Treatment of PJI. Andrej Trampuz Charité University Medicine Berlin Germany
|
|
|
- Sherman Turner
- 5 years ago
- Views:
Transcription




1 Treatment of PJI Andrej Trampuz Charité University Medicine Berlin Germany

2 Implants improved life quality



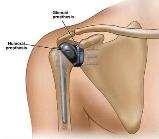
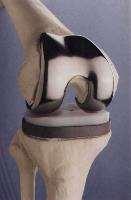


3
4 Treatment


5 Treatment concept To achieve high treatment success, a concerted surgical and antimicrobial concept is needed Cure rate >90%
6 Treatment algorithm Acute PJI Chronic PJI Long-term suppressive antibiotic therapy, permanent arthrodesis/girdlestone - Good bone/soft tissue? - Stable prosthesis? - No DTT (if known)? No Prosthesis exchange Eradication of infection not possible Yes - DTT (if known)? - Bad bone/soft tissue? - Fistula? - Multiple revisions? Yes No Débridement & retention, exchange of mobile parts One-stage exchange Two-stage exchange Three-stage exchange DTT = difficult-to-treat infections caused by pathogens resistant to biofilm-active antimicrobials - Rifampin-resistant staphylococci - Ciprofloxacin-resistant gram-negative bacteria - Fungi (Candida) - DTT-organism? - Bad bone/soft tissue? Short interval (2-3 weeks) No Unsatisfactory course? Yes Long interval (6-8 weeks)
7 Acute infection
 revision surgery if prolonged")
8 Prolonged discharge: early postoperative PJI? C-reactive protein (CRP) should decrease after surgery! Exclude other reasons of prolonged discharge (coagulopathy, hematoma, albumin deficiency) revision surgery if prolonged discharge (>7-10 days)

9 Acute pain & fever, 10 y after implantation
10 Bacterial count (log) The solution to pollution is dilution Systemic antibiotic Resistant strains No surgery Insufficient debridement, Sufficient debridement, change of mobile parts Time

11 Antibiotics without surgery Cure rate 8% Cure rate 9% Johnson et al. J Bone Joint Surg Br 1986; Bengtson et al. Acta Orhop Scand 1991
12 Always (!): Change of mobile parts Acute hip and knee infection Debridement & retention Intervention Not changing mobile parts Clinical success 4/52 (7%) Changing of mobile parts 50/55 (91%)
13 Zimmerli W et al. N Engl J Med 2004:351:

14 2004
15 Chronic infection

16 78-y-o female Primary hip prosthesis 4 months ago Since implantation pain, walking distance now 20 m CRP normal, no loosening on x-ray
17 Aspiration 4 months after implantation High leukocyte count in joint aspirate (59,000/µl)
18 Delayed (low-grade) infection Joint aspiration: Culture: Staphylococcus epidermidis Cell count: /µl leukocytes, 90% PMN CRP normal, no prosthesis loosening Prosthesis exchange: 1-stage exchange OR 2-stage exchange with short interval (2 weeks)
19 Treatment algorithm: chronic infection Chronic PJI Prosthesis exchange - DTT (if known)? - Bad bone/soft tissue? - Fistula? - Multiple revisions? Yes No One-stage exchange Two-stage exchange Three-stage exchange DTT = difficult-to-treat infections caused by pathogens resistant to biofilm-active antimicrobials - Rifampin-resistant staphylococci - Ciprofloxacin-resistant gram-negative bacteria - Fungi (Candida) - DTT-organism? - Bad bone/soft tissue? Short interval (2-3 weeks) No Unsatisfactory course? Yes Long interval (6-8 weeks)

20 Aim of PJI-algorithm To select the least invasive treatment option depending on the present features with the best functional result without compromising the cure rate!
21 Surgical procedures Type of surgery Intervention Antibiotics (total 12 weeks) Retention of fixed prosthetic components One-stage exchange Two-stage exchange (short interval) Change of mobile parts Explantation & implantation 2 weeks 10 weeks 2 weeks 10 weeks Explantation Implantation 2 we. 1 week 9 weeks Explantation Implantation Débridement & biopsies i.v. antibiotics without antibiofilm activity p.o. antibiotics without antibiofilm activity p.o. antibiotics with antibiofilm activity Ex- and reimplantation of prosthesis Two-stage exchange (long interval) Explantation 2 weeks 4 weeks 1 week 5 weeks Implantation Biofilm treatment Three-stage exchange 3 weeks 3 weeks 1 week 5 weeks
22 Surgical procedures Type of surgery Intervention Antibiotics (total 12 weeks) Retention of fixed prosthetic components One-stage exchange Two-stage exchange (short interval) Two-stage exchange (long interval) Three-stage exchange Change of mobile parts Explantation & implantation 2 weeks 10 weeks 2 weeks 10 weeks Explantation Implantation 2 we. 1 week 9 weeks Explantation Implantation 2 weeks 4 weeks 1 week 5 weeks Explantation Implantation 3 weeks 3 weeks 1 week 5 weeks Débridement & biopsies i.v. antibiotics without antibiofilm activity p.o. antibiotics without antibiofilm activity p.o. antibiotics with antibiofilm activity Ex- and reimplantation of prosthesis Osteomyelitis treatment
23 Strategy: long 2 W interval 1 W 9 W (6 weeks) Explantation 2 W Implantation 4 W 1 W 5 W Explantation Spacerwechsel No prosthesis 3 W 3 W Osteomyelitis therapy = Suppression Implantation Prosthesis 1 W 5 W Biofilm-active therapy = Eradication No rifampin during interval! rifampin
24 Surgical procedures No drug holidays before reimplantation Type of surgery Intervention Antibiotics (total 12 weeks) Retention of fixed prosthetic components One-stage exchange Two-stage exchange (short interval) Change of mobile parts Explantation & implantation 2 weeks 10 weeks 2 weeks 10 weeks Explantation Implantation 2 we. 1 week 9 weeks Explantation Implantation Débridement & biopsies i.v. antibiotics without antibiofilm activity p.o. antibiotics without antibiofilm activity p.o. antibiotics with antibiofilm activity Ex- and reimplantation of prosthesis Two-stage exchange (long interval) 2 weeks 4 weeks 1 week 5 weeks Explantation Implantation Three-stage exchange 3 weeks 3 weeks 1 week 5 weeks
25 Fast-track -study: Short vs. long interval in twostage prosthesis exchange Explantation 3 we Implantation Two stage (short interval) 4 weeks i.v. 8 weeks p.o. Explantation Implantation 7 weeks Two stage (long interval) 3 weeks i.v. 4 weeks p.o. 1 week i.v. 4 weeks p.o.
26 Median (days) Interval from explantation until reimplantation (hip & knee PJI) Cure rate >90% Year
27 Treatment concept of PJI: Acute infections (<3 weeks of symptoms) Stable prosthesis Good soft tissue No difficult to treat organism (see below) No Difficult-to-treat organism? Rifampin-R staphylococcus Ciprofloxacin-R Gram- rods Fungi Yes No Yes Debridement and retention One stage Only if good soft tissue or Two stage (short interval) Two stage (long interval) 2 weeks i.v. Explantation Explantation 6 weeks i.v. 10 weeks p.o. Explantation and implantation 2-3 weeks i.v. Implantation 2 weeks No treatment Implantation Debridement Biofilm treatment (with rifampin if applicable) Osteomyelitis treatment (no rifampin)






28 2 stage exchange: removal of all foreign material
29 No drug holidays No need: does not change the further treatment Not sensitive (local antibiotics if spacer in situ) Misleading (if false positive/contamination) Additional intervention - additional risk of infection Prolonged treatment (longer exposure to antibiotics and spacer, longer period of immobility) Holidays for patient = holidays for bacteria implantation of a new prosthesis when bacteria are recovered
30 Antibiotics




31 Properties of antibiotics Bactericidal activity Good oral bioavailability Knochenpenetration Good bone Activity against biofilms
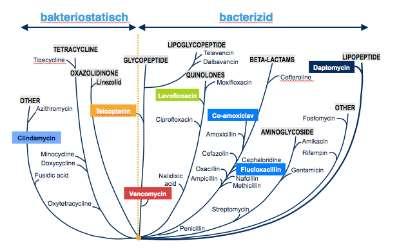
32 Bactericidal activity Bacteriostatic Bactericidal Tigecycline TETRACYCLINE OXAZOLIDINONE Linezolid LIPOGLYCOPEPTIDE Telavancin GLYCOPEPTIDE Dalbavancin QUINOLONES Moxifloxacin BETA-LACTAMS Ceftaroline Daptomycin LIPOPEPTIDE OTHER Azithromycin Clindamycin Minocycline Doxycycline Fusidic acid Oxytetracycline Teicoplanin Vancomycin Levofloxacin Ciprofloxacin Nalidixic acid Cefazolin Oxacillin Ampicillin Co-amoxiclav Amoxicillin Streptomycin Flucloxacillin Nafcillin Methicillin Fosfomycin AMINOGLYCOSIDE Amikacin Cephaloridine Rifampin Gentamicin OTHER Penicillin Rolinson GN. Int J Antimicrob Agents 2007;29:3 8
33 How much ends up in the bone? Drug Oral bioavailability Bone penetration Ampicillin/Sulbactam 50% 7% Cefuroxim, cefadroxil 50% 12% Levofloxacin 100% 77% Rifampin 80% 51% Cotrimoxazole 85% 55% Clindamycin 90% 45% Linezolid 100% 85% Sanford Guide to Antimicrobial Therapy nd ed. Lorian. Antibiotics in Laboratory Medicine. 5 th ed.
34 Antibiotics with biofilm-activity Staphylococci: rifampin (in combination) Gram-negative rods: ciprofloxacin Streptococci: penicillin G (amoxicillin p.o.) Enterococci: ampicillin + gentamicin

 Removal of cages after 5 days and sonication of cages Zimmerli W et al.")
35 Foreign body infection (FBI) model in guinea pigs Subcutaneous implantation of 4 Teflon cages Infection of cages with different inocula Systemic treatment of infection Aspiration of cage-fluid (planctonic bacteria?) Removal of cages after 5 days and sonication of cages Zimmerli W et al. J Clin Invest 1984;73:
36 Staphylococcal PJI El Helou et al. EJCMID 2010

37 Targeted therapy
38 Empiric treatment No specific exposure: Ampicillin/Sulbactam Fistula, VAC, multiple revisions etc: Piperacillin/Tazobactam Several previous interventions, MRSA-carrier: normal renal function (egfr > 60ml/min): add Vancomycin
39 Switch to oral treatment after surgery When CRP is nearly normalized... wound is closed and dry... organism and its susceptibility is known usually after 2 weeks
40 Rifampin precious but delicate
 Monitor liver enzymes (toxic hepatitis) Inform patient about red coloration of body fluids")
41 Rifampin Check interactions (CYP450-induction; anticoagulants, antiepileptics, antihypertensive agents, immunmodulators etc) Monitor liver enzymes (toxic hepatitis) Inform patient about red coloration of body fluids (urine, tears)

42 Rifampin: Quick emergence of resistance Do not use: Before surgery In the interval before re-implantation of prosthesis In open wounds As single antibiotic (monotherapy)
43 Therapy during interval: suppression Aim: suppression of the infection (no eradication) used substances: Organism Staphylococci Streptococci Enterococci Anaerobes Gram negative organisms substance Cotrimoxazol, Doxycyclin, Clindamycin Amoxicillin, Clindamycin, Levofloxacin Amoxicillin, (Linezolid) Clindamycin, Amoxicillin, Metronidazole Ciprofloxacin, Cotrimoxazol Seamless intake until implantation (no

44 Suppression with antibiotic cycling Longterm antibiotic therapy is splitted in treatment phases with different antibiotics instead of a single drug Changement of substance every 2-4 weeks 4 weeks cotrimoxazol Indications: No anti-biofilm-active agent available Intolerance of antibiotics/side effects 4 weeks drug holidays 4 weeks doxycyclin Benefits: 4 weeks Bacteria are getting confused prevention clindamycin of emergence of resistance Antibiotic tolerance is better, adverse effects are less
 adäquate Penetration in Haut/Weichteil, Knochen und Biofilm")
45 Warum Fosfomycin? Anforderung an ein Antibiotikum zur Therapie von Periprothetischen Infektionen (PPI) adäquate Penetration in Haut/Weichteil, Knochen und Biofilm Konzentrationsprofil nach Gabe von 100 mg/kg Fosfomycin Nach 3 h Knochenspiegel = Serum- /Weichgewebespiegel Fosfomycin Vancomycin Schintler 2009

46 Prosthetic Joint Infection Outcome with Fosfomycin The PROOF-study Andrej Trampuz, MD Head of Septic Surgery Unit Center for Musculoskeletal Surgery Charité University Medicine Berlin







47 Allergy Drug fever Toxic hepatitis Toxic nephritis Electrolyte imbalance Adverse effects Psychologic disturbances Myelosuppression C. difficile infection Diarrhea Eosinophilic pneumonia Achilles tendinopathy
 every 2-4 weeks Weight (>100kg and")
48 Monitoring und dose adjustment Monitoring Through level: Vancomycin 2x/week Dose adjustment Kidney function (egfr <60 or 50ml/min) Blood count, creatinin, electrolytes 1x/week Age: reduce dose in patients >75 Jahre Liver enzymes (Rifampin) every 2-4 weeks Weight (>100kg and <40kg)
49 Pathogenesis


50 Pathogenesis of PJI Contiguous spread from adjacent infected tissue Peri- /postinterventional colonisation 5% 20% Hematogenous spread from a distant focus through blood 75% PJIs treated at Charité, 01/ /2018
51 Diagnostic tests Positive test All episodes (n = 106) Increased serum CRP (>10 mg/l) 96/104 (92) Pathological WBC (>10 G/l or <4G/l) 61/104 (59) Elevated synovial fluid leukocyte count 64/64(100) Peri-implant tissue histopathology 86/95 (91) Culture (synovial fluid, tissue or sonication fluid) 99/106 (93) Blood culture 43/70 (61) PJI is easy to diagnose Rakow A, Renz N (own data)
52 Pathogens Highly virulent, i.e. S. aureus, gram-negative bacilli, Streptococcus spp. Rodriguez D, CMI 2010; Uckay I, CMI 2009; Tande AJ, Clin Microbiol Rev 2014 Predominantly monobacterial infections Coagulase-negative staphylococci, 8 Clostridium innocuum, 1 Culture-negative, 1 Gram-negative bacteria, monobacterial 1 polymicrobial 1 culture-negative Enterococcus faecalis, 13 Staphylococcus aureus, 43 Streptococcus spp., 32 Rakow A, Renz N (own data)
53 Primary foci: cohort of 106 episodes 1 (+3?) colon adenoma 1 GI bleeding 2 GI infections Gastrointestinal tract, 7 Others, 3 1 contralat. PJI 1 pneumonia 1 epidural abscess 7 dental treatments 5 dental infections Oral cavity, 12 Unknown, 34 2 manipulations 10 infections Urogenital tract, 12 Skin and soft tissue, 16 Cardiovascular system, 22 9 skin erosion (pedicure, skin disease, chronic ulcers) 7 skin and soft tissue infections 14 endocarditis 5 infected CIED 3 catheter infections Rakow A, Renz N (own data)
54 Investigation of cause Pathogen Source Diagnostics Staphylococci Blood cultures Echocardiography (TEE) Skin examination Streptococci S. oralis/mitis S. agalactiae S. dysgalactiae S. bovis/gallolyticus Enterococci Orthopantomogram (OPTG), dentist, TEE Urinanalysis, imaging abdomen, skin examination, OPTG Colonoscopy Urinanalysis, TEE Enterobacteriaceae Urinanalysis, CT Abdomen Renz N., Chirurg, 2017
55 Reality Bacteremia after tooth brushing and dental extraction Studies not usable (wrong design) Significant bacteremia after dental interventions Prophylaxis reduces bacteremia Clinical practice: association exsists 0 min 1.5min 5min 20min 40min 60min Lockhart PB. Circulation Prospective studies needed
56

57 Workshops:
58 Pocket Guide:


59 Consultation service:

60

 Diagnosis: Fast innovative")
61 Thank you Focus on implant, bone and joint-associated infections: Surgery: New concepts (retention, 1-stage, 2-stage short interval) Diagnosis: Fast innovative methods Antibiotics: Active against biofilms


62 Thank you! Consultation service Pocket Guide Workshops
Pocket Guide to Diagnosis & Treatment of Cardiovascular Implantable Electronic Device (CIED) Infections
 Infections") Pocket Guide to Diagsis & Treatment of Cardiovascular Implantable Electronic Device (CIED) Infections Draft Version : November 208 DEFINITION Pocket infection, if all 4 criteria are fulfilled: Investigation/sign
Pocket Guide to Diagsis & Treatment of Cardiovascular Implantable Electronic Device (CIED) Infections Draft Version : November 208 DEFINITION Pocket infection, if all 4 criteria are fulfilled: Investigation/sign
Pocket Guide to Diagnosis & Treatment of Vascular Graft Infections (VGI)
") Pocket Guide to Diagsis & Treatment of Vascular Graft Infections (VGI) DEFINITION Investigation /sign Local signs of infection Histopathology Microbiology Definitive Criteria Purulent wound secretion sinus
Pocket Guide to Diagsis & Treatment of Vascular Graft Infections (VGI) DEFINITION Investigation /sign Local signs of infection Histopathology Microbiology Definitive Criteria Purulent wound secretion sinus
Neurosurgical infections: New developments and outlook
 IMPLANTS 28.05.2015 Neurosurgical infections: New developments and outlook Andrej Trampuz, MD Infectious Diseases Specialist Head, Center for Septic Surgery Mª Eugenia Portillo, PhD Microbiologist Head,
IMPLANTS 28.05.2015 Neurosurgical infections: New developments and outlook Andrej Trampuz, MD Infectious Diseases Specialist Head, Center for Septic Surgery Mª Eugenia Portillo, PhD Microbiologist Head,
Pocket Guide to Diagnosis & Treatment of Ventricular Assist Device (VAD) Infections
 Infections") Pocket Guide to Diagnosis & Treatment of Ventricular Assist Device (VAD) Infections CLASSIFICATION OF VAD-INFECTIONS Draft Version 1: 1 November 2018 from Hannan M et al. Journal of Heart and Lung Transplantation,
Pocket Guide to Diagnosis & Treatment of Ventricular Assist Device (VAD) Infections CLASSIFICATION OF VAD-INFECTIONS Draft Version 1: 1 November 2018 from Hannan M et al. Journal of Heart and Lung Transplantation,
MANAGEMENT OF TOTAL JOINT ARTHROPLASTY INFECTIONS
 MANAGEMENT OF TOTAL JOINT ARTHROPLASTY INFECTIONS Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine TOTAL JOINT ARTHROPLASTIES In 2009: 1 million THA and TKA By 2030,
MANAGEMENT OF TOTAL JOINT ARTHROPLASTY INFECTIONS Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine TOTAL JOINT ARTHROPLASTIES In 2009: 1 million THA and TKA By 2030,
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how?
 Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Enterococcal PJI. Miquel Ekkelenkamp
 Enterococcal PJI Miquel Ekkelenkamp Enterococci: Gram-positive and round Formerly streptococci (but really quite different) Main clinical species : E. faecalis and E. faecium Mostly opportunistic pathogen
Enterococcal PJI Miquel Ekkelenkamp Enterococci: Gram-positive and round Formerly streptococci (but really quite different) Main clinical species : E. faecalis and E. faecium Mostly opportunistic pathogen
Antibiotic Prophylaxis Update
 Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
ANTIBIOTICS USED FOR RESISTACE BACTERIA. 1. Vancomicin
 ANTIBIOTICS USED FOR RESISTACE BACTERIA 1. Vancomicin Vancomycin is used to treat infections caused by bacteria. It belongs to the family of medicines called antibiotics. Vancomycin works by killing bacteria
ANTIBIOTICS USED FOR RESISTACE BACTERIA 1. Vancomicin Vancomycin is used to treat infections caused by bacteria. It belongs to the family of medicines called antibiotics. Vancomycin works by killing bacteria
Principles of Antimicrobial Therapy
 Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Help with moving disc diffusion methods from BSAC to EUCAST. Media BSAC EUCAST
 Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
LINEE GUIDA: VALORI E LIMITI
 Ferrara 28 novembre 2014 LINEE GUIDA: VALORI E LIMITI Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi EVIDENCE BIASED GERIATRIC MEDICINE Older patients with comorbid conditions
Ferrara 28 novembre 2014 LINEE GUIDA: VALORI E LIMITI Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi EVIDENCE BIASED GERIATRIC MEDICINE Older patients with comorbid conditions
Appropriate Antimicrobial Therapy for Treatment of
 Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Le infezioni di cute e tessuti molli
 Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Full Title of Guideline. Author: Contact Name and Job Title. Division & Speciality. Review date December 2020
 Full Title of Guideline Author: Contact Name and Job Title Division & Speciality Guideline for the treatment of prosthetic joint infections in adults Mr Peter James - Consultant Orthopaedic Surgeon Dr
Full Title of Guideline Author: Contact Name and Job Title Division & Speciality Guideline for the treatment of prosthetic joint infections in adults Mr Peter James - Consultant Orthopaedic Surgeon Dr
Management of Native Valve
 Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
The role of oral antibiotics in Prosthetic joint infection. Matthew Dryden MD
 The role of oral antibiotics in Prosthetic joint infection Matthew Dryden MD Persistence of bone infection Osteomyelitis in 1930 Prosthetic joint replacement demand is increasing When things go wrong Patient
The role of oral antibiotics in Prosthetic joint infection Matthew Dryden MD Persistence of bone infection Osteomyelitis in 1930 Prosthetic joint replacement demand is increasing When things go wrong Patient
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS
 VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Staph Cases. Case #1
 Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Introduction to Pharmacokinetics and Pharmacodynamics
 Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Routine internal quality control as recommended by EUCAST Version 3.1, valid from
 Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
GUIDELINE FOR ANTIMICROBIAL USE IN THE ORTHOPAEDIC AND TRAUMA DEPARTMENT
 GUIDELINE FOR ANTIMICROBIAL USE IN THE ORTHOPAEDIC AND TRAUMA DEPARTMENT Written by: Dr Ken. N. Agwuh, Consultant Microbiologist Mr Roger Helm, Consultant Orthopaedic Surgeon Mr T Kumar, Consultant Orthopaedic
GUIDELINE FOR ANTIMICROBIAL USE IN THE ORTHOPAEDIC AND TRAUMA DEPARTMENT Written by: Dr Ken. N. Agwuh, Consultant Microbiologist Mr Roger Helm, Consultant Orthopaedic Surgeon Mr T Kumar, Consultant Orthopaedic
Scottish Medicines Consortium
 Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
EUCAST recommended strains for internal quality control
 EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
Introduction to Chemotherapeutic Agents. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018
 Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
National Clinical Guideline Centre Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults
 National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Aminoglycosides. Spectrum includes many aerobic Gram-negative and some Gram-positive bacteria.
 Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Skin and Soft Tissue Infections Emerging Therapies and 5 things to know
 2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
MANAGEMENT STRATEGIES FOR ORTHOPEDIC IMPLANT-ASSOCIATED INFECTIONS. 5-6 March 2018 Berlin Germany. Endorsed by:
 MANAGEMENT STRATEGIES FOR ORTHOPEDIC IMPLANT-ASSOCIATED INFECTIONS 5-6 March 2018 Berlin Germany Endorsed by: Dear colleagues, It is our great pleasure to invite you to the first workshops on orthopedic
MANAGEMENT STRATEGIES FOR ORTHOPEDIC IMPLANT-ASSOCIATED INFECTIONS 5-6 March 2018 Berlin Germany Endorsed by: Dear colleagues, It is our great pleasure to invite you to the first workshops on orthopedic
Considerations for antibiotic therapy. Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen
 Considerations for antibiotic therapy Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen Infective Endocarditis There will never be a cure for this malignant disease! Sir
Considerations for antibiotic therapy Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen Infective Endocarditis There will never be a cure for this malignant disease! Sir
* gender factor (male=1, female=0.85)
") Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Medicinal Chemistry 561P. 2 st hour Examination. May 6, 2013 NAME: KEY. Good Luck!
 Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Doxycycline staph aureus
 Search Search Doxycycline staph aureus Mercer infection is the one of the colloquial terms given for MRSA (Methicillin-Resistant Staphylococcus Aureus ) infection. Initially, Staphylococcal resistance
Search Search Doxycycline staph aureus Mercer infection is the one of the colloquial terms given for MRSA (Methicillin-Resistant Staphylococcus Aureus ) infection. Initially, Staphylococcal resistance
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS
 PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
2012 ANTIBIOGRAM. Central Zone Former DTHR Sites. Department of Pathology and Laboratory Medicine
 2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
New Antibiotics for MRSA
 New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
Who should read this document? 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version? 3
 Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
Antibacterials. Recent data on linezolid and daptomycin
 Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center
 Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center Case 1 60 yo healthy female admitted for fevers and dysuria.
Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center Case 1 60 yo healthy female admitted for fevers and dysuria.
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Best Antimicrobials for Staphylococcus aureus Bacteremia
 Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Antimicrobial Susceptibility Testing: Advanced Course
 Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate
 Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Diagnosis: Presenting signs and Symptoms include:
 PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Compliance of manufacturers of AST materials and devices with EUCAST guidelines
 Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
Compliance of manufacturers of AST materials and devices with EUCAST guidelines Data are based on questionnaires to manufacturers of materials and devices for antimicrobial susceptibility testing. The
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Source: Portland State University Population Research Center (
 Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani
 Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Discussion Points. Decisions in Selecting Antibiotics
 Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Clinical Practice Standard
 Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
Inappropriate Use of Antibiotics and Clostridium difficile Infection. Jocelyn Srigley, MD, FRCPC November 1, 2012
 Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
S aureus infections: outpatient treatment. Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium
 S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
January 2014 Vol. 34 No. 1
 January 2014 Vol. 34 No. 1. and Minimum Inhibitory Concentration (MIC) Interpretive Standards for Testing Conditions Medium: diffusion: Mueller-Hinton agar (MHA) Broth dilution: cation-adjusted Mueller-Hinton
January 2014 Vol. 34 No. 1. and Minimum Inhibitory Concentration (MIC) Interpretive Standards for Testing Conditions Medium: diffusion: Mueller-Hinton agar (MHA) Broth dilution: cation-adjusted Mueller-Hinton
Should we test Clostridium difficile for antimicrobial resistance? by author
 Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
Antibiotic Prophylaxis in Spinal Surgery Antibiotic Guidelines. Contents
 Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE
 ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE Version 1.0 Date ratified June 2009 Review date June 2011 Ratified by Authors Consultation Nottingham Antibiotic Guidelines Committee
ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE Version 1.0 Date ratified June 2009 Review date June 2011 Ratified by Authors Consultation Nottingham Antibiotic Guidelines Committee
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
21 st Expert Committee on Selection and Use of Essential Medicines Peer Review Report Antibiotics Review
 (1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
(1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
2017 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
MRSA. ( Staphylococcus aureus; S. aureus ) ( community-associated )
 ( community-associated )") 005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
DOI: /zenodo
 www.imiamn.org.ua /journal.htm 38 UDC 616-008.87:616-002:616-089.843 MICROBIOLOGICAL PARAMETERS IN PATIENTS WITH INFLAMMATORY COMPLICATIONS AFTER KNEE AND HIP JOINTS ENDOPROSTHESIS REPLACEMENT AND THEIR
www.imiamn.org.ua /journal.htm 38 UDC 616-008.87:616-002:616-089.843 MICROBIOLOGICAL PARAMETERS IN PATIENTS WITH INFLAMMATORY COMPLICATIONS AFTER KNEE AND HIP JOINTS ENDOPROSTHESIS REPLACEMENT AND THEIR