Antibiotic Management of Prosthetic Joint Infections
|
|
|
- Suzan Strickland
- 6 years ago
- Views:
Transcription

1 Antibiotic Management of Prosthetic Joint Infections R Andrew Seaton Consultant Infectious Diseases and General Medicine NHS Greater Glasgow and Clyde
2 Declarations of interest Consultancy Novartis Pfizer Astrazeneca Astellas Cubist Research funding Novartis
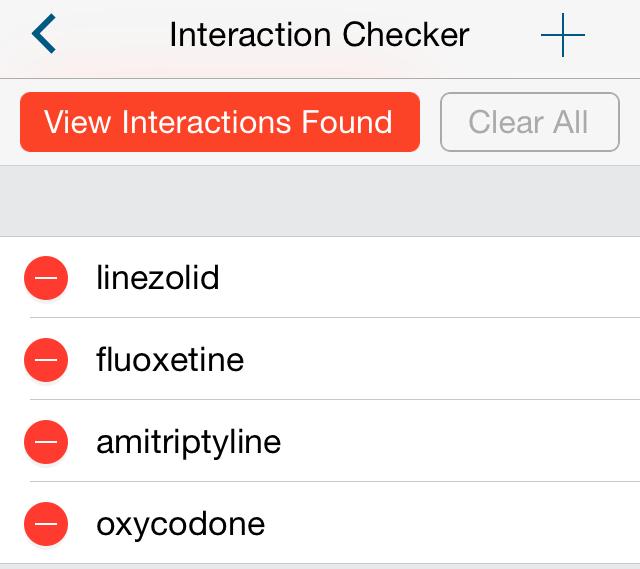
3 55 year old male, December 2014 Sepsis + R Hip pain Background COPD Depression Recent nasal polypectomy LTHR 2004, RTHR 2009 (complicated) Medication Oxycodone, Fluoxetine, Amitriptyline, Diazepam
4 Orthopaedic History (1) 23/11/09 RTHR 10/12/09 One Stage Rev 19/04/10 1 st Stage Rev 21/06/10 2 nd Stage Rev 23/07/12 1 st Stage Rev 17/09/12 2 nd Stage Rev Gp G Strep BCs + intra-op NG NG CNS 4/7 CNS 1/7 IV Ceftriaxone (OPAT) Then PO Amox 3 months
5 Orthopaedic History (2) 23/11/09 RTHR 10/12/09 One Stage Rev 19/04/10 1 st Stage Rev 21/06/10 2 nd Stage Rev 23/07/12 1 st Stage Rev 17/09/12 2 nd Stage Rev Gp G Strep BCs + intra-op NG NG CNS 4/7 CNS 1/7 IV Ceftriaxone (OPAT) Then PO Amox 3 months IV Cef + Rif (OPAT) 6 weeks IV Teicoplanin (OPAT) 6 weeks
6 Orthopaedic History (3) 23/11/09 RTHR 10/12/09 One Stage Rev 19/04/10 1 st Stage Rev 21/06/10 2 nd Stage Rev 23/07/12 1 st Stage Rev 17/09/12 2 nd Stage Rev Gp G Strep BCs + intra-op NG NG CNS 4/7 CNS 1/7 IV Ceftriaxone (OPAT) Then PO Amox 3 months IV Cef + Rif (OPAT) 6 weeks IV Teicoplanin (OPAT) 6 weeks
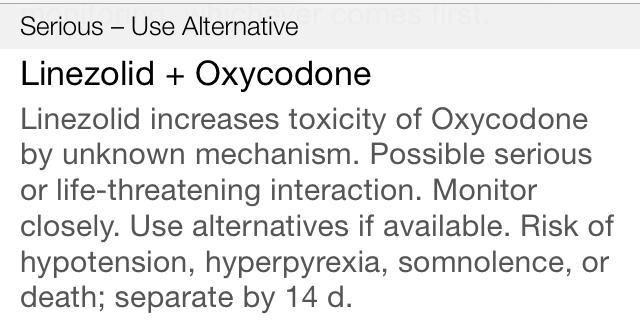
7 1 st Stage Rev 26/01/15 GBS (7 samples) (5 th THR) Sensitive: Penicillin, Vancomycin, Ceftriaxone, Linezolid Resistant: Doxycycline, Clindamycin, Levofloxacin Antibiotic Rx?
8 Antibiotic considerations Activity vs organism Penetration to site of infection (Activity in biofilm) Drug-Drug-Host interactions Side effects IV or oral Length of Rx Synergy
9 1 st Stage Rev 26/01/15 GBS (7 samples) (5 th THR) Sensitive: Penicillin, Vancomycin, Ceftriaxone, Linezolid Resistant: Doxycycline, Clindamycin, Levofloxacin Antibiotic Rx? Oxycodone Fluoxetine Amitriptyline Diazepam
10
11 Before Treatment: Prevention Patient factors: age, obesity, co-morbidity (DM) Asepsis, theatre airflow, maintain normothermia MSSA decolonisation Antibiotic prophylaxis: up to 24 hours (Norwegian arthroplasty study) UK favours single dose Choice: Fluclox + Gent associated with increase in risk of AKI (reversible), Cefuroxime: CDI risk Antibiotic-impregnated cement: Gent, Clinda, Vanc Negative pressure: Jubilee dressing Hand hygiene, ward environment, Pt education
12 Espehaug et al
13 Accepted wisdom? Osteomyelitis is rarely controlled without the combination of careful, complete surgical debridement and prolonged parenteral antibiotic therapy at high dosage Waldvogel et al N Engl J Med. 1970;282:316-22
14 Surgical approach Debridement of bone, Removal of polyethylene and metal work Antibiotic-impregnated spacers: Gentamicin, Vancomycin Retention of metal work only if Acute infection very recent implant i.e. before formation of biofilm Inoperable
15 Aim of Surgery: cure or suppress infection and maintain function Prosthetic Joint Infection 2 Stage Revision I Stage Revision Debridement and Retention Excision arthroplasty Amputation If >30 days post implant or >3 weeks of symptoms CURE If <30 days post implant or < 3 weeks of symptoms OR Revision not possible CURE or SUPRESS Bone stock, AMR, (Multiple) failed revisions Specialist orthopaedic decision CURE Osman et al CID 2013; 56: 1
16 Aim of antibiotic therapy To deliver an optimum concentration of antibiotic to which the organism is sensitive, direct to the site of infection to effect a cure To augment/ support (but not replace) the surgical approach For agents with time dependent characteristics, concentration must remain above the MIC of the organism for the maximum duration of the dosing interval
17 Route of administration in PJI Topical: Beads/ cement (primary or adjunct Rx) Intra-articular: infusion Oral Intravenous (+/- Oral, +/- Topical) Intramuscular
 Poor vascularity Uninfected/ uninflammed Presence of biofilm")
18 Factors affecting antibiotic bone penetration Reduced penetration if: Low concentration of drug at site of infection Cortical bone (c.f. cancellous) Poor vascularity Uninfected/ uninflammed Presence of biofilm
19 Free drug concentration correlates with concentration in bone (in ᵝ-lactams) Scaglioni et al AAC 1997; 41: 2292
20 PK / PD Principles IV delivered ᵝ-lactam
21 PK / PD Principles IV delivered ᵝ-lactam PO delivered ᵝ-lactam
22 PK / PD Principles IV delivered ᵝ-lactam IV delivered ᵝ-lactam Free concentration PO delivered ᵝ- lactam
23 PK / PD Principles IV delivered ᵝ-lactam IV delivered ᵝ-lactam Free concentration PO delivered ᵝ- lactam PO delivered Free conc ᵝ-lactam
24 ᵝ-lactams and bone penetration ᵝ-lactams penetrate bone at approximately 5-20% of serum concentrations (oxacillin, cefazolin, ceftriaxone, ceftazidime, piperacillin, meropenem, aztreonam all studied) IV delivered [ᵝ-lactam] far exceed the MICs of likely organisms in most cases (free concentration is adequate) Serum concentration of oral delivered ᵝ- lactams <10% of IV therefore unlikely to achieve adequate bone concentration Spellberg, Lipsky CID 2012; 54: 393
25 ᵝ-lactams and bone penetration Historical data support oral penicillins when used in combination with probenecid Reduction in renal excretion Higher peak serum concentration Limited data available No licence for this use Widely used in SSTI in Aus/NZ SM Bell, Med J Aust 1976; 2: 592
26 Vancomycin: non infected bone 7-13% of serum concentration (- free drug concentration) Graziani et al AAC 1988; 32: 1320
 Grazzino Clin Pharmakokinet 2008;")
27 Vancomycin: infected bone 20-89% of serum concentration (Corticol vs Cancellous) Grazzino Clin Pharmakokinet 2008; 47: 793


28 Teicoplanin: infected bone 12-49% of serum concentration Grazzino Clin Pharmakokinet 2008; 47: 793
29 Daptomycin 8mg/kg Penetration into Bone 71.3 [ ] 22.4 [ ] 3.1 [ ] Montange et al. Antimicrobial agents and Chemotherapy, 2014; 58:
30 Daptomycin in bone (DFI) Traunmüller F et al. J. Antimicrob. Chemother. 2010;65:

31 Potential advantages of IV therapy Mode of delivery for Beta lactams, GPs, Daptomycin Acute: sepsis / infection beyond the bone e.g. SAB, Endocarditis, severe SSTI Bioavailability Reliable serum concentration following IV administration Avoids problems with absorption Ability to deliver bigger doses Increased likelihood of achieving therapeutic concentration at site of infection Spectrum of activity (for certain agents) Chronic: compliance and tolerability Missed doses are less likely
32

33 Potential disadvantages of IV therapy Requires an IV device Painful to insert Source of infection/ SAB Thrombosis/ phlebitis / fracture Inconvenient dosing regimens Requires hospitalisation or OPAT Time consuming to administer Restrictions of device / Hassle Expensive Antimicrobial stewardship Use of agents associated with CDI May be unnecessarily broad spectrum Wellsphere.com
34 Clinical outcome data Mainly observational studies with few RCTs Too many variables make comparisons between different IV agents difficult Surgical approach Variable methodology Definitions of success Length/ consistency of follow up
35 Outcomes in OPAT Rx Osteomyelitis (n=454) Tice et al JAC 2003; 51: 1261
36 Outcomes in OPAT Rx OM (n=198) Mackintosh CL, White H.A, and Seaton R.A, JAC 2011


37 Kaplan-Meier survival estimate of time to treatment failure for all patients with OM per diagnosis 19 of 65 with PJI failed (71% success) : Surgery, related or unrelated admission, or unplanned prolongation of IV Rx Mackintosh CL, White H.A, and Seaton R.A, JAC 2011
38 Teicoplanin for Bone infection in Glasgow OPAT Indications Resistant staphylococcal infections (CoNS or MRSA) Gram-positive infections with β-lactam allergy Prior failure with β-lactams Dosing regimen Loading: 20 mg/kg for 3 days (inpatient or outpatient) Maintenance: 3 /week (butterfly) TDM at longest interval (72 hours) Target trough concentration for Bone infection: μg/ml <20 μg/ml: increase dose or reduce interval (alt. days) >30 μg/ml: reduce dose or increase interval (2 or 1 /week) Lamont E et al. J Antimicrob Chemother 2009;doi: /jac/dkp147
39 Hazard Ratio from Survival analysis (Cox regression) for the association of the initial IV Antibiotic with failure Initial IV Rx No. over the follow up period No. Failing Hazar d ratio Teicoplanin (34%) 1 Ceftriaxone (19.6%) Other 5 1 CI p Mackintosh CL, White H.A, and Seaton R.A, JAC 2011
40 Debridement, Antibiotics and Implant Retention (DAIR) 6 weeks IV AB Empiric Vanc + Meropenem Rationalized Ceftriaxone Teicoplanin ~12 months oral Byren et al JAC 2009; 63: 1264
41 DAIR and duration of IV Rx Multiple Cox repgression model HR 0.49 ( ), p=0.18 Byren et al JAC 2009; 63: 1264

42 Daptomycin in Bone infection: Observational data to 30 days post- Rx

43 Daptomycin vs SOC in 2 Stage Revision (Phase II study) Microbiological confirmed PJI Randomised: 6-8mg/kg Dapto vs GP/SSP No oral agent 6 weeks post 1 st stage TOC 2 weeks post 2 nd stage If success months 75 pts randomised Byren et al ACC 2012; 56: 5626

44 Microbiological success Byren et al ACC 2012; 56: 5626
45 Important Side-effects in OPAT agents Ceftriaxone: Rash, LFTs, diarrhoea, leucopenia Teicoplanin: Leucopenia, anaemia, TCP, fevers Daptomycin: CPK/ myotoxicity, Eosinophilic pneumonitis
46 Note: An ADR in an individual patient in some instances involved multiple drug reaction types (e.g. rash and fever); each ADR type is counted separately in frequency bars even where they stem from one ADR event. Relative frequency of adverse drug reaction (ADR) types, in all first OPAT episodes over 10 year study period. Rash Severe gastro-intestinal Chills or fever Leucopenia, thrombocytopenia Nephrotoxicity Hepatotoxicity Nature of ADR unrecorded Other Anaphylactoid Frequency of ADR type

47 % with ADR ADRs, Infection Type and AB Used Daptomycin Ceftriaxone Teicoplanin
48 Line related complications in OPAT Infection: 0 to 3 per 1000 OPAT patient days Associated with length of IV Rx Other line events thrombosis, mechanical and chemical phlebitis: 5 to 50 per 1000 OPAT patient days lowest risk in tunnelled central venous catheters Highest risk when flucloxacillin primary OPAT agent No additional risk of patient/ carer administration Barr DA et al EJCMID 2012;31:2611. Upton A et al NZMJ 2004;117:U1020. Fisher DA et al IJAA 2006;28:545, Esposito S et al J Chemother 2007;19:417. Matthews PC et al JAC 2007;60:356
49 80 Reasons for admission from OPAT
50 Oral Antibiotic Therapy
51 Comparison of IV s Oral Rx: End of Rx Conterno, Turchi, Cochrane review Sep 2013
52 Comparison of IV s Oral Rx: 12 months post Rx Conterno, Turchi, Cochrane review Sep 2013
53 Quinolones Cipro most studies but extrapolate for Levofloxacin High oral bioavailability Penetrates macrophages and neutrophils High bone: serum concentration (>7.3) Bone concentration is proportional to dose and in excess of MIC of sensitive organisms. [Bone] 2-10 ug/g Effective vs MSSA, CNS, GNB In G+ve infection advisable to use 2 nd agent to reduce R risk Beware QTc prolongation, drug interactions
54 Rifampicin High oral bioavailability Penetrates neutrophils Excellent bone penetration (1.7ug/g) Active in biofilm ++ Synergistic with other agents R develops quickly ++ Use only in combination (consider delay in administration) Drug interactions, LFTs

55 Garirgos et al, AAC, 2010: 54; 5241
56 Other Oral Antibiotics useful in PJI Sodium fusidate: caution statins, LFTs Trimethoprim: caution CKD, K+ Doxycycline: chelated by Fe, Ca, ant acids Clindamycin: CDI, LFTs Linezolid: Haem toxicity, neuropathy. Caution with RIF, other D-DIs Pristinamycin (unlicensed)
57
58 IDSA PJI Guidelines Procedure Organism IV Antibiotic Duration DAIR Staph Flucloxacillin Ceftriaxone Or Vancomycin Daptomycin Linezolid (IV/PO) With Rifampicin DAIR Other Pathogen specific IV or highly bio available oral combination Amputation Any Pathogen specific IV or highly bio available oral combination 2-6 weeks then oral combination Rx including RIF Total 3 months: THR, other 6 months: TKR 4-6 weeks then potentially indefinite suppressive Rx (?avoid RIF) hrs post amputation unless sepsis 4-6 weeks if residual infection Osman et al CID 2013; 56: 1
59 IDSA PJI Guidelines Procedure Organis m IV Antibiotic Duration One Stage Revision Staph Flucloxacillin Ceftriaxone Or Vancomycin Daptomycin Linezolid (PO) With Rifampicin 2-6 weeks then oral Rx Total 3 months: Rif + other Longer if required One Stage Revision Other Pathogen specific IV or highly bio available oral combination 4-6 weeks then potentially indefinite suppressive Rx (?avoid RIF) Resection arthroplasty / 1 st of 2 stage revision Any Pathogen specific IV (without Rifampicin) or highly bio available oral combination 4-6 weeks then stop Osman et al CID 2013; 56: 1

60 OVIVA study Comparing IV vs oral approach in OM (including PJI) 6/52 Rx Randomisation within 7 days of surgery or commencement of IV Abx
61 Conclusions Use a best guess/tailored IV antibiotic which will cover the likely/proven organisms Empirical and acute settings Use high dose therapy for optimum PK/PD Combine with Rifampicin if Staphylococcal infection and the aim is cure (timing) Duration dependent on surgery and availability of highly orally bio-available agents Resistance Drug interactions (including QTc) OPAT use is safe: Follow Good Practice Recommendations for OPAT IV Beta lactams probably more effective than GPs Equipoise in IV vs oral for longer term Rx
62
63 New Developments
64 OPAT trends over 10 yrs in NHS GGC Trend over time Referral from non-local hospital X 2 trend = Referral from secondary care X 2 trend = Co-morbidity X 2 trend = Non-SSTI infection X 2 trend = MRSA infections (as % of S. aureus) X 2 trend = G-ve infections (% of +ve cultures) X 2 trend = Self / carer antibiotic admin X 2 trend = Barr et al, IJAA 2012 p < p < p < p < p = p = p <
65 ESBL Resistant E. coli Implant infections Tigecycline Gent 4 xs MIC Fosfomycin Colistin Corvec et al, AAC, 2013; 57: 1421
66 Synergy between Fosfomycin and Colistin Corvec et al, AAC, 2013; 57: 1421
67 Growth during Rx and 5 days post Rx Corvec et al, AAC, 2013; 57: 1421
68 Background c.180 K TKR or THRs / year in UK 14 K in Scotland (2013) c % of all joint replacements Hip > knee Diagnosis Acute post-op vs Acute infection of established prosthesis: Heat, erythema, pain, swelling +/-wound Sub-acute: pain and radiological loosening Multiple tissue sampling w/o contamination Sonication (when available) Microbiological (PCR when available) Histological
 Streptococci Diphtheroids Pseudomonas Anaerobes Polymicrobial (Fifth Report of the Mandatory Surveillance of Surgical Site Infection in")
69 Common organisms Staph.aureus inc MRSA (40.6%) Coagulase negative staphylococci (15.9%) Coliforms (15.6%) Enterococci (9.6%) Streptococci Diphtheroids Pseudomonas Anaerobes Polymicrobial (Fifth Report of the Mandatory Surveillance of Surgical Site Infection in Orthopaedic Surgery)

70 Decline in inpatient SSI in TKR and TKR in Scotland Hip arthroplasty enhanced SSI surveillance: 0.76% by day 30 Majority are deep seated SSI SSHAIP, HPS, 2014

71 Fosfomycin + Colistin: Cure in biofilm Corvec et al, AAC, 2013; 57: 1421
72 Pharmacokinetic parameters of daptomycin at steady-state (Day 4 or 5) from 9 patients with diabetic foot infections treated with 6 mg/kg daptomycin Cmax (mg/l) Half life (h) AUC0-24* Plasma Subcutis inflamed Metatarsal bone * Steady state concentrations at baseline were used for concentrations at 24 hours The EUCAST breakpoint for staphylococci is 1 mg/l Traunmuller F et al, Journal of Antimicrobial Chemotherapy, 2010, Advance Access April 7
Role of IV Therapy in Bone and Joint Infection
 Role of IV Therapy in Bone and Joint Infection Andrew Seaton ID Consultant, Queen Elizabeth University Hospital Lead Doctor Antimicrobial Management Team, NHS GGC @raseaton66 OPAT The IVnOAT Perspective
Role of IV Therapy in Bone and Joint Infection Andrew Seaton ID Consultant, Queen Elizabeth University Hospital Lead Doctor Antimicrobial Management Team, NHS GGC @raseaton66 OPAT The IVnOAT Perspective
Consider the patient, the drug and the device how do you choose?
 Consider the patient, the drug and the device how do you choose? Tim Hills Lead Pharmacist Antimicrobials and Infection Control Nottingham University Hospitals NHS Trust OPAT Recommendations Drug Therapy
Consider the patient, the drug and the device how do you choose? Tim Hills Lead Pharmacist Antimicrobials and Infection Control Nottingham University Hospitals NHS Trust OPAT Recommendations Drug Therapy
Key considerations choice of antimicrobial agents Dr Andrew Seaton
 Key considerations choice of antimicrobial agents Dr Andrew Seaton Key Considerations choice of antimicrobial agents and managing the IV to oral switch R. Andrew Seaton NHS Greater Glasgow and Clyde, Scotland,
Key considerations choice of antimicrobial agents Dr Andrew Seaton Key Considerations choice of antimicrobial agents and managing the IV to oral switch R. Andrew Seaton NHS Greater Glasgow and Clyde, Scotland,
The role of oral antibiotics in Prosthetic joint infection. Matthew Dryden MD
 The role of oral antibiotics in Prosthetic joint infection Matthew Dryden MD Persistence of bone infection Osteomyelitis in 1930 Prosthetic joint replacement demand is increasing When things go wrong Patient
The role of oral antibiotics in Prosthetic joint infection Matthew Dryden MD Persistence of bone infection Osteomyelitis in 1930 Prosthetic joint replacement demand is increasing When things go wrong Patient
Oral antibiotics are not always straight forward
 Oral antibiotics are not always straight forward OPAT Regional Workshop 1 st May 2018 Fiona Robb, Antimicrobial Pharmacist NHS Greater Glasgow & Clyde Introduction Describe NHS GGC s Oral vs IV Antibiotics
Oral antibiotics are not always straight forward OPAT Regional Workshop 1 st May 2018 Fiona Robb, Antimicrobial Pharmacist NHS Greater Glasgow & Clyde Introduction Describe NHS GGC s Oral vs IV Antibiotics
MANAGEMENT OF TOTAL JOINT ARTHROPLASTY INFECTIONS
 MANAGEMENT OF TOTAL JOINT ARTHROPLASTY INFECTIONS Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine TOTAL JOINT ARTHROPLASTIES In 2009: 1 million THA and TKA By 2030,
MANAGEMENT OF TOTAL JOINT ARTHROPLASTY INFECTIONS Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine TOTAL JOINT ARTHROPLASTIES In 2009: 1 million THA and TKA By 2030,
Gram-Positive Infections and OPAT:
 Gram-Positive Infections and OPAT: Developments and Observations R. Andrew Seaton Gartnavel General Hospital Glasgow, Scotland, UK The views presented are the views of the speaker and not necessarily the
Gram-Positive Infections and OPAT: Developments and Observations R. Andrew Seaton Gartnavel General Hospital Glasgow, Scotland, UK The views presented are the views of the speaker and not necessarily the
Full Title of Guideline. Author: Contact Name and Job Title. Division & Speciality. Review date December 2020
 Full Title of Guideline Author: Contact Name and Job Title Division & Speciality Guideline for the treatment of prosthetic joint infections in adults Mr Peter James - Consultant Orthopaedic Surgeon Dr
Full Title of Guideline Author: Contact Name and Job Title Division & Speciality Guideline for the treatment of prosthetic joint infections in adults Mr Peter James - Consultant Orthopaedic Surgeon Dr
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring. Janis Chan Pharmacist, UCH 2008
 and their Monitoring. Janis Chan Pharmacist, UCH 2008") Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring Janis Chan Pharmacist, UCH 25-4-2008 2008 Aminoglycosides (AG) 1. Gentamicin 2. Amikacin 3. Streptomycin 4. Neomycin
Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring Janis Chan Pharmacist, UCH 25-4-2008 2008 Aminoglycosides (AG) 1. Gentamicin 2. Amikacin 3. Streptomycin 4. Neomycin
Appropriate Antimicrobial Therapy for Treatment of
 Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Best Antimicrobials for Staphylococcus aureus Bacteremia
 Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate
 Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Scottish Medicines Consortium
 Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Cellulitis. Assoc Prof Mark Thomas. Conference for General Practice Auckland Saturday 28 July 2018
 Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust
 PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
Treating Multi-drug Resistant Gramnegative. Fiona Robb Antimicrobial Pharmacist NHS Greater Glasgow & Clyde 9 th December 2016
 Treating Multi-drug Resistant Gramnegative Infections in OPAT Fiona Robb Antimicrobial Pharmacist NHS Greater Glasgow & Clyde 9 th December 2016 Overview To describe the emerging threat of Antimicrobial
Treating Multi-drug Resistant Gramnegative Infections in OPAT Fiona Robb Antimicrobial Pharmacist NHS Greater Glasgow & Clyde 9 th December 2016 Overview To describe the emerging threat of Antimicrobial
Introduction to Pharmacokinetics and Pharmacodynamics
 Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS
 PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Le infezioni di cute e tessuti molli
 Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
Curricular Components for Infectious Diseases EPA
 Curricular Components for Infectious Diseases EPA 1. EPA Title Promoting antimicrobial stewardship based on microbiological principles 2. Description of the A key role for subspecialists is to utilize
Curricular Components for Infectious Diseases EPA 1. EPA Title Promoting antimicrobial stewardship based on microbiological principles 2. Description of the A key role for subspecialists is to utilize
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams
 DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
Enterococcal PJI. Miquel Ekkelenkamp
 Enterococcal PJI Miquel Ekkelenkamp Enterococci: Gram-positive and round Formerly streptococci (but really quite different) Main clinical species : E. faecalis and E. faecium Mostly opportunistic pathogen
Enterococcal PJI Miquel Ekkelenkamp Enterococci: Gram-positive and round Formerly streptococci (but really quite different) Main clinical species : E. faecalis and E. faecium Mostly opportunistic pathogen
* gender factor (male=1, female=0.85)
") Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
S aureus infections: outpatient treatment. Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium
 S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Protocol for exit-site care and treatment of exit-site infections in peritoneal dialysis CONTROLLED DOCUMENT
 CONTROLLED DOCUMENT Protocol for exit-site care and treatment of exit-site infections in peritoneal dialysis CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Guideline Clinical The purpose
CONTROLLED DOCUMENT Protocol for exit-site care and treatment of exit-site infections in peritoneal dialysis CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Guideline Clinical The purpose
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
Outpatient parenteral antimicrobial treatment. Which antibiotics can be used?
 Outpatient parenteral antimicrobial treatment Which antibiotics can be used? Franky Buyle SBIMC-BVIKM March 30th 2017 Brussels Pharmacy Multidisciplinary Infection Team Ghent University Hospital, Belgium
Outpatient parenteral antimicrobial treatment Which antibiotics can be used? Franky Buyle SBIMC-BVIKM March 30th 2017 Brussels Pharmacy Multidisciplinary Infection Team Ghent University Hospital, Belgium
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how?
 Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Antibiotic Prophylaxis Update
 Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
Antibacterial therapy 1. د. حامد الزعبي Dr Hamed Al-Zoubi
 Antibacterial therapy 1 د. حامد الزعبي Dr Hamed Al-Zoubi ILOs Principles and terms Different categories of antibiotics Spectrum of activity and mechanism of action Resistancs Antibacterial therapy What
Antibacterial therapy 1 د. حامد الزعبي Dr Hamed Al-Zoubi ILOs Principles and terms Different categories of antibiotics Spectrum of activity and mechanism of action Resistancs Antibacterial therapy What
NHS Dumfries And Galloway. Surgical Prophylaxis Guidelines
 NHS Dumfries And Galloway Surgical Prophylaxis Guidelines The aim of surgical prophylaxis is to reduce rates of surgical site and health-care associated infections and so reduce surgical morbidity and
NHS Dumfries And Galloway Surgical Prophylaxis Guidelines The aim of surgical prophylaxis is to reduce rates of surgical site and health-care associated infections and so reduce surgical morbidity and
Management of Native Valve
 Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Pharmacology Week 6 ANTIMICROBIAL AGENTS
 Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Antibacterials. Recent data on linezolid and daptomycin
 Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Antimicrobial susceptibility
 Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Staph Cases. Case #1
 Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
Safety of an Out-Patient Intravenous Antibiotics Programme
 Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Who should read this document? 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version? 3
 Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
GUIDELINE FOR ANTIMICROBIAL USE IN THE ORTHOPAEDIC AND TRAUMA DEPARTMENT
 GUIDELINE FOR ANTIMICROBIAL USE IN THE ORTHOPAEDIC AND TRAUMA DEPARTMENT Written by: Dr Ken. N. Agwuh, Consultant Microbiologist Mr Roger Helm, Consultant Orthopaedic Surgeon Mr T Kumar, Consultant Orthopaedic
GUIDELINE FOR ANTIMICROBIAL USE IN THE ORTHOPAEDIC AND TRAUMA DEPARTMENT Written by: Dr Ken. N. Agwuh, Consultant Microbiologist Mr Roger Helm, Consultant Orthopaedic Surgeon Mr T Kumar, Consultant Orthopaedic
Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis
 Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis Steve SM Wong Alice Ho Miu Ling Nethersole Hospital Background PD peritonitis is a major cause of PD
Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis Steve SM Wong Alice Ho Miu Ling Nethersole Hospital Background PD peritonitis is a major cause of PD
Antibiotic Prophylaxis in Spinal Surgery Antibiotic Guidelines. Contents
 Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Surgical prophylaxis for Gram +ve & Gram ve infection
 Surgical prophylaxis for Gram +ve & Gram ve infection Professor Mark Wilcox Clinical l Director of Microbiology & Pathology Leeds Teaching Hospitals & University of Leeds, UK Heath Protection Agency Surveillance
Surgical prophylaxis for Gram +ve & Gram ve infection Professor Mark Wilcox Clinical l Director of Microbiology & Pathology Leeds Teaching Hospitals & University of Leeds, UK Heath Protection Agency Surveillance
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS
 Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
PATIENT DEMOGRAPHICS. Surname. Given name. Pacific Islander (non-maori) ADMISSION DETAILS
 ADMISSION DETAILS") Reviewer / hospital Date review started PATIENT DEMOGRAPHICS MRN DOB Sex Patient sticky label if available, else enter details here Surname Post-code Given name Australian Aborigine / TSI Middle Eastern
Reviewer / hospital Date review started PATIENT DEMOGRAPHICS MRN DOB Sex Patient sticky label if available, else enter details here Surname Post-code Given name Australian Aborigine / TSI Middle Eastern
Scottish Medicines Consortium
 Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS
 VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Considerations for antibiotic therapy. Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen
 Considerations for antibiotic therapy Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen Infective Endocarditis There will never be a cure for this malignant disease! Sir
Considerations for antibiotic therapy Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen Infective Endocarditis There will never be a cure for this malignant disease! Sir
SURGICAL ANTIBIOTIC PROPHYLAXIS GUIDELINES WITHIN ORTHOPAEDIC SURGERY FOR ADULT PATIENTS
 SURGICAL ANTIBIOTIC PROPHYLAXIS GUIDELINES WITHIN ORTHOPAEDIC SURGERY FOR ADULT PATIENTS Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if
SURGICAL ANTIBIOTIC PROPHYLAXIS GUIDELINES WITHIN ORTHOPAEDIC SURGERY FOR ADULT PATIENTS Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Septicaemia Definitions 1
 Septicaemia Definitions 1 Term Definition Bacteraemia Systemic Inflammatory response (SIRS) Sepsis Bacteria that can be cultured from the blood stream The systemic response to a wide range of stresses.
Septicaemia Definitions 1 Term Definition Bacteraemia Systemic Inflammatory response (SIRS) Sepsis Bacteria that can be cultured from the blood stream The systemic response to a wide range of stresses.
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report. July December 2013 Second and Third Quarters 2014
 Antimicrobial Stewardship Report. July December 2013 Second and Third Quarters 2014") H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report July December 213 Second and Third Quarters
H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report July December 213 Second and Third Quarters
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland
 Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
Sustaining an Antimicrobial Stewardship
 Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Antibiotic Prophylaxis in Adult Orthopaedic Surgery. Formulary/prescribing guideline
 Document type: Antibiotic Prophylaxis in Adult Orthopaedic Surgery Version: 2.0 Author (name): Author (designation): Validated by Formulary/prescribing guideline Dr Celia Chu, Dr Katy Edwards, Dr Pradeep
Document type: Antibiotic Prophylaxis in Adult Orthopaedic Surgery Version: 2.0 Author (name): Author (designation): Validated by Formulary/prescribing guideline Dr Celia Chu, Dr Katy Edwards, Dr Pradeep
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Outpatient parenteral antimicrobial treatment. Which antibiotics can be used?
 Outpatient parenteral antimicrobial treatment Which antibiotics can be used? Franky Buyle SBIMC-BVIKM March 30th 2017 Brussels Pharmacy Multidisciplinary Infection Team Ghent University Hospital, Belgium
Outpatient parenteral antimicrobial treatment Which antibiotics can be used? Franky Buyle SBIMC-BVIKM March 30th 2017 Brussels Pharmacy Multidisciplinary Infection Team Ghent University Hospital, Belgium
Grey Nuns Community Hospital (GNCH) Antimicrobial Stewardship Report
 Antimicrobial Stewardship Report") H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Grey Nuns Community Hospital (GNCH) Antimicrobial Stewardship Report to 214 Table of Contents I. Introduction..
H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Grey Nuns Community Hospital (GNCH) Antimicrobial Stewardship Report to 214 Table of Contents I. Introduction..
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens
 The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
Who should read this document 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version 3. Policy/Procedure/Guideline 3
 Antibiotic Prophylaxis in Cranial Neurosurgery Antibiotic Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Antibiotic Prophylaxis in Cranial Neurosurgery Antibiotic Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Pocket Guide to Diagnosis & Treatment of Cardiovascular Implantable Electronic Device (CIED) Infections
 Infections") Pocket Guide to Diagsis & Treatment of Cardiovascular Implantable Electronic Device (CIED) Infections Draft Version : November 208 DEFINITION Pocket infection, if all 4 criteria are fulfilled: Investigation/sign
Pocket Guide to Diagsis & Treatment of Cardiovascular Implantable Electronic Device (CIED) Infections Draft Version : November 208 DEFINITION Pocket infection, if all 4 criteria are fulfilled: Investigation/sign
Pharmacist Coordinated Antimicrobial Therapy: OPAT and Transitions of Care
 Pharmacist Coordinated Antimicrobial Therapy: OPAT and Transitions of Care Jennifer McCann, PharmD, BCCCP State Director of Clinical Pharmacy Services St. Vincent Health Indiana Conflicts of Interest No
Pharmacist Coordinated Antimicrobial Therapy: OPAT and Transitions of Care Jennifer McCann, PharmD, BCCCP State Director of Clinical Pharmacy Services St. Vincent Health Indiana Conflicts of Interest No
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Diagnosis: Presenting signs and Symptoms include:
 PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
LINEE GUIDA: VALORI E LIMITI
 Ferrara 28 novembre 2014 LINEE GUIDA: VALORI E LIMITI Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi EVIDENCE BIASED GERIATRIC MEDICINE Older patients with comorbid conditions
Ferrara 28 novembre 2014 LINEE GUIDA: VALORI E LIMITI Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi EVIDENCE BIASED GERIATRIC MEDICINE Older patients with comorbid conditions
Copyright 2012 Diabetes In Control, Inc. For permission to reprint, please contact Heather Moran, Production Editor, at
 Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
SHC Surgical Antimicrobial Prophylaxis Guidelines
 SHC Surgical Antimicrobial Prophylaxis Guidelines I. Purpose/Background This document is based upon the 2013 consensus guidelines from American Society of Health-System Pharmacists (ASHP), the Infectious
SHC Surgical Antimicrobial Prophylaxis Guidelines I. Purpose/Background This document is based upon the 2013 consensus guidelines from American Society of Health-System Pharmacists (ASHP), the Infectious
Compliance of manufacturers of AST materials and devices with EUCAST guidelines
 Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Antimicrobial Stewardship Programs The Same, but Different. Sara Nausheen, MD Kevin Kern, PharmD
 Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Prophylactic antibiotic timing and dosage. Dr. Sanjeev Singh AIMS, Kochi
 Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
SSTI s :A Guideline for Effective Treatment of Skin and Soft Tissue Infections
 SSTI s :A Guideline for Effective Treatment of Skin and Soft Tissue Infections Dr. Javan S. Bass, FACFAS Metro Foot & Ankle Centers, PC Georgia Podiatric Association Board of Directors Disclosures Bako
SSTI s :A Guideline for Effective Treatment of Skin and Soft Tissue Infections Dr. Javan S. Bass, FACFAS Metro Foot & Ankle Centers, PC Georgia Podiatric Association Board of Directors Disclosures Bako
This survey was sent only to EIN members with a pediatric infectious diseases practice.
 Infectious Diseases Society of America Emerging Infections Network Report for Query: Pediatric Outpatient Parenteral Antibiotic Therapy (OPAT) Overall response rate: 188/281 (66.9%) physicians responded
Infectious Diseases Society of America Emerging Infections Network Report for Query: Pediatric Outpatient Parenteral Antibiotic Therapy (OPAT) Overall response rate: 188/281 (66.9%) physicians responded
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
ß-lactams. Sub-families. Penicillins. Cephalosporins. Monobactams. Carbapenems
 β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
Jerome J Schentag, Pharm D
 Clinical Pharmacy and Optimization of Antibiotic Usage: How to Use what you have Learned in Pharmacokinetics and Pharmacodynamics of Antibiotics Jerome J Schentag, Pharm D Presented at UCL on Thursday
Clinical Pharmacy and Optimization of Antibiotic Usage: How to Use what you have Learned in Pharmacokinetics and Pharmacodynamics of Antibiotics Jerome J Schentag, Pharm D Presented at UCL on Thursday
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Staphylococcus aureus and Health Care associated Infections
 Staphylococcus aureus and Health Care associated Infections Common - but poorly measured Prof Peter Collignon The Canberra Hospital Australian National University What are health-care associated infections?
Staphylococcus aureus and Health Care associated Infections Common - but poorly measured Prof Peter Collignon The Canberra Hospital Australian National University What are health-care associated infections?
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate