65 CULTURING TECHNIQUES
66 DIAGNOSTIC STAINS Diagnostic stain Gram Stain Giemsa Stain Acid fast Acridine Orange Calcofluor White Organisms Visualized Best for bacteria, can visualize fungi and Acanthamoeba Bacteria, fungi, chlamydia, Acanthamoeba Mycobacterium, nocardia Bacteria,fungi, Acanthamoeba fungi, Acanthamoeba

67

68 GRAM STAIN PROCEDURE
69 STAINING PROPERTIES OF BACTERIA
70 INVITRO VIEW

71 TREATMENT OF BACTERIAL KERATITIS Review of Standard of Care And New Treatment Alternatives
72 GOALS OF THERAPY Preserve the globe Minimize stromal scar formation Minimize inducement of irregular astigmatism Vision rehabilitation PTK CL s or PK Collagen cross linking
73 MOST CASES OF COMMUNITY ACQUIRED BACTERIAL KERATITIS RESPOND TO EMPIRICAL TREATMENT WITH BROAD SPECTRUM ANTIBIOTICS Preferred Practice Guidelines on bacterial keratitis, AAO
74 KEYS TO SUCCESSFUL THERAPY RAPID RECOGNITION TIMELY INSTITUTION OF THERAPY APPROPRIATE FOLLOW-UP
75 MEDICAL TREATMENT Broad spectrum topical antibiotics Fluoroquinolones 2 nd generation.. Ciloxan, Ocuflox 3 rd generation Quixin 4 th generation Vigamox, Zymar, Besivance Fortified Antibiotics: When to use them Judicious Use of Corticosteroids
76 PROCEDURAL TREATMENT Cultures and smears Cultures and sensitivities Gram/ geimsa staining Deeper tissue corneal biopsy TISSUE GLUE Collagen cross linking PDT PTK PKP
77 BROAD SPECTRUM ANTIBIOTICS ARE THE MAINSTAY OF TREATMENT PREFERRED TREATMENT IN NON-SEVERE CASES

78 BROAD SPECTRUM ANTIBIOTICS THE FLUOROQUINOLONES 2 nd generation: ciprofloxacin, ofloxacin 3 rd generation: levofloxacin 4 th generation: moxifloxacin, gatifloxacin, besifloxacin
79 THE FLUOROQUINOLONES: SOME INTERESTING POINTS Some clinical trials have shown 4 th generation Fluoroquinolones to be as effective/potent as combined fortified antibiotics against the common pathogens that cause bacterial keratitis The Ofloxacin Study Group, Ophthalmology 1997 There are still concerns with resistance (2 nd and 3 rd gen) No difference in clinical efficacy or overall time to cure
80 TOPICAL FLUOROQUINOLONES: CLINICAL INDICATIONS Drug / concentration Indications Rec. treatment duration Ciprofloxacin 0.3% Ofloxacin 0.3% Conjunctivitis Corneal ulcers Conjunctivitis Corneal ulcers 7days 14 days 7 days 9 days 3 rd gen Levofloxacin 0.5% 4 th gen Bacterial conjunctivitis Corneal ulcers 7days Moxifloxacin 0.5% Bacterial conjunctivitis 7days TID Gatifloxacin 0.3% Bacterial conjunctivitis Days 1-2 q2h Days 3-7 QID
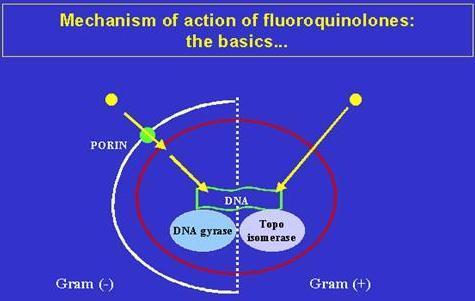
81 THE MECHANISM OF ACTION OF FLUOROQUINOLONES Fluoroquinolones inhibit bacterial DNA gyrase (topoisomerase II), topoisomerase IV OR BOTH. These are the key enzymes in bacterial DNA replication and transcription 2 nd generation FQ inhibit DNA gyrase 3 rd generation FQ inhibits DNA gyrase 4 th generation FQ inhibit both enzymes Inhibition of these enzymes will result in bacterial cell death
82 THE FLUOROQUINOLONES: MOA Topoisomerase IV is the main target for most gram + organisms DNA gyrase ( topoisomerase II) is the main target for most gram negatives 4 th Generation FQ inhibit both Gatifloxacin, Moxifloxacin, besifloxacin 2 nd generation FQ inhibit / target DNA gyrase ( topoisomerase II) Ciprofloxacin, ofloxacin
83

84
85 TOPICAL 4 TH GENERATION FQ ARE GOOD ALTERNATIVES TO COMBINATION FORTIFIEDS
86 THE 4 TH GEN FLUOROQUINOLONES Highly soluble with excellent tissue penetration BAK free..self preserved! (Vigamox) Formulated at near neutral (6.8) ph = comfort Less likely to select for resistance
87 4 TH GENERATION FLUOROQUINOLONES Several controlled studies have shown both gatifloxacin and moxifloxacin performed at least as well as standard therapy with fortified cefazolin and tobramycin Both 4 th gen fluoroquinolones are not approved for treatment of bacterial keratitis by the FDA Any use in this regard is off label So what is the standard of care?
88 THE 4 TH GEN FLUOROQUINOLONES The 4 th generation FQ s are more effective against Gram + organisms while maintaining adequate coverage against Gram (-) One FQ resistant organism is atypical mycobacterium
89 4 TH GEN FLUOROQUINOLONES: STUDIES SUPPORTING USE Parmar et al compared gatifloxacin 0.3% to ciprofloxacin 0.3% in treatment of bacterial keratitis ( ulcers > 2mm). Looked at the susceptibility to bacterial isolates Dosing q1h for bacterial ulcers Found susceptibility to gram + was 96% to gatifloxacin, 60% to ciprofloxacin Found susceptibility to gram Was 93% to gatifloxacin Was 86% to ciprofloxacin
90 4 TH GEN FLUOROQUINOLONES: STUDIES SUPPORTING USE Shah et al looked at bacterial corneal ulcers >2mm and randomized their treatment to: Moxifloxacin 0.5%, q1h for hours Gatifloxacin 0.3% q1h for hours Fortified AB ( 5% Cefazolin, 1.3% Tobramycin) or (10.4% Cefazolin with 5.2% Tobramycin) both q1h Cure rates for Fortifieds was 90% Cure rates Gatifloxacin/moxifloxacin group was 95%
91 MIC 90 S MIC 90 for Gram + s is lower for 4 th generation FQ than 2nd or 3 rd Especially for FQ resistant staph aureus MIC 90 for Gram s is better with the 2 nd generation than 4 th gen. FQ Of the 4 th generation FQ Moxifloxacin has a lower MIC 90 for most gram + Gatifloxacin has a lower MIC 90 for most gram One interesting fact is ciprofloxacin (2 nd gen.) had lower MIC 90 s than both the 4 th generation FQ against gram s ( esp pseudomonas species)
92 TOPICAL FLUOROQUINOLONES Current treatment of choice in non-severe bacterial keratitis Treatment is broken down into 2 critical phases each with a clear endpoint for clinical review and decision making Sterilization Phase Clinical signs may not indicate when sterilization has occurred after starting intensive therapy Sterilization often precedes both epithelialization and resolution of inflammatory signs Healing phase
93 DOSING OF THE FLUOROQUINOLONES IN SUSPECTED BACTERIAL KERATITIS Dosing needs to be aggressive early on in treatment Q 5-15 min to start for several hours Q 30 min through the first day Q 1-2 hours through the night Checking for improvement daily or every other day
94 DOSING IN LESS SEVERE KERATITIS Q2h, q3h with loading dose hs Cycloplegics for pain and synechia prevention.

95 SEVERE BACTERIAL KERATITIS

96 SEVERE BACTERIAL KERATITIS
97 FOLLOW-UP PROTOCOL Frequent initially every day until clinical improvement is seen Frequency of re-evaluation depends on extent of disease Then follow-up appointments can be spaced according to level of improvement and practitioner comfort level
98 NIGHT TIME THERAPY: DO I HAVE TO HAVE MY PATIENT GET UP DURING THE NIGHT? Depends on severity of disease If the patient has a central ulcer with reduced VA ---YES! Any features consistent with severe keratitis Yes! If the lesion is mid-peripheral and less ominous consider Ointment HS (as cover hs) Loading Dose HS Avoid using ointments in patients with severe keratitis!
99 FEATURES OF SEVERE INFECTIOUS KERATITIS Significant pain Dense central infiltrates Large Ulcers Hypopyon/ fibrin in AC Suppurative lesions/ liquifactive necrosis The stroma turns to soup! Unresponsive to initial therapy with 4 th gen FQ
100 FEATURES OF SEVERE INFECTIOUS KERATITIS Infection extending into sclera May require injected sub-conjunctival AB Heavy mucous discharge Impending perforation Gonococcal keratitis Requires systemic therapy Oral Azithromycin or Doxycycline 100 mg BID X 7 days
101 FEATURES SUGGESTIVE OF POSITIVE RESPONSE TO TREATMENT Decreased pain Decreased discharge Lessened eyelid edema Decreased density of stromal infiltrate Reduced stromal edema
102 FEATURES SUGGESTIVE OF POSITIVE RESPONSE TO TREATMENT Consolidation and sharper demarcation of stromal infiltrates perimeter Reduced A/C reaction, fibrin, hypopyon Re-epithelialization, reduced epithelial defect Measure it!!!

103

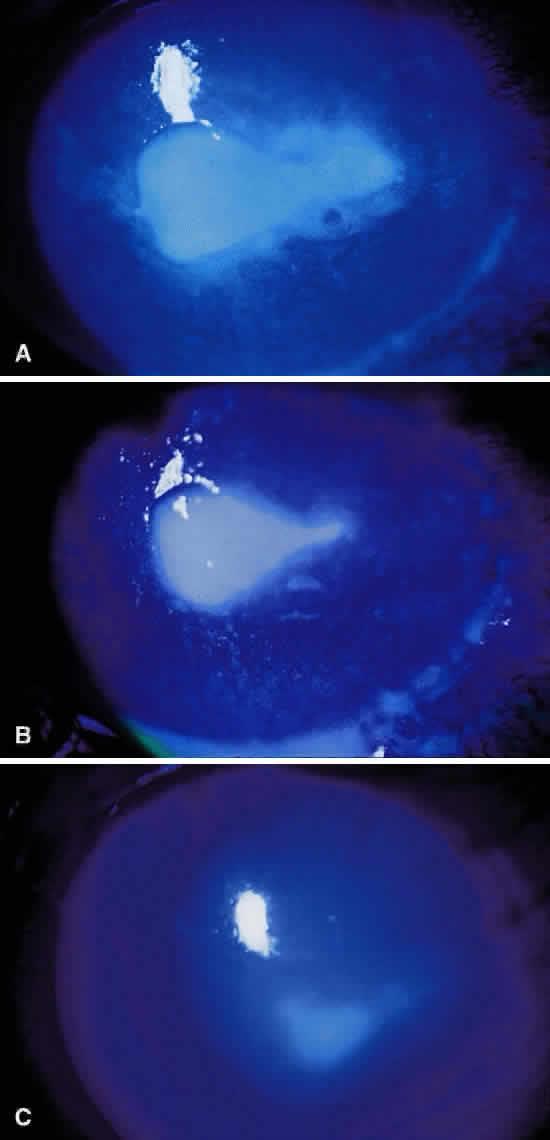
104 POSITIVE RESPONSE TO TREATMENT: SERRATIA
105 MODIFICATION OF THERAPY: Efficacy of treatment judged on clinical response to empirical treatment If condition improving therapy need not be adjusted on basis of lab results Dual AB therapy may not be necessary Modify the treatment plan if the eye shows a lack of response / improvement after hours Culture results may have an impact on the modification of therapy Especially when the response has been poor
106 WHAT ABOUT RESISTANCE: CAN IT HAPPEN? 2 concomitant mutations are necessary for the development of resistance to the 4 th generation fluoroquinolones
107 EMERGING CHALLENGES: BACTERIAL RESISTANCE TO FQ Already widespread resistance to 3 rd generation FQ Studies have shown increasing resistance to 2 nd generation FQ Prashant et al Ophthalmology July 1999 Studied cultured proven pseudomonas keratitis % were ciprofloxacin resistant % were ciprofloxacin resistant
108 THE MECHANISMS RESISTANCE TO FQ Mutation of target enzymes Formation of gyrase protecting proteins Reduction in cell permeability Increases in drug efflux Despite all this still a relatively low incidence of resistance to 4 th gen FQ

109 RESISTANCE TO THERAPY
110 NEW KIDS ON THE BLOCK: THE LATEST PLAYERS Zymaxid 0.5%, gatifloxacin, Zymar 0.3% Moxeza 0.5%, moxifloxacin with xanthan gum vehicle Prolongs contact time with the ocular tissues Increases tissue penetration Besivance 0.6%, besifloxacin ophthalmic suspension formulated with Durasite vehicle Good broad spectrum FQ Should have increased contact time and better tissue penetration as a result of Durasite No FDA labeling for bacterial keratitis, only bacterial conjunctivitis Novel fluoroquinolone without a systemic counterpart
111 BESIVANCE : BESIFLOXACIN Only dual halogenated fluoroquinolone AB Effective treatment in studies for : MRSA (previous FQ have shown to be poorly effective) MRSE Pseudomonas aeruginosa (FDA approval) on its labeling Potent balanced inhibition DNA gyrase inhibition- hits gram - s Topoisomerase IV inhibition hits gram + s bactercidal drug Uses the same Durasite muco-adhesive vehicle as Azasite

112 MODIFYING THERAPY IN SEVERE DISEASE
113 MODIFICATION OF AB THERAPY: SEVERE DISEASE Every 5-15 minutes in the 1 st few hours Every 15 minutes to 1 hour around the clock Patient sets alarm to get up during night! Cycloplegia pain from cilliary spasms reduce posterior synechia
114 WHAT IF THINGS ARE GOING BADLY? CONSIDER FORTIFIED ANTIBIOTICS! FOR SEVERE INFECTION OF EYES UNRESPONSIVE TO TREATMENT WITH SINGLE AGENTS
115 COMPOUNDING FORTIFIED ANTIBIOTICS Drug Effective against Concentration Cefazolin Gram + 50mg/ml Vancomycin Gram + 15mg/ml 25mg/ml 50mg/ml Tobramycin Gram - 14mg/ml Gentamycin Gram - 14mg/ml
116 FORTIFIED ANTIBIOTICS THE LONGSTANDING STANDARD OF CARE Probably the best choice in the eyes of the law Have withstood the test of time
117 TREATMENT PEARLS: SEVERE BACTERIAL KERATITIS Bandage CL s and Collagen shields are risky in treatment of severe bacterial keratitis They can become dislodged interrupting AB therapy May actually impair AB penetration into the ulcer bed Subconjunctival AB therapy in cases of scleral extension, systemic infection Steer away from ointments at night, the drops are more potent and these interfere with penetration of fortifieds or 4 th FQ Instead dose through the night!

118 TREATMENT ROLE OF STEROIDS When to pull the trigger!
119 CORTICOSTEROID USE FOR INFECTIOUS KERATITIS Many believe steroids have a place in treatment of bacterial keratitis Judicious use of steroids can reduce ocular morbidity Suppresses inflammation and subsequent scarring leading to better visual outcomes Ideally should not be used until culture results return or positive response to therapy
120 CORTICOSTEROID USE FOR INFECTIOUS KERATITIS In order to have success with steroid therapy Use the minimal amount of steroid required to control inflammation Optimal timing: AB response, C/S results, not fungal Careful dose regulation use adequate and appropriate concomitant AB Close follow up, monitor IOP
121 IN TREATMENT OF SEVERE BACTERIAL KERATITIS INVOLVING THE VISUAL AXIS General Rule of Thumb After 2-3 days of steady improvement with topical AB s safe to introduce a steroid
122 DISADVANTAGES WITH STEROID TREATMENT Recurrence of infection Local immunosuppression Inhibition of collagen synthesis predisposing to corneal melts No conclusive evidence that steroids alter the clinical outcome in bacterial keratitis Closer follow-up is necessary Optimal timing and dose regulation
123 TREATMENT IN COMPLICATED CASES Perforations, progressive unresponsive disease, Endophthalmitis
124 ADJUVANT THERAPY Collagenase inhibitors EDTA, Tetracyclines, Doxycycline Steroids? NSAIDS Tissue adhesives Debridement/ biopsy Bandage lenses/ collagen shields Therapeutic / tectonic PK
125 COLLAGEN CROSS-LINKING: NEW TREATMENT Collagen cross-linking (CXL) is a technique that uses riboflavin (B2) and Ultraviolet-A irradiation to cause a strengthening effect in corneal tissue which enhances its rigidity. The interactive effect of riboflavin with UV-A irradiation strengthens formation of chemical bonds between collagen fibrils in the corneal stroma and helps in increasing resistance against enzymatic digestion
126 COLLAGEN CROSS-LINKING Collagen cross-linking may be considered in treatment-resistant infectious keratitis or as an adjunct to antibiotics therapy
127 COLLAGEN CROSS-LINKING Three patients with Acanthamoeba keratitis were successfully treated with a topical application of 0.1% riboflavin solution and 30 minutes of UV irradiation focused on the corneal ulcer. [2]

128 TREATMENT IN COMPLICATED CASES Perforation Tissue glue
129 THERAPY IN COMPLICATED CASES Thin Corneas Impending perforation Tissue adhesives PK Lamellar PK Endophthalmitis


130

131 THANKS FOR YOUR ATTENTION
132 Gregory M. Schultz, O.D.,F.A.A.O. Eye Center of Virginia Williamsburg VA
Topical Antibiotic Update. Brad Sutton, O.D., F.A.A.O. Indiana University School of Optometry Indianapolis Eye Care Center No financial disclosures
 Topical Antibiotic Update Brad Sutton, O.D., F.A.A.O. Indiana University School of Optometry Indianapolis Eye Care Center No financial disclosures What do we have? We currently have many highly effective
Topical Antibiotic Update Brad Sutton, O.D., F.A.A.O. Indiana University School of Optometry Indianapolis Eye Care Center No financial disclosures What do we have? We currently have many highly effective
Infectious keratitis for the general ophthalmologist
 Infectious keratitis for the general ophthalmologist Presented by Chameen Samarawickrama - Westmead Hospital - Liverpool Hospital - University of Sydney - University of New South Wales The University of
Infectious keratitis for the general ophthalmologist Presented by Chameen Samarawickrama - Westmead Hospital - Liverpool Hospital - University of Sydney - University of New South Wales The University of
Clinical Features, Antibiotic Susceptibility Profile, and Outcomes of Infectious Keratitis Caused by Stenotrophomonas maltophilia
 Clinical Features, Antibiotic Susceptibility Profile, and Outcomes of Infectious Keratitis Caused by Stenotrophomonas maltophilia Sotiria Palioura, MD, MSc, PhD Cornea & External Disease Specialist Athens
Clinical Features, Antibiotic Susceptibility Profile, and Outcomes of Infectious Keratitis Caused by Stenotrophomonas maltophilia Sotiria Palioura, MD, MSc, PhD Cornea & External Disease Specialist Athens
Role of Moxifloxacin in Bacterial Keratitis
 Original Article Role of Moxifloxacin in Bacterial Keratitis Aamna Jabran, Aurengzeb Sheikh, Syed Ali Haider, Zia-ud-din Shaikh Pak J Ophthalmol 29, Vol. 25 No. 2.................................................................................
Original Article Role of Moxifloxacin in Bacterial Keratitis Aamna Jabran, Aurengzeb Sheikh, Syed Ali Haider, Zia-ud-din Shaikh Pak J Ophthalmol 29, Vol. 25 No. 2.................................................................................
Bacterial Resistance. The Battle of the Bugs: Treating Infections in the Age of Resistance. How Resistance Develops. The Age of Modern Medicine
 The Age of Modern Medicine The Battle of the Bugs: Treating Infections in the Age of Resistance Mark T. Dunbar, O.D., F.A.A.O. Bascom Palmer Eye Institute University of Miami, Miller School of Med Miami,
The Age of Modern Medicine The Battle of the Bugs: Treating Infections in the Age of Resistance Mark T. Dunbar, O.D., F.A.A.O. Bascom Palmer Eye Institute University of Miami, Miller School of Med Miami,
Downloaded from
 Guidelines for the Management of Suspected Microbial Keratitis in Settings with Limited Laboratory Facilities Wani MG, Consultant Ophthalmologist, Sakubva Eye Unit, Mutare Zimbabwe a Introduction Microbial
Guidelines for the Management of Suspected Microbial Keratitis in Settings with Limited Laboratory Facilities Wani MG, Consultant Ophthalmologist, Sakubva Eye Unit, Mutare Zimbabwe a Introduction Microbial
Burton's Microbiology for the Health Sciences. Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents
 Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
Bacterial Keratitis Limited Revision
 Bacterial Keratitis Limited Revision Prepared by the American Academy of Ophthalmology Cornea/External Disease Panel Cornea/External Disease Panel Members Robert S. Feder, MD, Chair Steven P. Dunn, MD
Bacterial Keratitis Limited Revision Prepared by the American Academy of Ophthalmology Cornea/External Disease Panel Cornea/External Disease Panel Members Robert S. Feder, MD, Chair Steven P. Dunn, MD
Study of Bacteriological Profile of Corneal Ulcers in Patients Attending VIMS, Ballari, India
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 7 (2016) pp. 200-205 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.507.020
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 7 (2016) pp. 200-205 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.507.020
Evaluation of Moxifloxacin 0.5% Eye Drops in Treatment of Bacterial Corneal Ulcers
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. II (Nov. 2017), PP 15-19 www.iosrjournals.org Evaluation of Moxifloxacin 0.5% Eye Drops
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. II (Nov. 2017), PP 15-19 www.iosrjournals.org Evaluation of Moxifloxacin 0.5% Eye Drops
A 3½-Year Study of Bacterial Keratitis From Odisha, India
 ORIGINAL CLINICAL STUDY A 3½-Year Study of Bacterial Keratitis From Odisha, India Bibhudutta Rautaraya, MD,* Savitri Sharma, MD,* Md. Hasnat Ali, MBA,Þ Sarita Kar, MSc,* Sujata Das, MS, FRCS(Glasg),* and
ORIGINAL CLINICAL STUDY A 3½-Year Study of Bacterial Keratitis From Odisha, India Bibhudutta Rautaraya, MD,* Savitri Sharma, MD,* Md. Hasnat Ali, MBA,Þ Sarita Kar, MSc,* Sujata Das, MS, FRCS(Glasg),* and
The Battle of Resistance: Treating Infections in the Age of Resistance
 The Age of Modern Medicine The Battle of Resistance: Treating Infections in the Age of Resistance Mark T. Dunbar, O.D., F.A.A.O. Bascom Palmer Eye Institute University of Miami, Miller School of Med Miami,
The Age of Modern Medicine The Battle of Resistance: Treating Infections in the Age of Resistance Mark T. Dunbar, O.D., F.A.A.O. Bascom Palmer Eye Institute University of Miami, Miller School of Med Miami,
CLPNA Pressure Ulcers ecourse: Module 5.6 Quiz II page 1
 CLPNA Pressure Ulcers ecourse: Module 5.6 Quiz II 1. What are the symptoms of an infected wound? a. Fever b. Edema c. Erythema d. Local pain and tenderness e. Induration of wound edge 2. A person with
CLPNA Pressure Ulcers ecourse: Module 5.6 Quiz II 1. What are the symptoms of an infected wound? a. Fever b. Edema c. Erythema d. Local pain and tenderness e. Induration of wound edge 2. A person with
Financial disclosures
 Financial disclosures Named co-inventor on PCT applications CH2012/0000090 and PCT2014/CH000075 Chief Scientific Officer EMAGine SA Historical decision in 2004 1. Future: extremely thin corneas Dresden
Financial disclosures Named co-inventor on PCT applications CH2012/0000090 and PCT2014/CH000075 Chief Scientific Officer EMAGine SA Historical decision in 2004 1. Future: extremely thin corneas Dresden
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Bacterial Keratitis Preferred Practice Pattern
 Bacterial Keratitis Preferred Practice Pattern 2018 by the American Academy of Ophthalmology Published by Elsevier Inc. https://doi.org/10.1016/j.ophtha.2018.10.018 ISSN 0161-6420/18 Secretary for Quality
Bacterial Keratitis Preferred Practice Pattern 2018 by the American Academy of Ophthalmology Published by Elsevier Inc. https://doi.org/10.1016/j.ophtha.2018.10.018 ISSN 0161-6420/18 Secretary for Quality
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Bacterial Resistance. Battle of the Bugs: Treating Infections in the Age of Resistance. How Resistance Develops 10/16/2009. The Age of Modern Medicine
 The Age of Modern Medicine Battle of the Bugs: Treating Infections in the Age of Resistance Mark T. Dunbar, O.D., F.A.A.O. Bascom Palmer Eye Institute University of Miami, Miller School of Med Miami, FL
The Age of Modern Medicine Battle of the Bugs: Treating Infections in the Age of Resistance Mark T. Dunbar, O.D., F.A.A.O. Bascom Palmer Eye Institute University of Miami, Miller School of Med Miami, FL
MOXICIP Eye Ointment (Moxifloxacin 0.5%)
") Published on: 19 Sep 2014 MOXICIP Eye Ointment (Moxifloxacin 0.5%) Composition Moxifloxacin 0.5% (5 mg/ml) Dosage Form Ophthalmic Ointment Pharmacology Pharmacodynamics Moxifloxacin is a member of the
Published on: 19 Sep 2014 MOXICIP Eye Ointment (Moxifloxacin 0.5%) Composition Moxifloxacin 0.5% (5 mg/ml) Dosage Form Ophthalmic Ointment Pharmacology Pharmacodynamics Moxifloxacin is a member of the
Burn Infection & Laboratory Diagnosis
 Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Protein Synthesis Inhibitors
 Protein Synthesis Inhibitors Assistant Professor Dr. Naza M. Ali 11 Nov 2018 Lec 7 Aminoglycosides Are structurally related two amino sugars attached by glycosidic linkages. They are bactericidal Inhibitors
Protein Synthesis Inhibitors Assistant Professor Dr. Naza M. Ali 11 Nov 2018 Lec 7 Aminoglycosides Are structurally related two amino sugars attached by glycosidic linkages. They are bactericidal Inhibitors
F1 IN THE NAME OF GOD
 F1 IN THE NAME OF GOD Slide 1 F1 FEIKO.IR.SOFT; 2011/07/06 Lid Laceration Conjunctival Hemorrhage a) No therapy is necessary b) Usually resolve in 7-12 days. Subconjunctival Hemorrhage Corneal Abrasion
F1 IN THE NAME OF GOD Slide 1 F1 FEIKO.IR.SOFT; 2011/07/06 Lid Laceration Conjunctival Hemorrhage a) No therapy is necessary b) Usually resolve in 7-12 days. Subconjunctival Hemorrhage Corneal Abrasion
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Introduction to Chemotherapeutic Agents. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018
 Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Antibiotics. Antimicrobial Drugs. Alexander Fleming 10/18/2017
 Antibiotics Antimicrobial Drugs Chapter 20 BIO 220 Antibiotics are compounds produced by fungi or bacteria that inhibit or kill competing microbial species Antimicrobial drugs must display selective toxicity,
Antibiotics Antimicrobial Drugs Chapter 20 BIO 220 Antibiotics are compounds produced by fungi or bacteria that inhibit or kill competing microbial species Antimicrobial drugs must display selective toxicity,
Selective toxicity. Antimicrobial Drugs. Alexander Fleming 10/17/2016
 Selective toxicity Antimicrobial Drugs Chapter 20 BIO 220 Drugs must work inside the host and harm the infective pathogens, but not the host Antibiotics are compounds produced by fungi or bacteria that
Selective toxicity Antimicrobial Drugs Chapter 20 BIO 220 Drugs must work inside the host and harm the infective pathogens, but not the host Antibiotics are compounds produced by fungi or bacteria that
مادة االدوية المرحلة الثالثة م. غدير حاتم محمد
 م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
Fluoroquinolone and fortified antibiotics for treating bacterial corneal ulcers
 378 Centre for Eye Research Australia, The University of Melbourne, 32 Gisborne Street, East Melbourne, Victoria 3002, Australia N Gangopadhyay M Daniell L Weih H R Taylor Correspondence to: Dr Mark Daniell
378 Centre for Eye Research Australia, The University of Melbourne, 32 Gisborne Street, East Melbourne, Victoria 3002, Australia N Gangopadhyay M Daniell L Weih H R Taylor Correspondence to: Dr Mark Daniell
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Evaluation of Microbiological Profile of Ear Discharge of Patients Attending Otorhinolaryngology
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Evaluation of Microbiological Profile of Ear Discharge of Patients Attending Otorhinolaryngology
American Association of Feline Practitioners American Animal Hospital Association
 American Association of Feline Practitioners American Animal Hospital Association Basic Guidelines of Judicious Therapeutic Use of Antimicrobials August 1, 2006 Introduction The Basic Guidelines to Judicious
American Association of Feline Practitioners American Animal Hospital Association Basic Guidelines of Judicious Therapeutic Use of Antimicrobials August 1, 2006 Introduction The Basic Guidelines to Judicious
Bacterial Keratitis Should optometrists treat in the community?
 Case Record 13 Bacterial Keratitis Should optometrists treat in the community? December 2008 Dr Peter Frampton DOptom MSc FCOptom BAppSc(Optom)(AUS) DipTp(AS) DipTp(SP) DipTp(IP) Introduction Can Optometrists
Case Record 13 Bacterial Keratitis Should optometrists treat in the community? December 2008 Dr Peter Frampton DOptom MSc FCOptom BAppSc(Optom)(AUS) DipTp(AS) DipTp(SP) DipTp(IP) Introduction Can Optometrists
Pathogens and Antibiotic Sensitivities in Post- Phacoemulsification Endophthalmitis, Kaiser Permanente, California,
 Pathogens and Antibiotic Sensitivities in Post- Phacoemulsification Endophthalmitis, Kaiser Permanente, California, 2007-2012 Geraldine R. Slean, MD, MS 1 ; Neal H. Shorstein, MD 2 ; Liyan Liu, MD, MS
Pathogens and Antibiotic Sensitivities in Post- Phacoemulsification Endophthalmitis, Kaiser Permanente, California, 2007-2012 Geraldine R. Slean, MD, MS 1 ; Neal H. Shorstein, MD 2 ; Liyan Liu, MD, MS
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Inhibiting Microbial Growth in vivo. CLS 212: Medical Microbiology Zeina Alkudmani
 Inhibiting Microbial Growth in vivo CLS 212: Medical Microbiology Zeina Alkudmani Chemotherapy Definitions The use of any chemical (drug) to treat any disease or condition. Chemotherapeutic Agent Any drug
Inhibiting Microbial Growth in vivo CLS 212: Medical Microbiology Zeina Alkudmani Chemotherapy Definitions The use of any chemical (drug) to treat any disease or condition. Chemotherapeutic Agent Any drug
Other ingredients are sodium chloride and purified water.
 Page 1 of 7 SCHEDULING STATUS Schedule 4 PROPRIETARY NAME AND DOSAGE FORM EXOCIN (Eye Drops) COMPOSITION EXOCIN contains: Preservative: Benzalkonium chloride 0,005 % m/v Other ingredients are sodium chloride
Page 1 of 7 SCHEDULING STATUS Schedule 4 PROPRIETARY NAME AND DOSAGE FORM EXOCIN (Eye Drops) COMPOSITION EXOCIN contains: Preservative: Benzalkonium chloride 0,005 % m/v Other ingredients are sodium chloride
Debate Series editors: Susan Lightman and Peter McCluskey
 1167... Series editors: Susan Lightman and Peter McCluskey Correspondence to: M Daniell, Royal Victorian Eye and Ear Hospital, Melbourne, Victoria, 3065, Australia; daniellm@ozemail.com.au Accepted for
1167... Series editors: Susan Lightman and Peter McCluskey Correspondence to: M Daniell, Royal Victorian Eye and Ear Hospital, Melbourne, Victoria, 3065, Australia; daniellm@ozemail.com.au Accepted for
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Bacterial Resistance of Respiratory Pathogens. John C. Rotschafer, Pharm.D. University of Minnesota
 Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali. Lec 1
 Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Guidelines for Laboratory Verification of Performance of the FilmArray BCID System
 Guidelines for Laboratory Verification of Performance of the FilmArray BCID System Purpose The Clinical Laboratory Improvement Amendments (CLIA), passed in 1988, establishes quality standards for all laboratory
Guidelines for Laboratory Verification of Performance of the FilmArray BCID System Purpose The Clinical Laboratory Improvement Amendments (CLIA), passed in 1988, establishes quality standards for all laboratory
Before we get started
 Pediatric Acute Bacterial Conjunctivitis: 2010 Update Before we get started Comment cards (90 day follow-up survey) Please hold questions until end of program Educational Objectives Educational Objectives
Pediatric Acute Bacterial Conjunctivitis: 2010 Update Before we get started Comment cards (90 day follow-up survey) Please hold questions until end of program Educational Objectives Educational Objectives
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Challenges Emerging resistance Fewer new drugs MRSA and other resistant pathogens are major problems
 Micro 301 Antimicrobial Drugs 11/7/12 Significance of antimicrobial drugs Challenges Emerging resistance Fewer new drugs MRSA and other resistant pathogens are major problems Definitions Antibiotic Selective
Micro 301 Antimicrobial Drugs 11/7/12 Significance of antimicrobial drugs Challenges Emerging resistance Fewer new drugs MRSA and other resistant pathogens are major problems Definitions Antibiotic Selective
4/29/12. Dr. Taravella does not have any financial interest in the material, methods or techniques presented.
 Dr. Taravella does not have any financial interest in the material, methods or techniques presented. Michael J. Taravella Professor of Ophthalmology Rocky Mountain Lions Eye Institute University of Colorado
Dr. Taravella does not have any financial interest in the material, methods or techniques presented. Michael J. Taravella Professor of Ophthalmology Rocky Mountain Lions Eye Institute University of Colorado
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Community Acquired Pneumonia: An Update on Guidelines
 Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Course: Microbiology in Health and Disease Office Hours: Before or after Class or by appointment
 SYLLABUS BIOL 2900 SECTIONS C AND D Spring, 2011 Course: Microbiology in Health and Disease Office Hours: Before or after Class or by appointment Semester Begins on January 10, 2011 and ends on May 2,
SYLLABUS BIOL 2900 SECTIONS C AND D Spring, 2011 Course: Microbiology in Health and Disease Office Hours: Before or after Class or by appointment Semester Begins on January 10, 2011 and ends on May 2,
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS
 Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Public Assessment Report Paediatric data. EXOCIN (OCUFLOX) Ofloxacin. Marketing Autorisation Holder: Allergan
 Ofloxacin. Marketing Autorisation Holder: Allergan") Public Assessment Report Paediatric data EXOCIN (OCUFLOX) Ofloxacin Marketing Autorisation Holder: Allergan Rapporteur: Co-Rapporteur: Currently approved indication(s): Pharmaceutical form(s) and strengths
Public Assessment Report Paediatric data EXOCIN (OCUFLOX) Ofloxacin Marketing Autorisation Holder: Allergan Rapporteur: Co-Rapporteur: Currently approved indication(s): Pharmaceutical form(s) and strengths
What s next in the antibiotic pipeline?
 What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
SYMMETRY FOAMING HAND SANITIZER with Aloe & Vitamin E Technical Data
 508 SYMMETRY FOAMING HAND SANITIZER with Aloe & Vitamin E Technical Data Physical Properties Active Ingredient: Ethyl Alcohol 62% (70% v/v) Appearance: Clear, Colorless Solution Fragrance: Floral Form:
508 SYMMETRY FOAMING HAND SANITIZER with Aloe & Vitamin E Technical Data Physical Properties Active Ingredient: Ethyl Alcohol 62% (70% v/v) Appearance: Clear, Colorless Solution Fragrance: Floral Form:
PACK-CXL. for infectious keratitis. Farhad Hafezi, MD PhD. Professor of Ophthalmology Keck School of Medicine USC Los Angeles, USA
 PACK-CXL for infectious keratitis Farhad Hafezi, MD PhD Professor of Ophthalmology University of Geneva Geneva, Switzerland Medical Director ELZA Institute Zurich, Switzerland Research Group Leader Lab.
PACK-CXL for infectious keratitis Farhad Hafezi, MD PhD Professor of Ophthalmology University of Geneva Geneva, Switzerland Medical Director ELZA Institute Zurich, Switzerland Research Group Leader Lab.
BIOL 2900 D 4.00 Microbiology in Health/Disease
 SYLLABUS BIOL 2900 - D Spring, 2017 Course: Microbiology in Health and Disease Instructor: Prafull C. Shah Office Hours: Before or after classes, or by appointment by Email to pcshah@valdosta.edu. Semester
SYLLABUS BIOL 2900 - D Spring, 2017 Course: Microbiology in Health and Disease Instructor: Prafull C. Shah Office Hours: Before or after classes, or by appointment by Email to pcshah@valdosta.edu. Semester
Redefining Infection Management. Proven Clinical Outcomes
 Proven Clinical Outcomes Proof of Bacteria-Binding1 In the first 30 seconds, 1 square centimeter of Cutimed Sorbact binds wound bacteria - after 2 hours, the amount of bacteria bound are more than would
Proven Clinical Outcomes Proof of Bacteria-Binding1 In the first 30 seconds, 1 square centimeter of Cutimed Sorbact binds wound bacteria - after 2 hours, the amount of bacteria bound are more than would
Course: Microbiology in Health and Disease
 SYLLABUS BIOL 2900 SECTION D SPRING 2012 Course: Microbiology in Health and Disease BIPIN PATEL Office Hours: Before or after Class or by appointment Semester Begins JANUARY 09 TO MAY 04 2012 2900 D 4.00
SYLLABUS BIOL 2900 SECTION D SPRING 2012 Course: Microbiology in Health and Disease BIPIN PATEL Office Hours: Before or after Class or by appointment Semester Begins JANUARY 09 TO MAY 04 2012 2900 D 4.00
Ophthalmology Research: An International Journal 2(6): , 2014, Article no. OR SCIENCEDOMAIN international
: , 2014, Article no. OR SCIENCEDOMAIN international") Ophthalmology Research: An International Journal 2(6): 378-383, 2014, Article no. OR.2014.6.012 SCIENCEDOMAIN international www.sciencedomain.org The Etiology and Antibiogram of Bacterial Causes of Conjunctivitis
Ophthalmology Research: An International Journal 2(6): 378-383, 2014, Article no. OR.2014.6.012 SCIENCEDOMAIN international www.sciencedomain.org The Etiology and Antibiogram of Bacterial Causes of Conjunctivitis
Antibacterial Agents & Conditions. Stijn van der Veen
 Antibacterial Agents & Conditions Stijn van der Veen Antibacterial agents & conditions Antibacterial agents Disinfectants: Non-selective antimicrobial substances that kill a wide range of bacteria. Only
Antibacterial Agents & Conditions Stijn van der Veen Antibacterial agents & conditions Antibacterial agents Disinfectants: Non-selective antimicrobial substances that kill a wide range of bacteria. Only
Microbiology : antimicrobial drugs. Sheet 11. Ali abualhija
 Microbiology : antimicrobial drugs Sheet 11 Ali abualhija return to our topic antimicrobial drugs, we have finished major group of antimicrobial drugs which associated with inhibition of protein synthesis
Microbiology : antimicrobial drugs Sheet 11 Ali abualhija return to our topic antimicrobial drugs, we have finished major group of antimicrobial drugs which associated with inhibition of protein synthesis
Lab Exercise: Antibiotics- Evaluation using Kirby Bauer method.
 Lab Exercise: Antibiotics- Evaluation using Kirby Bauer method. OBJECTIVES 1. Compare the antimicrobial capabilities of different antibiotics. 2. Compare effectiveness of with different types of bacteria.
Lab Exercise: Antibiotics- Evaluation using Kirby Bauer method. OBJECTIVES 1. Compare the antimicrobial capabilities of different antibiotics. 2. Compare effectiveness of with different types of bacteria.
INTRODUCTION TO WILDLIFE PHARMACOLOGY. Lisa Fosco Wildlife Rehabilitation Manager Toronto Wildlife Centre
 INTRODUCTION TO WILDLIFE PHARMACOLOGY Lisa Fosco Wildlife Rehabilitation Manager Toronto Wildlife Centre General Pharmacology Factors That Affect Drug Absorption The dosage form Blood supply to the area
INTRODUCTION TO WILDLIFE PHARMACOLOGY Lisa Fosco Wildlife Rehabilitation Manager Toronto Wildlife Centre General Pharmacology Factors That Affect Drug Absorption The dosage form Blood supply to the area
No-leaching. No-resistance. No-toxicity. >99.999% Introducing BIOGUARD. Best-in-class dressings for your infection control program
 Introducing BIOGUARD No-leaching. >99.999% No-resistance. No-toxicity. Just cost-efficient, broad-spectrum, rapid effectiveness you can rely on. Best-in-class dressings for your infection control program
Introducing BIOGUARD No-leaching. >99.999% No-resistance. No-toxicity. Just cost-efficient, broad-spectrum, rapid effectiveness you can rely on. Best-in-class dressings for your infection control program
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
number Done by Corrected by Doctor Dr Hamed Al-Zoubi
 number 8 Done by Corrected by Doctor Dr Hamed Al-Zoubi 25 10/10/2017 Antibacterial therapy 2 د. حامد الزعبي Dr Hamed Al-Zoubi Antibacterial therapy Figure 2/ Antibiotics target Inhibition of microbial
number 8 Done by Corrected by Doctor Dr Hamed Al-Zoubi 25 10/10/2017 Antibacterial therapy 2 د. حامد الزعبي Dr Hamed Al-Zoubi Antibacterial therapy Figure 2/ Antibiotics target Inhibition of microbial
PRESCRIBING INFORMATION
 PRESCRIBING INFORMATION Pr PENTAMYCETIN Chloramphenicol Ophthalmic Solution USP 0.25%, 0.5% Chloramphenicol Ophthalmic Ointment USP 1% Antibiotic Pr PENTAMYCETIN/HC Chloramphenicol and Hydrocortisone Eye
PRESCRIBING INFORMATION Pr PENTAMYCETIN Chloramphenicol Ophthalmic Solution USP 0.25%, 0.5% Chloramphenicol Ophthalmic Ointment USP 1% Antibiotic Pr PENTAMYCETIN/HC Chloramphenicol and Hydrocortisone Eye
Disclosure. Update on management of fungal keratitis. Acknowledgments. World Blindness 1993
 Update on management of fungal keratitis Tom Lietman, MD F I Proctor Foundation Department of Ophthalmology University of California San Francisco Disclosure Voriconazole donated by Pfizer Natamycin and
Update on management of fungal keratitis Tom Lietman, MD F I Proctor Foundation Department of Ophthalmology University of California San Francisco Disclosure Voriconazole donated by Pfizer Natamycin and
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Antibiotics in the future tense: The Application of Antibiotic Stewardship in Veterinary Medicine. Mike Apley Kansas State University
 Antibiotics in the future tense: The Application of Antibiotic Stewardship in Veterinary Medicine Mike Apley Kansas State University Changes in Food Animal Antibiotic Use How the uses of antibiotics in
Antibiotics in the future tense: The Application of Antibiotic Stewardship in Veterinary Medicine Mike Apley Kansas State University Changes in Food Animal Antibiotic Use How the uses of antibiotics in
Principles of Antimicrobial therapy
 Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
Cipro for gram positive cocci in urine
 Buscar... Cipro for gram positive cocci in urine 20-6-2017 Pneumonia can be generally defined as an infection of the lung parenchyma, in which consolidation of the affected part and a filling of the alveolar
Buscar... Cipro for gram positive cocci in urine 20-6-2017 Pneumonia can be generally defined as an infection of the lung parenchyma, in which consolidation of the affected part and a filling of the alveolar
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Package leaflet: Information for the user. HYDROCORTISON CUM CHLORAMPHENICOL 5 mg/g + 2 mg/g eye ointment hydrocortisone acetate, chloramphenicol
 Package leaflet: Information for the user HYDROCORTISON CUM CHLORAMPHENICOL 5 mg/g + 2 mg/g eye ointment hydrocortisone acetate, chloramphenicol Read all of this leaflet carefully before you start using
Package leaflet: Information for the user HYDROCORTISON CUM CHLORAMPHENICOL 5 mg/g + 2 mg/g eye ointment hydrocortisone acetate, chloramphenicol Read all of this leaflet carefully before you start using
Aminoglycosides. Spectrum includes many aerobic Gram-negative and some Gram-positive bacteria.
 Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
REVIEW OF OPHTHALMOLOGY SECTION OF WHO MODEL LIST OF ESSENTIAL MEDICINES. Sight Savers International and The Vision 2020 Technology Group
 REVIEW OF OPHTHALMOLOGY SECTION OF WHO MODEL LIST OF ESSENTIAL MEDICINES Anti infective agent Medicine suggested for inclusion Ciprofloxacin: 0.3 % eye drops Application submitted by Sight Savers International
REVIEW OF OPHTHALMOLOGY SECTION OF WHO MODEL LIST OF ESSENTIAL MEDICINES Anti infective agent Medicine suggested for inclusion Ciprofloxacin: 0.3 % eye drops Application submitted by Sight Savers International
Meropenem for all? Midge Asogan ICU Fellow (also ID AT)
") Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
PACKAGE LEAFLET: INFORMATION FOR THE USER. GENTAMICIN VISION 3 mg/g eye ointment Gentamicin
 PACKAGE LEAFLET: INFORMATION FOR THE USER GENTAMICIN VISION 3 mg/g eye ointment Gentamicin Read all of this leaflet carefully before you start using this medicine. - Keep this leaflet. You may need to
PACKAGE LEAFLET: INFORMATION FOR THE USER GENTAMICIN VISION 3 mg/g eye ointment Gentamicin Read all of this leaflet carefully before you start using this medicine. - Keep this leaflet. You may need to
Clinical Study Microbial Keratitis Profile at a University Hospital in Hong Kong
 International Scholarly Research Notices, Article ID 689742, 4 pages http://dx.doi.org/10.1155/2014/689742 Clinical Study Microbial Keratitis Profile at a University Hospital in Hong Kong Tracy H. T. Lai,
International Scholarly Research Notices, Article ID 689742, 4 pages http://dx.doi.org/10.1155/2014/689742 Clinical Study Microbial Keratitis Profile at a University Hospital in Hong Kong Tracy H. T. Lai,
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Class Update with New Drug Evaluation: Ototopical Antibiotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma
 Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma Lucio Petrizzi DVM DECVS Università degli Studi di Teramo Surgical site infections (SSI) Microbial contamination unavoidable Infection
Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma Lucio Petrizzi DVM DECVS Università degli Studi di Teramo Surgical site infections (SSI) Microbial contamination unavoidable Infection
In vitro antibiotic resistance in bacterial keratitis in London
 Br J Ophthalmol 2000;84:687 691 687 Moorfields Eye Hospital, London EC1V 2PD SJTuft Institute of Ophthalmology, London EC1V 9QS M Matheson Correspondence to: Mr S J Tuft, Moorfields Eye Hospital, City
Br J Ophthalmol 2000;84:687 691 687 Moorfields Eye Hospital, London EC1V 2PD SJTuft Institute of Ophthalmology, London EC1V 9QS M Matheson Correspondence to: Mr S J Tuft, Moorfields Eye Hospital, City
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements
 Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
INFECTIOUS DISEASES DIAGNOSTIC LABORATORY NEWSLETTER
 INFECTIOUS DISEASES DIAGNOSTIC LABORATORY NEWSLETTER University of Minnesota Health University of Minnesota Medical Center University of Minnesota Masonic Children s Hospital May 2017 Printed herein are
INFECTIOUS DISEASES DIAGNOSTIC LABORATORY NEWSLETTER University of Minnesota Health University of Minnesota Medical Center University of Minnesota Masonic Children s Hospital May 2017 Printed herein are
Diagnosis: Presenting signs and Symptoms include:
 PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
International Journal of Research and Review E-ISSN: ; P-ISSN:
 International Journal of Research and Review www.ijrrjournal.com E-ISSN: 2349-9788; P-ISSN: 2454-2237 Original Research Article Comparative Evaluation of Fourth Generation Fluoroquinolones with Fortified
International Journal of Research and Review www.ijrrjournal.com E-ISSN: 2349-9788; P-ISSN: 2454-2237 Original Research Article Comparative Evaluation of Fourth Generation Fluoroquinolones with Fortified
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Package leaflet: Information for the user. GENTAMICIN VISION 3 mg/ml eye drops, solution Gentamicin
 Package leaflet: Information for the user GENTAMICIN VISION 3 mg/ml eye drops, solution Gentamicin Read all of this leaflet carefully before you start taking this medicine because it contains important
Package leaflet: Information for the user GENTAMICIN VISION 3 mg/ml eye drops, solution Gentamicin Read all of this leaflet carefully before you start taking this medicine because it contains important
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Copyright 2012 Diabetes In Control, Inc. For permission to reprint, please contact Heather Moran, Production Editor, at
 Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
MICRO-ORGANISMS by COMPANY PROFILE
 MICRO-ORGANISMS by COMPANY PROFILE 2017 1 SAPROPHYTES AND PATHOGENES SAPROPHYTES Not dangerous PATHOGENES Inducing diseases Have to be eradicated WHERE ARE THERE? EVERYWHERE COMPANY PROFILE 2017 3 MICROORGANISMS
MICRO-ORGANISMS by COMPANY PROFILE 2017 1 SAPROPHYTES AND PATHOGENES SAPROPHYTES Not dangerous PATHOGENES Inducing diseases Have to be eradicated WHERE ARE THERE? EVERYWHERE COMPANY PROFILE 2017 3 MICROORGANISMS