4/10/2014. Prof.Dr.Mohamed Bassiouny Professor of Otolaryngology Alexandria University.
|
|
|
- Bertha Patrick
- 5 years ago
- Views:
Transcription
1 Prof.Dr.Mohamed Bassiouny Professor of Otolaryngology Alexandria University. 1
2 Aim When? What? For how long? Antibiotic Hamada, 5 month old baby referred to your office C/O ; Irritability, fever, vomiting and diarrhoea since 2 days. 2

3 The condition started since 2 days following URT infection. The family seeked medical advice. The family Dr assured the family,and gave only antipyretic. The condition worsened. 3

4 4

5 Omar 22 months. Pain in both ears since one day. 5
6 Youssef 4 years old. Pain in left ear since 2 days. 6


7 MOHAMED BASSIOUNY, M. D. Professor of Otolaryngology Faculty of Medicine Alexandria University 7

8 Definition: Acute Suppurative Inflammation of the Muco-periosteal Lining of the Middle Ear Cleft. Middle Ear Cleft = Eustachian tube + Tympanic Cavity + Mastoid Antrum + Mastoid Air Cells 8

9 Epidemiology Incidence of infection All children by 6 months of age: 48% All children by 1 year of age: 79% All children by 2 years of age: 91% The peak incidence of AOM is from ages 3-18 months. Average of 1.5 Acute Otitis Media episodes per year Despite the recent advances in antibacterial agents, the incidence of acute otitis media is on the rise. Acute otitis media Inflammation in the nasopharynx extends to the medial end of the Eustachian tube, creating stasis and inflammation, which, in turn, alter the pressure within the middle ear. Stasis also permits pathogenic bacteria to colonize the normally sterile middle ear space by direct extension from the nasopharynx. 9
10 Pathogenesis (1) Allergy URT infection Mechanical or functional obstruction of Eust. Tube Adenoid Negative middle ear pressure Inhibits the drainage Impaired mucociliary transport M.E.Effusion. ANTI-INFECTIVES FOR INTERNAL USE ONLY Pathogenesis (2) Reflux from nasophryngeal secretion Aspiration from high negative M.E. pressure Insufflation during crying or sneezing Contamination of effusion from nasopharyngeal secretion ANTI-INFECTIVES FOR INTERNAL USE ONLY 10
11 Pathogenesis (3) 1- Infant &young children have a shorter eustachian tube.. More susceptible to reflux of nasopharyngeal secretion into middle-ear space 2-Young children Increase frequency of viral upper RTIs. Odema of eustachian tube mucosa.. Increase of eustachian tube dysfunction 3- Reactive enlargement of lymphoid tissue ( Adenoids ) at eustachian tube orifice.. Mechanically block tube function 4- Passive exposure to cigarette smoke. Level of cotinine ( metabolite of nicotine ). Adverse effect on ciliary motion and mucociliary clearance ANTI-INFECTIVES FOR INTERNAL USE ONLY Causative pathogens in AOM ( as recovered from MEE) Pathogen % S. pneumoniae H. Influenza M. Catarrhalis 3-20 Viruses: respiratory syncytial virus, rhinovirus, coronavirus, parainfluenza, adenovirus, and enterovirus,
12 Diagnostic approach The history of AOM varies with age, but a number of constant features manifest during the otitis-prone years. Irritability or feeding difficulties may be the only indication of a septic focus in the neonate. Older children begin to demonstrate a consistent presence of fever (with or without a coexistent URTI) and otalgia or earache. In older children and adults, hearing loss becomes a constant feature of AOM & OME, with reports of ear stuffiness noted even before the detection of middle ear fluid. 12

13 13



14 14

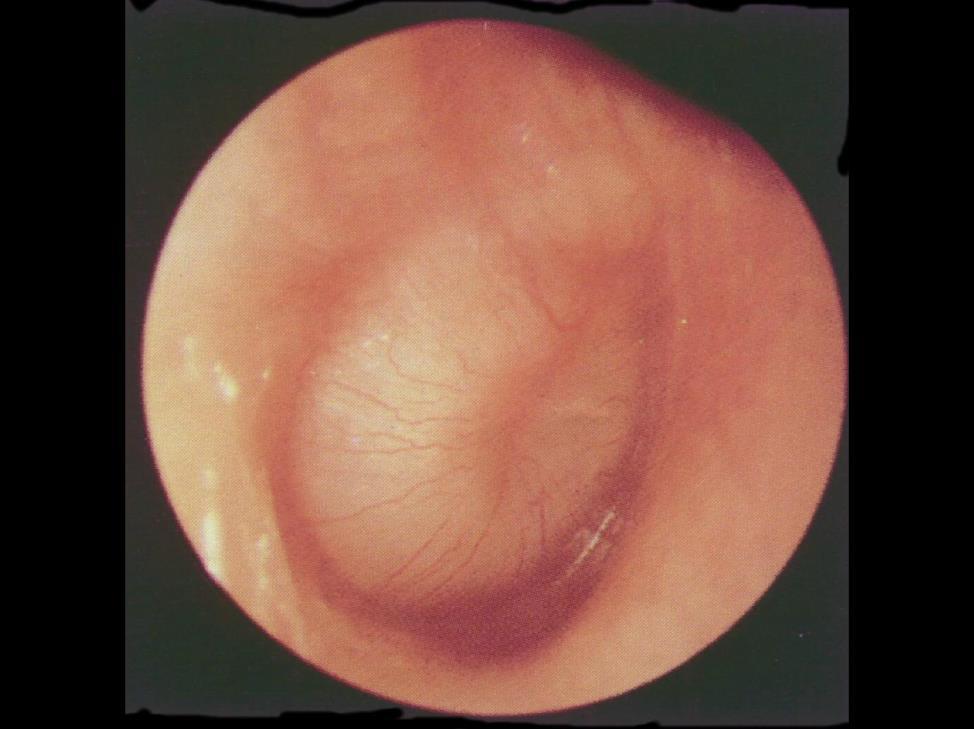
15 How to differentiate between congestion due to crying and otitis media? Otoscopic Diagnosis 15
16 Pneumatic Otoscopy and Tympanometry Pneumatic otoscopy is the primary diagnostic tool for diagnosing the presence of middle ear effusion (MEE) and AOM. Unless the eardrum is bulging (AOM), has air fluid levels, or is obviously a normal TM, the only way to be certain of the presence of MEE on physical exam is by noting the movement of the TM. A grey, erythematous, dull, or yellow TM may not reflect the presence of middle ear fluid. Tympanometry can be used to confirm the diagnosis of MEE. It should only be used to confirm a clinical diagnosis. NOW FOR SOME EXAMPLES Treatment SHOULD ANTIBIOTICS BE USED TO TREAT AOM? The answer is still controversial Spontaneous recovery in 81% of cases Antimicrobial therapy enhanced the primary control by 13.7% 16
17 In the preantibiotic era, complications of AOM such as mastoiditis were far more common than they are today; This difference may be due to the current routine use of antibiotics. It is not possible to determine which cases require antimicrobial therapy and which will resolve spontaneously. AOM in light of the recent guidelines of AAP. Prof. Dr. Mohamed Bassiouny, Professor of Otolaryngology. University of Alexandria 17



18 Scope of the guidelines: These guidelines provide recommendations for the management of uncomplicated acute otitis media in otherwise healthy children from 6 months through 12 years of age without tympanostomy tubes, anatomic abnormalities such as cleft palate or Down syndrome, immune deficiencies, or cochlear implants. Children with OME without AOM are also excluded. 18


19 Burden of the disease: Since the publication of the previous guidelines AOM management has witnessed many changes: Clinician visits for OM decreased from 950 per 1000 children in to 634 per 1000 children in There has been a proportional decrease in antibiotic prescriptions for OM from 760 per 1000 in to 484 per 1000 in The percentage of OM visits resulting in antibiotic prescriptions remained relatively stable (80% in ; 76% in ). Contributing factors to decrease in visits for OM include: Financial issues relating to insurance, such as copayments, that may limit doctor visits, public education campaigns regarding the viral nature of most infectious diseases, use of the PCV7 pneumococcal vaccine, and increased use of the influenza vaccine. Clinicians may also be more attentive to differentiating AOM from OM with effusion (OME), resulting in fewer visits coded for AOM and fewer antibiotic prescriptions written. Burden of the disease: Since the publication of the previous guidelines AOM management has witnessed many changes: clinician visits for OM decreased from 950 per 1000 children in to 634 Despite per 1000 children in all There this has been a proportional decrease in antibiotic prescriptions for OM from 760 per 1000 in to 484 per 1000 in The percentage of OM visits resulting in antibiotic prescriptions remained relatively stable (80% in ; 76% in ). Contributing factors to decrease in visits for OM include: including financial issues OM relating remains to insurance, the such most as copayments, common that may condition limit doctor visits, for public education campaigns regarding the viral nature of most infectious diseases, which useantibacterial of the PCV7 pneumococcal agents vaccine, are andprescribed increased use of the for influenza vaccine. Clinicians may also be more attentive to differentiating AOM children in the United States. from OM with effusion (OME), resulting in fewer visits coded for AOM and fewer antibiotic prescriptions written. 19

20 Regional perspective: Acute otitis media (AOM) is one of the most frequent diagnoses and reasons for prescribing antibiotics in children. 1 A recent data analysis conducted in Italy showed that Otitis Media represents a considerable burden for the healthcare system. 2 Another national survey conducted in Turkey showed that the medical and economic burden of AOM to the health economics in Turkey is considerable. 1 As such, the diagnosis and management of AOM has a significant impact on the health of children, cost of providing care, and overall use of antibacterial agents. Dinleyici EC et al., Results of a national study on the awareness of and attitudes toward acute otitis media (AOM) among clinicians and the estimated direct healthcare costs in Turkey (TR-AOM Study).Int J Pediatr Otorhinolaryngol Feb 21. doi:pii: S (13) /j.ijporl Marchisio P et al., Burden of acute otitis media in primary care pediatrics in Italy: a secondary data analysis from the Pedianet database. BMC Pediatr Nov 29;12(1):185. Key Action Statement 1A Clinicians should diagnose acute otitis media (AOM) in children who present with moderate to severe bulging of the tympanic membrane (TM) or new onset of otorrhea not due to acute otitis externa. Evidence Quality: Grade B. Strength: Recommendation.. 20
21 Rating The Evidence Grade A-At least one randomized well conducted study. Grade B-Well conducted study but not randomized. Grade C-Expert committee reports or opinions. Key Action Statement 1B Clinicians should diagnose AOM in children who present with mild bulging of the TM and recent (less than 48 hours) onset of ear pain (holding, tugging, rubbing of the ear in a nonverbal child) or intense erythema of the TM. Evidence Quality: Grade C. Strength: Recommendation. 21
22 Key Action Statement 1C: Clinicians should not diagnose AOM in children who do not have middle ear effusion (MEE) (based on pneumatic otoscopy and/or tympanometry). Evidence Quality: Grade B. Strength: Recommendation. Key Action Statement 2: The management of AOM should include an assessment of pain. If pain is present, the clinician should recommend treatment to reduce pain. Evidence Quality: Grade B. Strength: Strong Recommendation. 22
23 Key Action Statement 3A Severe AOM: The clinician should prescribe antibiotic therapy for AOM (bilateral or unilateral) in children 6 months and older with severe signs or symptoms (ie, moderate or severe otalgia or otalgia for at least 48 hours or temperature 39 C [102.2 F] or higher).. Evidence Quality: Grade B. Strength: Strong Recommendation Key Action Statement 3B Nonsevere bilateral AOM in young children: The clinician should prescribe antibiotic therapy for bilateral AOM in children 6 months through 23 months of age without severe signs or symptoms (ie, mild otalgia for less than 48 hours and temperature less than 39 C [102.2 F]). Evidence Quality: Grade B. Strength: Strong Recommendation 23
24 Key Action Statement 3C: Nonsevere unilateral AOM in young children: The clinician should either prescribe antibiotic therapy or offer observation with close follow-up based on joint decision making with the parent(s)/caregiver for unilateral AOM in children 6 months to 23 months of age without severe signs or symptoms (ie, mild otalgia for less than 48 hours and temperature less than 39 C [102.2 F]). When observation is used, a mechanism must be in place to ensure follow-up and begin antibiotic therapy if the child worsens or fails to improve within 48 to 72 hours of onset of symptoms. Evidence Quality: Grade B. Strength: Recommendation. Key Action Statement 3D: Nonsevere AOM in older children: The clinician should either prescribe antibiotic therapy or offer observation with close follow-up based on joint decision-making with the parent(s)/ caregiver for AOM (bilateral or unilateral) in children 24 months or older without severe signs or symptoms (ie, mild otalgia for less than 48 hours and temperature less than 39 C [102.2 F]). When observation is used, a mechanism must be in place to ensure follow-up and begin antibiotic therapy if the child worsens or fails to improve within 48 to 72 hours of onset of symptoms. Evidence Quality: Grade B. Strength: Recommendation. 24
25 Key Action Statement 4A Clinicians should prescribe amoxicillin for AOM when a decision to treat with antibiotics has been made and the child has not received amoxicillin in the past 30 days or the child does not have concurrent purulent conjunctivitis or the child is not allergic to penicillin. Evidence Quality: Grade B. Strength: Strong Recommendation Key Action Statement 4B Clinicians should prescribe an antibiotic with additional β- lactamase coverage for AOM when a decision to treat with antibiotics has been made, and the child has received amoxicillin in the last 30 days or has concurrent purulent conjunctivitis, or has a history of recurrent AOM unresponsive to amoxicillin. Evidence Quality: Grade C. Strength: Recommendation 25

26 Key Action Statement 4C: Clinicians should reassess the patient if the caregiver reports that the child s symptoms have worsened or failed to respond to the initial antibiotic treatment within 48 to 72 hours and determine whether a change in therapy is needed. Evidence Quality: Grade B. Strength: Recommendation. Recommended Antibiotics for (Initial or Delayed) Treatment and for Patients Who Have Failed Initial Antibiotic Treatment Initial Immediate or Delayed Antibiotic Treatment Recommended First-line Treatment Amoxicillin (80 90 mg/ kg per day in 2 divided doses) or Amoxicillin-clavulanate a (90 mg/kg per day of amoxicillin, with 6.4 mg/kg per day of clavulanate in 2 divided doses) Alternative Treatment (if Penicillin Allergy) Adapted from Lieberthal AS, Carroll AE, Chonmaitree T et al. Pediatrics 2013;131(3):e Antibiotic Treatment After hours of Failure of Initial Antibiotic Treatment Recommended First-line Treatment Cefdinir (14 mg/kg per day in Amoxicillin-clavulanate a 1 or 2 doses) c (90 mg/kg per day of amoxicillin, with 6.4 mg/kg per day of clavulanate in 2 divided doses) Alternative Treatment Ceftriaxone c, 3 days Clindamycin (30 40 mg/kg per day in 3 divided doses), with or without third-generation cephalosporin Cefuroxime (30 mg/kg per or Failure of second antibiotic day in 2 divided doses) c Cefpodoxime (10 mg/kg per day in 2 divided doses) c Ceftriaxone (50 mg IM or IV per day for 1 or 3 days) c Ceftriaxone (50 mg IM or IV for 3 days) c Clindamycin (30 40 mg/kg per day in 3 divided doses) plus third-generation cephalosporin Tympanocentesis b Consult specialist b IM, intramuscular; IV, intravenous; a May be considered in patients who have received amoxicillin in the previous 30 days or who have the otitis-conjunctivitis syndrome; b Perform tympanocentesis/drainage if skilled in the procedure, or seek a consultation from an otolaryngologist for tympanocentesis/drainage. If the tympanocentesis reveals multidrug-resistant bacteria, seek an infectious disease specialist consultation; c Cefdinir, cefuroxime, cefpodoxime, and ceftriaxone are highly unlikely to be associated with cross-reactivity with penicillin allergy on the basis of their distinct chemical structures. 26



27 Antibiotics therapy: 2004 Duration of Therapy: The optimal duration of therapy for patients with AOM is uncertain however recommendations are: Children younger than 2 years and children with severe symptoms 10 day course Children 2 to 5 years of age with mild or moderate AOM 7day course Children 6 years and older with mild to moderate symptoms 5-7 day course 27
28 Key Action Statement 5A: Clinicians should not prescribe prophylactic antibiotics to reduce the frequency of episodes of AOM in children with recurrent AOM. Evidence Quality: Grade B. Strength: Recommendation. Key Action Statement 5B: Clinicians may offer tympanostomy tubes for recurrent AOM (3 episodes in 6 months or 4 episodes in 1 year with 1 episode in the preceding 6 months). Evidence Quality: Grade B. Strength: Option. 28
29 Key Action Statement 6A: Clinicians should recommend pneumococcal conjugate vaccine to all children according to the schedule of the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention, American Academy of Pediatrics (AAP), and American Academy of Family Physicians (AAFP). Evidence Quality: Grade B. Strength: Strong Recommendation. Key Action Statement 6B: Clinicians should recommend annual influenza vaccine to all children according to the schedule of the Advisory Committee on Immunization Practices, AAP, and AAFP. Evidence Quality: Grade B. Strength: Recommendation.. 29
30 Key Action Statement 6C: Clinicians should encourage exclusive breastfeeding for at least 6 months. Evidence Quality: Grade B. Strength: Recommendation... Key Action Statement 6D: Clinicians should encourage avoidance of tobacco smoke exposure. Evidence Quality: Grade C. Strength: Recommendation 30
, documents exposure to tobacco smoke when measured in saliva,serum,or urine - High concentrations of cotinine in infants and children have")

31 3- Passive smoking - Exposure to smoke can result in changes in the mucosa of the URT, including decreased activity of cilia, increase secretion of mucus, and hyperplasia of goblet cells - A biochemical marker (Cotinine), documents exposure to tobacco smoke when measured in saliva,serum,or urine - High concentrations of cotinine in infants and children have been associated with increase incidence of AOM and prolonged time with middle ear effusion ANTI-INFECTIVES FOR INTERNAL USE ONLY Etzel,et al,1992. II- Environmental R.Fs. 1- Day care An increased incidence of RTIs occurs in children attending group day care compared with children in small-group or home day care Wald,et al,1988. ANTI-INFECTIVES FOR INTERNAL USE ONLY 31



32 2- Breast feeding - Children who are breast-fed have fewer episodes of O.M. than do infants who are bottle-fed - Breast-feeding for 3 months or more was associated with decreased incidence of A.O.M. in the 1st. Year of life - A constituent of breast milk appears to be the important protective factor rather than feeding position ANTI-INFECTIVES Jerome O.Klein,1998 FOR INTERNAL USE ONLY 4- Season Winter, and early spring during which the peak incidence of RTIs ANTI-INFECTIVES FOR INTERNAL USE ONLY Jerome O.Klein,

33 5- Poverty Take home messages: Prophylactic antibiotics should not be prescribed to reduce recurrences. Instead, these children may be offered the option of tympanostomy tubes. Amoxicillin remains the first-line agent; drugs that have additional beta-lactamase coverage are selected for kids who have already had it in the prior month or who are allergic to penicillin Pneumococcal conjugate vaccine and annual flu shots are recommended for all children 33
34 Take home messages: The 2004 guidelines used a three-part definition for acute otitis media: acute onset of symptoms, acute middle ear inflammation, and middle ear effusion. The 2013 update also requires middle ear effusion for diagnosis, but it now has to be based on tympanometry or pneumatic otoscopy. Additional diagnostic criteria include: moderate to severe bulging of the tympanic membrane or new onset of discharge not due to an infected ear canal, and mild bulging of the ear drum and onset of ear pain within 48 hours, which could be indicated by holding, tugging, rubbing of the ear for nonverbal children, or intense redness of the tympanic membrane. Antibiotics should be given for severe cases of bilateral or unilateral acute otitis media for children >6 months based on ear pain that is moderate or severe, lasts for at least 48 hours, or is accompanied by a temperature of >102.2 F. In less severe cases, watchful waiting could be offered instead of antibiotics unless both ears are affected in kids aged 6 23 months. Antibiotics should be given to older children with non severe AOM if their condition worsens or fails to improve within 48 to 72 hours of observation. Recurrent acute otitis media is defined as three episodes in six months or four episodes in the prior year with one in the past six months. Clinical decision making Several distinctive features of the drug under consideration, include: Antibacterial spectrum (Broad Spectrum) PK/PD (MIC, Tissue concentration & Eradication) Patient Satisfaction (e.g. Number of daily doses, Duration of therapy & Early relief of Symptoms) Tolerability Palatability Reasonable Cost (cost-effective) Clinicians also consider therapeutic efficacy based on clinical trials and the recommendations of respectful organizations
35 Clinical algorithm by the Clinical Advisory Committee on Treatment of Recurrent and Persistent AOM (2006) NO risk factors Amoxicillin 45 mg/kg (maximum 1.5 g/d) Or Amoxicillin 90 mg/kg (maximum 3 g/d) High risk for Penicillin-resistant S pneumoniae Amoxicillin 90 mg/kg or Amoxicillin/ clavulanate 90 mg/kg or Cefpodoxime or Cefprozil or Cefuroxime High risk for β-lactamasepositive H influenza, or M catarrhalis or Amoxicillin/clavulanate 45 mg/kg or Cefpodoxime or Cefprozil or Cefuroxime High risk for β-lactamasepositive H influenza, or M catarrhalis Amoxicillin 90 mg/kg or Amoxicillin/ clavulanate 90 mg/kg or Cefpodoxime or Cefprozil or Cefuroxime Failure Ceftriaxone or alternative oral agent with similar activity Failure Tympanocentesis Pichichero ME, Casey JR. Acute otitis media: Making sense of recent guidelines on antimicrobial treatment, J Fam Pract Apr;56(4): Consider a second line antibiotic in when: the clinician has a high suspicion for concurrent conjunctivitisotitis media syndrome, commonly caused by a beta-lactamase producing organism, For children with allergies to penicillin, or other reasons to consider alternative antibiotics Second choice antibiotics: Amoxicillin/clavulanate Cefdinir Cefprozil Cefuroxime Ceftriaxone Azithromycin Clarithromycin 35
36 Recommendatios You must be able to see clearly the drum. Beware of the red TM reflex. Use pneumatic otoscope Good antibiotherapy. A 10-day antibiotic course is the minimum. Return Visit is more important than the first one. When dealing with Meningitis, watch out for Otitis Media. When dealing with Meningitis, watch out for Otitis Media. IN uncomplicated otitis media you should prescribe antibiotic in ; infants less than 6 months, bilateral otitis media and in severe cases. 36
37 Antibiotic recommendations: It is important to note that alternative antibiotics vary in their efficacy against AOM pathogens. For example, recent US data on in vitro susceptibility of S. pneumoniae to cefdinir and cefuroxime are 70% to 80%, compared with 84% to 92% amoxicillin Efficacy. In vitro efficacy of cefdinir and cefuroxime against H. influenzae is approximately 98%, compared with 58% efficacy of amoxicillin and nearly 100% efficacy of amoxicillin/clavulanate. Macrolides, such as erythromycin and azithromycin, have limited efficacy against both H influenzae and S pneumoniae. Clindamycin lacks efficacy against H influenzae. Clindamycin alone (30 40 mg/kg per day in 3 divided doses) may be used for suspected penicillin-resistant S. pneumoniae; however, the drug will likely not be effective for the multidrug-resistant serotypes. Although a single injection of ceftriaxone is approved by the US FDA for the treatment of AOM, results of a double tympanocentesis study (before and 3 days after single dose ceftriaxone) by Leibovitz et al175 suggest that more than 1 ceftriaxone dose may be required to prevent recurrence of the middle ear infection within 5 to 7 days after the initial dose 37


38 Bacterial susceptibility to Antibiotics : Current data from different studies with non-aom sources and geographic locations that may not be comparable show that 58% to 82% of H. influenzae isolates are susceptible to regular and high-dose amoxicillin. Nationwide data suggest that 100% of M. catarrhalis derived from the upper respiratory tract are β-lactamase positive but remain susceptible to amoxicillin clavulanate. Bacterial susceptibility to Antibiotics : Susceptible pathogens Adequate MEF concentrations > MIC Selection of antibiotic to treat AOM is based on the suspected type of bacteria and antibiotic susceptibility pattern, although clinical pharmacology and clinical and microbiologic results and predicted compliance with the drug are also taken into account. Current US data from a number of centers indicates that approximately 83% and 87% of isolates of S. pneumoniae from all age groups are susceptible to regular (40 mg/kg/day) and high-dose amoxicillin (80 90 mg/kg/day divided twice daily), respectively. High-dose amoxicillin will yield middle ear fluid levels that exceed the minimum inhibitory concentration (MIC) of all S. pneumoniae serotypes that are intermediately resistant to penicillin (penicillin MICs, μg/ml), and many but not all highly resistant serotypes (penicillin MICs, 2 μg/ml) for a longer period of the dosing interval and has been shown to improve bacteriologic and clinical efficacy compared with the regular dose. Hoberman et al reported superior efficacy of high-dose amoxicillin/ clavulanate in eradication of S. pneumoniae (96%) from the middle ear at days 4 to 6 of therapy compared with azithromycin. 38

 accounts for less than 5% of AOM cases.")
39 Rationale for Antibiotic therapy: The rationale for antibiotic therapy in children with AOM is based on a high prevalence of bacteria in the accompanying MEE. Bacterial and viral cultures of middle ear fluid collected by tympanocentesis from children with AOM showed 55% with bacteria only and 15% with bacteria and viruses. Microbiology: The 3 most common bacterial pathogens in AOM are: S. pneumoniae Nont ypeable Haemophilus influenzae Moraxella catarrhalis. Streptococcus pyogenes (group A β-hemolytic streptococci) accounts for less than 5% of AOM cases. Recommendation 3A Observation without use of antibacterial agents in a child with uncomplicated AOM is an option for selected children based on diagnostic certainty, age, illness severity, and assurance of follow-up. The observation option for AOM refers to deferring antibacterial treatment of selected children for 48 to 72 hours and limiting management to symptomatic relief. The decision to observe or treat is based on the child s age, diagnostic certainty, and illness severity. To observe a child without initial antibacterial therapy, it is important that the parent/caregiver has a ready means of communicating with the clinician. There also must be a system in place that permits reevaluation of the child. If necessary, the parent/caregiver also must be able to obtain medication conveniently. 39
40 Clinical decision making Several distinctive features of the drug under consideration, include: Antibacterial spectrum (Broad Spectrum) PK/PD (MIC, Tissue concentration & Eradication) Patient Satisfaction (e.g. Number of daily doses, Duration of therapy & Early relief of Symptoms) Tolerability Palatability Reasonable Cost (cost-effective) Clinicians also consider therapeutic efficacy based on clinical trials and the recommendations of respectful organizations. 79 Clinical algorithm by the Clinical Advisory Committee on Treatment of Recurrent and Persistent AOM (2006) Antibiotic treatment with amoxicillin, TMP/SMX, or macrolides within prior month (TMP/SMX) =trimethoprim/ sulfamethoxazole NO Risk factor analysis Yes NOT RECOMMENDED Amoxicillin, TMP-SMX, Erythromycin, sulfisoxazole, azithromycin, clarithromycin NO risk factors Amoxicillin 45 mg/kg (maximum 1.5 g/d) Or Amoxicillin 90 mg/kg (maximum 3 g/d) High risk for Penicillin-resistant S pneumoniae Amoxicillin 90 mg/kg or Amoxicillin/ clavulanate 90 mg/kg or Cefpodoxime or Cefprozil or Cefuroxime High risk for β-lactamasepositive H influenza, or M catarrhalis Or Amoxicillin/clavulanate 45 mg/kg or Cefpodoxime or Cefprozil or Cefuroxime High risk for β-lactamasepositive H influenza, or M catarrhalis Amoxicillin 90 mg/kg or Amoxicillin/ clavulanate 90 mg/kg or Cefpodoxime or Cefprozil or Cefuroxime 40
41 Clinical algorithm by the Clinical Advisory Committee on Treatment of Recurrent and Persistent AOM (2006) NO risk factors Amoxicillin 45 mg/kg (maximum 1.5 g/d) Or Amoxicillin 90 mg/kg (maximum 3 g/d) High risk for Penicillin-resistant S pneumoniae Amoxicillin 90 mg/kg or Amoxicillin/ clavulanate 90 mg/kg or Cefpodoxime or Cefprozil or Cefuroxime High risk for β-lactamasepositive H influenza, or M catarrhalis or Amoxicillin/clavulanate 45 mg/kg or Cefpodoxime or Cefprozil or Cefuroxime High risk for β-lactamasepositive H influenza, or M catarrhalis Amoxicillin 90 mg/kg or Amoxicillin/ clavulanate 90 mg/kg or Cefpodoxime or Cefprozil or Cefuroxime Failure Ceftriaxone or alternative oral agent with similar activity Failure Tympanocentesis Pichichero ME, Casey JR. Acute otitis media: Making sense of recent guidelines on antimicrobial treatment, J Fam Pract Apr;56(4): Consider a second line antibiotic in when: the clinician has a high suspicion for concurrent conjunctivitisotitis media syndrome, commonly caused by a beta-lactamase producing organism, For children with allergies to penicillin, or other reasons to consider alternative antibiotics Second choice antibiotics: Amoxicillin/clavulanate Cefdinir Cefprozil Cefuroxime Ceftriaxone Azithromycin Clarithromycin 41
42 Recommendation 3A If a decision is made to treat with an antibacterial agent, the clinician should prescribe amoxicillin for most children. (This recommendation is based on randomized, clinical trials with limitations and a preponderance of benefit over risk.) When amoxicillin is used, the dose should be 80 to 90 mg/kg per day. (This option is based on extrapolation from microbiologic studies and expert opinion, with a preponderance of benefit over risk.) In patients who have severe illness (moderate to severe otalgia or fever of 39 C or higher42) and in those for whom additional coverage for lactamase positive Haemophilus nfluenzae and Moraxella catarrhalis is desired, therapy should be initiated with high-dose amoxicillin-clavulanate (90 mg/kg per day of amoxicillin component, with 6.4 mg/kg per day of clavulanate in 2 divided doses). This dose has sufficient potassium clavulanate to inhibit all -lactamase producing H influenzae and M catarrhalis Is there any significance for the age? 42
43 It is recommended that treatment with a 10-day course of antibiotics be given to children less than 2 years of age with AOM Amoxicillin, in the dose range of mg/kg/day is effective in the treatment of a first episode of AOM or for a recurrence more than 1 month since recovery from a prior episode of AOM Recommendation 4 If the patient fails to respond to the initial management option within 48 to 72 hours, the clinician must reassess the patient to confirm AOM and exclude other causes of illness. If AOM is confirmed in the patient initially managed with observation, the clinician should begin antibacterial therapy. If the patient was initially managed with an antibacterial agent, the clinician should change the antibacterial agent. 43
44 Recommendation 5 Clinicians should encourage the prevention of AOM through reduction of risk factors. Number of factors associated with early or recurrent AOM which are not amenable to change: for example, genetic predisposition, premature birth, male gender, Native American/Inuit ethnicity, family history of recurrent otitis media, presence of siblings in the household, and low socioeconomic status. Factors which are amenable to change: During infancy and early childhood, reducing the incidence of respiratory tract infections by altering child care center attendance patterns can reduce the incidence of recurrent AOM significantly. The implementation of breastfeeding for at least the first 6 months also seems to be helpful against the development of early episodes of AOM. Avoiding supine bottle feeding ( bottle propping ),reducing or eliminating pacifier use in the second 6 months of life, eliminating exposure to passive tobacco smoke have been postulated to reduce the incidence of AOM in infancy; (however, the utility of these interventions is unclear.) Immunoprophylaxis with killed121 and live-attenuated intranasal122 influenza vaccines has demonstrated more than 30% efficacy in prevention of AOM during the respiratory illness season. (Most of the children in these studies were older than 2 years.) Atypical presentation of AOM? 44


45 Atypical otitis media Otitis media in infancy. Acute necrotizing otitis media. Tuberculous otitis media. Mycobacterial otitis media 45
46 46



47 47

48 Recommendatios You must be able to see clearly the drum. Beware of the red TM reflex. Use pneumatic otoscope Good antibiotherapy. A 10-day antibiotic course is the minimum. Return Visit is more important than the first one. When dealing with Meningitis, watch out for Otitis Media. When dealing with Meningitis, watch out for Otitis Media. IN uncomplicated otitis media you should prescribe antibiotic in ; infants less than 6 months, bilateral otitis media and in severe cases. 48




49 49
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children
 Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Update on the Diagnosis and Management of O33s Media. Leslie Herrmann MD, FAAP Pediatrician
 Update on the Diagnosis and Management of O33s Media Leslie Herrmann MD, FAAP Pediatrician Disclosures I have no financial disclosures. Objec3ves Understand the new diagnos3c criteria for OM Know when
Update on the Diagnosis and Management of O33s Media Leslie Herrmann MD, FAAP Pediatrician Disclosures I have no financial disclosures. Objec3ves Understand the new diagnos3c criteria for OM Know when
Otitis Media. TOM PARTNER, NP suggestions
 Otitis Media TOM PARTNER, NP suggestions Treat Children with Omnicef (cedinir) as first choice because of less likely allergic reaction 14 mg /kg/ d (Once a day x 10 days) but do not exceed total of 600
Otitis Media TOM PARTNER, NP suggestions Treat Children with Omnicef (cedinir) as first choice because of less likely allergic reaction 14 mg /kg/ d (Once a day x 10 days) but do not exceed total of 600
PDF hosted at the Radboud Repository of the Radboud University Nijmegen
 PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/266/9665
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/266/9665
Acute Otitis Media in Pediatric Medicine Current Issues in Epidemiology, Diagnosis, and Management
 REVIEW ARTICLE Pediatr Drugs 2003; 5 Suppl. 1: 1-12 1174-5878/03/0001-0001/$30.00/0 Adis Data Information BV 2003. All rights reserved. Acute Otitis Media in Pediatric Medicine Current Issues in Epidemiology,
REVIEW ARTICLE Pediatr Drugs 2003; 5 Suppl. 1: 1-12 1174-5878/03/0001-0001/$30.00/0 Adis Data Information BV 2003. All rights reserved. Acute Otitis Media in Pediatric Medicine Current Issues in Epidemiology,
ANTIBIOTICS ACUTE OTITIS MEDIA (AOM) IN CHILDREN 3 MONTHS OF AGE OR OLDER GENERAL INFORMATIONS PREVENTIVE MEASURES DIAGNOSIS
 IN CHILDREN 3 MONTHS OF AGE OR OLDER GENERAL INFORMATIONS PREVENTIVE MEASURES DIAGNOSIS") MARCH 206 DRUG ANTIBIOTICS This optimal usage guide is mainly intended f primary care health professionnals. It is provided f infmation purposes only and should not replace the clinician s judgement. The
MARCH 206 DRUG ANTIBIOTICS This optimal usage guide is mainly intended f primary care health professionnals. It is provided f infmation purposes only and should not replace the clinician s judgement. The
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Critical Appraisal Topic. Antibiotic Duration in Acute Otitis Media in Children. Carissa Schatz, BSN, RN, FNP-s. University of Mary
 Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550
 and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550") Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550 Sinusitis Upper respiratory tract infections (URI) Common cold
Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550 Sinusitis Upper respiratory tract infections (URI) Common cold
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Telephone Max dose amoxicillin pediatrics P.O. Box 189 Navan, ON, K4B 1J4 Canada. Sitemap
 Telephone 613-835-9490 Max dose amoxicillin pediatrics P.O. Box 189 Navan, ON, K4B 1J4 Canada Sitemap 25 mg/kg/ dose ( Max : 500 mg/ dose ) PO twice daily for 10 days is recommended by the Infectious Diseases
Telephone 613-835-9490 Max dose amoxicillin pediatrics P.O. Box 189 Navan, ON, K4B 1J4 Canada Sitemap 25 mg/kg/ dose ( Max : 500 mg/ dose ) PO twice daily for 10 days is recommended by the Infectious Diseases
Acute Otitis Media, Roots and Tulips
 Focus on CME at the University of Saskatchewan Acute Otitis Media, Roots and Tulips I have an earache 2000 BC: Here, eat this root. 1000 AD: That root is heathen, say this prayer. 1850 AD: That prayer
Focus on CME at the University of Saskatchewan Acute Otitis Media, Roots and Tulips I have an earache 2000 BC: Here, eat this root. 1000 AD: That root is heathen, say this prayer. 1850 AD: That prayer
Antimicrobial prescribing pattern in acute tonsillitis: A hospital based study in Ajman, UAE
 Antimicrobial prescribing pattern in acute tonsillitis: A hospital based study in Ajman, UAE Lisha Jenny John 1*, Meenu Cherian 2, Jayadevan Sreedharan 3, Tambi Cherian 2 1 Department of Pharmacology,
Antimicrobial prescribing pattern in acute tonsillitis: A hospital based study in Ajman, UAE Lisha Jenny John 1*, Meenu Cherian 2, Jayadevan Sreedharan 3, Tambi Cherian 2 1 Department of Pharmacology,
2/19/2014. Erika Clark, PharmD, BCPS. Palmetto Health Children s Hospital Columbia, SC. Erika W. Clark Nothing to Disclose
 Erika Clark, PharmD, BCPS Palmetto Health Children s Hospital Columbia, SC Erika W. Clark Nothing to Disclose Understand the updated acute otitis media guidelines Review newest update to the guidelines
Erika Clark, PharmD, BCPS Palmetto Health Children s Hospital Columbia, SC Erika W. Clark Nothing to Disclose Understand the updated acute otitis media guidelines Review newest update to the guidelines
Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction
 Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani
 Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process High Priority
 MEASURE TYPE: Process High Priority") Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction Meaningful Measure Area: Appropriate
Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction Meaningful Measure Area: Appropriate
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process High Priority
 MEASURE TYPE: Process High Priority") Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction Meaningful Measure Area: Appropriate Use of Healthcare 2019 COLLECTION
Quality ID #66: Appropriate Testing for Children with Pharyngitis National Quality Strategy Domain: Efficiency and Cost Reduction Meaningful Measure Area: Appropriate Use of Healthcare 2019 COLLECTION
Choosing the Best Antibiotic in Problem Outpatient Infectious Disease Cases
 Choosing the Best Antibiotic in Problem Outpatient Infectious Disease Cases Dr. Earl Rubin Associate Professor Department of Pediatrics Division of Infectious Diseases Montreal Children s Hospital Disclosures
Choosing the Best Antibiotic in Problem Outpatient Infectious Disease Cases Dr. Earl Rubin Associate Professor Department of Pediatrics Division of Infectious Diseases Montreal Children s Hospital Disclosures
Antibiotics in the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease
 Antibiotics in the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease Sung Kyu Kim, M.D.Young Sam Kim, M.D. Department of Internal Medicine Yonsei University College of Medicine,
Antibiotics in the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease Sung Kyu Kim, M.D.Young Sam Kim, M.D. Department of Internal Medicine Yonsei University College of Medicine,
ce lesson Optimizing antibiotic therapy for common childhood respiratory infections By Susanne Moadebi, BSc Pharm, Pharm.D.
 Approved BY CCCEP FOR 1.5 CEUs CCCEP file #896-0309 This lesson has been approved for 1.5 CEUs by the Canadian Council on Continuing Edu ca tion in Pharmacy. Approved for 1.5 CEUs by l Ordre des pharmaciens
Approved BY CCCEP FOR 1.5 CEUs CCCEP file #896-0309 This lesson has been approved for 1.5 CEUs by the Canadian Council on Continuing Edu ca tion in Pharmacy. Approved for 1.5 CEUs by l Ordre des pharmaciens
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
Otitis Media. Quality Department
 Quality Department Guidelines for Clinical Care Ambulatory Otitis Media Otitis Media Guideline Team Team leader Heather L. Burrows, MD, PhD General Pediatrics Team members R. Alexander Blackwood, MD, PhD
Quality Department Guidelines for Clinical Care Ambulatory Otitis Media Otitis Media Guideline Team Team leader Heather L. Burrows, MD, PhD General Pediatrics Team members R. Alexander Blackwood, MD, PhD
Supplementary Online Content
 Supplementary Online Content Gerber JS, Prasad PA, Fiks AG, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians:
Supplementary Online Content Gerber JS, Prasad PA, Fiks AG, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians:
Great moments in acute otitis media
 Great moments in acute otitis media Michael Radetsky MD CM Albuquerque NM An evidenced based approach to reducing antibiotic use in children with acute otitis media: controlled before and after study Cates
Great moments in acute otitis media Michael Radetsky MD CM Albuquerque NM An evidenced based approach to reducing antibiotic use in children with acute otitis media: controlled before and after study Cates
Optimizing Clinical Diagnosis and Antibiotic Prescribing for Common Respiratory Tract Infections, Fanara Family Health Center- Rural Egypt
 Sameh F. Ahmed, et al Optimizing Clinical Diagnosis and Antibiotic Prescribing 105 Optimizing Clinical Diagnosis and Antibiotic Prescribing for Common Respiratory Tract Infections, Fanara Family Health
Sameh F. Ahmed, et al Optimizing Clinical Diagnosis and Antibiotic Prescribing 105 Optimizing Clinical Diagnosis and Antibiotic Prescribing for Common Respiratory Tract Infections, Fanara Family Health
Let me clear my throat: empiric antibiotics in
 Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
Volume 1; Number 7 November 2007
 Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Acute Pyelonephritis POAC Guideline
 Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
Outpatient Antimicrobial Therapy. Role of Antibacterials in Outpatient Treatment of Respiratory Tract Infection. Vicks Vapo Rub for Cold Symptoms
 Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy. Role of Antibacterials in Outpatient Treatment of Respiratory Tract Infection. Vicks VapoRub
 Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Community Acquired Pneumonia: An Update on Guidelines
 Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Invasive Group A Streptococcus (GAS)
") Invasive Group A Streptococcus (GAS) Cause caused by a bacterium commonly found on the skin and in the throat transmitted by direct, indirect or droplet contact with secretions from the nose, and throat
Invasive Group A Streptococcus (GAS) Cause caused by a bacterium commonly found on the skin and in the throat transmitted by direct, indirect or droplet contact with secretions from the nose, and throat
Volume. December Infection. Notes. length of. cases as 90% 1 week. tonsillitis. First Line. sore throat / daily for 5 days. quinsy >4000.
 Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
Delayed Prescribing for Minor Infections Resource Pack for Prescribers
 Delayed Prescribing for Minor Infections Resource Pack for Prescribers Background: Antibiotic resistance is an alarming threat to modern healthcare, and infectious illness remains a major global threat
Delayed Prescribing for Minor Infections Resource Pack for Prescribers Background: Antibiotic resistance is an alarming threat to modern healthcare, and infectious illness remains a major global threat
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA Upper Respiratory Infection (URI) GUIDELINE Summaries for Adults and Pediatrics. The guideline was reviewed and adopted by the Molina Healthcare of California Clinical Quality
MOLINA HEALTHCARE OF CALIFORNIA Upper Respiratory Infection (URI) GUIDELINE Summaries for Adults and Pediatrics. The guideline was reviewed and adopted by the Molina Healthcare of California Clinical Quality
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
$100 $200 $300 $400 $500
 Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
3/23/2017. Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc. Kathryn G. Smith: Nothing to disclose
 Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
Volume 2; Number 16 October 2008
 Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Physician Rating: ( 23 Votes ) Rate This Article:
 Rate This Article:") From Medscape Infectious Diseases Conquering Antibiotic Overuse An Expert Interview With the CDC Laura A. Stokowski, RN, MS Authors and Disclosures Posted: 11/30/2010 Physician Rating: ( 23 Votes ) Rate
From Medscape Infectious Diseases Conquering Antibiotic Overuse An Expert Interview With the CDC Laura A. Stokowski, RN, MS Authors and Disclosures Posted: 11/30/2010 Physician Rating: ( 23 Votes ) Rate
Child health. Otitis media in children (acute) Search date January 2007 Clare Bradley-Stevenson, Paddy O'Neill, and Tony Roberts. ...
 Search date January 2007 Clare Bradley-Stevenson, Paddy O'Neill, and Tony Roberts. ...") Search date January 27 Clare Bradley-Stevenson, Paddy O'Neill, and Tony Roberts................................................... ABSTRACT INTRODUCTION: In the UK, about 3% of children under 3 years of
Search date January 27 Clare Bradley-Stevenson, Paddy O'Neill, and Tony Roberts................................................... ABSTRACT INTRODUCTION: In the UK, about 3% of children under 3 years of
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT
 INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
DRAFT DRAFT. Paediatric Antibiotic Prescribing Guideline. May
 Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus
 Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
- Author's note: IAQ's are intended for training purposes and not meant to be required on every call.
 Earache Pediatric After-Hours Version - Standard - 2017 DEFINITION Pain or discomfort in or around the ear Child reports an earache Younger nonverbal child acts like he did with previous ear infection
Earache Pediatric After-Hours Version - Standard - 2017 DEFINITION Pain or discomfort in or around the ear Child reports an earache Younger nonverbal child acts like he did with previous ear infection
Prepared: August Review: July Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide.
 Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
According to a recent National ... PRESENTATION...
 ... PRESENTATION... in Treating Respiratory Tract Infections in an Age of Antibiotic Resistance Miguel Mogyoros, MD Presentation Summary Managing respiratory tract infections (RTIs) presents many challenges
... PRESENTATION... in Treating Respiratory Tract Infections in an Age of Antibiotic Resistance Miguel Mogyoros, MD Presentation Summary Managing respiratory tract infections (RTIs) presents many challenges
Class Update with New Drug Evaluation: Ototopical Antibiotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Breastfeeding Challenges - Mastitis & Breast Abscess -
 CLINICAL PRACTICE GUIDELINE Breastfeeding Challenges - Mastitis & Breast Abscess - SCOPE (Area): Maternity Unit, Emergency Department, Paediatrics SCOPE (Staff): Medical, Midwifery & Nursing DESIRED OUTCOME/OBJECTIVE
CLINICAL PRACTICE GUIDELINE Breastfeeding Challenges - Mastitis & Breast Abscess - SCOPE (Area): Maternity Unit, Emergency Department, Paediatrics SCOPE (Staff): Medical, Midwifery & Nursing DESIRED OUTCOME/OBJECTIVE
Antimicrobial Stewardship in Ambulatory Care
 Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Srirupa Das, Associate Director, Medical Affairs, Tushar Fegade, Manager, Clinical Research Abbott Healthcare Private Limited, Mumbai.
 Indian Medical Gazette JUNE 2015 225 Comparative A Randomized, Open Label, Prospective, Comparative Evaluating the Efficacy and Safety of Fixed Dose Combination of Cefpodoxime 200 Mg + Clavulanic Acid
Indian Medical Gazette JUNE 2015 225 Comparative A Randomized, Open Label, Prospective, Comparative Evaluating the Efficacy and Safety of Fixed Dose Combination of Cefpodoxime 200 Mg + Clavulanic Acid
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Antibiotic treatment and monitoring for suspected or confirmed early-onset neonatal infection bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to
Antibiotic treatment and monitoring for suspected or confirmed early-onset neonatal infection bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to
Outpatient Antimicrobial Therapy. Role of Antibacterials in Outpatient Treatment of Respiratory Tract Infection. Acute Bacterial Rhinosinusitis
 Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
10/9/2017. Evidence-Based Interventions to Reduce Inappropriate Prescription of Antibiotics. Prescribing for Respiratory Tract Infections
 Evidence-Based Interventions to Reduce Inappropriate Prescription of Antibiotics Ann Thomas, MD, MPH Oregon Public Health Division Prescribing for Respiratory Tract Infections Antibiotic use is primary
Evidence-Based Interventions to Reduce Inappropriate Prescription of Antibiotics Ann Thomas, MD, MPH Oregon Public Health Division Prescribing for Respiratory Tract Infections Antibiotic use is primary
Childhood ear infections consist of acute
 An ongoing CE program of The University of Florida College of Pharmacy and DRUG TOPICS The University of Florida College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as
An ongoing CE program of The University of Florida College of Pharmacy and DRUG TOPICS The University of Florida College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as
B. PACKAGE LEAFLET 1
 B. PACKAGE LEAFLET 1 PACKAGE LEAFLET NICILAN 400 mg/100 mg tablets for dogs 1. NAME AND ADDRESS OF THE MARKETING AUTHORISATION HOLDER AND OF THE MANUFACTURING AUTHORISATION HOLDER RESPONSIBLE FOR BATCH
B. PACKAGE LEAFLET 1 PACKAGE LEAFLET NICILAN 400 mg/100 mg tablets for dogs 1. NAME AND ADDRESS OF THE MARKETING AUTHORISATION HOLDER AND OF THE MANUFACTURING AUTHORISATION HOLDER RESPONSIBLE FOR BATCH
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Safety of an Out-Patient Intravenous Antibiotics Programme
 Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
** the doctor start the lecture with revising some information from the last one:
 Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Bacterial Resistance of Respiratory Pathogens. John C. Rotschafer, Pharm.D. University of Minnesota
 Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Antibiotics & treatment of Acute Bcterial Sinusitis. Walid Reda Product Manager. Do your antimicrobial options meet your needs?
 Antibiotics & treatment of Acute Bcterial Sinusitis Walid Reda Product Manager Do your antimicrobial options meet your needs? Antimicrobial Effects: What s involved? Effect in Humans: Serum concentration
Antibiotics & treatment of Acute Bcterial Sinusitis Walid Reda Product Manager Do your antimicrobial options meet your needs? Antimicrobial Effects: What s involved? Effect in Humans: Serum concentration
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
Pharmacology Week 6 ANTIMICROBIAL AGENTS
 Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
The World Health Organization has referred to. Antibiotic Resistance: The Iowa Experience DRUG UTILIZATION. Nancy Bell, RPh
 DRUG UTILIZATION Antibiotic Resistance: The Iowa Experience Nancy Bell, RPh Background: In the past 10 years, the number of strains of Streptococcus pneumoniae and other common respiratory pathogens that
DRUG UTILIZATION Antibiotic Resistance: The Iowa Experience Nancy Bell, RPh Background: In the past 10 years, the number of strains of Streptococcus pneumoniae and other common respiratory pathogens that
A first-line treatment for ear infections in children with ear tubes*
 A first-line treatment for ear infections in children with ear tubes* *Topical antibiotic ear drops are strongly recommended by the AAO-HNSF Clinical Practice Guidelines for tympanostomy tubes in children.1
A first-line treatment for ear infections in children with ear tubes* *Topical antibiotic ear drops are strongly recommended by the AAO-HNSF Clinical Practice Guidelines for tympanostomy tubes in children.1
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
SUMMARY OF PRODUCT CHARACTERISTICS. Bottle of powder: Active substance: ceftiofur sodium mg equivalent to ceftiofur...
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE VETERINARY MEDICINAL PRODUCT WONDERCEF powder and solvent for solution for injection for horses not intended for the production of foods for human consumption.
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE VETERINARY MEDICINAL PRODUCT WONDERCEF powder and solvent for solution for injection for horses not intended for the production of foods for human consumption.
Lyme disease: diagnosis and management
 National Institute for Health and Care Excellence Final Lyme disease: diagnosis and management [D] Evidence review for the management of erythema migrans NICE guideline 95 Evidence review April 2018 Final
National Institute for Health and Care Excellence Final Lyme disease: diagnosis and management [D] Evidence review for the management of erythema migrans NICE guideline 95 Evidence review April 2018 Final
These recommendations were approved for use by the Pharmaceutical and Therapeutics Committee, RCWMCH on 1 February 2017.
 Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
ECHO: Management of URIs. Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018
 ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
Keywords: amoxicillin/clavulanate, respiratory tract infection, antimicrobial resistance, pharmacokinetics/pharmacodynamics, appropriate prescribing
 Journal of Antimicrobial Chemotherapy (2004) 53, Suppl. S1, i3 i20 DOI: 10.1093/jac/dkh050 Augmentin (amoxicillin/clavulanate) in the treatment of community-acquired respiratory tract infection: a review
Journal of Antimicrobial Chemotherapy (2004) 53, Suppl. S1, i3 i20 DOI: 10.1093/jac/dkh050 Augmentin (amoxicillin/clavulanate) in the treatment of community-acquired respiratory tract infection: a review
number Done by Corrected by Doctor Dr.Malik
 number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007
 Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Is amoxicillin good for viral infections
 Is amoxicillin good for viral infections 19-6-2017 Is Amoxicillin Good For Throat Infection. They will not help sore throats caused by allergies or viral infections such as colds amoxicillin is. Reviews
Is amoxicillin good for viral infections 19-6-2017 Is Amoxicillin Good For Throat Infection. They will not help sore throats caused by allergies or viral infections such as colds amoxicillin is. Reviews
Outpatient Antimicrobial Therapy. Role of Antibacterials in Outpatient Treatment of Respiratory Tract Infection. Vicks VapoRub
 Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
مادة االدوية المرحلة الثالثة م. غدير حاتم محمد
 م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antimicrobial susceptibility pattern of clinical isolates from cases of ear infection using amoxicillin and cefepime
 Perveen et al. SpringerPlus 2013, 2:288 a SpringerOpen Journal RESEARCH Antimicrobial susceptibility pattern of clinical isolates from cases of ear infection using amoxicillin and cefepime Shaheen Perveen
Perveen et al. SpringerPlus 2013, 2:288 a SpringerOpen Journal RESEARCH Antimicrobial susceptibility pattern of clinical isolates from cases of ear infection using amoxicillin and cefepime Shaheen Perveen
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
The Turkish Journal of Pediatrics 2008; 50:
 The Turkish Journal of Pediatrics 2008; 50: 120-125 Original Comparison of the effect of benzathine penicillin G, clarithromycin, cefprozil and amoxicillin/clavulanate on the bacteriological response and
The Turkish Journal of Pediatrics 2008; 50: 120-125 Original Comparison of the effect of benzathine penicillin G, clarithromycin, cefprozil and amoxicillin/clavulanate on the bacteriological response and
ESCMID Online Lecture Library. by author
 Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Marc Decramer 3. Respiratory Division, University Hospitals Leuven, Leuven, Belgium
 AAC Accepts, published online ahead of print on April 0 Antimicrob. Agents Chemother. doi:./aac.0001- Copyright 0, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.
AAC Accepts, published online ahead of print on April 0 Antimicrob. Agents Chemother. doi:./aac.0001- Copyright 0, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.
American Association of Feline Practitioners American Animal Hospital Association
 American Association of Feline Practitioners American Animal Hospital Association Basic Guidelines of Judicious Therapeutic Use of Antimicrobials August 1, 2006 Introduction The Basic Guidelines to Judicious
American Association of Feline Practitioners American Animal Hospital Association Basic Guidelines of Judicious Therapeutic Use of Antimicrobials August 1, 2006 Introduction The Basic Guidelines to Judicious
DOSAGE FORMS AND STRENGTHS Otic Suspension: Each OTIPRIO vial contains 1 ml of 6% (60 mg/ml) ciprofloxacin otic suspension. (3)
 ciprofloxacin otic suspension. (3)") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use OTIPRIO safely and effectively. See full prescribing information for OTIPRIO. OTIPRIO (ciprofloxacin
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use OTIPRIO safely and effectively. See full prescribing information for OTIPRIO. OTIPRIO (ciprofloxacin
How Low Can We Go? Readdressing Antibiotic Duration for Common Childhood Infections
 How Low Can We Go? Readdressing Antibiotic Duration for Common Childhood Infections Rebecca Levorson, MD Andrew Nuibe, MD, MSCI Pediatric Infectious Diseases Disclosures Dr. Rebecca Levorson: I have no
How Low Can We Go? Readdressing Antibiotic Duration for Common Childhood Infections Rebecca Levorson, MD Andrew Nuibe, MD, MSCI Pediatric Infectious Diseases Disclosures Dr. Rebecca Levorson: I have no
Women s Antimicrobial Guidelines Summary
 Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
Update on Fluoroquinolones. Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO
 Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Infection Comments First Line Agents Penicillin Allergy History of multiresistant. line treatment: persist for >7 days they may be
 Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
MANAGEMENT OF PELVIC INFLAMMATORY DISEASE
 GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
UTI Dr S Mathijs Department of Pharmacology
 UTI Dr S Mathijs Department of Pharmacology Introduction Responsible for > 7 million consultations annually 15% of all antibiotic prescriptions 40% of all hospital acquired infections Significant burden
UTI Dr S Mathijs Department of Pharmacology Introduction Responsible for > 7 million consultations annually 15% of all antibiotic prescriptions 40% of all hospital acquired infections Significant burden
ANTIBIOTICS. SCHOOL AGE AND ADOLESCENCE Respiratory viruses Respiratory viruses Respiratory viruses Streptococcus pneumoniae
 MARCH 2016 DRUG ANTIBIOTICS This optimal usage guide is mainly intended f primary care health professionnals. It is provided f infmation purposes only and should not replace the clinician s judgement.
MARCH 2016 DRUG ANTIBIOTICS This optimal usage guide is mainly intended f primary care health professionnals. It is provided f infmation purposes only and should not replace the clinician s judgement.