Healthcare Associated Infections. Stephanie M. Podolski, MPH, MSPA, PA-C Hospitalist PA Maine General Medical Center
|
|
|
- Mae Clarke
- 5 years ago
- Views:
Transcription
1 Healthcare Associated Infections Stephanie M. Podolski, MPH, MSPA, PA-C Hospitalist PA Maine General Medical Center

2
3 Disclosures No financial or business related disclosures to report
4 Overview Pneumonia (HAP and VAP) Gastrointestinal Illness Urinary Tract Infections Primary Bloodstream Infections Surgical site infections (inpatient surgery) Line infections (PICC, Midline or Central Line Associated Infections) Antibiotic Resistant Infections
5 Healthcare-Associated Infections (HAIs) Infections acquired while patient s receive medical treatment in a health care facility Threat to patient safety Often preventable Surveillance and data collections through the National Healthcare Safety Network and the Emerging Infections Program
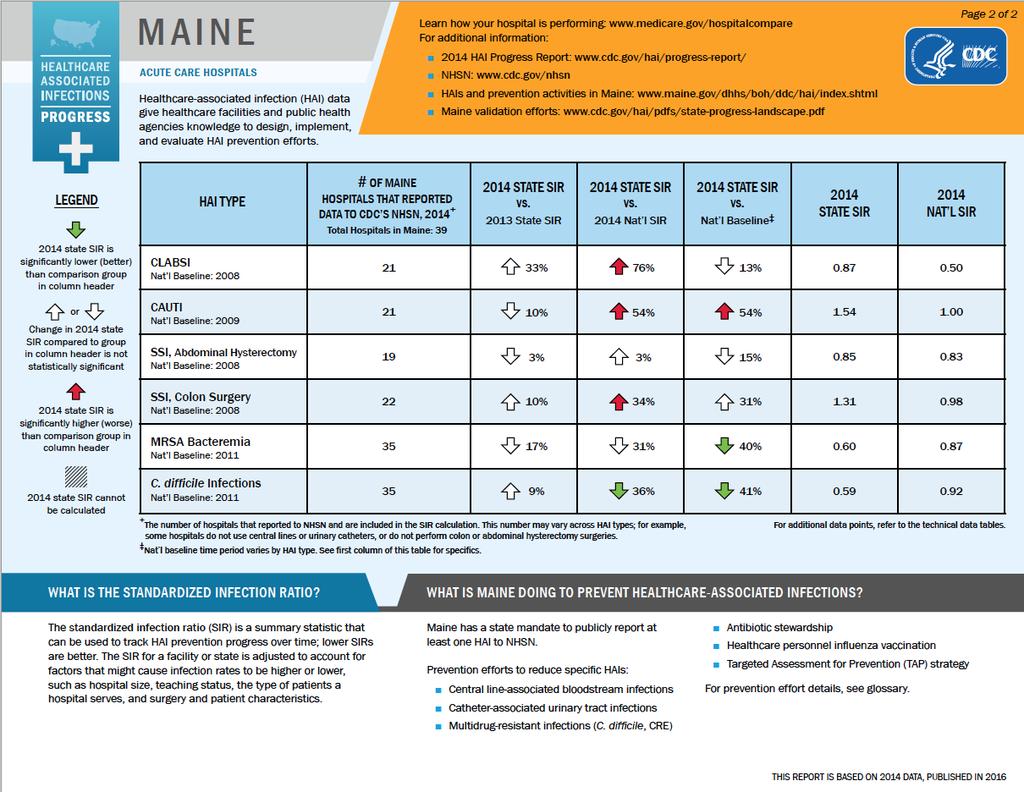
6 Healthcare-Associated Infections (HAIs) 1 in 25 hospitalized patients will acquire a healthcare-associated infection each day The CDC s annual National and State Healthcare-Associated Infections Progress Report found: 50% decrease in central line-associated blood stream infections between 2008 and 2014 No change in the rate of catheter-associated UTIs between 2009 and % decrease in surgical site infections in specifically tracked procedures 8% decrease in hospital onset C. difficile infections between 2011 and % decrease in hospital onset MRSA bacteremia between 2011 and 2014
7 Types of Infections
8 Central Line Associated Blood Stream Infections (CLABSIs) Central line is a catheter that is placed in a large major vein in the neck, chest (often close to groin) or groin Strict protocol for insertion, followed by strict infection control prevention practices Provide patient with education regarding proper maintenance and monitoring Remove central line as soon as no longer needed CLABSI: when bacteria or viruses enter the bloodstream through the central line Results in thousands of deaths per year Adds billions of dollars in added U.S. healthcare costs Entirely preventable
9 Surgical Site Infection (SSI) SSI: an infection that occurs in the part of the body where the surgery took place Superficial involving skin only Tissues under the skin, organs or implanted material Symptoms: redness, pain, fever, chills, purulent drainage Treatment: Antibiotics usually start broad spectrum and tailor toward appropriate organism based on culture
10 SSI Prevention Patient education Medical providers, nurses, and staff must follow CDC surgical infection prevention guidelines Clean hands and arms up to elbows with antiseptic prior to surgery Clean hands with soap and water or alcohol based hand rub before and after caring for each patient. Shave patient as indicated (area where procedure will occur) Wear hair covers, masks, gowns, and gloves during surgery and maintain sterile technique When indicated, give antibiotics 60 minutes pre-op and stop within 24 hours post-op Use appropriate antiseptic on skin prior to operation
11 Catheter Associated UTI (CAUTI) UTI: infection related to urethra, bladder, ureters or kidneys. HA UTI: Approximately 75% are associated with a urinary catheter (15-20% of patients have catheters during hospitalization) CAUTI: infection related to use of urinary catheter. prolonged use is highest risk factor Should only be used for appropriate clinical indications

12 CDC Guidelines: Appropriate Use

13 CDC Guidelines: Inappropriate Use

14 CDC: Alternative Recommendations
15 CAUTI Prevention Is Key Ensure Proper Urinary Catheter Placement Techniques with Nursing Staff Ensure Proper Urinary Catheter Maintenance Techniques and Protocols are Followed Know if your hospital has a Quality Improvement Program PAs need to continue surveillance and monitoring inpatient and outpatient Long term catheters change every 30 days Consider Urology Involvement
16 Pneumonia: Definitions Health Care Associated Pneumonia (HCAP) Hospitalized within 90 days of infection Reside in nursing home or long term care facility Received parenteral antimicrobial therapy, chemotherapy or wound care within 30 days Ventilator Acquired Pneumonia (VAP): pneumonia during mechanical ventilation or sustained immediately after Community Acquire Pneumonia No contact to medical institutions. Common organisms S. Pneumonia, H. influenza, M. catarrhalis Less common atypical bacteria (Chlamydia pneumonia, Mycoplasma pneumonia, Legionella)
17 Pneumonia in Hospitalized Patients Community Acquired Pneumonia (CAP) Usual treatment is macrolide and cephalosporin. If risk for pseudomonas or aspiration, then consider Fluoroquinolone or broad spectrum antibiotic, such as Zosyn. CURB-65 score is a Pneumonia Severity Score» Confusion» BUN >19 mg/dl» Respiratory Rate >30» Systolic BP 90 or Diastolic BP 60» Age 65 For severe pneumonia (CURB-65 score >=3), steroid (oral) could improve mortality, reduce risk for ARDS, shorten length of stay. Routine coverage for atypical pneumonia is probably not necessary Duration of therapy for CAP 5-7 days are adequate for mild to moderate cases.
18 Pneumonia in Hospitalized Patients HCAP (Health Care Associated Pneumonia) term used to include VAP and HAP. Concept of "HCAP" is removed by 2016 Clinical Practice Guidelines by the Infectious Disease Society of America and the American Thoracic Society because Most patients with HCAP do not have antibiotic resistant pathogens Broad spectrum prescribing should be based on a narrow set of risk factors that better predict the presence of resistant pathogens HAP (hospital acquired pneumonia) and VAP (ventilator-associated pneumonia) are still treated with broader spectrum antibiotic than CAP.
19 Ventilator Associated Pneumonia (VAP) VAP: lung infection that develops in a person who is on a ventilator by means of tracheostomy or endotracheal tube (intubation) Treatment: Broad spectrum IV antibiotics Prevention while in the hospital Elevate head of bed degrees unless other medical conditions prevent this Monitor patient s ability to breathe on their own daily Proper hand hygiene from staff and family/friends Adequate oral hygiene
20 Pneumonia follow-up If the patient has COPD, re-order PFT s after completion of antibiotic and steroid course Always reassess for possibility of aspiration or other risk factors, immunosuppression, environmental factors, etc. Ensure that the patient has had PCV13 and PPSV23 May require outpatient Pulmonary consult
21 Clostridium Difficile Colitis Clostridium difficile is a spore forming, Gram positive anaerobic bacillus that produces two exotoxins (A and B) Accounts for 15-25% of antibiotic associated diarrhea Fluoroquinolones, penicillins, cephalosporins, clindamycin Doxycycline has the smallest risk PPIs increase the risk of C.diff by 65% First line treatment: Oral vancomycin (125 mg QID) for days OR metronidazole 500 mg TID for days Probiotics while on antibiotics
22 Clostridium Difficile Colitis Diseases resulting from C. Difficile: Pseudomembranous colitis Toxic megacolin Perforations of the colon Sepsis Death (rarely)
23 Bacteremia Bacteremia describes the presence of viable bacteria in the blood. Two Types: Transient or sustained bacteremia. Transient: usually 2 10 minutes. Common e.g. after toothbrushing, various procedures, such as organ biopsies. Sustained: a bacteremia lasting over minutes and often days to weeks. **Important to find source of Bacteremia
24 How does bacteremia occur? Bacteria enter the circulatory and lymphatic systems through acute infections or breaches of the skin barrier or mucosa. Breaches occur common means teeth brushing, insect bites or small wounds Usually our immune system will prevent microscopic bacteremia below threshold of detection Once threshold is broken, bacteremia can lead to septicemia with dangerous complications such as toxemia, sepsis, and septic shock. FUN FACT: Once symptomatic, the immune response to the infection results in the clinical signs and symptoms rather than exposure to the microbes themselves.
25 Bacteremia KEY POINT: In the patient with bacteremia, it is important to determine if the patient has transient vs. sustained bacteremia. How do you do this? Can you tell if a patient has bacteremia by Hx and P.E.?
26 Blood Cultures Blood Culture Rule of Thumb: In suspected bacteremic patients, obtain at least two blood cultures BEFORE any Antibiotics! Collection of samples can be done back to back. The previous common practice of separating each culture by minutes can increase time to antibiotic administration. Make sure skin prep and procedure in which blood cultures are drawn is accurate in order to avoid contamination (RN or Lab) Positive blood cultures: R/o skin contaminants Remember staph coagulase (-) and (+) are commonly on the skin Define etiology and Identify pathogens Two or more spaced blood cultures allow the determination of transient vs. sustained bacteremia. Sustained bacteremias are more worrisome. Allow for bacterial susceptibilities to Antibiotics to be done. Goal will be to narrow the spectrum of antibiotic treatment ASAP
27 Organisms Involved in HAIs Actinetobacter Burkholderia cepacia Clostridium difficile Clostridium Sordellii Carbapenem-resistant Enterobacteriaceae (CRE Gram-negative Bacteria Hepatitis HIV Klebsiella MRSA Mycobacterium acscessus Norovirus Pseudomonas aeruginosa Staphylococcus aureus Tuberculosis VISA/VRSA Vancomycin-resistant Enterococci (VRE)

28 HAI Progress Report
29
30 Why Do We Care? Often times HAI require broad spectrum antibiotic treatment, and if provided to patients over an extended period of time, then this can increase population resistance. Important note: Know your states antibiotic resistance by population we want to be stewards of appropriate antibiotic prescribing.
31 CDC Antibiotic Resistance Patient Safety Atlas Data collected from U.S. Healthcare facilities that reported at least one HAI to CDC NHSN Dates collected: , with updates in 12/2015 Reported events; CLABSI, CAUTI, and SSI Reported pathogens: MRSA Carbapenem-resistant Enterobacteriaceae (CRE) Multidrug-resistance Pseudomonas aeruginosa

32 National Average for Antibiotic Resistance?

33 New England Antibiotic Resistance by State
34
35 Preventing HAIs Targeted Assessment for Prevention (protocols and proper procedures for nursing and medical provider insertion and maintenance of catheters, etc.) Infection Control and Prevention Plans Patient Information Packets Outpatient follow-up care guides
36 Systemic Inflammatory Response Syndrome (SIRS) and Sepsis
37 SIRS Systemic Inflammatory Response Syndrome (SIRS) SIRS is an appropriate response to infection or any other stimulus that activates physiological inflammatory response. New Data from New England Journal suggests we stop screening people for SIRS There is potential that every hospitalized person will meet SIRS criteria at least once during a hospital stay
38 History of SIRS Systemic inflammatory response system (SIRS) has been a term used clinically for more than 20 years. SIRS is considered present when two of more of the acute findings of tachycardia, leukocytosis or leukopenia, fever or hypothermia or tachypnea (elevated respiratory rate) were present If a source of infection was found and documented and SIRS criteria was indeed met, then patients were said to have sepsis. PROBLEM: Sepsis became a commonly used clinical term. After reassessing this concept, in 2012, a consensus of experts concluded that SIRS was a potentially misleading term and this nomenclature was discarded. The 2012 consensus group defined sepsis as a systemic, deleterious host response to infection leading to severe sepsis (acute organ dysfunction secondary to documented or suspected infection) and septic shock (severe sepsis plus hypotension not reversed by fluid resuscitation). The term septic patient was still embraced by the 2012 consensus group but a more fluid definition was acceptable. Then the Sepsis 2015 Guidelines came Along and everything changed
39 Sepsis Redefinition Sepsis is not simply infection + two or more SIRS criteria Why was it changed? Too many variables Definition for severe sepsis is confusing 4 different ways to classify sepsis in the U.S. Different criteria caused different mortality measurements Mortality for Septic Shock United States % Australia 22% Germany 60.5% The Netherlands 60%
40 Sepsis New Definition Sepsis is life threatening organ dysfunction caused by a dysregulated host response to infection
41 Septic Shock Septic shock is a subset of sepsis in which profound circulatory, cellular and metabolic abnormalities are associated with a greater risk of mortality than with sepsis alone. Definition of sepsis with: Cellular/metabolic abnormalities lactate elevation High risk for mortality
42 Sepsis and Septic Shock Pathophysiology At low concentrations, pro-inflammatory cytokines such as interleukin 1 (IL-1) and tumor necrosis factor-α (TNF-α) play important roles in the host s immune defenses. Large circulating amounts of pro-inflammatory cytokines can result in a life threatening immune response. IL-1 induces vasodilation (widening of blood vessels) and reduces the tight junctions between vascular endothelial cells, leading to widespread edema. As fluids move out of circulation into tissues, blood pressure begins to drop (hypotension). Without proper monitoring, the blood pressure can fall below the level necessary to maintain proper kidney and respiratory functions leading to septic shock. Also note: excessive release of cytokines during the inflammatory response can lead to the formation of blood clots. Hypotension and blood clot formation can lead to multiple organ failure and death.
43 Sequential Organ Failure Assessment (SOFA) A score, used primarily in the ICU, of 2 points or more is associated with an in-hospital mortality of greater than 10%. Septic shock is a subset of sepsis Clinically identified as having vasopressor requirement to maintain a mean arterial pressure (MAP) of 65 mmhg or greater and serum lactate level greater than 2 mml/l in the absence of hypovolemia. Associated with hospital mortality rates of 40%
44 Quick SOFA (qsofa) To be used to identify patients showing signs of possible sepsis Screening tool used in acute care setting Must have two of the following: Respiratory rate of 22/min or greater Altered mentation Systolic BP 100 mmhg or less
45 What causes sepsis? Bacteria are the most common pathogens associated with the development of sepsis, and septic shock. gram-positive and gram-negative pathogens The most common infection associated with sepsis is bacterial pneumonia, accounting for about half of all cases, followed by intra-abdominal infections and urinary tract infections. Additional sources for bacterial infections: superficial wounds surgical wounds animal bites indwelling catheters (urinary, central lines, PICC/mid-lines, dialysis, etc.) NOTE: fungus and viruses can also cause Sepsis
46 Case Study #1 35 year old paraplegic female with history of Type 1 Diabetes, ESRD, neurogenic bladder with chronic indwelling Foley Catheter, chronic wheel chair bound status, chronic ischial decubitis ulcers (followed by wound care) and immobility who presented to the hospital with diarrhea, flank pain, elevated blood sugars, fever, chills, fatigue, worsening wounds Vital Signs: Temp BP 89/53, HR 111 RR 20, SPO2 98% on RA Labs: WBC 22,000 hemoglobin 12.8, hematocrit 30, platelets 235. UC: growing Gram negative rod Lactic acid: 3.1 Bilateral ischial decubitis wounds, (status post surgery and recent surgical debridement): necrotic appearing borders with foul smelling discharge
47 Case Study #1 What type of infection(s) are you worried about in this patient scenario? What other labs or tests do you want? Who should we consult?
48 Diagnoses 1. Recurrent catheter associated urinary tract infection (UTI) with UC growing Enterobacter cloacae, pseudomonas 2 morphotypes. 2. Bilateral chronic ischial decubitus ulcer/osteomyelitis. Repeat wound cultures showing polymicrobial infection. Primary culture growing at this point in time Streptococcus viridans and enterococcus species, additional mixed pathogens. 3. Sepsis, multifactorial secondary to CAUTI and infected ischial decubitus ulcer with underlying osteomyelitis currently on vacuumassisted closure (VAC) therapy. 4. Clostridium difficile colitis treated and resolved.
49 Case Study #2 72 year old male with a history of bronchiectasis and severe pulmonary fibrosis. History of acute hypoxic respiratory failure in June 2017, requiring intubation and ventilator support. Identified to have pneumonia post initiation of ventilator while hospitalized. Stabilized and then extubated.
50 Case Study #2 What type of infection(s) are you worried about in this patient scenario? What labs and tests do you want? Who do you want to consult?
51 Case Study #2 Sputum culture collected post extubation in June 2017 growing Mycobacterium Avium Complex and Pseudomonas Aeruginosa (initially only resistant to Cipro) Treated with IV Cefepime per ID In August 2017 Repeat Sputum Culture performed showing Pseudomonas pneumonia persists and now organism is resistant to Cipro and Cefepime Treatment changed to Zosyn and meropenem per ID In September 2017 Repeat Sputum Culture performed showing Pseudomonas infection continues and now organism is PAN RESISTANT Started on IV Zerbaxa (ceftolozane/tazobactam), eventually transitioned to IV Colistin per ID Patient died suddenly one morning without warning at the end of September (with some signs of clinical stability and improvement)
52 Case Study #3 67 year old male presented to the ER with chief complaint of SOB. He has a history of COPD, not O2 or steroid dependent, previous pneumonia, hypertension, and hyperlipidemia. Patient is encephalopathic. Vital Signs: Temp HR 101, RR 24, SPO2 82% on room air BP: 136/82 Lactic Acid level 2.1 Daughter found him confused at home and called
53 Case Study #3 What criteria does he meet at time of admission? What other information do you want?
54 Case Study #3 CXR: Right lower lobe pneumonia WBC: 20,000 H and H stable Platelet Count stable BUN 20, Cr 1.4 (baseline is usually normal for him) Given a Albuterol Neb in ER and started on oxygen via nasal cannula, SPO2 now 90. ABG not done Sputum culture pending Blood cultures are growing strep pneumoniae Repeat Labs in morning pending UC is pending.
55 Case Study #3 Diagnosis Sepsis, present on admission, secondary to Right lower lobe pneumonia Strep pneumonia bacteremia, secondary to above Acute on chronic hypoxic respiratory failure Acute on chronic COPD exacerbation Acute Kidney Injury Treatment Admit to Hospital IV azithromycin and IV ceftriaxone, q6 hour nebulizers (changed to DuoNebs), lite IV fluid hydration, oxygen to maintain SPO2 above 92% Monitor oxygen needs and ensure he has 48 hours IV antibiotics without fever before switching to oral
56 Resources f_faqs_hcp.html

57 Questions??
Meropenem for all? Midge Asogan ICU Fellow (also ID AT)
") Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Infection Prevention Highlights for the Medical Staff. Pamela Rohrbach MSN, RN, CIC Director of Infection Prevention
 Highlights for the Medical Staff Pamela Rohrbach MSN, RN, CIC Director of Infection Prevention Standard Precautions every patient every time a. Hand Hygiene b. Use of Personal Protective Equipment (PPE)
Highlights for the Medical Staff Pamela Rohrbach MSN, RN, CIC Director of Infection Prevention Standard Precautions every patient every time a. Hand Hygiene b. Use of Personal Protective Equipment (PPE)
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Antibiotic stewardship in long term care
 Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Preventing Multi-Drug Resistant Organism (MDRO) Infections. For National Patient Safety Goal
 Infections. For National Patient Safety Goal") Preventing Multi-Drug Resistant Organism (MDRO) Infections For National Patient Safety Goal 07.03.01 2009 Methicillin Resistant Staphlococcus aureus (MRSA) About 3-8% of the population at large is a carrier
Preventing Multi-Drug Resistant Organism (MDRO) Infections For National Patient Safety Goal 07.03.01 2009 Methicillin Resistant Staphlococcus aureus (MRSA) About 3-8% of the population at large is a carrier
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Healthcare-associated Infections Annual Report December 2018
 December 2018 Healthcare-associated Infections Annual Report 2011-2017 TABLE OF CONTENTS INTRODUCTION... 1 METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS INFECTIONS... 2 MRSA SURVEILLANCE... 3 CLOSTRIDIUM
December 2018 Healthcare-associated Infections Annual Report 2011-2017 TABLE OF CONTENTS INTRODUCTION... 1 METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS INFECTIONS... 2 MRSA SURVEILLANCE... 3 CLOSTRIDIUM
03/09/2014. Infection Prevention and Control A Foundation Course. Talk outline
 Infection Prevention and Control A Foundation Course 2014 What is healthcare-associated infection (HCAI), antimicrobial resistance (AMR) and multi-drug resistant organisms (MDROs)? Why we should be worried?
Infection Prevention and Control A Foundation Course 2014 What is healthcare-associated infection (HCAI), antimicrobial resistance (AMR) and multi-drug resistant organisms (MDROs)? Why we should be worried?
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Multi-Drug Resistant Organisms (MDRO)
") Multi-Drug Resistant Organisms (MDRO) 2016 What are MDROs? Multi-drug resistant organisms, or MDROs, are bacteria resistant to current antibiotic therapy and therefore difficult to treat. MDROs can cause
Multi-Drug Resistant Organisms (MDRO) 2016 What are MDROs? Multi-drug resistant organisms, or MDROs, are bacteria resistant to current antibiotic therapy and therefore difficult to treat. MDROs can cause
Welcome! 10/26/2015 1
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Treatment of septic peritonitis
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship
 Curriculum for Antimicrobial Stewardship") General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
General Surgery Small Group Activity (Facilitator Notes) Curriculum for Antimicrobial Stewardship Facilitator instructions: Read through the facilitator notes and make note of discussion points for each
Hospital Acquired Infections in the Era of Antimicrobial Resistance
 Hospital Acquired Infections in the Era of Antimicrobial Resistance Datuk Dr Christopher KC Lee Infectious Diseases Unit Department of Medicine Sungai Buloh Hospital Patient Story 23 Year old female admitted
Hospital Acquired Infections in the Era of Antimicrobial Resistance Datuk Dr Christopher KC Lee Infectious Diseases Unit Department of Medicine Sungai Buloh Hospital Patient Story 23 Year old female admitted
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Community-Associated C. difficile Infection: Think Outside the Hospital. Maria Bye, MPH Epidemiologist May 1, 2018
 Community-Associated C. difficile Infection: Think Outside the Hospital Maria Bye, MPH Epidemiologist Maria.Bye@state.mn.us 651-201-4085 May 1, 2018 Clostridium difficile Clostridium difficile Clostridium
Community-Associated C. difficile Infection: Think Outside the Hospital Maria Bye, MPH Epidemiologist Maria.Bye@state.mn.us 651-201-4085 May 1, 2018 Clostridium difficile Clostridium difficile Clostridium
Dr. Shaiful Azam Sazzad. MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College
 Critical Care Medicine Dhaka Medical College") Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Objectives. Basic Microbiology. Patient related. Environment related. Organism related 10/12/2017
 Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
What bugs are keeping YOU up at night?
 What bugs are keeping YOU up at night? Barbara DeBaun, RN, MSN, CIC 26 th Annual Medical Surgical Nursing Conference South San Francisco, CA April 15, 2016 Objectives Describe the top three infectious
What bugs are keeping YOU up at night? Barbara DeBaun, RN, MSN, CIC 26 th Annual Medical Surgical Nursing Conference South San Francisco, CA April 15, 2016 Objectives Describe the top three infectious
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Hand washing/hand hygiene reduces the number of microorganisms on the hands and is the most important practice to prevent the spread of infection.
 1. Hand Hygiene Quick Reference Chart Hand washing/hand hygiene reduces the number of microorganisms on the hands and is the most important practice to prevent the spread of infection. WHEN Before: Direct
1. Hand Hygiene Quick Reference Chart Hand washing/hand hygiene reduces the number of microorganisms on the hands and is the most important practice to prevent the spread of infection. WHEN Before: Direct
What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa.
 Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
Pneumonia What is pneumonia? Infection of the lung parenchyma Causative agents include bacteria, viruses, fungi, protozoa www.netmedicine.com/xray/xr.htm Definition acute infectious disease, etiology usually
Running head: CLOSTRIDIUM DIFFICILE 1
 Running head: CLOSTRIDIUM DIFFICILE 1 Clostridium difficile Infection Christy Lee Fenton Mountainland Applied Technology College CLOSTRIDIUM DIFFICILE 2 Clostridium difficile Infection Approximately 200,000
Running head: CLOSTRIDIUM DIFFICILE 1 Clostridium difficile Infection Christy Lee Fenton Mountainland Applied Technology College CLOSTRIDIUM DIFFICILE 2 Clostridium difficile Infection Approximately 200,000
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Antimicrobial Prophylaxis in the Surgical Patient. M. J. Osgood
 Antimicrobial Prophylaxis in the Surgical Patient M. J. Osgood Outline Definitions surgical site infection (SSI) Risk factors Wound classification Microbiology of SSIs Strategies for prevention of SSIs
Antimicrobial Prophylaxis in the Surgical Patient M. J. Osgood Outline Definitions surgical site infection (SSI) Risk factors Wound classification Microbiology of SSIs Strategies for prevention of SSIs
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC
 Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings. Carlos Reyes Sacin, MD, AAHIVS
 Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
1/30/ Division of Disease Control and Health Protection. Division of Disease Control and Health Protection
 Surveillance, Outbreaks, and Reportable Diseases, Oh My! Assisted Living Facility, Nursing Home and Surveyor Infection Prevention Training February 2015 A.C. Burke, MA, CIC Health Care-Associated Infection
Surveillance, Outbreaks, and Reportable Diseases, Oh My! Assisted Living Facility, Nursing Home and Surveyor Infection Prevention Training February 2015 A.C. Burke, MA, CIC Health Care-Associated Infection
Conflict of interest: We have no conflict of interest to report on this topic of SSI reduction for total knees.
 Reducing SSI- Knees TIFFANY KENNERK MBA, MSN, RN, NE -BC, ONC CYNTHIA SEAMAN BSN, RN, ONC, CMSRN ~COMMUNITY HOSPITALS AND WELLNESS CENTERS~ Conflict of interest: We have no conflict of interest to report
Reducing SSI- Knees TIFFANY KENNERK MBA, MSN, RN, NE -BC, ONC CYNTHIA SEAMAN BSN, RN, ONC, CMSRN ~COMMUNITY HOSPITALS AND WELLNESS CENTERS~ Conflict of interest: We have no conflict of interest to report
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Let me clear my throat: empiric antibiotics in
 Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
8/17/2016 ABOUT US REDUCTION OF CLOSTRIDIUM DIFFICILE THROUGH THE USE OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM
 Mary Moore, MS CIC MT (ASCP) Infection Prevention Coordinator Great River Medical Center, West Burlington REDUCTION OF CLOSTRIDIUM DIFFICILE THROUGH THE USE OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM ABOUT
Mary Moore, MS CIC MT (ASCP) Infection Prevention Coordinator Great River Medical Center, West Burlington REDUCTION OF CLOSTRIDIUM DIFFICILE THROUGH THE USE OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM ABOUT
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings?
 An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
CLINICAL PROTOCOL FOR COMMUNITY ACQUIRED PNEUMONIA. SCOPE: Western Australia. CORB score equal or above 1. All criteria must be met:
 CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Antimicrobial Stewardship in Ambulatory Care
 Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Bad Bugs. Pharmacist Learning Objectives. Antimicrobial Resistance. Patient Case. Pharmacy Technician Learning Objectives 4/8/2016
 Pharmacist Learning Objectives Antimicrobial Resistance Julie Giddens Pharm D, BCPS Infectious Disease Clinical Pharmacist OSF Saint Francis Medical Center Peoria, IL The speaker has no conflicts to disclose
Pharmacist Learning Objectives Antimicrobial Resistance Julie Giddens Pharm D, BCPS Infectious Disease Clinical Pharmacist OSF Saint Francis Medical Center Peoria, IL The speaker has no conflicts to disclose
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Surveillance of Multi-Drug Resistant Organisms
 Surveillance of Multi-Drug Resistant Organisms Karen Hoffmann, RN, MS, CIC Associate Director Statewide Program for Infection Control and Epidemiology (SPICE) University of North Carolina School of Medicine
Surveillance of Multi-Drug Resistant Organisms Karen Hoffmann, RN, MS, CIC Associate Director Statewide Program for Infection Control and Epidemiology (SPICE) University of North Carolina School of Medicine
IDSA GUIDELINES COMMUNITY ACQUIRED PNEUMONIA
 page 1 / 5 page 2 / 5 idsa guidelines community acquired pdf IDSA/ATS Guidelines for CAP in Adults CID 2007:44 (Suppl 2) S29 such as blood and sputum cultures. Conversely, these cultures may have a major
page 1 / 5 page 2 / 5 idsa guidelines community acquired pdf IDSA/ATS Guidelines for CAP in Adults CID 2007:44 (Suppl 2) S29 such as blood and sputum cultures. Conversely, these cultures may have a major
9/30/2016. Dr. Janell Mayer, Pharm.D., CGP, BCPS Dr. Lindsey Votaw, Pharm.D., CGP, BCPS
 Dr. Janell Mayer, Pharm.D., CGP, BCPS Dr. Lindsey Votaw, Pharm.D., CGP, BCPS 1 2 Untoward Effects of Antibiotics Antibiotic resistance Adverse drug events (ADEs) Hypersensitivity/allergy Drug side effects
Dr. Janell Mayer, Pharm.D., CGP, BCPS Dr. Lindsey Votaw, Pharm.D., CGP, BCPS 1 2 Untoward Effects of Antibiotics Antibiotic resistance Adverse drug events (ADEs) Hypersensitivity/allergy Drug side effects
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
2010 ARO/CDI Prevalence Survey. MRSA [ ] VRE [ ] Clostridium difficile [ ]
![2010 ARO/CDI Prevalence Survey. MRSA [ ] VRE [ ] Clostridium difficile [ ]](/thumbs/89/98738029.jpg "2010 ARO/CDI Prevalence Survey. MRSA [ ] VRE [ ] Clostridium difficile [ ]") 2010 ARO/CDI Prevalence Survey 1) Patient identifier: 2) Hospital number: 3) Is the patient currently (day of survey) infected or colonized with (check all that apply): MRSA [ ] VRE [ ] Clostridium difficile
2010 ARO/CDI Prevalence Survey 1) Patient identifier: 2) Hospital number: 3) Is the patient currently (day of survey) infected or colonized with (check all that apply): MRSA [ ] VRE [ ] Clostridium difficile
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
11/22/2016. Hospital-acquired Infections Update Disclosures. Outline. No conflicts of interest to disclose. Hot topics:
 Hospital-acquired Infections Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Hospital-acquired Infections Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 1 Reviewing the organisms
 Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 1 Reviewing the organisms Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 1 Reviewing the organisms Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy
 biopsy") Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy Dr. Fidelma Fitzpatrick Consultant Microbiologist, Co-chair, NCCP Prostate Bx Infection Project Board Fidelma.fitzpatrick@hse.ie
Prevention & Management of Infection post Trans Rectal Ultrasound (TRUS) biopsy Dr. Fidelma Fitzpatrick Consultant Microbiologist, Co-chair, NCCP Prostate Bx Infection Project Board Fidelma.fitzpatrick@hse.ie
Provincial Drugs & Therapeutics Committee Memorandum Version 2
 Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults
 Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
Trea%ng Sepsis in 2016 Are the Big Guns Losing the War?
 Trea%ng Sepsis in 2016 Are the Big Guns Losing the War? ERIC HODGSON FCA (Crit Care) Inkosi Albert Luthuli Central Hospital & NELSON R MANDELA SCHOOL OF MEDICINE DURBAN, KZN Declaration Advisory boards
Trea%ng Sepsis in 2016 Are the Big Guns Losing the War? ERIC HODGSON FCA (Crit Care) Inkosi Albert Luthuli Central Hospital & NELSON R MANDELA SCHOOL OF MEDICINE DURBAN, KZN Declaration Advisory boards
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles
 Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them?
 Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them? Roberta B. Carey, PhD Centers for Disease Control and Prevention Division of Healthcare Quality Promotion Why worry? MDROs Clinical
Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them? Roberta B. Carey, PhD Centers for Disease Control and Prevention Division of Healthcare Quality Promotion Why worry? MDROs Clinical
Safety of an Out-Patient Intravenous Antibiotics Programme
 Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Antimicrobial Stewardship
 Antimicrobial Stewardship Antimicrobial Stewardship Studies have estimated that 30 50% of antibiotics prescribed in acutecare hospitals are unnecessary or inappropriate 1 Antimicrobial stewardship definition:
Antimicrobial Stewardship Antimicrobial Stewardship Studies have estimated that 30 50% of antibiotics prescribed in acutecare hospitals are unnecessary or inappropriate 1 Antimicrobial stewardship definition:
Surgical Site Infections (SSIs)
") Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
Surgical Site Infections (SSIs) Postoperative infections presenting at any level Incisional superficial (skin, subcutaneous tissue) Incisional deep (fascial plane and muscles) Organ/space related (anatomic
Clostridium Difficile Primer: Disease, Risk, & Mitigation
 Clostridium Difficile Primer: Disease, Risk, & Mitigation KALVIN YU, M.D. CHIEF INTEGRATION OFFICER, SCPMG/SCAL KAISER PERMANENTE ASSOCIATE PROFESSOR INFECTIOUS DISEASE, COLLEGE OF GLOBAL PUBLIC HEALTH,
Clostridium Difficile Primer: Disease, Risk, & Mitigation KALVIN YU, M.D. CHIEF INTEGRATION OFFICER, SCPMG/SCAL KAISER PERMANENTE ASSOCIATE PROFESSOR INFECTIOUS DISEASE, COLLEGE OF GLOBAL PUBLIC HEALTH,
Int.J.Curr.Microbiol.App.Sci (2017) 6(3):
 6(3):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
Source: Portland State University Population Research Center (
 Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
ESISTONO LE HCAP? Francesco Blasi. Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano
 ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
Antibiotic Prophylaxis in Spinal Surgery Antibiotic Guidelines. Contents
 Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Antibiotic Prophylaxis in Spinal Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): Authors Division: DCSS & Tertiary Medicine Unique
Dr.Asad A. Khan FRCPC Consultant, Division of Infectious Diseases Tawam Hospital Al Ain, UAE
 MDR Enterobacteriaceae in community acquired infections Dr.Asad A. Khan FRCPC Consultant, Division of Infectious Diseases Tawam Hospital Al Ain, UAE Introduction Case presentation Epidemiology Objectives
MDR Enterobacteriaceae in community acquired infections Dr.Asad A. Khan FRCPC Consultant, Division of Infectious Diseases Tawam Hospital Al Ain, UAE Introduction Case presentation Epidemiology Objectives
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017
 Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
M5 MEQs 2016 Session 3: SOB 18/11/16
 M5 MEQs 2016 Session 3: SOB 18/11/16 http://tinyurl.com/hn7qzt3 Question 1 Ms Tan is a 52 year old female with no past medical history. She comes to the emergency department presenting with a fever for
M5 MEQs 2016 Session 3: SOB 18/11/16 http://tinyurl.com/hn7qzt3 Question 1 Ms Tan is a 52 year old female with no past medical history. She comes to the emergency department presenting with a fever for
Update on Fluoroquinolones. Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO
 Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
The Rise of Antibiotic Resistance: Is It Too Late?
 The Rise of Antibiotic Resistance: Is It Too Late? Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine None DISCLOSURES THE PROBLEM Antibiotic resistance is one of the
The Rise of Antibiotic Resistance: Is It Too Late? Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine None DISCLOSURES THE PROBLEM Antibiotic resistance is one of the
The role of Infection Control Nurse in Prevention of Surgical Site Infection (SSI) April 2013
 April 2013") The role of Infection Control Nurse in Prevention of Surgical Site Infection (SSI) April 2013 Impact of SSI 2 nd common health- care associated infection (HCAI) 14-16% of HCAI Post operation SSI prolong
The role of Infection Control Nurse in Prevention of Surgical Site Infection (SSI) April 2013 Impact of SSI 2 nd common health- care associated infection (HCAI) 14-16% of HCAI Post operation SSI prolong
Infection Control & Prevention
 Infection Control & Prevention Objectives: Define the term multi-drug resistant organism (MDRO). Recognize risk factors for developing MDROs. Describe the clinical manifestations and medical treatment
Infection Control & Prevention Objectives: Define the term multi-drug resistant organism (MDRO). Recognize risk factors for developing MDROs. Describe the clinical manifestations and medical treatment
Role of the nurse in diagnosing infection: The right sample, every time
 BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
Infectious Disease in PA/LTC an Update. Karyn P. Leible, MD, CMD, FACP October 2015
 Infectious Disease in PA/LTC an Update Karyn P. Leible, MD, CMD, FACP October 2015 Disclosures Dr. Leible has no financial disclosures relevant to this presentation. Introduction Objectives The participant
Infectious Disease in PA/LTC an Update Karyn P. Leible, MD, CMD, FACP October 2015 Disclosures Dr. Leible has no financial disclosures relevant to this presentation. Introduction Objectives The participant
Medicinal Chemistry 561P. 2 st hour Examination. May 6, 2013 NAME: KEY. Good Luck!
 Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Summary of the latest data on antibiotic resistance in the European Union
 Summary of the latest data on antibiotic resistance in the European Union EARS-Net surveillance data November 2017 For most bacteria reported to the European Antimicrobial Resistance Surveillance Network
Summary of the latest data on antibiotic resistance in the European Union EARS-Net surveillance data November 2017 For most bacteria reported to the European Antimicrobial Resistance Surveillance Network
Multidrug Resistant Organisms (MDROs) and Clostridium difficile (C. diff)
 and Clostridium difficile (C. diff)") PATIENT & CAREGIVER EDUCATION Multidrug Resistant Organisms (MDROs) and Clostridium difficile (C. diff) This information explains multidrug resistant organisms (MDROs) and Clostridium difficile (C. diff),
PATIENT & CAREGIVER EDUCATION Multidrug Resistant Organisms (MDROs) and Clostridium difficile (C. diff) This information explains multidrug resistant organisms (MDROs) and Clostridium difficile (C. diff),
Community-acquired pneumonia: Time to place a CAP on length of treatment?
 LOGIN TO LEARN: An Engaging and Interactive Journal Club for Pharmacists and Students Community-acquired pneumonia: Time to place a CAP on length of treatment? Jennifer Ball, PharmD Learning Objectives
LOGIN TO LEARN: An Engaging and Interactive Journal Club for Pharmacists and Students Community-acquired pneumonia: Time to place a CAP on length of treatment? Jennifer Ball, PharmD Learning Objectives
Your Guide to Managing. Multi Drug-resistant Organisms (MDROs)
") Agency for Integrated Care 5 Maxwell Road #10-00 Tower Block MND Complex Singapore 069110 Singapore Silver Line: 1800-650-6060 Email: enquiries@aic.sg Website: www.silverpages.sg Facebook: www.facebook.com/carerssg
Agency for Integrated Care 5 Maxwell Road #10-00 Tower Block MND Complex Singapore 069110 Singapore Silver Line: 1800-650-6060 Email: enquiries@aic.sg Website: www.silverpages.sg Facebook: www.facebook.com/carerssg
DRAFT DRAFT. Paediatric Antibiotic Prescribing Guideline. May
 Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Paediatric Antibiotic Prescribing Guideline www.oxfdahsn.g/children Magdalen Centre Nth, 1 Robert Robinson Avenue, Oxfd Science Park, OX4 4GA, United Kingdom t: +44(0) 1865 784944 e: info@oxfdahsn.g Follow
Keeping Antibiotics Working: Nursing Leadership in Action
 Keeping Antibiotics Working: Nursing Leadership in Action Pat McLaine, DrPH, MPH, RN Robyn Gilden, PhD, RN Department of Family and Community Health Maryland Nurses Association October 2016 US 2 million
Keeping Antibiotics Working: Nursing Leadership in Action Pat McLaine, DrPH, MPH, RN Robyn Gilden, PhD, RN Department of Family and Community Health Maryland Nurses Association October 2016 US 2 million
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS
 VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
VCH PHC SURGICAL PROPHYLAXIS RECOMMENDATIONS CARDIAC Staphylococcus aureus, S. epidermidis, except for For patients with known MRSA colonization, recommend decolonization with Antimicrobial Photodynamic
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus
 Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
DATA COLLECTION SECTION BY FRONTLINE TEAM. Patient Identifier/ Medical Record number (for facility use only)
") Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
ANTIMICROBIAL STEWARDSHIP: THE ROLE OF THE CLINICIAN SAM GUREVITZ PHARM D, CGP BUTLER UNIVERSITY COLLEGE OF PHARMACY AND HEALTH SCIENCES
 ANTIMICROBIAL STEWARDSHIP: THE ROLE OF THE CLINICIAN SAM GUREVITZ PHARM D, CGP BUTLER UNIVERSITY COLLEGE OF PHARMACY AND HEALTH SCIENCES 1 Crisis: Antibiotic Resistance Success Strategy 2 OBJECTIVES Discuss
ANTIMICROBIAL STEWARDSHIP: THE ROLE OF THE CLINICIAN SAM GUREVITZ PHARM D, CGP BUTLER UNIVERSITY COLLEGE OF PHARMACY AND HEALTH SCIENCES 1 Crisis: Antibiotic Resistance Success Strategy 2 OBJECTIVES Discuss
Overview of C. difficile infections. Kurt B. Stevenson, MD MPH Professor Division of Infectious Diseases
 Overview of C. difficile infections Kurt B. Stevenson, MD MPH Professor Division of Infectious Diseases Conflicts of Interest I have no financial conflicts of interest related to this topic and presentation.
Overview of C. difficile infections Kurt B. Stevenson, MD MPH Professor Division of Infectious Diseases Conflicts of Interest I have no financial conflicts of interest related to this topic and presentation.
Clostridium difficile Colitis
 Update on Clostridium difficile Colitis Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
Update on Clostridium difficile Colitis Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship
 Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Vaccination as a potential strategy to combat Antimicrobial Resistance in the elderly
 Vaccination as a potential strategy to combat Antimicrobial Resistance in the elderly Wilbur Chen, MD, MS 22-23 March 2017 WHO meeting on Immunization of the Elderly The Problem Increasing consumption
Vaccination as a potential strategy to combat Antimicrobial Resistance in the elderly Wilbur Chen, MD, MS 22-23 March 2017 WHO meeting on Immunization of the Elderly The Problem Increasing consumption
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger