The population structure of Staphylococcus aureus among general practice patients from The Netherlands
|
|
|
- Phyllis Jenkins
- 5 years ago
- Views:
Transcription
1 Postprint Version 1.0 Journal website Pubmed link DOI /J X The population structure of Staphylococcus aureus among general practice patients from The Netherlands G. A. DONKER 1, R. H. DEURENBERG 2, C. DRIESSEN 2, S. SEBASTIAN 2, S. NYS 2 AND E. E. STOBBERINGH 2 1 ) Netherlands Institute for Health Services Research (NIVEL), Utrecht and 2 ) Department of Medical Microbiology, University Hospital Maastricht, Maastricht, The Netherlands Corresponding author and reprint requests: R. H. Deurenberg, Department of Medical microbiology, Maastricht Infection Centre (MINC) University Hospital Maastricht, PO Box 5800, 6202 AZ Maastricht, The Netherlands ruud.deurenberg@mumc.nl ABSTRACT To investigate the prevalence, the antibiotic resistance pattern and the population structure of Staphylococcus aureus, S. aureus isolates from the anterior nostrils of patients of general practitioners (GPs) were analysed. Insight into the S. aureus population structure is essential, as nasal carriers of S. aureus are at increased risk of developing an S. aureus infection. S. aureus was isolated from nasal swabs from 2691 patients with no sign of an infection collected in 29 GP practices in The Netherlands. The susceptibility pattern for several classes of antibiotics was determined, as well as the S. aureus genetic background, using spa typing. S. aureus was isolated from 617 of the 2691 (23%) nasal swabs. The prevalences of resistance to ciprofloxacin, co-trimoxazole, fusidic acid, macrolides and mupirocin were 0.2%, 0%, 6%, 5% and 1%, respectively. Half of the isolates were associated with a genetic background common to the major methicillin- resistant S. aureus (MRSA) clones, e.g. clonal complex (CC)1, CC5, CC8, CC22, CC30 and CC45, and the remainder were mainly associated with CC7, CC12, CC15, CC26, CC51 and CC101. The low prevalences of resistance suggest that, in the Dutch situation, S. aureus isolates from patients visiting their GP because of complaints not related to infection do not represent a large reservoir of antibiotic resistance genes. Although no MRSA isolates were found, the genetic background of some of the S. aureus isolates is commonly observed among community-associated (CA)-MRSA clones (CC1, CC8 and CC30), and this might suggest that these isolates have the potential to become CA-MRSA.
2 INTRODUCTION Staphylococcus aureus is a potential hospital-associated (HA) and communityassociated (CA) pathogen that can cause a wide variety of infectious diseases, ranging from minor skin infections to postoperative wound infections and necrotizing pneumonia [1]. It has been shown previously that nasal carriers of S. aureus are at increased risk of developing an S. aureus infection [2]. In addition, it has been shown that S. aureus of any genotype can become a life-threatening pathogen, but that some clones are more virulent than others [3]. Methicillin-resistant S. aureus (MRSA) is an increasing problem worldwide, in the form of both HA-MRSA and CA-MRSA. In The Netherlands, the prevalence of MRSA in hospitals has doubled during the last few years, from 1% in 2002 to 2% in 2006 [4]. Furthermore, several studies have reported the emergence of CA-MRSA in The Netherlands [5,6]. CA-MRSA can cause necrotizing pneumonia and severe skin infections in patients not at risk of MRSA acquisition. CA-MRSA is characterized by the presence of Panton Valentine leukocidin (PVL), the mobile resistance determinant staphylococcal cassette chromosome mec (SCCmec) type IV or V, and a continent-specific genetic background, i.e. clonal complex (CC)1, CC8, CC30 or CC80 in Europe [7]. It has previously been hypothesized that MRSA originated through the transfer of SCCmec from MRSA or methicillin-resistant coagulase-negative staphylococci to extant methicillinsusceptible S. aureus (MSSA) lineages, and that the genetic background of S. aureus determines the stability of the new MRSA clone [8,9]. However, the origin of CA-MRSA is not known, i.e. whether SCCmec has been acquired by MSSA in the community, or whether CA-MRSA is derived from HA-MRSA. Okuma et al. [10] showed that CA-MRSA represent novel acquisitions of SCCmec type IV in the community. However, Aires de Sousa et al. [11] raised the possibility that some CA-MRSA clones may originate in hospitals, as several similarities between CA-MRSA and HA-MRSA isolates were found. In addition to the increased prevalence of MRSA, there is a growing concern regarding the prevalence of antibiotic-resistant microorganisms. Antibiotic use is generally considered to be the main risk factor for antibiotic resistance. Therefore, optimal use of antibiotics may contribute to the control of the problem of antibiotic resistance. Thus, for optimal use of antibiotics, i.e. the right empirical choice for the bacterial population, actual data on antibiotic resistance are essential. However, in The Netherlands, no actual data concerning antibiotic resistance of S. aureus, the main causative agent of skin infections, among general practitioner (GP) patients, are available. The present study investigated the prevalence of antibiotic resistance of S. aureus isolates from patients visiting their GP who had no sign of an infection, with the aim of guiding antibiotic prescribing by GPs. Furthermore, the population structure of the S. aureus isolates was determined using spa typing to investigate whether the S. aureus isolates had a genetic background commonly observed among CA-MRSA isolates. MATERIALS AND METHODS Study population Patients visiting 29 GP practices, distributed among four regions in The Netherlands, participated in this study. The majority of these practices participated in the sentinel project of The Netherlands Institute for Health Services Research. The number of participating practices per region was as follows: two from the northern part of The Netherlands (region I), three from the eastern part (region II), 11 from the middle (region III), and 13 from the southern part (region IV). During 2005, from 2691 patients with no sign of an infection, a nose swab was taken from the anterior nostrils, including 186 from region I, 296 from region II, 901 from region III, and 1308 from region IV. Each participating GP included, at random, patients (age >12 years). The S. aureus prevalence data and the antibiotic susceptibility patterns of
3 the S. aureus strains from his or her patients were sent to the GP anonymously. This study was approved by the ethical committee of the University Hospital Maastricht. Isolation of S. aureus The nasal swabs were sent to the Department of Medical Microbiology of the University Hospital Maastricht for further analyses. The swabs were analysed for the presence of S. aureus using standard microbiological methods, which included culture on medium containing colistin and naladixic acid (BD Diagnostics, Erembodegem-Aalst, Belgium) and nutrient broth (Oxoid, Badhoevedorp, The Netherlands) containing 6.5% NaCl, as well as oxacillin resistance screening agar (Oxoid, The Netherlands), for the isolation of MRSA. All isolates were identified as S. aureus by Gram stain, and catalase and coagulase testing [12]. Antimicrobial susceptibility testing The susceptibility pattern of the S. aureus isolates was determined according to CLSI guidelines, using the microbroth dilution method with Mueller Hinton II cation-adjusted broth (Becton Dickinson, Franklin Lakes, NJ, USA), an inoculum of CFU/mL, and overnight incubation at 37 C [13]. The microtitre plates for the determination of the MIC contained freeze-dried antibiotics (MCS Diagnostics, Swalmen, The Netherlands). Susceptibility to the following antimicrobial agents (range in mg/l) was determined: cefaclor ( ), cefuroxime ( ), clindamycin ( ), ciprofloxacin (0.25 4), clarithromycin ( ), gentamicin ( ), imipenem ( ), linezolid ( ), moxifloxacin (0.12 4), oxacillin ( ), penicillin ( ), rifampin ( ), teicoplanin ( ), tetracycline ( ), trimethoprim sulphamethoxazole (0.015/ /680) and vancomycin ( ). Susceptibility to fusidic acid (100 μg) and mupirocin (10 μg) (Rosco, Taastrup, Denmark) was determined using the disk diffusion method according to CLSI guidelines [13]. All isolates resistant to clarithromycin were tested for inducible clindamycin resistance using the D-test according to CLSI guidelines [14]. Genotypic determinations The oxacillin-resistant isolates were analysed for the presence of the meca gene, using a real-time PCR assay that was developed in the Department of Medical Microbiology of the University Hospital Maastricht. The primers and the TaqMan probe for the detection of meca were designed on the basis of the published sequence (GenBank accession no. X52593) of the meca gene [15]. The sequences of the forward (meca_fp) and reverse (meca_rp) primer were 5'-TGAAGTGGTAAATGGTAATATCGACTTAA-3' and 5'- TAATTCGAGTGCTACTCTAGCAAAGAA-3', respectively (Sigma Genosys, Haverhill, UK). The sequence of the VIC-labeled MGB probe (meca_pr) was 5'- CAAGCAATAGAATCATCAGATAA-3' (Applied Biosystems, Nieuwerk a/d IJssel, The Netherlands). A real-time PCR for the S. aureus-specific fema gene served as an internal control [16]. The following reaction conditions were used in the TaqMan assay: 0.3 μm fema_fp, 0.3 μm fema_rp, 100 nm fema-pr, 0.6 μm meca_fp, 0.6 μm meca_rp, 125 mm meca_pr, 1 TaqMan Universal PCR Master Mix and 4 μl of a 0.5 McFarland suspension ( CFU/mL) in a total volume of reaction mixture of 50 μl. Amplification was performed on the ABI PRISM 7000 Sequence Detection System, using the following programme: 2 min at 50 C and 10 min at 95 C, followed by 42 cycles of 15 s at 95 C and 60 s at 60 C. The presence of the IleS-2 gene, coding for high-level mupirocin resistance, was investigated by PCR as described previously [17]. Real-time amplification of the spa locus, followed by sequencing, was performed as described previously [18]. The spa types were clustered into spa-ccs using the algorithm based upon repeat pattern (BURP) with the Ridom StaphType version 1.5 software package ( The default settings recommended by the manufacturer were used. As it has been shown that spa typing, together with the algorithm BURP, yields results that
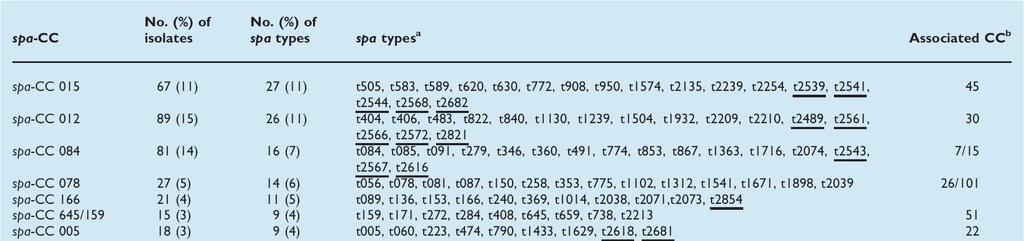
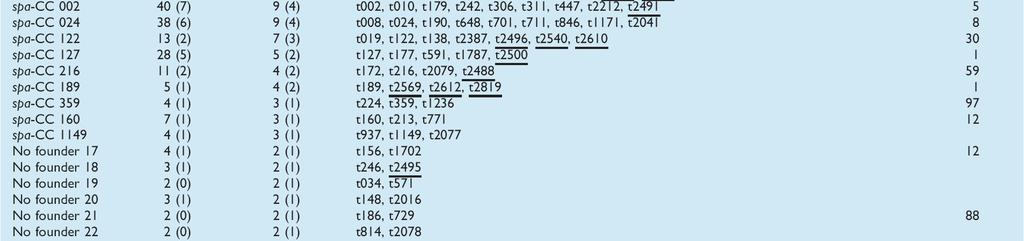
4 are in concordance with typing results obtained by multilocus sequence typing (MLST) and pulsed-field gel electrophoresis [18,19], the associated CCs, as determined with MLST, were allocated through the Ridom SpaServer ( The presence of PVL was investigated on a random subset of 100 isolates with a diverse genetic background, using real-time PCR [20]. Statistical analyses Significant statistical differences were calculated using the Mann Whitney U-test, using SPSS 14.0 (SPSS Inc., Gorinchem, The Netherlands). A p-value of <0.05 was considered to be statistically significant. RESULTS Antibiotic susceptibility pattern S. aureus was isolated from 617 of the 2691 nose swabs received, resulting in a prevalence of 23%. Only one sample from each patient was included in the study. Of the 617 isolates, 595 were available for further analyses; the remaining 22 isolates could not be cultured from the frozen stocks. All isolates were sensitive to clindamycin, trimethroprim sulphamethoxazole and vancomycin. Penicillin resistance was observed among 68% of the isolates. Resistance to oxacillin was observed in four isolates. The MIC values were 4 and 8 mg/l for two strains each. None of the 595 S. aureus strains harboured the meca gene, and they were therefore not classified as MRSA. Resistance to clarithromycin and susceptibility to clindamycin was observed in 30 isolates (5%). The D-test showed that 17 of these S. aureus isolates (57%) had the inducible clindamycin resistance phenotype. Resistance to fusidic acid was observed in 36 isolates (6%), and 2% of the isolates (n = 20) were resistant to tetracycline. Resistance to mupirocin was observed in two isolates, which harboured the IleS-2 gene (Table 1). [TABLE 1] No statistically significant differences (p >0.05) were observed in the distribution of the resistance patterns in the four regions. Distribution of spa types and BURP analyses The 595 MSSA isolates had 244 different spa types, and BURP analysis classified these into 23 spa-ccs (including seven with no founder) and 46 singletons. Twenty-five spa types were excluded from the analysis because the spa region was less than five spa repeats in length (Table 2). New spa types were observed among 48 of the 244 spa types (20%). The most common spa types observed were t002 (4.1%), t005 (1.7%), t008 (4.1%), t012 (5.6%), t015 (2.9%), t021 (3.4%), t026 (2.5%), t056 (1.7%), t084 (3.6%), t091 (5.6%) and t127 (3.6%). Each of the remaining 233 spa types (61.2% of the isolates) accounted for between 0.2% and 1.4% each. [TABLE 2] The most common spa-ccs were spa-cc 012 (15%), spa-cc 015 (11%), spa-cc 002 (7%), spa-cc 024 (6%), spa-cc 127 (5%), spa-cc 005 (3%), spa-cc 122 (2%) and spa- CC 216 (2%). These spa-ccs were associated with genetic backgrounds commonly found among endemic MRSA clones, i.e. CC30, CC45, CC5, CC8, CC1, CC22, CC30 and CC59, respectively (Table 2). Further major spa-ccs were spa-cc 084 (14%), spa-cc 078 (5%), spa-cc 166 (4%) and spa-cc 645/159 (4%). These spa-ccs are associated with CC7/15, CC26/101, an unknown CC, and CC51 respectively, usually observed among MSSA clones. The remaining spa-ccs accounted for <1% of the MSSA isolates (Table 2). The four borderline oxacillin-resistant S. aureus (BORSA) isolates were associated with MLST CC1, CC5, CC12 and CC97.
5 No statistically significant differences (p >0.05) were observed in the distribution of the spa-ccs in the four regions (Table 3). [TABLE 3] Prevalence of PVL None of the MSSA isolates tested harboured PVL. DISCUSSION The prevalence of nasal colonization with S. aureus in the Dutch community (23%) was in agreement with the prevalence in patients admitted to Dutch hospitals (24.4%) [21]. The results of the present study showed a low prevalence of resistance among S. aureus isolates cultured from the nose of patients attending their GP with no sign of an infection. The highest resistance rate was found for penicillin, i.e. 68%, which is still relatively low as compared to the resistance levels found among clinical isolates [1]. The low prevalence of resistance to the antibiotics commonly used by GPs is in line with the general observation of low extramural antibiotic use in The Netherlands [22]. The higher resistance to fusidic acid in comparison with mupirocin (6% vs. <1%) reflects the higher use of fusidic acid than of mupirocin in cases of proven or possible staphylococcal infection. The latter compound is indicated for use only in cases of MRSA colonization. The low rates of resistance to mupirocin and fusidic acid support the current Dutch GP standard for treatment of skin infections. Fusidic acid is the antibiotic of first choice for skin infections, whereas mupirocin is indicated for S. aureus infections caused by fusidic-resistant S. aureus strains. However, the population structure of nasal carriage isolates and clinical isolates can be different [3]. It has been shown that resistance genes can be located on mobile genetic elements in the genome of S. aureus, e.g. transposon Tn554 carrying the erma gene. In addition, S. aureus strains can carry plasmids on which resistance genes are present. Both transposons and plasmids are mobile and can thus be transferred to other S. aureus strains of different lineages, possibly due to antibiotic pressure [23]. The four isolates for which the MIC of oxacillin was 4 or 8 mg/l, but which did not harbour the meca gene, were classified as BORSA [24]. Isolates of this kind have been described previously in a few reports, mostly in a clinical setting, and the mechanism of β- lactam resistance is not clear at the moment, but could involve increased production of β- lactamases [24], or several amino acid substitutions in penicillin-binding protein 2 [25]. The presence of BORSA as part of the commensal nasal flora has, to the best of our knowledge, not been described previously. The clinical significance for the individual patient, or for the patient population in general, has not been investigated, and it is not known whether these isolates are 'precursors' for MRSA and/or whether these isolates spread as easily as MRSA. Although the mechanism of resistance of BORSA and that of MRSA are different, the four BORSA strains had genetic backgrounds (CC1, CC5, CC12 and CC97) that have previously been observed among MRSA isolates. CC1 and CC5 are endemic MRSA lineages [26], whereas sporadic MRSA isolates associated with CC12 and CC97, i.e. ST12-MRSA-IV and ST97-MRSA-IV, have been observed before [27,28]. Furthermore, it has been suggested previously that low-level resistance could be the gateway to high-level resistance [29]. For this study, spa typing, together with BURP analyses, was used to determine the genetic background of the S. aureus isolates. Next, the spa typing/burp data were associated with the MLST CC on the SpaServer, as has been done previously [30 33]. Several spa types correspond to a single sequence type (ST) as determined with MLST, but they remain within an assigned clonal cluster. Furthermore, several studies have shown a good correlation between MLST and spa typing/burp [18,19]. A disadvantage of spa typing is that it sometimes lacks discriminatory power, due to the related spa repeat patterns within different clonal lineages, possibly caused by recombination events involving the spa
6 locus [18]. However, careful study of the figures generated by BURP analyses can resolve this problem [30]. In the present study, 52% of the MSSA isolates that could be classified into spa-ccs had a genetic background commonly observed in either epidemic HA-MRSA clones, i.e. CC5, CC8, CC22, CC30 and CC45 [26], or CA-MRSA clones, i.e. CC1, CC8, CC30 and CC59 [7]. This percentage is comparable to that found in a recent study in Belgium, in which 45% of the MSSA isolates had a genetic background common to the major MRSA clones [34]. MSSA isolates with a CC1, CC5, CC8, CC30 and CC45 background have been described previously in Brazil and Germany, in Danish isolates from the 1960s and 1970s, and in the Dutch and English community [35 40]. CC59 is a common genetic background among CA- MRSA isolates in Asian countries, e.g. Singapore and Taiwan, but has also been observed recently in The Netherlands [7,41 43]. A recent study among children and elderly people in The Netherlands showed that CC30 and CC45 were the most prevalent (47.3%) MSSA clones in the Rotterdam area in the west of The Netherlands [44]. The present study found these MSSA clones in only 26% of the study population. A reason for the difference in prevalence could be the population studied, or the fact that the present study covered GP patients from throughout The Netherlands. Although an outbreak of the communityassociated ST80-MRSA-IV clone has recently been described in the north of The Netherlands, no MSSA isolates with this genetic background were observed in the present study [6]. The fact that MSSA isolates with a genetic background common to CA-MRSA clones were found might suggest that these MSSA isolates could be recipients for SCCmec type IV or V, as these elements are suggested to be highly mobile [8], as has been shown previously with the S. aureus CC30 clone. This clone was prevalent in the 1950s as a penicillin-resistant S. aureus clone, but is now re-emerging, both in the hospital environment as the ST36-MRSA-II clone, and in the community as the PVL-positive ST30- MRSA-IV clone [26,45]. The transfer of SCCmec has been shown to occur frequently in the global evolution of MRSA [39,46,47]. However, high-resolution typing using MLST and S. aureus surface (sas) genes is needed to investigate the possible transfer of SCCmec into these MSSA lineages [39]. Several S. aureus clones with a genetic background that differs from the major MRSA clones, e.g. CC7, CC12, CC15, CC26, CC51, CC97 and CC101, were found. The observation that more MSSA CCs were found than CCs from endemic MRSA clones suggests that the MSSA population is more heterogeneous. Similar observations have been made in Belgium, Brazil, Germany and Portugal [34,37,48,49]. Recently, MSSA isolates of CC7, CC9, CC12, CC15, CC25, CC51 and CC101 have been observed in Belgium and in the English community, although no MRSA isolates with these genetic backgrounds were found [34,40]. Similarly, in Portugal, MSSA isolates of CC9, CC12, CC15, CC25 and CC51 have been found in the community and the hospital environment, whereas no MRSA isolates grouped into these CCs were observed [48]. The CC51 genetic background has been found among Danish MSSA isolates from the 1960s, and among Dutch MSSA isolates observed between 1997 and 2002 in the community [3,36]. These observations support the existence of successful MSSA lineages, e.g. CC7 and CC15, both in the Dutch community and beyond. This also suggests that these MSSA lineages, as compared to other lineages, possess characteristics that favour their persistence in the host, as well as transfer between hosts. Further research is necessary to investigate these characteristics. The absence of PVL-positive isolates is in agreement with the study of Melles et al., which revealed a low PVL prevalence among isolates from nasal carriers (0.6%) and among blood culture isolates (2.1%). However, a PVL prevalence of 38.9% was observed among S. aureus strains that caused abscesses and arthritis, which is in agreement with the involvement of PVL in soft tissue infections [3]. In conclusion, the results suggest that the S. aureus isolates tested did not comprise a large reservoir of antibiotic resistance genes. As the MSSA isolates observed had a heterogeneous
7 genetic background, both common and uncommon to major MRSA clones, and as SCCmec type IV and V are mobile, it is likely that new CA-MRSA clones could emerge in the future. ACKNOWLEDGEMENTS G. A. Donker and R. H. Deurenberg contributed equally to this study. The authors thank all the GPs who participated in the study. TRANSPARENCY DECLARATION The Dutch Working Party on Antibiotic Policy (SWAB) provided financial support for this study. All authors have no conflict of interest to declare. REFERENCES Lowy FD. Staphylococcus aureus infections. N Engl J Med 1998; 339: Wertheim HF, Melles DC, Vos MC et al. The role of nasal carriage in Staphylococcus aureus infections. Lancet Infect Dis 2005; 5: Melles DC, Gorkink RF, Boelens HA et al. Natural population dynamics and expansion of pathogenic clones of Staphylococcus aureus. J Clin Invest 2004; 114: Tiemersma EW, Bronzwaer SL, Lyytikainen O et al. Methicillin-resistant Staphylococcus aureus in Europe, Emerg Infect Dis 2004; 10: Wannet WJ, Spalburg E, Heck ME et al. Emergence of virulent methicillin-resistant Staphylococcus aureus strains carrying Panton Valentine leucocidin genes in the Netherlands. J Clin Microbiol 2005; 43: Stam-Bolink EM, Mithoe D, Baas WH, Arends JP, Moller AV. Spread of a methicillin-resistant Staphylococcus aureus ST80 strain in the community of the northern Netherlands. Eur J Clin Microbiol Infect Dis 2007; 26: Tristan A, Bes M, Meugnier H et al. Global distribution of Panton Valentine leukocidinpositive methicillin-resistant Staphylococcus aureus, Emerg Infect Dis 2007; 13: Hanssen AM, Ericson Sollid JU. SCCmec in staphylococci: genes on the move. FEMS Immunol Med Microbiol 2006; 46: Katayama Y, Robinson DA, Enright MC, Chambers HF. Genetic background affects stability of meca in Staphylococcus aureus. J Clin Microbiol 2005; 43: Okuma K, Iwakawa K, Turnidge JD et al. Dissemination of new methicillin-resistant Staphylococcus aureus clones in the community. J Clin Microbiol 2002; 40: Aires de Sousa M, de Lencastre H. Evolution of sporadic isolates of methicillin-resistant Staphylococcus aureus (MRSA) in hospitals and their similarities to isolates of communityacquired MRSA. J Clin Microbiol 2003; 41: Isenberg HD, ed. Clinical microbiology procedures handbook, 2nd edn. Washington: ASM Press, Clinical Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing, twelfth informational supplement, M100-S12. Villanova, PA: CLSI, O'Sullivan MV, Cai Y, Kong F, Zeng X, Gilbert GL. Influence of disk separation distance on accuracy of the disk approximation test for detection of inducible clindamycin resistance in Staphylococcus spp. J Clin Microbiol 2006; 44: Ryffel C, Tesch W, Birch-Machin I et al. Sequence comparison of meca genes isolated from methicillin-resistant Staphylococcus aureus and Staphylococcus epidermidis. Gene 1990; 94: Deurenberg RH, Nieuwenhuis RF, Driessen C et al. The prevalence of the Staphylococcus aureus tst gene among community- and hospital-acquired strains and isolates from Wegener's granulomatosis patients. FEMS Microbiol Lett 2005; 245: Anthony RM, Connor AM, Power EG, French GL. Use of the polymerase chain reaction for rapid detection of high-level mupirocin resistance in staphylococci. Eur J Clin Microbiol Infect Dis 1999; 18:
8 Strommenger B, Kettlitz C, Weniger T, T Harmsen D, Friedrich AW, Witte W. Assignment of Staphylococcus isolates to groups by spa typing, smai macrorestriction analysis, and multilocus sequence typing. J Clin Microbiol 2006; 44: Strommenger B, Braulke C, Heuck D et al. Spa typing of Staphylococcus aureus as a frontline tool in epidemiological typing. J Clin Microbiol 2008; 46: Deurenberg RH, Vink C, Driessen C et al. Rapid detection of Panton Valentine leukocidin from clinical isolates of Staphylococcus aureus strains by real-time PCR. FEMS Microbiol Lett 2004; 240: Wertheim HF, Vos MC, Ott A et al. Risk and outcome of nosocomial Staphylococcus aureus bacteraemia in nasal carriers versus non-carriers. Lancet 2004; 364: Goossens H, Ferech M, Vander Stichele R, Elseviers M. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet 2005; 365: Lindsay JA, Holden MT. Understanding the rise of the superbug: investigation of the evolution and genomic variation of Staphylococcus aureus. Funct Integr Genomics 2006; 6: Keseru JS, Gal Z, Barabas G, Benko I, Szabo I. Investigation of beta-lactamases in clinical isolates of Staphylococcus aureus for further explanation of borderline methicillin resistance. Chemotherapy 2005; 51: Nadarajah J, Lee MJ, Louie L et al. Identification of different clonal complexes and diverse amino acid substitutions in penicillin-binding protein 2 (PBP2) associated with borderline oxacillin resistance in Canadian Staphylococcus aureus isolates. J Med Microbiol 2006; 55: Deurenberg RH, Vink C, Kalenic S, Friedrich AW, Bruggeman CA, Stobberingh EE. The molecular evolution of methicillin-resistant Staphylococcus aureus. Clin Microbiol Infect 2007; 13: Shore A, Rossney AS, Keane CT, Enright MC, Coleman DC. Seven novel variants of the staphylococcal chromosomal cassette mec in methicillin-resistant Staphylococcus aureus isolates from Ireland. Antimicrob Agents Chemother 2005; 49: Ellington MJ, Yearwood L, Ganner M, East C, Kearns AM. Distribution of the ACME-arcA gene among methicillin-resistant Staphylococcus aureus from England and Wales. J Antimicrob Chemother 2008; 61: Goldstein F. The potential clinical impact of low-level antibiotic resistance in Staphylococcus aureus. J Antimicrob Chemother 2007; 59: 1 4. Nulens E, Stobberingh EE, van Dessel H et al. Molecular characterization of Staphylococcus aureus bloodstream isolates in a Dutch university hospital between 1999 and J Clin Microbiol 2008; 46: Ruppitsch W, Indra A, Stoger A et al. Classifying spa types in complexes improves interpretation of typing results for methicillin-resistant Staphylococcus aureus. J Clin Microbiol 2006; 44: Werbick C, Becker K, Mellmann A et al. Staphylococcal chromosomal cassette mec type I, spa type, and expression of pls are determinants of reduced cellular invasiveness of methicillin-resistant Staphylococcus aureus isolates. J Infect Dis 2007; 195: von Eiff C, Maas D, Sander G, Friedrich AW, Peters G, Becker K. Microbiological evaluation of a new growth-based approach for rapid detection of methicillin-resistant Staphylococcus aureus. J Antimicrob Chemother 2008; 61: Hallin M, Denis O, Deplano A et al. Genetic relatedness between methicillin-susceptible and methicillin-resistant Staphylococcus aureus: results of a national survey. J Antimicrob Chemother 2007; 59: Robinson DA, Enright MC. Evolution of Staphylococcus aureus by large chromosomal replacements. J Bacteriol 2004; 186: Gomes AR, Westh H, de Lencastre H. Origins and evolution of methicillin-resistant Staphylococcus aureus clonal lineages. Antimicrob Agents Chemother 2006; 50: Vivoni AM, Diep BA, de Gouveia Magalhaes AC et al. Clonal composition of Staphylococcus aureus isolates at a Brazilian university hospital: identification of international circulating lineages. J Clin Microbiol 2006; 44:
9 Vandenesch F, Naimi T, T Enright MC et al. Community-acquired methicillin-resistant Staphylococcus aureus carrying Panton Valentine leukocidin genes: worldwide emergence. Emerg Infect Dis 2003; 9: Robinson DA, Enright MC. Evolutionary models of the emergence of methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother 2003; 47: Grundmann H, Hori S, Enright MC et al. Determining the genetic structure of the natural population of Staphylococcus aureus: a comparison of multilocus sequence typing with pulsed-field gel electrophoresis, randomly amplified polymorphic DNA analysis, and phage typing. J Clin Microbiol 2002; 40: Boyle-Vavra S, Ereshefsky B, Wang CC, Daum RS. Successful multiresistant communityassociated methicillin-resistant Staphylococcus aureus lineage from Taipei, Taiwan, that carries either the novel staphylococcal chromosome cassette mec (SCCmec) type VT or SCCmec type IV. J Clin Microbiol 2005; 43: Hsu LY, Koh YL, Chlebicka NL et al. Establishment of ST30 as the predominant clonal type among community-associated methicillin-resistant Staphylococcus aureus isolates in Singapore. J Clin Microbiol 2006; 44: Huijsdens XW, van Santen-Verheuvel MG, Spalburg E et al. Multiple cases of familial transmission of community-acquired methicillin-resistant Staphylococcus aureus. J Clin Microbiol 2006; 44: Melles DC, Tenover FC, Kuehnert MJ et al. Overlapping population structures of nasal isolates of Staphylococcus aureus from healthy Dutch and American individuals. J Clin Microbiol 2008; 46: Robinson DA, Kearns AM, Holmes A et al. Re-emergence of early pandemic Staphylococcus aureus as a community-acquired methicillin-resistant clone. Lancet 2005; 365: Coombs GW. Methicillin-resistant Staphylococcus aureus clones, Western Australia. Emerg Infect Dis 2006; 12: Coombs GW, Nimmo GR, Bell JM et al. Genetic diversity among community methicillinresistant Staphylococcus aureus strains causing outpatient infections in Australia. J Clin Microbiol 2004; 42: Aires de Sousa M, Conceicao T, T Simas C, de Lencastre H. Comparison of genetic backgrounds of methicillin-resistant and -susceptible Staphylococcus aureus isolates from Portuguese hospitals and the community. J Clin Microbiol 2005; 43: Layer F, Ghebremedhin B, Konig W, Konig B. Heterogeneity of methicillin-susceptible Staphylococcus aureus strains at a German university hospital implicates the circulatingstrain pool as a potential source of emerging methicillin-resistant S. aureus clones. J Clin Microbiol 2006; 44:

10 TABLES Table 1. Antibiotic susceptibility pattern by region

11 Table 2. Composition of the spa-ccs

12 TABLE 3. Distribution of the spa-ccs by region
The population structure of Staphylococcus aureus among general practice patients from The Netherlands
 ORIGINAL ARTICLE 10.1111/J.1469-0691.2008.02662.X The population structure of Staphylococcus aureus among general practice patients from The Netherlands G. A. Donker 1, R. H. Deurenberg 2, C. Driessen
ORIGINAL ARTICLE 10.1111/J.1469-0691.2008.02662.X The population structure of Staphylococcus aureus among general practice patients from The Netherlands G. A. Donker 1, R. H. Deurenberg 2, C. Driessen
Microbiological Surveillance of Methicillin Resistant Staphylococcus aureus (MRSA) in Belgian Hospitals in 2003
 in Belgian Hospitals in 2003") Microbiological Surveillance of Methicillin Resistant Staphylococcus aureus (MRSA) in Belgian Hospitals in 3 Final report Olivier Denis and Marc J. Struelens Reference Laboratory for Staphylococci Department
Microbiological Surveillance of Methicillin Resistant Staphylococcus aureus (MRSA) in Belgian Hospitals in 3 Final report Olivier Denis and Marc J. Struelens Reference Laboratory for Staphylococci Department
MRSA surveillance 2014: Poultry
 Vicky Jasson MRSA surveillance 2014: Poultry 1. Introduction In the framework of the FASFC surveillance, a surveillance of MRSA in poultry has been executed in order to determine the prevalence and diversity
Vicky Jasson MRSA surveillance 2014: Poultry 1. Introduction In the framework of the FASFC surveillance, a surveillance of MRSA in poultry has been executed in order to determine the prevalence and diversity
Int.J.Curr.Microbiol.App.Sci (2018) 7(8):
 7(8):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 7 Number 08 (2018) Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2018.708.378
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 7 Number 08 (2018) Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2018.708.378
Geoffrey Coombs 1, Graeme Nimmo 2, Julie Pearson 1, Samantha Cramer 1 and Keryn Christiansen 1
 Community Onset MRSA Infections in Australia: A Tale of Two Clones Geoffrey Coombs 1, Graeme Nimmo 2, Julie Pearson 1, Samantha Cramer 1 and Keryn Christiansen 1 Community Associated MRSA First isolated
Community Onset MRSA Infections in Australia: A Tale of Two Clones Geoffrey Coombs 1, Graeme Nimmo 2, Julie Pearson 1, Samantha Cramer 1 and Keryn Christiansen 1 Community Associated MRSA First isolated
Antimicrobial Resistance
 Antimicrobial Resistance Consequences of Antimicrobial Resistant Bacteria Change in the approach to the administration of empiric antimicrobial therapy Increased number of hospitalizations Increased length
Antimicrobial Resistance Consequences of Antimicrobial Resistant Bacteria Change in the approach to the administration of empiric antimicrobial therapy Increased number of hospitalizations Increased length
Antimicrobial Resistance Acquisition of Foreign DNA
 Antimicrobial Resistance Acquisition of Foreign DNA Levy, Scientific American Horizontal gene transfer is common, even between Gram positive and negative bacteria Plasmid - transfer of single or multiple
Antimicrobial Resistance Acquisition of Foreign DNA Levy, Scientific American Horizontal gene transfer is common, even between Gram positive and negative bacteria Plasmid - transfer of single or multiple
Methicillin-Resistant Staphylococcus aureus
 Methicillin-Resistant Staphylococcus aureus By Karla Givens Means of Transmission and Usual Reservoirs Staphylococcus aureus is part of normal flora and can be found on the skin and in the noses of one
Methicillin-Resistant Staphylococcus aureus By Karla Givens Means of Transmission and Usual Reservoirs Staphylococcus aureus is part of normal flora and can be found on the skin and in the noses of one
Antimicrobial Resistance and Molecular Epidemiology of Staphylococcus aureus in Ghana
 Antimicrobial Resistance and Molecular Epidemiology of Staphylococcus aureus in Ghana Beverly Egyir, PhD Noguchi Memorial Institute for Medical Research Bacteriology Department, University of Ghana Background
Antimicrobial Resistance and Molecular Epidemiology of Staphylococcus aureus in Ghana Beverly Egyir, PhD Noguchi Memorial Institute for Medical Research Bacteriology Department, University of Ghana Background
Annual survey of methicillin-resistant Staphylococcus aureus (MRSA), 2015
, 2015") Annual survey of methicillin-resistant Staphylococcus aureus (MRSA), 2015 Helen Heffernan and Sarah Bakker Nosocomial Infections Laboratory, Institute of Environmental Science and Research Limited (ESR);
Annual survey of methicillin-resistant Staphylococcus aureus (MRSA), 2015 Helen Heffernan and Sarah Bakker Nosocomial Infections Laboratory, Institute of Environmental Science and Research Limited (ESR);
Consequences of Antimicrobial Resistant Bacteria. Antimicrobial Resistance. Molecular Genetics of Antimicrobial Resistance. Topics to be Covered
 Antimicrobial Resistance Consequences of Antimicrobial Resistant Bacteria Change in the approach to the administration of empiric antimicrobial therapy Increased number of hospitalizations Increased length
Antimicrobial Resistance Consequences of Antimicrobial Resistant Bacteria Change in the approach to the administration of empiric antimicrobial therapy Increased number of hospitalizations Increased length
Detection of Methicillin Resistant Strains of Staphylococcus aureus Using Phenotypic and Genotypic Methods in a Tertiary Care Hospital
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 7 (2017) pp. 4008-4014 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.607.415
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 7 (2017) pp. 4008-4014 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.607.415
MID 23. Antimicrobial Resistance. Consequences of Antimicrobial Resistant Bacteria. Molecular Genetics of Antimicrobial Resistance
 Antimicrobial Resistance Molecular Genetics of Antimicrobial Resistance Micro evolutionary change - point mutations Beta-lactamase mutation extends spectrum of the enzyme rpob gene (RNA polymerase) mutation
Antimicrobial Resistance Molecular Genetics of Antimicrobial Resistance Micro evolutionary change - point mutations Beta-lactamase mutation extends spectrum of the enzyme rpob gene (RNA polymerase) mutation
Methicillin resistant Staphylococcus aureus (MRSA) Lina Cavaco
 Lina Cavaco") Methicillin resistant Staphylococcus aureus (MRSA) Lina Cavaco licav@food.dtu.dk 1 DTU Food, Technical University of Denmark Staphylococcus aureus Gram positive cocci Catalase positive Coagulase postive
Methicillin resistant Staphylococcus aureus (MRSA) Lina Cavaco licav@food.dtu.dk 1 DTU Food, Technical University of Denmark Staphylococcus aureus Gram positive cocci Catalase positive Coagulase postive
Spread of a methicillin-resistant Staphylococcus aureus ST80 strain in the community of the northern Netherlands
 Eur J Clin Microbiol Infect Dis (2007) 26:723 727 DOI 10.1007/s10096-007-0352-y CONCISE ARTICLE Spread of a methicillin-resistant Staphylococcus aureus ST80 strain in the community of the northern Netherlands
Eur J Clin Microbiol Infect Dis (2007) 26:723 727 DOI 10.1007/s10096-007-0352-y CONCISE ARTICLE Spread of a methicillin-resistant Staphylococcus aureus ST80 strain in the community of the northern Netherlands
Annual survey of methicillin-resistant Staphylococcus aureus (MRSA), 2014
, 2014") Annual survey of methicillin-resistant Staphylococcus aureus (MRSA), 2014 Helen Heffernan, Sarah Bakker, Kristin Dyet, Deborah Williamson Nosocomial Infections Laboratory, Institute of Environmental Science
Annual survey of methicillin-resistant Staphylococcus aureus (MRSA), 2014 Helen Heffernan, Sarah Bakker, Kristin Dyet, Deborah Williamson Nosocomial Infections Laboratory, Institute of Environmental Science
Antimicrobial Resistance
 Antimicrobial Resistance Consequences of Antimicrobial Resistant Bacteria Change in the approach to the administration of Change in the approach to the administration of empiric antimicrobial therapy Increased
Antimicrobial Resistance Consequences of Antimicrobial Resistant Bacteria Change in the approach to the administration of Change in the approach to the administration of empiric antimicrobial therapy Increased
Epidemiology of community MRSA obtained from the UK West Midlands region.
 Epidemiology of community MRSA obtained from the UK West Midlands region. J. Rollason a, L. Bastin b, A. C. Hilton a, D. G. Pillay c, T. Worthington a, C. Mckeon c, P. De c, K. Burrows c and P. A. Lambert
Epidemiology of community MRSA obtained from the UK West Midlands region. J. Rollason a, L. Bastin b, A. C. Hilton a, D. G. Pillay c, T. Worthington a, C. Mckeon c, P. De c, K. Burrows c and P. A. Lambert
Research Article Genotyping of Methicillin Resistant Staphylococcus aureus Strains Isolated from Hospitalized Children
 International Pediatrics, Article ID 314316, 4 pages http://dx.doi.org/10.1155/2014/314316 Research Article Genotyping of Methicillin Resistant Staphylococcus aureus Strains Isolated from Hospitalized
International Pediatrics, Article ID 314316, 4 pages http://dx.doi.org/10.1155/2014/314316 Research Article Genotyping of Methicillin Resistant Staphylococcus aureus Strains Isolated from Hospitalized
EDUCATIONAL COMMENTARY - Methicillin-Resistant Staphylococcus aureus: An Update
 EDUCATIONAL COMMENTARY - Methicillin-Resistant Staphylococcus aureus: An Update Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain
EDUCATIONAL COMMENTARY - Methicillin-Resistant Staphylococcus aureus: An Update Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain
Tel: Fax:
 CONCISE COMMUNICATION Bactericidal activity and synergy studies of BAL,a novel pyrrolidinone--ylidenemethyl cephem,tested against streptococci, enterococci and methicillin-resistant staphylococci L. M.
CONCISE COMMUNICATION Bactericidal activity and synergy studies of BAL,a novel pyrrolidinone--ylidenemethyl cephem,tested against streptococci, enterococci and methicillin-resistant staphylococci L. M.
Hong-Kai Wang 1, Chun-Yen Huang 1 and Yhu-Chering Huang 1,2*
 Wang et al. BMC Infectious Diseases (2017) 17:470 DOI 10.1186/s12879-017-2560-0 RESEARCH ARTICLE Open Access Clinical features and molecular characteristics of childhood communityassociated methicillin-resistant
Wang et al. BMC Infectious Diseases (2017) 17:470 DOI 10.1186/s12879-017-2560-0 RESEARCH ARTICLE Open Access Clinical features and molecular characteristics of childhood communityassociated methicillin-resistant
Prevalence & Risk Factors For MRSA. For Vets
 For Vets General Information Staphylococcus aureus is a Gram-positive, aerobic commensal bacterium of humans that is carried in the anterior nares of approximately 30% of the general population. It is
For Vets General Information Staphylococcus aureus is a Gram-positive, aerobic commensal bacterium of humans that is carried in the anterior nares of approximately 30% of the general population. It is
Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins
 Staphylococcus aureus Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins Quintessential Pathogen? Nizet
Staphylococcus aureus Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins Quintessential Pathogen? Nizet
Ca-MRSA Update- Hand Infections. Washington Hand Society September 19, 2007
 Ca-MRSA Update- Hand Infections Washington Hand Society September 19, 2007 Resistant Staph. Aureus Late 1940 s -50% S.Aureus resistant to PCN 1957-80/81 strain- of S.A. highly virulent and easily transmissible
Ca-MRSA Update- Hand Infections Washington Hand Society September 19, 2007 Resistant Staph. Aureus Late 1940 s -50% S.Aureus resistant to PCN 1957-80/81 strain- of S.A. highly virulent and easily transmissible
University of Groningen
 University of Groningen Cross-border dissemination of methicillin-resistant Staphylococcus aureus, Euregio Meuse- Rhin region Deurenberg, Ruud H; Nulens, Eric; Valvatne, Havard; Sebastian, Silvie; Driessen,
University of Groningen Cross-border dissemination of methicillin-resistant Staphylococcus aureus, Euregio Meuse- Rhin region Deurenberg, Ruud H; Nulens, Eric; Valvatne, Havard; Sebastian, Silvie; Driessen,
Staphylococcus aureus
 Staphylococcus aureus Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins Quintessential Pathogen? Nizet
Staphylococcus aureus Significant human pathogen. SSTI Biomaterial related infections Osteomyelitis Endocarditis Toxin mediated diseases TSST Staphylococcal enterotoxins Quintessential Pathogen? Nizet
MICRONAUT MICRONAUT-S Detection of Resistance Mechanisms. Innovation with Integrity BMD MIC
 MICRONAUT Detection of Resistance Mechanisms Innovation with Integrity BMD MIC Automated and Customized Susceptibility Testing For detection of resistance mechanisms and specific resistances of clinical
MICRONAUT Detection of Resistance Mechanisms Innovation with Integrity BMD MIC Automated and Customized Susceptibility Testing For detection of resistance mechanisms and specific resistances of clinical
Staphylococcus aureus Programme 2007 (SAP 2007) Hospital Survey MRSA Epidemiology and Typing Report
 Hospital Survey MRSA Epidemiology and Typing Report") AGAR The Australian Group on Antimicrobial Resistance http://antimicrobial-resistance.com Staphylococcus aureus Programme 2007 (SAP 2007) Hospital Survey MRSA Epidemiology and Typing Report PREPARED BY:
AGAR The Australian Group on Antimicrobial Resistance http://antimicrobial-resistance.com Staphylococcus aureus Programme 2007 (SAP 2007) Hospital Survey MRSA Epidemiology and Typing Report PREPARED BY:
Changing epidemiology of methicillin-resistant Staphylococcus aureus colonization in paediatric intensive-care units
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2012 Changing epidemiology of methicillin-resistant Staphylococcus aureus colonization in paediatric intensive-care
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2012 Changing epidemiology of methicillin-resistant Staphylococcus aureus colonization in paediatric intensive-care
Annual survey of methicillin-resistant Staphylococcus aureus (MRSA), 2008
, 2008") Annual survey of methicillin-resistant Staphylococcus aureus (MRSA), 2008 Each year ESR conducts a one-month survey of methicillin-resistant Staphylococcus aureus (MRSA) to provide ongoing information
Annual survey of methicillin-resistant Staphylococcus aureus (MRSA), 2008 Each year ESR conducts a one-month survey of methicillin-resistant Staphylococcus aureus (MRSA) to provide ongoing information
Genetic Lineages of Methicillin-Resistant Staphylococcus aureus Acquired during Admission to an Intensive Care Unit of a General Hospital
 Original Paper Received: April 10, 2016 Accepted: November 8, 2016 Published online: November 8, 2016 Genetic Lineages of Methicillin-Resistant Staphylococcus aureus Acquired during Admission to an Intensive
Original Paper Received: April 10, 2016 Accepted: November 8, 2016 Published online: November 8, 2016 Genetic Lineages of Methicillin-Resistant Staphylococcus aureus Acquired during Admission to an Intensive
Epidemiology of MRSA in Australia
 Epidemiology of MRSA in Australia Graeme R Nimmo Director, Division of Microbiology Pathology Queensland Central Laboratory, Herston QLD 429 Tel: (7) 3636 8 Fax: (7) 3636 1336 Email: Graeme_Nimmo@health.
Epidemiology of MRSA in Australia Graeme R Nimmo Director, Division of Microbiology Pathology Queensland Central Laboratory, Herston QLD 429 Tel: (7) 3636 8 Fax: (7) 3636 1336 Email: Graeme_Nimmo@health.
Community-onset Staphylococcus aureus infections presenting to general practices in South-eastern Australia
 Epidemiol. Infect. (2014), 142, 501 511. Cambridge University Press 2013 doi:10.1017/s0950268813001581 Community-onset Staphylococcus aureus infections presenting to general practices in South-eastern
Epidemiol. Infect. (2014), 142, 501 511. Cambridge University Press 2013 doi:10.1017/s0950268813001581 Community-onset Staphylococcus aureus infections presenting to general practices in South-eastern
January 2014 Vol. 34 No. 1
 January 2014 Vol. 34 No. 1. and Minimum Inhibitory Concentration (MIC) Interpretive Standards for Testing Conditions Medium: diffusion: Mueller-Hinton agar (MHA) Broth dilution: cation-adjusted Mueller-Hinton
January 2014 Vol. 34 No. 1. and Minimum Inhibitory Concentration (MIC) Interpretive Standards for Testing Conditions Medium: diffusion: Mueller-Hinton agar (MHA) Broth dilution: cation-adjusted Mueller-Hinton
Helen Heffernan and Sarah Bakker Nosocomial Infections Laboratory, Institute of Environmental Science and Research Limited (ESR); October 2018
; October 2018") 2017 survey of methicillin-resistant Staphylococcus aureus (MRSA) Helen Heffernan and Sarah Bakker Nosocomial Infections Laboratory, Institute of Environmental Science and Research Limited (ESR); October
2017 survey of methicillin-resistant Staphylococcus aureus (MRSA) Helen Heffernan and Sarah Bakker Nosocomial Infections Laboratory, Institute of Environmental Science and Research Limited (ESR); October
Absence of LA-MRSA CC398 as nasal colonizer of pigs raised
 AEM Accepts, published online ahead of print on 9 December 2011 Appl. Environ. Microbiol. doi:10.1128/aem.07260-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions.
AEM Accepts, published online ahead of print on 9 December 2011 Appl. Environ. Microbiol. doi:10.1128/aem.07260-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions.
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
National MRSA Reference Laboratory
 Author: Gráinne Brennan Date: 23/02/2017 Date of Issue: 23/02/2017 National MRSA Reference Laboratory User s Manual NMRSARL Users Manual Page 1 of 12 Table of Contents Page 1. Location... 3 2. Contact
Author: Gráinne Brennan Date: 23/02/2017 Date of Issue: 23/02/2017 National MRSA Reference Laboratory User s Manual NMRSARL Users Manual Page 1 of 12 Table of Contents Page 1. Location... 3 2. Contact
Failure of Cloxacillin in a Patient with BORSA Endocarditis ACCEPTED
 JCM Accepts, published online ahead of print on 30 December 2008 J. Clin. Microbiol. doi:10.1128/jcm.00571-08 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 30 December 2008 J. Clin. Microbiol. doi:10.1128/jcm.00571-08 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All
Presence of extended spectrum β-lactamase producing Escherichia coli in
 1 2 Presence of extended spectrum β-lactamase producing Escherichia coli in wild geese 3 4 5 A. Garmyn* 1, F. Haesebrouck 1, T. Hellebuyck 1, A. Smet 1, F. Pasmans 1, P. Butaye 2, A. Martel 1 6 7 8 9 10
1 2 Presence of extended spectrum β-lactamase producing Escherichia coli in wild geese 3 4 5 A. Garmyn* 1, F. Haesebrouck 1, T. Hellebuyck 1, A. Smet 1, F. Pasmans 1, P. Butaye 2, A. Martel 1 6 7 8 9 10
Trinity College Dublin, Ireland. College, St. James s Hospital, Dublin, Ireland
 G.I. Brennan et al. Original article Evaluation of commercial chromogenic media for the detection of meticillin-resistant Staphylococcus aureus G.I. Brennan a,b,*, C. Herra c, D.C. Coleman b, B. O Connell
G.I. Brennan et al. Original article Evaluation of commercial chromogenic media for the detection of meticillin-resistant Staphylococcus aureus G.I. Brennan a,b,*, C. Herra c, D.C. Coleman b, B. O Connell
 This is an author version of the contribution published on: Corcione S,Motta I,Fossati L,Campanile F,Stefani S,Cavallo R,Di Perri G,Ranieri VM,De Rosa FG Molecular epidemiology of methicillin-resistant
This is an author version of the contribution published on: Corcione S,Motta I,Fossati L,Campanile F,Stefani S,Cavallo R,Di Perri G,Ranieri VM,De Rosa FG Molecular epidemiology of methicillin-resistant
Community-associated methicillin-resistant Staphylococcus aureus infections
 British Medical Bulletin Advance Access published April 1, 2010 Community-associated methicillin-resistant Staphylococcus aureus infections Fiona J. Cooke and Nicholas M. Brown * Clinical Microbiology
British Medical Bulletin Advance Access published April 1, 2010 Community-associated methicillin-resistant Staphylococcus aureus infections Fiona J. Cooke and Nicholas M. Brown * Clinical Microbiology
Community-associated meticillin-resistant Staphylococcus aureus: the case for a genotypic definition
 Journal of Hospital Infection 81 (2012) 143e148 Available online at www.sciencedirect.com Journal of Hospital Infection journal homepage: www.elsevierhealth.com/journals/jhin Review Community-associated
Journal of Hospital Infection 81 (2012) 143e148 Available online at www.sciencedirect.com Journal of Hospital Infection journal homepage: www.elsevierhealth.com/journals/jhin Review Community-associated
Received 19 June 2012; returned 12 July 2012; revised 19 July 2012; accepted 22 July 2012
 J Antimicrob Chemother 2012; 67: 2809 2813 doi:10.1093/jac/dks329 Advance Access publication 31 August 2012 The newly described meca homologue, meca LGA251, is present in methicillin-resistant Staphylococcus
J Antimicrob Chemother 2012; 67: 2809 2813 doi:10.1093/jac/dks329 Advance Access publication 31 August 2012 The newly described meca homologue, meca LGA251, is present in methicillin-resistant Staphylococcus
56 Clinical and Laboratory Standards Institute. All rights reserved.
 Table 2C 56 Clinical and Laboratory Standards Institute. All rights reserved. Table 2C. Zone Diameter and Minimal Inhibitory Concentration Breakpoints for Testing Conditions Medium: Inoculum: diffusion:
Table 2C 56 Clinical and Laboratory Standards Institute. All rights reserved. Table 2C. Zone Diameter and Minimal Inhibitory Concentration Breakpoints for Testing Conditions Medium: Inoculum: diffusion:
Staphylococcus aureus
 The National Reference Centre (NRC) for S. aureus of Université Libre de Bruxelles (ULB) provides the following tasks: - Identification and antimicrobial susceptibility testing of Staphylococcus sp. strains
The National Reference Centre (NRC) for S. aureus of Université Libre de Bruxelles (ULB) provides the following tasks: - Identification and antimicrobial susceptibility testing of Staphylococcus sp. strains
European Antimicrobial Resistance Surveillance System (EARSS) in Scotland: 2004
 in Scotland: 2004") European Antimicrobial Resistance Surveillance System (EARSS) in Scotland: 2004 SECOND ANNUAL REPORT MJ Coyne 1, SJ Dancer 1, G Edwards 2, 3, D Morrison 2. 1 Health Protection Scotland, 2 Scottish MRSA
European Antimicrobial Resistance Surveillance System (EARSS) in Scotland: 2004 SECOND ANNUAL REPORT MJ Coyne 1, SJ Dancer 1, G Edwards 2, 3, D Morrison 2. 1 Health Protection Scotland, 2 Scottish MRSA
SCOTTISH MRSA REFERENCE LABORATORY
 Title SCOTTISH MRSA REFERENCE LABORATORY LABORATORY PROCEDURE NUMBER / VERSION User Manual DATE OF ISSUE 20/01/2017 REVIEW INTERVAL AUTHORISED BY AUTHOR 1 Year Dr. B. Jones Dr E. Dickson COPY 1 of 1 Master
Title SCOTTISH MRSA REFERENCE LABORATORY LABORATORY PROCEDURE NUMBER / VERSION User Manual DATE OF ISSUE 20/01/2017 REVIEW INTERVAL AUTHORISED BY AUTHOR 1 Year Dr. B. Jones Dr E. Dickson COPY 1 of 1 Master
Characteristics of community- and hospitalacquired meticillin-resistant Staphylococcus aureus strains carrying SCCmec type IV isolated in Malaysia
 Journal of Medical Microbiology (2009), 58, 1213 1218 DOI 10.1099/jmm.0.011353-0 Characteristics of community- and hospitalacquired meticillin-resistant Staphylococcus aureus strains carrying SCCmec type
Journal of Medical Microbiology (2009), 58, 1213 1218 DOI 10.1099/jmm.0.011353-0 Characteristics of community- and hospitalacquired meticillin-resistant Staphylococcus aureus strains carrying SCCmec type
Bacterial whole genome sequencing in clinical microbiology, infection control and public health. Julian Parkhill. FIS, Birmingham, November 2013
 Bacterial whole genome sequencing in clinical microbiology, infection control and public health Julian Parkhill FIS, Birmingham, November 2013 Falling costs of genomics 2003 Cost/genome Throughput 60,000
Bacterial whole genome sequencing in clinical microbiology, infection control and public health Julian Parkhill FIS, Birmingham, November 2013 Falling costs of genomics 2003 Cost/genome Throughput 60,000
CME/SAM. Validation and Implementation of the GeneXpert MRSA/SA Blood Culture Assay in a Pediatric Setting
 Microbiology and Infectious Disease / Xpert MRSA/SA in Pediatric Blood Cultures Validation and Implementation of the GeneXpert MRSA/SA Blood Culture Assay in a Pediatric Setting David H. Spencer, MD, PhD,
Microbiology and Infectious Disease / Xpert MRSA/SA in Pediatric Blood Cultures Validation and Implementation of the GeneXpert MRSA/SA Blood Culture Assay in a Pediatric Setting David H. Spencer, MD, PhD,
Performance Information. Vet use only
 Performance Information Vet use only Performance of plates read manually was measured in three sites. Each centre tested Enterobacteriaceae, streptococci, staphylococci and pseudomonas-like organisms.
Performance Information Vet use only Performance of plates read manually was measured in three sites. Each centre tested Enterobacteriaceae, streptococci, staphylococci and pseudomonas-like organisms.
Prevalence and Molecular Characteristics of Methicillin-resistant Staphylococcus aureus Isolates in a Neonatal Intensive Care Unit
 Journal of Bacteriology and Virology 2016. Vol. 46, No. 2 p.99 103 http://dx.doi.org/10.4167/jbv.2016.46.2.99 Communication Prevalence and Molecular Characteristics of Methicillin-resistant Staphylococcus
Journal of Bacteriology and Virology 2016. Vol. 46, No. 2 p.99 103 http://dx.doi.org/10.4167/jbv.2016.46.2.99 Communication Prevalence and Molecular Characteristics of Methicillin-resistant Staphylococcus
In vitro activity of tigecycline against methicillin-resistant Staphylococcus aureus, including livestock-associated strains
 Eur J Clin Microbiol Infect Dis (2010) 29:503 507 DOI 10.1007/s10096-010-0886-2 ARTICLE In vitro activity of tigecycline against methicillin-resistant Staphylococcus aureus, including livestock-associated
Eur J Clin Microbiol Infect Dis (2010) 29:503 507 DOI 10.1007/s10096-010-0886-2 ARTICLE In vitro activity of tigecycline against methicillin-resistant Staphylococcus aureus, including livestock-associated
Detection of inducible clindamycin resistance among clinical isolates of Staphylococcus aureus in a tertiary care hospital
 ISSN: 2319-7706 Volume 3 Number 9 (2014) pp. 689-694 http://www.ijcmas.com Original Research Article Detection of inducible clindamycin resistance among clinical isolates of Staphylococcus aureus in a
ISSN: 2319-7706 Volume 3 Number 9 (2014) pp. 689-694 http://www.ijcmas.com Original Research Article Detection of inducible clindamycin resistance among clinical isolates of Staphylococcus aureus in a
MRSA. ( Staphylococcus aureus; S. aureus ) ( community-associated )
 ( community-associated )") 005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
*Corresponding Author:
 Original Research Article DOI: 10.18231/2394-5478.2017.0098 Prevalence and factors associated with the nasal colonization of Staphylococcus aureus and Methicillin-Resistant Staphylococcus aureus among
Original Research Article DOI: 10.18231/2394-5478.2017.0098 Prevalence and factors associated with the nasal colonization of Staphylococcus aureus and Methicillin-Resistant Staphylococcus aureus among
CHAPTER 1 INTRODUCTION
 1 CHAPTER 1 INTRODUCTION The Staphylococci are a group of Gram-positive bacteria, 14 species are known to cause human infections but the vast majority of infections are caused by only three of them. They
1 CHAPTER 1 INTRODUCTION The Staphylococci are a group of Gram-positive bacteria, 14 species are known to cause human infections but the vast majority of infections are caused by only three of them. They
Help with moving disc diffusion methods from BSAC to EUCAST. Media BSAC EUCAST
 Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
ESCMID Online Lecture Library. by author
 ESCMID Postgraduate Technical Workshop Antimicrobial susceptibility testing and surveillance of resistance in Gram-positive cocci: laboratory to clinic Current epidemiology of invasive enterococci in Europe
ESCMID Postgraduate Technical Workshop Antimicrobial susceptibility testing and surveillance of resistance in Gram-positive cocci: laboratory to clinic Current epidemiology of invasive enterococci in Europe
Persistence of livestock-associated MRSA after short term occupational exposure to
 JCM Accepts, published online ahead of print on 12 January 2011 J. Clin. Microbiol. doi:10.1128/jcm.00493-10 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 12 January 2011 J. Clin. Microbiol. doi:10.1128/jcm.00493-10 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
Should we test Clostridium difficile for antimicrobial resistance? by author
 Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
SCOTTISH MRSA REFERENCE LABORATORY
 Title SCOTTISH MRSA REFERENCE LABORATORY LABORATORY PROCEDURE NUMBER / VERSION User Manual DATE OF ISSUE 17/05/2014 REVIEW INTERVAL AUTHORISED BY AUTHOR 2 Years Dr. B. Jones B. Cosgrove COPY 1 of 1 Master
Title SCOTTISH MRSA REFERENCE LABORATORY LABORATORY PROCEDURE NUMBER / VERSION User Manual DATE OF ISSUE 17/05/2014 REVIEW INTERVAL AUTHORISED BY AUTHOR 2 Years Dr. B. Jones B. Cosgrove COPY 1 of 1 Master
What s new in EUCAST methods?
 What s new in EUCAST methods? Derek Brown EUCAST Scientific Secretary Interactive question 1 MIC determination MH-F broth for broth microdilution testing of fastidious microorganisms Gradient MIC tests
What s new in EUCAST methods? Derek Brown EUCAST Scientific Secretary Interactive question 1 MIC determination MH-F broth for broth microdilution testing of fastidious microorganisms Gradient MIC tests
Prevalence and Risk Factor Analysis for Methicillin-Resistant Staphylococcus aureus Nasal Colonization in Children Attending Child Care Centers
 JOURNAL OF CLINICAL MICROBIOLOGY, Mar. 2011, p. 1041 1047 Vol. 49, No. 3 0095-1137/11/$12.00 doi:10.1128/jcm.02235-10 Copyright 2011, American Society for Microbiology. All Rights Reserved. Prevalence
JOURNAL OF CLINICAL MICROBIOLOGY, Mar. 2011, p. 1041 1047 Vol. 49, No. 3 0095-1137/11/$12.00 doi:10.1128/jcm.02235-10 Copyright 2011, American Society for Microbiology. All Rights Reserved. Prevalence
STAPHYLOCOCCI: KEY AST CHALLENGES
 Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
The molecular epidemiology of methicillin-resistant Staphylococcus aureus (MRSA) in the major countries of East Asia
 in the major countries of East Asia") Boston University OpenBU Theses & Dissertations http://open.bu.edu Boston University Theses & Dissertations 2017 The molecular epidemiology of methicillin-resistant Staphylococcus aureus (MRSA) in the
Boston University OpenBU Theses & Dissertations http://open.bu.edu Boston University Theses & Dissertations 2017 The molecular epidemiology of methicillin-resistant Staphylococcus aureus (MRSA) in the
Impact of a Standardized Protocol to Address Outbreak of Methicillin-resistant
 Impact of a Standardized Protocol to Address Outbreak of Methicillin-resistant Staphylococcus Aureus Skin Infections at a large, urban County Jail System Earl J. Goldstein, MD* Gladys Hradecky, RN* Gary
Impact of a Standardized Protocol to Address Outbreak of Methicillin-resistant Staphylococcus Aureus Skin Infections at a large, urban County Jail System Earl J. Goldstein, MD* Gladys Hradecky, RN* Gary
RESISTANCE OF STAPHYLOCOCCUS AUREUS TO VANCOMYCIN IN ZARQA, JORDAN
 RESISTANCE OF STAPHYLOCOCCUS AUREUS TO VANCOMYCIN IN ZARQA, JORDAN Hussein Azzam Bataineh 1 ABSTRACT Background: Vancomycin has been widely used in the treatment of infections caused by Methicillin-Resistant
RESISTANCE OF STAPHYLOCOCCUS AUREUS TO VANCOMYCIN IN ZARQA, JORDAN Hussein Azzam Bataineh 1 ABSTRACT Background: Vancomycin has been widely used in the treatment of infections caused by Methicillin-Resistant
Community-Associated Methicillin-Resistant Staphylococcus aureus: Epidemiology and Clinical Consequences of an Emerging Epidemic
 CLINICAL MICROBIOLOGY REVIEWS, July 2010, p. 616 687 Vol. 23, No. 3 0893-8512/10/$12.00 doi:10.1128/cmr.00081-09 Copyright 2010, American Society for Microbiology. All Rights Reserved. Community-Associated
CLINICAL MICROBIOLOGY REVIEWS, July 2010, p. 616 687 Vol. 23, No. 3 0893-8512/10/$12.00 doi:10.1128/cmr.00081-09 Copyright 2010, American Society for Microbiology. All Rights Reserved. Community-Associated
Routine internal quality control as recommended by EUCAST Version 3.1, valid from
 Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
Accepted March 26, 2012
 Journal of Bacteriology Research Vol. 4(2), pp. 15-23, July 2012 Available online at http://www.academicjournals.org/jbr DOI: 10.5897/JBR12.005 ISSN 2006-9871 2012 Academic Journals Full Length Research
Journal of Bacteriology Research Vol. 4(2), pp. 15-23, July 2012 Available online at http://www.academicjournals.org/jbr DOI: 10.5897/JBR12.005 ISSN 2006-9871 2012 Academic Journals Full Length Research
An Approach to Linezolid and Vancomycin against Methicillin Resistant Staphylococcus Aureus
 Article ID: WMC00590 ISSN 2046-1690 An Approach to Linezolid and Vancomycin against Methicillin Resistant Staphylococcus Aureus Author(s):Dr. K P Ranjan, Dr. D R Arora, Dr. Neelima Ranjan Corresponding
Article ID: WMC00590 ISSN 2046-1690 An Approach to Linezolid and Vancomycin against Methicillin Resistant Staphylococcus Aureus Author(s):Dr. K P Ranjan, Dr. D R Arora, Dr. Neelima Ranjan Corresponding
Can we trust the Xpert?
 Can we trust the Xpert? An evaluation of the Xpert MRSA/SA BC System and an assessment of potential clinical impact Dr Kessendri Reddy Division of Medical Microbiology, NHLS Tygerberg Fakulteit Geneeskunde
Can we trust the Xpert? An evaluation of the Xpert MRSA/SA BC System and an assessment of potential clinical impact Dr Kessendri Reddy Division of Medical Microbiology, NHLS Tygerberg Fakulteit Geneeskunde
ORIGINAL ARTICLE /j x
 ORIGINAL ARTICLE 10.1111/j.1469-0691.2008.02064.x Community-associated Staphylococcus aureus infections and nasal carriage among children: molecular microbial data and clinical characteristics G. Sdougkos
ORIGINAL ARTICLE 10.1111/j.1469-0691.2008.02064.x Community-associated Staphylococcus aureus infections and nasal carriage among children: molecular microbial data and clinical characteristics G. Sdougkos
Solmaz Ohadian Moghadam 1, Mohammad Reza Pourmand 1,, Mahmood Mahmoudi 2 and Hooman Sadighian 3. RESEARCH LETTER Taxonomy & Systematics ABSTRACT
 FEMS Microbiology Letters, 362, 2015, fnv043 doi: 10.1093/femsle/fnv043 Advance Access Publication Date: 20 March 2015 Research Letter RESEARCH LETTER Taxonomy & Systematics Molecular characterization
FEMS Microbiology Letters, 362, 2015, fnv043 doi: 10.1093/femsle/fnv043 Advance Access Publication Date: 20 March 2015 Research Letter RESEARCH LETTER Taxonomy & Systematics Molecular characterization
Principles of Antimicrobial Therapy
 Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
A 12-year survey of methicillin-resistant Staphylococcus aureus infections in Greece: ST80-IV epidemic?
 ORIGINAL ARTICLE BACTERIOLOGY A 12-year survey of methicillin-resistant Staphylococcus aureus infections in Greece: ST80-IV epidemic? E. Drougka 1,2, A. Foka 1,2, A. Liakopoulos 3, A. Doudoulakakis 4,
ORIGINAL ARTICLE BACTERIOLOGY A 12-year survey of methicillin-resistant Staphylococcus aureus infections in Greece: ST80-IV epidemic? E. Drougka 1,2, A. Foka 1,2, A. Liakopoulos 3, A. Doudoulakakis 4,
Methicillin-resistant Staphylococcus aureus (MRSA) on Belgian pig farms
 on Belgian pig farms") Methicillinresistant Staphylococcus aureus (MRSA) on Belgian pig farms Dewaele I., De Man I., Stael A., Delputte P., Butaye P., Vlaemynck G., Herman L., Heyndrickx M., Rasschaert G. 1 ILVO: Institute for
Methicillinresistant Staphylococcus aureus (MRSA) on Belgian pig farms Dewaele I., De Man I., Stael A., Delputte P., Butaye P., Vlaemynck G., Herman L., Heyndrickx M., Rasschaert G. 1 ILVO: Institute for
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
Volume-7, Issue-2, April-June-2016 Coden IJABFP-CAS-USA Received: 5 th Mar 2016 Revised: 11 th April 2016 Accepted: 13 th April 2016 Research article
 Volume-7, Issue-2, April-June-2016 Coden IJABFP-CAS-USA Copyrights@2016 Received: 5 th Mar 2016 Revised: 11 th April 2016 Accepted: 13 th April 2016 Research article A STUDY ON ANTIBIOTIC SUSCEPTIBILITY
Volume-7, Issue-2, April-June-2016 Coden IJABFP-CAS-USA Copyrights@2016 Received: 5 th Mar 2016 Revised: 11 th April 2016 Accepted: 13 th April 2016 Research article A STUDY ON ANTIBIOTIC SUSCEPTIBILITY
CA-MRSA a new problem in Indonesia?
 CA-MRSA a new problem in Indonesia? Latre Buntaran Clinical Microbiologist Consultant Indonesia Coordinator of ANSORP Study Secretary General of INASIC Community Associated MRSA Papua New Guinea Asia Europe
CA-MRSA a new problem in Indonesia? Latre Buntaran Clinical Microbiologist Consultant Indonesia Coordinator of ANSORP Study Secretary General of INASIC Community Associated MRSA Papua New Guinea Asia Europe
Abstract. Background. Editor: G. Lina
 ORIGINAL ARTICLE BACTERIOLOGY Evidence of transmission of a Panton Valentine leukocidin-positive community-acquired methicillin-resistant Staphylococcus aureus clone: a family affair P. Cocchi 1, G. Taccetti
ORIGINAL ARTICLE BACTERIOLOGY Evidence of transmission of a Panton Valentine leukocidin-positive community-acquired methicillin-resistant Staphylococcus aureus clone: a family affair P. Cocchi 1, G. Taccetti
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Methicillin-Resistant Staphylococcus aureus (MRSA) in Food. Production Animals
 in Food. Production Animals") Methicillin-Resistant Staphylococcus aureus (MRSA) in Food Production Animals W. VANDERHAEGHEN 1,2 K. HERMANS 2 F. HAESEBROUCK 2 P. BUTAYE 1,2 1 Operational Directorate of Bacterial Diseases, Veterinary
Methicillin-Resistant Staphylococcus aureus (MRSA) in Food Production Animals W. VANDERHAEGHEN 1,2 K. HERMANS 2 F. HAESEBROUCK 2 P. BUTAYE 1,2 1 Operational Directorate of Bacterial Diseases, Veterinary
Antibiotic Reference Laboratory, Institute of Environmental Science and Research Limited (ESR); August 2017
; August 2017") Antimicrobial susceptibility of Shigella, 2015 and 2016 Helen Heffernan and Rosemary Woodhouse Antibiotic Reference Laboratory, Institute of Environmental Science and Research Limited (ESR); August 2017
Antimicrobial susceptibility of Shigella, 2015 and 2016 Helen Heffernan and Rosemary Woodhouse Antibiotic Reference Laboratory, Institute of Environmental Science and Research Limited (ESR); August 2017
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
EUCAST recommended strains for internal quality control
 EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
Compliance of manufacturers of AST materials and devices with EUCAST guidelines
 Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
Microbiological and Genotypic Analysis of Methicillin-Resistant ACCEPTED. 1. Department of Medicine, New York Medical College, Valhalla, NY
 AAC Accepts, published online ahead of print on 7 July 2008 Antimicrob. Agents Chemother. doi:10.1128/aac.00357-08 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions.
AAC Accepts, published online ahead of print on 7 July 2008 Antimicrob. Agents Chemother. doi:10.1128/aac.00357-08 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions.
Infections caused by Methicillin-Resistant Staphylococcus
 MRSA infections are no longer limited to hospitals. An infectious disease specialist offers insight on what this means for dermatologists. By Robert S. Jones, DO, Reading, PA Infections caused by Methicillin-Resistant
MRSA infections are no longer limited to hospitals. An infectious disease specialist offers insight on what this means for dermatologists. By Robert S. Jones, DO, Reading, PA Infections caused by Methicillin-Resistant
Typing of Methicillin Resistant Staphylococcus Aureus Using DNA Fingerprints by Pulsed-field Gel Electrophoresis
 Published online: 16/07/2016 Published print:08/2016 ORIGINAL PAPER Typing of Methicillin Resistant Staphylococcus Aureus Using DNA Fingerprints by Pulsed-field Gel Electrophoresis Velma Rebic 1, Ana Budimir
Published online: 16/07/2016 Published print:08/2016 ORIGINAL PAPER Typing of Methicillin Resistant Staphylococcus Aureus Using DNA Fingerprints by Pulsed-field Gel Electrophoresis Velma Rebic 1, Ana Budimir
Methicillin-resistant coagulase-negative staphylococci Methicillin-resistant. spa Staphylococcus aureus
 126 2005 Methicillin-resistant coagulase-negative staphylococci Methicillin-resistant Staphylococcus aureus 1) 1) 1) 1) 1) 2) 3) 4) 2) 1) MBC 2) 3) 4) 17 3 28 17 8 22 Methicillin-resistant Staphylococcus
126 2005 Methicillin-resistant coagulase-negative staphylococci Methicillin-resistant Staphylococcus aureus 1) 1) 1) 1) 1) 2) 3) 4) 2) 1) MBC 2) 3) 4) 17 3 28 17 8 22 Methicillin-resistant Staphylococcus
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust
 PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
North West Neonatal Operational Delivery Network Working together to provide the highest standard of care for babies and families
 Document Title and Reference : Guideline for the management of multi-drug resistant organisms (MDRO) Main Author (s) Simon Power Ratified by: GM NSG Date Ratified: February 2012 Review Date: March 2017
Document Title and Reference : Guideline for the management of multi-drug resistant organisms (MDRO) Main Author (s) Simon Power Ratified by: GM NSG Date Ratified: February 2012 Review Date: March 2017
Int.J.Curr.Microbiol.App.Sci (2016) 5(12):
 5(12):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 12 (2016) pp. 644-649 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.512.071
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 12 (2016) pp. 644-649 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.512.071
BMR Microbiology. Research Article
 www.advancejournals.org Open Access Scientific Publisher Research Article A STUDY OF METICILLIN RESISTANT PATTERN ON CLINICAL ISOLATES OF Staphylococcus aureus IN TERTIARY CARE HOSPITALS OF POKHARA Suresh
www.advancejournals.org Open Access Scientific Publisher Research Article A STUDY OF METICILLIN RESISTANT PATTERN ON CLINICAL ISOLATES OF Staphylococcus aureus IN TERTIARY CARE HOSPITALS OF POKHARA Suresh