Infectious keratitis for the general ophthalmologist
|
|
|
- Alicia Sullivan
- 5 years ago
- Views:
Transcription




1 Infectious keratitis for the general ophthalmologist Presented by Chameen Samarawickrama - Westmead Hospital - Liverpool Hospital - University of Sydney - University of New South Wales The University of Sydney Page 1
2 Financial disclosures Early Career Research Fellowship (Westmead Charitable Trust) Acknowledgment Inspiration for this lecture is from education provided by: Mr. Steve Tuft Mr. John Dart The University of Sydney Page 2
3 Microbial keratitis Common cause of visual morbidity Management requires appropriate treatments in an appropriate time frame Regional and temporal changes in pathogens The University of Sydney Page 3
4 Key questions 1. What organisms occur? 2. What are the risk factors? 3. How do I diagnose it? 4. What treatments should I give? 5. Who should get steroids? 6. What can go wrong? The University of Sydney Page 4
5 1. Which organisms BACTERIA PROTISTS FUNGI Gram +ve, Gram ve, acid fast Acanthamoeba Yeast, mould, Microsporidia Modified by local risk factors that can vary with time Resulting in geographic and temporal changes SURVEILLANCE FOR EMERGING PATHOGENS The University of Sydney Page 5

6 Geographic variations (Gram +ve) 49% 83% 41% 62% 36% 68% 54% 71% 71% Shah. BJO. 2011;95: The University of Sydney Page 6
7 What about Australia and New Zealand (Gram +ve) 20% (2016) 51% (2008) 76% (2005) 51% (1996) 66% (2005) 72% (2003) 75% (2015) The University of Sydney Page 7
8 What about Australia and New Zealand (Fungi) 12% (2016) 9% (2008) 4% (2005) 0% (1996) 5% (2005) 9% (2003) 2% (2015) The University of Sydney Page 8
9 Organisms can even change by season Green. Cornea. 2008;27:33-9 The University of Sydney Page 9
10 2. Risk factors vary by region Risk factors for MK (2001-3) TRAUMA 36% CONTACT LENS 34% OTHER/UNKNOWN 10% OSD/SYSTEMIC 7% HSV 7% MULTIFACTORIAL 6% 0% 5% 10% 15% 20% 25% 30% 35% 40% Keay. Ophthalmol. 2006;113: The University of Sydney Page 10
11 Risk factors vary over time Green. Cornea. 2008;27:33-9 The University of Sydney Page 11
12 Contact lens wear is an increasing risk factor strong association with Gram ve isolates Causative organisms in culture proven CL related MK * P. aeruginosa Serratia spp. Other Gram -ve spp. Staphlococcus spp. Nocardia spp. Reasonable Streptococcus to spp. assume Other Gram +ve spp keratitis Acanthamoeba in Fungi contact lens wearer is Pseudomonas aeruginosa until proven otherwise Stapleton. AJO. 2007;144: The University of Sydney Page 12




13 Contact lens wear new pathogens Microsporidia The University of Sydney Page 13



14 Contact lens wear new pathogens Fusarium The University of Sydney Page 14



15 Contact lens wear new pathogens Acanthamoeba The University of Sydney Page 15




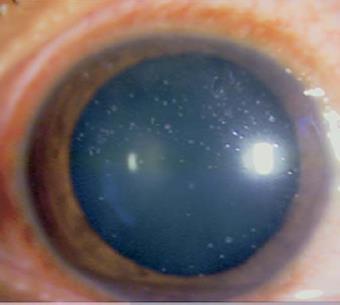
16 3. Features of a microbial keratitis is unreliable Gram +ve Fungi Gram -ve The University of Sydney Page 16 AK


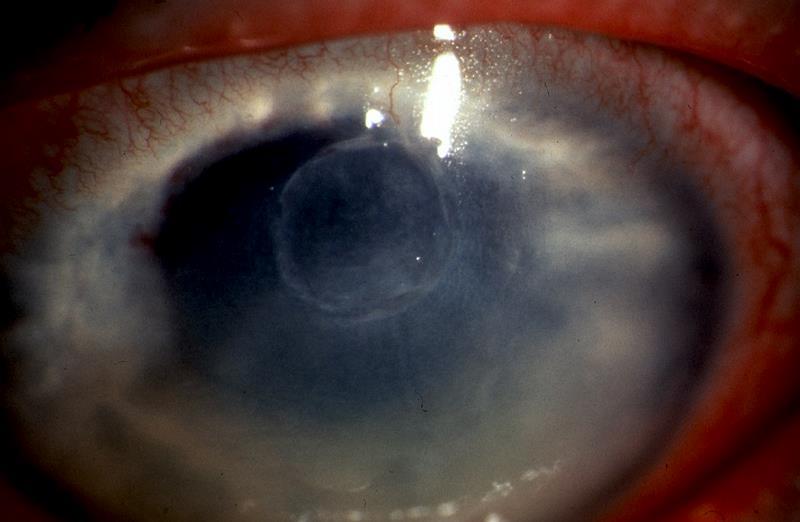
17 Appearance modified by steroids Crystalline keratopathy The University of Sydney Page 17
18 Have to rely on clinical suspicion Organism Risks Onset Bacteria CLs, OSD, surgery Acute (1-2 days) Fungi Trauma, CLs, immunosuppression Variable Protozoa CLs, trauma Subacute (1-7 days) HSV Atopy, steroids Subacute (1-7 days) 1:20 cases are non-bacterial Investigation is mandatory for unresponsive cases The University of Sydney Page 18 Stapleton. Ophthalmol. 2008;115:



19 Basic investigations 2x glass slides Blood agar Chocolate blood agar Saboraud agar Thioglycolate broth Viral swab (for PCR) Suspicion of acanthamoeba Non-nutrient agar Acanthamoeba PCR HSV serology Negative IgG or rising IgM helpful Samarawickrama. BJO Open Ophthalmol. 2017;1:e00044 The University of Sydney Page 19



20 Ancillary tests confocal microscopy Operator dependent 50% sensitivity 65-82% specificity High repeatability Do not rely on confocal for diagnosis if the response to treatment is poor The University of Sydney Page 20 Hau et al. BJO. 2010;94:

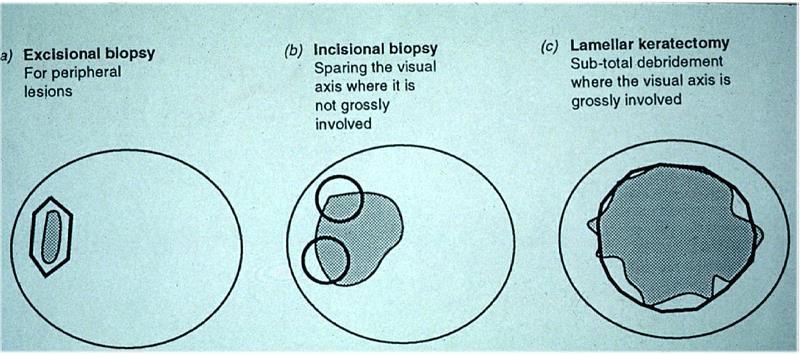
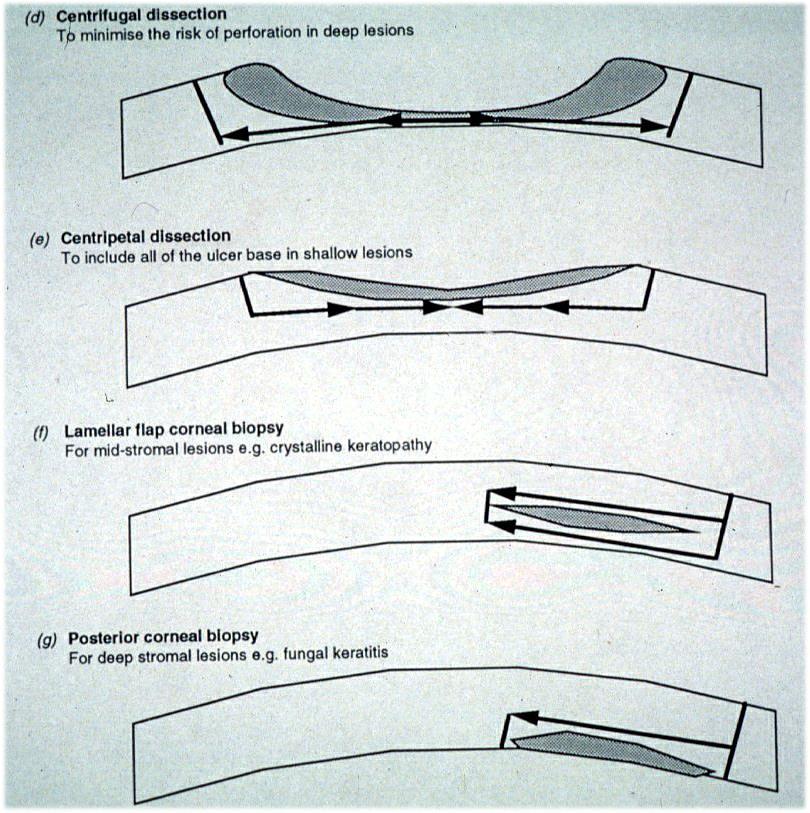
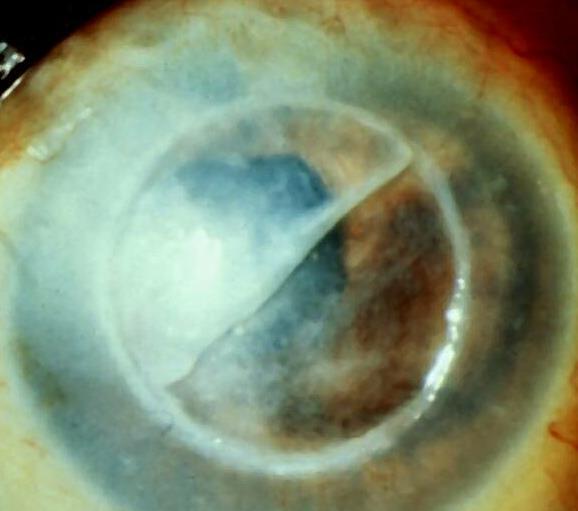
21 Debridement acanthamoeba and fungi biopsy and culture Reduces pathogen load Enhances penetration Especially antifungals Can be curative for acanthamoeba if performed within the first 3 weeks Significant only if positive Bacon. Ophthalmol. 1993;100: Brooks. Cornea. 1994;13:186-9 The University of Sydney Page 21

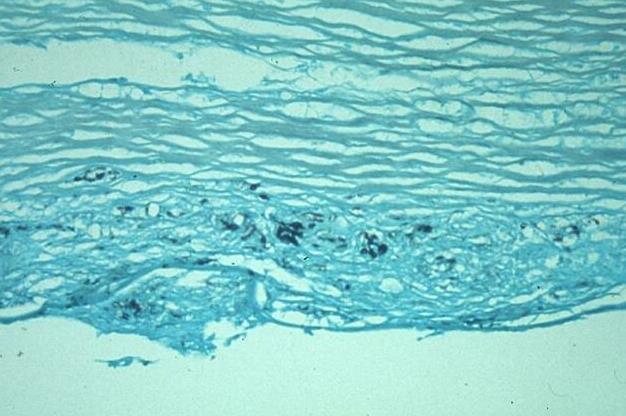
 Gomori silver stain (fungi) The")
22 Histology corneal biopsy or excisional keratoplasty Confirms the diagnosis Viability uncertain Acanthamoeba cysts (H&E; modified Gomori) Gomori silver stain (fungi) The University of Sydney Page 22

23 4. Treatment aims 1. Eliminate infection 2. Control inflammation 3. Control pain 4. Avoid toxicity 5. Identify complications 6. Restore vision The University of Sydney Page 23



24 Sterilization and healing Microbial keratitis Investigation Sterilization Damage limitation Healing The University of Sydney Page 24

25 Management strategies for keratitis Use algorithms and lists To consider all causes Aid in rational planning of diagnosis and treatments The University of Sydney Page 25
26 When to treat without investigation The 95% typical bacterial keratitis Small infiltrate (<1mm) Sudden onset Typical risk factors (CL, trauma, OSD) When NOT to treat without investigation (culture and ideally PCR and confocal) The 5% atypical cases (fungi, acanthamoeba & others) CL/trauma/OSD cases with specific risk factors No identifiable risk factors Those which don t fit clinically with bacterial disease The University of Sydney Page 26
27 Empirical Treatments Based on probability for common organisms in your area (90% bacterial) Highlights importance of ongoing microbial surveillance Initial therapy for BACTERIAL keratitis Unless strong alternative evidence Modulated by risk factors on a case by case basis Treat precipitating causes (eg. exposure, trichiasis etc) Treat ALL cases as PROVISIONAL DIAGNOSIS The University of Sydney Page 27
28 What empirical antibiotic to use Monotherapy (commercially available, stable for 30days fluoroquinolone) vs Dual Therapy (home made, fortified, 7 day unstable aminoglycoside-cephalosporin) What s the evidence? 16 high quality trials involving 1823 patients 4 RCTs comparing ofloxacin to gentamicin-cefazolin involving 440 patients Constantinou. Ophthalmol. 2007;114: Panda. Eye. 1999;13:744-7 Pavesio. Ophthalmol. 1997;104: O Brien. Arch Ophthalmol. 1995;113: meta-analysis McDonald. BJO. 2014;98: The University of Sydney Page 28
29 Ofloxacin vs Gentamicin-Cefazolin No difference in treatment success (RR 0.94: 95% CI 0.68 to 1.30) no difference when fluoroquinolones as a class compared to aminoglycoside-cephalosporins; 10 trials with 1265 patients (RR 1.01: 95% CI 0.94 to 1.08) The University of Sydney Page 29 McDonald. BJO. 2014;98:1470-7
30 Ofloxacin vs Gentamicin-Cefazolin No difference in treatment success (RR 0.94: 95% CI 0.68 to 1.30) no difference when fluoroquinolones as a class compared to aminoglycoside-cephalosporins; 10 trials with 1265 patients (RR 1.01: 95% CI 0.94 to 1.08) No difference in time to cure (MD 3.57: 95% CI to 11.37) no difference when fluoroquinolones as a class compared to aminoglycoside-cephalosporins; 4 trials with 259 patients (MD 2.09: 95% CI to 5.44) No difference in serious complications Corneal perforation Therapeutic keratoplasty Enucleation The University of Sydney Page 30 McDonald. BJO. 2014;98:1470-7

31 Ofloxacin vs Gentamicin-Cefazolin Ofloxacin reduced risk of ocular discomfort by 78% with NNT of patients, RR 0.22: 95% CI 0.13 to 0.39 Fluoroquinolones as a class reduced the risk of ocular discomfort by 68% with NNT of 6 3 trials, 693 patients, RR 0.32: 95% CI 0.22 to 0.47 Ofloxacin reduced risk of chemical conjunctivitis by 80% with NNT of patients, RR 0.20: 95% CI 0.10 to 0.41 Ciprofloxacin has a 24 fold increased risk of white precipitates, rarely seen in ofloxacin The University of Sydney Page 31 McDonald. BJO. 2014;98:1470-7
32 Resistance to fluoroquinolones? Green. Cornea. 2008;27:33-9 The University of Sydney Page 32

33 Clear winner Investigate ALL cases where infection is not improving after 5 days Hourly D/N Hourly by day 2 hourly by day QID days The University of Sydney Page 33

34 Herxheimer effect Acute inflammatory response due to death of microbe with appropriate antimicrobial treatments Reaction to endotoxin-like products Common in Gram negative bacterial keratitis and acanthamoeba keratitis Can look worse, but patient feels better! The University of Sydney Page 34
35 5. Steroids for bacterial keratitis (3 month results) 500 culture positive BACTERIAL cases Exclusions: fungus, acanthamoeba, HSV, impending perforation, previous PK Moxifloxacin q1h for 48hrs prior to randomization, then tapered Prednisolone 1% QID for 7d, BD for 7d, then daily for 7 days (3 weeks total) BSCVA at 3 months Scar Re-epithelialization Perforation IOP P=0.82 P=0.4 P=0.44 P>0.99 Higher in placebo (p=0.04) Subgroup analysis suggests benefit of steroids for severe central ulcers Baseline BSCVA (CF or worse) Location (central 4mm) P=0.03 P=0.04 The University of Sydney Page 35 SCUT. Arch Ophthalmol. 2012;130:143-50
36 Steroids for bacterial keratitis (12 month results) BSCVA at 12 months Scar Entire cohort results P=0.39 P=0.69 Subgroup analysis: Nocardia vs Non-nocardia keratitis BSCVA at 12 months Nocardia infections P=0.10 Non-Nocardia infections P=0.02 (mean 1 line improvement) Scar Nocardia infections P=0.02 (larger scar) Non-Nocardia infections P= line benefit of steroids for non-nocardia microbial keratitis SCUT 2. AJO. 2014;157: The University of Sydney Page 36
37 6. When things don t work to plan If clinically not improving after 5 days, re-evaluate your treatment paradigm and INVESTIGATE FURTHER Poor compliance Uncommon organism Reassess microbiology Unrepresentative culture Polymicrobial infection (10%) Culture negative Treatment toxicity (aminoglycosides) Persistent inflammation Failure to heal Consult your algorithm for progression Do NOT sit on these patients The University of Sydney Page 37
38 CULTURE - CULTURE, PCR or CONFOCAL + Treated before or inadequate treatment Consider other possible causes Adequate treatment for likely causes CONFOCAL PCR RECULTURE after hours off therapy BIOPSY PERFORATION Inadequate treatment Treatment toxicity Persistent inflammation Intensive treatment Reduce toxicity No preservatives or aminoglycosides Treat host response Trial of steroids Debride RESOLUTION Infection uncontrolled Glue Infection controlled Unrepresentative culture Failure to heal Correct precipitating factors EYE LOST Therapeutic/ tectonic penetrating transplant RESOLUTION The University of Sydney Page 38
39 The University of Sydney Page 39 Allan. BJO. 1995;79:777-86



40 Special cases Mycobacteria Acid fast aerobic bacteria Lowenstein-Jensen medium Microsporidia Unicellular, obligate intracellular fungi Stains (Gram, Giemsa, acid fast) Nocardia Gram + rods (bacteria) with acid fast branching filaments Strict aerobes Blood, chocolate blood, Saboraud Propionibacterium acnes Gram + anaerobic rod Capnocytophaga Gram anaerobic rod Chocolate blood agar in increased CO 2 The University of Sydney Page 40
41 Fungal keratitis Superficial infection 1. Natamycin 5% 2. Debride lesion If no response in 7 days 3. Add Chlorhexidine 0.2% Diagnosis Empirical therapy Deep stromal infection/endophthalmitis 1. Natamycin 5% and Chlorhexidine 0.2% 2. Oral Voriconazole* If no response in 7 days Alternatives: Voriconazole 1% Amphotericin 0.15% Culture results Yeast (min 1 month) 1. Amphotericin 0.15% 2. Voriconazole 1% 3. Chlorhexidine 0.2% Filamentary (3 months) 1. Natamycin 5% 2. Chlorhexidine 0.2% 3. Intralesional Voriconazole 4. Intracameral Voriconazole 5. Excisional/therapeutic keratoplasty MUTT1. JAMA Ophthalmol. 2013;131:422-9 MUTT2. JAMA Ophthalmol. 2016;134: FlorCruz. Cochrane Database. 2015;4:CD The University of Sydney Page 41
 12.5µg in 0.05ml 7. Use topical antifungals for months 8.")
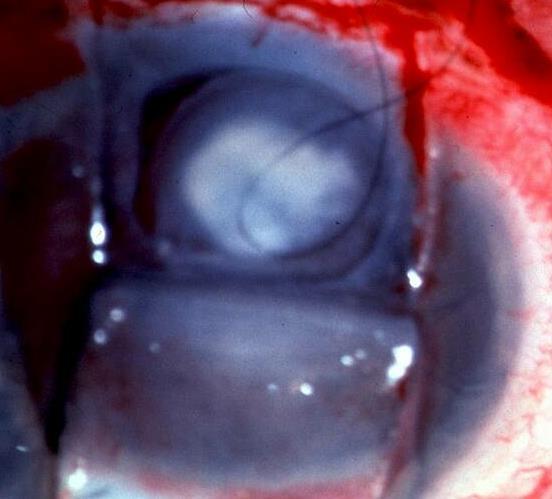
42 Excisional keratoplasty Early surgical intervention (2-3 weeks) in deteriorating cases or extension into anterior chamber or sclera 1. 2mm clearance 2. Remove iris and lens as required 3. Peripheral iridectomy 4. Voriconazole µg in 0.1ml 5. Interupted sutures 6. Intracameral tissue plasminogen activator (tpa) 12.5µg in 0.05ml 7. Use topical antifungals for months 8. Use cyclosporin A (antifungal and anti-inflammatory) 9. IV amphotericin in bad cases 10. No topical steroids for 4-8 weeks or longer Failure rate for first grafts are about 20-30% The University of Sydney Page 42
43 Steroids for fungal keratitis Steroids exacerbate growth of fungus DO NOT use for filamentary fungus Can use carefully for Candida (after 2-4 weeks) if infiltrate improving but cornea vascularizing The University of Sydney Page 43
44 Acanthamoeba keratitis Choice based on in vitro cysticidal data MARKED superiority of biguanides 82 respondents from Cornea Society USA Biguanide with diamidines most widely used combination therapy In vitro evidence that Timolol Sandoz 0.5%: Damages acanthamoeba on a mitochodrial level Potentially encourages excystation Drug (cidal conc µg/ml) Biguanides Polyhexanide (PHMB) Troph The University of Sydney Page 44 Cyst Chlorhex Diamidines Propamidine (Brolene) Haxamidine Kilvington. IOVS. 2004;45:165-9 Oldenburg. Cornea. 2011;30: Sifaoui. Exp Parasitol. 2017;183:117-23
45 Acanthamoeba treatment paradigm PHMB + Brolene Q1h day and night for 48 hours Q1h by day for 5-7 days Then reduce to 6x/day Taper to QID as disease is brought under control Drug toxicity is common with diamidines but NOT PHMB Stop brolene first Timolol 0.5% BD for entirety of treatment When have you won: 1 month off ALL treatment (including steroids) without any signs of inflammation The University of Sydney Page 45
 Continue biguanides for")
 Persistent inflammation does not always equate to viable organisms The University of Sydney")
46 Control inflammation Topical Steroids In cases of: Increasing inflammation Vascularization Melt Defer for 2 weeks after initiation of treatment Only use with biguanides (PHMB or chlorhexidine) Continue biguanides for 4 weeks after steroids discontinued Worsening pain or scleritis Oral NSAIDS Oral steroids Immunosuppression (cyclosporin) Persistent inflammation does not always equate to viable organisms The University of Sydney Page 46
47 Summary Know the common organisms in your area Know the risk factors Know the presenting features Use a management algorithm to aid rational planning of diagnoisis and treatments Fluoroquinolone monotherapy is effective for the majority of bacterial keratitis Remember 1 in 20 are fungal or amoeba High index of suspicion 10% are polymicrobial Investigate ALL cases of presumed bacterial keratitis not improving after 5 days The University of Sydney Page 47
48 References 1. Shah. BJO. 2011;95: Leck. BJO. 2002;86: Samarawickrama. Health Infect. 2015;20: Butler. BJO. 2005;89: Green. Cornea. 2008;27: Gebauer. Eye. 1996;10: Richards. CEO. 2016;44: Leibovitch. EJO. 2005;15: Wong. BJO. 2003;87: Keay. Ophthalmol. 2006;113: Stapleton. AJO. 2007;144: Stapleton. Eye & CL. 2013;39: Tran. CEO. 2014;42: Stapleton. Ophthalmol. 2008;115: Samarawickrama. BJO Open Ophthalmol. 2017;1:e Hau et al. BJO. 2010;94: Bacon. Ophthalmol. 1993;100: Brooks. Cornea. 1994;13: Constantinou. Ophthalmol. 2007;114: Panda. Eye. 1999;13: Pavesio. Ophthalmol. 1997;104: O Brien. Arch Ophthalmol. 1995;113: McDonald. BJO. 2014;98: SCUT. Arch Ophthalmol. 2012;130: SCUT 2. AJO. 2014;157: SCUT Nocardia. AJO. 2012;154: Allan. BJO. 1995;79: MUTT1. JAMA Ophthalmol. 2013;131: MUTT2. JAMA Ophthalmol. 2016;134: FlorCruz. Cochrane Database. 2015;4:CD Kilvington. IOVS. 2004;45: Oldenburg. Cornea. 2011;30: Sifaoui. Exp Parasitol. 2017;183: The University of Sydney Page 48
Clinical Features, Antibiotic Susceptibility Profile, and Outcomes of Infectious Keratitis Caused by Stenotrophomonas maltophilia
 Clinical Features, Antibiotic Susceptibility Profile, and Outcomes of Infectious Keratitis Caused by Stenotrophomonas maltophilia Sotiria Palioura, MD, MSc, PhD Cornea & External Disease Specialist Athens
Clinical Features, Antibiotic Susceptibility Profile, and Outcomes of Infectious Keratitis Caused by Stenotrophomonas maltophilia Sotiria Palioura, MD, MSc, PhD Cornea & External Disease Specialist Athens
Disclosure. Update on management of fungal keratitis. Acknowledgments. World Blindness 1993
 Update on management of fungal keratitis Tom Lietman, MD F I Proctor Foundation Department of Ophthalmology University of California San Francisco Disclosure Voriconazole donated by Pfizer Natamycin and
Update on management of fungal keratitis Tom Lietman, MD F I Proctor Foundation Department of Ophthalmology University of California San Francisco Disclosure Voriconazole donated by Pfizer Natamycin and
Study of Bacteriological Profile of Corneal Ulcers in Patients Attending VIMS, Ballari, India
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 7 (2016) pp. 200-205 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.507.020
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 7 (2016) pp. 200-205 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.507.020
Role of Moxifloxacin in Bacterial Keratitis
 Original Article Role of Moxifloxacin in Bacterial Keratitis Aamna Jabran, Aurengzeb Sheikh, Syed Ali Haider, Zia-ud-din Shaikh Pak J Ophthalmol 29, Vol. 25 No. 2.................................................................................
Original Article Role of Moxifloxacin in Bacterial Keratitis Aamna Jabran, Aurengzeb Sheikh, Syed Ali Haider, Zia-ud-din Shaikh Pak J Ophthalmol 29, Vol. 25 No. 2.................................................................................
CLINICAL DECISION MAKING IN MICROBIAL KERATITIS. Gregory M. Schultz, O.D.,F.A.A.O. Eye Center of Virginia Williamsburg and Gloucester Virginia
 CLINICAL DECISION MAKING IN MICROBIAL KERATITIS Gregory M. Schultz, O.D.,F.A.A.O. Eye Center of Virginia Williamsburg and Gloucester Virginia : GOALS OF THIS COURSE: QUESTIONS WE WILL ANSWER Do I have
CLINICAL DECISION MAKING IN MICROBIAL KERATITIS Gregory M. Schultz, O.D.,F.A.A.O. Eye Center of Virginia Williamsburg and Gloucester Virginia : GOALS OF THIS COURSE: QUESTIONS WE WILL ANSWER Do I have
A 3½-Year Study of Bacterial Keratitis From Odisha, India
 ORIGINAL CLINICAL STUDY A 3½-Year Study of Bacterial Keratitis From Odisha, India Bibhudutta Rautaraya, MD,* Savitri Sharma, MD,* Md. Hasnat Ali, MBA,Þ Sarita Kar, MSc,* Sujata Das, MS, FRCS(Glasg),* and
ORIGINAL CLINICAL STUDY A 3½-Year Study of Bacterial Keratitis From Odisha, India Bibhudutta Rautaraya, MD,* Savitri Sharma, MD,* Md. Hasnat Ali, MBA,Þ Sarita Kar, MSc,* Sujata Das, MS, FRCS(Glasg),* and
Downloaded from
 Guidelines for the Management of Suspected Microbial Keratitis in Settings with Limited Laboratory Facilities Wani MG, Consultant Ophthalmologist, Sakubva Eye Unit, Mutare Zimbabwe a Introduction Microbial
Guidelines for the Management of Suspected Microbial Keratitis in Settings with Limited Laboratory Facilities Wani MG, Consultant Ophthalmologist, Sakubva Eye Unit, Mutare Zimbabwe a Introduction Microbial
Debate Series editors: Susan Lightman and Peter McCluskey
 1167... Series editors: Susan Lightman and Peter McCluskey Correspondence to: M Daniell, Royal Victorian Eye and Ear Hospital, Melbourne, Victoria, 3065, Australia; daniellm@ozemail.com.au Accepted for
1167... Series editors: Susan Lightman and Peter McCluskey Correspondence to: M Daniell, Royal Victorian Eye and Ear Hospital, Melbourne, Victoria, 3065, Australia; daniellm@ozemail.com.au Accepted for
Fluoroquinolone and fortified antibiotics for treating bacterial corneal ulcers
 378 Centre for Eye Research Australia, The University of Melbourne, 32 Gisborne Street, East Melbourne, Victoria 3002, Australia N Gangopadhyay M Daniell L Weih H R Taylor Correspondence to: Dr Mark Daniell
378 Centre for Eye Research Australia, The University of Melbourne, 32 Gisborne Street, East Melbourne, Victoria 3002, Australia N Gangopadhyay M Daniell L Weih H R Taylor Correspondence to: Dr Mark Daniell
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Financial disclosures
 Financial disclosures Named co-inventor on PCT applications CH2012/0000090 and PCT2014/CH000075 Chief Scientific Officer EMAGine SA Historical decision in 2004 1. Future: extremely thin corneas Dresden
Financial disclosures Named co-inventor on PCT applications CH2012/0000090 and PCT2014/CH000075 Chief Scientific Officer EMAGine SA Historical decision in 2004 1. Future: extremely thin corneas Dresden
Bacterial Keratitis Should optometrists treat in the community?
 Case Record 13 Bacterial Keratitis Should optometrists treat in the community? December 2008 Dr Peter Frampton DOptom MSc FCOptom BAppSc(Optom)(AUS) DipTp(AS) DipTp(SP) DipTp(IP) Introduction Can Optometrists
Case Record 13 Bacterial Keratitis Should optometrists treat in the community? December 2008 Dr Peter Frampton DOptom MSc FCOptom BAppSc(Optom)(AUS) DipTp(AS) DipTp(SP) DipTp(IP) Introduction Can Optometrists
Evaluation of Moxifloxacin 0.5% Eye Drops in Treatment of Bacterial Corneal Ulcers
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. II (Nov. 2017), PP 15-19 www.iosrjournals.org Evaluation of Moxifloxacin 0.5% Eye Drops
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. II (Nov. 2017), PP 15-19 www.iosrjournals.org Evaluation of Moxifloxacin 0.5% Eye Drops
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Pathogens and Antibiotic Sensitivities in Post- Phacoemulsification Endophthalmitis, Kaiser Permanente, California,
 Pathogens and Antibiotic Sensitivities in Post- Phacoemulsification Endophthalmitis, Kaiser Permanente, California, 2007-2012 Geraldine R. Slean, MD, MS 1 ; Neal H. Shorstein, MD 2 ; Liyan Liu, MD, MS
Pathogens and Antibiotic Sensitivities in Post- Phacoemulsification Endophthalmitis, Kaiser Permanente, California, 2007-2012 Geraldine R. Slean, MD, MS 1 ; Neal H. Shorstein, MD 2 ; Liyan Liu, MD, MS
REVIEW OF OPHTHALMOLOGY SECTION OF WHO MODEL LIST OF ESSENTIAL MEDICINES. Sight Savers International and The Vision 2020 Technology Group
 REVIEW OF OPHTHALMOLOGY SECTION OF WHO MODEL LIST OF ESSENTIAL MEDICINES Anti infective agent Medicine suggested for inclusion Ciprofloxacin: 0.3 % eye drops Application submitted by Sight Savers International
REVIEW OF OPHTHALMOLOGY SECTION OF WHO MODEL LIST OF ESSENTIAL MEDICINES Anti infective agent Medicine suggested for inclusion Ciprofloxacin: 0.3 % eye drops Application submitted by Sight Savers International
Burn Infection & Laboratory Diagnosis
 Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Strategies for the management of microbial keratitis
 British J7ournal of Ophthalmology 1995; 79: 777-786 777 PERSPECTIVE Strategies for the management of microbial keratitis Bruce D S Allan, John K G Dart Microbial keratitis results from a complex interaction
British J7ournal of Ophthalmology 1995; 79: 777-786 777 PERSPECTIVE Strategies for the management of microbial keratitis Bruce D S Allan, John K G Dart Microbial keratitis results from a complex interaction
Topical Antibiotic Update. Brad Sutton, O.D., F.A.A.O. Indiana University School of Optometry Indianapolis Eye Care Center No financial disclosures
 Topical Antibiotic Update Brad Sutton, O.D., F.A.A.O. Indiana University School of Optometry Indianapolis Eye Care Center No financial disclosures What do we have? We currently have many highly effective
Topical Antibiotic Update Brad Sutton, O.D., F.A.A.O. Indiana University School of Optometry Indianapolis Eye Care Center No financial disclosures What do we have? We currently have many highly effective
The CARI Guidelines Caring for Australians with Renal Impairment. 10. Treatment of peritoneal dialysis associated fungal peritonitis
 10. Treatment of peritoneal dialysis associated fungal peritonitis Date written: February 2003 Final submission: July 2004 Guidelines (Include recommendations based on level I or II evidence) The use of
10. Treatment of peritoneal dialysis associated fungal peritonitis Date written: February 2003 Final submission: July 2004 Guidelines (Include recommendations based on level I or II evidence) The use of
Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis
 Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis Steve SM Wong Alice Ho Miu Ling Nethersole Hospital Background PD peritonitis is a major cause of PD
Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis Steve SM Wong Alice Ho Miu Ling Nethersole Hospital Background PD peritonitis is a major cause of PD
Delayed-Onset Post-Keratoplasty Endophthalmitis Caused by Vancomycin-Resistant Enterococcus faecium
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Inhibiting Microbial Growth in vivo. CLS 212: Medical Microbiology Zeina Alkudmani
 Inhibiting Microbial Growth in vivo CLS 212: Medical Microbiology Zeina Alkudmani Chemotherapy Definitions The use of any chemical (drug) to treat any disease or condition. Chemotherapeutic Agent Any drug
Inhibiting Microbial Growth in vivo CLS 212: Medical Microbiology Zeina Alkudmani Chemotherapy Definitions The use of any chemical (drug) to treat any disease or condition. Chemotherapeutic Agent Any drug
Bacterial Keratitis Preferred Practice Pattern
 Bacterial Keratitis Preferred Practice Pattern 2018 by the American Academy of Ophthalmology Published by Elsevier Inc. https://doi.org/10.1016/j.ophtha.2018.10.018 ISSN 0161-6420/18 Secretary for Quality
Bacterial Keratitis Preferred Practice Pattern 2018 by the American Academy of Ophthalmology Published by Elsevier Inc. https://doi.org/10.1016/j.ophtha.2018.10.018 ISSN 0161-6420/18 Secretary for Quality
Eradiaction of Resistant Organisms:
 Eradiaction of Resistant Organisms: Can we do it and does it help? Noah Lechtzin, MD; MHS Director, Adult CF Program Outline Evidence resistant organisms are bad MRSA, B cepacia, Pseudomonas, Fungal infections
Eradiaction of Resistant Organisms: Can we do it and does it help? Noah Lechtzin, MD; MHS Director, Adult CF Program Outline Evidence resistant organisms are bad MRSA, B cepacia, Pseudomonas, Fungal infections
Clinical Study Microbial Keratitis Profile at a University Hospital in Hong Kong
 International Scholarly Research Notices, Article ID 689742, 4 pages http://dx.doi.org/10.1155/2014/689742 Clinical Study Microbial Keratitis Profile at a University Hospital in Hong Kong Tracy H. T. Lai,
International Scholarly Research Notices, Article ID 689742, 4 pages http://dx.doi.org/10.1155/2014/689742 Clinical Study Microbial Keratitis Profile at a University Hospital in Hong Kong Tracy H. T. Lai,
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
In vitro antibiotic resistance in bacterial keratitis in London
 Br J Ophthalmol 2000;84:687 691 687 Moorfields Eye Hospital, London EC1V 2PD SJTuft Institute of Ophthalmology, London EC1V 9QS M Matheson Correspondence to: Mr S J Tuft, Moorfields Eye Hospital, City
Br J Ophthalmol 2000;84:687 691 687 Moorfields Eye Hospital, London EC1V 2PD SJTuft Institute of Ophthalmology, London EC1V 9QS M Matheson Correspondence to: Mr S J Tuft, Moorfields Eye Hospital, City
Research Article Spectrum and Sensitivity of Bacterial Keratitis Isolates in Auckland
 Ophthalmology Volume 2016, Article ID 3769341, 8 pages http://dx.doi.org/10.1155/2016/3769341 Research Article Spectrum and Sensitivity of Bacterial Keratitis Isolates in Auckland S. Marasini, 1 S. Swift,
Ophthalmology Volume 2016, Article ID 3769341, 8 pages http://dx.doi.org/10.1155/2016/3769341 Research Article Spectrum and Sensitivity of Bacterial Keratitis Isolates in Auckland S. Marasini, 1 S. Swift,
Redefining Infection Management. Proven Clinical Outcomes
 Proven Clinical Outcomes Proof of Bacteria-Binding1 In the first 30 seconds, 1 square centimeter of Cutimed Sorbact binds wound bacteria - after 2 hours, the amount of bacteria bound are more than would
Proven Clinical Outcomes Proof of Bacteria-Binding1 In the first 30 seconds, 1 square centimeter of Cutimed Sorbact binds wound bacteria - after 2 hours, the amount of bacteria bound are more than would
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS
 Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Treatment of septic peritonitis
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
The Inpatient Management of Febrile Neutropenia
 UCSF Medical Center Adult Blood and Marrow Transplant Program 400 Parnassus Avenue, San Francisco, CA 94143 SOP # CL 120.05 The Inpatient Management of Febrile Neutropenia BACKGROUND: Neutropenia results
UCSF Medical Center Adult Blood and Marrow Transplant Program 400 Parnassus Avenue, San Francisco, CA 94143 SOP # CL 120.05 The Inpatient Management of Febrile Neutropenia BACKGROUND: Neutropenia results
Antibiotic therapy of acute gastroenteritis
 Antibiotic therapy of acute gastroenteritis Potential goals Clinical improvement (vs control) Fecal eradication of the pathogen and decrease infectivity Prevent complications Acute gastroenteritis viruses
Antibiotic therapy of acute gastroenteritis Potential goals Clinical improvement (vs control) Fecal eradication of the pathogen and decrease infectivity Prevent complications Acute gastroenteritis viruses
مادة االدوية المرحلة الثالثة م. غدير حاتم محمد
 م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Class Update with New Drug Evaluation: Ototopical Antibiotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
CLINICAL PROTOCOL FOR COMMUNITY ACQUIRED PNEUMONIA. SCOPE: Western Australia. CORB score equal or above 1. All criteria must be met:
 CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
PACK-CXL. for infectious keratitis. Farhad Hafezi, MD PhD. Professor of Ophthalmology Keck School of Medicine USC Los Angeles, USA
 PACK-CXL for infectious keratitis Farhad Hafezi, MD PhD Professor of Ophthalmology University of Geneva Geneva, Switzerland Medical Director ELZA Institute Zurich, Switzerland Research Group Leader Lab.
PACK-CXL for infectious keratitis Farhad Hafezi, MD PhD Professor of Ophthalmology University of Geneva Geneva, Switzerland Medical Director ELZA Institute Zurich, Switzerland Research Group Leader Lab.
Proceedings of the 13th International Congress of the World Equine Veterinary Association WEVA
 www.ivis.org Proceedings of the 13th International Congress of the World Equine Veterinary Association WEVA October 3-5, 2013 Budapest, Hungary Reprinted in IVIS with the Permission of the WEVA Organizers
www.ivis.org Proceedings of the 13th International Congress of the World Equine Veterinary Association WEVA October 3-5, 2013 Budapest, Hungary Reprinted in IVIS with the Permission of the WEVA Organizers
Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma
 Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma Lucio Petrizzi DVM DECVS Università degli Studi di Teramo Surgical site infections (SSI) Microbial contamination unavoidable Infection
Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma Lucio Petrizzi DVM DECVS Università degli Studi di Teramo Surgical site infections (SSI) Microbial contamination unavoidable Infection
PRESCRIBING INFORMATION
 PRESCRIBING INFORMATION Pr PENTAMYCETIN Chloramphenicol Ophthalmic Solution USP 0.25%, 0.5% Chloramphenicol Ophthalmic Ointment USP 1% Antibiotic Pr PENTAMYCETIN/HC Chloramphenicol and Hydrocortisone Eye
PRESCRIBING INFORMATION Pr PENTAMYCETIN Chloramphenicol Ophthalmic Solution USP 0.25%, 0.5% Chloramphenicol Ophthalmic Ointment USP 1% Antibiotic Pr PENTAMYCETIN/HC Chloramphenicol and Hydrocortisone Eye
F1 IN THE NAME OF GOD
 F1 IN THE NAME OF GOD Slide 1 F1 FEIKO.IR.SOFT; 2011/07/06 Lid Laceration Conjunctival Hemorrhage a) No therapy is necessary b) Usually resolve in 7-12 days. Subconjunctival Hemorrhage Corneal Abrasion
F1 IN THE NAME OF GOD Slide 1 F1 FEIKO.IR.SOFT; 2011/07/06 Lid Laceration Conjunctival Hemorrhage a) No therapy is necessary b) Usually resolve in 7-12 days. Subconjunctival Hemorrhage Corneal Abrasion
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
SSTI s :A Guideline for Effective Treatment of Skin and Soft Tissue Infections
 SSTI s :A Guideline for Effective Treatment of Skin and Soft Tissue Infections Dr. Javan S. Bass, FACFAS Metro Foot & Ankle Centers, PC Georgia Podiatric Association Board of Directors Disclosures Bako
SSTI s :A Guideline for Effective Treatment of Skin and Soft Tissue Infections Dr. Javan S. Bass, FACFAS Metro Foot & Ankle Centers, PC Georgia Podiatric Association Board of Directors Disclosures Bako
Study of Microbiological Profile and their Antibiogram in Patients with Chronic Suppurative Otitis Media
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 981-985 http://www.ijcmas.com Original Research Article Study of Microbiological Profile
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 981-985 http://www.ijcmas.com Original Research Article Study of Microbiological Profile
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
UCSF Medical Center Guidelines for Inpatient Management of Febrile Neutropenia
 Published on Infectious Diseases Management Program at UCSF (https://idmp.ucsf.edu) Home > UCSF Medical Center Guidelines for Inpatient Management of Febrile Neutropenia UCSF Medical Center Guidelines
Published on Infectious Diseases Management Program at UCSF (https://idmp.ucsf.edu) Home > UCSF Medical Center Guidelines for Inpatient Management of Febrile Neutropenia UCSF Medical Center Guidelines
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Evaluation of Microbiological Profile of Ear Discharge of Patients Attending Otorhinolaryngology
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Evaluation of Microbiological Profile of Ear Discharge of Patients Attending Otorhinolaryngology
Antibiotics in vitro : Which properties do we need to consider for optimizing our therapeutic choice?
 Antibiotics in vitro : Which properties do we need to consider for optimizing our therapeutic choice? With the support of Wallonie-Bruxelles-International 1-1 In vitro evaluation of antibiotics : the antibiogram
Antibiotics in vitro : Which properties do we need to consider for optimizing our therapeutic choice? With the support of Wallonie-Bruxelles-International 1-1 In vitro evaluation of antibiotics : the antibiogram
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland
 Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
CADTH. Rapid Response Report: Peer-Reviewed Summary with Critical Appraisal. Canadian Agency for Drugs and Technologies in Health
 Canadian Agency for Drugs and Technologies in Health Agence canadienne des médicaments et des technologies de la santé Rapid Response Report: Peer-Reviewed Summary with Critical Appraisal CADTH Intracameral
Canadian Agency for Drugs and Technologies in Health Agence canadienne des médicaments et des technologies de la santé Rapid Response Report: Peer-Reviewed Summary with Critical Appraisal CADTH Intracameral
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Surgical Wound Management in Dogs using an Improved Stable Chlorine Dioxide Antiseptic Solution.
 Case Report Surgical Wound Management in Dogs using an Improved Stable Chlorine Dioxide Antiseptic Solution. Chapnick A 1 and Wilkins RJ *2 Journal of Veterinary Science & Animal Husbandry Volume 1 Issue
Case Report Surgical Wound Management in Dogs using an Improved Stable Chlorine Dioxide Antiseptic Solution. Chapnick A 1 and Wilkins RJ *2 Journal of Veterinary Science & Animal Husbandry Volume 1 Issue
Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550
 and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550") Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550 Sinusitis Upper respiratory tract infections (URI) Common cold
Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550 Sinusitis Upper respiratory tract infections (URI) Common cold
Antimicrobial Prophylaxis in the Surgical Patient. M. J. Osgood
 Antimicrobial Prophylaxis in the Surgical Patient M. J. Osgood Outline Definitions surgical site infection (SSI) Risk factors Wound classification Microbiology of SSIs Strategies for prevention of SSIs
Antimicrobial Prophylaxis in the Surgical Patient M. J. Osgood Outline Definitions surgical site infection (SSI) Risk factors Wound classification Microbiology of SSIs Strategies for prevention of SSIs
Bacterial Keratitis Limited Revision
 Bacterial Keratitis Limited Revision Prepared by the American Academy of Ophthalmology Cornea/External Disease Panel Cornea/External Disease Panel Members Robert S. Feder, MD, Chair Steven P. Dunn, MD
Bacterial Keratitis Limited Revision Prepared by the American Academy of Ophthalmology Cornea/External Disease Panel Cornea/External Disease Panel Members Robert S. Feder, MD, Chair Steven P. Dunn, MD
Microbial keratitis is a major cause of corneal opacity and
 Immunology and Microbiology Bacterial Susceptibility to Topical Antimicrobials and Clinical Outcome in Bacterial Keratitis Stephen Kaye, 1 Stephen Tuft, 2 Timothy Neal, 3 Derek Tole, 4 John Leeming, 5
Immunology and Microbiology Bacterial Susceptibility to Topical Antimicrobials and Clinical Outcome in Bacterial Keratitis Stephen Kaye, 1 Stephen Tuft, 2 Timothy Neal, 3 Derek Tole, 4 John Leeming, 5
Parasites Infections Allergy Pemphigus Acne Indolent ulcer Neck ulcers. Flea Allergy Dermatitis Cheyletiella. Contagious demodicosis in a shelter
 Douglas J. DeBoer, D.V.M., Diplomate A.C.V.D. School of Veterinary Medicine University of Wisconsin-Madison Parasites Infections Allergy Pemphigus Acne Indolent ulcer Neck ulcers Flea Allergy Dermatitis
Douglas J. DeBoer, D.V.M., Diplomate A.C.V.D. School of Veterinary Medicine University of Wisconsin-Madison Parasites Infections Allergy Pemphigus Acne Indolent ulcer Neck ulcers Flea Allergy Dermatitis
Diagnosis: Presenting signs and Symptoms include:
 PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Mono- versus Bitherapy for Management of HAP/VAP in the ICU
 Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Copyright 2012 Diabetes In Control, Inc. For permission to reprint, please contact Heather Moran, Production Editor, at
 Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
An Evidence Based Approach to Antibiotic Prophylaxis in Oral Surgery
 An Evidence Based Approach to Antibiotic Prophylaxis in Oral Surgery Nicholas Makhoul DMD. MD. FRCD(C). Dip ABOMS. FACS. Director, Division of Oral and Maxillofacial Surgery Assistant Professor McGill
An Evidence Based Approach to Antibiotic Prophylaxis in Oral Surgery Nicholas Makhoul DMD. MD. FRCD(C). Dip ABOMS. FACS. Director, Division of Oral and Maxillofacial Surgery Assistant Professor McGill
Reduce the risk of recurrence Clear bacterial infections fast and thoroughly
 Reduce the risk of recurrence Clear bacterial infections fast and thoroughly Clearly advanced 140916_Print-Detailer_Englisch_V2_BAH-05-01-14-003_RZ.indd 1 23.09.14 16:59 In bacterial infections, bacteriological
Reduce the risk of recurrence Clear bacterial infections fast and thoroughly Clearly advanced 140916_Print-Detailer_Englisch_V2_BAH-05-01-14-003_RZ.indd 1 23.09.14 16:59 In bacterial infections, bacteriological
Introduction to Chemotherapeutic Agents. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018
 Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Antimicrobial therapy in critical care
 Antimicrobial therapy in critical care KARLEE JOHNSTON LEAD PHARMACIST DIVISION OF CRITICAL CARE CANBERRA HOSPITAL AND HEALTH SERVICE Outline 1. Let s talk about sepsis 2. PK/PD considerations 3. Selecting
Antimicrobial therapy in critical care KARLEE JOHNSTON LEAD PHARMACIST DIVISION OF CRITICAL CARE CANBERRA HOSPITAL AND HEALTH SERVICE Outline 1. Let s talk about sepsis 2. PK/PD considerations 3. Selecting
2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania
 2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania Day 1: Saturday 30 th September 2017 09:00 09:20 Registration
2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania Day 1: Saturday 30 th September 2017 09:00 09:20 Registration
Disclosures! Update on Keratoprosthesis! Penetrating Keratoplasty! Keratoprostheses! 12/3/11
 Disclosures Update on Keratoprosthesis I have no financial interests in any of the techniques or products discussed. Bennie H. Jeng, M.D. Associate Professor of Ophthalmology Department of Ophthalmology
Disclosures Update on Keratoprosthesis I have no financial interests in any of the techniques or products discussed. Bennie H. Jeng, M.D. Associate Professor of Ophthalmology Department of Ophthalmology
Prophylactic antibiotic timing and dosage. Dr. Sanjeev Singh AIMS, Kochi
 Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Anti-infective Studies
 Anti-infective Studies Blast-related Polytraumatic Extremity Wounds and Infectious Outcomes: Trauma Infectious Disease Outcomes Study and Trauma-associated Osteomyelitis Trauma Infectious Disease Outcomes
Anti-infective Studies Blast-related Polytraumatic Extremity Wounds and Infectious Outcomes: Trauma Infectious Disease Outcomes Study and Trauma-associated Osteomyelitis Trauma Infectious Disease Outcomes
Burton's Microbiology for the Health Sciences. Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents
 Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
No-leaching. No-resistance. No-toxicity. >99.999% Introducing BIOGUARD. Best-in-class dressings for your infection control program
 Introducing BIOGUARD No-leaching. >99.999% No-resistance. No-toxicity. Just cost-efficient, broad-spectrum, rapid effectiveness you can rely on. Best-in-class dressings for your infection control program
Introducing BIOGUARD No-leaching. >99.999% No-resistance. No-toxicity. Just cost-efficient, broad-spectrum, rapid effectiveness you can rely on. Best-in-class dressings for your infection control program
International Journal of Research and Review E-ISSN: ; P-ISSN:
 International Journal of Research and Review www.ijrrjournal.com E-ISSN: 2349-9788; P-ISSN: 2454-2237 Original Research Article Comparative Evaluation of Fourth Generation Fluoroquinolones with Fortified
International Journal of Research and Review www.ijrrjournal.com E-ISSN: 2349-9788; P-ISSN: 2454-2237 Original Research Article Comparative Evaluation of Fourth Generation Fluoroquinolones with Fortified
Schedule of Accreditation
 Schedule of Accreditation Organisation Name INAB Reg No Contact Name Address Saolta University Health Care Group Sligo University Hospital Microbiology Department 321MT Anne O'Toole Contact Phone No 071
Schedule of Accreditation Organisation Name INAB Reg No Contact Name Address Saolta University Health Care Group Sligo University Hospital Microbiology Department 321MT Anne O'Toole Contact Phone No 071
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania
 2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania Day 1: Saturday 30 th September 2017 Time Topic/Activity
2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania Day 1: Saturday 30 th September 2017 Time Topic/Activity
TREATMENT OF PERITONEAL DIALYSIS (PD) RELATED PERITONITIS. General Principles
 RELATED PERITONITIS. General Principles") WA HOME DIALYSIS PROGRAM (WAHDIP) GUIDELINES General Principles 1. PD related peritonitis is an EMERGENCY early empiric treatment followed by close review is essential 2. When culture results and sensitivities
WA HOME DIALYSIS PROGRAM (WAHDIP) GUIDELINES General Principles 1. PD related peritonitis is an EMERGENCY early empiric treatment followed by close review is essential 2. When culture results and sensitivities
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
INTRODUCTION TO WILDLIFE PHARMACOLOGY. Lisa Fosco Wildlife Rehabilitation Manager Toronto Wildlife Centre
 INTRODUCTION TO WILDLIFE PHARMACOLOGY Lisa Fosco Wildlife Rehabilitation Manager Toronto Wildlife Centre General Pharmacology Factors That Affect Drug Absorption The dosage form Blood supply to the area
INTRODUCTION TO WILDLIFE PHARMACOLOGY Lisa Fosco Wildlife Rehabilitation Manager Toronto Wildlife Centre General Pharmacology Factors That Affect Drug Absorption The dosage form Blood supply to the area
Role of the nurse in diagnosing infection: The right sample, every time
 BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
Pharm 262: Antibiotics. 1 Pharmaceutical Microbiology II DR. C. AGYARE
 Pharm 262: 1 Pharmaceutical Microbiology II Antibiotics DR. C. AGYARE Reference Books 2 HUGO, W.B., RUSSELL, A.D. Pharmaceutical Microbiology. 6 th Ed. Malden, MA: Blackwell Science, 1998. WALSH, G. Biopharmaceuticals:
Pharm 262: 1 Pharmaceutical Microbiology II Antibiotics DR. C. AGYARE Reference Books 2 HUGO, W.B., RUSSELL, A.D. Pharmaceutical Microbiology. 6 th Ed. Malden, MA: Blackwell Science, 1998. WALSH, G. Biopharmaceuticals:
Himani B. Pandya, Ph.D (medical microbiology) Tutor, S.B.K.S Medical College and Research Institute Gujarat, INDIA
 Tutor, S.B.K.S Medical College and Research Institute Gujarat, INDIA") Prevalence and Microbiological diagnosis of Helicobacter pylori infection and it s antibiotic resistance pattern in the patients suffering from Acid-peptic Diseases Himani B. Pandya, Ph.D (medical microbiology)
Prevalence and Microbiological diagnosis of Helicobacter pylori infection and it s antibiotic resistance pattern in the patients suffering from Acid-peptic Diseases Himani B. Pandya, Ph.D (medical microbiology)
MANAGEMENT OF PELVIC INFLAMMATORY DISEASE
 GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
What Is Thought To Be The Problem?
 Do We Need an Alternative Approach to the Management of Osteomyelitis? Jeffrey C. Karr DPM, CWS, ABLES, FAPWCA, FCCWS Founder, Central Florida Limb Salvage Alliance Chairman, Founder: The Osteomyelitis
Do We Need an Alternative Approach to the Management of Osteomyelitis? Jeffrey C. Karr DPM, CWS, ABLES, FAPWCA, FCCWS Founder, Central Florida Limb Salvage Alliance Chairman, Founder: The Osteomyelitis
Multi-drug resistant microorganisms
 Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
Drug Class Literature Scan: Otic Antibiotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
THE MOLECULAR GENETIC ANALYSIS OF
 THE MOLECULAR GENETIC ANALYSIS OF DIABETIC FOOT WOUNDS ERIN E KLEIN, DPM, MS SARAH E HALLER, DPM; BRETT J WAVERLY, DPM; LOWELL WEIL, DPM; ADAM E FLEISCHER, DPM, MPH WEIL FOOT & ANKLE INSTITUTE DES PLAINES,
THE MOLECULAR GENETIC ANALYSIS OF DIABETIC FOOT WOUNDS ERIN E KLEIN, DPM, MS SARAH E HALLER, DPM; BRETT J WAVERLY, DPM; LOWELL WEIL, DPM; ADAM E FLEISCHER, DPM, MPH WEIL FOOT & ANKLE INSTITUTE DES PLAINES,