PRIMARY CARE ANTIMICROBIAL GUIDE
|
|
|
- Mervyn Cannon
- 5 years ago
- Views:
Transcription
1 PRIMARY CARE ANTIMICROBIAL GUIDE GENERATED AT WED JAN 31 10:32:36 UTC WHAT'S NEW IN THIS VERSION? 1.1 WHAT'S NEW IN THIS VERSION? Welcome to the MicroGuide app for the East Kent CCGs antibiotic prescribing guideline for primary care. The East Kent CCGs include Ashford, Canterbury and Coastal, South Kent Coast and Thanet CCGs. This guideline was approved for use in East Kent from September This application will be updated as and when the East Kent CCGs guideline is updated. The full PHE (Public Health England) document can be viewed here. Updates January Update to version Supporting information - penicillin allergy- Traffic light colour coding inserted and drugs colour coded.
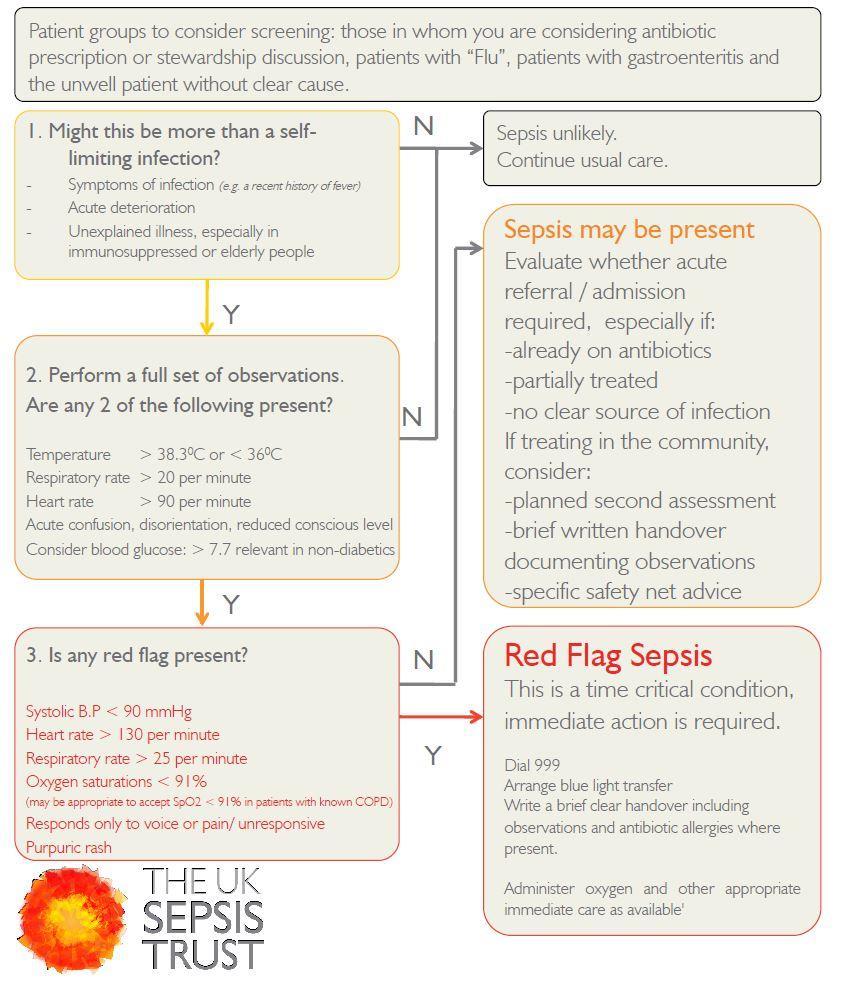
2 November Update to version Bites (animal/human) Clarification and doses for treatment in children. November Update to version As per PHE September 2017 update May update to recurrent UTI section. February Updates to Urinary Tract Infections: UTI General Information, Uncomplicated UTI January First Release of Public version. December Initial launch of the East Kent CCGs MicroGuide app. 2 SEPSIS - RECOGNITION AND MANAGEMENT 2.1 SEPSIS SCREENING AND ACTION TOOL Sepsis Screening and Action Tool Sepsis is a time critical condition. Screening, early intervention and immediate treatment saves lives. This tool should be applied to all adult patients who are not pregnant who have a suspected infection or their clinical observations are outside of normal limits.
3
4 2.2 GENERAL PRACTICE MANAGEMENT OF SEPSIS General Practice and Management of Sepsis This section contains a clinical toolkit that has been developed in partnership with the Royal College of General Practitioners. It is designed to provide operational solutions to the complexities challenging the reliable identification and management of sepsis in the primary care setting, and complements clinical toolkits designed for other clinical areas. The toolkit aims to make GPs and other primary care clinicians familiar with the significant morbidity and mortality associated with severe sepsis and to structure their knowledge and skills so that they can recognise the condition earlier. It advises on specific safety netting in patients presenting with signs and symptoms of infection and addresses the need to work collaboratively with health professionals in other clinical areas to ensure that appropriate further assessment is undertaken and time-critical care is delivered rapidly when necessary. This toolkit is compatible with international guidelines on sepsis management, with the Department of Healthâ s document â Start Smartthen Focusâ, and with guidance on infection management in primary care issued by the Health Protection Agency. Click hereto view the toolkit in detail. 2.3 REFERENCES AND FURTHER INFORMATION Spotting the Sick Child Spotting the Sick Child is an interactive tool commissioned by the Department of Health and Health Education England to support health professionals in the assessment of the acutely sick child. You can register for guidance and training to improve your understanding, as children need a different approach from adults and many health professionals are anxious about assessing children. 3 PRINCIPLES OF TREATMENT
5 Principles of Treatment 1. This guidance is based on the best available evidence but use professional judgement and involve patients in management decisions. 2. It is important to initiate antibiotics as soon as possible in severe infection. 3. Where an empirical therapy has failed or special circumstances exist, microbiological advice can be obtained from Prescribe an antibiotic only when there is likely to be a clear clinical benefit. 5. Consider a â Noâ or â Back-up/Delayedâ, antibiotic strategy for acute self-limiting upper respiratory tract infections and mild UTI symptoms. 6. Limit prescribing over the telephone to exceptional cases. 7. Use simple generic antibiotics if possible. Avoid broad spectrum antibiotics (eg. co-amoxiclav, quinolones and cephalosporins) when narrow spectrum antibiotics remain effective, as they increase risk of CLOSTRIDIUM DIFFICILE, MRSA and resistant UTIs, particularly in patients over the age of 75 years. 8. A dose and duration of treatment for adults is usually suggested within this guidance, but may need modification for age, weight and renal function. In severe or recurrent cases consider a larger dose or longer course. 9. Child doses are provided when appropriate. 10. Please refer to BNF for further dosing and interaction information (e.g. interaction between macrolides and statins) if needed and please check for hypersensitivity. 11. Lower threshold for antibiotics in immunocompromised or those with multiple morbidities; consider culture and seek advice. 12. Avoid widespread use of topical antibiotics (especially those agents also available as systemic preparations, e.g. fusidic acid). 13. In pregnancy take specimens to inform treatment; where possible avoid tetracyclines, aminoglycosides, quinolones, HIGH DOSE metronidazole (2 g) unless benefit outweighs risks. Short-term use of nitrofurantoin (at term, theoretical risk of neonatal haemolysis) is not expected to cause foetal problems. Trimethoprim is also unlikely to cause problems unless poor dietary folate intake or taking another folate antagonist eg antiepileptic. 14. This guidance should not be used in isolation; it should be supported with patient information about back-up/delayed antibiotics, infection severity and usual duration, clinical staff education, and audits. Materials are available on the RCGP TARGET website. 4 BODY SYSTEMS 4.1 UPPER RESPIRATORY TRACT INFECTIONS PRESCRIBING ADVICE Most respiratory tract infections are self-limiting, therefore antibiotics are rarely necessary. Consider a delayed antibiotic prescription strategy.
6 Giving out antibiotics automatically for upper respiratory tract infections increases the number of future consultations for the same symptoms. The NICE pathway for respiratory tract infections states that all patients should be offered: 1. Advice about the natural history of the illness and total illness length 2. Advice regarding management of symptoms, particularly analgesics and antipyretics (a patient information leaflet is available through the RCGP TARGET toolkit) AVERAGE ILLNESS LENGTH 4.2 NATURAL HISTORY AND AVERAGE ILLNESS LENGTH FOR COMMON RESPIRATORY TRACT INFECTIONS AVERAGE TOTAL ILLNESS LENGTHS Acute otitis media - 4 days Acute sore throat/ acute pharyngitis/ acute tonsillitis - 1 week Common cold weeks Acute rhinosinusitis weeks Acute cough/ acute bronchitis - 3 weeks
7 4.2.2 NATURAL HISTORY
8
9 NICE PATHWAY 4.3 NICE PATHWAY FOR SELF-LIMITING RESPIRATORY TRACT INFECTIONS - ANTIBIOTIC PRESCRIBING OVERVIEW The NICE pathway covers prescribing of antibiotics for self-limiting respiratory tract infections in adults and children in primary care and brings together all NICE guidance, quality standards and materials. To view the pathway click here. (Please note the pathway is best viewed on a tablet or desktop/laptop) INFLUENZA Influenza Annual vaccination is essential for all those at risk of influenza. For otherwise healthy adults, antivirals are not recommended. Treat 'at risk' patients: when influenza is circulating in the community, and ideally within 48 hours of onset (do not wait for lab report) or in a care home where influenza is likely.
10 Patients at risk include: pregnant (including up to 2 weeks post-partum), 65 years or over, chronic respiratory disease (including COPD and asthma), significant cardiovascular disease (not hypertension), immunocompromised, diabetes mellitus, chronic neurological, renal or liver disease, morbid obesity (BMI â 40). Use 5 days treatment with Oseltamivir 75mg bd. If resistance to oseltamivir or severe immunosuppression, use zanamivir 10mg BD (2 inhalations by diskhaler for up to 10 days) and seek advice. See PHE Influenza guidance for treatment of patients under 13 years or in severe immunosuppresion (and seek advice). References and further information NICE guidance - influenza prophylaxis Public Health England - influenza treatment ACUTE OTITIS EXTERNA 4.4 ACUTE OTITIS EXTERNA (AOE)
11 First use analgesia Cure rates similar at 7 days for topical acetic acid or antibiotic +/- steroid. If cellulitis/disease extending outside ear canal, start oral antibiotics & refer to exclude malignant OE. First Line Acetic acid ear spray 2% (Ear-calm )* 1 spray TDS for 7 days *For patients who pay for prescriptions Ear-calm spray is available to purchase from pharmacies for less than a prescription charge. Second Line Neomycin sulphate with corticosteroid drops 3 drops TDS for a minimum of 7 days to 14 days maximum OR Otomize ear spray (neomycin sulfate with dexamethasone) 1 spray TDS for a minimum of 7 days to 14 days maximum. If cellulitis or disease extends outse of ear canal Flucloxacillin 250mg QDS for 7 days. For sever: 500mg QDS for 7 days Children's dosages Children 1 month to 1 year of age â 62.5 mg to 125 mg, four times a day for 7 days. Children 2â 9 years of age â 125 mg to 250 mg, four times a day for 7 days.
12 4.4.1 REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Otitis externa ACUTE OTITIS MEDIA 4.5 ACUTE OTITIS MEDIA PRESCRIBING NOTES AND GENERAL ADVICE Optimise analgesia and target antibiotics AOM resolves in 60% in 24hrs without antibiotics, which only reduce pain at 2 days (NNT15) and does not prevent deafness. Consider 2 or 3-day delayed or immediate antibiotics for pain relief if: <2 years AND bilateral AOM (NNT4) or bulging membrane, or symptom score >8 for: fever; tugging ears; crying; irritability; difficulty sleeping; less playful; eating less (0 = no symptoms; 1 = a littles; 2 = a lot). All ages with otorrhoea NNT3. Abx to prevent Mastoiditis NNT >4000. First Line Amoxicillin
13 Neonate (7-28 days): 30mg/kg TDS (maximum per dose 125mg) for 5 days Child 1 month-1 year: 125mg TDS for 5 days Child 1-5 years: 250mg TDS for 5 days Child 5-17 years: 500mg TDS for 5 days Adult: 500mg TDS for 5 days Alternative ONLY if penicillin allergic Erythromycin Child < 2years 125mg QDS for 5 days Child 2-8 years: 250mg QDS for 5 days Child 8-18 years: mg QDS for 5 days Adult: mg QDS for 5 days NB: prescribe enteric coated/ gastro resistant tablets when prescribing tablet formulation OR Clarithromycin Child 1 monthâ 11 years (body-weight up to 8 kg)
14 7.5 mg/kg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 8â 11 kg) 62.5 mg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 12â 19 kg) 125 mg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 20â 29 kg) mg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 30â 40 kg) 250 mg twice daily for 5 days. Child 12â 17 years 250 mg twice daily for 5 days, increased to 500 mg twice daily, if required in severe infections REFERENCES AND FURTHER INFORMATION
15 NICE Clinical Knowledge Summaries: Otitis media (acute) NICE - fever in under 5s assessment and initial management ACUTE RHINOSINUSITIS Acute rhinosinusitis AVOID ANTIBIOTICS AS 80% RESOLVE IN 14 DAYS WITHOUT, AND THEY ONLY OFFER MARGINAL BENEFIT AFTER 7 DAYS (NNT = 15). Use adequate analgesia Consider 7-day delayed or immediate antibiotic when purulent nasal discharge (NNT 8). In persistent infection use an agent with anti-anaerobic activity eg. co-amoxiclav. First Line AMOXICILLIN CAPSULES 500MG TDS FOR 7 DAYS OR DOXYCYCLINE CAPSULES (ADULTS) 200MG STAT, THEN 100MG OD FOR 7 DAYS
16 4.5.8 OR (IF PNEUMOCOCCAL) PHENOXYMETHYLPENICILLIN TABLETS 500MG QDS FOR 7 DAYS If allergic to penicillin and doxycycline not appropriate Clarithromycin tablets 250mg-500mg BD (adult dose) OR Erythromycin e/c tablets can be used; see otitis media doses Second line for persistant symptoms Co-amoxiclav tablets 625mg TDS for 7 days REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Acute sinusitis ACUTE SINUSITIS Acute Sinusitis Prescribing notes and general advice For symptoms <10 days do not offer antibiots as most resolve in 14 days without. Antibiotics only offer marginal benefit after 7 days (NNT 15)
17 For symptoms > 10days no antibiotic or back-up antibiotic. If several of: purulent nasal discharge; severe localised unilateral pain; fever; marked deterioration after initial milder phase. Systemically very unwell, or more serious signs and symptoms: immediate antibiotic. Suspected complications: eg sepsis, intraorbital or intracranial, refer to secondary care Self-care: paracetamol/ibuprofen for pain/fever. Consider high dose nasal steroid if > 12 years. nasal decongestants or saline may help some. First Line for delayed Phenoxymethylpenicillin Adults: 500mg QDS for 5 days Children's dosages: For Child 1â 11 months 62.5â mg 4 times a day; increased if necessary up to 12.5â mg/kg 4 times a day. For Child 1â 5 years 125â mg 4 times a day; increased if necessary up to 12.5â mg/kg 4 times a day. For Child 6â 11 years 250â mg 4 times a day; increased if necessary up to 12.5â mg/kg 4 times a day.
18 For Child 12â 17 years 500â mg 4 times a day; increased if necessary up to 1â g 4 times a day. For very unwell or worsening: Co-amoxiclav Adults: 500/125mg TDS for 5 days Children's dosasges: Doses for 125/31mg suspension For Neonate 0.25â ml/kilogram 3 times a day. For Child 1â 11 months 0.25â ml/kilogram 3 times a day, dose doubled in severe infection. For Child 1â 5 years 0.25â ml/kilogram 3 times a day, alternatively 5â ml 3 times a day, dose doubled in severe infection Doses for 250/62mg suspension
19 For Child 6â 11 years 0.15â ml/kilogram 3 times a day, alternatively 5â ml 3 times a day, dose doubled in severe infection DOSES FOR 400/57MG SUSPENSION For Child 2 monthsâ 1 year 0.15â ml/kilogram twice daily, doubled in severe infection. For Child 2â 6 years (body-weight 13â 21 kg) 2.5â ml twice daily, doubled in severe infection. For Child 7â 12 years (body-weight 22â 40 kg) 5â ml twice daily, doubled in severe infection. For Child 12â 17 years (body-weight 41 kg and above) 10â ml twice daily; increased if necessary to 10â ml 3 times a day, increased frequency to be used in severe infection. For Penicillin allergic Doxycycline capsules for adults and children > 12 years: 200mg stat then 100mg OD for 5 days OR Clarithromycin For adults: 500mg BD for 5 days
20 Children's dosages for 5 days For Neonate 7.5â mg/kg twice daily. For Child 1 monthâ 11 years (body-weight up to 8 kg) 7.5â mg/kg twice daily. For Child 1 monthâ 11 years (body-weight 8â 11 kg) 62.5â mg twice daily. For Child 1 monthâ 11 years (body-weight 12â 19 kg) 125â mg twice daily. For Child 1 monthâ 11 years (body-weight 20â 29 kg) 187.5â mg twice daily. For Child 1 monthâ 11 years (body-weight 30â 40 kg) 250â mg twice daily. For Child 12â 17 years 250â mg twice daily usually for 7â 14 days, increased to 500â mg twice daily, if required in severe infections.
21 References and further information NICE Clinical Knowledge Summaries: Acute sinusitis ACUTE SORE THROAT Acute sore throat Prescribing notes and general advice Avoid Antibiotics as 82% of cases resolve in 7 days, and pain is only reduced by 16 hours. CKS Feverpain Use FeverPAIN Score : Fever in last 24 hours; Purulence; Attend rapidly under threee days; severyly Inflamed tonsils; No cough or coryza. Score 0-1: 13-18% streptococci - no antibiotic 2-3: 34-40% streptococci - 3 day delayed antibiotic 4-5: 62-65% streptococci - if severe, immediate antibiotic, or 48-hour delayed antibiotic Advise paracetamol, self-care, and safety net.
22 First Line Phenoxymethylpenicillin tablets 500mg QDS or 1g BD (if mild). If sever 500mg QDS for 5-10 days Children's dosage Child 1â 11 months 62.5 mg 4 times a day for 10 days; increased if necessary up to 12.5 mg/kg 4 times a day Child 1â 5 years 125 mg 4 times a day for 10 days; increased if necessary up to 12.5 mg/kg 4 times a day Child 6â 11 years 250 mg 4 times a day for 10 days; increased if necessary up to 12.5 mg/kg 4 times a day Child 12â 17 years 500 mg 4 times a day for 10 days; increased if necessary up to 1 g 4 times a day If allergic to penicillin Clarithromycin tablets mg BD for 5 days Children's dosage Child 1 monthâ 11 years (body-weight up to 8 kg) 7.5 mg/kg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 8â 11 kg) 62.5 mg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 12â 19 kg) 125 mg twice daily for 5 days.
23 Child 1 monthâ 11 years (body-weight 20â 29 kg) mg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 30â 40 kg) 250 mg twice daily for 5 days. Child 12â 17 years 250 mg twice daily for 5 days, increased to 500 mg twice daily, if required in severe infections. Penicillin allergy in pregnancy Erythromycin mg QDS for 5 days References and further information NICE Clinical Knowledge Summaries: Acute sore throat SCARLET FEVER Scarlet Fever Prescribing notes and gernal advice Prompt treatment with appropriate antibiotics significantly reduces the risk of complications. Observe immunocompromised individuals (diabetes; women in the puerperal period; chickenpox) as they are at increased risk of developing invasive infections. First Line Mild: analgesia
24 Phenoxymethylpenicillin tablets Adult: 500mg QDS for 10 days 62.5mg QDS for children aged 1 month to 11 months 125mg for children aged 1 year to 5 years 11 months 250mg for children aged 6 years to 11 years 11 months mg for children aged 12 years to 17 years 11 months Penicillin allergy Clarithromycin tablets mg BD for 5 days Child 1 monthâ 11 years (body-weight up to 8 kg) 7.5 mg/kg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 8â 11 kg) 62.5 mg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 12â 19 kg) 125 mg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 20â 29 kg) mg twice daily for 5 days. Child 1 monthâ 11 years (body-weight 30â 40 kg) 250 mg twice daily for 5 days.
25 Child 12â 17 years 250 mg twice daily for 5 days, increased to 500 mg twice daily, if required in severe infections. References and further information NICE Clinical Knowledge Summaries: Scarlet fever 4.6 LOWER RESPIRATORY TRACT INFECTIONS ACUTE COUGH/ BRONCHITIS 4.7 ACUTE COUGH/ BRONCHITIS Antibiotic little benefit if no co-morbidity. Antibiotics have little benefit in otherwise healthy adults so avoid. Consider 7 days delayed antibiotic with symptomatic advice. Symptom resolution can take up to 3 weeks CONSIDER IMMEDIATE ANTIBIOTICS IF: > 80 years of age and with one of the following:
26 hospitalisation in the past year, oral steroids, diabetic, congestive heart failure, OR > 65 years of age with two of the above. Consider using CRP test if antibiotic being considered. If CRP < 20mg/L no antibiotics, mg/L delayed, CRP > 100mg immediate antibiotics GENERAL ADVICE Use paracetamol or ibuprofen as required, drink plenty of fluids. Symptom resolution can take up to 3 weeks. First Line: Amoxicillin capsules 500mg TDS for 5 days OR Doxycycline capsules 200mg stat on day 1 then 100mg OD for a further 4 days (total treatment duration 5 days) Note: Low doses of penicillins are more likely to select out resistance hence we recommend 500mg of amoxicillin. Do NOT use quinolones (ciprofloxacin, ofloxacin) first line due to poor pneumococcal activity. Reserve all quinolones (including levofloxacin) for proven resistant organisms.
27 4.7.3 REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Chest infections (adult) NICE Clinical Guideline - respiratory tract infections (self limiting): prescribing antibiotics ACUTE EXACERBATION OF COPD 4.8 ACUTE EXACERBATION OF COPD Treat exacerbations promptly with antibiotics if purulent sputum and increased dyspnoea and/or increased sputum volume. Risk factors for antibiotic resistant organisms include co-morbid disease, severe COPD, frequent exacerbations and antibiotics in the last 3 months. First Line Amoxicillin capsules 500mg TDS for 5 days OR Doxycycline capsules 200mg stat on day 1, then 100mg OD for a further 4 days (total duration of treatment 5 days) OR
28 Clarithromycin tablets 500mg BD for 5 days Note: Low doses of penicillins are more likely to select out resistance hence we recommend 500mg of amoxicillin. Do NOT use quinolones (ciprofloxacin, ofloxacin) first line due to poor pneumococcal activity. Reserve all quinolones (including levofloxacin) for proven resistant organisms. Second Line (if resistance) Co-amoxiclav tablets 625mg TDS for 5 days! Increased risk of C.diff infection with co-amoxiclav REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Chest infections NICE Clinical Guideline - chronic obstructive pulmonary disease in over 16s: diagnosis and management EKPG Inhaled Therapy for COPD PNEUMONIA (COMMUNITY ACQUIRED) Community acquired pneumonia (treatment in the community) Manage using clinical judgement and CRB-65 score (see below) to guide mortality risk, place of care and antibiotics.
29 CRB-65 score for mortality risk assessment in primary care Each CRB-65 parameter scores 1: Confusion (AMT <8) Raised respiratory rate (â 30 breaths per minute) Low blood pressure (systolic â 90mmHg or diastolic â 60mmHg) Age â 65 years Patients are stratified for risk of death as follows: 0: low risk (<1% mortality risk) - consider home based care 1 or 2: intermediate risk (1-10% mortality risk) - consider hospital assessment 3 or 4: high risk (more than 10% mortality risk) - urgent hospital admission Always give safety net advice and likely duration of symptoms Mycoplasma infection is rare in over 65s If CRB-65 = 0 Amoxicillin capsules 500mg TDS OR Clarithromycin tablets 500mg BD OR Doxycycline capsules 200mg STAT on day 1 then 100mg OD
30 Duration for CRB-65=0: Use 5 days. Review at 3 days and extend to 7-10 days if poor response If CRB-65 = 1 or 2 and AT HOME Clinically assess need for dual therapy for atypicals: Amoxicillin capsules 500mg TDS AND Clarithromycin tablets 500mg BD for 7-10 days OR Doxycycline capsules 200mg STAT on day 1 then 100mg OD for 7-10 days (Doxycycline provides cover against atypicals) REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Chest infections BTS Guidelines for the Management of Community Acquired Pneumonia Pneumonia in adults: diagnosis and management NICE Clinical Guideline [CG191] December SUSPECTED MENINGITIS 4.10 SUSPECTED MENINGOCOCCAL DISEASE TRANSFER ALL PATIENTS TO HOSPITAL IMMEDIATELY. IF time before hospital admission, and non-blanching rash give IV benzylpenicillin or cefotaxime unless definite history of hypersensitivity.
31 First Line: BENZYLPENICILLIN IV INJECTION (GIVE IM IF VEIN CANNOT BE FOUND) Adults and children â 10 years of age: 1200mg Children 1 â 9 years of age: 600mg Children <1 year of age: 300mg Second Line: (penicillin allergy) CEFOTAXIME IV INJECTION (GIVE IM IF VEIN CANNOT BE FOUND) Adults and children â 12 years of age: 1 gram Children <12 years of age: 50mg/kg Prescribing notes and general advice Prevention of secondary cases: Only prescribe following advice from the Public Health Doctor 9am - 5pm Out of hours: Contact on-call Doctor via switchboard
32 References and further information NICE Clinical Knowledge Summaries: Meningitis Meningitis Research Foundation: General Practice Resources and Information 4.11 URINARY TRACT INFECTIONS UTI GENERAL INFORMATION 5 UTI GENERAL INFORMATION Do not treat asymptomatic bacteriuria in the elderly (>65years); it is common and is not associated with increased morbidity. Amoxicillin resistance is common, therefore ONLY use if culture confirms susceptibility. References and further information REFER TO PHE UTI GUIDANCE FOR DIAGNOSIS INFORMATION As antimicrobial resistance and E. COLI bacteraemia in the community is increasing, use nitrofurantoin first line, ALWAYS give safety net and self-care advice, and consider risks for resistance. Give TARGET UTI leaflet
33 Target UTI Leaflet Public Health England UTI - quick reference guide UNCOMPLICATED UTI 5.2 UNCOMPLICATED UTI IN ADULTS (i.e.no fever, rigors or flank pain in adults) Women with severe/or â 3 symptoms: treat All patients first line antibiotic: Nitrofurantoin if GFR >45ml/min; if GFR 30-45ml/min only use if resistance and no alternative. Women, mild/or â 2 symptoms: Pain relief and consider back-up/delayed antibiotic. If urine NOT cloudy, 97% negative predictive value of UTI. If urine cloudy, use dipstick to guide treatment. Nitrite, leucocytes, blood all negative 76% NPV; nitrite plus blood or leucocytes has 92% positive predictive value Men: Consider prostatitis and send pre-treatment MSU OR if symptoms mild/non-specific, use negative dipstick to exclude UTI. >65 years: treat if fever â 38Â C or 1.5Â C above base twice in 12 hours AND dysuria OR â 2 other symptoms. If treatment failure always perform culture As antimicrobial resistance and E.COLI bacteraemia in the community is increasing (including multiresistant extended-spectrum beta-lactamase E.COLI) use nitrofurantoin first line ALWAYS give safety net and self care advice, and consider risks for resistance. Give TARGET UTI leaflet
34 First Line: Nitrofurantoin MR 100mg BD For women of all ages: 3 days. For men: 7 days. If low risk of resistance (younger women with acute UTI and no resistance risks): Trimethoprim tablets 200mg BD. For women of all ages: 3 days. For men 7 days. If first line options unsuitable: IF GFR<45ML/MIN: Pivmecillinam 400mg stat then 200mg TDS. For women of all ages: 3 days. For men: 7 days. IF HIGH RISK OF RESISTANCE: Fosfomycin (Monuril) 3g stat in women; men: second 3g dose 3 days later (unlicensed) Risk factors for increased resistance include: care home resident recurrent UTI (2 in 6 months; â 3 in 12 months) hospitalisation >7 days in the last 6 months unresolving urinary symptoms recent travel to a country with increased antimicrobial resistance previous UTI resistant to trimethoprim, cephalosporins or quinolones If risk of resistance: send urine for culture and susceptibilities, and always safety net. IF ORGANISM SUSCEPTIBLE: Amoxicillin capsules 500mg TDS. For women of all ages: 3 days. For men: 7 days. In treatment failure: always perform culture REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Urinary tract infection (lower) - women
35 NICE Clinical Knowledge Summaries: Urinary tract infection (lower) - men SIGN guidance: Management of suspected bacterial UTI in adults MHRA Drug Safety Update (Nitrofurantoin) September ACUTE PYELONEPHRITIS 5.3 ACUTE PYELONEPHRITIS (I.E. FEVER/RIGORS AND LOIN PAIN) 5.4 IF ADMISSION NOT NEEDED, SEND MSU FOR CULTURE AND SUSCEPTIBILITY AND START ANTIBIOTICS. 5.5 IF NO RESPONSE WITHIN 24 HOURS, SEEK ADVICE. If ESBL risk and with microbiology advice consider IV antibiotic via outpatients (OPAT). First line Ciprofloxacin tablets 500mg BD for 7 days OR Co-amoxiclav tablets 500/125mg TDS for 7 days
36 If lab report shows sensitive: Trimethoprim tablets 200mg BD for 14 days 6 REFERENCES AND FURTHER INFORMATION NICE - Acute pyelonephritis UTI IN PREGNANCY 6.2 UTI IN PREGNANCY Send MSU for culture. Start antibiotics in all with significant bacteriuria, even if asymptomatic. Short term use of nitrofurantoin in pregnancy is unlikely to cause problems to the foetus. However, the BNF recommends that nitrofurantoin should be avoided at term - may produce neonatal haemolysis. Avoid trimethoprim if low folate status or on folate antagonist (e.g. antiepileptics or proguanil). First Line Nitrofurantoin tablets 100mg m/r BD for 7 days. OR If susceptible Amoxicillin capsules 500mg TDS for 7 days.
37 Second Line Trimethoprim tablets 200mg BD (off-label) for 7 days. Give folate if 1st trimester. Third Line Cefalexin capsules 500mg BD for 7 days REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Urinary tract infection (lower) - women UTI IN CHILDREN 6.3 UTI IN CHILDREN Child <3 months: refer urgently for assessment. Child â 3 months: use positive nitrite test to guide. Start antibiotics: also send pre-treatment MSU. Imaging: only refer if child <6 months, or recurrent or atypical UTI GENERAL ADVICE
38 6.3.2 MOST CHILDREN ARE WELL HOURS AFTER STARTING TREATMENT. IF THE INFANT OR CHILD IS STILL UNWELL AFTER HOURS THEY SHOULD RETURN FOR REASSESSMENT. Encourage adequate fluid intake (for example check that the child is passing adequate amounts of urine or is having wet nappies). Treatment choices Lower UTI: Trimethoprim or Nitrofurantoin for 3 days NB: Nitrofurantoin liquid 25mg/5ml costs  for 300ml. Trimethoprim Suspension 50mg/5ml Sugar Free costs  6.00 for 300 ml. (Drug Tariff December 2016). IF susceptible: Amoxicillin for 3 days Second Line: Cefalexin for 3 days Upper UTI: refer to paediatrics to: obtain a urine sample for culture; assess for signs of systemic infection; consider systemic antimicrobials. Trimethoprim dosing for children: Neonate Initially 3 mg/kg for 1 dose, then 1â 2 mg/kg twice daily. Child 4â 5 weeks 4 mg/kg twice daily (max. per dose 200 mg). Child 6 weeksâ 5 months 4 mg/kg twice daily (max. per dose 200 mg), alternatively 25 mg twice daily.
39 Child 6 monthsâ 5 years 4 mg/kg twice daily (max. per dose 200 mg), alternatively 50 mg twice daily. Child 6â 11 years 4 mg/kg twice daily (max. per dose 200 mg), alternatively 100 mg twice daily. Child 12â 17 years 200 mg twice daily. Nitrofurantoin dosing for children: Using immediate release preparations: Child 3 months to 11 years 750 micrograms/kg four times a day Child years 50mg four times a day Using modified release preparations: Child years 100mg twice daily dose to be taken with food. Amoxicillin dosing for children: Child 1 to 11 months
40 125mg 3 times a day; increased if necessary up to 30mg/kg 3 times a day. For Child 1 to 4 years 250mg 3 times a day; increased if necessary up to 30mg/kg 3 times a day. For Child 5 to 11 years 500mg 3 times a day; increased if necessary up to 30mg/kg 3 times a day (max. per dose 1g). For Child 12 to 17 years 500mg 3 times a day; increased if necessary up to 1g 3 times a day, use increased dose in severe infections. Cefalexin dosing for children: Neonate up to 7 days 25 mg/kg twice daily (max. per dose 125 mg). Neonate 7 days to 20 days 25 mg/kg 3 times a day (max. per dose 125 mg). Neonate 21 days to 28 days 25 mg/kg 4 times a day (max. per dose 125 mg).
41 Child 1â 11 months 12.5 mg/kg twice daily, alternatively 125 mg twice daily. Child 1â 4 years 12.5 mg/kg twice daily, alternatively 125 mg 3 times a day. Child 5â 11 years 12.5 mg/kg twice daily, alternatively 250 mg 3 times a day. Child 12â 17 years 500 mg 2â 3 times a day. 6.4 REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Urinary tract infection - children NICE CG54: Urinary tract infections in children RECURRENT UTI IN NON-PREGNANT WOMEN: 2 IN 6 MONTHS OR 3 UTIS PER YEAR 6.5 RECURRENT UTI IN NON-PREGNANT WOMEN: 2 IN 6 MONTHS OR Â 3 UTIS PER YEAR First Line: Advise simple measures, including hydration and analgesia. Cranberry products work for some women, but good evidence is lacking.
42 Second Line: Standby or post coital antibiotics. Third Line: Antibiotic prophylaxis. Consider methenamine if no renal or hepatic impairment. Antibiotic options: First line: Nitrofurantoin 100mg m/r POST COITAL stat (off label) OR PROPHYLAXIS OD at night. Duration of treatment: 3-6 months; then review recurrence rate and need Second line: Ciprofloxacin 500mg POST COITAL stat (off label) OR PROPHYLAXIS OD at night. Duration of treatment: 3-6 months; then review recurrence rate and need (Quinolones should only be used for long term prophylaxis in exceptional circumstances). If recent culture sensitive: Trimethoprim tablets 100mg POST COITAL stat (off label) OR PROPHYLAXIS OD at night. Duration of treatment: 3-6 months; then review recurrence rate and need Methenamine hippurate 1g BD for 6 months Notes This guidance relates to patients being treated in primary care. More complex patients under the care of urologists may require alternative prophylactic antibiotics tailored to their individual needs and sensitivity patterns. This may involve the use of rotational antibiotics. Rotational antibiotics should not be initiated in primary care except on consultant microbiologist or urology advice.
43 References and further information NICE Guidelines: UTI in women ACUTE PROSTATITIS 6.6 ACUTE PROSTATITIS Send MSU for culture and start antibiotics. 4 week course may prevent chronic prostatitis. Quinolones achieve higher prostate levels. First Line Ciprofloxacin tablets 500mg BD for 28 days, OR Ofloxacin tablets 200mg BD for 28 days Second Line Trimethoprim tablets 200mg BD for 28 days References and further information
44 NICE Clinical Knowledge Summaries - Acute prostatitis PATIENTS WITH CATHETERS IN SITU 6.7 PATIENTS WITH CATHETERS IN SITU WHEN TO TREAT For every day a catheter is left in, 5-10% of patients will become colonised with bacteria. Unless catheterisation is short term all patients can be assumed to have bacteria in their urine. In the presence of a catheter, antibiotics will not eradicate bacteriuria; only treat if systemically unwell (pyrexial) or pyelonephritis likely. Do not use prophylactic antibiotics for catheter changes unless history of catheter change associated UTI or trauma. Take sample if new onset of delirium, or two or more symptoms of UTI PRESCRIBING NOTES AND GENERAL ADVICE Do not use dipstick testing to diagnose UTI in patients with catheters. A catheter specimen of urine sample is necessary in suspected catheter related UTI but CSU samples should not be sent in the absence of clinical evidence of a UTI TREATMENT CHOICES Therapy is not indicated for asymptomatic patients.
45 6.7.4 REFERENCES AND FURTHER INFORMATION SIGN guidance: Management of suspected bacterial UTI in adults 6.8 GASTROINTESTINAL TRACT INFECTIONS INFECTIOUS DIARRHOEA - GASTROENTERITIS 6.9 INFECTIOUS DIARRHOEA Refer previously healthy children with acute painful or bloody diarrhoea to exclude E. COLI 0157 infection. Antibiotic therapy usually not indicated for bacterial infection unless patient systemically unwell. If systemically unwell and campylobacter suspected (e.g. undercooked meat and abdominal pain), consider Clarithromycin tablets mg BD for 5-7 days if treated early (within 3 days) Fluid replacement essential
46 6.9.2 REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: gastroenteritis TRAVELLERS' DIARRHOEA 6.10 TRAVELLER'S DIARRHOEA Only consider standby antibiotics for remote areas or people at high-risk of severe illness with travellers' diarrhoea. If standby treatment appropriate give Ciprofloxacin tablets 500mg twice a day for 3 days as a private prescription. If quinolone resistance high (e.g. south Asia): consider bismuth subsalicylate (Pepto Bismol) 2 tablets QDS as prophylaxis or for 2 days treatment (advise patient to purchase from a pharmacy) REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: travellers' diarrhoea NaTHNaC: Health Professionals â travellersâ diarrhoea THREADWORMS
47 6.11 THREADWORMS Treat all household contacts at the same time PLUS advise hygiene measures for 2 weeks (hand hygiene, pants at night, morning shower (including perianal area) PLUS wash sleepwear, bed linen, and dust and vacuum on day one. Child <6 months add perianal wet wiping or washes 3 hourly during day. All patients over 6 months of age (off label if <2 years) Mebendazole 100mg STAT dose (but repeat in 2 weeks if infestation persists). Child <6 months of age Mebendazole is unlicensed, use hygiene measures alone for 6 weeks. References and further information NICE Clinical Knowledge Summaries: Threadworm BNF for Children: 4. Drugs for threadworms C.DIFF INFECTION
48 CLOSTRIDIUM DIFFICILE infection Stop unnecessary antibiotics and/or PPIs. Mild cases (<4 episodes of diarrhoea/day) may resond without metronidazole. 70% respond to metronidazole (MTZ) in 5 days; 92% in 14 days. If severe symptoms or signs (see below) should treat with oral Vancomycin, review progress closely and/or consider hospital referral. Definition of Severe: T >38.5 o C, or WCC >15, or rising creatinine or signs/symptoms of severe colitis. See additional advice on Clostridium difficile infection First episode: Metronidazole tablets (MTZ) 400mg or 500mg TDS for days Second episode/severe/type 027: Oral Vancomycin 125mg QDS for days Recurrent disease: Oral Vancomycin 125mg QDS, consider taper, for days OR ON CONSULTANT MICROBIOLOGIST ADVICE: Fidaxomicin 200mg BD for 10 days
49 REFERENCES AND FURTHER INFORMATION Clostridium difficile - GOV.UK NICE Clinical Knowledge Summaries: Diarrhoea â antibiotic associated HELICOBACTER PYLORI Eradication of HELICOBACTER PYLORI Treat all positives in known DU, GU or low grade MALToma. In non-ulcer dyspepsia NNT is 14. Do not offer eradication for GORD. Do not use clarithromycin, metronidazole or quinolone if used in the past year for any infection. Penicillin allergy: Use PPI + clarithromycin + metronidazole. If previous clarithromycin use PPI + bismuth salt + metronidazole + tetracycline. Relapse and previous metronidazole and clarithromycin: Use PPI + amoxicillin + either tetracycline or levofloxacin. In penicillin allergy use PPI + tetracycline + levofloxacin.
50 Retest for H. pylori post DU/GU or relapse after second line therapy; using breath or stool test OR consider endoscopy for culture and susceptibility. Always use PPI twice daily First Line PPI BD PLUS Amoxicillin capsules 1g BD AND EITHER: Clarithromycin tablets 500mg BD OR Metronidazole tablets 400mg BD Prescribe treatment course for 7 days (14 days for MALToma) Penicillin allergy PPI BD PLUS Clarithromycin tablets 500mg BD AND Metronidazole tablets 400mg BD Prescribe treatment course for 7 days (14 days for MALToma) If previous clarithromycin: PPI BD PLUS Metronidazole tablets 400mg BD PLUS Tetracycline tablets 500mg QDS PLUS EITHER: Tripotassium dicitratobismuthate (De-Noltab ) 240mg BD OR
51 Bismuth Subsalicylate 525mg QDS Prescribe treatment course for 7 days (14 days for MALToma) Relapse and previous metronidazole + clarithromycin PPI BD PLUS Amoxicillin capsules 1g BD AND EITHER Tetracycline tablets 500mg QDS OR Levofloxacin 250mg BD Prescribe for 14 days in relapse or MALToma. References and further information NICE CKS Dyspepsia - proven peptic ulcer NICE CG184: Dyspepsia and gastro-oesophageal reflux disease ORAL CANDIDIASIS 6.12 ORAL CANDIDIASIS Topical azoles more effective than topical nystatin. Oral candidiasis rare in immunocompetent adults; consider undiagnosed risk factors including HIV. Fluconazole if extensive/severe candidiasis; if HIV or immunosuppression use 100mg. Treatment
52 Miconazole oral gel 20mg/mL QDS for 7 days or until 2 days after symptoms If miconazole not tolerated Nystatin suspension (Nystan brand most cost effective) 100,000 units/ml QDS for 7 days or until 2 days after symptoms Fluconazole orally 50mg OD OR 100mg OD if HIV or immunosuppression for 7 days + further 7 days if persistant REFERENCES AND FURTHER INFORMATION NICE CKS Candida Oral 6.13 GENITAL TRACT INFECTIONS STI SCREENING 6.14 STI SCREENING People with risk factors should be screened for chlamydia, gonorrhoea, HIV, syphilis. Refer individual and partners to GUM service. Risk factors: <25 years of age, no condom use, recent (<12 months)/frequent change of partner, symptomatic partner, area of high HIV.
53 CHLAMYDIA TRACHOMATIS/URETHRITIS 6.15 CHLAMYDIA TRACHOMATIS/URETHRITIS Opportunistically screen all aged 15 â 25 years. Treat partners and refer to local GUM service. In pregnancy or breastfeeding: azithromycin is the most effective option. Due to lower cure rate in pregnancy, test for cure 6 weeks after treatment PRESCRIBING NOTES AND GENERAL ADVICE Sexual intercourse (including oral sex) should be avoided until both the person diagnosed with chlamydia and any partners have completed the course of treatment. (If single dose azithromycin is given, sexual abstinence for the following 7 days is advised or until any sexual partners have completed their treatment, whichever is the longer.) First Line: Azithromycin tablets 1g stat (NB tablets are more cost effective than capsules) OR Doxycycline capsules 100mg BD for 7 days
54 Pregnant or breastfeeding Azithromycin tablets 1g (off-label use) stat OR Erythromycin e/c tablets 500mg QDS for 7 days OR Amoxicillin capsules 500mg TDS for 7 days REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Chlamydia British Association for Sexual Health & HIV: Chlamydia guideline SIGN: Management of genital chlamydia trachomatis infection EPIDIDYMITIS 6.16 EPIDIDYMITIS Usually due to Gram-negative enteric bacteria in men over 35 years with low risk of STI.
55 If under 35 years or STI risk, refere to GUM Ofloxacin tablets 200mg BD for 14 days OR Doxycycline capsules 100mg BD for days OR Ciprofloxacin tablets 500mg BD for 10 days If patient is high risk of STI: Refer to GUM clinic VAGINAL CANDIDIASIS 6.17 VAGINAL CANDIDIASIS All topical and oral azoles give 75% cure. In pregnancy avoid oral azoles and use intravaginal treatment for 7 days. Treatment options:
56 Clotrimazole 500mg pessary or 10% vaginal cream stat OR Oral Fluconazole 150mg orally stat. In pregnancy: Clotrimazole 100mg pessary at night for 6 nights OR Miconazole intravaginal cream 2% 5g intravaginally BD for 7 days REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: vaginal candidiasis BACTERIAL VAGINOSIS 6.18 BACTERIAL VAGINOSIS Oral metronidazole (MTZ) is as effective as topical treatment but is cheaper.
57 Less relapse with 7 days of oral MTZ than 2g stat at 4 weeks. Pregnant/breastfeeding: Avoid 2g stat dose. Treating partners does not reduce relapse. First Line: Oral Metronidazole tablets 400mg BD for 7 days OR Metronidazole tablets 2g stat* *2g stat dose of metronidazole should not be used in pregnant/breastfeeding women Alternative options: Metronidazole vaginal gel 0.75% 5g applicator intravaginally at night for 5 nights. OR Clindamycin cream 2% 5g applicator intravaginally at night for 7 nights REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Bacterial vaginosis â summary
58 GENITAL HERPES Genital herpes Prescribing notes and general advice Advise: Saline bathing, analgesia, or topical lidocain for pain, and discuss transmission First episode: treat within five days if new lesions or systemic symptoms, and refer to GUM. Recurrent: self-care if mild or immediate short course antiviral treatment, or suppressive therapy if more than six episodes per year First Line Oral Aciclovir tablets 400mg TDS for 5 days Aciclovir tablets 800mg TDS for 2 days if recurrent OR Valaciclovir tablets 500mg BD for 5 days OR Famciclovir tablets 250mg TDS for 5 days. Famciclovir tablets 1gram BD for 1 days if recurrent References and further information
59 NICE Clinical Knowlege Summaries: Herpes simplex-genital GONORRHOEA 6.19 GONORRHOEA Antibiotic resistance is now very high. Use IM ceftriaxone plus azithromycin and refer to GUM. Treatment Ceftriaxone injection 500mg IM Stat PLUS Azithromycin tablets 1g Stat REFERENCES AND FURTHER INFORMATION NICE CKS Management of Gonorrhoea TRICHOMONIASIS
60 6.20 TRICHOMONIASIS Treat partners simultaneously and refer to GUM service. In pregnancy or breastfeeding, avoid 2g single dose metronidazole (MTZ). Consider clotrimazole for symptomatic relief (but NOT cure) if MTZ declined PRESCRIBING NOTES AND GENERAL ADVICE Trichomoniasis is a sexually transmitted infection. Advise sexual abstinence until treatment is completed and any partners have also been treated and followed up. First Line: Metronidazole tablets 400mg BD for 5-7 days OR 2g Stat. Second Line: Clotrimazole pessary 100mg pessary at night for 6 nights REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Trichomoniasis
61 PELVIC INFLAMMATORY DISEASE 6.21 PELVIC INFLAMMATORY DISEASE Refer woman and contacts to GUM service. Always culture for gonorrhoea and chlamydia. If gonorrhoea likely (partner has it, severe symptoms, sex abroad), resistance to quinolones is high, use ceftriaxone regimen or refer to GUM PRESCRIBING NOTES AND GENERAL ADVICE Provide pain relief with ibuprofen or paracetamol. Advise of the need to use a barrier method of contraception (such as a condom) until both the woman and her partner(s) have completed treatment. First Line: Metronidazole tablets 400mg BD for 14 days PLUS
62 EITHER Ofloxacin tablets 400mg BD for 14 days OR Doxycycline capsules 100mg BD for 14 days. If high risk of gonorrhoea Add Ceftriaxone injection 500mg IM stat REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Pelvic inflammatory disease 6.22 SKIN INFECTIONS ACNE Acne Prescribing notes and general advcie Treatment depends on the type and severity of acne. Patients with severe disease (e.g. nodulocystic acne) should be referred.
63 Treat with oral antibiotics for at least 3 months if clinical improvement continues for a further 3 months. If no improvement try an alternative antibiotic before referral. Mild (open and closed comedones) or moderate (inflammatory lesions): First line: self care (wash with mild soap; do not scrub; avoid make-up) Second line: topical retinoid or benzoyl peroxide Third line: add topical antibiotics, or consider addition of oral antibiotic. Sever (docules and cysts): add oral antibiotic (for 3 months max) and refer. First Line Self care Second Line Topical retinoid apply thinly OD for 6-8 weeks Benzoyl peroxide 5% cream OD-BD for 6-8 weeks Third line Topical Clindamycin cream 1% apply Thinly BD for 12 weeks If treatment failure/sever: Tetracycline tablets 500mg BD for 6-12 weeks OR
64 Doxycycline capsules 100mg OD for 6-12 weeks (Photosensitivity is reported to be a particular problem with doxycycline, so consider avoiding this in people who are exposed to a lot of sunlight.) NOTE: Avoid oral tetracyclines in pregnant or breastfeeding women and in children younger than 12 years of age, as they are deposited in the teeth and bones of the unborn or developing child. References and further information NICE Clinical knowledge summaries: Acne vulgaris BITES (HUMAN AND ANIMAL) 6.23 BITES (HUMAN AND ANIMAL) ANIMAL BITE Thorough irrigation is important. Assess tetanus and rabies risk (NB bats in UK). Seek microbiology advice if not human, dog or cat bite. Give prophylaxis if cat bite/puncture wound; bite to hand, foot, face, joint, tendon, ligament; immunocompromised/diabetic/asplenic/cirrhotic/presence of prosthetic valve or prosthetic joint. HUMAN BITE Thorough irrigation is important. Also assess risk of tetanus, rabies, HIV, hepatitis B/C. Antibiotic prophylaxis is advised.
65 Prophylaxis or treatment (animal or human) Co-amoxiclav tablets mg TDS for 7 days If penicillin allergic Bite from cat/dog/man: Adults and children over 12 years Metronidazole tablets 400mg TDS PLUS Doxycycline capsules 100mg BD for 7 days, review at 24 and 48 hours. Children (aged less than 12 years Metronidazole and Clarithromycin â either include doses or note â see BNF for doseâ Contact a microbiologist for advice in the event of severe infection or failure to respond to antibiotics Human bite: Adults and children: Metronidazole tablets mg TDS PLUS Clarithromycin tablets mg BD for 7 days, review at 24 and 48 hours. Children doses: Metronidazole: For Child 1 month
66 7.5â mg/kg every 12â hours usually treated for 7 days For Child 2 monthsâ 11 years 7.5â mg/kg every 8â hours (max. per dose 400â mg) usually treated for 7 days For Child 12â 17 years 400â mg every 8â hours usually treated for 7 days Clarithromycin: For Neonate 7.5â mg/kg twice daily. For Child 1 monthâ 11 years (body-weight up to 8 kg) 7.5â mg/kg twice daily. For Child 1 monthâ 11 years (body-weight 8â 11 kg) 62.5â mg twice daily. For Child 1 monthâ 11 years (body-weight 12â 19 kg) 125â mg twice daily. For Child 1 monthâ 11 years (body-weight 20â 29 kg) 187.5â mg twice daily. For Child 1 monthâ 11 years (body-weight 30â 40 kg)
67 250â mg twice daily. For Child 12â 17 years 250â mg twice daily usually for 7â 14 days, increased to 500â mg twice daily, if required in severe infections. Co-amoxiclav: Doses for 125/31mg suspension For Neonate 0.25â ml/kilogram 3 times a day. For Child 1â 11 months 0.25â ml/kilogram 3 times a day, dose doubled in severe infection. For Child 1â 5 years 0.25â ml/kilogram 3 times a day, alternatively 5â ml 3 times a day, dose doubled in severe infection Doses for 250/62mg suspension For Child 6â 11 years 0.15â ml/kilogram 3 times a day, alternatively 5â ml 3 times a day, dose doubled in severe infection DOSES FOR 400/57MG SUSPENSION For Child 2 monthsâ 1 year
68 0.15â ml/kilogram twice daily, doubled in severe infection. For Child 2â 6 years (body-weight 13â 21 kg) 2.5â ml twice daily, doubled in severe infection. For Child 7â 12 years (body-weight 22â 40 kg) 5â ml twice daily, doubled in severe infection. For Child 12â 17 years (body-weight 41 kg and above) 10â ml twice daily; increased if necessary to 10â ml 3 times a day, increased frequency to be used in severe infection. References and further information NICE Clinical Knowledge Summaries: Bites â human and animal CELLULITIS AND ERYSIPELAS 6.24 CELLULITIS
69 Class I: patient afebrile and healthy other than cellulitis, use oral flucloxacillin alone. Class II: febrile and ill, or comorbidity, admit for intravenous treatment, or use OPAT (if available). Class III: toxic appearence: admit. If river or sea water exposure, discuss with specialist. Erysipelas: often facial and unilateral. Use flucloxacillin for non-facial erysipelas Treatment options: Flucloxacillin capsules 500mg QDS for 7 days, if slow response continue for a further 7 days. If penicillin allergic: Clarithromycin tablets 500mg BD for 7 days, if slow response continue for a further 7 days. If on statins: Doxycycline capsules 200mg stat then 100mg OD for 7 days, if slow response continue for a further 7 days. If unresolving: Clindamycin capsules mg QDS for 7 days, if slow response continue for a further 7 days. If facial: Co-amoxiclav tablets 500/125mg TDS for 7 days, if slow response continue for a further 7 days. General Guidance: If after 14 days treatment the patient has not responded then advice should be sought from the microbiologist.
70 References and further information NHS Clinical Knowledge Summaries: Cellulitis â acute CHICKENPOX AND SHINGLES Varicella zoster (chickenpox) and Herpes zoster (shingles) Pregnant/immunocompromised/neonate: seek urgent specialist advice. Varicella zoster/chicken pox: IF onset of rash <24hr and >14 years or severe pain or dense/oral rash or secondary household case or taking steroids or smoker consider aciclovir. Herpes zoster/shingles: Treat if >50 years and within 72 hrs of onset of rash, (as post-herpetic neuralgia rare if <50 years); or if active opthalmic or Ramsay Hunt or eczema. First Line: If indicated Aciclovir tablets 800mg five times a day for 7 days. Child 1 month - 2 years: 200mg 4 times daily for 5 days
71 Child 2-5 years: 400mg 4 times daily for 5 days Child 6-11 years: 800mg 4 times daily for 5 days Child years: 800mg 5 times daily for 7 days Second Line for shingles (herpes zoster) if compliance a problem as 10 times the cost Valaciclovir tablets 1g TDS for 7 days OR Famciclovir tablets 500 mg TDS for 7 days OR alternatively 750mg BD for 7 days (NB. FAMCICLOVIR IS SIGNIFICANTLY MORE EXPENSIVE, ONLY USE IF VALACICLOVIR NOT APPROPRIATE) References and further information NICE Clinical Knowledge Summaries: Chickenpox NICE Clinical Knowledge Summaries: Shingles COLD SORES
72 6.25 COLD SORES Cold sores resolve after 7-10 days without treatment. Topical antivirals applied prodromally reduce duration by hours and can be purchased from a pharmacy. References and further information NICE CKS Cold Sores ECZEMA 6.26 ECZEMA If no visible signs of infection, use of antibiotics (alone or with steroids) encourages resistance and does not improve healing. In eczema with visible signs of infection, use treatment as in Impetigo. References and further information NICE Clinical Knowledge Summaries: Eczema â atopic
73 FUNGAL INFECTION OF THE FINGERNAIL OR TOENAIL 6.27 FUNGAL INFECTION OF THE FINGERNAIL OR TOENAIL (DERMATOPHYTE INFECTION - NAIL) Take nail clippings: start therapy only if infection is confirmed by laboratory. Oral terbinafine is more effective than oral azole. Liver reactions rare with oral antifungals. If candida or non-dermatophyte infection confirmed use oral Itraconazole. For children seek specialist advice PRESCRIBING NOTES AND GENERAL ADVICE Discuss the likely benefits and adverse effects of treatment so the person can make a fully informed choice. Treatment does not always cure the infection. Cure rates range between approximately 60â 80%. Treatment that eradicates the infection sometimes does not restore the nail's appearance to normal. The drugs need to be taken for several months, or longer for resistant nails. Unpleasant adverse effects can occur. These include headache, itching, loss of the sense of taste, gastrointestinal symptoms, rash, and fatigue. Although abnormal liver function tests are not uncommon, liver failure and other serious adverse effects are rare.
74 First Line: Terbinafine tablets 250mg OD FINGERS: TREAT FOR 6-12 WEEKS TOES: TREAT FOR 3-6 MONTHS Terbinafine is fungicidal, so treatment time is shorter than with fungistatic imidazoles. Second Line: Itraconazole capsules 200mg BD FINGERS: 7 DAYS TREATMENT IN EACH MONTH (IE REPEAT AFTER 21 DAY INTERVAL) FOR 2 MONTHS TOES: 7 DAYS TREATMENT IN EACH MONTH (IE REPEAT AFTER 21 DAY INTERVAL) FOR 3 MONTHS Third Line for very superficial as limited evidence of effectiveness: Amorolfine nail lacquer 5% 1-2x/weekly FINGERS: 6 MONTHS TOES: 12 MONTHS NB. Amorolfine 5% nail laquer not recommended for NHS prescribing as limited evidence of effectiveness, advise to purchase over the counter if requested. References and further information
75 NICE Clinical Knowledge Summaries: Fungal nail infection FUNGAL SKIN INFECTION 6.28 FUNGAL SKIN INFECTION (DERMATOPHYTE INFECTION - SKIN) Terbinafine is fungicidal: treatment time is shorter than with fungistatic imidazoles. If candida possible, use imidazole. If intractable, send skin scrapings for culture and if infection confirmed, use ORAL terbinafine/itraconazole. Scalp: discuss, oral therapy indicated. First Line: Terbinafine cream 1% topical BD 1-2 weeks and for 1-2 weeks after healing (i.e. 4-6 weeks). Second Line: Imidazole topical cream BD 1-2 weeks and for 1-2 weeks after healing (i.e. 4-6 weeks). For athletes foot only:
76 Undecanoic acid + dichlorophen (Mycota ) spray application BD 1-2 weeks and for 1-2 weeks after healing (i.e. 4-6 weeks). References and further information NICE CKS: Fungal skin infection â body and groin NICE CKS: Fungal skin infection â foot NICE CKS: Fungal skin infection â scalp FOOT AND LEG ULCERS Foot and leg ulcers Ulcers always colonised. Bacteria will always be present. Antibiotics do not improve healing unless active infection. If signs of active infection*, send pre-treatment swab. Review antibiotics after culture results. *Culture swabs and antibiotics are ONLY indicated if there is evidence of clinical infection i.e. cellulitis with >2cm surrounding erythema, increased pain, purulent exudate, odour, enlarging ulcer or pyrexia.
77 Review after culture results. Anaerobes may be significant. Specialist guidance should be sought for diabetics. In these patients coliform/pseudomonas infections may be significant. First Line: Active infection if cellulitis/increased pain/pyrexia/purulent exudate/odour. If active infection: Flucloxacillin capsules 500mg QDS for 7 days, if slow response continue for a further 7 days. If penicillin allergic Active infection if cellulitis/increased pain/pyrexia/purulent exudate/odour. If active infection: Clarithromycin tablets 500mg BD for 7 days, if slow response continue for a further 7 days. References and further information NICE Clinical Knowledge Summaries: Leg ulcer â venous
78 IMPETIGO 6.29 IMPETIGO For extensive, severe or bullous impetigo, use oral antibiotics. Reserve topical antibiotics for very localised lesions to reduce the risk of resistance. Reserve mupirocin for MRSA. Prescribing notes and general advice Hygiene measures are important to aid healing and stop the infection spreading to other sites on the body and to other people. Children and adults should stay away from school or work until the lesions are dry and scabbed over, or, if the lesions are still crusted or weeping, for 48 hours after antibiotic treatment has started. First Line: Flucloxacillin capsules oral 500mg QDS for 7 days Flucloxacillin dosing in children: Child 1 monthâ 1 year 62.5â 125mg 4 times a day for 7 days. Child 2â 9 years 125â 250mg 4 times a day for 7 days.
79 Child 10â 17 years 250â 500mg 4 times a day for 7 days. If penicillin allergic: Clarithromycin tablets oral mg BD for 7 days Clarithromycin dosing for children Child 1 month - 11 years: Body weight under 8kg: 7.5mg/kg twice daily for 7 days Body weight 8kg - 11kg: 62.5mg twice daily for 7 days Body weight 12kg - 19kg: 125mg twice daily for 7 days Body weight 20kg - 29kg: 187.5mg twice daily for 7 days Body weight 30kg - 40kg: 250mg twice daily for 7 days Child years: 250mg twice daily for 7 days, increased if necessary in severe infections to 500mg twice daily for up to 14 days OR Fusidic acid cream apply TDS for 5 days MRSA ONLY: Mupirocin ointment TDS for 5 days
80 References and further information NICE Clinical Knowledge Summaries: Impetigo MASTITIS Mastitis Prescribing notes and general advice S. AUREUS is the most common infection pathogen. Suspect if woman has: a painful breast; fever and/or general malaise; a tender, red breast. Berastfeeding: oral antibiotics are appropriate, where indicated. Women should continue feeding, including from the affected breast. First Line Flucloxacillin capsules 500mg QDS for days Pinicillin allergy: Erythromycin mg QDS for days OR
81 Clarithromycin tablets 500mg BD for days References and further information NICE Clinical Knowledge Summaries: Mastitis and breast abscess PVL 7.2 PANTON-VALENTINE LEUKOCIDIN (PVL) Panton-Valentine Leukocidin (PVL) is a toxin produced by 4.9% of STAPH AUREUS from boils/abscesses. This bacteria can rarely cause severe invasive infections in healthy people; if found suppresion therapy should be given. Send swabs if recurrent boils/abcesses. At risk: close contact in communities, contact sports, and poor hygiene. References and further information PHE Guidance, data and analysis SCABIES
82 7.3 SCABIES Prescribing notes and general advice Encourage the family not to delay treatment. Simultaneously (within 24 hours) treat all members of the household, close contacts and sexual contacts (even in the absence of symptoms). Pregnant or breastfeeding women should also be treated with an insecticide. Advise the individual to avoid close body contact with others until their partners and close contacts have been treated. Consider symptomatic treatment for itching eg cromamiton. Advise the person that itching may take several weeks to resolve.consider an oral sedating antihistamine (e.g. chlorphenamine) at night if the itch is interfering with sleep Machine wash (at 50Â C or above) clothes, towels, and bed linen, on the day of application of the first treatment For children under 2 months old, seek specialist advice from a paediatric dermatologist. (Scabies is rare in children under 2 months old.) First Line: Permethrin cream 5% 2 applications, 1 week apart. Adult: Apply once weekly for 2 doses, apply 5% preparation over whole body including face, neck, scalp and ears then wash off after 8-12 hours. If hands are washed with soap within 8 hours of application, they should be treated again with cream. Child, 2 months - 17 years: Apply once weekly for 2 doses, apply 5% preparation over whole body including face, neck, scalp and ears then wash off after 8-12 hours. If hands are washed with soap within 8 hours of application, they should be treated again with cream.
83 Second line if allergy Malathion liquid 0.5% 2 applications, 1 week apart Adult: Apply once weekly for 2 doses, apply 0.5% preparation over whole body and wash off after 24 hours. If hands are washed with soap within 24 hours, they should be retreated. Child: Apply once weekly for 2 doses, apply 0.5% preparation over whole body and wash off after 24 hours. If hands are washed with soap within 24 hours, they should be retreated REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Scabies 7.4 EYE INFECTIONS CONJUNCTIVITIS 7.5 CONJUNCTIVITIS Treat if severe, as most are viral or are self-limiting.
84 Bacterial conjunctivitis is usually unilateral and also self-limiting. It is characterised by red eye with mucopurulent, not watery, discharge. 65% resolve on placebo by day 5. Fusidic acid has less Gram-negative activity. Prescribing notes and general advice Remove contact lenses, if worn, until all symptoms and signs of infection have completely resolved and any treatment has been completed for 24 hours. Clean away infected secretions from eyelids and lashes with cotton wool soaked in water. Wash hands regularly, particularly after touching infected secretions, and to avoid sharing pillows and towels to avoid spreading infection. If symptoms persist for longer than 2 weeks the patient should reconsult for investigation of the cause. People should urgently seek medical attention if they develop marked eye pain or photophobia, loss of visual acuity, or marked redness of the eye. Advise parents that it is not necessary to exclude a child from school or childcare if they have infective conjunctivitis, unless there is an outbreak of infective conjunctivitis. First Line: If severe Chloramphenicol eye drops 0.5% DROPS* 2 hourly for 2 days, then 4 hourly (whilst awake) AND Chloramphenicol eye ointment 1%* at night, all continued until 48 hours after resolution.
85 *For patients who pay for prescriptions chloramphenicol 0.5% eye drops (in max. pack size 10 ml) and 1% eye ointment (in max. pack size 4 g) can be purchased from pharmacies for treatment of acute bacterial conjunctivitis in adults and children over 2 years; max. duration of treatment 5 days. This is often less than a prescription charge. Second Line: If severe Fusidic acid 1% gel 1% apply BD, continue for 48 hours after resolution. NB. Fusidic acid 1% eye gel is significantly more expensive than chloramphenicol 0.5% eye drops, only use if treatment is absolutely necessary and chloramphenicol is contraindicated. 7.6 REFERENCES AND FURTHER INFORMATION NICE Clinical Knowledge Summaries: Conjunctivitis â infective RCGP fact sheet: Management of infective conjunctivitis in primary care BLEPHARITIS Blepharitis Prescribing notes and general advice First line: lid hygiene for symptom control, including: warm compressses; lid massage and scrubs; gental washing; avoiding cosmetics. Second line: topical antibiotics if hygiene mesasure are ineffective after 2 weeks. Signs of Meibomian gland dysfunction, or acne rosacea: consider oral antibiotics. First Line
86 Self care Second Line Chloramphenicol eye ointment 1% apply BD for 6 week trial Third line Oxytetracycline 500mg BD for 4 weeks initially then 250mg BD for 8 weeks maintenance. OR Doxycycline capsules 100mg OD for 4 weeks initially then 50mg od for 8 weeks maintenance. Reference and further information NICE Clinical Knowledge Summaries: Blepharitis 7.7 DENTAL INFECTIONS (EMERGENCY TREATMENT) 7.8 DENTAL INFECTION - EMERGENCY TREATMENT This guidance is not designed to be a definitive guide to oral conditions. It is for GPs for the management of acute oral conditions pending being seen by a dentist or dental specialist.
87 GPs should not routinely be involved in dental treatment and, if possible, advice should be sought from the patientâ s dentist, who should have an answerphone message with details of how to access treatment out-of-hours, or contact NHS 111. For emergency out-of-hours care in East Kent we are served by Dentaline. Their access number is For emergency appointments in the daytime patients should call 111 or to be directed to a dental practice able to see them Patients can find details of their local dentists and whether they are accepting new patients via NHS choices: Search/Dentist/LocationSearch/3 Mucosal ulceration and inflammation (simple gingivitis) Temporary pain and swelling relief can be attained with saline mouthwash. Use antiseptic mouthwash,if more severe and pain limits oral hygiene to treat or prevent secondary infection. The primary cause for mucosal ulceration or inflammation (aphthous ulcers, oral lichen planus, herpes simplex infection, oral cancer) needs to be evaluated and treated. Simple saline mouthwash: half a teaspoon of salt dissolved in glass of warm water. Always spit out after use. Use until lesions resolve or less pain allows oral hygiene. Chlorhexidine %: rinse mouth for 1 minute twice daily with 5ml diluted with 5-10ml of water (do not use within 30mins of toothpaste). Always spit out after use. Use until lesions resolve or less pain allows oral hygiene. Hydrogen peroxide 6% (spit out after use): rinse mouth for 2 mins three times daily with 15ml diluted in half a glass of warm water. Always spit out after use. Use until lesions resolve or less pain allows oral hygiene. Acute necrotising ulcerative gingivitis
88 Commence metronidazole and refer to dentist for scaling and oral hygiene advice. Use in combination with antiseptic mouthwash if pain limits oral hygiene. Metronidazole tablets 400mg TDS for 3 days Chlorhexidine or hydrogen peroxide mouthwash until oral hygiene possible. See dosing above in mucosal ulceration. Pericoronitis Refer to dentist for irrigation and debridement. If persistant swelling or systemic symptoms use metronidazole. Use antiseptic mouthwash if pain and trismus limit oral hygiene. First Line: Amoxicillin capsules 500mg TDS for 3 days Second Line: Metronidazole tablets 400mg TDS for 3 days Chlorhexidine or hydrogen peroxide mouthwash until oral hygiene possible. See dosing above in mucosal ulceration. Dental abcess Regular analgesia should be first option until a dentist can be seen for urgent drainage, as repeated courses of antibiotics for abcess are not appropriate. Repeated antibiotics alone, without drainage are ineffective in preventing spread of infection. Antibiotics are recommended if there are signs of severe infection, systemic symptoms or high risk of complications. Severe odontogenic infections; defined as cellulitis plus signs of sepsis, difficulty in swallowing, impending airway obstruction, Ludwig's angina. Refer urgently for admission to protect airway, achieve surgical drainage and IV antibiotics.
89 The empirical use of cephalosporins, co-amoxiclav, clarithromycin and clindamycin do not offer any advantage for most dental patients and should only be used if no response to first line drugs when referral is the preferred option. IF PUS drain by incision, tooth extraction or via root canal. Send pus for microbiology. IF SPREADING INFECTION (lymph node involvement or systemic signs i.e. fever and malaise) ADD metronidazole, prescribe both antibacterials for 5 days. TRUE PENICILLIN ALLERGY: use clarithromycin. If severe. refer to hospital. First Line: Amoxicillin capsules 500mg TDS for up to 5 days (review at 3 days), if spreading infection, ADD Metronidazole tablets 400mg TDS for 5 days OR Phenoxymethylpenicillin tablets 500mg-1g QDS for up to 5 days (review at 3 days), if spreading infection, ADD Metronidazole tablets 400mg TDS for 5 days (review at 3 days). True penicillin allergy: Clarithromycin tablets 500mg BD for up to 5 days (review at 3 days), if spreading infection ADD Metronidazole tablets 400mg TDS for 5 days (review at 3 days). References and further information NICE Clinical Knowledge Summaries: Dental abscess Management of Acute Dental Problems, Quick Reference Guide for healthcare professionals, March 2013
90 8 SUPPORTING INFORMATION STEPS FOR GOOD ANTIMICROBIAL PRESCRIBING STEPS FOR GOOD ANTIMICROBIAL PRESCRIBING PRACTICE Prescribe an antibiotic only when there is likely to be a clear clinical benefit 2. Do not prescribe an antibiotic for viral sore throat, simple coughs and colds 3. Consider a no, or delayed, antibiotic strategy for acute self-limiting upper respiratory tract infections 4. Limit prescribing over the telephone for exceptional cases 5. Use simple generic antibiotics first whenever possible (see information in this guide) 6. Avoid broad spectrum antibiotics where a narrow spectrum agent will be effective 7. Avoid widespread use of topical antibiotics (especially those agents also available as systemic preparations) 8. In pregnancy AVOID tetracyclines, aminoglycosides, quinolones and high dose metronidazole. Short term use of trimethoprim (theoretical risk in first trimester in patients with poor diet, as folate antagonist) or nitrofurantoin (at term, theoretical risk of neonatal haemolysis) is unlikely to cause problems to the foetus 9. Document clinical indication, duration, dose and route in patient records 10. Where a â best guessâ therapy has failed or special circumstances exist, microbiological advice can be obtained from your local microbiologist 8.4 CLOSTRIDIUM DIFFICILE
91 8.5 Clostridium difficile INFECTION CLOSTRIDIUM DIFFICILE (CDI) can be present in the gut without causing illness. It is estimated to be present in the lower bowel of around 5% of the population. The natural intestinal flora normally prevent overgrowth of C.DIFF, however when antimicrobial therapy is given to patients it can upset this and allow C.DIFF to multiply. The toxins produced by C.DIFF damage the lining of the GI tract and cause symptoms ranging from mild diarrhoea to severe pseudomembranous colitis and toxic megacolon. Patients should be reviewed regularly and admission arranged if there are signs of severe disease (>5-7 stools/day, temperature >38.5 o C, hypotension, tachycardia, ileus, abdominal tenderness) In mild cases, simply stopping aggravating antibiotics is all that is required and if symptoms have settled by the time the result is known then treatment is not required. First line treatment is oral Metronidazole tablets 400mg TDS for days C. DIFFICILE can be detectable in faeces for several weeks and repeat samples are unnecessary. Treat according to symptoms and do not send repeat samples unless requested by a Consultant Microbiologist. Antibiotic use should be avoided for a minimum of 6 weeks after an episode of CDI or in C. DIFFICILE carriers. If there is evidence of another infection that requires treatment during this period, then microbiological advice should be sought. Up to 20% of cases relapse after resolution of symptoms. Relapse is defined by reoccurrence of symptoms, there is no need for further samples. Recurrences should be treated promptly with metronidazole or, if the initial illness was severe, oral vancomycin. After first relapse, the risk of another is increased. Discuss all relapses with a Consultant Microbiologist for further advice: o Ensure that all documentation and onward referrals to other services includes details of CLOSTRIDIUM DIFFICILE history o If the patient lives in a shared care setting ensure that IPC advice is given o Ensure that the patient is given an advice leaflet o Probiotics have a limited use for the prevention and treatment of CLOSTRIDIUM DIFFICILE and cannot be recommended.
92 Understanding C. DIFFICILE results Diarrhoeal stools are tested for both C. DIFFICILE antigen (which indicates the presence of the organism in the gut) and C. DIFFICILE toxin (which is produced by the organism and causes damage to the gut). C. DIFFICILE GDH antigen C. DIFFICILE toxin Interpretation No evidence of C. DIFFICILE infection NOT detected DETECTED DETECTED NOT detected NOT detected DETECTED Consider other causes including viruses. Stop any C. DIFFICILE treatment that has been commenced If symptoms persist send repeat sample in 5 days This could be C. DIFFICILE colonisation or early disease Stop antibiotics if possible Correlate with the clinical picture and treat if appropriate Diarrhoea is very likely to be caused by C. DIFFICILE Stop antibiotics if possible Treatment for C. DIFFICILE should be commenced A root cause analysis will be initiated Seek Consultant Microbiologist advice on if unsure â out of hours contact via hospital switchboard.
93 Prudent antimicrobial prescribing Only prescribe antimicrobials when indicated by the clinical condition of the patient or the results of microbiological investigation. Do not prescribe antimicrobials for sore throat, coughs and colds in patients at low risk of complications. Consider a no, or delayed, antibiotic strategy where possible. If an antimicrobial is required, follow the treatment recommendations in this guide, choosing a narrow spectrum agent where possible. Broad spectrum antibiotics should be reserved for the treatment of serious infections when the pathogen is not known. Which patients are most at risk of CDI? Patients are more at risk of CDI if they are: High risk patient Frail older patients >65 years Long term conditions requiring frequent antibiotics Recent antibiotic exposure within previous 2 months Those who take Proton Pump Inhibitors (PPIs eg omeprazole, lansoprazole etc) High risk environment Contact with C.DIFF patients
94 Recent hospital admission Lives in a shared social and/or care setting High risk antibiotics (the 4Cs)? Clindamycin Ciprofloxacin and other quinolones Cephalosporins (expecially 2nd & 3rd generation) Co-amoxiclav Aminopenicillins (e.g. amoxycillin) have also been implicated in increased C. DIFFICILE infection (may be related to volume of prescribing). Compared to narrow spectrum antibiotics, broad spectrum antibiotics are more likely to significantly change gut flora. Association of acid suppressive therapies, particularly PPIs,with CDI. PPIs have been associated with an increased incidence of CDI Risk of CDI is further increased if antibiotic are used with PPIs Review on-going need for acid suppressants and consider stepdown of treatment When can broad spectrum antibiotics be recommended? There are very few indications for broad spectrum cephalosporins or quinolones in primary care. When using broad spectrum antibiotics counsel patients at risk, to be alert for signs of CDI and to stop their antibiotic and seek medical help if diarrhoea develops. If prescribing antimicrobials to patients with a history of CDI seek microbiology advice.

95 8.6 PENICILLIN ALLERGY 8.7 TREATING PENICILLIN ALLERGIC PATIENTS Penicillins are among the most useful and frequently prescribed antibiotics, however as with all medicines they can cause adverse reactions. These include allergic reactions ranging from mild rash to life threatening anaphylaxis.
96 All cases of penicillin allergy, including nature of reaction, should be recorded in the patientâ s notes. Allergy is one of the most common and important adverse effects of penicillin and related drugs such as amoxicillin (including co-amoxiclav), flucloxacillin and piperacillin and can occur in 1-10% of exposed individuals. Anaphylaxis is rare, with an estimated frequency of 1-5 per 10,000 courses administered, but can be fatal. Furthermore the chemical structure of cephalosporins (cefalexin, cefuroxime etc) is similar to that of penicillins and cross-sensitivity can occur in up to 10% of patients. Penicillins are often the cornerstone of treatment for serious infections and sepsis in the hospital setting. If a patient has a documented penicillin allergy, alternative antibiotics will need to be prescribed. This could require use of quinolones or cephalosporins, with higher risk of C. DIFFICILE infection, or gentamicin or vancomycin, which are nephrotoxic and ototoxic. Optimal management of the patient may be compromised if a patient has been wrongly attributed with a penicillin allergy. All available drug sensitivity issues should be recorded. It is important to clarify and record the nature of the reaction. Check with the patient and the medical notes prior to all prescribing. Please do not label a patient as being allergic to an antibiotic on the basis of side effects of a drug (e.g. nausea, diarrhoea etc.) Type 1 reaction â Immediate anaphylaxis (IgE mediated) Any patient describing anaphylaxis following penicillin exposure must not be prescribed any penicillin again, nor any cephalosporin. Patients with a history of immediate hypersensitivity following administration of penicillin, recognisable by features of urticaria, laryngeal oedema, bronchospasm, hypotension or local swelling within 72 hours of administration, should not receive a penicillin. Patients who are truely allergic to one penicillin will be allergic to all because the hypersensitivity is related to the basic penicillin structure. Patients with a history of immediate hypersensitivity to penicillin may also react to the cephalosporins and other beta-lactam antibiotics. They should not receive these antibiotics. Type 2 reactions â Delayed reaction (non-ige mediated)
97 More commonly penicillin hypersensitivity manifests as a rash, the typical presentation being a maculopapular, erythematous rash symmetrically disposed over the legs, buttocks and trunk. Patients with a definite history of non-urticarial rash allergy to penicillin should not receive a penicillin but the likelihood of serious crosssensitivity with cephalosporins or carbapenems is very low so other non-penicillin beta lactam antibiotics can be used in these patients. Very rarely penicillins can cause pemphigus vulgaris or pemphigoid-like reactions. Penicillins and cephalosporins should not be prescribed to these patients. Patients often describe side effects such as diarrhoea or nausea as â allergiesâ, so careful history taking is extremely important to distinguish between true allergy and manageable side effects. Similarly patients reporting minor rashes restricted to small areas of the body, or who develop rashes more than 72 hours after exposure, probably do not have genuine hypersensitivity. For serious infections for which penicillins are the preferred treatment, vague histories of such reactions do not contra-indicate penicillin use. Discuss with microbiology if necessary. It is also worth noting that maculo-papular rashes can also occur in patients treated with either ampicillin or amoxicillin who have concomitant viral infections such as glandular fever. Such reactions are not allergic phenomena and do not contra-indicate future use of these or related drugs. Penicillin Allergy Risk Colour Coding For patients with a type 1 hypersensitivity reaction to penicillin: Drugs in RED are contra-indicated Drugs in ORANGE are NOT for use in patients with a severe penicillin allergy, unless at the discretion of microbiology. Use with caution in patients with a history of minor allergic symptoms. Drugs in GREEN are considered safe

98 In life threatening infections such as bacterial meningitis, consider using 3 rd generation cephalosporins even in patients with a history of penicillin allergy.
99 8.8 EDUCATION AND TRAINING 8.9 EDUCATIONAL RESOURCES Antimicrobial prescribing and stewardship (APS) competencies The goal is to improve the quality of antimicrobial treatment and stewardship and so reduce the risks of inadequate, inappropriate and ill-effects of treatment. This will improve the safety and quality of patient care, and make a significant contribution to the reduction in the emergence and spread of antimicrobial resistance. Antimicrobial stewardship is an important element of the UK five-year antimicrobial resistance strategy. Antimicrobial resistance is a global public health issue driven by the overuse of antimicrobials and inappropriate prescribing. The increase in resistance is making antimicrobial agents less effective and contributing to infections that are hard to treat. The number of infections due to multi-drug resistant organisms is growing, however, the number of new antibiotics in the pieline is extremely limited. Antimicrobial stewardship initiatives aim to improve the prescribing of all agents, whether they target bacterial, viral, fungal, mycobacterial or protozal infections. Bacterial resistance potentially complicates the management of every infection, no matter how mild they may be at the time of first presentation. Educating the public and clinicians in the prudent use of antimicrobials as part of an antimicrobial stewardship programme is of paramount importance to preserve these crucial treatments and to help control resistance. Antimicrobial stewardship competencies were designed to complement the National Institute for Health and Care Excellence (NICE) National Prescribing Centreâ s (NPC) generic competency framework for all prescribers. Competencies are described as a â œcombination of knowledge, skills, motives and personal traitsâ, development of which should help individuals to continually improve their performance and to work more effectively. The APS competencies can be used by any independent prescriber to help develop their prescribing practice at any point in their professional development in relation to prescribing antimicrobials.
 in collaboration with professional societies including GPs, pharmacists,")
100 PHE Antimicrobial Prescribing and Stewardship Competencies TARGET antibiotics toolkit The TARGET toolkit has been developed by the RCGP, PHE and The Antimicrobial Stewardship in Primary Care (ASPIC) in collaboration with professional societies including GPs, pharmacists, microbiologists, clinicians, guidance developers and other stakeholders. The toolkit provides a wealth of information about antibiotic prescribing including: Patient information leaflets Resources for clinicians Training resources to help fulfil CPD and revalidation requirements Audit toolkits Self-assessment checklist providing strategies to help optimize antibiotic prescribing in primary care
 is urging members of the public and healthcare professionals to join in the campaign and take action and help make sure")
101 8.10 ANTIBIOTIC RESISTANCE IS ONE OF THE BIGGEST THREATS FACING US TODAY. Antibiotic Guardian, an initiative developed by Public Health England (PHE) is urging members of the public and healthcare professionals to join in the campaign and take action and help make sure antibiotics work now and in the future. To become an Antibiotic Guardian people choose and enact a pledge about how they will make better use of antibiotics. What we want you to do: To slow resistance we need to cut the unnecessary use of antibiotics. We invite the public, students and educators, farmers, the veterinary and medical communities and professional organisations, to become Antibiotic Guardians. Call to action: Choose one simple pledge about how youâ ll make better use of antibiotics and help save these vital medicines from becoming obsolete. To make your pledge and become an antibiotic guardian see link below:
102 Antibiotic Guardian - make your pledge 8.11 DELAYED PRESCRIBING 8.12 DELAYED PRESCRIBING AND PATIENT INFORMATION LEAFLETS DELAYED PRESCRIPTION STRATEGIES A delayed prescription strategy aims to reduce the usage of antibiotics while providing a safety net for people who genuinely need antibiotics. Usually the person should be advised to use the antibiotic prescription only if their condition has deteriorated WITHIN 3 days or not improved AFTER 3 days. The strategy can be implemented in a number of ways including: People may be issued a script and advised not to redeem it unless it is required. If necessary, the prescription can be post-dated. People can be asked to re-attend the GP surgery reception after 3 days to collect the prescription (if required). If symptoms significantly deteriorate before this time, a telephone consultation can be considered. Always give advice and reassure the patient as well as giving the prescription. Consider giving written advice (such as a patient information leaflet, see link below). TARGET RCGP - treat your infection patient leaflets
103 8.13 PATIENT INFORMATION 8.14 PATIENT INFORMATION LEAFLETS There is evidence that the use of leaflets or booklets outlining the natural history of respiratory tract infections (and information about when to reconsult) can result in reduced antibiotic prescribing. Reductions in antibiotic prescribing have been shown to result in reductions in future demand for consultations. Self-care advice sheets for patients These have been designed for prescribers to use with patients presenting with self-limiting respiratory tract infections for whom no prescription, or a delayed antibiotic prescription is appropriate. The advice sheets have been designed to be used as a tool for prescribers to interact with patients during the consultation, rather than as a â parting giftâ. Treat your infection - patient information leaflet TARGET RCGP - treat your infection patient leaflet
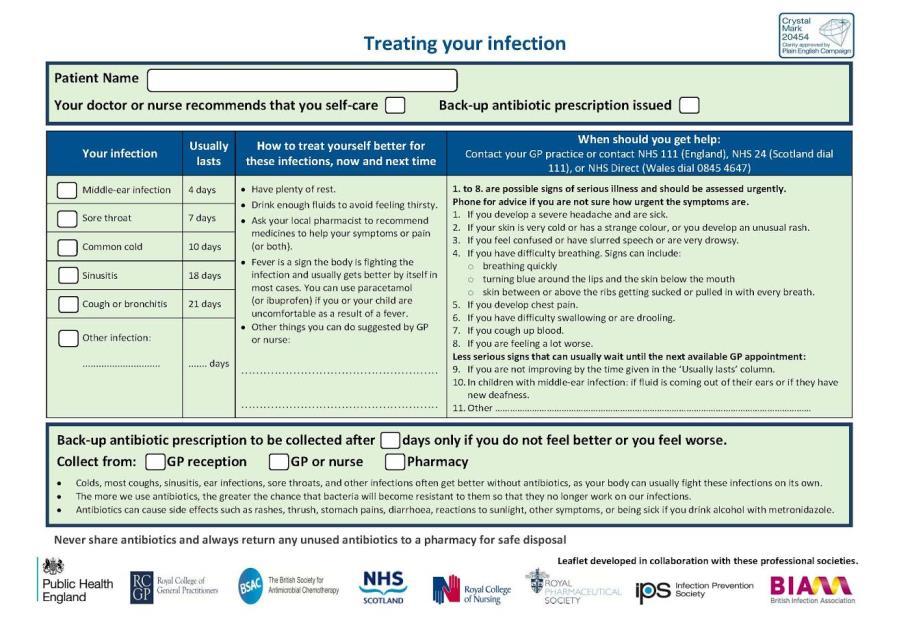
104
Volume. December Infection. Notes. length of. cases as 90% 1 week. tonsillitis. First Line. sore throat / daily for 5 days. quinsy >4000.
 Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
PRIMARY CARE ANTIMICROBIAL GUIDE
 PRIMARY CARE ANTIMICROBIAL GUIDE GENERATED AT THU DEC 27 15:17:38 UTC 2018 1 WHAT'S NEW IN THIS VERSION? What's new in this version? Welcome to the MicroGuide app for the four East Kent CCGs antibiotic
PRIMARY CARE ANTIMICROBIAL GUIDE GENERATED AT THU DEC 27 15:17:38 UTC 2018 1 WHAT'S NEW IN THIS VERSION? What's new in this version? Welcome to the MicroGuide app for the four East Kent CCGs antibiotic
NHS The NHS in Rotherham ANTIMICROBIAL SUMMARY PROTOCOL FOR THE MANAGEMENT OF INFECTION IN PRIMARY CARE Next review due December 2019
 NHS ANTIMICROBIAL SUMMARY PROTOCOL F THE MANAGEMENT OF INFECTION IN PRIMARY CARE 2017-2019 Next review due December 2019 To be used in conjunction with the detailed Antimicrobial Protocol for the Management
NHS ANTIMICROBIAL SUMMARY PROTOCOL F THE MANAGEMENT OF INFECTION IN PRIMARY CARE 2017-2019 Next review due December 2019 To be used in conjunction with the detailed Antimicrobial Protocol for the Management
Volume 2; Number 16 October 2008
 Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Delayed Prescribing for Minor Infections Resource Pack for Prescribers
 Delayed Prescribing for Minor Infections Resource Pack for Prescribers Background: Antibiotic resistance is an alarming threat to modern healthcare, and infectious illness remains a major global threat
Delayed Prescribing for Minor Infections Resource Pack for Prescribers Background: Antibiotic resistance is an alarming threat to modern healthcare, and infectious illness remains a major global threat
Community Antibiotic Guidelines For Common Infections in Adults
 Coventry & Warwickshire Area Prescribing Committee Clinical Guideline CG005 Community Antibiotic Guidelines For Common Infections in Adults Coventry and Warwickshire Microbiology Appendix A Guideline developed
Coventry & Warwickshire Area Prescribing Committee Clinical Guideline CG005 Community Antibiotic Guidelines For Common Infections in Adults Coventry and Warwickshire Microbiology Appendix A Guideline developed
MANAGEMENT OF INFECTION GUIDANCE FOR PRIMARY CARE PRESCRIBERS IN NORTHAMPTONSHIRE
 MANAGEMENT OF INFECTION GUIDANCE FOR PRIMARY CARE PRESCRIBERS IN NORTHAMPTONSHIRE Aims to provide a simple, empirical approach to the treatment of common infections to promote the safe, effective and economic
MANAGEMENT OF INFECTION GUIDANCE FOR PRIMARY CARE PRESCRIBERS IN NORTHAMPTONSHIRE Aims to provide a simple, empirical approach to the treatment of common infections to promote the safe, effective and economic
Volume 1; Number 7 November 2007
 Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Prepared: August Review: July Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide.
 Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
Women s Antimicrobial Guidelines Summary
 Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
Northern Ireland Management of Infection Guidelines for Primary Care 2013 For Review 2015
 Northern Ireland Management of Infection Guidelines for Primary Care 2013 For Review 2015 Health and Social Care Board 1 2 Contents Page Contents Page Aims and principles of treatment 5 Hypersensitivity
Northern Ireland Management of Infection Guidelines for Primary Care 2013 For Review 2015 Health and Social Care Board 1 2 Contents Page Contents Page Aims and principles of treatment 5 Hypersensitivity
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT
 INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: DEC 2015
Guidelines for Antimicrobial treatment for treatment of confirmed infections adults
 Guidelines for Antimicrobial treatment for treatment of confirmed infections adults This guideline gives recommendations for treatment of confirmed infections in adults for children please see the Paediatric
Guidelines for Antimicrobial treatment for treatment of confirmed infections adults This guideline gives recommendations for treatment of confirmed infections in adults for children please see the Paediatric
Acute Pyelonephritis POAC Guideline
 Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
Acute Pyelonephritis POAC Guideline Refer full regional pathway http://aucklandregion.healthpathways.org.nz/33444 EXCLUSION CRITERIA: COMPLICATED PYELONEPHRITIS Discuss with relevant specialist for advice
Guideline for Management of Infection in Primary Care (based on the PHE Management of Infection Guidance for Primary Care 2014)
") Guideline for Management of Infection in Primary Care (based on the PHE Management of Infection Guidance for Primary Care 2014) Ratified by: Prescribing & Medicines Management Group Date ratified: Name
Guideline for Management of Infection in Primary Care (based on the PHE Management of Infection Guidance for Primary Care 2014) Ratified by: Prescribing & Medicines Management Group Date ratified: Name
BNF CHAPTER 5: INFECTIONS
 BNF CHAPTER 5: INFECTIONS December 2012. South East Essex PCT Drug and Therapeutics Committee Aims to provide a simple, safe, effective, economical and empirical approach to the treatment of common infections
BNF CHAPTER 5: INFECTIONS December 2012. South East Essex PCT Drug and Therapeutics Committee Aims to provide a simple, safe, effective, economical and empirical approach to the treatment of common infections
Formulary and Prescribing Guidelines
 SECTION 18: ANTIMICROBIAL PRESCRIBING Formulary and Prescribing Guidelines 18.1 Aims To provide a simple, safe, effective, economical empirical and evidence based approach to the treatment of common infections
SECTION 18: ANTIMICROBIAL PRESCRIBING Formulary and Prescribing Guidelines 18.1 Aims To provide a simple, safe, effective, economical empirical and evidence based approach to the treatment of common infections
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
SECTION 18: ANTIMICROBIAL PRESCRIBING. Formulary and Prescribing Guidelines
 SECTION 18: ANTIMICROBIAL PRESCRIBING Formulary and Prescribing Guidelines 18.1 Aims To provide a simple, safe, effective, economical empirical and evidence based approach to the treatment of common infections
SECTION 18: ANTIMICROBIAL PRESCRIBING Formulary and Prescribing Guidelines 18.1 Aims To provide a simple, safe, effective, economical empirical and evidence based approach to the treatment of common infections
DRAFT DRAFT. Paediatric Antibiotic Prescribing Guideline. May
 Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Infection Management Summary of changes (February 2014 to December 2017)
") Infection Management Summary of changes (February 2014 to December 20) *Significant changes from November 20 have been highlighted in yellow DATE TOPIC CHANGE November 20 Principles of Treatment primary
Infection Management Summary of changes (February 2014 to December 20) *Significant changes from November 20 have been highlighted in yellow DATE TOPIC CHANGE November 20 Principles of Treatment primary
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT
 INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: APRIL
INFECTIONS IN CHILDREN-ANTIMICROBIAL MANAGEMENT Name & Title Of Authors: Dr M Milupi, Consultant Microbiologist Dr N Rao,Consultant Paediatrician Dr V Desai Consultant Paediatrician Date Revised: APRIL
Infection Comments First Line Agents Penicillin Allergy History of multiresistant. line treatment: persist for >7 days they may be
 Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
Issue Number 1. Medicines Management Team (MMT) Thurrock CCG
 Thurrock CCG") Ratifying CCG Board Sub-Committee Brentwood & Basildon Medicines Management Committee on behalf of BRENTWOOD & BASILDON CCG and THURROCK CCG. Date of Issue (Version 1) August 2015 Issue Number 1 Date of
Ratifying CCG Board Sub-Committee Brentwood & Basildon Medicines Management Committee on behalf of BRENTWOOD & BASILDON CCG and THURROCK CCG. Date of Issue (Version 1) August 2015 Issue Number 1 Date of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
PRIMARY CARE ANTIBIOTICS FORMULARY AND GUIDANCE
 PRIMARY CARE ANTIBIOTICS FORMULARY AND GUIDANCE Title Primary Care Antibiotics Formulary and Guidance Reference 1. PHE-Management of infection guidance for primary care, November 2017 (https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attac
PRIMARY CARE ANTIBIOTICS FORMULARY AND GUIDANCE Title Primary Care Antibiotics Formulary and Guidance Reference 1. PHE-Management of infection guidance for primary care, November 2017 (https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attac
2.1 Upper respiratory tract infections : Tonsillitis Sinusitis Acute Otitis Media Acute Otitis Externa Chronic Otitis Externa Influenza
 ADULT ANTIMICROBIAL TREATMENT GUIDELINES FOR PRIMARY CARE The guidelines are navigable by means of hyperlinks between sections. Please navigate around topics and sections by clicking on the underlined
ADULT ANTIMICROBIAL TREATMENT GUIDELINES FOR PRIMARY CARE The guidelines are navigable by means of hyperlinks between sections. Please navigate around topics and sections by clicking on the underlined
your hospitals, your health, our priority PARC (Policy Approval and Ratification Committee) STANDARD OPERATING PROCEDURE:
 STANDARD OPERATING PROCEDURE:") STANDARD OPERATING PROCEDURE: TRUST ANTIBIOTIC TREATMENT SOP SOP NO: TW10/136 SOP 1 VERSION NO: VERSION 6.1 (JANUARY 2013) APPROVING COMMITTEE: INFECTION PREVENTION AND CONTROL COMMITTEE DATE THIS VERSION
STANDARD OPERATING PROCEDURE: TRUST ANTIBIOTIC TREATMENT SOP SOP NO: TW10/136 SOP 1 VERSION NO: VERSION 6.1 (JANUARY 2013) APPROVING COMMITTEE: INFECTION PREVENTION AND CONTROL COMMITTEE DATE THIS VERSION
Wirral Antimicrobial Guidelines and Management of Common Infections in Primary Care
 2017 Wirral Antimicrobial Guidelines and Management of Common Infections in Primary Care Strategies to Optimise Prescribing of Antimicrobials in Primary Care Adapted from the Pan Mersey Antimicrobial Guidelines
2017 Wirral Antimicrobial Guidelines and Management of Common Infections in Primary Care Strategies to Optimise Prescribing of Antimicrobials in Primary Care Adapted from the Pan Mersey Antimicrobial Guidelines
Management of infection guidelines for primary and community services
 Management of infection guidelines for primary and community services Aims of these guidelines To encourage the rational and cost-effective use of antibiotics; To minimise the emergence of bacterial resistance
Management of infection guidelines for primary and community services Aims of these guidelines To encourage the rational and cost-effective use of antibiotics; To minimise the emergence of bacterial resistance
Summary table Infections in primary care
 Summary table Infections in primary care This summary has been based on PHE publication gateway no. 2017227. (pub. Nov 17) Management and treatment of common infections. GCCG local adaptation: June 2018
Summary table Infections in primary care This summary has been based on PHE publication gateway no. 2017227. (pub. Nov 17) Management and treatment of common infections. GCCG local adaptation: June 2018
Wirral Antimicrobial Guidelines and Management of Common Infections in Primary Care
 2016 Wirral Antimicrobial Guidelines and Management of Common Infections in Primary Care Strategies to Optimise Prescribing of Antimicrobials in Primary Care Adapted from the Pan Mersey Antimicrobial Guidelines
2016 Wirral Antimicrobial Guidelines and Management of Common Infections in Primary Care Strategies to Optimise Prescribing of Antimicrobials in Primary Care Adapted from the Pan Mersey Antimicrobial Guidelines
ANTIBIOTIC GUIDELINES Adult and Paediatric
 ANTIBIOTIC GUIDELINES Adult and Paediatric See BNF or Summary of Product Characteristics for full prescribing information Aim To produce simple, appropriate and cost-effective guidelines for the treatment
ANTIBIOTIC GUIDELINES Adult and Paediatric See BNF or Summary of Product Characteristics for full prescribing information Aim To produce simple, appropriate and cost-effective guidelines for the treatment
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children
 Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Greater Manchester Antimicrobial Guidelines
 Greater Manchester Antimicrobial Guidelines July 2018 Version 1.4 Revision date: September 2018 Full review date: April 2019 DOCUMENT CONTROL Document location Copies of this document can be obtained from:
Greater Manchester Antimicrobial Guidelines July 2018 Version 1.4 Revision date: September 2018 Full review date: April 2019 DOCUMENT CONTROL Document location Copies of this document can be obtained from:
Infection Management Summary of changes (Feb-14 to Aug-16)
") Infection Management Summary of changes (Feb-14 to Aug-16) Influenza (CAS alert 28 th June-16; noted at TSAPG 10/08/16 & approved PAMM Acute Sore Throat DoH update 28 th June 2016: https://www.cas.dh.gov.uk/viewandacknowledgment/viewalert.aspx?alertid=102
Infection Management Summary of changes (Feb-14 to Aug-16) Influenza (CAS alert 28 th June-16; noted at TSAPG 10/08/16 & approved PAMM Acute Sore Throat DoH update 28 th June 2016: https://www.cas.dh.gov.uk/viewandacknowledgment/viewalert.aspx?alertid=102
Management of Infection guidance for Primary Care for Wiltshire/Swindon/BaNES CCG September 2017
 Principles of Treatment 1. This guidance is based on the best available evidence but use professional judgement and involve patients in management decisions. 2. This guidance should not be used in isolation;
Principles of Treatment 1. This guidance is based on the best available evidence but use professional judgement and involve patients in management decisions. 2. This guidance should not be used in isolation;
Author s: Clinical Standards Group and Effectiveness Sub-Board
 Trust Antibiotic Policy for the Management of Common Infections in Accident and Emergency and Cromer Minor Injuries Unit (Paediatrics) Accident and Emergency, Norfolk and Norwich and For Use in: Cromer
Trust Antibiotic Policy for the Management of Common Infections in Accident and Emergency and Cromer Minor Injuries Unit (Paediatrics) Accident and Emergency, Norfolk and Norwich and For Use in: Cromer
Management of infection guidelines for primary and community services
 Management of infection guidelines for primary and community services May 2018 Aims of these guidelines To encourage the rational and cost-effective use of antibiotics To minimise the emergence of bacterial
Management of infection guidelines for primary and community services May 2018 Aims of these guidelines To encourage the rational and cost-effective use of antibiotics To minimise the emergence of bacterial
Cork and Kerry SARI Newsletter; Vol. 2 (2), December 2006
, December 2006") Cork and SARI Newsletter; Vol. 2 (2), December 6 Item Type Newsletter Authors Murray, Deirdre;O'Connor, Nuala;Condon, Rosalind Download date 31/1/18 15:27:31 Link to Item http://hdl.handle.net/1147/67296
Cork and SARI Newsletter; Vol. 2 (2), December 6 Item Type Newsletter Authors Murray, Deirdre;O'Connor, Nuala;Condon, Rosalind Download date 31/1/18 15:27:31 Link to Item http://hdl.handle.net/1147/67296
Intro Who should read this document 2 Key practice points 2 Background 2
 Antibiotic Guidelines: Obstetric Anti-Infective Prescribing Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Kelly Alexander / Frances Garraghan
Antibiotic Guidelines: Obstetric Anti-Infective Prescribing Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Kelly Alexander / Frances Garraghan
Cephalosporins, Quinolones and Co-amoxiclav Prescribing Audit
 Cephalosporins, Quinolones and Co-amoxiclav Prescribing Audit Executive Summary Background Antibiotic resistance poses a significant threat to public health, as antibiotics underpin routine medical practice.
Cephalosporins, Quinolones and Co-amoxiclav Prescribing Audit Executive Summary Background Antibiotic resistance poses a significant threat to public health, as antibiotics underpin routine medical practice.
Management of infection guidelines for primary and community services
 Management of infection guidelines for primary and community services Aims of these guidelines To encourage the rational and cost-effective use of antibiotics; To minimise the emergence of bacterial resistance
Management of infection guidelines for primary and community services Aims of these guidelines To encourage the rational and cost-effective use of antibiotics; To minimise the emergence of bacterial resistance
Great Yarmouth and Waveney area Antibiotic Formulary. Primary Care, Community Services and Out of Hours. Revision date: Autumn 2018
 Great Yarmouth and Waveney area Antibiotic Formulary 2018 Primary Care, Community Services and Out of Hours Revision date: Autumn 2018 The broad spectrum quinolones, clindamycin, co-amoxiclav, second and
Great Yarmouth and Waveney area Antibiotic Formulary 2018 Primary Care, Community Services and Out of Hours Revision date: Autumn 2018 The broad spectrum quinolones, clindamycin, co-amoxiclav, second and
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
MANAGEMENT OF PELVIC INFLAMMATORY DISEASE
 GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC
 Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Antibiotic Stewardship Program
 Antibiotic Stewardship Program KISS PRINCIPLE: KEEP IT SIMPLE AND SUSCEPTIBLE PRESENTED BY: WILLIAM G. DAY, DPH, PD, RPH, FASCP Start an Antimicrobial Stewardship Program: Identify Champions and Gather
Antibiotic Stewardship Program KISS PRINCIPLE: KEEP IT SIMPLE AND SUSCEPTIBLE PRESENTED BY: WILLIAM G. DAY, DPH, PD, RPH, FASCP Start an Antimicrobial Stewardship Program: Identify Champions and Gather
Antimicrobial Guidelines for Primary Care
 Primary Care Approved for use in: NHS Blackburn with Darwen CTP NHS East Lancashire Antimicrobial Guidelines for Primary Care February 2012 Version 3.0 Please destroy all copies of version 2.0 due to an
Primary Care Approved for use in: NHS Blackburn with Darwen CTP NHS East Lancashire Antimicrobial Guidelines for Primary Care February 2012 Version 3.0 Please destroy all copies of version 2.0 due to an
Management of infection guidelines for primary and community services
 Management of infection guidelines for primary and community services October 2018 Contents Upper respiratory tract infections 5 Otitis media (child doses) 5 Acute diffuse Otitis externa 5 Influenza treatment
Management of infection guidelines for primary and community services October 2018 Contents Upper respiratory tract infections 5 Otitis media (child doses) 5 Acute diffuse Otitis externa 5 Influenza treatment
Infection Guidance in Primary Care
 Principles of treatment: Infection Guidance in Primary Care 1. This guidance is based on the best available evidence, but use professional judgement and involve patients in management decisions. 2. This
Principles of treatment: Infection Guidance in Primary Care 1. This guidance is based on the best available evidence, but use professional judgement and involve patients in management decisions. 2. This
Update on Fluoroquinolones. Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO
 Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Leicester, Leicestershire and Rutland ANTIMICROBIAL POLICY AND GUIDANCE FOR PRIMARY CARE
 Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group Community Hospitals Urgent Care Centres and Out
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group Community Hospitals Urgent Care Centres and Out
North East London (NEL) Management of Infection Guidance for Primary Care
 Management of Infection Guidance for Primary Care") North East London (NEL) Management of Infection Guidance for Primary Care Adapted from the Public Health England (PHE) Management of infection guidance for primary care for consultation and local adaptation
North East London (NEL) Management of Infection Guidance for Primary Care Adapted from the Public Health England (PHE) Management of infection guidance for primary care for consultation and local adaptation
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE
 ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE Version 1.0 Date ratified June 2009 Review date June 2011 Ratified by Authors Consultation Nottingham Antibiotic Guidelines Committee
ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE Version 1.0 Date ratified June 2009 Review date June 2011 Ratified by Authors Consultation Nottingham Antibiotic Guidelines Committee
This Primary Care Antimicrobial Treatment Guidelines is intended to be accessed electronically only.
 PRIMARY CARE ANTIMICROBIAL TREATMENT GUIDELINES April 2015 Date Ratified by Area Prescribing Committee: April 2015 Date to be Reviewed: April 2017 This Antimicrobial Treatment Guidelines is intended to
PRIMARY CARE ANTIMICROBIAL TREATMENT GUIDELINES April 2015 Date Ratified by Area Prescribing Committee: April 2015 Date to be Reviewed: April 2017 This Antimicrobial Treatment Guidelines is intended to
Antimicrobial Prescribing Guidelines for Primary Care 2017
 Antimicrobial Prescribing Guidelines for Primary Care 2017 TABLE OF CONTENTS PRINCIPLES OF TREATMENT 3 SUMMARY OF UPDATES TO GUIDELINES 4 UPPER RESPIRATORY TRACT INFECTIONS Influenza 5 Pharyngitis / Sore
Antimicrobial Prescribing Guidelines for Primary Care 2017 TABLE OF CONTENTS PRINCIPLES OF TREATMENT 3 SUMMARY OF UPDATES TO GUIDELINES 4 UPPER RESPIRATORY TRACT INFECTIONS Influenza 5 Pharyngitis / Sore
Antimicrobial Guidelines and Management of Common Infections in Primary Care
 2015 Antimicrobial Guidelines and Management of Common Infections in Primary Care Strategies to Optimise Prescribing of Antimicrobials in Primary Care Adapted from the Pan-Mersey Antimicrobial guidelines
2015 Antimicrobial Guidelines and Management of Common Infections in Primary Care Strategies to Optimise Prescribing of Antimicrobials in Primary Care Adapted from the Pan-Mersey Antimicrobial guidelines
Let me clear my throat: empiric antibiotics in
 Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
Antimicrobial Prescribing Guidelines for Primary Care 2017
 Antimicrobial Prescribing Guidelines for Primary Care 2017 TABLE OF CONTENTS PRINCIPLES OF TREATMENT 3 SUMMARY OF UPDATES TO GUIDELINES 4 UPPER RESPIRATORY TRACT INFECTIONS Influenza 6 Pharyngitis / Sore
Antimicrobial Prescribing Guidelines for Primary Care 2017 TABLE OF CONTENTS PRINCIPLES OF TREATMENT 3 SUMMARY OF UPDATES TO GUIDELINES 4 UPPER RESPIRATORY TRACT INFECTIONS Influenza 6 Pharyngitis / Sore
Suffolk Antibiotic Formulary for use in Primary Care and A&E
 Suffolk Antibiotic Formulary for use in Primary Care and A&E Autumn 2017 - Autumn 2019 An electronic version of this formulary is available on West Suffolk CCG and Ipswich and East Suffolk CCG medicines
Suffolk Antibiotic Formulary for use in Primary Care and A&E Autumn 2017 - Autumn 2019 An electronic version of this formulary is available on West Suffolk CCG and Ipswich and East Suffolk CCG medicines
Worcestershire Guidelines for Primary Care Antimicrobial Prescribing
 Worcestershire Guidelines for Primary Care Antimicrobial Prescribing Fifth Edition v.5 Updated February 2018 Review date: October 2018 Always consider if antibiotic treatment is necessary Prescribing antibiotics
Worcestershire Guidelines for Primary Care Antimicrobial Prescribing Fifth Edition v.5 Updated February 2018 Review date: October 2018 Always consider if antibiotic treatment is necessary Prescribing antibiotics
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007
 Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Antibiotic Prophylaxis in Spinal Surgery Antibiotic Guidelines. Contents
 Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
North East London (NEL) Management of Infection Guidance for Primary Care
 Management of Infection Guidance for Primary Care") North East London (NEL) Management of Infection Guidance for Primary Care Adapted from the Public Health England (PHE) Management of infection guidance for primary care for consultation and local adaptation
North East London (NEL) Management of Infection Guidance for Primary Care Adapted from the Public Health England (PHE) Management of infection guidance for primary care for consultation and local adaptation
Antibiotic Formulary 2015/16
 ww Great Yarmouth and Waveney area Primary Care, Community Services and Out of Hours Antibiotic Formulary 2015/16 Revision date: Autumn 2016 Primary Care, Community Services and Out of Hours - Antibiotics
ww Great Yarmouth and Waveney area Primary Care, Community Services and Out of Hours Antibiotic Formulary 2015/16 Revision date: Autumn 2016 Primary Care, Community Services and Out of Hours - Antibiotics
Pharmaceutical issues relating to STI s. June Minton Lead HIV/GUM & Infectious Diseases Pharmacist University College London Hospitals NHS Trust
 Pharmaceutical issues relating to STI s June Minton Lead HIV/GUM & Infectious Diseases Pharmacist University College London Hospitals NHS Trust Objectives Treatment options for syphilis, LGV, TV, gonorrhoea
Pharmaceutical issues relating to STI s June Minton Lead HIV/GUM & Infectious Diseases Pharmacist University College London Hospitals NHS Trust Objectives Treatment options for syphilis, LGV, TV, gonorrhoea
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
North Yorkshire Guidance for use of Antimicrobials in Primary Care
 North Yorkshire Guidance for use of Antimicrobials in Primary Care North Yorkshire Guidance for use of Antimicrobials in Primary Care January 2012 Version 2.00 January 2012 Acknowledgements This document
North Yorkshire Guidance for use of Antimicrobials in Primary Care North Yorkshire Guidance for use of Antimicrobials in Primary Care January 2012 Version 2.00 January 2012 Acknowledgements This document
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Workshop on the use of antibiotics. Dr Rosemary Ikram FRCPA Consultant Clinical Microbiologist
 Workshop on the use of antibiotics. Dr Rosemary Ikram FRCPA Consultant Clinical Microbiologist Declaration of affiliations. Working with: BPAC, DHBSS laboratory schedule group, IANZ, Pharmacy Brands (UTI
Workshop on the use of antibiotics. Dr Rosemary Ikram FRCPA Consultant Clinical Microbiologist Declaration of affiliations. Working with: BPAC, DHBSS laboratory schedule group, IANZ, Pharmacy Brands (UTI
1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient
 1 Chapter 79, Self-Assessment Questions 1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient with normal renal function is: A. Trimethoprim-sulfamethoxazole B. Cefuroxime
1 Chapter 79, Self-Assessment Questions 1. The preferred treatment option for an initial UTI episode in a 22-year-old female patient with normal renal function is: A. Trimethoprim-sulfamethoxazole B. Cefuroxime
$100 $200 $300 $400 $500
 Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Remember, prescribe an antibiotic only when there is likely to be a clear clinical benefit
 Treatment of infections in Primary Care Principles of Treatment Infections of the ear, nose and oropharynx Respiratory tract infections Meningitis Infections of the genito-urinary system and sexually transmitted
Treatment of infections in Primary Care Principles of Treatment Infections of the ear, nose and oropharynx Respiratory tract infections Meningitis Infections of the genito-urinary system and sexually transmitted
Does flagyl treat gonorrhea and chlamydia
 Does flagyl treat gonorrhea and chlamydia The Borg System is 100 % Does flagyl treat gonorrhea and chlamydia Mild Chlamydia infection, limited to the cervix, can be treated with a single dose of an antibiotic
Does flagyl treat gonorrhea and chlamydia The Borg System is 100 % Does flagyl treat gonorrhea and chlamydia Mild Chlamydia infection, limited to the cervix, can be treated with a single dose of an antibiotic
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Helicobacter pylori testing and eradication in adults bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly
Helicobacter pylori testing and eradication in adults bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly
UTI Dr S Mathijs Department of Pharmacology
 UTI Dr S Mathijs Department of Pharmacology Introduction Responsible for > 7 million consultations annually 15% of all antibiotic prescriptions 40% of all hospital acquired infections Significant burden
UTI Dr S Mathijs Department of Pharmacology Introduction Responsible for > 7 million consultations annually 15% of all antibiotic prescriptions 40% of all hospital acquired infections Significant burden
CLINICAL PROTOCOL FOR COMMUNITY ACQUIRED PNEUMONIA. SCOPE: Western Australia. CORB score equal or above 1. All criteria must be met:
 CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
Antimicrobial Resistance, Everyone s Fight. Charlotte Makanga Consultant Antimicrobial Pharmacist Betsi Cadwaladr University Health Board
 Antimicrobial Resistance, Everyone s Fight Charlotte Makanga Consultant Antimicrobial Pharmacist Betsi Cadwaladr University Health Board Antimicrobial Resistance Antimicrobial resistance happens when microorganisms
Antimicrobial Resistance, Everyone s Fight Charlotte Makanga Consultant Antimicrobial Pharmacist Betsi Cadwaladr University Health Board Antimicrobial Resistance Antimicrobial resistance happens when microorganisms
ECHO: Management of URIs. Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018
 ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
Antibiotic Guidelines
 Antibiotic Guidelines Antibiotics were first discovered in the middle of the 20 th century and have since saved millions of lives and practically eradicated previously fatal conditions such as tuberculosis
Antibiotic Guidelines Antibiotics were first discovered in the middle of the 20 th century and have since saved millions of lives and practically eradicated previously fatal conditions such as tuberculosis
Treatment of Sexually Transmitted Infections. Wolverton Centre Guidelines
 Treatment of Sexually Transmitted Infections Wolverton Centre Guidelines Updated Jan 2018 Please ensure that you have the latest version. V: Department Folder/Standard Operating Guides/Clinical Governance/Treatment
Treatment of Sexually Transmitted Infections Wolverton Centre Guidelines Updated Jan 2018 Please ensure that you have the latest version. V: Department Folder/Standard Operating Guides/Clinical Governance/Treatment
Antimicrobial Stewardship in Continuing Care. Urinary Tract Infections Clinical Checklist
 Antimicrobial Stewardship in Continuing Care Urinary Tract Infections Clinical Checklist December 2014 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis at the
Antimicrobial Stewardship in Continuing Care Urinary Tract Infections Clinical Checklist December 2014 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis at the
Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy
 biopsy") Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy Dr. Fidelma Fitzpatrick Consultant Microbiologist, Co-chair, NCCP Prostate Bx Infection Project Board Fidelma.fitzpatrick@hse.ie
Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy Dr. Fidelma Fitzpatrick Consultant Microbiologist, Co-chair, NCCP Prostate Bx Infection Project Board Fidelma.fitzpatrick@hse.ie
National Antimicrobial Prescribing Survey
 Indication documented Surgical prophylaxis >24 hrs Allergy mismatch Microbiology mismatch Incorrect route Incorrect dose/frequency Incorrect duration Therapeutic Guidelines Local guidelines * Non-compliant
Indication documented Surgical prophylaxis >24 hrs Allergy mismatch Microbiology mismatch Incorrect route Incorrect dose/frequency Incorrect duration Therapeutic Guidelines Local guidelines * Non-compliant
OBSTETRICS & GYNAECOLOGY. Penicillin G 5 million units IV ; followed by 2.5 million units 4hourly upto delivery
 OBSTETRICS & GYNAECOLOGY A.OBSTETRICS Infection/Condition/likely organism Intrapartum Group B Streptococcal (GBS) infection; positive mothers Suggested treatment Preferred Penicillin G 5 million units
OBSTETRICS & GYNAECOLOGY A.OBSTETRICS Infection/Condition/likely organism Intrapartum Group B Streptococcal (GBS) infection; positive mothers Suggested treatment Preferred Penicillin G 5 million units
Infection Control and Antibiotic Resistance. Xenia Bray
 Infection Control and Antibiotic Resistance Xenia Bray Learning Objectives Explain why antimicrobial resistance is considered to be one of the greatest public health risks in the UK and globally Apply
Infection Control and Antibiotic Resistance Xenia Bray Learning Objectives Explain why antimicrobial resistance is considered to be one of the greatest public health risks in the UK and globally Apply
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
ANTIMICROBIAL PRESCRIBING GUIDELINES
 Bedfordshire and Luton Community ANTIMICROBIAL PRESCRIBING GUIDELINES No. 10 (2) (May 2018) Addressing known local sensitivities Before you open this book Do you need to prescribe an antibiotic or is it
Bedfordshire and Luton Community ANTIMICROBIAL PRESCRIBING GUIDELINES No. 10 (2) (May 2018) Addressing known local sensitivities Before you open this book Do you need to prescribe an antibiotic or is it
Antimicrobial Guide and Management of Common Infections in Primary Care
 2015/16 Antimicrobial Guide and Management of Common Infections in Primary Care Strategies to Optimise Prescribing of Antimicrobials in Primary Care Currently under review Version: 7.0 Abridged Currently
2015/16 Antimicrobial Guide and Management of Common Infections in Primary Care Strategies to Optimise Prescribing of Antimicrobials in Primary Care Currently under review Version: 7.0 Abridged Currently
Protocol for exit-site care and treatment of exit-site infections in peritoneal dialysis CONTROLLED DOCUMENT
 CONTROLLED DOCUMENT Protocol for exit-site care and treatment of exit-site infections in peritoneal dialysis CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Guideline Clinical The purpose
CONTROLLED DOCUMENT Protocol for exit-site care and treatment of exit-site infections in peritoneal dialysis CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Guideline Clinical The purpose
Symptoms of cellulitis (n=396) %
 %") Cellulitis and lymphoedema Vaughan Keeley May 2012 What is cellulitis? - also called erysipelas, acute inflammatory episodes etc. - bacterial infection of skin + subcutaneous tissues - more common in people
Cellulitis and lymphoedema Vaughan Keeley May 2012 What is cellulitis? - also called erysipelas, acute inflammatory episodes etc. - bacterial infection of skin + subcutaneous tissues - more common in people
NHS SOUTH WEST ESSEX. Antimicrobial Prescribing Guidance For Primary Care
 NHS SOUTH WEST ESSEX Antimicrobial Prescribing Guidance For Primary Care 1 This document has been reviewed by: Dr Justin Edward, Consultant Microbiologist, BTUH Olubusola Daramola, Prescribing Advisor/Antibiotics
NHS SOUTH WEST ESSEX Antimicrobial Prescribing Guidance For Primary Care 1 This document has been reviewed by: Dr Justin Edward, Consultant Microbiologist, BTUH Olubusola Daramola, Prescribing Advisor/Antibiotics
Remember: AIEs are painful: analgesics should be prescribed regularly and p.r.n. palliativedrugs.com November/December newsletter
 ACUTE INFLAMMATORY EPISODES IN A LYMPHOEDEMATOUS LIMB Acute inflammatory episodes (AIEs), often called cellulitis, are common in lymphoedema: mild: pain, increased swelling, erythema (well-defined or blotchy)
ACUTE INFLAMMATORY EPISODES IN A LYMPHOEDEMATOUS LIMB Acute inflammatory episodes (AIEs), often called cellulitis, are common in lymphoedema: mild: pain, increased swelling, erythema (well-defined or blotchy)
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Content. In the beginning Antimicrobial Stewardship 2. Antimicrobial Prescribing with cases to cover
 Content Safe & Effective Prescribing of Antimicrobials: Whistle-stop update for non-medical prescribers Elaine Roberts Lead Pharmacist, Antimicrobials BCUHB East 1. Antimicrobial Stewardship 2. Antimicrobial
Content Safe & Effective Prescribing of Antimicrobials: Whistle-stop update for non-medical prescribers Elaine Roberts Lead Pharmacist, Antimicrobials BCUHB East 1. Antimicrobial Stewardship 2. Antimicrobial
Role of the nurse in diagnosing infection: The right sample, every time
 BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical