Richard A. Jacobs, M.D., PhD.
|
|
|
- Britney Payne
- 5 years ago
- Views:
Transcription


 Environmental exposures Role of cultures")


1 Richard A. Jacobs, M.D., PhD. Location of infx may help define bacteriology Primary infx (breach of intact skin) usually monomicrobial; Secondary infx (pre-existing abnormality) often polymicrobial Impaired immunity -- rapidly progressive (requiring early and aggressive Rx) and can be due to unusual organisms (procedures to define etiology more important) Environmental exposures Role of cultures Location of infx may help define bacteriology Primary infx (breach of intact skin) usually monomicrobial; Secondary infx (pre-existing abnormality) often polymicrobial Impaired immunity -- rapidly progressive (requiring early and aggressive Rx) and can be due to unusual organisms (procedures to define etiology more important) Environmental exposures Role of cultures
 M.")


 and not")

")

 Indicated for: Failure to respond Immunocompromised Suspect deep tissue")
2 Mycobacterial (M. fortuitum) furunculosis assoc. with footbaths at nail salon M. chelonae cellulitis assoc with face lifts (methylene blue) M. abscessus infections assoc with cosmetic surgery in the Dominican Republic Pseudomonas Hot-Foot Syndrome assoc. with wading pools with abrasive grit on floor Aeromonas hydrophilia wound infections associated with mud football. Hot Tub Lung due to Mycobacterium avium complex in otherwise healthy individuals Tropical Diabetic Hand Syndrome seen in tropical areas (usually Africa/India, but also US) and not assoc with vascular disease or periphral neuropathy --Staph and strep most common, but mixed infections occur Location of infx may help define bacteriology Primary infx (breach of intact skin) usually monomicrobial; Secondary infx (pre-existing abnormality) often polymicrobial Impaired immunity -- rapidly progressive (requiring early and aggressive Rx) and can be due to unusual organisms(procedures to define etiology more important) Environmental exposures Role of cultures Diagnosis usually made clinically Culture of leading edge -- positive in 15-40%, especially those with underlying diseases (diabetes, malignancy) Indicated for: Failure to respond Immunocompromised Suspect deep tissue infections (myositis, fasciitis) Blood Cultures 757 pts with cellulitis; 553 with 710 BC s Only 11(1.6%) positive -- most ß- hemolytic strep; one with vibrio and one with Morganella Low yield, did not change therapy or outcome and expensive





3 Literature does not address: Immunocompromised patients Patients with multiple co-morbidities Unusual exposures Complicated soft tissue infections (myositis,fasciitis) Superficial and deep venous thrombosis Contact dermatitis Insect stings/tick bites Fixed drug eruptions Hydradenitis suppurativa Erythema nodosum Panniculitis Sweet syndrome Pyoderma Gangrenosum A 66 year old woman with chronic LE edema secondary to CHF presents with the acute onset of a red, warm swollen and tender left foot. Erythema and tenderness extend to the mid-tibial area. What is the diagnosis? What is the bacterial etiology? What is appropriate therapy?
 Hospital-associated -- may include gram-neg organisms (E.")

 cultures, 9 were S.")
 FNA or Bx of cellulitis in ED Of 11 (+) cultures, 7 S.")
 cultures, 7 were S.")
4 Outpatient -- Usually caused by Strep. pyogenes (Gp A strep); less commonly by S. aureus and rarely by other strep (gp B,C,G) Hospital-associated -- may include gram-neg organisms (E.coli, klebs, pseudomonas, enterobacter) as well as staph (including MRSA) and strep Decubitus/Diabetic/Vascular Ulcers -- polymicrobial including staph, strep, enterococcus, enteric gram-negatives, pseudomonas, anaerobes Animal Bites -- Pasteurella multocida (< 24hours); staph, strep, mouth anaerobes later Human Bites -- aerobic and anaerobic mouth flora as well as Eikenella corrodens How common is S.aureus? FNA of patients with cellulitis in walk-in ED Of 26 (+) cultures, 9 were S. aureus (Scand J Infect Dis 1989;21:537) FNA of patients with cellulitis admitted to teaching hospital Of 33 (+) cultures, 11 were S. aureus (Arch Int Med 1988;148:2451) FNA or Bx of cellulitis in ED Of 11 (+) cultures, 7 S. aureus (Arch Int Med 1986;146:295) How common is S. aureus? FNA or Bx of patients with cellulitis admitted to the hospital Of 8 (+) cultures, 7 were S. aureus (Arch Int Med 1989;149:293) FNA of cellulitis in Pediatric Acute Care Clinic Of 9 (+) cultures, 6 were S. aureus (Pediatr Infect Dis J 1987;6:685) THE WAY IT WAS Gp A strep + MSSA = dicloxacillin or cephalexin (Keflex ) THE WAY IT IS Gp A strep +?? MRSA
5 TMP-SMX (95-100%); doxy/minocycline (90-95%); clindamycin (85-95%) are active against CA-MRSA TMP-SMX and doxy/mino +/- against gp A strep If use these must add ß-lactam [PCN, Amox, 1 st gen ceph (Keflex )] Clinda active against gp A strep Outpatient Dicloxacillin or Keflex IF low prevalence of CA-MRSA TMP-SMX or doxy/mino + ß-lactam Clindamycin Duration of therapy Standard 7-14days Recent data suggests 5 days as good as 10 days Hospital-associated Vancomycin +/- a third generation cephalosporin * IDSA guidelines on Rx of S&ST infections--summer of 2009 Purulent wounds and cellulitis with purulent drainage--50% caused by CA-MRSA Treatment should include MRSA Clindamycin TMP-SMX/doxycycline + ß-lactam PURE CELLULITIS (without purulent drainage or abscess) The role of CA-MRSA is unknown; in addition to coverage for ß-hemolytic streptococci, empiric therapy for CA-MRSA may be considered CELLULITIS WITH PURULENT DRAINAGE Empiric therapy for CA-MRSA is recommended A 10 year old boy is in the park with friends. As he goes after a ball, he passes close to a dog that was resting in the shade. The dog jumps up, chases the boy and bites him on the leg inflicting several puncture wounds on the calf. The father, who was supposed to be closely monitoring the boy, calls in a panic and wants to know what to do. Is it a high risk bite that requires prophylactic antibiotics? If so, which one and for how long?




6 1. Dog 2. Cat 3. Human 4. Monkey 5. Pig ANIMAL LITERATURE UCSF CAT 30-50% 50% HUMAN 15-30% 16% DOG 2-4% 4% HIGH RISK LOW RISK ANIMAL LOCATION OF WOUND TYPE OF WOUND INTERVAL BETWEEN BITE TO OBTAINING MEDICAL CARE Biting species Cat Pig Human Primate Wound Location Hand Over a joint Foot Through-and-through oral Wound Type Puncture Dirty Crush Old Patient Elderly Asplenic Alcoholic Diabetic Steroids PVD Dog Rodent Face Scalp Mucosal Clean Recent Abrasion/Open POLYMICROBIAL Median of 5 isolates per culture 56% aerobic and anaerobic 36% aerobic only 1% anaerobic only 7% now growth PASTEURELLA MOST COMMON ISOLATE 50% of dog bites and 75% of cat bites STREPTOCOCCI, STAPHYLOCOCCI, MORAXELLA AND NEISSSERIA MOST COMMON AEROBES FUSOBACTERIUM, BACTEROIDES, PORPHYROMONAS AND PREVOTELLA MOST COMMON ANAEROBES
7 PASTEURELLA GNR Susceptible to PCN and its derivatives, 2nd and 3rd generation cephalosporins, tetracyclines, quinolones and TMP-SMX NOT SENSITIVE TO DRUGS OFTEN USED TO TREAT CELLULITIS--1st generation cephalosporins, penicillinase-resistant penicillins, clindamycin, erythromycin ANAEROBES Often produce ß-lactamase NOT WELL STUDIED no consensus tendency is to be liberal High risk animal cat, human, primate High risk type puncture, crush High risk location hand foot,face High risk individual splenectomy,dm, immunocompromised, prednisone CHOICE OF ANTIBIOTICS For simplicity would favor Augmentin in most cases, even though less expensive more narrow spectrum regimens might work Duration 5 days COMBINATION ß-LACTAM + ß-LACTAMASE INHIBITOR Unasyn (ampicillin + sulbactam) Timentin (ticarcillin + clavulanic acid) Zosyn (piperacillin + tazobactam) Augmentin (amoxicillin + clavulanic acid) 2nd GENERATION CEPHALOSPORIN WITH ANAEROBIC ACTIVITY Cefoxitin CLINDAMYCIN + FlUOROQUINOLONE CARBAPENEM--ERTAPENEM THREE TYPES Clenched Fist Injury (CFI) % infx rate and often assoc with fx, septic arthritis, osteo, tendon rupture Occlusive bites (non-cfis) -- low risk of infection similar to that of lacerations (5%) if superficial; if deep, similar to CFI Self-inflicted bites (oral and mucocutaneous) --oral low risk of infection; through-and through or mucocutaneous injuries have about 30% infection rate POLYMICROBIAL 4 isolates/wound--3 aerobes and 1 anaerobe 54% aerobic + anaerobic 44% aerobic 2% anaerobic
--most common Eikenella part of normal oral flora Sensitive")



 Zosyn (piperacillin + tazobactam) Augmentin")

8 Streptococci (84%), staphylococci (54%) and Eikenella corrodens (30%)--most common Eikenella part of normal oral flora Sensitive to PCN, 2nd and 3rd generation cephalosporins, quinolones, TMP-SMX Others--Haemophilus, corynebacterium, neisseria, gamella Prevotella, fusobacterium, veillonella, peptostreptococcus-- often produce ß- lactamase NOT WELL STUDIED High Risk Bites Bites to the hand Through-and-through mucosal bites Augmentin reasonable choice for 5 days COMBINATION ß-LACTAM + ß-LACTAMASE INHIBITOR Unasyn (ampicillin + sulbactam) Timentin (ticarcillin + clavulanic acid) Zosyn (piperacillin + tazobactam) Augmentin (amoxicillin + clavulanic acid) 2nd GENERATION CEPHALOSPORIN WITH ANAEROBIC ACTIVITY Cefoxitin CLINDAMYCIN + FlUOROQUINOLONE CARBAPENEM--ERTAPENEM
 but can occur in adults Predisposing factors include warm climate, crowding, poor")

 can occur Heals slowly with depigmentation Dx by appearance; if any doubt can culture 1st generation")
 less effective -- fail to eradicate skin")
 Bimodal distribution --")
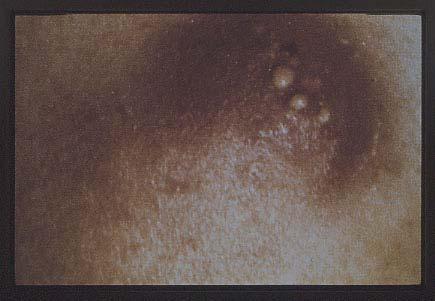
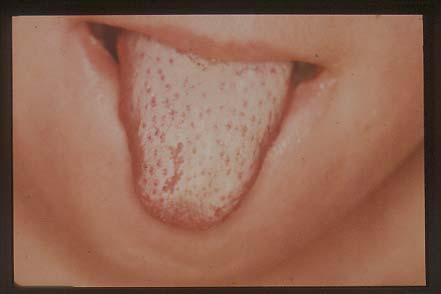
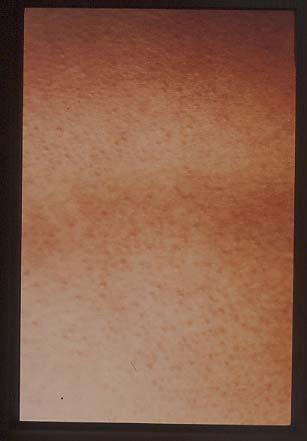
9 Caused by gp A strep (rarely gp B,C and G) and S. aureus Disease of children (age 2-5) but can occur in adults Predisposing factors include warm climate, crowding, poor hygiene-- inoculation of organism from colonized skin into abrasions, insect bites,etc Papule > evanescent vesicle > pustule that enlarges > breaks down over 4-6 days > seropurulent discharge that dries to form typical thick golden-yellow crust Superinfection (S. aureus) can occur Heals slowly with depigmentation Dx by appearance; if any doubt can culture 1st generation cephalosporin (Keflex ), penicillinase-resistant penicillin (dicloxacillin) or amoxicillin-clavulanic acid (Augmentin ) Clindamycin for penicillin allergic patient Topical antibiotics (mupirocin) less effective -- fail to eradicate skin colonization or prevent new lesion formation Non-suppurative complication -- poststreptococcal GN Antibiotics do NOT prevent GN Rheumatic fever not reported Caused by gp A strep (occasionally other gps) Bimodal distribution -- infants/children and older adults Usually face and extremities; abdomen if assoc with surgery Painful, raised, erythematous, rapidly spreading lesion with well demarcated edges Systemic symptoms common



, fever, elevation of")


 Carbuncles")
10 Infection of the submandibular space, usually associated with dental extraction Caused by oral flora -- aerobic and anaerobic strep, fusobacterium, bacteroides spp Acute onset with brawny, painful edema ( bull-neck appearance ), fever, elevation of tongue with drooling and dysphagia Maintain airway Antibiotics --PCN +flagyl or clindamycin Surgery if abscess forms or fails to respond in several days Folliculitis Furunculosis (boils) Carbuncles (coalescent boils) Recurrent furunculosis





11


 Rx = Vitamin C 1 gram/day X 4-6 weeks Result = clinical improvement and improvement in neutrophil function Conclusion: Lazy")

12 Increasing frequency Most commonly due to MRSA Pathogenesis: Nasopharyngeal colonization Skin colonization (axilla, groin,perirectal) 25% continuously colonized 50% intermittently colonized 25% never colonized Treatment--eradicate colonization Lack of evidence-based data The role of decolonization in preventing recurrent infection is unclear and more data is needed to establish efficacy and identify optimal regimens Emphasize personal hygiene Decolonization can be considered in selected cases--recurrent infections despite good hygiene Recommend nasal Mupirocin and body decolonization with chlorhexidine baths ORAL ANTIBIOTICS ARE NOT ROUTINELY RECOMMENDED My personal approach TMP-SMX DS BID + Rifampin 300mg BID X 5 days--repeat every 6 weeks for 8 courses Hibiclens 2 X per week Personal Hygiene Clothes daily Towels Q 3 days Sheets Q week Vitamin C Patients with recurrent furunculosis Negative nasopharyngeal cultures Neutrophil dysfunction (chemotaxis, phagocytosis, superoxide generation) Rx = Vitamin C 1 gram/day X 4-6 weeks Result = clinical improvement and improvement in neutrophil function Conclusion: Lazy Leukocytes -- transient neutrophil dysfunction improved by vitamin C, perhaps through its antioxidant effect A 25 y.o. previously healthy farm worker sustained trauma to his penis 2 days prior to admission. He presented to a local ED where he was found to have a small necrotic area on his penis that progressed while he was in the ED. He was given a dose of ceftriaxone and transferred to UCSF.





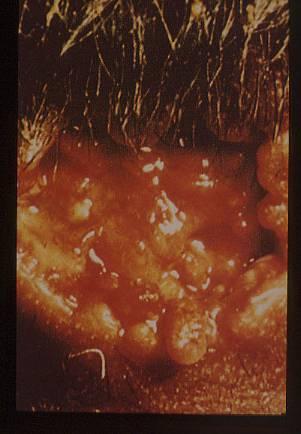
13 What is the diagnosis? What is the bacteriology? What is appropriate therapy? Type I Anaerobes (peptostreptococcus, bacteroides, anaerobic/microaerophilic streptococci) Enteric gram-negative bacilli (E. coli, klebsiella, proteus, serratia, etc) Type II (hemolytic streptococcal gangrene) Group A streptococcus + S. aureus
 Pain/Swelling Exudate")

 Systemic symptoms/signs out of proportion to local findings Anesthesia of involved area A 50 y/o faculty")

14 Progressive Bacterial Synergistic Gangrene Synergistic Necrotizing Cellulitis Gas Gangrene Necrotizing Cutaneous Mucormycosis Anaerobic Cellulitis Fournier s Gangrene Incubation Period Onset (gradual/acute) Pain/Swelling Exudate (Thin/Thick/Dark/SS/Purule nt/seropurulent/dishwater Gas Odor (Sour/Sweet) Consider polymicrobial Broad spectrum antibiotics Vancomycin + flagyl + tobramycin Flagyl + 3rd generation cephalosporin ß-lactam + ß-lactamase inhibitor + tobramycin Carbapenem Surgery High risk patient -- diabetes, trauma, surgery Wound necrosis Gas Exudate (foul smelling) Systemic symptoms/signs out of proportion to local findings Anesthesia of involved area A 50 y/o faculty member 4 months prior Cactus fell on hand ED for removal of spines Rx = Augmentin X 7 days 3 months prior - pain in index finger 3 weeks prior - pustule with drainage and nodular lymphangitis No systemic symptoms and not immunocompromised


 Mycobacterium marinum")


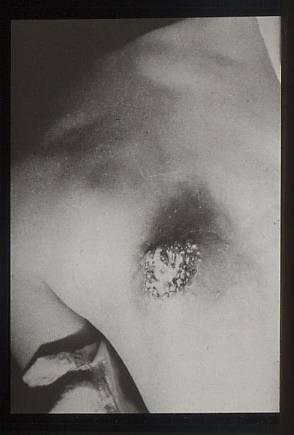
15 ORGANISM Gp A streptoccocus S. aureus Pasteurella multocida Spirillium minor Filariasis FREQUENCY Common Occasional Occasional Rare Rare What is the diagnosis? Common causes Sporothrix schenckii Nocardia (brasiliensis>asteroides) Mycobacterium marinum Francisella tularensis Leishmania species Less common causes Fungi - cocci, crypto, histo, blasto Mycobacteria - chelonae, kansasii, aviumintracellulare, tuberculosis Bacteria - S. aureus, gp A strep, Pseudomonas pseudomallei, Bacillus anthracis







16




17





18 Schwartz MN. Cellulitis. N Engl J Med 2004;350:904 Baddour LM. Recent considerations in recurrent cellulitis. Current Infect Dis Reports 2001;3:461 Bisno AL and Stevens DL. Streptococcal infections of skin and soft tissues. N Engl J Med 1996;334:240 Smego RA et al. Lymphocutaneous Syndrome-A review of non-sporothrix causes. Medicine 1999;78:38 Stevens DL et al Practice guidelines for the diagnosis and management of skin and soft tissue infections. Clin Infect Dis 2005;41:1373 Anaya DA, Dellinger EP. Necrotizing soft-tissue infection: diagnosis and management. Clin Infect Dis 2007;44:705 Chambers HF et al. Management of skin and soft-tissue infections. N Engl J Med 2008;359:1063 Singer AJ, Dagum AB. Current management of acute cutaneous wounds. N Engl J Med 2008;359:1037
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Overview Management of Skin and Soft Tissue Infections in the MRSA Era
 Overview Management of Skin and Soft Tissue Infections in the MRSA Era April 2011 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Management of Recurrent SSTIs Necrotizing soft
Overview Management of Skin and Soft Tissue Infections in the MRSA Era April 2011 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Management of Recurrent SSTIs Necrotizing soft
Skin & Soft Tissue Infections (SSTIs)
") Skin & Soft Tissue Infections (SSTIs) Marnie Peterson, Pharm.D., Ph.D. College of Pharmacy peter377@umn.edu (612) 626-4388 SSTIs Objectives To classify types of skin infections To present a case of cellulitis
Skin & Soft Tissue Infections (SSTIs) Marnie Peterson, Pharm.D., Ph.D. College of Pharmacy peter377@umn.edu (612) 626-4388 SSTIs Objectives To classify types of skin infections To present a case of cellulitis
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Copyright 2012 Diabetes In Control, Inc. For permission to reprint, please contact Heather Moran, Production Editor, at
 Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
Cellulitis. Assoc Prof Mark Thomas. Conference for General Practice Auckland Saturday 28 July 2018
 Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Dirty Wounds. Christopher M. Ziebell, MD, FACEP
 Dirty Wounds Christopher M. Ziebell, MD, FACEP Types Fresh Water Salt Water Bites Cats Humans Dogs and other mammals Freshwater Trauma Recognize this finger? Lindsey Lohan Microbiology Usual suspects:
Dirty Wounds Christopher M. Ziebell, MD, FACEP Types Fresh Water Salt Water Bites Cats Humans Dogs and other mammals Freshwater Trauma Recognize this finger? Lindsey Lohan Microbiology Usual suspects:
5/26/10. Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis Animal bites Unusual skin and soft tissue infections
 Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis
Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
THERAPY OF ANAEROBIC INFECTIONS LUNG ABSCESS BRAIN ABSCESS
 THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
A. Incision and drainage alone B. Incision and drainage plus oral anti-mrsa antimicrobial agent C. Oral anti-mrsa antimicrobial agent
 Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Necrotizing fasciitis Animal bites Other skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor
Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs) Necrotizing fasciitis Animal bites Other skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Risk factors? Insect bites? Hygiene? Household crowding Health literacy
 Recurrent boils Commonest sites face, neck, armpits, shoulders, and buttocks (bottom) infection of the hair root or sweat pore Occur in otherwise healthy people (higher rates in diabetics, eczema, iron
Recurrent boils Commonest sites face, neck, armpits, shoulders, and buttocks (bottom) infection of the hair root or sweat pore Occur in otherwise healthy people (higher rates in diabetics, eczema, iron
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections
 Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Secondary bacterial infections complicating skin lesions
 J. Med. Microbiol. Vol. 51 (2002), 808 812 # 2002 Society for General Microbiology ISSN 0022-2615 REVIEW ARTICLE Secondary bacterial infections complicating skin lesions ITZHAK BROOK Department of Pediatrics,
J. Med. Microbiol. Vol. 51 (2002), 808 812 # 2002 Society for General Microbiology ISSN 0022-2615 REVIEW ARTICLE Secondary bacterial infections complicating skin lesions ITZHAK BROOK Department of Pediatrics,
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
Antimicrobial Susceptibility Testing: Advanced Course
 Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
number Done by Corrected by Doctor Dr.Malik
 number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
Disclosures. Consider This Case. Objectives. Consequences of Bites. Animal Bites: What to Do and What to Avoid. Animal Bites: Epidemiology
 Animal Bites: What to Do and What to Avoid Meg Fisher, MD Medical Director Disclosures I have no disclosures I do not plan to discuss off label uses of drugs Objectives Manage a child who is bitten Discuss
Animal Bites: What to Do and What to Avoid Meg Fisher, MD Medical Director Disclosures I have no disclosures I do not plan to discuss off label uses of drugs Objectives Manage a child who is bitten Discuss
Diagnosis and Management of Skin and Soft-tissue Infections
 Diagnosis and Management of Skin and Soft-tissue Infections Skin and soft tissue infections (SSTIs), are referred as skin and skin structure infections. These infections also represent a group of infections
Diagnosis and Management of Skin and Soft-tissue Infections Skin and soft tissue infections (SSTIs), are referred as skin and skin structure infections. These infections also represent a group of infections
Replaces:04/14/16. Formulated: 1997 SKIN AND SOFT TISSUE INFECTION
 Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antimicrobials. Antimicrobials
 Antimicrobials For more than 50 years, antibiotics have come to the rescue by routinely producing rapid and long-lasting miracle cures. However, from the beginning antibiotics have selected for resistance
Antimicrobials For more than 50 years, antibiotics have come to the rescue by routinely producing rapid and long-lasting miracle cures. However, from the beginning antibiotics have selected for resistance
4/28/11. Update: 2011 IDSA MRSA Treatment Guidelines. Necrotizing fasciitis Animal bites Other skin and soft tissue infections
 Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs)
Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Update: 2011 IDSA MRSA Treatment Guidelines Skin and soft tissue infections (SSTIs)
Objectives. Impetigo 8/6/2013
 Bacterial Infections E.J. Mayeaux, Jr., M.D. Professor of Family Medicine Professor of Obstetrics & Gynecology Louisiana State University Health Sciences Center Shreveport, LA No disclosures to report.
Bacterial Infections E.J. Mayeaux, Jr., M.D. Professor of Family Medicine Professor of Obstetrics & Gynecology Louisiana State University Health Sciences Center Shreveport, LA No disclosures to report.
Skin and Soft Tissue Infections Emerging Therapies and 5 things to know
 2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
2015 Antibiogram. Red Deer Regional Hospital. Central Zone. Alberta Health Services
 2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
Basic principles of antibiotic use
 Basic principles of antibiotic use Michal Holub Department of Infectious Diseases First Faculty of Medicine Charles University and Military University Hospital, Prague 1. Is antibiotical treatment indicated
Basic principles of antibiotic use Michal Holub Department of Infectious Diseases First Faculty of Medicine Charles University and Military University Hospital, Prague 1. Is antibiotical treatment indicated
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Annual U.S. ED Visits for Skin and Soft Tissue Infections,
 Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis Animal bites Unusual skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious
Abscess, cellulitis Recurrent skin and soft tissue infections Necrotizing fasciitis Animal bites Unusual skin and soft tissue infections Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
S aureus infections: outpatient treatment. Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium
 S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
Cell Wall Weakeners. Antimicrobials: Drugs that Weaken the Cell Wall. Bacterial Cell Wall. Bacterial Resistance to PCNs. PCN Classification
 Cell Wall Weakeners Antimicrobials: Drugs that Weaken the Cell Wall Beta Lactams Penicillins Cephalosporins Carbapenems Aztreonam Vancomycin Teicoplanin Bacterial Cell Wall Bacterial cytoplasm is hypertonic
Cell Wall Weakeners Antimicrobials: Drugs that Weaken the Cell Wall Beta Lactams Penicillins Cephalosporins Carbapenems Aztreonam Vancomycin Teicoplanin Bacterial Cell Wall Bacterial cytoplasm is hypertonic
Symptoms of cellulitis (n=396) %
 %") Cellulitis and lymphoedema Vaughan Keeley May 2012 What is cellulitis? - also called erysipelas, acute inflammatory episodes etc. - bacterial infection of skin + subcutaneous tissues - more common in people
Cellulitis and lymphoedema Vaughan Keeley May 2012 What is cellulitis? - also called erysipelas, acute inflammatory episodes etc. - bacterial infection of skin + subcutaneous tissues - more common in people
InPHARMation. Pharmacy and Therapeutics Committee Update May 23 rd, 2018 Meeting
 VOLUME FOUR; ISSUE 5 May 23, 2018 Edited by: Gregory K. Perry, PharmD, BCPS-AQID InPHARMation Pharmacy and Therapeutics Committee Update May 23 rd, 2018 Meeting The Pharmacy and Therapeutics Committee
VOLUME FOUR; ISSUE 5 May 23, 2018 Edited by: Gregory K. Perry, PharmD, BCPS-AQID InPHARMation Pharmacy and Therapeutics Committee Update May 23 rd, 2018 Meeting The Pharmacy and Therapeutics Committee
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS
 Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship
 Curriculum for Antimicrobial Stewardship") General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
Antimicrobial susceptibility
 Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
** the doctor start the lecture with revising some information from the last one:
 Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Chapter 61 Mammalian Bites
 Chapter 61 Mammalian Bites Episode Overview: 1. List 5 pathogens responsible for infection from dog bite 2. List 4 risk factors for overwhelming sepsis from dog bite 3. What first line antibiotic is a
Chapter 61 Mammalian Bites Episode Overview: 1. List 5 pathogens responsible for infection from dog bite 2. List 4 risk factors for overwhelming sepsis from dog bite 3. What first line antibiotic is a
Tropical infections caused by Staphylococcus aureus
 Tropical infections caused by Staphylococcus aureus Michael Ellis, MD Infectious Diseases Division Uniformed Services University of the Health Sciences February 2015 Introduction Tropical Pyomyositis Cutaneous
Tropical infections caused by Staphylococcus aureus Michael Ellis, MD Infectious Diseases Division Uniformed Services University of the Health Sciences February 2015 Introduction Tropical Pyomyositis Cutaneous
The Bug Stops Here: Treating Resistant Staph Infections Holly Roberts, DVM, MS, DACVD Blue Pearl Veterinary Specialists San Antonio, TX
 The Bug Stops Here: Treating Resistant Staph Infections Holly Roberts, DVM, MS, DACVD Blue Pearl Veterinary Specialists San Antonio, TX 1. Staphylococcus bacteria a. Gram positive b. Opportunistic pathogens
The Bug Stops Here: Treating Resistant Staph Infections Holly Roberts, DVM, MS, DACVD Blue Pearl Veterinary Specialists San Antonio, TX 1. Staphylococcus bacteria a. Gram positive b. Opportunistic pathogens
Discussion Points. Decisions in Selecting Antibiotics
 Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
QUICK REFERENCE. Pseudomonas aeruginosa. (Pseudomonas sp. Xantomonas maltophilia, Acinetobacter sp. & Flavomonas sp.)
") Pseudomonas aeruginosa (Pseudomonas sp. Xantomonas maltophilia, Acinetobacter sp. & Flavomonas sp.) Description: Greenish gray colonies with some beta-hemolysis around each colony on blood agar (BAP),
Pseudomonas aeruginosa (Pseudomonas sp. Xantomonas maltophilia, Acinetobacter sp. & Flavomonas sp.) Description: Greenish gray colonies with some beta-hemolysis around each colony on blood agar (BAP),
Pinni Meedha Mojutho Ammanu Dengina Koduku Part 1 Kama Kathalu
 Search for: Search Search Does levaquin cover anaerobes Pinni Meedha Mojutho Ammanu Dengina Koduku Part 1 Kama Kathalu Levofloxacin, sold under the trade names Levaquin among others, is an antibiotic.
Search for: Search Search Does levaquin cover anaerobes Pinni Meedha Mojutho Ammanu Dengina Koduku Part 1 Kama Kathalu Levofloxacin, sold under the trade names Levaquin among others, is an antibiotic.
Antibiotic Use in the Emergency Department
 Antibiotic Use in the Emergency Department Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
Antibiotic Use in the Emergency Department Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Mrsa abscess and cellulitis
 Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
Search Mrsa abscess and cellulitis An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The. Staph
2012 ANTIBIOGRAM. Central Zone Former DTHR Sites. Department of Pathology and Laboratory Medicine
 2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
2016 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Methicillin Resistant Staphylococcus aureus:
 Methicillin Resistant Staphylococcus aureus: Action-Oriented Guidance for Community-Based Prevention Jackie Dawson, PhD Public Health Epidemiologist Chelan, Douglas, Grant, Kittitas, & Okanogan Counties
Methicillin Resistant Staphylococcus aureus: Action-Oriented Guidance for Community-Based Prevention Jackie Dawson, PhD Public Health Epidemiologist Chelan, Douglas, Grant, Kittitas, & Okanogan Counties
CELLULITIS / SKIN INFECTIONS
 Skin Infections Assessment Investigations Cellulitis Management Abscess Management Infection Control Antibiotic Choice Education Recurrent Infections Referral to Community Nursing References Skin Infections
Skin Infections Assessment Investigations Cellulitis Management Abscess Management Infection Control Antibiotic Choice Education Recurrent Infections Referral to Community Nursing References Skin Infections
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Principles of Antibiotics Use & Spectrum of Some
 Principles of Antibiotics Use & Spectrum of Some Rabee Adwan. MD Infectious Diseases Consultant (Pediatric and Adult) Head Of ID Unit and IPAC Committee- AL-Makassed Hospital-AlQuds Head of IPAC Committee
Principles of Antibiotics Use & Spectrum of Some Rabee Adwan. MD Infectious Diseases Consultant (Pediatric and Adult) Head Of ID Unit and IPAC Committee- AL-Makassed Hospital-AlQuds Head of IPAC Committee
2017 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Protein Synthesis Inhibitors
 Protein Synthesis Inhibitors Assistant Professor Dr. Naza M. Ali 11 Nov 2018 Lec 7 Aminoglycosides Are structurally related two amino sugars attached by glycosidic linkages. They are bactericidal Inhibitors
Protein Synthesis Inhibitors Assistant Professor Dr. Naza M. Ali 11 Nov 2018 Lec 7 Aminoglycosides Are structurally related two amino sugars attached by glycosidic linkages. They are bactericidal Inhibitors
Pharmacology Week 6 ANTIMICROBIAL AGENTS
 Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections. Skin & Soft Tissue Infections (SSTI)
 Skin & Soft Tissue Infections. Skin & Soft Tissue Infections (SSTI)") Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections 2007 Abscess Cellulitis Bradley W Frazee, MD, FACEP Dept of Emergency Medicine Alameda County Medical Center - Highland Hospital Associate
Skin & Soft Tissue Infections (SSTI) Skin & Soft Tissue Infections 2007 Abscess Cellulitis Bradley W Frazee, MD, FACEP Dept of Emergency Medicine Alameda County Medical Center - Highland Hospital Associate
Epidemiology and Microbiology of Surgical Wound Infections
 JOURNAL OF CLINICAL MICROBIOLOGY, Feb. 2000, p. 918 922 Vol. 38, No. 2 0095-1137/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Epidemiology and Microbiology of Surgical
JOURNAL OF CLINICAL MICROBIOLOGY, Feb. 2000, p. 918 922 Vol. 38, No. 2 0095-1137/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Epidemiology and Microbiology of Surgical
Update on Fluoroquinolones. Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO
 Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Bacterial skin infection
 D i v i s i o n o f P e d i a t r i c E m e r g e n c y M e d i c i n e P a g e 1 Bacterial skin infection Cellulitis w/o abscess Abscess Deep tissue involvement Multiple abscesses Perirectal Anterior
D i v i s i o n o f P e d i a t r i c E m e r g e n c y M e d i c i n e P a g e 1 Bacterial skin infection Cellulitis w/o abscess Abscess Deep tissue involvement Multiple abscesses Perirectal Anterior
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how?
 Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Medicinal Chemistry 561P. 2 st hour Examination. May 6, 2013 NAME: KEY. Good Luck!
 Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Secondary peritonitis
 Secondary peritonitis Caused by spillage of gastrointestinal microorganisms into the peritoneal cavity secondary to loss of the integrity of the mucosal barriers Etiology: perforation of peptic ulcer traumatic
Secondary peritonitis Caused by spillage of gastrointestinal microorganisms into the peritoneal cavity secondary to loss of the integrity of the mucosal barriers Etiology: perforation of peptic ulcer traumatic
Skin and Soft Tissue Infections
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 28: Skin and Soft Tissue Infections Author Antoni Trilla, MD, PhD, MSc Chapter Editor Ziad A. Memish, MD, FRCPC, FACP Topic Outline Staphylococcal Skin
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 28: Skin and Soft Tissue Infections Author Antoni Trilla, MD, PhD, MSc Chapter Editor Ziad A. Memish, MD, FRCPC, FACP Topic Outline Staphylococcal Skin
Let me clear my throat: empiric antibiotics in
 Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance
 Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
Beta-lactams 1 รศ. พญ. มาล ยา มโนรถ ภาคว ชาเภส ชว ทยา. Beta-Lactam Antibiotics. 1. Penicillins 2. Cephalosporins 3. Monobactams 4.
 Beta-lactams 1 รศ. พญ. มาล ยา มโนรถ ภาคว ชาเภส ชว ทยา จ ดประสงค การศ กษา เม อส นส ดการเร ยนการสอน และการศ กษาด วยตนเองเพ มเต ม น กศ กษาสามารถ 1. อธ บายกลไกการออกฤทธ และกลไกการด อยาของยากล ม penicillins
Beta-lactams 1 รศ. พญ. มาล ยา มโนรถ ภาคว ชาเภส ชว ทยา จ ดประสงค การศ กษา เม อส นส ดการเร ยนการสอน และการศ กษาด วยตนเองเพ มเต ม น กศ กษาสามารถ 1. อธ บายกลไกการออกฤทธ และกลไกการด อยาของยากล ม penicillins
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
ß-lactams. Sub-families. Penicillins. Cephalosporins. Monobactams. Carbapenems
 β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
Source: Portland State University Population Research Center (
 Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Antimicrobial Resistance Trends in the Province of British Columbia
 655 West 12th Avenue Vancouver, BC V5Z 4R4 Tel 604.707.2443 Fax 604.707.2441 www.bccdc.ca Antimicrobial Resistance Trends in the Province of British Columbia 2013 Prepared by the Do Bugs Need Drugs? Program
655 West 12th Avenue Vancouver, BC V5Z 4R4 Tel 604.707.2443 Fax 604.707.2441 www.bccdc.ca Antimicrobial Resistance Trends in the Province of British Columbia 2013 Prepared by the Do Bugs Need Drugs? Program
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children
 Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Burn Infection & Laboratory Diagnosis
 Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
BactiReg3 Event Notes Module Page(s) 4-9 (TUL) Page 1 of 21
 4-9 (TUL) Page 1 of 21") www.wslhpt.org 2601 Agriculture Drive Madison, WI 53718 (800) 462-5261 (608) 265-1111 2015-BactiR Reg3 Shipment Date: September 14, 2015 Questions or comments should be directed to Amanda Weiss at 800-462-5261
www.wslhpt.org 2601 Agriculture Drive Madison, WI 53718 (800) 462-5261 (608) 265-1111 2015-BactiR Reg3 Shipment Date: September 14, 2015 Questions or comments should be directed to Amanda Weiss at 800-462-5261
Subacute Adenitis. Ann M. Loeffler, MD
 Subacute Adenitis Ann M. Loeffler, MD Lymphadenitis Swelling and hyperplasia of sinusoidal lining cells Infiltration of leukocytes +/- abscess formation Granulomatous or non-granulomatous Pyogenic adenitis
Subacute Adenitis Ann M. Loeffler, MD Lymphadenitis Swelling and hyperplasia of sinusoidal lining cells Infiltration of leukocytes +/- abscess formation Granulomatous or non-granulomatous Pyogenic adenitis