Antimicrobial Use in Clinical Practice
|
|
|
- Meredith Martin
- 5 years ago
- Views:
Transcription

1 Antimicrobial Use in Clinical Practice Dr. Andrew M. Morris Mt. Sinai Hospital/University Health Network Department of Medicine
2 Introductory tips don t learn too many individual antibiotics no doctor should know more than about a dozen antibiotics try to understand principles rather than specifics, and don t bother learning dosages Dr. Vellend covered many of the basic principles surrounding antimicrobial use... any repetition is deliberate (to aid in recollection)

3 An example of an antimicrobial repertoire amoxicillin/ ampicillin cloxacillin piperacillintazobactam cephalexin/ cefazolin cefotaxime or ceftriaxone azithromycin or clarithromycin clindamycin metronidazole ciprofloxacin levofloxacin or moxifloxacin trimethoprim-sulfamethoxazole gentamicin vancomycin
4 Antimicrobial rules to live by treat the patient, not the lab report don t take credit for curing a self-limited disease with antibiotics don t use broad-spectrum, risky, expensive or new antibiotics for treating mild/minor infections don t treat a fever with antibiotics don t stick with a losing combination i.v. antibiotics should be avoided the best antibiotics are made of steel when the stakes are high, don t be a minimalist
5 Case 1 45 yo woman, previously well works as a pharmaceutical rep; triathlete allergic to penicillin (hives) because of genetic screening, had bilateral prophylactic mastectomies (with plan for tissue expander breast implants) post-operatively, wound healed well: a drain was left in situ (for a seroma), and the clinic nurse sent the fluid for Gram stain and culture prior to removing the drain

6 Case 1
7 Case 1 Date: (14:09) Patient: Merrick, Linda H. ( ) Requesting MD: Singh, P.J. Specimen: Surgical wound (collected ) Gram: No pus cells. Many gram positive cocci, few gram positive bacilli Culture: Isolate 01 Staphylococcus aureus, heavy growth amoxicillin R ciprofloxacin S cefazolin S clindamycin S cloxacillin S cotrimoxazole S tetracycline S vancomycin S
8 Case 1 What antibiotic should you start? What class? What route? How would you monitor response to therapy?
9 Rule #1 Treat the patient, not the lab report
10 Case 2 15m old toddler, male first-born child to social worker and primary school teacher previously healthy, appropriate achievement of ages/stages/ milestones has had fever, irritability, and decreased food intake for >24 hours parents say that the only thing that helps is Tylenol

11 Case 2 physical exam is noteworthy for a healthy-looking child who is crying, febrile (38.1 ), with a dull right tympanic membrane Dx: acute otitis media
12 Case 2 Should you start an antibiotic?

13 Antibiotics and acute otitis media (AOM) whether or not to give antibiotics for AOM is controversial (meaning we don t yet have a clear answer ) practice guidelines around the world vary regarding antimicrobial approach to AOM in Ontario, the Guidelines Advisory Committee recommends ABx for any symptomatic episode of AOM in the Netherlands, guidelines recommend, initially, analgesics alone for symptomatic AOM in children over 6 months of age
14 Estimated antibiotic prescriptions dispensed by 2,000,000 month in Canadian retail pharmacy 1,600,000 1,200, , ,000 0 Jan03 Feb03 Mar03 Apr03 May03 Jun03 Jul03 Aug03 Sep03 Oct03 Nov03 Dec03 p.o. solids p.o. liquids ( kids) Jan04 Feb04 Mar04 Apr04 May04 Jun04 Jul04 Aug04 Sep04 Oct04 Nov04 Dec04 Jan05


15 Antibiotic consumption correlates with resistance Total consumption of macrolide antibiotics by outpatients in Finland from Frequency of resistance to erythromycin among Group A Strep isolates from throatswab and pus samples in Finland in 1990 and NEJM 1997;337:441-6
 of antibiotics or a standard antibiotic prescription 100% 80% 60% 40% 20% 0% Script filled Fever Ear pain Diarrhea JAMA")
16 Wait-and-see prescription vs Up-front Abx for AOM one study WASP Standard ABx Prescription randomized 283 kids (age 6m-12y) to either a waitand-see prescription (WASP) of antibiotics or a standard antibiotic prescription 100% 80% 60% 40% 20% 0% Script filled Fever Ear pain Diarrhea JAMA 2006;296:
17 Rule #2 Don t take credit for curing a self-limited disease with antibiotics
 endocarditis prophylaxis prior to dental procedures")
18 Other examples of diseases where utility of ABx is questionable sinusitis acute exacerbations of COPD boils (following incision and drainage) endocarditis prophylaxis prior to dental procedures
19 Case 3 57 yo F, store manager history of obesity, diet- and exercisecontrolled DM Type 2, hyperlipidemia, hypertension and hypothyroidism presents to family physician with fever, cough, sputum production, and some mild pleuritic chest pain for 2d
20 Case 3 physical exam noteworthy for: looks generally well (i.e. not in extremis) T 38.6, RR 20, BP 126/78, HR 99 oropharynx clear normal fremitus and percussion, with crackles heard over left lower lung field remainder of exam normal/ unremarkable

21 Case 3
22 Case 3 Diagnosis: Community-acquired pneumonia Should patient be managed as an outpatient or sent to ER? What antibiotic(s) should be used to treat her?
23 Community-acquired pneumonia there are 2 algorithms that are recommended to predict severity of CAP: CURB-65 and Pneumonia Severity Index (PSI) using either of these algorithms, this patient is low risk
24 CURB-65 CURB-65 (Confusion, Urea > 7, RR > 30, BP < 90mmHg systolic or 60mmHg diastolic, age > 65) easy, fast relies on mostly clinical factors... but is unreliable to guide site of care Am J Med 2005;118: Eur Respir J 2006;27:
25 CURB-65 CURB day mortality: 0 0.7% 1 2.1% 2 9.2% % % %

26 PSI stratifies patients into 5 groups a collection of 20 variables, predominantly historical derived from 1 cohort and validated with another cohort uptake has been rather low, but PSI calculators are readily available (e.g. NEJM 1997;336:243-50

27 What antibiotics to use for outpatient CAP the Brits recommend penicillins the Aussies recommend penicillins or doxycycline for low-risk in N. America, macrolide or doxycycline are recommended for very low risk, but with underlying co-morbidities (e.g. heart, lung or renal disease, DM, alcoholism, etc.) a respiratory fluoroquinolone OR a β-lactam + macrolide are recommended

28 Outpatient CAP controversy exists over what is the best choice because: microbiology would suggest covering atypical bacteria (e.g. Legionella, Mycoplasma, and Chlamydophila) is necessary resistance patterns suggest that macrolides are not a great choice cost considerations are a matter of perspective


29 Covering atypical bacteria doesn t seem to matter Number of patients failing to achieve clinical cure or improvement with β lactam antibiotics compared with antibiotics active against atypical pathogens in all cause non-severe community acquired pneumonia BMJ 2005;330:456-62
 azithromycin 500 mg then 250 daily = $22 (generic) clarithromycin 500mg bid = $26 levofloxacin 500mg daily = $28 moxifloxacin 400mg daily = $34 amoxicillin-clav 2g bid = $44")
30 Newer antibiotics are usually more expensive Approximate cost for 5 days treatment: amoxicillin 1g q8h = $10 (generic) doxycycline 100mg bid = $12 (generic) cefuroxime 500mg bid = $20 (generic) azithromycin 500 mg then 250 daily = $22 (generic) clarithromycin 500mg bid = $26 levofloxacin 500mg daily = $28 moxifloxacin 400mg daily = $34 amoxicillin-clav 2g bid = $44

31 New antibiotics might carry a safety risk grepafloxacin removed in 1999 due to safety concerns regarding fatal cardiac arrhythmias sparfloxacin removed in 2001 due to phototoxicity trovafloxacin removed in 2001 due to hepatotoxicity gatifloxacin removed in 2006 due to dysglycaemia gemifloxacin causes rash in 32% of women <40 yrs telithromycin carries a black box warning regarding hepatotoxicity
32 Case 3 Dx: outpatient community-acquired pneumonia amoxicillin or another oral β-lactam (e.g. cephalosporin) seems reasonable guidelines would also support broader coverage (e.g. doxycycline, macrolides + β-lactam, or respiratory fluoroquinolones) but does the patient s CAP risk justify broader/ newer coverage?
33 Rule #3 Don t use broad-spectrum, dangerous, expensive or new antibiotics for treating mild/minor infections

34 Case 4 50 yo M, truck driver currently on disability benefits history of hypertension, hyperlipidemia, smoking (50 pack-years), obesity, asthma and osteoarthritis presents to ER with fever, cough, retrosternal chest pain and SOB x 4 days physical exam largely unremarkable, although looks unwell, has RR/ HR, 38.1 and requires supplemental oxygen
35 Case 4 chest x-ray unremarkable (apart from some evidence of emphysema) CBC: Hb 125 g/l (slightly low), WBC 19.7 x 10 6 /L (high) with neutrophilia, platelets 510 x 10 9 /L (slightly high) chemistry normal urinalysis normal ECG: sinus tachycardia
36 Case 4 Dx: community-acquired pneumonia started on levofloxacin 750mg daily given enoxaparin for DVT prophylaxis after 24hrs afebrile, albeit remains tachycardic and tachypneic--doesn t feel better repeat CXR reported as normal discharged home on levofloxacin 750mg daily, but returns to ER within 8hrs with worsening SOB
37 Case 4 What antibiotics?
38 Case 4 patient was seen by ER doc, who prescribed amoxicillin-clavulanic acid, and was discharged from ER patient went to pharmacy to fill prescription, but suffered a cardiac arrest and died at the pharmacy coroner notified, who ordered an autopsy
39 Case 4 Diagnosis at autopsy: massive pulmonary embolism
40 Rule #4 Don t treat a fever with antibiotics
41 Case 5 66-year-old woman admitted for CAP history of COPD, penicillin allergy and chronic lymphocytic leukemia (not currently requiring Rx) had received a 10d course of ciprofloxacin 6 months earlier and a 10d course of levofloxacin 1 month previously, both for the treatment of an acute exacerbation of COPD
42 Case 5 2 wks before admission, URTI developed. 8d before admission, ciprofloxacin was begun because of respiratory symptoms at admission, her clinical condition had deteriorated, and she was found to have a RLL/RML infiltrate and a small rightsided pleural effusion blood cultures grew S. pneumoniae Rx was switched oral levofloxacin daily
43 Case 5 pleural fluid cultures on the fourth hospital day grew S. pneumoniae. on 5th hospital day, septic shock developed and patient died the following day eventually, testing was performed which demonstrated fluoroquinolone-resistant S. pneumoniae NEJM 2002;346:747-50
44 Case 5 post-mortem testing was performed on the blood and pleural fluid isolates which demonstrated fluoroquinolone-resistant S. pneumoniae NEJM 2002;346:747-50
45 Rule #5 Don t stick with a losing combination
46 Case 6 12 year-old F, at camp, with insect bite to arm subsequent erythema, swelling, warmth and pain surrounding insect bite over course of hours afebrile, stable, feels otherwise well advised by camp MD to go to ER

47 Case 6 WBC 13.5 x 10 6 /L remainder of bloodwork normal started on i.v. cefazolin for 14d for cellulitis... and camp fun was ruined
48 Cellulitis ~ 80% of cellulitis is caused by Group A Streptococcus (most of remainder caused by methicillin-sensitive S. aureus) there is no penicillin-resistant Group A Strep patients rarely get very sick with cellulitis 5 days levofloxacin is as good as 10 days

49 Cellulitis e disease is self-limited and a large majority of the cases get well without any internal medication. I can speak definitely on this point, having, at the Philadelphia Hospital, treated many cases in this way. William Osler, M.D. e Principles and Practice of Medicine: Designed for the use of practitioners and students of medicine. New York, Appleton and Company. 1893

50 Rule #6 i.v. antibiotics should be avoided and remember Rule #2: don t take credit for curing a self-limited disease with antibiotics (although almost all MDs would treat cellulitis with antibiotics)
51 Case 7 39 yo M undergoing radiation therapy for intra-abdominal lymphoma currently on prednisone 20mg daily no prior antimicrobial therapy presented to ER in septic shock, with BP 65/pulse, HR 140, RR 40, T 38.7 oxygen saturation on 100% O 2 by noninvasive positive-pressure ventilation chest x-ray: diffuse white out abdomen rigid... CT abdomen pending
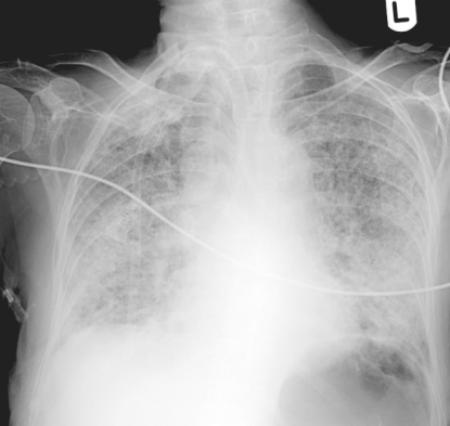
52 Case 7
53 Case 7 Dx: Peritonitis antibiotics? Which ones? what else?
. http://radiographics.rsnajnls.")
54 Case 7 Perforated appendix with peritonitis. Axial contrastenhanced CT scan shows enhancement and disruption (arrow) of the appendiceal wall. Inflamed bowel wall and severe fat stranding are also present (arrowheads).
55 Peritonitis in an antibiotic-naive patient patient needs surgery +/- drains
56 Peritonitis in an antibiotic-naive patient need to treat gut organisms (gramnegative aerobes and anaerobes, predominantly) many MDs will also want to cover Gram-positives, although probably unnecessary many regimens available
 pip-tazo OR meropenem OR")
57 Peritonitis in an antibiotic-naive patient amp&gent OR cefotaxime/ceftriaxone OR ciprofloxacin/levofloxacin + metronidazole (OR clindamycin) pip-tazo OR meropenem OR moxifloxacin
58 Rule #7 The best antibiotics are made of steel Rule #8 When the stakes are high, don t be a minimalist
59 Antimicrobial rules to live by treat the patient, not the lab report don t take credit for curing a self-limited disease with antibiotics don t use broad-spectrum, risky, expensive or new antibiotics for treating mild/minor infections don t treat a fever with antibiotics don t stick with a losing combination i.v. antibiotics should be avoided the best antibiotics are made of steel when the stakes are high, don t be a minimalist
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Lifting the lid off CAP guidelines
 Lifting the lid off CAP guidelines Dr. Andrew M. Morris September 5, 2007 12:00-13:00 web.mac.com/idologist Objectives 1. To review the epidemiology of community-acquired pneumonia (CAP) 2. To explore
Lifting the lid off CAP guidelines Dr. Andrew M. Morris September 5, 2007 12:00-13:00 web.mac.com/idologist Objectives 1. To review the epidemiology of community-acquired pneumonia (CAP) 2. To explore
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
CLINICAL PROTOCOL FOR COMMUNITY ACQUIRED PNEUMONIA. SCOPE: Western Australia. CORB score equal or above 1. All criteria must be met:
 CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC
 Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Antibiotics & Common Infections: Stewardship, Effectiveness, Safety & Clinical Pearls. Welcome We will begin shortly.
 Antibiotics & Common Infections: Stewardship, Effectiveness, Safety & Clinical Pearls Welcome We will begin shortly. The Canadian Pharmacists Association is pleased to be collaborating with the following
Antibiotics & Common Infections: Stewardship, Effectiveness, Safety & Clinical Pearls Welcome We will begin shortly. The Canadian Pharmacists Association is pleased to be collaborating with the following
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance
 Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Cellulitis. Assoc Prof Mark Thomas. Conference for General Practice Auckland Saturday 28 July 2018
 Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
21 st Expert Committee on Selection and Use of Essential Medicines Peer Review Report Antibiotics Review
 (1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
(1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani
 Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children
 Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship
 Curriculum for Antimicrobial Stewardship") General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
National Clinical Guideline Centre Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults
 National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Community Acquired Pneumonia: An Update on Guidelines
 Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
$100 $200 $300 $400 $500
 Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Community-Acquired Pneumonia. Community-Acquired Pneumonia. Community Acquired Pneumonia (CAP): definition
: definition") Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Community-Acquired Pneumonia Talk will focus on adults Guideline for healthy infants
Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Community-Acquired Pneumonia Talk will focus on adults Guideline for healthy infants
Measure Information Form
 Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Pneumonia. Community Acquired Pneumonia (CAP): definition. At least 2 new symptoms
: definition. At least 2 new symptoms") Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Community Acquired Pneumonia (CAP): definition At least 2 new symptoms Fever or hypothermia Cough Rigors
Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Community Acquired Pneumonia (CAP): definition At least 2 new symptoms Fever or hypothermia Cough Rigors
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Antimicrobial Stewardship in Ambulatory Care
 Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Control emergence of drug-resistant. Reduce costs
 ...PRESENTATIONS... Guidelines for the Management of Community-Acquired Pneumonia Richard E. Chaisson, MD Presentation Summary Guidelines for the treatment of community-acquired pneumonia (CAP) have been
...PRESENTATIONS... Guidelines for the Management of Community-Acquired Pneumonia Richard E. Chaisson, MD Presentation Summary Guidelines for the treatment of community-acquired pneumonia (CAP) have been
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Safety of an Out-Patient Intravenous Antibiotics Programme
 Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Aminoglycosides. Spectrum includes many aerobic Gram-negative and some Gram-positive bacteria.
 Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
M5 MEQs 2016 Session 3: SOB 18/11/16
 M5 MEQs 2016 Session 3: SOB 18/11/16 http://tinyurl.com/hn7qzt3 Question 1 Ms Tan is a 52 year old female with no past medical history. She comes to the emergency department presenting with a fever for
M5 MEQs 2016 Session 3: SOB 18/11/16 http://tinyurl.com/hn7qzt3 Question 1 Ms Tan is a 52 year old female with no past medical history. She comes to the emergency department presenting with a fever for
ECHO: Management of URIs. Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018
 ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
Antibiotics in the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease
 Antibiotics in the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease Sung Kyu Kim, M.D.Young Sam Kim, M.D. Department of Internal Medicine Yonsei University College of Medicine,
Antibiotics in the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease Sung Kyu Kim, M.D.Young Sam Kim, M.D. Department of Internal Medicine Yonsei University College of Medicine,
Pinni Meedha Mojutho Ammanu Dengina Koduku Part 1 Kama Kathalu
 Search for: Search Search Does levaquin cover anaerobes Pinni Meedha Mojutho Ammanu Dengina Koduku Part 1 Kama Kathalu Levofloxacin, sold under the trade names Levaquin among others, is an antibiotic.
Search for: Search Search Does levaquin cover anaerobes Pinni Meedha Mojutho Ammanu Dengina Koduku Part 1 Kama Kathalu Levofloxacin, sold under the trade names Levaquin among others, is an antibiotic.
2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING TOTAL HIP AND KNEE ARTHROPLASTY
 Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING TOTAL HIP AND KNEE ARTHROPLASTY FINAL Working Group: E. Henderson, M. John, I. Davis, S. Dunford,
Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING TOTAL HIP AND KNEE ARTHROPLASTY FINAL Working Group: E. Henderson, M. John, I. Davis, S. Dunford,
Presenter: Marc Meyer, BPharm, RPh, CIC, FAPIC Clinical Pharmacists, Infection Preventionist, Antibiotic Stewardship Pharmacist Southwest Health
 Presenter: Marc Meyer, BPharm, RPh, CIC, FAPIC Clinical Pharmacists, Infection Preventionist, Antibiotic Stewardship Pharmacist Southwest Health System, Cortez, Colorado None How do AU vendors and NHSN
Presenter: Marc Meyer, BPharm, RPh, CIC, FAPIC Clinical Pharmacists, Infection Preventionist, Antibiotic Stewardship Pharmacist Southwest Health System, Cortez, Colorado None How do AU vendors and NHSN
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Clinical Practice Standard
 Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
National Antimicrobial Prescribing Survey
 Indication documented Surgical prophylaxis >24 hrs Allergy mismatch Microbiology mismatch Incorrect route Incorrect dose/frequency Incorrect duration Therapeutic Guidelines Local guidelines * Non-compliant
Indication documented Surgical prophylaxis >24 hrs Allergy mismatch Microbiology mismatch Incorrect route Incorrect dose/frequency Incorrect duration Therapeutic Guidelines Local guidelines * Non-compliant
Objectives. Review basic categories of intra-abdominal infection and their respective treatments. Community acquired intra-abdominal infection
 Objectives Review basic categories of intra-abdominal infection and their respective treatments Community acquired intra-abdominal infection Mild/Moderate Severe Acute biliary tract infections Nosocomial
Objectives Review basic categories of intra-abdominal infection and their respective treatments Community acquired intra-abdominal infection Mild/Moderate Severe Acute biliary tract infections Nosocomial
Community Acquired Pneumonia. Epidemiology: Acute Lower Respiratory Tract Infections. Community Acquired Pneumonia (CAP) Outline
 Outline") Community Acquired Pneumonia (CAP) Outline Lisa G. Winston, MD University of California, San Francisco Zuckerberg San Francisco General Epidemiology Diagnosis Microbiology Risk stratification Treatment
Community Acquired Pneumonia (CAP) Outline Lisa G. Winston, MD University of California, San Francisco Zuckerberg San Francisco General Epidemiology Diagnosis Microbiology Risk stratification Treatment
Volume. December Infection. Notes. length of. cases as 90% 1 week. tonsillitis. First Line. sore throat / daily for 5 days. quinsy >4000.
 Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
Antibiotic Stewardship at MetroWest Medical Center. Colleen Grocer, RPh, BCOP Co-Chair, Antibiotic Stewardship Committee
 Antibiotic Stewardship at MetroWest Medical Center Colleen Grocer, RPh, BCOP Co-Chair, Antibiotic Stewardship Committee Antibiotic Stewardship Committee Subcommittee of Pharmacy and Therapeutics. Also
Antibiotic Stewardship at MetroWest Medical Center Colleen Grocer, RPh, BCOP Co-Chair, Antibiotic Stewardship Committee Antibiotic Stewardship Committee Subcommittee of Pharmacy and Therapeutics. Also
Infectious Disease Update 2017
 Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering
 SMC No. (650/10) Bayer Schering") moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
Volume 2; Number 16 October 2008
 Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Outpatient Antimicrobial Therapy. Role of Antibacterials in Outpatient Treatment of Respiratory Tract Infection. Vicks Vapo Rub for Cold Symptoms
 Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy. Role of Antibacterials in Outpatient Treatment of Respiratory Tract Infection. Vicks VapoRub
 Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings?
 An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Can you treat mrsa with amoxicillin
 Can you treat mrsa with amoxicillin 15-8-2017 Community-associated MRSA You can pick up MRSA outside the hospital, especially if you :. (a related drug developed to treat these germs). Amoxicillin and
Can you treat mrsa with amoxicillin 15-8-2017 Community-associated MRSA You can pick up MRSA outside the hospital, especially if you :. (a related drug developed to treat these germs). Amoxicillin and
Outpatient Antimicrobial Therapy. Role of Antibacterials in Outpatient Treatment of Respiratory Tract Infection. Acute Bacterial Rhinosinusitis
 Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Community-acquired pneumonia: Time to place a CAP on length of treatment?
 LOGIN TO LEARN: An Engaging and Interactive Journal Club for Pharmacists and Students Community-acquired pneumonia: Time to place a CAP on length of treatment? Jennifer Ball, PharmD Learning Objectives
LOGIN TO LEARN: An Engaging and Interactive Journal Club for Pharmacists and Students Community-acquired pneumonia: Time to place a CAP on length of treatment? Jennifer Ball, PharmD Learning Objectives
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT
 INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
OBSTETRICS & GYNAECOLOGY. Penicillin G 5 million units IV ; followed by 2.5 million units 4hourly upto delivery
 OBSTETRICS & GYNAECOLOGY A.OBSTETRICS Infection/Condition/likely organism Intrapartum Group B Streptococcal (GBS) infection; positive mothers Suggested treatment Preferred Penicillin G 5 million units
OBSTETRICS & GYNAECOLOGY A.OBSTETRICS Infection/Condition/likely organism Intrapartum Group B Streptococcal (GBS) infection; positive mothers Suggested treatment Preferred Penicillin G 5 million units
Antibiotics in the trenches: An ER Doc s Perspective
 Antibiotics in the trenches: An ER Doc s Perspective Peter Currie, MD Medical Director for Quality Emergency Physicians Professional Association (EPPA) Agenda Emergency Medicine Specific Disease Processes
Antibiotics in the trenches: An ER Doc s Perspective Peter Currie, MD Medical Director for Quality Emergency Physicians Professional Association (EPPA) Agenda Emergency Medicine Specific Disease Processes
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections
 Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Volume 1; Number 7 November 2007
 Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Update on Fluoroquinolones. Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO
 Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Choosing the Best Antibiotic in Problem Outpatient Infectious Disease Cases
 Choosing the Best Antibiotic in Problem Outpatient Infectious Disease Cases Dr. Earl Rubin Associate Professor Department of Pediatrics Division of Infectious Diseases Montreal Children s Hospital Disclosures
Choosing the Best Antibiotic in Problem Outpatient Infectious Disease Cases Dr. Earl Rubin Associate Professor Department of Pediatrics Division of Infectious Diseases Montreal Children s Hospital Disclosures
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings. Carlos Reyes Sacin, MD, AAHIVS
 Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
THERAPY OF ANAEROBIC INFECTIONS LUNG ABSCESS BRAIN ABSCESS
 THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
Community-Acquired Pneumonia Current & Future State
 Community-Acquired Pneumonia Current & Future State Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial relationships to
Community-Acquired Pneumonia Current & Future State Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial relationships to
3/23/2017. Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc. Kathryn G. Smith: Nothing to disclose
 Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
3/1/2016. Antibiotics --When Less is More. Most Urgent Threats. Serious Threats
 Antibiotics --When Less is More Ralph Gonzales, MD, MSPH Associate Dean, Clinical Innovation School of Medicine VP, Clinical Innovation, UCSF Health Most Urgent Threats Serious Threats Multidrug-Resistant
Antibiotics --When Less is More Ralph Gonzales, MD, MSPH Associate Dean, Clinical Innovation School of Medicine VP, Clinical Innovation, UCSF Health Most Urgent Threats Serious Threats Multidrug-Resistant
Mrsa abscess and cellulitis
 Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
Doxycycline for strep pneumonia
 Doxycycline for strep pneumonia Antibiotic Levofloxacin (Levaquin) 750 mg, 500 mg for the treatment of respiratory, skin, and urinary tract infections, user reviews and ratings. 14-12-1995 John G. Bartlett,
Doxycycline for strep pneumonia Antibiotic Levofloxacin (Levaquin) 750 mg, 500 mg for the treatment of respiratory, skin, and urinary tract infections, user reviews and ratings. 14-12-1995 John G. Bartlett,
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017
 Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
Infection Comments First Line Agents Penicillin Allergy History of multiresistant. line treatment: persist for >7 days they may be
 Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
Prepared: August Review: July Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide.
 Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements
 Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
Women s Antimicrobial Guidelines Summary
 Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
10/9/2017. Evidence-Based Interventions to Reduce Inappropriate Prescription of Antibiotics. Prescribing for Respiratory Tract Infections
 Evidence-Based Interventions to Reduce Inappropriate Prescription of Antibiotics Ann Thomas, MD, MPH Oregon Public Health Division Prescribing for Respiratory Tract Infections Antibiotic use is primary
Evidence-Based Interventions to Reduce Inappropriate Prescription of Antibiotics Ann Thomas, MD, MPH Oregon Public Health Division Prescribing for Respiratory Tract Infections Antibiotic use is primary
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING HIP AND KNEE ARTHROPLASTY
 Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING HIP AND KNEE ARTHROPLASTY FINAL Working Group: Dominik Mertz (Chair) Elizabeth Henderson, Johan
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING HIP AND KNEE ARTHROPLASTY FINAL Working Group: Dominik Mertz (Chair) Elizabeth Henderson, Johan
Bai-Yi Chen MD. FCCP
 Treatment strategies for hospitalized versus nonhospitalized CAP patients: Asian perspective Bai-Yi Chen MD. FCCP Professor of Medicine Division of Infectious Disease, Infection Control Team The First
Treatment strategies for hospitalized versus nonhospitalized CAP patients: Asian perspective Bai-Yi Chen MD. FCCP Professor of Medicine Division of Infectious Disease, Infection Control Team The First
PHAMACOLOGY 2 nd EXAM QUESTIONS 2012/2013
 PHAMACOLOGY 2 nd EXAM QUESTIONS 2012/2013 1.from the pharmacological point of view, which of the following intervention is correct? a) treating postpartum non-obstructive urinary retention by intramuscular
PHAMACOLOGY 2 nd EXAM QUESTIONS 2012/2013 1.from the pharmacological point of view, which of the following intervention is correct? a) treating postpartum non-obstructive urinary retention by intramuscular
What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa.
 Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
SECTION 3A. Section 3A Criteria for Optional Special Authorization of Select Drug Products
 SECTION 3A Criteria for Optional Special Authorization of Select Drug Products Section 3A Criteria for Optional Special Authorization of Select Drug Products CRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION
SECTION 3A Criteria for Optional Special Authorization of Select Drug Products Section 3A Criteria for Optional Special Authorization of Select Drug Products CRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION
Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550
 and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550") Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550 Sinusitis Upper respiratory tract infections (URI) Common cold
Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550 Sinusitis Upper respiratory tract infections (URI) Common cold
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES
 AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Can levaquin treat group b strep
 Can levaquin treat group b strep The Borg System is 100 % Can levaquin treat group b strep IBS - Symptoms, Diet and Treatment. IBS, is the common slang term or abbreviation for Irritable Bowel Syndrome
Can levaquin treat group b strep The Borg System is 100 % Can levaquin treat group b strep IBS - Symptoms, Diet and Treatment. IBS, is the common slang term or abbreviation for Irritable Bowel Syndrome
Pharmacology Week 6 ANTIMICROBIAL AGENTS
 Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
The Perils of Mixing Warfarin & Antibiotics: A Potentially Deadly Combination
 The Perils of Mixing Warfarin & Antibiotics: A Potentially Deadly Combination Lynn McNicoll, MD, FRCPC, AGSF Associate Professor of Medicine, Department of Medicine Warren Alpert Medical School of Brown
The Perils of Mixing Warfarin & Antibiotics: A Potentially Deadly Combination Lynn McNicoll, MD, FRCPC, AGSF Associate Professor of Medicine, Department of Medicine Warren Alpert Medical School of Brown
your hospitals, your health, our priority PARC (Policy Approval and Ratification Committee) STANDARD OPERATING PROCEDURE:
 STANDARD OPERATING PROCEDURE:") STANDARD OPERATING PROCEDURE: TRUST ANTIBIOTIC TREATMENT SOP SOP NO: TW10/136 SOP 1 VERSION NO: VERSION 6.1 (JANUARY 2013) APPROVING COMMITTEE: INFECTION PREVENTION AND CONTROL COMMITTEE DATE THIS VERSION
STANDARD OPERATING PROCEDURE: TRUST ANTIBIOTIC TREATMENT SOP SOP NO: TW10/136 SOP 1 VERSION NO: VERSION 6.1 (JANUARY 2013) APPROVING COMMITTEE: INFECTION PREVENTION AND CONTROL COMMITTEE DATE THIS VERSION
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department