Current Perspectives on the Management of Community Acquired Pneumonia
|
|
|
- Rudolf Blankenship
- 5 years ago
- Views:
Transcription
1 Current Perspectives on the Management of Community Acquired Pneumonia Dr. Roland Leung MBBS MD FRACP FCCP FHKCP FHKAM(Med) Specialist in Respiratory Medicine
2 Outline of Presentation Diagnosis and its pitfalls Common pathogens in CAP Antibiotic resistance Management guidelines

3 Definition: Signs/symptoms of acute infection plus acute infiltrate on CXR or auscultatory findings Signs and symptoms: chill and/or fever, pleuritic chest pain, productive cough, tachypnea, tachycardia, crackles and/or consolidation Clinical sequelae: bacteremia, metastatic foci of infection, death No association between signs/symptoms and bacterial aetiology The Disease Process Bartlett JG, et al. Clin Infect Dis. 2000;31: Donowitz GR, Mandell GL. Principles and Practice of Infectious Diseases 1995: Fang GD, et al. Medicine (Baltimore). 1990;69:
4 Morbidity and Mortality Hospitalisations Deaths Bartlett et al, 500,000/year 45,000/year 2000 (USA) 0.27% of general population 2-30% of inpatients 1.0% of elderly < 1% of outpatients population ( 65 years) Huchon G et al, 22-51% of 7% of inpatients 1998 patients with CAP 29% of severe (North America/ infections Europe) Bartlett JG, et al. Clin Infect Dis. 2000;31: Huchon G, Woodhead M. Eur Resp Rev. 1998;8:
5 Pneumonia: X-Ray Normal not pneumonia Lobar pattern Bilateral Basal Bronchopneumonia Diffuse Cavitating Upper lobe
6 False-negative CXR first 24 hours of infection Dehydration Severe neutropenia Infection with P carinii % of cases of normal CXR J AIDS 1994;7:39
7 Pneumonia: Differential Diagnosis Pulmonary embolism Endobronchial obstruction/atelectasis Extrinsic Allergic alveolitis Cryptogenic Fibrosing Alveolitis Sepsis and ARDS
8 Pneumonia: Classification Lobar Bronchopneumonia Atypical Pneumonia Cavitating Pneumonia Viral pneumonia Nosocomial pneumonia Pneumonia in the immunosuppressed
9 Host Risk Factors for Infection Defective phagocytosis Advanced age Institutionalization Immune dysfunction Risk of infection Alcoholism Comorbidity Smoking Poor nutrition Huchon G, et al. Eur Resp Rev. 1998;8: Koivula I, et al. Am J Med. 1994;96: Baik I, et al. Arch Intern Med. 2000;160:
10 Methods for aetiologic diagnosis Stains Culture Antibody detection Antigen detection Nucleic acid detection
11 Sputum Gram Stain Specific for infecting organism when >25PMN & <10 SEC/low power field Clearly predominant pathogen Most patients do not produce a diagnostic specimen Physicians are more likely than nurses to collect diagnostic sputum samples Common error of interpretation Interpretating poor specimen Missing influenza, other GNB Misinterpret oral flora as pneumococci
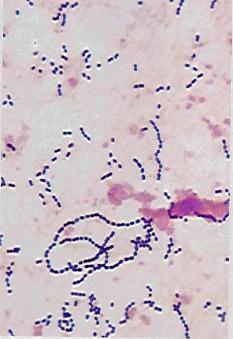
12
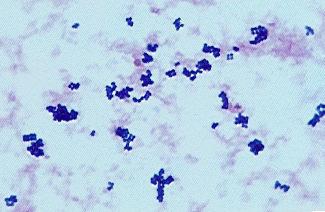
13
14 Sputum culture Sensitive but not specific Specialized media improves sensitivity Screening with gram stain improve sensitivity & specificity Diagnostic for organism that do not colonize respiratory tract MTB, Legionella, Mycoplasma, Chlamydia RNA viruses, Coccidioides, Histoplasma, Blastomyces
15 Difficulty in obtaining sputum About 10-30% of patients have non-productive cough 15-30% of patients have received antibiotics prior to evaluation Many possible important pathogens are not detected with conventional culture ie Legionella, C pneumoniae The quality of microbiologic studies is often substandard
16 Serologic Diagnosis Limited value: antibody rises occurs 2-4 weeks after onset symptoms A single elevated titre can be helpful in dx of infection caused by : M. pneumoniae C. pneumoniae Legionella spp. Coxiella burnetti Corona virus (SARS)
17 Key Pathogens Associated with Community- Acquired Pneumonia (CAP) USA M pneumoniae Legionella spp C pneumoniae Anaerobes/ aspiration 7% 8% Aerobic gramnegative rods Other 8% 7% 5% 10% 34% S pneumoniae 6% S aureus 15% H influenzae and M catarrhalis Eron JJ, et al. Hosp Formul. 1994;29:
18 Key Pathogens Associated with Community- Acquired Pneumonia (CAP) Europe (5,961 Adult Hospitalized CAP Patients in 26 Prospective Studies from 10 European Countries) S pneumoniae C pneumoniae Viral M pneumoniae Legionella spp Atypicals: 25% H Influenzae G-neg Enterobacteria Proportion of Cases (%) Woodhead MA. Chest 1998;113:183S 187S
19 Etiology of CAP in Hong Kong No. of case (%) H influenzae M pneumoniae 7 10 S pneumoniae Klebsiella Pseudomonas aeruginosa TB MSSA Acinetobacter Branhamella Catarrhalis No identifiable agent
20 Prince of Wales Hospital Antibiogram 2008 Top 10 Isolates from All Units in Respiratory Specimens Eterobacter sp. 3% M. catarrhalis 4% Others 17% P. aeruginosa 18% H. influenzae 15% Acietobacter sp. 5% Candida sp. 10% M. tuberculosis 5% S. pneumoniae Klebsiella sp. 8% S. aureus 7% 8% Specimens no.: 2745
21 HK West Cluster Antibiogram 2008 Top 7 Isolates from All Units in Respiratory Specimens P. aeruginosa 12% H. influenzae 9% S. aureus 9% Others 55% S. peumoniae 3% E. coli 3% Klebsiella sp. 6% M. catarrahlis 3%
22 Pathogens by underlying disease Conditions Infectious agents None S. pneum, Mycoplasma, Chamydia, H. flu. Age>60 S. pneum, H. flu, S. aureus, GNR, influenza COPD S. pneum, H. flu, M. cat ETOH S. pneum, GNR, anaerob, S. aur, H. flu CRF/DM S. pneum, S. aureus, GNR Bronchiectasis H. flu, S. aureus, P. aerug Influenza S. pneum, H. flu, S aureus

23 Pathogens by underlying disease
24 Prevalence of Atypical Pathogens N Mp (%) Cp (%) Leg (%) Marrie et al, 1996 (Canada) File et al, 1997 (USA) Sopena et al, 1998 (Spain) Steinhoff et al, 1996 (Germany) Lieberman et al, 1996 (Israel) Neill et al, 1996 (New Zealand) Bohte et al, 1994 (Netherlands) N, number of patients; Mp, Mycoplasma pneumoniae; Cp, Chlamydia pneumoniae; Leg, Legionella species. Lieberman D. Clin Chest Med. 1999;20: Marrie TJ, et al. Am J Med. 1996;101: File TM, et al. Antimicrob Agents Chemother. 1997;41: Sopena N, et al. Chest. 1998;113: Steinhoff D, et al. Clin Infect Dis. 1996;22: Lieberman D, et al. Eur Respir J. 1996;9: Neill AM, et al. Thorax. 1996;51: Bohte R, et al. Thorax. 1995;50:543-7.
25 Incidence of M. pneumoniae Acute Infection in Children with Lower Respiratory Tract Diseases Age Group (years) Diagnosis 2-4 (%) 5-7 (%) >7 (%) All (%) Acute bronchitis 14/62 (22.5) 10/34 (29.4) 12/17 (70.5) 36/113 (31.8) Wheezing 12/53 (22.6) 5/15 (33.3) 7/14 (50.0) 24/82 (29.2) Pneumonia 43/209 (20.5) 56/123 (45.5) 51/86 (59.3) 150/418 (35.8) All 67/324 (21.3) 71/172 (41.3) 70/117 (59.8) 210/613 (34.3) Principi N, et al. Clin Infect Dis 2001
26 Incidence of C. pneumoniae Acute Infection in Children with Lower Respiratory Tract Diseases Age Group (years) Diagnosis 2-4 (%) 5-7 (%) >7 (%) All (%) Acute bronchitis 5/62 (8.0) 12/34 (35.2) 5/17 (29.4) 22/113 (19.4) Wheezing 8/53 (15.0) 7/15 (46.6) 4/14 (28.5) 19/82 (23.1) Pneumonia 18/209 (8.6) 13/123 (10.5) 15/86 (17.4) 46/418 (11.0) All 31/324 (9.6) 32/172 (18.6) 24/117 (20.5) 87/613 (14.1) Principi N, et al. Clin Infect Dis 2001
27 Implications of Atypical Pneumonia Clinical and radiographic features of atypical infection similar to those of typical infections Classification into atypical and typical syndromes does not accurately predict etiology Atypical pathogens are a frequent cause of CAP Clinical outcomes similar for atypical and typical pathogens Empiric therapy must include coverage of atypical pathogens Empiric therapy should include an agent that penetrates intracellularly and attains high intracellular concentrations Reimann HA. JAMA. 1938;111: Liebermann D. Clin Chest Med. 1999;20: Marrie TJ, et al. Am J Med. 1996;101:
28 Treatment Guidelines for CAP Community-acquired pneumonia (CAP) is a major cause of morbidity and mortality, and internationally is the leading cause of death from an infectious disease and the sixth leading cause of death overall. Over the past decade international societies have published and revised guidelines for the management of patients with CAP. e.g. ATS-IDSA (2007), European Respiratory Society (ERS) (2005), IMPACT(2005), etc.
29 Rationale for Antibiotic Therapy Guidelines Ensure appropriate prescribing Promote the rational use of antibiotics Limit the emergence of resistance Conserve new agents Ensure cost-effective practice Educate physicians but Are only a starting point Niederman MS. Curr Opin Pulm Med. 1996;2:161-5.
30 Risk Stratification The goals of stratification include Avoiding antimicrobial treatment when it is not indicated (e.g., for viral infections), To support use of the 3 D s the right Drug, at the right Dose, for the right Duration One of the most important considerations in patient stratification is determining the site of care Evaluating the severity of the patient s illness and Deciding whether the patient can be treated safely as an outpatient
31 Site-of-Care Decisions Site-of-care decisions are important areas for improvement in CAP i.e. hospital vs. outpatient i.e. intensive care unit vs. general ward Severity-of-illness scores Pneumonia Severity Index (PSI), also known as the Pneumonia Patient Outcomes Research Team (PORT) Effective, but requires consideration of many variables CURB-65 Simple, does not require a blood test CRB-65 More simplify version of CURB-65
32 CURB-65

33 CRB-65
34 Respiratory Tract Infections Hong Kong Hospital Authority IMPACT guideline Second Edition (version 2.2) Updated 10 Feb 2003
35 Respiratory Tract Infections RTI Usual organism Preferred regimens Acute bacterial exacerbation of COPD respiratory viruses; S. pneumoniae; H. influenzae; B. catarrhalis b IV/PO Augmentin or Unasyn CAP, not hospitalized CAP, hospitalized in general ward CAP, hospitalized in ICU or serious pneumonia S. pneumoniae; H. influenzae; Mycoplasma pneumoniae; Chlamydia pneumoniae; C. psittaci (Influenza A; M. tuberculosis) As above As above + Enterobacteriaceae PO Augmentin or Unasyn ± macrolide IV/PO Augmentin or Unasyn ± macrolide (IV piperacillin-tazobactam or cefotaxime ceftriaxone) + a macrolide Bronchiectasis; acute bacterial exacerbation or pneumonia P. aeruginosa (most) (PO ciprofloxacin or IV ticarcillin-clavulana piperacillin-tazobactam) ± an aminoglycos Aspiration pneumonia oral anaerobes : bacteroides, peptostreptococci, fusobacterium, S. milleri (IV penicillin G + PO metronidazole) or PO clindamycin
36 Hospitalacquired pneumonia (HAP) HAP; onset < 4 days after admission + no previous antibiotics HAP; onset < 4 days after admission + had antibiotics recently; OR onset 5 days after admission OR mechanical ventilation Respiratory Tract Infections Usual organisms S. pneumoniae; H. influenzae; B. catarrhalis; S. aureus MRSA; P. aeruginosa; acinetobacters; Klebsiella spp.; Enterobacter spp. Preferred regimens IV/PO ampicillinsulbactam or amoxycillinclavulanate (IV ticarcillinclavulanate or piperacillintazobactam) ± an aminoglycoside Alternatives cefuroxime if patient is penicillinallergic --
37 ERS IDSA CIDS/CTS *Preferred option. Outpatients Treatment Options (1) Penicillin*, aminopenicillin ± β-lactamase inhibitor (especially if H influenzae suspected), macrolide, tetracycline, cephalosporin, quinolone, oral streptogramin Macrolide, doxycycline, fluoroquinolone Macrolide*, doxycycline COPD, no recent R X COPD, recent R X Macrolide*, doxycycline Fluoroquinolone*, amoxicillin/clavulanate + macrolide Suspected Amoxicillin/clavulanate ± macroaspiration macrolide*, fluoroquinolone + macrolide Nursing home Fluoroquinolone, amoxicillin/clavulanate + macrolide Huchon G, et al. Eur Resp Rev. 1998;8: Bartlett JG, et al. Clin Infect Dis. 2000;31: Mandell LA, et al. Clin Infect Dis. 2000;31:
38 Outpatients Treatment Options (2) CDCP Macrolide*, doxycycline*, antipneumococcal β-lactam ATS No CPD, no Advanced-generation macrolide*, modifiers doxycycline With CPD and/or other modifier β-lactam a + (macrolide*, doxycycline), antipneumococcal fluoroquinolone *Preferred option. a Oral cefpodoxime, cefuroxime, high-dose amoxicillin, amoxicillin/clavulanate or parenteral ceftriaxone then oral cefpodoxime. Heffelfinger JD, et al. Arch Intern Med. 2000;160: American Thoracic Society. Am J Respir Crit Care Med. 2001;163:
39 Hospitalized General Ward Patients Treatment Options (1) ERS IDSA CIDS/CTS ([β-lactam/β-lactamase inhibitor, 2nd- or 3rd-gen. cephalosporin, benzylpenicillin, amoxicillin, ampicillin] ± [macrolide, 2nd-gen. fluoroquinolone]), 3rd-gen. fluoroquinolone Pulmonary abscess, cavitated pneumonia, suspected macroaspiration Amoxicillin/clavulanate, clindamycin (Cefotaxime, ceftriaxone) + macrolide, fluoroquinolone Respiratory fluoroquinolone*, 2nd- to 4th-generation cephalosporin + macrolide *Preferred option. Huchon G, et al. Eur Resp Rev. 1998;8: Bartlett JG, et al. Clin Infect Dis. 2000;31: Mandell LA, et al. Clin Infect Dis. 2000;31:
40 CDCP Hospitalized General Ward Patients Treatment Options (2) β-lactam + macrolide*, newer fluoroquinolone ATS No CPD, no Azithromycin*, doxycyline + modifiers β-lactam, antipneumococcal fluoroquinolone CPD and/or other modifier *Preferred option. a Cefotaxime, ceftriaxone, ampicillin/sulbactam, high-dose ampicillin. Intravenous β-lactam a + (macrolide, doxycycline), antipneumococcal fluoroquinolone Heffelfinger JD, et al. Arch Intern Med. 2000;160: American Thoracic Society. Am J Respir Crit Care Med. 2001;163:
41 Empirical Antibiotics for CAP Sanford 2010 IDSA 2007 IMPAC 2005 Outpatient: no cardiopulmonary disease or modifying factors Azithro Azithro-ER Macrolide (Azithro) Unasyn +/- macrolide (Azithro) Outpatient: cardiopulmonary disease +/- modifying factors Azithro + AM-CL Macrolide (Azithro) + ß lactam Inpatient, non-icu Ceftriaxone + Azithro Macrolide (Azithro) + ß lactam (Tazocin/ Sulperazon) AM-CL +/- Macrolide (Azithro) Inpatient, ICU Tazocin + Azithro If CA-MRSA is a consideration, add Linezolid ß lactam (Tazocin/ Sulperazon) + Azithro Tazocin + Macrolide (Azithro)
42 Effect of Macrolide Inclusion on Mortality Gleason et al, 1999 Gleason PP, et al. Arch Intern Med. 1999;159: d Mortality, % (95% CI) Community LCF Total study Initial antimicrobial dwelling dwelling cohort regimens (n = 9751) (n = 3194) (n = 12,945) 2nd-generation cephalosporin only 2nd-generation cephalosporin plus macrolides Nonpseudomonal 3rd generation cephalosporins only Nonpseudomonal 3rd generation cephalosporins plus macrolides
43 Effect of Macrolide Inclusion on Mortality Dudas et al, 2000 Predictors of mortality: multivariate analysis Odds ratio Variable P value (95% CI) Change in initial antibiotic (2.1 to 5.1) ICU admission (1.4 to 4.7) > 8 h to administration of first antibiotic (1.3 to 4.9) Age (decades) (1.3 to 1.8) SCr (1.0 mg/dl) (1.0 to 1.4) RR (10 breaths/min) (1.5 to 2.4) WBC 10,000 cells/mm (1.1 to 1.9) 2 nd -/3 rd -Generation CEPH or β-lactam/ (0.2 to 0.8) β-lactamase inhibitor + macrolide (non-icu) 2 nd -/3 rd -Generation CEPH or β-lactam/ (0.2 to 1.6) β-lactamase inhibitor + macrolide (ICU) Dudas V, et al. Ann Pharmacother. 2000;34:
44 American Thoracic Society 2001 Approach Evaluate prognostic factors and social factors Treat as outpatient Hospitalize patient No CPD, no modifiers CPD and/or modifiers Mild-to-moderate infection (general ward) Severe infection (ICU) No CPD, no modifiers CPD and/or modifiers No risk of P aeruginosa Risk of P aeruginosa American Thoracic Society. Am J Respir Crit Care Med. 2001;163:
45 Pathogens by Disease Severity Outpatient, no modifiers Outpatient, modifiers Hospitalized, general ward Hospitalized, ICU S pneumoniae M pneumoniae C pneumoniae H influenzae < 5% mortality GNB, gram-negative bacilli. a Including drug-resistant pneumococci. S pneumoniae a M pneumoniae C pneumoniae H influenzae Enteric GNB < 5% mortality, 20%hospitalization S pneumoniae a M pneumoniae C pneumoniae H influenzae Enteric GNB Legionella spp Anaerobes 5-25% mortality S pneumoniae a M pneumoniae H influenzae Enteric GNB Legionella spp S aureus P aeruginosa 50% mortality American Thoracic Society. Am J Respir Crit Care Med. 2001;163:
46 Switch from Intravenous to Oral Therapy Guideline criteria for switch to oral therapy: Clinically and hematologically stable Able to tolerate oral drug administration (no gastrointestinal disturbance) Usually appropriate after ~3 days of parenteral therapy Ramirez criteria for switch to oral therapy: Improvement in cough and shortness of breath White blood cells normalizing Afebrile for 8 h No abnormal gastrointestinal absorption Huchon G, et al. Eur Resp Rev. 1998;8: Bartlett JG, et al. Clin Infect Dis. 2000;31: Mandell LA, et al. Clin Infect Dis. 2000;31: American Thoracic Society. Am J Respir Crit Care Med. 2001;163: Ramirez JA. Diagn Microbiol Infect Dis. 1995;22:
47 IV-to-Oral Azithromycin versus Cefuroxime + Erythromycin Vergis et al, 2000 (1) Prospective, comparative, non-blinded, multicenter study at 4 centers in USA ( ) Adults (age 18 years) hospitalized with CAP Two treatment regimens: Azithromycin 500 mg IV od for 2-5 days Azithromycin 500 mg PO od to complete 7-10 days Cefuroxime 750 mg IV tid for 2-7 days + Erythromycin g IV qid for 2-7 days Cefuroxime axetil 500 mg PO bid to complete 7-10 days Erythromycin g PO qid up to 21 days Vergis EN, et al. Arch Intern Med. 2000;160:
48 IV-to-Oral Azithromycin versus Cefuroxime + Erythromycin Vergis et al, 2000 (2) Azithromycin IV then PO 91% Cefuroxime + erythromycin IV then PO 91% Patients (%) P = NS 0 n = 67 n = 78 Clinical cure Vergis EN, et al. Arch Intern Med. 2000;160:
49 IV-to-Oral Azithromycin versus Cefuroxime + Erythromycin Vergis et al, 2000 (4) No. of patients (%) Treatment-related adverse event Azithromycin Cef + ery P All events 8/67 (12%) 38/78 (49%) < Infusion site reactions 4/67 (6%) 28/78 (36%) < Gastrointestinal tract 1/67 (1%) 18/78 (23%) Abnormal liver 5/67 (7%) 2/78 (3%) NS injury markers Ototoxic effects 0/67 (0%) 1/78 (1%) NS Cef + ery, cefuroxime + erythromycin; NS, P > Vergis EN, et al. Arch Intern Med. 2000;160:
50 Activity of 9 oral agents against various bacterial strains MIC 90 (µg/ml) and (%) of strains sensitive at PK/PD breakpoint Agent PK/PD Breakpoint (µg/ml) Penicillin-Susceptible Pneumococci (70 strains) Penicillin-Intermediate Pneumococci (68 strains) Penicillin-Resistant Pneumococci (69 strains) Augmentin 2.00 <0.015(100%) 0.50(100%) 4(90%) Cefpodoxime (97%) 1.00(89%) 4(3%) Cefdinir (97%) 2.00(78%) 8(2%) Cefditoren (99%) 0.25(94%) 1(7%) Cefprozil (97%) 2.00(76%) 16(1%) Cefuroxime (97%) 2.00(85%) 8(0%) Cefixime (90%) >4(40%) >4(0%) Azithromycin (92%) >16(89%) >16(43%) Clarithromycin (94%) >16(84%) >16(45%) Peric M, Browne FA, Jacobs MR et al. Activity if nine oral agents against gram-positive and gram-negative bacteria encountered in community-acquired infections: use of pharmacokinetic / pharmacodynamic breakpoints in the comparative assessment of beta-lactam and macrolide antimicrobial agents. Clin Therap 2003 Jan 25(1):
51 Activity of 9 oral agents against various bacterial strains MIC 90 (µg/ml) and (%) of strains sensitive at PK/PD breakpoint Agent β-lactamase +ve Haemophilus influenza (46 strains) β-lactamase -ve Haemophilus influenza (54 strains) Moraxella catarrhalis (49 strains) Methicillin-Sensitive Stapylococcus aureus (100 strains) Augmentin 2.0(96%) 1.0(100%) 0.06(100%) 0.5(100%) Cefpodoxime 0.06(98%) 0.12(100%) 0.51(94%) 2(3%) Cefdinir 0.50(89%) 1.0(87%) 0.12(100%) 0.25(100%) Cefditoren 0.015(100%) 0.015(100%) 0.25(96%) 0.5(50%) Cefprozil 32(7%) 8(20%) 2(73%) 1.0(99%) Cefuroxime 2(78%) 4(68%) 1.0(90%) 1(91%) Cefixime 0.06(100%) 0.06(100%) 0.12(100%) >4(2%) Azithromycin 2(0%) 2(0%) 0.12(100%) >16(0%) Clarithromycin 16(0%) 16(0%) 0.12(100%) >16(45%) Peric M, Browne FA, Jacobs MR et al. Activity if nine oral agents against gram-positive and gram-negative bacteria encountered in community-acquired infections: use of pharmacokinetic / pharmacodynamic breakpoints in the comparative assessment of beta-lactam and macrolide antimicrobial agents. Clin Therap 2003 Jan 25(1):
52 Pricing Comparison (Oral) Product Presentations Dosage Daily cost Augmentin 375mg tds $4.5 Augmentin 1g bd $5.4 Klacid 250mg bd $5.6 Zinnat 250mg bd $5.5 Unasyn 375mg bd $5.0 Zithromax 250mg od $7.0
53 Pricing Comparison (IV) Product Presentations Dosage Daily cost Augmentin 1.2g Q8H $68 Klacid 500mg Q12H $125 Zinacef 750mg Q8H $62 Unasyn 750mg Q8H $105 Zithromax 500mg Q24H $245
54 Role of Macrolides in Treatment of CAP (1) Inpatients Outpatients Mild Severe ERS 98 Mono Adj* Comb* IDSA 00 Mono* Comb* Comb* CDCP 00 Mono* Comb* Comb* Mono, monotherapy; Adj, optional add-on (adjunctive) therapy; Comb, combination therapy; *, recommended first-line use. Huchon G, et al. Eur Resp Rev. 1998;8: Bartlett JG, et al. Clin Infect Dis. 2000;31: Heffelfinger JD, et al. Arch Intern Med. 2000;160:
55 Rationale for Clinical Use of Azithromycin Broad-spectrum activity Gram-positive respiratory pathogens Gram-negative respiratory pathogens, including β-lactamase producers Highly active against atypical respiratory pathogens High levels in respiratory tissue Infected tissue targeted Tissue levels sustained beyond duration of therapy Simple dosing regimen Once daily 3 days Well tolerated Few drug drug interactions Barry AL, et al. Antimicrob Agents Chemother. 1994;38: Fung-Tomc JC, et al. Antimicrob Agents Chemother. 1995;39: Hammerschlag MR, et al. Antimicrob Agents Chemother. 1992;36: Ishida K, et al. Antimicrob Agents Chemother. 1994;38: Nimmo GR, et al. J Antimicrob Chemother. 1995;36: Schentag JJ, et al. Am J Med. 1991;91(Suppl 3A):S5-S11. Baldwin DR, et al. Eur Resp J. 1990;3:
56 Oral Azithromycin Pooled Analysis Study Designs No. patients Therapy Dose Frequency Duration treated Azithromycin 500 mg od 3 days 299 Clarithromycin 250 mg bid 10 days 164 Roxithromycin 150 mg bid 10 days 53 od, once daily; bid, twice daily. O'Doherty B, et al. Eur J Clin Microbiol Infect Dis. 1998;17(Suppl 2): Rizzato R, et al. Eur Resp J. 1995;8: Pontani D, et al. Program & Abstracts 5th ICMAS, 2000; Seville. Abstract no Schönwald S, et al. Scand J Infect Dis. 1994;26: Schönwald S, et al. Infection. 1999;27:46-50.
57 Clinical success* (% patients) Oral Azithromycin Pooled Analysis Clinical Efficacy Azithromycin (3 days, 500 mg, od) Roxithromycin (10 days, 150 mg, bid) *Cure plus improvement at end of treatment. Clarithromycin (10 days, 250 mg, bid) 97% 93% 94% n = 299 n = 164 n = 53 O'Doherty B, et al. Eur J Clin Microbiol Infect Dis. 1998;17(Suppl 2): Rizzato R, et al. Eur Resp J. 1995;8: Pontani D, et al. Program & Abstracts 5th ICMAS, 2000; Seville. Abstract no Schönwald S, et al. Scand J Infect Dis. 1994;26: Schönwald S, et al. Infection. 1999;27:46-50.
58 Oral Azithromycin Pooled Analysis Bacteriologic Efficacy Bacteriologic success* (% isolates) Azithromycin (3 days, 500 mg, od) 98% n = 80 Clarithromycin (10 days, 250 mg, bid) 91% n = 35 *Eradication or presumed eradication at end of study. O'Doherty B, et al. Eur J Clin Microbiol Infect Dis. 1998;17(Suppl 2): Schönwald S, et al. Infection. 1999;27: Schönwald S, et al. Scand J Infect Dis. 1994;26:
59 100 Oral Azithromycin Pooled Analysis Treatment-Related Adverse Events Azithromycin (3 days, 500 mg, od) Roxithromycin (10 days, 150 mg, bid) Clarithromycin (10 days, 250 mg, bid) 80 Patients (%) % 13% 6% 0 *All treated patients. n = 332 n = 192 n = 53 O'Doherty B, et al. Eur J Clin Microbiol Infect Dis. 1998;17(Suppl 2): Rizzato R, et al. Eur Resp J. 1995;8: Pontani D, et al. Program & Abstracts 5th ICMAS, 2000; Seville. Abstract no Schönwald S, et al. Scand J Infect Dis. 1994;26: Schönwald S, et al. Infection. 1999;27:46-50.
60 IV-to-Oral Azithromycin versus Cefuroxime ± Erythromycin Plouffe et al, 2000 (1) Prospective, comparative, open-label, parallel-group, multicenter study Adults (age 16 years) hospitalized with CAP Two treatment regimens: Azithromycin 500 mg IV od for 2-5 days Cefuroxime 750 mg IV tid for 2-7 days +/ +/ Erythromycin g IV qid for 2-7 days Plouffe J, et al. Antimicrob Agents Chemother. 2000;44: Azithromycin 500 mg PO od to complete 7-10 days Cefuroxime axetil 500 mg PO bid to complete 7-10 days Erythromycin 500 mg PO qid up to 21 days
61 IV-to-Oral Azithromycin versus Cefuroxime ± Erythromycin Plouffe et al, 2000 (2) 100 Azithromycin IV then PO Cefuroxime +/ erythromycin IV then PO Patients (%) % 74% 75% P > 0.05 P > % 20 0 n = 137 n = 131 n = 130 n = days posttherapy 4-6 weeks posttherapy Clinical success Plouffe J, et al. Antimicrob Agents Chemother. 2000;44:
62 IV-to-Oral Azithromycin versus Cefuroxime ± Erythromycin Plouffe et al, 2000 (3) 100 Azithromycin IV then PO Cefuroxime +/ erythromycin IV then PO Patients (%) % 74% 80% 80% 20 0 n = 30 S pneumoniae n = 27 n = 15 H influenzae n = 10 Clinical success Plouffe J, et al. Antimicrob Agents Chemother. 2000;44:
63 IV-to-Oral Azithromycin versus Cefuroxime ± Erythromycin Plouffe et al, 2000 (4) 5 Duration of IV therapy (days) P < Azithromycin (n = 150) Cefuroxime + erythromycin (n = 68) Cefuroxime only (n = 73) Treatment Plouffe J, et al. Antimicrob Agents Chemother. 2000;44: Data on file, Pfizer Inc.
64 IV-to-Oral Azithromycin versus Cefuroxime ± Erythromycin Plouffe et al, 2000 (5) Duration of total therapy (days) Azithromycin (n = 150) P < Cefuroxime + erythromycin (n = 68) 9.2 Cefuroxime only (n = 73) Treatment Plouffe J, et al. Antimicrob Agents Chemother. 2000;44: Data on file, Pfizer Inc.
65 IV-to-Oral Azithromycin versus Cefuroxime ± Erythromycin Plouffe et al, 2000 (6) Plouffe J, et al. Antimicrob Agents Chemother. 2000;44: No. of patients (%) Treatment-related adverse event Azithromycin Cef ± Ery P All events 39 (19%) 49 (24%) NS Diarrhea 11 (5%) 16 (8%) NS Nausea 4 (2%) 16 (8%) Abdominal pain 2 (1%) 2 (1%) NS Vomiting 0 (0%) 4 (2%) NS Insertion site pain 11 (5%) 12 (6%) NS Insertion site infection 7 (3%) 14 (7%) NS or inflammation Cef ± Ery, cefuroxime ± erythromycin; NS, P > 0.05.
66 Case Fatality Rate by Antibiotic Regimen Mufson and Stanek, 1999 Bacteremic pneumococcal pneumonia Number of cases Case fatality rate (%) 50 No. of patients who died No. of patients who lived β-lactam β-lactam + non-macrolide β-lactam + macrolide 0 Mufson MA, Stanek RJ. Am J Med. 1999;107:34S-43S.
67 Effect of Macrolide Inclusion on Length of Hospital Stay 6 Length of stay (days) P = P = P = Yes No (n = 51) (n = 25) Ceftriaxone sodium within first 24 h Yes No (n = 12) (n = 64) Macrolide within first 24 h Yes No (n = 27) (n = 49) Macrolide at any time Stahl JE, et al. Arch Intern Med. 1999;159:
68 Role of Macrolides in Treatment of CAP Broad antimicrobial activity Empiric therapy High drug concentrations Once-daily, 3-day dosing in respiratory tissues (azithromycin only) Monotherapy for mild-tomoderate infections; Use in outpatients combination therapy for and inpatients severe infections Intravenous and oral Simplified IV-to-oral formulations therapy Good safety profile Good compliance Effective combined Potential to reduce with cephalosporin treatment costs
69 Susceptibility to Antibiotic Agents: SENTRY Program, Canada, 1997 Susceptibility (% isolates) a S pneumoniae H influenzae M catarrhalis Agent (n = 151) (n = 74) (n = 28) Penicillin Amoxicillin Amoxi/clav Cefotaxime a Isolates from 8 Canadian centers; susceptibility according to NCCLS break points. Amoxi/clav, amoxicillin/clavulanate. Jones RN, et al. Diagn Microbiol Infect Dis. 2000;37:
Community Acquired Pneumonia: An Update on Guidelines
 Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
National Clinical Guideline Centre Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults
 National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
Control emergence of drug-resistant. Reduce costs
 ...PRESENTATIONS... Guidelines for the Management of Community-Acquired Pneumonia Richard E. Chaisson, MD Presentation Summary Guidelines for the treatment of community-acquired pneumonia (CAP) have been
...PRESENTATIONS... Guidelines for the Management of Community-Acquired Pneumonia Richard E. Chaisson, MD Presentation Summary Guidelines for the treatment of community-acquired pneumonia (CAP) have been
Bai-Yi Chen MD. FCCP
 Treatment strategies for hospitalized versus nonhospitalized CAP patients: Asian perspective Bai-Yi Chen MD. FCCP Professor of Medicine Division of Infectious Disease, Infection Control Team The First
Treatment strategies for hospitalized versus nonhospitalized CAP patients: Asian perspective Bai-Yi Chen MD. FCCP Professor of Medicine Division of Infectious Disease, Infection Control Team The First
Measure Information Form
 Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani
 Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE. Measure Information Form
 Last Updated: Version 3.2a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form Organization Set Measure ID#
Last Updated: Version 3.2a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form Organization Set Measure ID#
Antibiotics in the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease
 Antibiotics in the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease Sung Kyu Kim, M.D.Young Sam Kim, M.D. Department of Internal Medicine Yonsei University College of Medicine,
Antibiotics in the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease Sung Kyu Kim, M.D.Young Sam Kim, M.D. Department of Internal Medicine Yonsei University College of Medicine,
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE. Measure Information Form Collected For: CMS Voluntary Only
 Last Updated: Version 4.4a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form Collected For: CMS Voluntary
Last Updated: Version 4.4a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form Collected For: CMS Voluntary
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
ESISTONO LE HCAP? Francesco Blasi. Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano
 ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa.
 Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
Management of Hospital-acquired Pneumonia
 Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
More than 4 million episodes of communityacquired
 Overview of Recent Guidelines for the Management of Community-Acquired Pneumonia David C. Rhew, MD More than 4 million episodes of communityacquired pneumonia (CAP) occur each year in the United States,
Overview of Recent Guidelines for the Management of Community-Acquired Pneumonia David C. Rhew, MD More than 4 million episodes of communityacquired pneumonia (CAP) occur each year in the United States,
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Pneumonia. Community Acquired Pneumonia (CAP): definition. At least 2 new symptoms
: definition. At least 2 new symptoms") Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Community Acquired Pneumonia (CAP): definition At least 2 new symptoms Fever or hypothermia Cough Rigors
Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Community Acquired Pneumonia (CAP): definition At least 2 new symptoms Fever or hypothermia Cough Rigors
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Bacterial Resistance of Respiratory Pathogens. John C. Rotschafer, Pharm.D. University of Minnesota
 Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Antimicrobial Stewardship in Ambulatory Care
 Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC
 Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance
 Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective
 : The Belgian perspective") ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective Antwerpen 8 november 2002 Yvan Valcke MD PhD AZ Maria Middelares Sint-Niklaas ACUTE EXACERBATIONS of COPD (AE-COPD) Treatment of AECB Role
ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective Antwerpen 8 november 2002 Yvan Valcke MD PhD AZ Maria Middelares Sint-Niklaas ACUTE EXACERBATIONS of COPD (AE-COPD) Treatment of AECB Role
ORIGINAL INVESTIGATION. Associations Between Initial Antimicrobial Therapy and Medical Outcomes for Hospitalized Elderly Patients With Pneumonia
 ORIGINAL INVESTIGATION Associations Between Initial Antimicrobial Therapy and Medical Outcomes for Hospitalized Elderly Patients With Pneumonia Patrick P. Gleason, PharmD; Thomas P. Meehan, MD, MPH; Jonathan
ORIGINAL INVESTIGATION Associations Between Initial Antimicrobial Therapy and Medical Outcomes for Hospitalized Elderly Patients With Pneumonia Patrick P. Gleason, PharmD; Thomas P. Meehan, MD, MPH; Jonathan
Community Acquired Pneumonia. Epidemiology: Acute Lower Respiratory Tract Infections. Community Acquired Pneumonia (CAP) Outline
 Outline") Community Acquired Pneumonia (CAP) Outline Lisa G. Winston, MD University of California, San Francisco Zuckerberg San Francisco General Epidemiology Diagnosis Microbiology Risk stratification Treatment
Community Acquired Pneumonia (CAP) Outline Lisa G. Winston, MD University of California, San Francisco Zuckerberg San Francisco General Epidemiology Diagnosis Microbiology Risk stratification Treatment
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements
 Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
Pharmacokinetics. Absorption of doxycycline is not significantly affected by milk or food, but coadministration of antacids or mineral supplements should be avoided. PDR Drug Summaries are concise point-of-care
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering
 SMC No. (650/10) Bayer Schering") moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Guidelines for Empiric Antimicrobial Prescribing in Community-Acquired Pneumonia*
 special reports Guidelines for Empiric Antimicrobial Prescribing in Community-Acquired Pneumonia* Thomas M. File, Jr, MD, FCCP; Javier Garau, MD; Francesco Blasi, MD, PhD; Christian Chidiac, MD; Keith
special reports Guidelines for Empiric Antimicrobial Prescribing in Community-Acquired Pneumonia* Thomas M. File, Jr, MD, FCCP; Javier Garau, MD; Francesco Blasi, MD, PhD; Christian Chidiac, MD; Keith
Community-Acquired Pneumonia. Community-Acquired Pneumonia. Community Acquired Pneumonia (CAP): definition
: definition") Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Community-Acquired Pneumonia Talk will focus on adults Guideline for healthy infants
Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Community-Acquired Pneumonia Talk will focus on adults Guideline for healthy infants
Antibiotics Use And Concordance To Guidelines For Patients Hospitalized With Community Acquired Pneumonia (CAP)
") Antibiotics Use And Concordance To Guidelines For Patients Hospitalized With Community Acquired Pneumonia (CAP) SF Teoh 1, Samsinah Hussain 1, CK Liam 2 1 Departments of Pharmacy, Faculty of Medicine,
Antibiotics Use And Concordance To Guidelines For Patients Hospitalized With Community Acquired Pneumonia (CAP) SF Teoh 1, Samsinah Hussain 1, CK Liam 2 1 Departments of Pharmacy, Faculty of Medicine,
Int.J.Curr.Microbiol.App.Sci (2017) 6(3):
 6(3):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
CLINICAL PROTOCOL FOR COMMUNITY ACQUIRED PNEUMONIA. SCOPE: Western Australia. CORB score equal or above 1. All criteria must be met:
 CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Community Acquired Pneumonia (CAP)
") Community Acquired Pneumonia (CAP) The following guidelines have been developed to aid clinicians in the investigation and management of patients with CAP at the Royal Liverpool University Hospital (RLUH).
Community Acquired Pneumonia (CAP) The following guidelines have been developed to aid clinicians in the investigation and management of patients with CAP at the Royal Liverpool University Hospital (RLUH).
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007
 Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia. Po-Ren Hsueh. National Taiwan University Hospital
 Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship
 Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Antimicrobial Cycling. Donald E Low University of Toronto
 Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
ESCMID Online Lecture Library. by author
 Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Outpatient Antimicrobial Therapy. Role of Antibacterials in Outpatient Treatment of Respiratory Tract Infection. Acute Bacterial Rhinosinusitis
 Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Outpatient Antimicrobial Therapy B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy University of California San Francisco Role of Antibacterials in Outpatient Treatment
Objectives 4/26/2017. Co-Investigators Sadie Giuliani, PharmD, BCPS Claude Tonnerre, MD Jayme Hartzell, PharmD, MS, BCPS
 IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
Fluoroquinolones in 2007: the Angels, the Devils, and What Should the Clinician Do?
 Fluoroquinolones in 2007: the Angels, the Devils, and What Should the Clinician Do? David C. Hooper, M.D. Division of Infectious Diseases Infection Control Unit Massachusetts General Hospital Harvard Medical
Fluoroquinolones in 2007: the Angels, the Devils, and What Should the Clinician Do? David C. Hooper, M.D. Division of Infectious Diseases Infection Control Unit Massachusetts General Hospital Harvard Medical
Infectious Disease Update 2017
 Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days
 Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Antibiotics & treatment of Acute Bcterial Sinusitis. Walid Reda Product Manager. Do your antimicrobial options meet your needs?
 Antibiotics & treatment of Acute Bcterial Sinusitis Walid Reda Product Manager Do your antimicrobial options meet your needs? Antimicrobial Effects: What s involved? Effect in Humans: Serum concentration
Antibiotics & treatment of Acute Bcterial Sinusitis Walid Reda Product Manager Do your antimicrobial options meet your needs? Antimicrobial Effects: What s involved? Effect in Humans: Serum concentration
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
Community-acquired pneumonia: Time to place a CAP on length of treatment?
 LOGIN TO LEARN: An Engaging and Interactive Journal Club for Pharmacists and Students Community-acquired pneumonia: Time to place a CAP on length of treatment? Jennifer Ball, PharmD Learning Objectives
LOGIN TO LEARN: An Engaging and Interactive Journal Club for Pharmacists and Students Community-acquired pneumonia: Time to place a CAP on length of treatment? Jennifer Ball, PharmD Learning Objectives
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Safety of an Out-Patient Intravenous Antibiotics Programme
 Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Sustaining an Antimicrobial Stewardship
 Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children
 Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
ORIGINAL INVESTIGATION. Doxycycline Is a Cost-effective Therapy for Hospitalized Patients With Community-Acquired Pneumonia
 ORIGINAL INVESTIGATION Doxycycline Is a Cost-effective Therapy for Hospitalized Patients With Community-Acquired Pneumonia Reba K. Ailani, MD; Gautami Agastya, MD; Rajesh K. Ailani, MD; Beejadi N. Mukunda,
ORIGINAL INVESTIGATION Doxycycline Is a Cost-effective Therapy for Hospitalized Patients With Community-Acquired Pneumonia Reba K. Ailani, MD; Gautami Agastya, MD; Rajesh K. Ailani, MD; Beejadi N. Mukunda,
Hospital-acquired pneumonia (HAP) is the second
 is the second") Guidelines and Critical Pathways for Severe Hospital-Acquired Pneumonia* Stanley Fiel, MD, FCCP Hospital-acquired pneumonia (HAP) is associated with high morbidity and mortality. Early, appropriate, and
Guidelines and Critical Pathways for Severe Hospital-Acquired Pneumonia* Stanley Fiel, MD, FCCP Hospital-acquired pneumonia (HAP) is associated with high morbidity and mortality. Early, appropriate, and
ß-lactams. Sub-families. Penicillins. Cephalosporins. Monobactams. Carbapenems
 β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
Antimicrobial treatment of community acquired pneumonia in adults: A conference report
 CONSENSUS CONFERENCE Antimicrobial treatment of community acquired pneumonia in adults: A conference report THE CANADIAN COMMUNITY ACQUIRED PNEUMONIA CONSENSUS CONFERENCE GROUP C OMMUNLTY ACQUIRED PNEUMONI
CONSENSUS CONFERENCE Antimicrobial treatment of community acquired pneumonia in adults: A conference report THE CANADIAN COMMUNITY ACQUIRED PNEUMONIA CONSENSUS CONFERENCE GROUP C OMMUNLTY ACQUIRED PNEUMONI
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles
 Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550
 and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550") Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550 Sinusitis Upper respiratory tract infections (URI) Common cold
Rational use of antibiotic in upper respiratory tract infection (URI) and community acquired pneumonia รศ.จามร ธ รตก ลพ ศาล 23 พฤษภาคม 2550 Sinusitis Upper respiratory tract infections (URI) Common cold
جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی
 جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی ویرایش دوم بر اساس ed., 2017 CLSI M100 27 th تابستان ۶۹۳۱ تهیه
جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی ویرایش دوم بر اساس ed., 2017 CLSI M100 27 th تابستان ۶۹۳۱ تهیه
Choosing an Antibiotic
 Principles of Antibiotic Use - The 6 Step Plan Robin J Green MBBCh, DCH, FC Paed, DTM&H, MMed, FCCP, PhD, Dip Allergy, FAAAAI Department of Paediatrics and Child Health 1 Choosing an Antibiotic Disease/Site
Principles of Antibiotic Use - The 6 Step Plan Robin J Green MBBCh, DCH, FC Paed, DTM&H, MMed, FCCP, PhD, Dip Allergy, FAAAAI Department of Paediatrics and Child Health 1 Choosing an Antibiotic Disease/Site
Community-Acquired Pneumonia Current & Future State
 Community-Acquired Pneumonia Current & Future State Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial relationships to
Community-Acquired Pneumonia Current & Future State Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial relationships to
Considerations in antimicrobial prescribing Perspective: drug resistance
 Considerations in antimicrobial prescribing Perspective: drug resistance Hasan MM When one compares the challenges clinicians faced a decade ago in prescribing antimicrobial agents with those of today,
Considerations in antimicrobial prescribing Perspective: drug resistance Hasan MM When one compares the challenges clinicians faced a decade ago in prescribing antimicrobial agents with those of today,
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how?
 Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Community-acquired pneumonia (CAP) is a common,
 is a common,") OUTCOMES IN PRACTICE A Tool for Appropriate Antibiotic Use in the Management of Community-Acquired Pneumonia Alan B. Bernstein, MD, MPH, Thomas M. File Jr, MD, and Jeffrey S. Markowitz, DrPH Community-acquired
OUTCOMES IN PRACTICE A Tool for Appropriate Antibiotic Use in the Management of Community-Acquired Pneumonia Alan B. Bernstein, MD, MPH, Thomas M. File Jr, MD, and Jeffrey S. Markowitz, DrPH Community-acquired
Optimising antibiotic policies in the Netherlands, part VIII. Revised SWAB Guidelines for antimicrobial therapy of Community-acquired pneumonia
 Optimising antibiotic policies in the Netherlands, part VIII Revised SWAB Guidelines for antimicrobial therapy of Community-acquired pneumonia Dutch Working Party on Antibiotic Policy (SWAB), April 2005
Optimising antibiotic policies in the Netherlands, part VIII Revised SWAB Guidelines for antimicrobial therapy of Community-acquired pneumonia Dutch Working Party on Antibiotic Policy (SWAB), April 2005
Scottish Medicines Consortium
 Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP)
") IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES
 AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham