Sepsis Pearls & Pitfalls in Infectious Diseases
|
|
|
- Lorena McBride
- 5 years ago
- Views:
Transcription




1 Sepsis Pearls & Pitfalls in Infectious Diseases Gompol Suwanpimolkul MD., M.Sc. Assistant Professor of Medicine Infectious Diseases Division Internal Medicine Department King Chulalongkorn Memorial Hospital Thai Red Cross Society
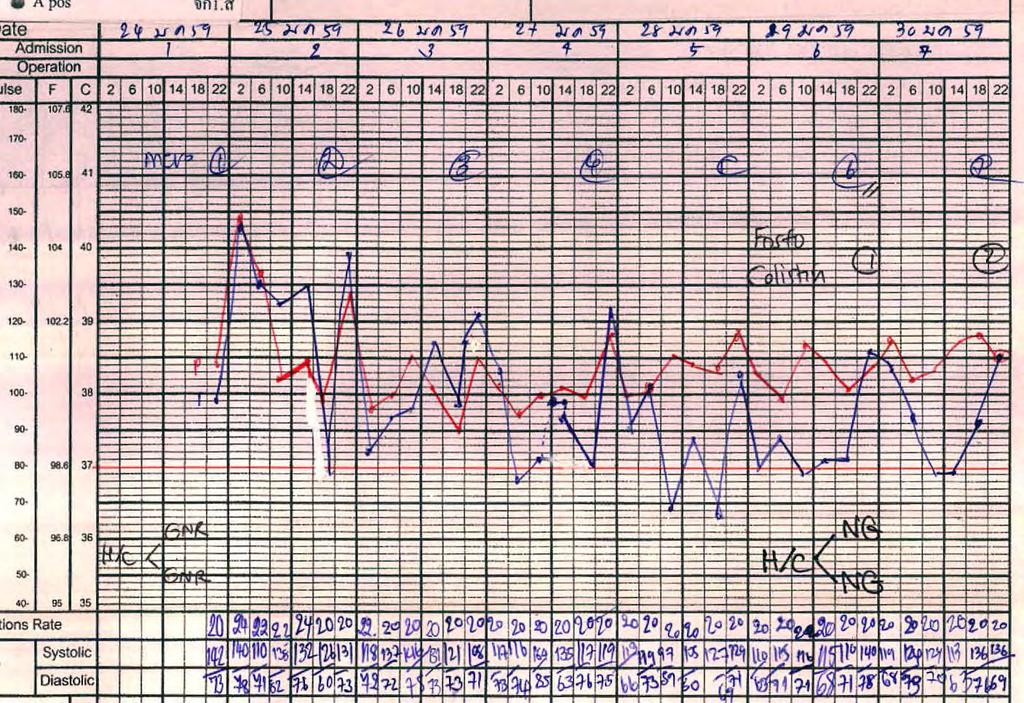
2 Present illness Previous status : Could do ADL functional class I CC: fever with chill for 1 day PTA Underlying: CA colon (adenocarcinoma) present with clinical gut obstruction 6 wks before this admission (24/1/2559) 9/12/58 Clinical gut obstruction Colonoscope: mass at sigmoid colon 5 x 4 cm bx: adeno CA Dx: CA sigmoid colon invade bladder with obstruction 12/12/58 Flexible cystoscopy with loop transverse colostomy 19/12/58 Pelvic exenteration with ileal conduit 2/1/59 post op 2 wks Fever with chill CT abdomen (4/01/59) H/C NG, Rx meropenem x 10 days

3 4/1/2559 There is a rim enhancing fluid collection in pelvic cavity measuring about 1.2x8.7 cm


4 4/1/2559 There is another 4.3 x 4.3 cm rim-enhancing fluid collection with internal air bubbles in pelvic cavity
5 Present illness Previous status : Could do ADL functional class I CC: fever with chill for 1 day PTA Underlying: CA colon (adenocarcinoma) present with clinical gut obstruction 6 wks before this admission (24/1/2559) 9/12/58 Clinical gut obstruction Colonoscope: mass at sigmoid colon 5 x 4 cm bx: adeno CA Dx: CA sigmoid colon invade bladder with obstruction 12/12/58 Flexible cystoscopy with loop transverse colostomy 19/12/58 Pelvic exenteration with ileal conduit 2/1/59 post op 2 wks Fever with chill CT abdomen (4/01/59) H/C NG, Rx meropenem x 10 days 12/1/59 D/C Off drain
6 Developed fever with chill 1 day PTA (2 weeks after previous admission)
7 Physical examination A middle aged Thai male patient, alert GA: drowsiness BT 41C, RR 24/min, PR 150 bpm regular, BP 90/60 mmhg Skin: normal skin turgor HEENT: not pale conjunctiva, anicteric sclera Lung: tachypnea, trachea in midline, equal, no adventitious sound Abdomen: colostomy, active bowel sound Load NSS fluid 500 cc at ER BP 110/70
8

9 JAMA. 2016;315(8):

10 Creatinine baseline 1.02
11 Creatinine baseline 1.02 Na 135, K 4.5, CL 100, HCO3 14, Lactate 2

12 JAMA. 2016;315(8):
![Sequential [Sepsis-Related] Organ Failure](/docs-images/95/124641222/images/13-1.jpg "Assessment Score JAMA. 2016;315(8):801-810.")
13 Sequential [Sepsis-Related] Organ Failure Assessment Score JAMA. 2016;315(8):
14 ( 2 mmol/l) JAMA. 2016;315(8):
15 What is the best empirical antibiotic (s)?
16 Have a guess! What s organism?? 1. Acinetobacter baumanni 2. Pseudomonas aeruginosa 3. Stenotrophomonas maltophilia 4. Klebsiella pneumoniae
17 BMC Infectious Diseases 2014, 14:489
18 Septicemia Exogenous (Environment or zoonosis) Commensal bacteria (normal microflora*) Gram positive Gram negative Gram positive Gram negative Bacillus antracis S. suis Listeria sp. Aeromonas spp. Vibrio spp. Salmonella cholerasuis C. canimorsus Burkholderia pseudomallei S. pneumoniae Viridans streptococcus S. pyogenes S. aureus coagulase negative Staphylococci Enterococci spp. N.menigitidis H. influenza E.coli Klebsiella spp. Enterobacter spp. Pseudomonas spp. * Microflora in special population: ICU patient, prolonged board spectrum antibiotic, neutropenia: Multi-drug resistance organism, Acinetobacter baumannii, Pseudomonas aeruginosa, Stenotrophomonas maltophilia, Candida spp.
19 H/C: Klebsiella pneumoniae x II (8.5, 9 hr.)
20 Which is the best appropriate antibiotic? 1. Meropenem 2. Piperacillin/Tazobactam 3. Trimethoprim-sulfamethoxazole 4. Colistin 5. Fosfomycin 6. Colistin + Meropenem
21 Percentage of susceptible bacteria department of microbiology Faculty of Medicine Chulalongkorn University Not included; colistin and Tigly Acinetobacter baumanni Pseudomonas aeruginosa E. coli Klebsiella pneumoniae Carbapenem (% susceptible) Cefoper/Sulbac Pip/Tazo Ceftazidime Amikacin
22
23
24 Doripenem R > 32 µg/ml Fosfomycin R >1024 µg/ml Imipenem R 8 µg/ml Meropenem R 16 µg/ml Colistin - 2 µg/ml Trimethoprim-sulfamethoxazole S µg/ml

25 Still high grade fever despite of colistin day 4

26 4/1/ /1/2559 Post removed drainage tube in pelvic cavity with resolution of 2 rim enhancing intraabdominal fluid collection as well as resolution of circumferential bowel wall thickening

27 30/1/2559 Interval developed ill defined hypodense lesions scatter in both renal parenchyma, more prominent in right side, probable lobar nephronia and/or early abscess formation


28 4/2/2559 Several ill defined hypodense lesions scattered in the right kidney, measured up to 2.5 cm with perinephric fat stranding and thickening of renal fascia likely abscess formation
29 7/2/2559 Interventionist simple aspiration Turbid fluid 8 cc
30 Aspirate renal abscess

31 Aspirate renal abscess

32 Trimethoprim-sulfamethoxazole
33 Empiric antimicrobial choice? Administration of effective intravenous antimicrobials within the first hour of recognition of septic shock (grade 1B) and severe sepsis without septic shock (grade 1C) as the goal of therapy. Initial empiric anti-infective therapy of one or more drugs that have activity against all likely pathogens (bacterial and/or fungal or viral) and that penetrate in adequate concentrations into tissues presumed to be the source of sepsis (grade 1B). Crit Care Med 2013; 41:
34 Combination therapy Combination therapy for suspected or known Pseudomonas aeruginosa or other multidrug-resistant Gram-negative pathogens, pending susceptibility results, increases the likelihood that at least one drug is effective against that strain and positively affects outcome Empiric combination therapy should not be administered for more than 3 5 days. De-escalation to the most appropriate single therapy should be performed as soon as the susceptibility profile is known (grade 2B). Crit Care Med 2007; 35: JAMA 2012; 307: Crit Care Med 2013; 41:
35 Adequate antimicrobial therapy First, antimicrobial agent(s) should be initiated as soon as possible after the onset of sepsis Second, empirically, should be broad enough to cover the potential causative microorganisms Finally, appropriate antimicrobial dosing to Maximize microbial killing Minimize the development of multidrug antimicrobial resistance and Avoid concentration-related adverse drug reactions. F. Pea. Clin.Infect.Dis.2006;42:
36 Antibiotic dosing for patients who are critically ill Early and appropriated antibiotic administration reduces mortality rates but less information is available about the effect of appropriate dose regimens on clinical outcome one dose fits all Jason Roberts. Lancet Infect Dis 2014;14:498
37 The range of altered pathophysiology in patients with critical illness and it effects on drug concentrations Critical illness Hyperdynamic Increased cardiac output Altered fluid balance Third spacing or altered protein binding No organ dysfunction Renal or Hepatic dysfunction Organ support RRT, ECMO Increased clearance (CL) Increased volume of Distributions (Vd) Unchanged Vd And clearance Increased Vd and Decrease CL Increased Vd and possible CL Decrease plasma concentrations Decrease plasma concentrations Normal plasma concentrations Increased plasma concentrations Increased or decreased plasma concentrations RRT=renal replacement therapy ECMO=extracorporeal membrane oxygenation Jason A Roberts. Lancet Infect Dis 2014;14:
38 PK/PD Observed in Critically Ill Patients Volume of distribution change: Hydrophilic drugs Half life of antibiotics: Augmented renal clearance (GFR > 130 ml/1.73 m2 in sepsis) Many hydrophilic drugs are eliminate by GFR Hypoalbuminemia: High protein bound antibiotics Tissue penetration: Low tissue penetration End Organ dysfunction (Renal) : Hydrophilic drug - Time dependent: Decrease dose - Concentration dependent: increase interval - Mode of dialysis End Organ dysfunction (Hepatic) : Lipophilic drug Advanced Drug Delivery Reviews 2014;77:3 11
 have epithelial lining fluid to plasma exposure ratio of at least 1 High exposure ratios are not always seen for hydrophilic antibiotics")
39 Effect of critical illness on antibiotic pharmacokinetics Pulmonary system Optimum antibiotic concentrations in the Epithelial lining fluid determine therapeutic success The more lipophilic antibiotics (Fluroquinolone, macrolides and oxazolidinones) have epithelial lining fluid to plasma exposure ratio of at least 1 High exposure ratios are not always seen for hydrophilic antibiotics Extracellular pathogen Therefore, hydrophilic drugs suggest the use of higher doses in severe pneumonia, extended or continuous infusion of β lactam antibiotics or administration via nebulization Jason Roberts. Lancet Infect Dis 2014;14:498
40 Antibiotics and Sites of infection Agents target antibiotics Lipid-soluble agents blood-brain barrier chloramphenicol, trimethoprim and isoniazid Highly ionized poor BBB aminoglycoside compound High concentrated excreted by ampicillin, doxycycline* in the bile liver Superior concen bone/prostate (new) fluroquinolones in the bone/prostate * More effective than 1 st gen cephalosporins or amimoglycoside (not greatly con in bile) in treating cholangitis Mandell 2014
41 Antibiotics and Local factors Local factors sites poor antibiotics concentration Pulmonary surfactant Lung daptomycin* Bound to and inactivated abscesses by purulent material** Aminiglycoside ***, polymyxins Bound by hemoglobin hematoma penicillin, tetacyclines Glycocalyx, biofilm foreign body interfere with phagocytosis *daptomycin is bound by pulmonary surfactant ** Penicillin may be more active in purulent material, clinical experience strongly suggests that appropriate drainage greatly enhance the efficacy *** inactive against anaerobic condition: oxygen is required for the transport of aminoglycoside into the bacterial cell Mandell 2014
42 Review of pathophysiological alterations during critical illness and their potential effect on pharmacokinetics of antimicrobial agents. SIRS, systemic inflammatory response syndrome; Vd, volume of distribution.
43 Hydrophilic antimicrobials Aminoglycosides Beta-lactams Carbapenems Cephalosporins Penicillins Glycopeptides Polymyxin B Fosfomycin Low Vd Low intracellular penetration Predominant renal clearance sepsis Lipophilic antimicrobials Fluroquinolones Glycylcycline Macrolides Metronidazole Tetracyclines Lincosamides Trimethoprim-sulfamethoxazole Clindamycin High Vd Good intracellular penetration Predominant hepatic clearance sepsis Need for increased loading dose Need for increased or decreased maintenance dose No need for increased loading dose No need for maintenance dose adjustments* Physicochemical properties of antimicrobial in severe sepsis. *Need for dose reductions only indicated in case of severe hepatic failure.
44 Hypoalbuminemia: High protein bound antibiotics (>85-90%) Reduce concentration of albumin could raise the unbound fractions of protein-bound drugs (free drug ) Unbound fractions antibiotic are available not only for elimination but also for distribution Impact on antibiotics that high protein binding Ceftriaxone Cloxacillin Ertapenem Daptomycin Hypoalbumin may contribute to initial target concentrations but failure to maintain sufficient drug throughout the dosing interval Jason A Roberts. Lancet Infect Dis 2014;14:
45 Optimal dosage to start antimicrobial therapy It must be considered that the target plasma concentration (Ct) that is achieved with the first dose - loading dose (LD) depends solely on the volume of distribution (Vd) of the drug (LD = Ct Vd) - Maintenance dose (LD) depends solely on the Clearance of the drug (MD = Ct CL) Federico Pea1 and Pierluigi Viale, Bench-to-bedside review: Appropriate antibiotic therapy in severe sepsis and septic shock - does the dose matter?, Critical Care 2009, 13:214 (doi: /cc7774)
46 Concentration-dependent antibiotics The efficacy of these agents is related to the achievement of high Cmax/MIC ratio (>10) and AUC/MIC ratio (>100 to 125) Accordingly, high dosage, short-course therapy regimens with a once daily administration schedule may yield more rapid bacterial killing or prevention of resistance development Federico Pea1 and Pierluigi Viale, Bench-to-bedside review: Appropriate antibiotic therapy in severe sepsis and septic shock - does the dose matter?, Critical Care 2009, 13:214 (doi: /cc7774)
47 Time-dependent antibiotics strongly suggest that extended infusion of β-lactams may improve clinical outcome in critically ill patients with severe infections, and indicate that continuous infusion may be the best approach in terms of maximizing efficacy with time-dependent antimicrobials. Indeed, the stability of an antibiotic in solution at room temperature is an important consideration when choosing to administer time-dependent antibiotics by continuous infusion Federico Pea1 and Pierluigi Viale, Bench-to-bedside review: Appropriate antibiotic therapy in severe sepsis and septic shock - does the dose matter?, Critical Care 2009, 13:214 (doi: /cc7774)
48 Stability of time-dependent antibiotics in solution for intravenous infusion Antibiotic Time of stability at Solvent Room temperature (+25 C; hours) Piperacillin/tazobactam >72 Sterile water for injection Ceftazidime 24 Sterile water for injection Imipenem 3.3 Sterile water for injection Meropenem 5.15 Sterile water for injection Vancomycin >696 Sterile water for injection Stability was defined as times during which antibiotic remains >90% stable in solution Critical Care 2009, 13:214
49 Time dependent antibiotic Continuous drip vs Conventional
50 Time dependent antibiotic Continuous drip vs bolus Ann Pharm 2006 (Spain) (VAP) Mero 1 gm drip 360 min q 6 h (N=42) Mero 1 gm drip 30 min q 6 h (N=47) P-value Clinical cure rate MIC > 0.5 MIC % 80.95% 100% 59.57% 29.41% 76.67% < Clin Ther 2007 (Spain) (VAP) Cefta 2 g drip 720 min q 12 h (N=56) Cefta 2 g drip 30 min q 12 h (N=65) P-value Clinical cure rate MIC = 8 MIC = % 75% 90% 52.3% 14.3% 38.5% <
51 Time dependent antibiotic Continuous drip vs bolus Int J Anti A 2009 (Spain) (VAP) Pip/Tazo 4.5 g drip 360 min q 6 h (N=37) Pip/Tazo 4.5 g drip 30 min q 6 h (N=46) P-value Clinical cure rate MIC = 4 MIC = 8 MIC = % 90.6% 88.9% 87.5% 56.5% 76% 40% 16.7% < J Crit Care 2010 (USA) (HAP) Mero 2 gm drip 3 h q 8 h (N=94) Mero 2 gm drip 30 min q 8 h (N=74) P-value Mortality rate 8.5% 21.6% <0.029
52 Time dependent antibiotic Continuous drip vs bolus CID 2007 (USA) (Pseudomonas sepsis) Pip/Tazo g drip 240 min q 8 h (N=102) Pip/Tazo g drip 30 min q 8 h (N=92) P-value Mortality rate APACHE II < 17 APACHE II % 12.2% 3.7% 31.6% Prospective multicenter Double-blind randomized controlled trial CID 2013 (5 Australia, 1 HK) (Severe sepsis) Mero or Pip/Tazo continuous infusion (N=30) Mero or Pip/Tazo bolus (N=30) P-value Plasma antibiotic concentration >MIC Clinical cure with in 28 days Survival hospital discharge 82% 70% 90% 29% 43% 80%
,")
53 Joel M. Dulhunty. Am J Respir Crit Care Med 20015; The BLING II study was a prospective, multicenter, double-blind, double-dummy, randomized controlled trial It was conducted in 25 ICUs in Australia (17), New Zealand (7), and Hong Kong (1) Carbapenem or Piperacillin/Tazobactam The primary outcome was the number of alive ICU-free days at Day 28. Secondary outcomes were 90-day survival, clinical cure 14 days post antibiotic cessation, alive organ failure free days at Day 14, and duration of bacteremia.

54 Baseline Characteristics of the Intention-to-Treat Population Joel M. Dulhunty. Am J Respir Crit Care Med 20015;

55 Microbiologic Characteristics Identified organisms only 19% of cases > 50% were E.coli and Klebsiella pneumoniae, drug resistant less than 4% Joel M. Dulhunty. Am J Respir Crit Care Med 20015;

56 Primary and Secondary Outcomes, Clinical Results, and Adverse Events Joel M. Dulhunty. Am J Respir Crit Care Med 20015;
57 Discussion Limitations of the study: Why negative outcome? 1. Microbiological documented only 19% of patients Possibility that a significant number of patients with noninfectious causes mimicking severe sepsis were enrolled 2. Not demonstrated of MIC The theoretical advantage of continuous infusion is crucially dependent on the MIC more useful among high MIC Organisms are highly susceptible to antibiotics the probability of not reaching PK-PD target using conventional dosing is very small very low prevalence of E.coli and K. pneumoniae resistance (0-4.5%) in Australia 3. Not demonstrated of PK/PD: some beta-lactam need target only 70% ft > MIC to achieve clinical cure, arguing that more prolonged exposure might not be necessary
58 Studies reporting PK/PD indices from preclinical and clinical assessments, by antibiotic class Antibiotics Clinical studies Concentration dependent Aminoglycoside Clinical cure Cmax/MIC 8-10; AUC/MIC > 70 Time-dependent Carbapenems Clinical cure 75% T>MIC Microbiological cure 54% T>MIC Cephalosporins Clinical cure 100% T>MIC Microbiological cure % T>MIC Penicillins Clinical cure - Microbiological cure 40-50% T>MIC Concentration dependent and Time-dependent Fluroquinolones Clinical cure AUC0-24/MIC > ; Cmax/MIC >8 Microbiological cure AUC0-24/MIC >34-125; Cmax/MIC >8 Vancomycin Clinical cure AUC0-24/MIC > Microbiological cure AUC0-24/MIC >400 Tigecycline Clinical cure AUC0-24/MIC > Microbiological cure AUC0-24/MIC > Jason A Roberts. Lancet Infect Dis 2014;14:
59 General PK characteristics of various antibiotics and possible changes that can occur during fluid shift in critically ill patients Antibiotic class Increased Vd Decreased Cmax Plasma Protein CL TDM required? with with T1/2 (h) binding fluid shift fluid shift Aminoglycosides Yes Yes 2-3 Low by renal function Yes, to ensure high Cmax and adequate CL Β-lactams Yes Yes (except Low (except by renal function optional Ceftri 6-9 h) ceftri* & Cloxa Carbapenems Yes Yes 1 (except Low (except by renal function optional Erta 4 h) Ertapenem) Glycopeptides Yes Yes Vanco (4-6) 30-55% by renal function to ensure plasma Cmin > 15 mg/ml Tigecycline Unlikely Unlikely % decrease with cholestasis No Colistin likely likely Unknown by renal function optional Ceftriaxone > 95% bound to albumin Hypoalbuminemic in critical ill unbound drug (free) has a 100 increased CL and 90% greater of Vd Jason A Roberts. Crit Care Med 2009;37(3):843
60 Antimicrobial Therapy in Patients Receiving Renal Replacement Therapy Type of antibiotics The mode of RRT Mode of replacement fluid administration (predilution or postdilution) and Dose of RRT delivered** Effluent volume: most important Effluent volume is dependent on both effluent flow and duration of CRRT Filter surface area on the ultrafiltration and/or: Very high ultrafiltration flow (QUF) > 2-3 l/hour dialysate flow rates (QD) Very high dialysate flow rates (QD) > 1-2 l/hour F. Pea. Clin Pharmacokinet 2007; 46 (12): J A Jamal Curr Opin Crit Care 2012;18:
61 Renal replacement therapy vs Antibiotics In general drugs with High volumes of distribution (> 1 L/kg) Lipophilic drugs or High protein bound (more than 80%) poorly eliminated by renal replacement therapy
62 Renal replacement therapy Continuous RRT can be applied as continuous venovenous hemofiltration (CVVH), continuous venovenous hemodialysis (CVVHD), and continuous venovenous hemodiafiltration (CVVHDF) Intermittent Sustained low-efficiency dialysis (SLED): Hybrid modality J.A.Jamal. Curr.Opin.Crit.Care 2012;18:
63 Antimicrobial Therapy in Patients Receiving Renal Replacement Therapy Removal of solutes from the blood through semi-permeable membranes during RRT may occur by means of two different physicochemical processes, namely, diffusion or convection. Intermittent haemodialysis (IHD) is essentially a diffusive technique and CVVH is a convective technique, CVVHDF is a combination of both. As a general rule, the efficiency of drug removal by the different techniques is expected to be CVVHDF > CVVH > IHD CLCRRT is expected to be clinically relevant for drugs with dominant renal clearance, especially when presenting a limited volume of distribution and poor plasma protein binding. F. Pea. Clin Pharmacokinet 2007; 46 (12):
64 Antimicrobial Therapy in Patients Receiving Renal Replacement Therapy Consistently, CLCRRT should be clinically relevant particularly for most hydrophilic antimicrobial agents (e.g. β-lactams, aminoglycosides, glycopeptides), whereas it should assume much lower relevance for lipophilic compounds (e.g. fluoroquinolones, oxazolidinones), which generally are nonrenally cleared. However, there are some notable exceptions: ceftriaxone and oxacillin, although hydrophilics, are characterised by primary biliary elimination levofloxacin and ciprofloxacin, although lipophilics, are renally cleared. F. Pea. Clin Pharmacokinet 2007; 46 (12):
65 Sustained low-efficiency dialysis (SLED: Hybrid modality ) All of these approaches are very efficient in removing hydrophilic antimicrobials, in particular those with low protein binding properties and high renal clearance Time-dependent antibiotics such as β-lactams: need supplemental doses of antibiotics during or follow SLED treatment or prolong infusion times to maintain T>MIC J A Jamal Curr Opin Crit Care 2012;18:

66 Continuous venovenous hemodialysis. The countercurrent flow maintains a concentration gradient across the membrane. Protein bound molecules are unable to cross the membrane G Choi Crit Care Med 2009 Vol. 37, No. 7

67 A, Hemofiltration (continuous venovenous hemofiltration) (predilution). Dilution of blood with replacement fluid before the blood enters the filter results in a fall in concentration in the filter and hence a reduction in efficiency of solute removal. Protein bound molecules are unable to cross the membrane. B, Hemofiltration (continuous venovenous hemofiltration) (postdilution). G Choi Crit Care Med 2009 Vol. 37, No. 7
68 Critical ill septic patient Loading dose: Vd hydrophilic drugs Maintain dose: CL Large volume of distribution Large volume resuscitate Invasive ventilation Surgical procedure Initial High Loading Dose Renal or hepatic impairment Vasopressors Increase CO Increase diuresis No Yes Increase Clearance or Adjust dose accordingly Augmented Renal Clearance (ARC) (>120 ml/min per 1.73 m2) Maintain high dose Reassess after hr. Any of: Bacteria with low MIC Normalization of creatinine clearance Sepsis resolution Adjust Dose
69 Conclusions We should start antimicrobial within 1 hours after diagnosis Initial empiric anti-infective therapy of one or more drugs that have activity against all likely pathogens Combination empirical therapy for Neutropenic patients with severe sepsis Multidrug-resistant bacterial pathogens such as Acinetobacter and Pseudomonas spp., CRE BL/BI plus aminoglycide or quinolone or Carbapenem plus aminoglycide or quinolone Empiric combination therapy should not be administered for more than 3 5 days. Source control is also very important
70 Conclusions Five main issues can be detected in critically ill patients regarding altered PK: increased volume of distribution (Vd), altered protein binding, augmented renal clearance, impaired renal clearance and hepatic dysfunction
71 Conclusions loading dose (LD) depends on the volume of distribution (Vd) of the drug Maintenance dose (LD) depends on the Clearance of the drug Volume of distribution change in critical illness: Hydrophilic drugs suboptimal level Time dependent antibiotics: prefer CI or extended infusion (Stability and drug compatibility), particularly in high MIC organisms.
72 Thank you for your attentions!
Antimicrobial Pharmacokinetics/dynamics Bedside Applications in the Critically Ill
 Antimicrobial Pharmacokinetics/dynamics Bedside Applications in the Critically Ill Arthur RH van Zanten, MD PhD Internist-intensivist Department of Intensive care Gelderse Vallei Hospital, Ede The Netherlands
Antimicrobial Pharmacokinetics/dynamics Bedside Applications in the Critically Ill Arthur RH van Zanten, MD PhD Internist-intensivist Department of Intensive care Gelderse Vallei Hospital, Ede The Netherlands
Pharmacokinetics and Pharmacodynamics of Antimicrobials in the Critically Ill Patient
 Pharmacokinetics and Pharmacodynamics of Antimicrobials in the Critically Ill Patient Rania El-Lababidi, Pharm.D., BCPS (AQ-ID), AAHIVP Manager, Pharmacy Education and Training Cleveland Clinic Abu Dhabi
Pharmacokinetics and Pharmacodynamics of Antimicrobials in the Critically Ill Patient Rania El-Lababidi, Pharm.D., BCPS (AQ-ID), AAHIVP Manager, Pharmacy Education and Training Cleveland Clinic Abu Dhabi
Introduction to Pharmacokinetics and Pharmacodynamics
 Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
Antimicrobial therapy in critical care
 Antimicrobial therapy in critical care KARLEE JOHNSTON LEAD PHARMACIST DIVISION OF CRITICAL CARE CANBERRA HOSPITAL AND HEALTH SERVICE Outline 1. Let s talk about sepsis 2. PK/PD considerations 3. Selecting
Antimicrobial therapy in critical care KARLEE JOHNSTON LEAD PHARMACIST DIVISION OF CRITICAL CARE CANBERRA HOSPITAL AND HEALTH SERVICE Outline 1. Let s talk about sepsis 2. PK/PD considerations 3. Selecting
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams
 DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Int.J.Curr.Microbiol.App.Sci (2017) 6(3):
 6(3):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
2012 ANTIBIOGRAM. Central Zone Former DTHR Sites. Department of Pathology and Laboratory Medicine
 2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali. Lec 1
 Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia. Po-Ren Hsueh. National Taiwan University Hospital
 Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
These recommendations were approved for use by the Pharmaceutical and Therapeutics Committee, RCWMCH on 1 February 2017.
 Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy
 Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy Leonardo Pagani MD Director Unit for Hospital Antimicrobial Chemotherapy
Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy Leonardo Pagani MD Director Unit for Hospital Antimicrobial Chemotherapy
Dr. Shaiful Azam Sazzad. MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College
 Critical Care Medicine Dhaka Medical College") Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
ICU Volume 14 - Issue 4 - Winter 2014/ Matrix
 ICU Volume 14 - Issue 4 - Winter 2014/2015 - Matrix Antibiotic Management in the ICU Eleni Patrozou ******@***gmail.com Intensivist - Hygeia Hospital, Athens, Greece Infectious Diseases Division - Alpert
ICU Volume 14 - Issue 4 - Winter 2014/2015 - Matrix Antibiotic Management in the ICU Eleni Patrozou ******@***gmail.com Intensivist - Hygeia Hospital, Athens, Greece Infectious Diseases Division - Alpert
Mono- versus Bitherapy for Management of HAP/VAP in the ICU
 Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
Antimicrobial Susceptibility Testing: Advanced Course
 Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections
 for the treatment of Acinetobacter baumannii infections") ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
ANTIMICROBIAL PRESCRIBING Optimization through Drug Dosing and MIC
 ANTIMICROBIAL PRESCRIBING Optimization through Drug Dosing and MIC PREFACE INTRODUCTION The wide use and frequent misuse of antimicrobials in all countries has resulted in the emergence of drug resistance,
ANTIMICROBIAL PRESCRIBING Optimization through Drug Dosing and MIC PREFACE INTRODUCTION The wide use and frequent misuse of antimicrobials in all countries has resulted in the emergence of drug resistance,
2015 Antibiogram. Red Deer Regional Hospital. Central Zone. Alberta Health Services
 2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
48 th Annual Meeting. IDWeek and ICAAC: The Cliffs Notes Version. Skin and Soft Tissue Infections. Skin and Soft Tissue Infections.
 48 th Annual Meeting IDWeek and ICAAC: The Cliffs Notes Version Yanina Pasikhova Pharm.D., BCPS-AQ ID, AAHIVP Infectious Diseases Pharmacist Moffitt Cancer Center Navigating the Oceans of Opportunity Skin
48 th Annual Meeting IDWeek and ICAAC: The Cliffs Notes Version Yanina Pasikhova Pharm.D., BCPS-AQ ID, AAHIVP Infectious Diseases Pharmacist Moffitt Cancer Center Navigating the Oceans of Opportunity Skin
Cost high. acceptable. worst. best. acceptable. Cost low
 Key words I Effect low worst acceptable Cost high Cost low acceptable best Effect high Fig. 1. Cost-Effectiveness. The best case is low cost and high efficacy. The acceptable cases are low cost and efficacy
Key words I Effect low worst acceptable Cost high Cost low acceptable best Effect high Fig. 1. Cost-Effectiveness. The best case is low cost and high efficacy. The acceptable cases are low cost and efficacy
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Management of Hospital-acquired Pneumonia
 Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Pharmacology Week 6 ANTIMICROBIAL AGENTS
 Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Proceedings of the 13th International Congress of the World Equine Veterinary Association WEVA
 www.ivis.org Proceedings of the 13th International Congress of the World Equine Veterinary Association WEVA October 3-5, 2013 Budapest, Hungary Reprinted in IVIS with the Permission of the WEVA Organizers
www.ivis.org Proceedings of the 13th International Congress of the World Equine Veterinary Association WEVA October 3-5, 2013 Budapest, Hungary Reprinted in IVIS with the Permission of the WEVA Organizers
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Sepsis is the most common cause of death in
 ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Scottish Medicines Consortium
 Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Mechanism of antibiotic resistance
 Mechanism of antibiotic resistance Dr.Siriwoot Sookkhee Ph.D (Biopharmaceutics) Department of Microbiology Faculty of Medicine, Chiang Mai University Antibiotic resistance Cross-resistance : resistance
Mechanism of antibiotic resistance Dr.Siriwoot Sookkhee Ph.D (Biopharmaceutics) Department of Microbiology Faculty of Medicine, Chiang Mai University Antibiotic resistance Cross-resistance : resistance
ESCMID Online Lecture Library. by author
 Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Antimicrobial Therapy
 Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Disclosure: Dr. Spach has no significant financial interest in any of the
Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Disclosure: Dr. Spach has no significant financial interest in any of the
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Outline. Antimicrobial resistance. Antimicrobial resistance in gram negative bacilli. % susceptibility 7/11/2010
 Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی
 جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی ویرایش دوم بر اساس ed., 2017 CLSI M100 27 th تابستان ۶۹۳۱ تهیه
جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی ویرایش دوم بر اساس ed., 2017 CLSI M100 27 th تابستان ۶۹۳۱ تهیه
DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY*
 44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
2017 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2016 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Why we perform susceptibility testing
 22 nd June 2015 Why we perform susceptibility testing Robin A Howe Antimicrobial use in Primary Care Why do we perform AST? Clinical Clinical Prediction Prediction of of Efficacy Efficacy Why do we perform
22 nd June 2015 Why we perform susceptibility testing Robin A Howe Antimicrobial use in Primary Care Why do we perform AST? Clinical Clinical Prediction Prediction of of Efficacy Efficacy Why do we perform
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani
 Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Protein Synthesis Inhibitors
 Protein Synthesis Inhibitors Assistant Professor Dr. Naza M. Ali 11 Nov 2018 Lec 7 Aminoglycosides Are structurally related two amino sugars attached by glycosidic linkages. They are bactericidal Inhibitors
Protein Synthesis Inhibitors Assistant Professor Dr. Naza M. Ali 11 Nov 2018 Lec 7 Aminoglycosides Are structurally related two amino sugars attached by glycosidic linkages. They are bactericidal Inhibitors
2009 ANTIBIOGRAM. University of Alberta Hospital and the Stollery Childrens Hospital
 2009 ANTIBIOGRAM University of Alberta Hospital and the Stollery Childrens Hospital Division of Medical Microbiology Department of Laboratory Medicine and Pathology 2 Table of Contents Page Introduction.....
2009 ANTIBIOGRAM University of Alberta Hospital and the Stollery Childrens Hospital Division of Medical Microbiology Department of Laboratory Medicine and Pathology 2 Table of Contents Page Introduction.....
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how?
 Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
2010 ANTIBIOGRAM. University of Alberta Hospital and the Stollery Children s Hospital
 2010 ANTIBIOGRAM University of Alberta Hospital and the Stollery Children s Hospital Medical Microbiology Department of Laboratory Medicine and Pathology Table of Contents Page Introduction..... 2 Antibiogram
2010 ANTIBIOGRAM University of Alberta Hospital and the Stollery Children s Hospital Medical Microbiology Department of Laboratory Medicine and Pathology Table of Contents Page Introduction..... 2 Antibiogram
Maximizing the efficacy of antibiotic therapy
 Community Acquired Pneumonia Maximizing the efficacy of antibiotic therapy João Gonçalves Pereira, MD, PhD ICU Director Hospital Vila Franca Xira Antibiotics and Pneumonia Survival in Bacteremic Pneumococcal
Community Acquired Pneumonia Maximizing the efficacy of antibiotic therapy João Gonçalves Pereira, MD, PhD ICU Director Hospital Vila Franca Xira Antibiotics and Pneumonia Survival in Bacteremic Pneumococcal
CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE)
") CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE) Bartsch SM et al. Potential economic burden of carbapenem-resistent Enterobacteriaceae (CRE) in the United States. Clin Microbiol Infect 2017;23(1):48e9-e16.
CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE) Bartsch SM et al. Potential economic burden of carbapenem-resistent Enterobacteriaceae (CRE) in the United States. Clin Microbiol Infect 2017;23(1):48e9-e16.
Fighting MDR Pathogens in the ICU
 Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
What do we know on PK/PD of β-lactams
 What do we know on PK/PD of β-lactams Françoise Van Bambeke, PharmD, PhD Pharmacologie cellulaire et moléculaire Louvain Drug Research Institute Université catholique de Louvain, Brussels, Belgium
What do we know on PK/PD of β-lactams Françoise Van Bambeke, PharmD, PhD Pharmacologie cellulaire et moléculaire Louvain Drug Research Institute Université catholique de Louvain, Brussels, Belgium
Diagnosis: Presenting signs and Symptoms include:
 PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC
 Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Maximizing the efficacy of antibiotic therapy
 Community Acquired Pneumonia Maximizing the efficacy of antibiotic therapy João Gonçalves Pereira, MD, PhD ICU Director Hospital Vila Franca Xira Antibiotics and Pneumonia Survival in Bacteremic Pneumococcal
Community Acquired Pneumonia Maximizing the efficacy of antibiotic therapy João Gonçalves Pereira, MD, PhD ICU Director Hospital Vila Franca Xira Antibiotics and Pneumonia Survival in Bacteremic Pneumococcal
* gender factor (male=1, female=0.85)
") Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
CHSPSC, LLC Antimicrobial Stewardship Education Series
 CHSPSC, LLC Antimicrobial Stewardship Education Series March 8, 2017 Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 1 Featured Speaker: Larry Danziger, Pharm.D. Professor of Pharmacy
CHSPSC, LLC Antimicrobial Stewardship Education Series March 8, 2017 Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 1 Featured Speaker: Larry Danziger, Pharm.D. Professor of Pharmacy
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Trea%ng Sepsis in 2016 Are the Big Guns Losing the War?
 Trea%ng Sepsis in 2016 Are the Big Guns Losing the War? ERIC HODGSON FCA (Crit Care) Inkosi Albert Luthuli Central Hospital & NELSON R MANDELA SCHOOL OF MEDICINE DURBAN, KZN Declaration Advisory boards
Trea%ng Sepsis in 2016 Are the Big Guns Losing the War? ERIC HODGSON FCA (Crit Care) Inkosi Albert Luthuli Central Hospital & NELSON R MANDELA SCHOOL OF MEDICINE DURBAN, KZN Declaration Advisory boards
CF WELL Pharmacology: Microbiology & Antibiotics
 CF WELL Pharmacology: Microbiology & Antibiotics Bradley E. McCrory, PharmD, BCPS Clinical Pharmacy Specialist Pulmonary Medicine Cincinnati Children s Hospital Medical Center January 26, 2017 Disclosure
CF WELL Pharmacology: Microbiology & Antibiotics Bradley E. McCrory, PharmD, BCPS Clinical Pharmacy Specialist Pulmonary Medicine Cincinnati Children s Hospital Medical Center January 26, 2017 Disclosure
Antibiotics: mode of action and mechanisms of resistance. Slides made by Special consultant Henrik Hasman Statens Serum Institut
 Antibiotics: mode of action and mechanisms of resistance. Slides made by Special consultant Henrik Hasman Statens Serum Institut This presentation Definitions needed to discuss antimicrobial resistance
Antibiotics: mode of action and mechanisms of resistance. Slides made by Special consultant Henrik Hasman Statens Serum Institut This presentation Definitions needed to discuss antimicrobial resistance
Help with moving disc diffusion methods from BSAC to EUCAST. Media BSAC EUCAST
 Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Burton's Microbiology for the Health Sciences. Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents
 Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
Antimicrobial susceptibility
 Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Appropriate Antimicrobial Therapy for Treatment of
 Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Principles of Antimicrobial therapy
 Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
4 th and 5 th generation cephalosporins. Naderi HR Associate professor of Infectious Diseases
 4 th and 5 th generation cephalosporins Naderi HR Associate professor of Infectious Diseases Classification Forth generation: Cefclidine, cefepime (Maxipime),cefluprenam, cefoselis,cefozopran, cefpirome
4 th and 5 th generation cephalosporins Naderi HR Associate professor of Infectious Diseases Classification Forth generation: Cefclidine, cefepime (Maxipime),cefluprenam, cefoselis,cefozopran, cefpirome
Reducing the Burden of Severe Sepsis and Infections in Indian ICUs
 Reducing the Burden of Severe Sepsis and Infections in Indian ICUs J.V. Divatia Professor & Head Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai India Infections in the ICU
Reducing the Burden of Severe Sepsis and Infections in Indian ICUs J.V. Divatia Professor & Head Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai India Infections in the ICU
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases
 The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient
 1 Chapter 79, Self-Assessment Questions 1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient with normal renal function is: A. Trimethoprim-sulfamethoxazole B. Cefuroxime
1 Chapter 79, Self-Assessment Questions 1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient with normal renal function is: A. Trimethoprim-sulfamethoxazole B. Cefuroxime
Contribution of pharmacokinetic and pharmacodynamic parameters of antibiotics in the treatment of resistant bacterial infections
 Contribution of pharmacokinetic and pharmacodynamic parameters of antibiotics in the treatment of resistant bacterial infections Francois JEHL Laboratory of Clinical Microbiology University Hospital Strasbourg
Contribution of pharmacokinetic and pharmacodynamic parameters of antibiotics in the treatment of resistant bacterial infections Francois JEHL Laboratory of Clinical Microbiology University Hospital Strasbourg
ESISTONO LE HCAP? Francesco Blasi. Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano
 ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
Rational use of antibiotics
 Rational use of antibiotics Uga Dumpis MD, PhD,, DTM Stradins University Hospital Riga, Latvia ugadumpis@stradini.lv BALTICCARE CONFERENCE, PSKOV, 16-18.03, 18.03, 2006 Why to use antibiotics? Prophylaxis
Rational use of antibiotics Uga Dumpis MD, PhD,, DTM Stradins University Hospital Riga, Latvia ugadumpis@stradini.lv BALTICCARE CONFERENCE, PSKOV, 16-18.03, 18.03, 2006 Why to use antibiotics? Prophylaxis
Medicinal Chemistry 561P. 2 st hour Examination. May 6, 2013 NAME: KEY. Good Luck!
 Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Infectious Disease: Drug Resistance Pattern in New Mexico
 Infectious Disease: Drug Resistance Pattern in New Mexico Are these the world's sexiest accents? Obi C. Okoli, MD.,MPH. Clinic for Infectious Diseases Las Cruces, NM. Are these the world's sexiest accents?
Infectious Disease: Drug Resistance Pattern in New Mexico Are these the world's sexiest accents? Obi C. Okoli, MD.,MPH. Clinic for Infectious Diseases Las Cruces, NM. Are these the world's sexiest accents?
La sepsi Il ruolo dell antibiotico terapia
 Congresso Nazionale AcEMC Fermo 11-12 Maggio 2017 La sepsi Il ruolo dell antibiotico terapia Michele Bartoletti Infectious Disease Unit - Sant Orsola Hospital, Bologna, Italy Disclosures: none Epidemiology
Congresso Nazionale AcEMC Fermo 11-12 Maggio 2017 La sepsi Il ruolo dell antibiotico terapia Michele Bartoletti Infectious Disease Unit - Sant Orsola Hospital, Bologna, Italy Disclosures: none Epidemiology
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Combating Antimicrobial Resistance with Extended Infusion Beta-lactams. Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident
 Combating Antimicrobial Resistance with Extended Infusion Beta-lactams Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident Disclosure The presenter has no conflicts of interest to disclose with material
Combating Antimicrobial Resistance with Extended Infusion Beta-lactams Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident Disclosure The presenter has no conflicts of interest to disclose with material
Disclosure. Objectives. Combating Antimicrobial Resistance with Extended Infusion Beta-lactams
 Combating Antimicrobial Resistance with Extended Infusion Beta-lactams Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident Disclosure The presenter has no conflicts of interest to disclose with material
Combating Antimicrobial Resistance with Extended Infusion Beta-lactams Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident Disclosure The presenter has no conflicts of interest to disclose with material
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate
 Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons