Head to Toe: Common infections in Hospital settings. Katya Calvo MD Medical Director of Antimicrobial Stewardship Division of Infectious Diseases
|
|
|
- Jonas O’Connor’
- 5 years ago
- Views:
Transcription
1 Head to Toe: Common infections in Hospital settings Katya Calvo MD Medical Director of Antimicrobial Stewardship Division of Infectious Diseases
2 Objectives To identify at least one common infection in each organ system To identify likely pathogen related to infection To be able to chose antibiotic regimen based on suspected site of infection
3 "The man who asks a question is a fool for a minute, the man who does not ask is a fool for life." - Confucius
4 Important Points No consensus on definition of fever Sometimes defined as > 38.0 ⁰C (100.4 ⁰F) Arbo. Am J Med 1993; 95: Bone. Chest 1992; 101: Single elevation of > 38.3 ⁰C (101.0 ⁰F) Hughes. Clin Infect Dis 2002; 34: Neutropenic pts: >38.0 ⁰C for more than an hour Hughes. Clin Infect Dis 2002; 34: A substantial proportion of infected patients are not febrile Up to 50% of patients with fever do not have an infection (in hospitalized patients) Arbo. Am J Med 1993; 95:

5 Head-to-Toe Meningitis Sinusitis Endocarditis Pneumonia Diarrhea Lines Urinary Cellulitis
6 Case 1 24 year old female college students wakes up not feeling well, tells her roomate she will skip classes that morning. Roomate does not see her at lunch and when returns to her room at 3 pm, she is not arousable. In the ED she is noted to have a fever of ⁰F, stiff neck and petechial lesions on her lower extremities.
7 What are common pathogens in Acute Meningitis? Streptococcus pneumoniae Neisseria meningiditis Haemophilus influenzae

8 Mandell: Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 7th ed.
9 Questions for you What antibiotics will you start empirically? Would initial antibiotics change if patient were a 65 year old alcoholic? When do we worry about chronic meningitis? Should you add Acyclovir?
10 Antibiotic Summary Empiric regimen Ceftriaxone 2 gm IV q 12 + Vancomycin (loading dose) For possible PCN resistant Streptococcus For immunocompromized Add Ampicillin 2gm IV q 4 hours If encephalitis is in your differential Acyclovir 10 mg/kg IV q 8
11 Case 2 65 year old male with HTN and DM II, presents to your clinic with 5 weeks of weight loss, night sweats, low grade fevers and on exam you note a new murmur, and note conjunctival hemorrhages and splinter hemorrhages of the toes (because you actually took his socks off!) A thorough history reveals a dental extraction 6 weeks prior
12 Common pathogen in community acquired endocarditis (native valve) Staphylococcus aureus Streptococcus Strep. viridans Strep. bovis Enterococcus HAECK Gram negative organisms De sa DD. Mayo Clin Proc. 2010;85:422-6 McDonald. Infec Dis Clin North Am. 2009;23: Murdoch. Arch Intern Med. 2009;169: Baddour. Circulation. 2005;111:e394-e434
13 Common pathogen in community acquired endocarditis (prosthetic valve) Early (< 2mo) Coag negative Staph Staph aureus Gram negative bacilli Intermediate (> 2 mo, < 1 yr) Coag neg Staph Staph Aureus Fungi Enterococcus Late (>12 mo) Streptococcus Staph aureus
14 Common pathogen in IVDA Staphylococcus aureus Streptococcus Enterococcus Gram negative bacilli Fungi Candida
15 Questions for you What antibiotic would you start empirically What must you do prior to starting antibiotics TTE or TEE?
16 Antibiotic Summary Empiric regimen Ampicillin --- Unasyn 3 gm IV q 6 + Nafcillin --- Vancomycin + Gentamicin 1 gm/kg q 8 (synergy dose)
17 Case 3 53 year old female with Hypothyroidism presents with 1 week of cough, yellow sputum production and a 2 day history of right flank pain. She has felt increasingly SOB. In the office, you check an SpO2 and it is 87% on RA
18 Terminology Community Acquired Pneumonia (CAP) Health-care Associated Pneumonia (HCAP) Any patient who was hospitalized in an acute-care hospital for 2 or more days within 90 days of presentation Residents of nursing homes, long-term care facility Received home infusion therapy (30 d) Chronic dialysis (30 d) Home wound care (30 d) Family member with multidrug-resistant pathogen Hospital Acquired Pneumonia (HAP) Ventilator Associated Pneumoina (VAP)

19 Pathogens in CAP File. Lancet 2003;362;
20 Questions for you What empiric antibiotics would you start? What tests to order for diagnosis? When do you add anaerobic coverage? When would you cover for Pseudomonas?
21 Risk factors for Pseudomonas Structural lung disease + steroid use, prior antibiotic therapy. Mandell. CID 2007;44:s27-72
22 Antibiotic Summary Empiric regimen Ceftriaxone 1-2 gm IV q day + Azithromycin 500 mg po q day OR Doxycycline 100 mg po BID If Aspiration is a concern Add Clindamycin 600 mg IV q 8 Use Unasyn 3 gm IV q 6 instead of Ceftriaxone If Pseudomonas is a concern No need to double cover Zosyn q IV 8 (extended infusion) DO NOT USE CIPROFLOXACIN
23
24 HCAP/HAP/VAP HCAP Cover Pseudomonas and MRSA No need to double cover Pseudomonas HAP/VAP Cover Pseudomonas and MRSA NEED to double cover at least for 1 st dose after diagnosis CMS rules
25 Case 4 23 year old female G1P1 with a 2 month old comes to your office with diarrhea. She states that she is having 5-10 watery BM, and sometimes she does not get to the bathroom in time. No fever, no abdominal pain, just cramping.
26 Clostridium difficile infection New testing at UNM 2 step process Loose stool tested for GDH antigen and Toxin by EIA If indicated, PCR test done
27 Antibiotic Summary Initial therapy Mild/Moderate Metronidazole 500 mg po TID x days Severe (WBC 15 or SCr 1.5 x baseline) Vancomycin 125 mg po QID x days Severe, complicated (hypotension, shock, ileus, megacolon) Vancomycin 500 mg po QID + Metronidazole 500 mg IV q 8 1 st recurrence Same as initial 2 nd recurrence Vancomycin in tapered and/or pulse regimen Do not use Metronidazole Cohen. Infect Control Hosp Epidemiol 2010;31:431-55
28 Case 5 A 45 year old female comes to your office with 3 days of frequency, urgency and dysuria. On exam she is afebrile with no CVA tenderness
29 Terminology Asymptomatic Bacteriuria Acute Uncomplicated Cystitis/Pyelonephritis No pregnancy, DM, Functional or anatomical abnormalities, immunosuppression Pyelonephritis requiring hospitalization Complicated UTI Males Catheter-Associated UTI (CA-UTI)
30 SHOULD BE SCREENED Pregnant women at least once early in pregnancy Men before a transurethral resection of the prostate Other urologic procedures for which mucosal bleeding is anticipated NO SCREENING Premenopausal, nonpregnant women Diabetic women Older persons living in the community Elderly, institutionalized patients Persons with spinal cord injury Catheterized patients while the catheter remains in situ Nicole et al. CID 2005;40:
31 Pathogens in Acute Uncomplicated UTI or Pyelonephritis Uropathogens E. coli Proteus Klebsiella Enterobacter Pseudomonas Staphylococcus aureus is not normal!
32 Treatment Acute Uncomplicated Cystitis Nitrofurantoin monohydrate/macrocrystals 100 mg po BID for 5 days TMP-SMX 1 DS tablet BID for 3 days Fosfomycin trometamol 3gm in a single dose Gupta.CID 2011;52:e

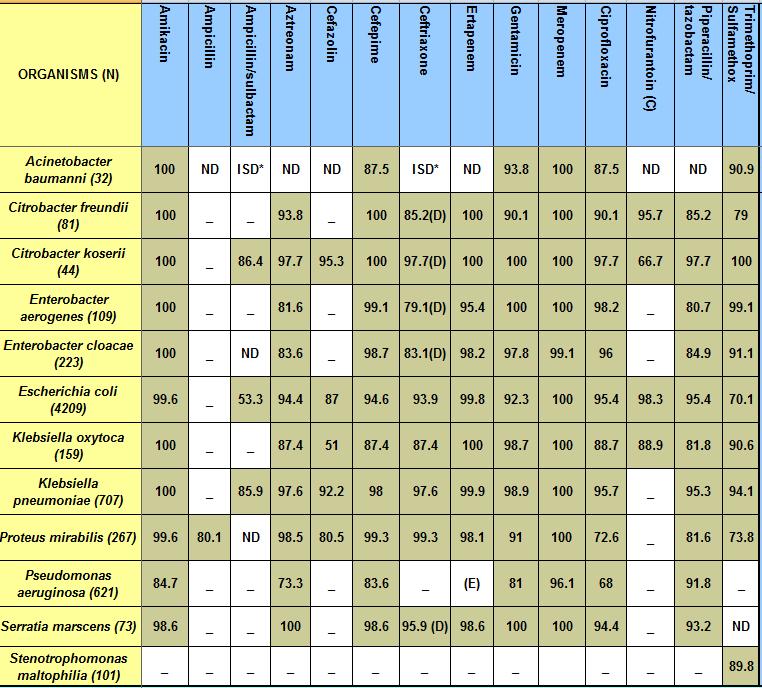
33 TRICORE NON-HOSPITAL UTI ANTIBIOGRAM
34 Bactrim not to be used as first line when prevalence of resistance is more than 20% Ciprofloxacin not to be used as first line when prevalence of resistance more than 10%
35 Acute Uncomplicated Pyelonephritis 1 st Line: 7 days of therapy Ciprofloxacin 500 mg 1 PO BID Cipro ER 1000 mg 1 PO daily Alternative: 14 days of therapy Amoxicillin/clavulanate (Augmentin) 875/125 mg PO BID Cephalexin 500 mg PO QID TMP/SMX DS 1 PO BID Talan DA, et al. JAMA. 2000;283(12): Gupta, CID 2011;52:e
36 Pyelonephritis requiring Hospitalization 14 days Start with IV and then change to PO after pt is afebrile for hrs 1st line: Ceftriaxone 1 g IV q24h Ciprofloxacin 400 mg IV q12h Ampicillin 2 g IV q6h + gentamicin 3 mg/kg IV q24h Talan DA, et al. JAMA. 2000;283(12): Gupta, CID 2011;52:e
37 CAUTI -Treatment Duration 7 days for patients who have prompt resolution of symptoms 5 day therapy with Levofloxacin may be considered in patients with CA-UTI who are not severly ill Peterson et al. Urology 2008;71: day therapy may be considered in women < 65yrs, without upper tract symptoms whose catheter has been removed Harding et al. Ann Intern Med 1991;114: days for patient with delayed response Hooton et al. CID 2010;50:
38 Case 6 A 47 year old male, no PMH, is seen in your office due to a left lower extremity abscess (1x1 cm) self draining with surrounding erythema, approximately a 4 cm circumference. The area is tender and warm. Patient is afebrile, looks stable. He denies any trauma to area and there have been no animal contact.
39 Pathogens in Skin and Soft Tissue infections Erysipelas: fiery red, tender, painful plaque with well-demarcated edges. Commonly caused by streptococcal species, usually S. pyogenes Cellulitis associated with furuncles, carbuncles, or abscesses is usually caused by S. aureus Cellulitis that is diffuse or unassociated with a defined portal is most commonly caused by streptococcal species.
40 Questions for you What can you do in the office that may help management? What antibiotic are you going to prescribe? What is considered a treatment failure? Do we always worry about MRSA?
41 Antibiotic Summary Erysipelas Dicloxacillin 250 mg po QID Amoxicillin 500 mg mg po TID Cellulitis with Abscess Doxycycline 100 mg IV/PO BID SMX/TMP 2 DS tabs PO BID-TID Vancomycin (inpatient) Cellulitis without Abscess Cephalexin 500 mg PO QID Cefazolin 1 g IV q8h (inpatient) Nafcillin 12 g IV CI (inpatient) Stevens. CID 2005;41:
42 Questions for me?
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles
 Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient
 1 Chapter 79, Self-Assessment Questions 1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient with normal renal function is: A. Trimethoprim-sulfamethoxazole B. Cefuroxime
1 Chapter 79, Self-Assessment Questions 1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient with normal renal function is: A. Trimethoprim-sulfamethoxazole B. Cefuroxime
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
Antibiotic Duration for Common Infections
 Antibiotic Duration for Common Infections Emily Spivak, MD, MHS Division of Infectious Diseases Medical Director, Antimicrobial Stewardship Program University of Utah Hospitals and Clinics Learning Objectives
Antibiotic Duration for Common Infections Emily Spivak, MD, MHS Division of Infectious Diseases Medical Director, Antimicrobial Stewardship Program University of Utah Hospitals and Clinics Learning Objectives
Disclosures. Nothing Medically I own FiPhysician LLC, a financial planning and investment company (FiPhysician.com)
") "How to work around (with) administration to build an Antimicrobial Stewardship Program AND how to get dumb (oops reluctant) doctors to do the right thing" David Graham, MD Disclosures Nothing Medically
"How to work around (with) administration to build an Antimicrobial Stewardship Program AND how to get dumb (oops reluctant) doctors to do the right thing" David Graham, MD Disclosures Nothing Medically
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Stewardship in the Long Term Care Setting. Lisa Venditti, R.Ph., FASCP, Founder and CEO Long Term Solutions Inc LTSRX.
 Antibiotic Stewardship in the Long Term Care Setting Lisa Venditti, R.Ph., FASCP, Founder and CEO Long Term Solutions Inc. 845.208.3328 LTSRX.com 1 Resistant Bacteria Crisis The Centers for Medicare &
Antibiotic Stewardship in the Long Term Care Setting Lisa Venditti, R.Ph., FASCP, Founder and CEO Long Term Solutions Inc. 845.208.3328 LTSRX.com 1 Resistant Bacteria Crisis The Centers for Medicare &
Guidelines for Treatment of Urinary Tract Infections
 Guidelines for Treatment of Urinary Tract Infections Overview This document details the Michigan Hospital Medicine Safety (HMS) Consortium preferred antibiotic choices for treatment of uncomplicated and
Guidelines for Treatment of Urinary Tract Infections Overview This document details the Michigan Hospital Medicine Safety (HMS) Consortium preferred antibiotic choices for treatment of uncomplicated and
Provincial Drugs & Therapeutics Committee Memorandum Version 2
 Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults
 Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Discussion Points. Decisions in Selecting Antibiotics
 Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Update on Fluoroquinolones. Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO
 Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Antimicrobial Stewardship in the ER. Dr. Michael Armitage Maritime Trauma and EM Conference April 5, 2014
 Antimicrobial Stewardship in the ER Dr. Michael Armitage Maritime Trauma and EM Conference April 5, 2014 Declaration of Conflict of Interest I DO NOT have an affiliation(financial or otherwise) with a
Antimicrobial Stewardship in the ER Dr. Michael Armitage Maritime Trauma and EM Conference April 5, 2014 Declaration of Conflict of Interest I DO NOT have an affiliation(financial or otherwise) with a
Clinical Practice Standard
 Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
21 st Expert Committee on Selection and Use of Essential Medicines Peer Review Report Antibiotics Review
 (1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
(1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS
 VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
Antibiotic Stewardship
 Antibiotic Stewardship Nick Zaksek Pharm D., BCPS AQ-ID Infectious Disease POMA 2019 1 Disclosures None 2 Objectives Practice good Antibiotic stewardship and foster the notion of antibiotic stewardship
Antibiotic Stewardship Nick Zaksek Pharm D., BCPS AQ-ID Infectious Disease POMA 2019 1 Disclosures None 2 Objectives Practice good Antibiotic stewardship and foster the notion of antibiotic stewardship
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance
 Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
Antimicrobial Stewardship in Ambulatory Care
 Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings?
 An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
Antibiotics in the trenches: An ER Doc s Perspective
 Antibiotics in the trenches: An ER Doc s Perspective Peter Currie, MD Medical Director for Quality Emergency Physicians Professional Association (EPPA) Agenda Emergency Medicine Specific Disease Processes
Antibiotics in the trenches: An ER Doc s Perspective Peter Currie, MD Medical Director for Quality Emergency Physicians Professional Association (EPPA) Agenda Emergency Medicine Specific Disease Processes
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Antimicrobial Stewardship
 Antimicrobial Stewardship Antimicrobial Stewardship Studies have estimated that 30 50% of antibiotics prescribed in acutecare hospitals are unnecessary or inappropriate 1 Antimicrobial stewardship definition:
Antimicrobial Stewardship Antimicrobial Stewardship Studies have estimated that 30 50% of antibiotics prescribed in acutecare hospitals are unnecessary or inappropriate 1 Antimicrobial stewardship definition:
Copyright 2012 Diabetes In Control, Inc. For permission to reprint, please contact Heather Moran, Production Editor, at
 Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center
 Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center Case 1 60 yo healthy female admitted for fevers and dysuria.
Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center Case 1 60 yo healthy female admitted for fevers and dysuria.
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Drug Class Prior Authorization Criteria Intravenous Antibiotics
 Drug Class Prior Authorization Criteria Intravenous Antibiotics Line of Business: Medicaid P&T Approval Date: August 15, 2018 Effective Date: October 1, 2018 This drug class prior authorization criteria
Drug Class Prior Authorization Criteria Intravenous Antibiotics Line of Business: Medicaid P&T Approval Date: August 15, 2018 Effective Date: October 1, 2018 This drug class prior authorization criteria
2017 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Suggested treatment. Inj Crystalline Penicillin 50,000U/Kg i.v. 4-6hrly (if child cannot swallow) 40mg/Kg/dose BID x 10days
 40mg/Kg/dose BID x 10days") GUIDELINES FOR TREATMENT OF INFECTIONS IN CHILDREN A. RESPIRATORY TRACT INFECTIONS UPPER RESPIRATORY TRACT INFECTIONS Infection/Condition/likely organism Suggested treatment Preferred Alternative Acute
GUIDELINES FOR TREATMENT OF INFECTIONS IN CHILDREN A. RESPIRATORY TRACT INFECTIONS UPPER RESPIRATORY TRACT INFECTIONS Infection/Condition/likely organism Suggested treatment Preferred Alternative Acute
your hospitals, your health, our priority PARC (Policy Approval and Ratification Committee) STANDARD OPERATING PROCEDURE:
 STANDARD OPERATING PROCEDURE:") STANDARD OPERATING PROCEDURE: TRUST ANTIBIOTIC TREATMENT SOP SOP NO: TW10/136 SOP 1 VERSION NO: VERSION 6.1 (JANUARY 2013) APPROVING COMMITTEE: INFECTION PREVENTION AND CONTROL COMMITTEE DATE THIS VERSION
STANDARD OPERATING PROCEDURE: TRUST ANTIBIOTIC TREATMENT SOP SOP NO: TW10/136 SOP 1 VERSION NO: VERSION 6.1 (JANUARY 2013) APPROVING COMMITTEE: INFECTION PREVENTION AND CONTROL COMMITTEE DATE THIS VERSION
Examples of Antimicrobial Stewardship Interventions: a couple of starter projects
 Examples of Antimicrobial Stewardship Interventions: a couple of starter projects Jennifer Ott, PharmD, BCPS Clinical Pharmacist Specialist Infectious Diseases Billings Clinic jott4@billingsclinic.org
Examples of Antimicrobial Stewardship Interventions: a couple of starter projects Jennifer Ott, PharmD, BCPS Clinical Pharmacist Specialist Infectious Diseases Billings Clinic jott4@billingsclinic.org
Infectious Disease Update 2017
 Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections
 Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
MANAGING COMMON INFECTIONS IN OLDER ADULTS
 MANAGING COMMON INFECTIONS IN OLDER ADULTS Ghinwa Dumyati, MD Professor of Medicine Infectious Diseases Division and Center for Community Health University of Rochester Medical Center Objectives 1. Review
MANAGING COMMON INFECTIONS IN OLDER ADULTS Ghinwa Dumyati, MD Professor of Medicine Infectious Diseases Division and Center for Community Health University of Rochester Medical Center Objectives 1. Review
TOH GUIDELINES FOR EMPIRIC ANTIBIOTIC THERAPY
 TOH GUIDELINES FOR EMPIRIC ANTIBIOTIC THERAPY Developed by the Antimicrobial Subcommittee of the Pharmacy & Therapeutics Committee CONTENTS BONE AND JOINT INFECTIONS 2 CENTRAL NERVOUS SYSTEM INFECTIONS
TOH GUIDELINES FOR EMPIRIC ANTIBIOTIC THERAPY Developed by the Antimicrobial Subcommittee of the Pharmacy & Therapeutics Committee CONTENTS BONE AND JOINT INFECTIONS 2 CENTRAL NERVOUS SYSTEM INFECTIONS
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Septicaemia Definitions 1
 Septicaemia Definitions 1 Term Definition Bacteraemia Systemic Inflammatory response (SIRS) Sepsis Bacteria that can be cultured from the blood stream The systemic response to a wide range of stresses.
Septicaemia Definitions 1 Term Definition Bacteraemia Systemic Inflammatory response (SIRS) Sepsis Bacteria that can be cultured from the blood stream The systemic response to a wide range of stresses.
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
$100 $200 $300 $400 $500
 Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
** the doctor start the lecture with revising some information from the last one:
 Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
High Risk Emergency Medicine. Antibiotic Pitfalls
 High Risk Emergency Medicine Antibiotic Pitfalls David, MD MS Assistant Professor Department of Emergency Medicine University of California, San Francisco I. Antibiotic Resistance Development of resistance
High Risk Emergency Medicine Antibiotic Pitfalls David, MD MS Assistant Professor Department of Emergency Medicine University of California, San Francisco I. Antibiotic Resistance Development of resistance
2015 Updates in Therapeutics: The Pharmacotherapy Preparatory Review & Recertification Course Infectious Diseases Curtis L. Smith, Pharm.D.
 2015 Updates in Therapeutics: The Pharmacotherapy Preparatory Review & Recertification Course Infectious Diseases Curtis L. Smith, Pharm.D., BCPS Ferris State University Conflict of Interest Disclosures
2015 Updates in Therapeutics: The Pharmacotherapy Preparatory Review & Recertification Course Infectious Diseases Curtis L. Smith, Pharm.D., BCPS Ferris State University Conflict of Interest Disclosures
Antibiotic Stewardship NOW!
 Antibiotic Stewardship NOW! The More We Use Antibiotics, the More We Lose Antibiotics Nick Zaksek Pharm D. BCPS AQ ID PADONA 2019 Antimicrobial Stewardship Coordinated interventions designed to improve
Antibiotic Stewardship NOW! The More We Use Antibiotics, the More We Lose Antibiotics Nick Zaksek Pharm D. BCPS AQ ID PADONA 2019 Antimicrobial Stewardship Coordinated interventions designed to improve
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
HOW TO INTERPRET CULTURE RESULTS. Karen Brust, MD November 29, 2012
 HOW TO INTERPRET CULTURE RESULTS Karen Brust, MD November 29, 2012 DISCLOSURES NONE CULTURE RESULTS Based on susceptibility patterns CLSI: international, interdisciplinary, Nonprofit,
HOW TO INTERPRET CULTURE RESULTS Karen Brust, MD November 29, 2012 DISCLOSURES NONE CULTURE RESULTS Based on susceptibility patterns CLSI: international, interdisciplinary, Nonprofit,
PRMCE ANTI-INFECTIVES SELECTION GUIDELINE FOR ADULTS (Revision October 22, 2015)
") PRMCE ANTI-INFECTIVES SELECTION GUIDELINE FOR ADULTS (Revision October 22, 2015) SKIN AND SOFT TISSUE INFECTIONS: Mild A. Cellulitis: MRSA uncommonly causes cellulitis in the absence of a wound or abscess.
PRMCE ANTI-INFECTIVES SELECTION GUIDELINE FOR ADULTS (Revision October 22, 2015) SKIN AND SOFT TISSUE INFECTIONS: Mild A. Cellulitis: MRSA uncommonly causes cellulitis in the absence of a wound or abscess.
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
* gender factor (male=1, female=0.85)
") Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
% Susceptible Atlanta VAMC January - December 2018
 # tested Penicillin (non-meningeal) Penicillin (meningeal) Erythromycin Clindamycin Rifampin Vancomycin Trimeth-Sulfa # tested Amp / Sulbactam Piperacillin/Tazo Cefazolin (Urine ONLY) 4 Ceftriaxone Ceftazidime
# tested Penicillin (non-meningeal) Penicillin (meningeal) Erythromycin Clindamycin Rifampin Vancomycin Trimeth-Sulfa # tested Amp / Sulbactam Piperacillin/Tazo Cefazolin (Urine ONLY) 4 Ceftriaxone Ceftazidime
3/23/2017. Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc. Kathryn G. Smith: Nothing to disclose
 Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
Best Practices: Goals of Antimicrobial Stewardship
 Best Practices: Goals of Antimicrobial Stewardship Gail Scully, M.D, M.P.H. and Elizabeth Radigan, PharmD, BCPS UMass Memorial Medical Center Division of Infectious Disease Department of Medicine September
Best Practices: Goals of Antimicrobial Stewardship Gail Scully, M.D, M.P.H. and Elizabeth Radigan, PharmD, BCPS UMass Memorial Medical Center Division of Infectious Disease Department of Medicine September
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT
 INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS
 Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Cipro for gram positive cocci in urine
 Buscar... Cipro for gram positive cocci in urine 20-6-2017 Pneumonia can be generally defined as an infection of the lung parenchyma, in which consolidation of the affected part and a filling of the alveolar
Buscar... Cipro for gram positive cocci in urine 20-6-2017 Pneumonia can be generally defined as an infection of the lung parenchyma, in which consolidation of the affected part and a filling of the alveolar
Cork and Kerry SARI Newsletter; Vol. 2 (2), December 2006
, December 2006") Cork and SARI Newsletter; Vol. 2 (2), December 6 Item Type Newsletter Authors Murray, Deirdre;O'Connor, Nuala;Condon, Rosalind Download date 31/1/18 15:27:31 Link to Item http://hdl.handle.net/1147/67296
Cork and SARI Newsletter; Vol. 2 (2), December 6 Item Type Newsletter Authors Murray, Deirdre;O'Connor, Nuala;Condon, Rosalind Download date 31/1/18 15:27:31 Link to Item http://hdl.handle.net/1147/67296
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
PAGE 1 of 3 PURPOSE To assure that DOP inmates with Soft Tissue Infections are receiving high quality Primary Care for their infections and that the risk of infecting other inmates or staff is minimized.
Preserve the Power of Antibiotics
 PROVIDERInsight News for providers in Northeast Nebraska April 2016 Preserve the Power of Antibiotics Antimicrobial stewardship interventions have been proven to improve individual patient outcomes, reduce
PROVIDERInsight News for providers in Northeast Nebraska April 2016 Preserve the Power of Antibiotics Antimicrobial stewardship interventions have been proven to improve individual patient outcomes, reduce
UTI Dr S Mathijs Department of Pharmacology
 UTI Dr S Mathijs Department of Pharmacology Introduction Responsible for > 7 million consultations annually 15% of all antibiotic prescriptions 40% of all hospital acquired infections Significant burden
UTI Dr S Mathijs Department of Pharmacology Introduction Responsible for > 7 million consultations annually 15% of all antibiotic prescriptions 40% of all hospital acquired infections Significant burden
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Antibiotic Stewardship - Fine Tuning Your Program for Purposeful Change
 Antibiotic Stewardship - Fine Tuning Your Program for Purposeful Change Kaylee Adams PharmD, BCGP Medication Managers, LLC Stacey Rexrode PharmD, BCGP Jude Rx, LLC Disclosure We have no relevant financial
Antibiotic Stewardship - Fine Tuning Your Program for Purposeful Change Kaylee Adams PharmD, BCGP Medication Managers, LLC Stacey Rexrode PharmD, BCGP Jude Rx, LLC Disclosure We have no relevant financial
Objectives. Antibiotic Prophylaxis in Urologic Procedures: A Review of the CUA Guidelines & Local Epidemiology of Drug Resistance
 Antibiotic Prophylaxis in Urologic Procedures: A Review of the CUA Guidelines & Local Epidemiology of Drug Resistance David Hogarth UBC Urology PGY-1 May 24, 2017 Objectives 1. To review the current CUA
Antibiotic Prophylaxis in Urologic Procedures: A Review of the CUA Guidelines & Local Epidemiology of Drug Resistance David Hogarth UBC Urology PGY-1 May 24, 2017 Objectives 1. To review the current CUA
Medicinal Chemistry 561P. 2 st hour Examination. May 6, 2013 NAME: KEY. Good Luck!
 Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
9/9/2015. Disclosure / Contact. Pneumonia Stats. Exploring the Clinical and Regulatory Impact of Pneumonia in Long Term Care
 Exploring the Clinical and Regulatory Impact of Pneumonia in Long Term Care Rob Shulman R.Ph. CGP FASCP Director of Consulting Services Remedi SeniorCare William M. Vaughan,RN, BSN Vice President, Education
Exploring the Clinical and Regulatory Impact of Pneumonia in Long Term Care Rob Shulman R.Ph. CGP FASCP Director of Consulting Services Remedi SeniorCare William M. Vaughan,RN, BSN Vice President, Education
DRAFT DRAFT. Paediatric Antibiotic Prescribing Guideline. May
 Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Community Acquired Pneumonia: An Update on Guidelines
 Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Antibiotic stewardship in long term care
 Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Management of Native Valve
 Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings. Carlos Reyes Sacin, MD, AAHIVS
 Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
The Rise of Antibiotic Resistance: Is It Too Late?
 The Rise of Antibiotic Resistance: Is It Too Late? Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine None DISCLOSURES THE PROBLEM Antibiotic resistance is one of the
The Rise of Antibiotic Resistance: Is It Too Late? Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine None DISCLOSURES THE PROBLEM Antibiotic resistance is one of the
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Objectives. Review basic categories of intra-abdominal infection and their respective treatments. Community acquired intra-abdominal infection
 Objectives Review basic categories of intra-abdominal infection and their respective treatments Community acquired intra-abdominal infection Mild/Moderate Severe Acute biliary tract infections Nosocomial
Objectives Review basic categories of intra-abdominal infection and their respective treatments Community acquired intra-abdominal infection Mild/Moderate Severe Acute biliary tract infections Nosocomial
TITLE: NICU Late-Onset Sepsis Antibiotic Practice Guideline
 Site: Saint Joseph Hospital - NICU Original Effective Date: 6/1/2016 Next Review Date: 6/1/2019 TITLE: Practice Guideline Purpose: Timely and appropriate treatment of late-onset sepsis with antibiotic
Site: Saint Joseph Hospital - NICU Original Effective Date: 6/1/2016 Next Review Date: 6/1/2019 TITLE: Practice Guideline Purpose: Timely and appropriate treatment of late-onset sepsis with antibiotic
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Prudent Use of Antibiotics in Long Term Care Residents with Suspected UTI
 Prudent Use of Antibiotics in Long Term Care Residents with Suspected UTI Shira Doron, MD Assistant Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston,
Prudent Use of Antibiotics in Long Term Care Residents with Suspected UTI Shira Doron, MD Assistant Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston,
Improving Antimicrobial Therapy in Elders. Margo Schilling MD April 2, st Annual Family Physician Refresher Course
 Improving Antimicrobial Therapy in Elders Margo Schilling MD April 2, 2014 41 st Annual Family Physician Refresher Course Objectives Distinguish between symptomatic UTI and asymptomatic bacteriuria in
Improving Antimicrobial Therapy in Elders Margo Schilling MD April 2, 2014 41 st Annual Family Physician Refresher Course Objectives Distinguish between symptomatic UTI and asymptomatic bacteriuria in
Making every antibiotic count. Bacterial Meningitis. INDICATION FOR THERAPY USUAL CAUSATIVE ORGANISMS Age y EMPIRIC ANTIBIOTIC REGIMENS
 Bacterial Meningitis INDICATION FOR THERAPY USUAL CAUSATIVE ORGANISMS Age 18-50 y S. pneumoniae* N. meningitides* H. influenzae* EMPIRIC ANTIBIOTIC REGIMENS Ceftriaxone 2 g IV q12h Vancomycin 20mg/kg x
Bacterial Meningitis INDICATION FOR THERAPY USUAL CAUSATIVE ORGANISMS Age 18-50 y S. pneumoniae* N. meningitides* H. influenzae* EMPIRIC ANTIBIOTIC REGIMENS Ceftriaxone 2 g IV q12h Vancomycin 20mg/kg x
Antibiotic Stewardship In Post Acute and Long Term Care 2017
 Antibiotic Stewardship In Post Acute and Long Term Care 2017 Alex T. Makris, MD, CMD What is Antibiotic Stewardship Coordinated program that promotes the appropriate use of antimicrobials, improves patient
Antibiotic Stewardship In Post Acute and Long Term Care 2017 Alex T. Makris, MD, CMD What is Antibiotic Stewardship Coordinated program that promotes the appropriate use of antimicrobials, improves patient
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance