Intraabdominal infections
|
|
|
- Hester Lyons
- 5 years ago
- Views:
Transcription
1 Intraabdominal infections Appendicitis Cholecystitis Diverticulitis Cholangiitis Acalculosus cholecystitis Purulent Liver abscess Peritonitis Perirenal abscess AbscessSpontaneous bacterial peritonitis Perforation Gastroenteritis
2 Definition An uncomplicated IAI does not spread throughout the peritoneum and is limited to a single organ A complicated IAI (ciai) is diagnosed when the initial infection has spread into the peritoneal space Complicated IAIs are of major concern because of their high prevalence and their high morbidity and mortality rates. overall mortality rate for IAIs was 10.5 % typically polymicrobial, as the gastrointestinal tract contains a large variety of microorganisms Sartelli M, Catena F, Ansaloni L, Coccolini F, Corbella D, Moore EE, et al. Complicated intra-abdominal infections worldwide: the definitive data of the CIAOW Study. World J Emerg Surg. 2014;9:37. doi: /
3 MORTALITY OF INTRA-ABDOMINAL INFECTIONS Mortality % Localized Abscess Localized Peritonitis Diffuse Suppurative Peritonitis Combined Complicated Infection
4 Definition complicated IAI (ciai) Infections that spread beyond the hollow viscus of origin into the peritoneal space and are associated with: abscess formation or peritonitis primary = spontaneous bacterial peritonitis arises without a breach in the peritoneal cavity or GI tract secondary occurs as a result of spillage of gut organisms through a physical hole in the GI tract or through a necrotic gut wall may be community acquired or healthcare associated tertiary peritonitis in a critically ill patient which persists or recurs at least 48 h after apparently adequate management of primary or secondary peritonitis
5 Microbiology Abscesses or secondary peritonitis health care associated intra-abdominal infection usually due to nosocomial organisms particular to the site of the operation and specific hospital and unit community acquired infections infections derived from stomach, duodenum, biliary system and proximal small bowel: Gram positive and Gram negative aerobic and facultative bacteria distal small bowel: Gram negative facultative and aerobic bacteria Anaerobes large bowel: Facultative and obligate anaerobic bacteria Streptococi and enterococci commonly present Tertiary peritonitis coagulase negative staphylococci Pseudomonas Candida Enterococci
6 Empiric antimicrobial coverage needs to be adequate for Grampositive, Gramnegative, aerobic, and anaerobic bacteria. Coverage for anaerobic bacteria is especially important for infections that originate from the distalsmallbowel, appendix, or colon
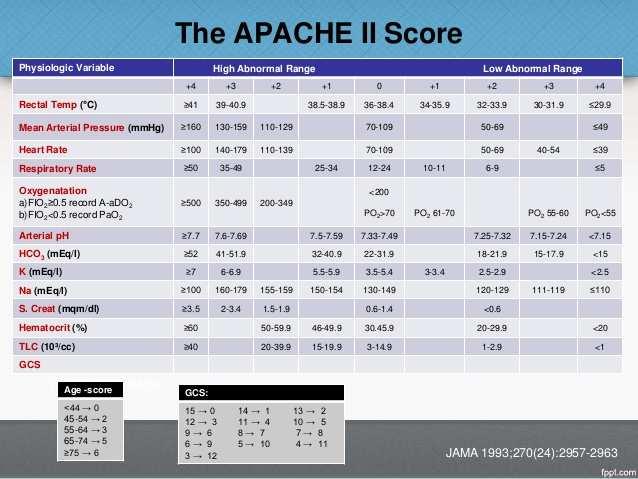
7 Complicated IAI The 2010 Surgical Infection Society (SIS)/Infectious Diseases Society of America (IDSA) guidelines for the management of ciais identify three distinct treatment categories: low-risk community-acquired (CA), high-risk CA, and healthcare-associated ciais. Factors that identify a CA infection as high risk include Acute Physiology and Chronic Health Evaluation (APACHE) II score greater than 15, extensive cardiovascular disease, poor nutritional status, failure to achieve sufficient source control, immunosuppression, extended length of hospital stay before the operation ( 5 days), and extended use of preoperative antimicrobial treatment ( 2 days)
8
9 Clinicalfeatures difficult to diagnose in the critically ill patient because history is usually unobtainable and physical signs usually masked by decreased conscious level consider diagnosis in the appropriate clinical setting in patients with otherwise unexplained signs of sepsis or organ dysfunction: recent abdominal surgery source of arterial emboli peripheral vascular disease thrombotic disorder recent arteriography history of reduced splanchnic blood flow (eg use of vasopressors or prolonged shock) unexpected shortness of breath or supraventricular tachycardia occurring 3-4 days after an abdominal operation, new onset renal dysfunction or elevated bilirubin or transaminases should all raise suspicion of intra-abdominal infection
10 Investigations Microbiological Blood cultures often negative polymicrobial or anaerobic bacteraemia should raise possibility of anaerobic infection Community acquired infections: Gram stain of no value Healthcare associated infections: Gram stain may be valuable in defining need for specific therapy S.aureus or Enterococcus spp. Radiological
11 Diagnostic approach to intra-abdominal infection AXR look for free gas, bowel obstruction, or subtle signs of intestinal ischaemia water-soluble contrast studies can show leaks injection of contrast into drains, fistulae or sinus tracts may help demonstrate anatomy of complex infectios and help monitor adequacy of abscess drainage Ultrasound advantage of being portable and almost risk-free useful for: identifying abscesses and fluid collections guidance of percutaneous drainage procedures detection of free fluid evaluation of biliary tree disadvantages: operator dependent difficult to perform in patients who have abdominal dressings or paralytic ileus CT abdomen
12 Diagnostic approach to intra-abdominal infection Abdominal CT with use of IV and oral or rectal contrast most causes of secondary peritonitis can be readily diagnosed requires movement of potentially unstable patient out of ICU relative contraindications: renal dysfunction: contrast may aggravate renal dysfunction paralytic ileus a negative CT generally indicates a very low probability of a process that can be reversed by surgical intervention, however bowel ischaemia cannot be excluded, particularly in the early stages
13 Invasive investigations in ICU judicious probing of surgical wounds with sterile culture swab or gloved finger can often identify collections of infected material immediately adjacent to incision diagnostic peritoneal lavage may reveal bacteria, white cells, bile or intestinal contents bloody lavage return suggests acute intestinal ischaemia bedside laparoscopy difficult experience in critically ill patients largely anecdotal
14 Antibacterials Management 1. physiological resuscitation 2. systemic antibiotics 3. source control Should be administered as soon as infection is suspected and preferably before surgical intervention (to minimize the risk of surgical wound infection.
15 Choice of antibacterials for community acquired infection should be active against enteric Gram negative aerobic and facultative bacilli and ᵦ-lactam susceptible Gram positive cocci for distal small bowel and colon-derived infections antibacterials should cover anaerobes. Same recommendation also applies to more proximal GI perforations when obstruction is present avoid agents used to treat nosocomial infection in the ICU, except for high risk patients inclusion of antibacterials that cover enterococcal infections provides no benefit in terms of outcome for patients with community acquired infections suitable regimes include: cefazolin or cefuroxime plus metronidazole metronidazole plus quinolone(eg moxifloxacin or gatifloxacin) high risk patients should be given antibacterials with a wider spectrum of activity suitable regimes include: Piperacillin/tazobactam Imipenem, meropenem 3rd or 4th gen cephalosporin plus metronidazole ciprofloxacin plus metronidazole aztreonam plus metronidazole risk factors: higher APACHE II poor nutritional status significant cardiovascular disease inability to obtain adequate source control immunosuppression
16 Choice of antibacterials forhealthcare associated infection More resistant flora routinely encountered Organisms seen are similar to those seen in other nosocomial infections Treatment should be based on knowledge of local nosocomial flora and their resistance patterns Agents which cover enterococci should be used when enterococci are isolated from patients with healthcare associated infections Role of antibiotics in tertiary peritonitis is poorly defined little evidence that they significantly alter outcome some recommend the use of narrow spectrum agents based on results of culture and sensitivity and avoidance of agents with anti-anaerobic activity there are some data which suggest that use of antibiotics with antianaerobic activity increases gut colonization with Candida and vancomycin resistant Enterococci.
17 Duration of therapy No more that 24 h for: bowel injuries due to penetrating, blunt or iatrogenic trauma that are repaired within 12 h intraoperative contamination of operative field by enteric contents acute perforations of stomach, duodenum and proximal jejunum in absence of antacid therapy or malignancy For patients with established infections: until resolution of signs of infection occurs. This assessment should be based on signs of sepsis and return of GI function if source control is adequate the role of antibiotics is largely adjuvant and the course can usually be restricted to 5-7 days further investigation is indicated or patients with persistent or recurrent clinical evidence of intra-abdominal infection after 5-7 days of therapy
18 Source control Physical measures to eradicated focus of infection, prevent on-going contamination and ultimately to restore optimal anatomy and function 1. drainage 2. debridement 3. definitive management Successful source control and antibiotic management is associated with resolution of clinical features of systemic inflammation and reversal of organ dysfunction. Progression or failure of resolution of organ dysfunction suggests persistence of the disease and the need for further intervention

19 1. Drainage formation of an abscess isolates infection from surrounding sterile tissues but has disadvantage of preventing influx of host immune cells and antibiotics drainage converts to a controlled sinus or fistula percutaneous ultrasound or CT guided drainage is initial intervention of choice for management of localized, radiologically defined infectious foci can also be used as a temporizing measure eg. to decompress infected retroperitoneal collections in patients with necrotizing pancreatitis so operative intervention can be delayed until it is safer indications for surgical drainage: failure of percutaneous drainage collections with a significant solid tissue component requiring debridement simultaneous managment of a source of ongoing contamination when local peritoneal defences have not contained the infectious focus, resulting in generalized peritonitis
20 2. Debridement in contrast to drainage which removes the liquid component of an infection, debridement is the physical removal of infected or necrotic solid removal debridement less frequently required in patients with intra-abdominal infection main indications in this setting: intestinal infarction infected peripancreatic necrosis decision of when to operate relates to relative risks and benefits. Thus the benefit of early excision of necrotic bowel vastly outweighs the risks. In contrast, the bacterial burden in infected retroperitoneal necrosis is lower and the organisms sequestered in the necrotic tissue are less able to gain access to the circulation. In addition early exploration is difficult because of poor demarcation between viable and non viable tissue. As a result there is a trend to delayed rather than immediate intervention
21 Diverticulosis Diverticulosis is extremely common, affecting 50-80% of people older than 80 years Complications Acute diverticulitis Bleeding Perforation Stage I Stage II Stage III Stage IV Stages of diverticulitis Small, confined pericolic abscess Distant abscess (retroperitoneal or pelvic) Generalized supportive peritonitis from rupture of abscess (noncommunicating with bowel lumen) Fecal peritonitis caused by free communicating perforation
22 Diverticulitis - Treatment Outpatient vs. Hospital admission Need for narcotics to control pain Presence of peritoneal signs Comorbidities, signs of sepsis Inability to tolerate oral liquids Complications that may potentially require surical intervention Abscess peritonitis Outpatient Broad-spectrum AB that covers Gr- rods and anaerobes, eg.: Trimethoprim/sulfamethoxazole Cipro+metronidazole Clindamycin+gentamycin Clear liquid diet Close FU In hospital
23 Diverticulitis In-hospital Treatment Iv hydration Electrolyte correction Bowel rest (nothing per mouth) Iv broad spectrum AB Ampicillin+/-aminoglycoside+/-metronidazole Carbapenems for more severe cases Pain, fever, WBC are to diminish in few days Dietary intake can be advanced gradually If fever or pain persists look for complications Abscess Stricture obstruction
24 Acute diarrhea 90% of acute diarrhea is infectious Presence of blood would suggest an invasive bacterial infection Enteroinvasive or haemorhagic E.coli Campylobacter Shigella Salmonella If leukocytes are present in stool it is supicious for Salmonella Shigella Yersinia Enteroinvasive or haemorhagic E.coli Clostridium diff Campylobacter Entamoeba histolytica The majority of diarrheas are viral and self-limited
 Rotavirus Giardia lamblia Salmonella Norovirus E.")

25 Traveller s diarrhea Bacteria Viruses Parasites E.Coli (all types) Rotavirus Giardia lamblia Salmonella Norovirus E. histolytica Shigella Vibrio non-cholera Campylobacter Symptom occurence after eating a salad containing mayonnaise Within 6 hours S. aureus 8-12 hours Clostridium perfingens hours E. coli Treatment Prevention Ciprofloxacin 2x500 mg 1-2 days Cryptosporidium parvum Azithromycin single 1000 mg (10 mg/kg in children) - pregnant
26 Postoperative fever Most common postop complication 50% after major surgeries Typically resolves spontaneously If occurs within 36 hours post laparotomy Bowel injury with leakage of GI content into the peritoneum Invasive soft-tissue wound infection B-haemolytic Streptococci HD instability, shock Clostridium Toxic shock syndrome Staph.aureus
 Walk (DVT) Wonder drugs (drug fever)")
27 Postoperative fever Wind (pneumonia) Water (UTI) Wound (SSI) Walk (DVT) Wonder drugs (drug fever)
28 Intraop up to 24h postop Onset Infectious Noninfectious Preexisting Urinary catheter Intraop leakage Invasive soft-tissue Toxic shock sy 1 day to 1 week UTI Pneumonia SSI Catheter related Cellulitis 1-4 weeks after SSI Thrombophlebitis Pseudomembr colitis Device related Abscess > 1 month Transfusion hepatitis IE SSI Device related Vascular graft inf Surgical trauma Medications Blood products (during transfusion) Malignant hyperthermia AMI Alcohol/drug withdrawal Pancreatitis PE Thrombophlebitis Benign postop fever Medication toxicity DVT/PE Postpericardiotomy syndrome
29 Type of surgery ~ fever Laparoscopy less fever Cardiothoracic pleural effusion pneumonia Abdominal deep abdominal abscess, pancreatitis Gynecological deep pelvic abscess, pelvic thrombophlebitis Genitourinary UTI Neurosurgery meningitis, DVT
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT DRAFT AS CURRENTLY OUT FOR CONSULTATION BUT CAN BE UTILISED IN PRESENT FORMAT Name & Title Of Author: Date Revised: Approved by Committee/Group:
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT DRAFT AS CURRENTLY OUT FOR CONSULTATION BUT CAN BE UTILISED IN PRESENT FORMAT Name & Title Of Author: Date Revised: Approved by Committee/Group:
Objectives. Review basic categories of intra-abdominal infection and their respective treatments. Community acquired intra-abdominal infection
 Objectives Review basic categories of intra-abdominal infection and their respective treatments Community acquired intra-abdominal infection Mild/Moderate Severe Acute biliary tract infections Nosocomial
Objectives Review basic categories of intra-abdominal infection and their respective treatments Community acquired intra-abdominal infection Mild/Moderate Severe Acute biliary tract infections Nosocomial
Antimicrobial Prophylaxis in the Surgical Patient. M. J. Osgood
 Antimicrobial Prophylaxis in the Surgical Patient M. J. Osgood Outline Definitions surgical site infection (SSI) Risk factors Wound classification Microbiology of SSIs Strategies for prevention of SSIs
Antimicrobial Prophylaxis in the Surgical Patient M. J. Osgood Outline Definitions surgical site infection (SSI) Risk factors Wound classification Microbiology of SSIs Strategies for prevention of SSIs
Surgical Site Infections (SSIs)
") Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
Treatment of septic peritonitis
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Antibiotic prophylaxis guideline for colorectal, hepatobiliary and vascular surgery for adult patients.
 Antibiotic prophylaxis guideline for colorectal, hepatobiliary and vascular surgery for adult patients. Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience,
Antibiotic prophylaxis guideline for colorectal, hepatobiliary and vascular surgery for adult patients. Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience,
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS
 VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
Intra-abdominal anaerobic infections. Diagnostics and therapy
 Intra-abdominal anaerobic infections. Diagnostics and therapy Elisabeth Nagy MD. PhD. DSc. Institute of Clinical Microbiology, Faculty of Medicine, University of Szeged 4th ESCMID School, Szeged, Hungary
Intra-abdominal anaerobic infections. Diagnostics and therapy Elisabeth Nagy MD. PhD. DSc. Institute of Clinical Microbiology, Faculty of Medicine, University of Szeged 4th ESCMID School, Szeged, Hungary
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Objectives. Basic Microbiology. Patient related. Environment related. Organism related 10/12/2017
 Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Secondary peritonitis
 Secondary peritonitis Caused by spillage of gastrointestinal microorganisms into the peritoneal cavity secondary to loss of the integrity of the mucosal barriers Etiology: perforation of peptic ulcer traumatic
Secondary peritonitis Caused by spillage of gastrointestinal microorganisms into the peritoneal cavity secondary to loss of the integrity of the mucosal barriers Etiology: perforation of peptic ulcer traumatic
Infection Comments First Line Agents Penicillin Allergy History of multiresistant. line treatment: persist for >7 days they may be
 Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
Gastrointestinal Infections Infection Comments First Line Agents Penicillin Allergy History of multiresistant Campylobacter Antibiotics not recommended. Erythromycin 250mg PO 6 Alternative to first N/A
ESCMID Online Lecture Library. by author
 Anaerobic Bacteria in Intra-Abdominal Infections and Bacteremia Maria Hedberg, Umeå University, Umeå, Sweden Anaerobic Bacteria: Next Generation Technology Meets Anaerobic Diagnostics ESCMID Postgraduate
Anaerobic Bacteria in Intra-Abdominal Infections and Bacteremia Maria Hedberg, Umeå University, Umeå, Sweden Anaerobic Bacteria: Next Generation Technology Meets Anaerobic Diagnostics ESCMID Postgraduate
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Prophylactic antibiotic timing and dosage. Dr. Sanjeev Singh AIMS, Kochi
 Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS
 Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Original Date: 02/2010 Purpose: To maximize antibiotic stewardship for intraabdominal infection in the Precedes: 4/2013
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Antibiotic Therapy: Intra-Abdominal Infections Clinical Practice Algorithm Original Date: 02/2010 Purpose: To maximize
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Antibiotic Therapy: Intra-Abdominal Infections Clinical Practice Algorithm Original Date: 02/2010 Purpose: To maximize
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
THERAPY OF ANAEROBIC INFECTIONS LUNG ABSCESS BRAIN ABSCESS
 THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance
 Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Case 2 Synergy satellite event: Good morning pharmacists! Case studies on antimicrobial resistance 22nd Congress of the EAHP "Hospital pharmacists catalysts for change", 22-24 March 2017, Cannes Disclosure
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Meropenem for all? Midge Asogan ICU Fellow (also ID AT)
") Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship
 Curriculum for Antimicrobial Stewardship") General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
Antimicrobial Prophylaxis in Digestive Surgery
 Antimicrobial Prophylaxis in Digestive Surgery Toar JM. Lalisang, MD, PhD Digestive Surgery Division Cipto Mangunkusumo Hospital Medical Faculty Universitas Indonesia Antibiotic must be present before
Antimicrobial Prophylaxis in Digestive Surgery Toar JM. Lalisang, MD, PhD Digestive Surgery Division Cipto Mangunkusumo Hospital Medical Faculty Universitas Indonesia Antibiotic must be present before
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Gynaecological Surgery in Adults Surgical Antibiotic Prophylaxis
 Gynaecological Surgery in Adults Surgical Antibiotic Prophylaxis Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date
Gynaecological Surgery in Adults Surgical Antibiotic Prophylaxis Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date
Role of the nurse in diagnosing infection: The right sample, every time
 BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma
 Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma Lucio Petrizzi DVM DECVS Università degli Studi di Teramo Surgical site infections (SSI) Microbial contamination unavoidable Infection
Antimicrobial Selection and Therapy for Equine Musculoskeletal Trauma Lucio Petrizzi DVM DECVS Università degli Studi di Teramo Surgical site infections (SSI) Microbial contamination unavoidable Infection
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
Scottish Medicines Consortium
 Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Antibiotic Prophylaxis Update
 Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
IDSA GUIDELINES EXECUTIVE SUMMARY
 IDSA GUIDELINES Diagnosis and Management of Complicated Intra-abdominal Infection in Adults and Children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America Joseph
IDSA GUIDELINES Diagnosis and Management of Complicated Intra-abdominal Infection in Adults and Children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America Joseph
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
SURGICAL ANTIBIOTIC PROPHYLAXIS GUIDELINES WITHIN ORTHOPAEDIC SURGERY FOR ADULT PATIENTS
 SURGICAL ANTIBIOTIC PROPHYLAXIS GUIDELINES WITHIN ORTHOPAEDIC SURGERY FOR ADULT PATIENTS Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if
SURGICAL ANTIBIOTIC PROPHYLAXIS GUIDELINES WITHIN ORTHOPAEDIC SURGERY FOR ADULT PATIENTS Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if
Intra-abdominal Infections
 Intra-abdominal Infections Marnie Peterson, Pharm.D., Ph.D., BCPS College of Pharmacy peter377@umn.edu 2006 Marnie Peterson. This presentation is provided to facilitate the learning of participants within
Intra-abdominal Infections Marnie Peterson, Pharm.D., Ph.D., BCPS College of Pharmacy peter377@umn.edu 2006 Marnie Peterson. This presentation is provided to facilitate the learning of participants within
Preventing Multi-Drug Resistant Organism (MDRO) Infections. For National Patient Safety Goal
 Infections. For National Patient Safety Goal") Preventing Multi-Drug Resistant Organism (MDRO) Infections For National Patient Safety Goal 07.03.01 2009 Methicillin Resistant Staphlococcus aureus (MRSA) About 3-8% of the population at large is a carrier
Preventing Multi-Drug Resistant Organism (MDRO) Infections For National Patient Safety Goal 07.03.01 2009 Methicillin Resistant Staphlococcus aureus (MRSA) About 3-8% of the population at large is a carrier
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Antibiotics Guidelines: Gastrointestinal Infections
 Antibiotics Guidelines: Gastrointestinal Infections Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Antibiotics Guidelines: Gastrointestinal Infections Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Antibiotic stewardship in long term care
 Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Who should read this document? 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version? 3
 Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Copyright 2012 Diabetes In Control, Inc. For permission to reprint, please contact Heather Moran, Production Editor, at
 Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
DATA COLLECTION SECTION BY FRONTLINE TEAM. Patient Identifier/ Medical Record number (for facility use only)
") Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS
 PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
Chapter Anaerobic infections (individual fields): prevention and treatment of postoperative infections
: prevention and treatment of postoperative infections") J Infect Chemother (2011) 17 (Suppl 1):62 66 DOI 10.1007/s10156-010-0141-x GUIDELINES Chapter 2-5-1. Anaerobic infections (individual fields): prevention and treatment of postoperative infections Ó Japanese
J Infect Chemother (2011) 17 (Suppl 1):62 66 DOI 10.1007/s10156-010-0141-x GUIDELINES Chapter 2-5-1. Anaerobic infections (individual fields): prevention and treatment of postoperative infections Ó Japanese
Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis
 Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis Steve SM Wong Alice Ho Miu Ling Nethersole Hospital Background PD peritonitis is a major cause of PD
Randomized Controlled Trial on Adjunctive Lavage for Severe Peritoneal Dialysis- Related Peritonitis Steve SM Wong Alice Ho Miu Ling Nethersole Hospital Background PD peritonitis is a major cause of PD
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Dr. Shaiful Azam Sazzad. MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College
 Critical Care Medicine Dhaka Medical College") Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Surgical infection ผ.ศ. น.พ. กำธร มำลำธรรม หน วยโรคต ดเช อ ภำคว ชำอำย รศำสตร คณะแพทยศำสตร โรงพยำบำลรำมำธ บด
 Surgical infection ผ.ศ. น.พ. กำธร มำลำธรรม หน วยโรคต ดเช อ ภำคว ชำอำย รศำสตร คณะแพทยศำสตร โรงพยำบำลรำมำธ บด 1 Scope Surgical prophylaxis: Pharmacologic approach to prevent SSI Antimicrobial therapy for
Surgical infection ผ.ศ. น.พ. กำธร มำลำธรรม หน วยโรคต ดเช อ ภำคว ชำอำย รศำสตร คณะแพทยศำสตร โรงพยำบำลรำมำธ บด 1 Scope Surgical prophylaxis: Pharmacologic approach to prevent SSI Antimicrobial therapy for
** the doctor start the lecture with revising some information from the last one:
 Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
DRAFT DRAFT. Paediatric Antibiotic Prescribing Guideline. May
 Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Neurosurgery Antibiotic Prophylaxis Guideline
 Neurosurgery Antibiotic Prophylaxis Guideline Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version
Neurosurgery Antibiotic Prophylaxis Guideline Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
Antibiotic Prophylaxis in Spinal Surgery Antibiotic Guidelines. Contents
 Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Protein Synthesis Inhibitors
 Protein Synthesis Inhibitors Assistant Professor Dr. Naza M. Ali 11 Nov 2018 Lec 7 Aminoglycosides Are structurally related two amino sugars attached by glycosidic linkages. They are bactericidal Inhibitors
Protein Synthesis Inhibitors Assistant Professor Dr. Naza M. Ali 11 Nov 2018 Lec 7 Aminoglycosides Are structurally related two amino sugars attached by glycosidic linkages. They are bactericidal Inhibitors
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Burn Infection & Laboratory Diagnosis
 Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
Pharmacology Week 6 ANTIMICROBIAL AGENTS
 Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Microbiological evaluation and antimicrobial treatment of complicated intra-abdominal infections
 Microbiological evaluation and antimicrobial treatment of complicated intra-abdominal s H van der Plas Helen van der Plas, FCP(SA), Cert ID(SA)Phys, DTM&H, Senior Specialist and Senior Lecturer Division
Microbiological evaluation and antimicrobial treatment of complicated intra-abdominal s H van der Plas Helen van der Plas, FCP(SA), Cert ID(SA)Phys, DTM&H, Senior Specialist and Senior Lecturer Division
Aminoglycosides. Spectrum includes many aerobic Gram-negative and some Gram-positive bacteria.
 Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
Aminoglycosides The only bactericidal protein synthesis inhibitors. They bind to the ribosomal 30S subunit. Inhibit initiation of peptide synthesis and cause misreading of the genetic code. Streptomycin
Who should read this document 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version 3. Policy/Procedure/Guideline 3
 Antibiotic Prophylaxis in Cranial Neurosurgery Antibiotic Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Antibiotic Prophylaxis in Cranial Neurosurgery Antibiotic Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Pocket Guide to Diagnosis & Treatment of Vascular Graft Infections (VGI)
") Pocket Guide to Diagsis & Treatment of Vascular Graft Infections (VGI) DEFINITION Investigation /sign Local signs of infection Histopathology Microbiology Definitive Criteria Purulent wound secretion sinus
Pocket Guide to Diagsis & Treatment of Vascular Graft Infections (VGI) DEFINITION Investigation /sign Local signs of infection Histopathology Microbiology Definitive Criteria Purulent wound secretion sinus
American Association of Feline Practitioners American Animal Hospital Association
 American Association of Feline Practitioners American Animal Hospital Association Basic Guidelines of Judicious Therapeutic Use of Antimicrobials August 1, 2006 Introduction The Basic Guidelines to Judicious
American Association of Feline Practitioners American Animal Hospital Association Basic Guidelines of Judicious Therapeutic Use of Antimicrobials August 1, 2006 Introduction The Basic Guidelines to Judicious
Cefuroxime 1.5gm IV and Metronidazole 500mg IV. Metronidazole 500mg IV/Ampicillin-sulbactam e 3g/Ceftriaxone 2gm. +Metronidazole 500mg/Ertapenem 1gm
 SURGICAL ANTIBIOTIC PROPHYLAXIS GENERAL SURGERY* PROCEDURE RECOMMENDED AGENTS a,b Clean None None ALTERNATIVE AGENTS (If allergic to penicillin or colonized/infected with MRSA at any site) Clean with potential
SURGICAL ANTIBIOTIC PROPHYLAXIS GENERAL SURGERY* PROCEDURE RECOMMENDED AGENTS a,b Clean None None ALTERNATIVE AGENTS (If allergic to penicillin or colonized/infected with MRSA at any site) Clean with potential
03/09/2014. Infection Prevention and Control A Foundation Course. Talk outline
 Infection Prevention and Control A Foundation Course 2014 What is healthcare-associated infection (HCAI), antimicrobial resistance (AMR) and multi-drug resistant organisms (MDROs)? Why we should be worried?
Infection Prevention and Control A Foundation Course 2014 What is healthcare-associated infection (HCAI), antimicrobial resistance (AMR) and multi-drug resistant organisms (MDROs)? Why we should be worried?
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
ORIGINAL ARTICLES. Appropriate Use of the Carbapenems. 1. Introduction. 2. Ertapenem (group 1) 2.1 Appropriate use POSITION STATEMENT
 2.1 Appropriate use POSITION STATEMENT") POSITION STATEMENT Appropriate Use of the Carbapenems AJBrink, C Feldman, D C Grolman, D Muckart, J Pretorius, G A Richards, M Senekal, W Sieling The carbapenems are a group of broad-spectrum betalactam
POSITION STATEMENT Appropriate Use of the Carbapenems AJBrink, C Feldman, D C Grolman, D Muckart, J Pretorius, G A Richards, M Senekal, W Sieling The carbapenems are a group of broad-spectrum betalactam
Provincial Drugs & Therapeutics Committee Memorandum Version 2
 Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults
 Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
Multi-Drug Resistant Organisms (MDRO)
") Multi-Drug Resistant Organisms (MDRO) 2016 What are MDROs? Multi-drug resistant organisms, or MDROs, are bacteria resistant to current antibiotic therapy and therefore difficult to treat. MDROs can cause
Multi-Drug Resistant Organisms (MDRO) 2016 What are MDROs? Multi-drug resistant organisms, or MDROs, are bacteria resistant to current antibiotic therapy and therefore difficult to treat. MDROs can cause
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
PHAMACOLOGY 2 nd EXAM QUESTIONS 2012/2013
 PHAMACOLOGY 2 nd EXAM QUESTIONS 2012/2013 1.from the pharmacological point of view, which of the following intervention is correct? a) treating postpartum non-obstructive urinary retention by intramuscular
PHAMACOLOGY 2 nd EXAM QUESTIONS 2012/2013 1.from the pharmacological point of view, which of the following intervention is correct? a) treating postpartum non-obstructive urinary retention by intramuscular
Scottish Surveillance of Healthcare Infection Programme (SSHAIP) Health Protection Scotland SSI Surveillance Protocol 7th Edition 2017 Question &
 Health Protection Scotland SSI Surveillance Protocol 7th Edition 2017 Question &") Contents General... 4 Pre-op... 4 Peri-op... 5 Post-op... 8 Caesarean Section... 12 Orthopaedics... 14 Large Bowel:... 15 Vascular... 17 General Pre-op Q: If a patient is an emergency admission is the
Contents General... 4 Pre-op... 4 Peri-op... 5 Post-op... 8 Caesarean Section... 12 Orthopaedics... 14 Large Bowel:... 15 Vascular... 17 General Pre-op Q: If a patient is an emergency admission is the
Guidelines for the Medical management of Diabetic Foot Infection
 Guidelines for the Medical management of Diabetic Foot Infection Introduction and summary points - Foot infections in diabetic patients usually begin with skin ulceration - However, skin wounds with no
Guidelines for the Medical management of Diabetic Foot Infection Introduction and summary points - Foot infections in diabetic patients usually begin with skin ulceration - However, skin wounds with no
3/20/2011. Code 215 of Hammurabi: If a physician performed a major operation on
 The Good Antibiotics: the Good, the Bad and the Ugly John P. Cello, MD Professor of Medicine and Surgery, University of California, San Francisco Most organisms can be readily identified by culture, special
The Good Antibiotics: the Good, the Bad and the Ugly John P. Cello, MD Professor of Medicine and Surgery, University of California, San Francisco Most organisms can be readily identified by culture, special
Community-Associated C. difficile Infection: Think Outside the Hospital. Maria Bye, MPH Epidemiologist May 1, 2018
 Community-Associated C. difficile Infection: Think Outside the Hospital Maria Bye, MPH Epidemiologist Maria.Bye@state.mn.us 651-201-4085 May 1, 2018 Clostridium difficile Clostridium difficile Clostridium
Community-Associated C. difficile Infection: Think Outside the Hospital Maria Bye, MPH Epidemiologist Maria.Bye@state.mn.us 651-201-4085 May 1, 2018 Clostridium difficile Clostridium difficile Clostridium
مادة االدوية المرحلة الثالثة م. غدير حاتم محمد
 م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
NHS Dumfries And Galloway. Surgical Prophylaxis Guidelines
 NHS Dumfries And Galloway Surgical Prophylaxis Guidelines The aim of surgical prophylaxis is to reduce rates of surgical site and health-care associated infections and so reduce surgical morbidity and
NHS Dumfries And Galloway Surgical Prophylaxis Guidelines The aim of surgical prophylaxis is to reduce rates of surgical site and health-care associated infections and so reduce surgical morbidity and
Diagnosis: Presenting signs and Symptoms include:
 PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
PERITONITIS TREATMENT PROTOCOL CARI - Caring for Australasians with Renal Impairment - CARI Guidelines complete list ISPD Guidelines: http://www.ispd.org/lang-en/treatmentguidelines/guidelines Objective
Invasive Group A Streptococcus (GAS)
") Invasive Group A Streptococcus (GAS) Cause caused by a bacterium commonly found on the skin and in the throat transmitted by direct, indirect or droplet contact with secretions from the nose, and throat
Invasive Group A Streptococcus (GAS) Cause caused by a bacterium commonly found on the skin and in the throat transmitted by direct, indirect or droplet contact with secretions from the nose, and throat
Dr. NAFRIALDI, PhD, SpPD, SpFK
 Dr. NAFRIALDI, PhD, SpPD, SpFK Lahir: Bukittinggi, 30 Oktober 1961. Pendidikan Dokter Umum: FKUI, 1986 S2 Farmakologi: Universite Claude Bernard, Lyon, Perancis, 1991 S3 Farmakologi: Universite Montpellier,
Dr. NAFRIALDI, PhD, SpPD, SpFK Lahir: Bukittinggi, 30 Oktober 1961. Pendidikan Dokter Umum: FKUI, 1986 S2 Farmakologi: Universite Claude Bernard, Lyon, Perancis, 1991 S3 Farmakologi: Universite Montpellier,
Gastric Dilatation-Volvulus
 Gastric Dilatation-Volvulus The term "ACVS Diplomate" refers to a veterinarian who has been board certified in veterinary surgery. Only veterinarians who have successfully completed the certification requirements
Gastric Dilatation-Volvulus The term "ACVS Diplomate" refers to a veterinarian who has been board certified in veterinary surgery. Only veterinarians who have successfully completed the certification requirements
Replaces:04/14/16. Formulated: 1997 SKIN AND SOFT TISSUE INFECTION
 Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
Effective Date: 04/13/17 Replaces:04/14/16 Page 1 of 7 POLICY To standardize the clinical management and housing of offenders with skin and soft tissue infections, thereby reducing the transmission and
NEONATAL Point Prevalence Survey. Ward Form
 Appendix 2 NEONATAL Point Prevalence Survey Ward Form Please fill in one form for each ward included in PPS Date of survey Person completing form (Auditor code) Hospital Name Department/Ward Neonatal departments
Appendix 2 NEONATAL Point Prevalence Survey Ward Form Please fill in one form for each ward included in PPS Date of survey Person completing form (Auditor code) Hospital Name Department/Ward Neonatal departments
Developed by Kathy Wonderly RN, MSEd,CPHQ Developed: October 2009 Most recently updated: December 2014
 Developed by Kathy Wonderly RN, MSEd,CPHQ Developed: October 2009 Most recently updated: December 2014 The Center for Medicare and Medicaid (CMS) is moving away from collecting data on the process of care
Developed by Kathy Wonderly RN, MSEd,CPHQ Developed: October 2009 Most recently updated: December 2014 The Center for Medicare and Medicaid (CMS) is moving away from collecting data on the process of care
SOFT Movement Survey of FMT Programs
 Appendix 1 (as supplied by the authors): Survey SOFT Movement Survey of FMT Programs Part 1: General Information about your Fecal Microbiota Transplant (FMT) Program 1) Please fill out the information
Appendix 1 (as supplied by the authors): Survey SOFT Movement Survey of FMT Programs Part 1: General Information about your Fecal Microbiota Transplant (FMT) Program 1) Please fill out the information
Tubo-ovarian abscess in OPAT
 Tubo-ovarian abscess in OPAT James Hatcher Consultant in Infectious Diseases and Medical Microbiology OUTLINE What is a tubo-ovarian abscess Current recommendations Our experience and challenges How to
Tubo-ovarian abscess in OPAT James Hatcher Consultant in Infectious Diseases and Medical Microbiology OUTLINE What is a tubo-ovarian abscess Current recommendations Our experience and challenges How to
Treatment of peritonitis in patients receiving peritoneal dialysis Antibiotic Guidelines. Contents
 Treatment of peritonitis in patients receiving Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Jude Allen (Pharmacist) Additional author(s): Dr David Lewis, Dr Dimitrios Poulikakos,
Treatment of peritonitis in patients receiving Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Jude Allen (Pharmacist) Additional author(s): Dr David Lewis, Dr Dimitrios Poulikakos,