Combining antibiotics: when does it make sense and why? José Manuel Pereira
|
|
|
- Annabelle Ramsey
- 5 years ago
- Views:
Transcription



1 Combining antibiotics: when does it make sense and why? José Manuel Pereira Serviço de Medicina Intensiva do Centro Hospitalar S. João, EPE Faculdade de Medicina da Universidade do Porto Grupo de Infecção e Sepsis

2 Let s use antibiotics wisely! Adequate Antibiotic Treatment Avoid Unnecessary Antibiotics Correct antibiotic therapy Combination therapy? Proper dosing & interval Monitor cultures Susceptibilities? Colonization vs. infection Duration of therapy Monitor clinical endpoints Diagnostic evaluation A BALANCING ACT
3 Appropriateness of initial antimicrobial therapy Inappropriate initial antimicrobial therapy for septic shock occurs in about 20% of patients and is associated with a fivefold reduction in survival. Kumar A et al. Chest 2009; 136:
4 Mortality rates Rello et al Alvarez-Lerma Appropriate therapy Inappropriate therapy Ibrahim et al Luna et al Garnacho-Montero et al Vallés et al Mortality (%) Rello J et al. Am J Respir Crit Care Med 1997;156: ; Alvarez-Lerma et al. Intensive Care Med 1996;22: ; Ibrahim et al. Chest 2000;118: ; Vallés et al. Chest 2003;123: ; Luna et al. Chest 1997;111: Garnacho-Montero et al. Crit Care Med 2003;31: ;


5 Surviving Sepsis Guidelines
6 Potential Advantages Achieve broader cover for the empiric therapy Treatment of mixed infections Prevention of the development of resistance Reduce toxicity Achieve antibacterial sinergysm
7 Synergism In vitro for many antibiotic combinations Calandra T et al. Am J Med 1986; 80: 45. Kumar A et al. ICAAC Proc 2004; 26: A-1296; Darras-Joly C et al. Antimicrob Agents Chemother 1996; 40: 2147; Giamarellou H. Am J Med 1986; 80: 126. Giamarellou H et al. Antimicrob Agents Chemother 1984; 25: 534. Clinical studies of infection (including endocarditis, Gram negative bacteremia and neutropenic infections) Anderson ET et al. Chemotherapy 1978;24(1): Bouza E et al. Med Clin North Am 2000;84(6): ; De Jongh CA et al. Am J Med 1986;80(5C): Specific types of infection: HIV Tuberculosis Helicobacter pylori
8 Is clinical proof necessary? The Lab Real Life Use of measured antibiotic concentrations administered at precise time points and tested against a standard inoculum of bacteria Antibiotic concentrations in the host is determined by: dose, volume distribution and elimination rate of atb patient s age, volume status, weight, renal and hepatic function, hypoalbuminemia site of infection Bacterial load is highly variable
9 Potential Disadvantages Antagonism drug to drug interaction Adverse events Development of antimicrobial resistance Increased costs
10 When to use combination antibiotic therapy? Severe sepsis/ Septic shock Combination antibiotic therapy MRMo Source of infection
11 When to use combination antibiotic therapy? Severe sepsis/ Septic shock Combination antibiotic therapy MRMo Source of infection
12 Severe Sepsis/Septic Shock Meta-analysis of 62 eligible datasets demonstrated an estimated pooled OR for death/clinical failure of (95% CI, ) for combination compared to monotherapy regimens (p= 0.094) Combination therapy demonstrates a significant advantage over monotherapy when the rate of death/clinical failure exceeds 25% (pooled OR, 0.54; 95% CI, ; p = ) Kumar A et al. Crit Care Medicine 2010; 38 :
13 Severe Sepsis/Septic Shock Kumar A et al. Crit Care Medicine 2010; 38 :
14 Severe Sepsis/Septic Shock Hazard ratio 0.77; 95% CI ; p =.0002 Kumar A et al. Crit Care Medicine 2010; 38:
15 Severe Sepsis/Septic Shock The beneficial impact of combination therapy applied to both Gram positive and Gram-negative infections Combination therapy was also associated: Reduction in ICU (35.7% vs. 28.8%; OR 0.75; 95% CI ; p=.0006) and hospital mortality (47.8% vs. 37.4%; OR 0.69; 95% CI ; p <.0001). Increased ventilator (10 [0 25] vs. 17 [0 26]; p =.008) and pressor/ inotrope-free days (23 [0 28] vs. 25 [0 28]; p=.007) up to 30 days. Kumar A et al. Crit Care Medicine 2010; 38:
16 Severe Sepsis/Septic Shock Restricted to patients treated with β- lactams in combination with aminoglycosides, fluoroquinolones or macrolides/clindamycin. The most potent β-lactams including carbapenems failed to exhibit evidence of combination therapy benefit. In this circumstance, the addition of a second drug may have little incremental benefit Kumar A et al. Crit Care Medicine 2010; 38 :
17 Severe Sepsis/Septic Shock n= 1372 pts Mortality rate: DCCT 34% vs. non-dcct 40%; p= Díaz-Martín et al. Critical Care 2012, 16:R223
18 When to use combination antibiotic therapy? Severe sepsis/ Septic shock Combination antibiotic therapy MRMo Source of infection



19 Bacterial Meningitis If risk factors for Listeria monocytogenes: Age > 50 years or < 2 months Diabetes Alchoolism Immunosupression Malignancy 3rd Gen Cephalosporin + Ampicillin Tunkel AR et al. CID 2004; 39 :
20 Endocarditis Leibovici L International Journal of Antimicrobial Agents 2010; 36S: S46 S49


21 Endocarditis Mortality OR % CI Clinical Failure OR % CI Bacteriological Failure OR % CI Leibovici L International Journal of Antimicrobial Agents 2010; 36S: S46 S49
22 Endocarditis and Staph aureus Vancomycin + gentamicin In humans more rapid clearance of MSSA (2.7 d vs 3.3 d) In vitro synergy > for CA-MRSA and > for gentamicin-sensitive MRSA Does not reduce morbidity or mortality Korzeniowski O et al. Ann Int Med. 1982;97: Shelburne SA et al. Antimicrob Agents Chemother. 2004;48:



23 Endocarditis and Staph aureus Renal impairment as an adverse event was more frequent with standard therapy (18.1 % vs. 6.7 %; p= 0.009)

24 Endocarditis and Staph aureus
25 Endocarditis and Staph aureus Vancomycin + gentamicin In humans more rapid clearance of MSSA (2.7 d vs 3.3 d) In vitro synergy > for CA-MRSA and > for gentamicin-sensitive MRSA Does not reduce morbidity or mortality Korzeniowski O et al. Ann Int Med. 1982;97: Shelburne SA et al. AAC. 2004;48: Vancomycin + rifampicin In vitro Most often indifference Synergistic against MRSA growing in biofilm MRSA NVE (RCT) Days bacteremic Vancomycin 7 (5-11) Vancomycin + rifampin 9 (6-13) Maybe only in prosthetic valve or other foreign bodies Raad I et al. AAC 2007; 51: Bayer AS et al. J Infect Dis 1985; 151: Levine DP et al. Annals Intern Med. 1991;115: ; Shelburne SA et al. AAC. 2004;48:
26 Enterococcus spp. The enterococci are inherently more resistant to β-lactam antibiotics and are typically more tolerant to the bactericidal activity of these and other antimicrobial agents that act at the level of cell wall synthesis. In vitro bactericidal synergism between penicillin G and streptomycin against enterococci (1950) Synergistic and bactericidal therapy can be reliably achieved with the addition of an aminoglycoside to the β-lactam (or other cell wall agent such as vancomycin), as long as the organism does not exhibit high-level resistance to the aminoglycoside, making this combination the standard of care for severe enterococcal infections (endocarditis and meningitis)


27 Abdominal Infections SIS and IDSA GUIDELINES Solomkin JS et al. Clinical Infectious Diseases 2010; 50:133 64

28 Abdominal Infections Bochud PY et al. Crit Care Med 2004; 32:S


.")
29 Combination therapy in ciai infections Colonized with MRSA or who are at risk of having an infection due to this organism because of prior treatment failure and significant antibiotic exposure (B-II). Postoperative infection, previous use of cephalosporins or other antimicrobial agents selecting for Enterococcus species, immunocompromised, and pts with valvular heart disease or prosthetic intravascular materials (B-II). If Candida is grown from intra-abdominal cultures (B- II) Solomkin JS et al. Clinical Infectious Diseases 2010; 50:133 64

30 Community-Acquired Pneumonia
31 Community-Acquired Pneumonia AUTHOR POPULATION TYPE Nº COMBO SUPERIOR Gleason CAP Retro Yes Mufson, 1999 Bact. Pneumo Retro 328 Yes Waterer, 2001 Bact. Pneumo Retro 225 Yes Martinez, 2003 Bact. Pneumo Retro 409 Yes Weiss, 2004 Bact. Pneumo Retro 95 Yes Harbarth Pneumococcal sepsis Retro 107 No Garcia-Vasquez CAP Retro 1391 Yes
32 261 patients received BLM and 254 received FQ For PSI class V patients, there were lower 14-day and 30-day mortality rates with BLM than with FQ (14-day rates, 8.2% vs. 26.8% [p= 0.02]; 30-day rates, 18.4% vs. 36.6% [p= 0.05]). No differences in mortality between treatment groups were noted for the lower PSI classes. Lodise TP et al. Antimicrobial Agents and Chemotherapy 2007; 51:
33 Prospective, multicenter, observational study to evaluate if combination antibiotic therapy for severe bacteremic pneumococcal pneumonia is associated with a lower mortality. 592 of 844 patients with bacteremia due to St. pneumoniae global critically ill patients 10,4 vs. 11,5%, p= NS 23,4 vs. 55,3%, p= 0,0015 Baddour LM et al. AJRCCM 2004; 170:
 Combination antibiotic therapy seems to increase ICU survival")
34 No Shock Shock Prospective observational cohort study of 529 adults with severe CAP OR = % CI p= 0.01 p = 0.99 Even when monotherapy was appropriate, it achieved a lower 28-day survival than an adequate antibiotic combination OR 1,64 (1,01-2,64) Combination antibiotic therapy seems to increase ICU survival in patients with severe CAP and shock Rodriguez A (CAPUCI group) et al. Crit Care Med 2007; 35:
35 Dual Therapy in Severe CAP WHY Yes? Synergy? NO. Lin E et al. Antimicrob Agents Chemother 2003; 47: Better coverage of atypical microorganisms? Low incidence of atypical pathogens in the positive studies & Results adjusted for empirical innappropriate therapy
 and hospital admission within 30 days of discharge (OR, 0.67; p= 0.02).")
36 Retrospective study of 2209 Medicare patients with bacteremic pneumonia The initial use of any antibiotic active against atypical organisms was associated with a decreased risk of 30-day mortality (OR 0.76; p= 0.03) and hospital admission within 30 days of discharge (OR, 0.67; p= 0.02). Even when an alternative pathogen is identified, treatment including a macrolide results in improved outcome in patients with bacteremic CAP or HCAP Metersky ML et al. Chest 2007; 131:

37 Dual Therapy in Severe CAP Then WHY Yes? Action in two different bacteria sites - cell wall for beta-lactams - inhibition of protein synthesis for macrolides Combination of two mechanisms - huge lysis by beta-lactams - inhibition of virulence factors production by macrolides Macrolide immunomodulatory effects - Decrease of IL-6, IL-8, IL-1 and TNF and epithelial cell adherence
38 To investigate the effects of clarithromycin ( mg/l) alone or in combination with ceftriaxone (0.1 and 0.25 mg/l) on pneumolysin production by both macrolide-susceptible and -resistant strains of Streptococcus pneumoniae. Exposure of not only macrolide-susceptible strains, but also the macrolide-resistant strains, of S. pneumoniae to sub-mics of clarithromycin resulted in dose-related inhibition of the pneumolysin production, whereas production of the toxin was unaffected by ceftriaxone. These observations demonstrate that even in the setting of macrolide resistance the production of pneumolysin, a key virulence factor of the pneumococcus, is attenuated by exposure of this microbial pathogen to clarithromycin. Anderson R et al. J Antimicrob Chemother 2007; 59:
39 Dual Therapy in Severe CAP Adrie et al. Critical Care 2013, 17:R265
40 Dual Therapy in Severe CAP Dual therapy was associated with a higher frequency of initial adequate antibiotic therapy. Initial adequate antibiotic therapy was significantly associated with better survival (shr), 0.63; 95% CI 0.42 to 0.94; p = 0.02); this effect was strongest in patients with: Streptococcus pneumoniae CAP (shr, 0.05; 95% CI, ; p = 0.001) Septic shock (shr: 0.62; 95% CI 0.38 to 1.00; p = 0.05) No difference in 60-day mortality was found between monotherapy (β-lactam) and either of the two dual-therapy groups (β-lactam plus macrolide or fluoroquinolone). Adrie et al. Critical Care 2013, 17:R265
41 Dual Therapy in Severe CAP The rates of nosocomial pneumonia and multidrug-resistant bacteria were not significantly different across these three groups. Adrie et al. Critical Care 2013, 17:R265

42 Ventilator Associated Pneumonia

43 Inadequate Initial Antimicrobial Therapy for VAP
44 AJRCCM 2005; 171: Ventilator Associated Pneumonia ATS GUIDELINES
 or MD pneumonia (RR 0.86, 0.63 1.16) No significant differences in rates of superinfections (RR 0.77, 0.48 1.22) or serious adverse events (RR 0.84, 0.48 1.49) Aarts MA et al.")
45 Ventilator Associated Pneumonia n= 1459 patients MORTALITY RR 0.94; 95% CI No significant difference in treatment failure in patients with clinically suspected pneumonia (RR 0.88, ) or MD pneumonia (RR 0.86, ) No significant differences in rates of superinfections (RR 0.77, ) or serious adverse events (RR 0.84, ) Aarts MA et al. Crit Care Med 2008;36:108 17

46 Heyland D et al. Crit Care Med 2008;36: For critically ill patients who have suspected late VAP and who are at low risk for difficult-to-treat gram-negative bacteria, monotherapy is associated with similar outcomes compared with combination therapy. For those patients at high risk of difficult-to-treat gram-negative bacteria, combination therapy is safe and may be associated with better microbiological and clinical outcomes.
47 IV + Aerosolized Antibiotics Treatment success All-cause mortality: OR = 0.84, 95% CI Microbiological success: OR = 2.06, 95% CI Drug-related adverse effects: OR = 0.34, 95% CI Development of resistance: 6.5% (IV+aerosolized) Ioannidou E et al Journal of Antimicrobial Chemotherapy 2007; 60:
48 Rattanaumpawan P et al. JAC 2010; 65: pts with Gram-negative VAP Most of the cases were caused by MDR A. baumannii and/or Ps aeruginosa Duration of IV antibiotics: 9.5 vs days (p= 0.005) Nebulized CMS as adjunctive therapy for Gram-negative seems to be safe but a beneficial effect on clinical outcome was not ascertained Kofteridis DP et al. CID 2010; 51: pts with Gram-negative VAP (mostly MDR-Ab) No significant differences were observed regarding eradication of pathogens (p=.679), clinical cure (p=.10), and mortality (p=289) No AS colistin related adverse events were recorded.
49 Colistin IV + Aerosolized Retrospective, 1:1 matched case-control study (n= 208) AS-IV colistin cohort: had a higher clinical cure rate (69.2% vs 54.8%, p=.03) required fewer days of MV after VAP onset (8 days vs 12 days, p=.001) higher eradication of the causative organism (63.4% vs 50%, p =.08). No differences were observed in all-cause ICU mortality, length of ICU stay after VAP onset, or rates of acute kidney injury (AKI) during colistin therapy. Tumbarello M et al. Chest 2013; 144:

50 When to use combination antibiotic therapy? Severe sepsis/ Septic shock Combination antibiotic therapy MRMo Source of infection
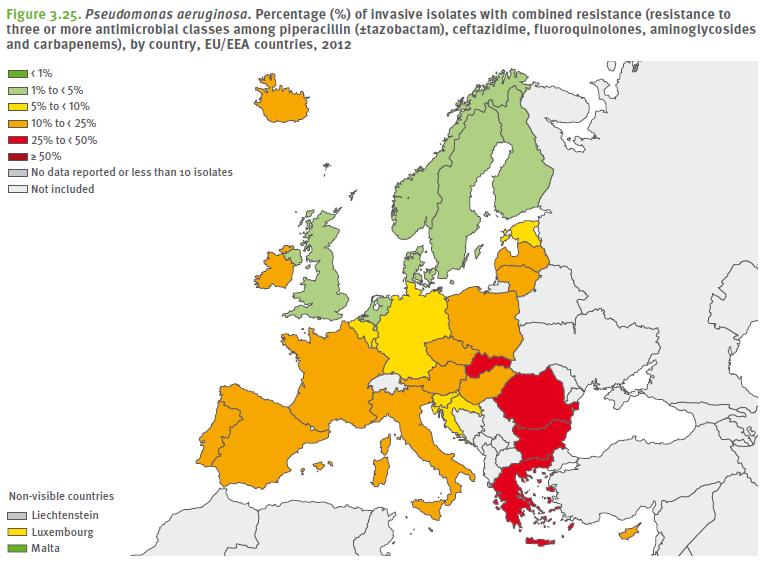
51 Pseudomonas aeruginosa
52 Combination Antibiotics Pseudomonas aeruginosa Broaden the antimicrobial spectrum Synergism Decrease emergence of antimicrobial resistance Minimize superinfection
53 In vitro synergism Wide ranges of results Dependent on several methodological factors: - method of synergy test used - susceptibility patterns of the isolates - concentrations of antibiotics used The greatest likelihood of synergy is an aminoglycoside with an antipseudomonal penicillin (~ 90%), and then, in decreasing order, with a cephalosporin (~ 80%) or a carbapenem (~ 50%). The interaction of fluoroquinolones combined with β-lactams or aminoglycosides was usually autonomous (additive) or indifferent. For quinolone combinations plus antipseudomonal β-lactams, the β-lactam drug accomplished most of the bacterial killing.
54 Ps aeruginosa Bacteremia Inadequate therapy and 28 day-mortality (AOR: 3,02; 95% CI: ,93; p = 0.02) Park et al. BMC Infectious Diseases 2012, 12:308

55 Ps aeruginosa VAP Retrospective, observational, cohort study 183 episodes of monomicrobial P. aeruginosa VAP Initial use of combination therapy significantly reduces the likelihood of inappropriate therapy, which is associated with higher risk of death. However, administration of only one effective antimicrobial or combination therapy provides similar outcomes, suggesting that switching to monotherapy once the susceptibility is documented is feasible and safe. Garnacho-Montero J et al Crit Care Med 2007; 35:
 indicating no mortality benefit with combination therapy Analysis of only Ps.")
56 Ps aeruginosa Bacteremia Meta-analysis of 17 studies to determine whether a combination of > 2 antibiotics reduces mortality in patients with Gram-negative bacteremia Most studies used beta-lactams or aminoglycosides alone and in combination. OR 0,96 (95% CI 0,7-1,32) indicating no mortality benefit with combination therapy Analysis of only Ps. aeruginosa bacteremias showed a significant mortality benefit (OR 0,5, 95% CI 0,3-0,79), but few patient and aminoglycosides in the monotherapy arm This meta-analysis does not support the routine use of combination antibiotherapy for Gram negative bacteremia beyond settings where Ps. aeruginosa bacteraemia is strongly suspected Safdar N et al. Lancet Inf Dis 2004; 4 :
 as variables that were independently associated with decreased allcause 28-day mortality No significant difference in terms of the emergence of antimicrobial resistance between the monotherapy")
57 Ps aeruginosa Bacteremia The absence of septic shock at the time of bacteremia (AOR 0.07; 95% CI, ; p = 0.008), and combination therapy (AOR 0.05; 95% CI ; p = 0.002) as variables that were independently associated with decreased allcause 28-day mortality No significant difference in terms of the emergence of antimicrobial resistance between the monotherapy and combination therapy group (21.9% and 12.1% respectively; p = 0.29). However, the 2-week bacteria eradication rate (54.5% vs. 18.8%, p = 0.04) and the 4-week eradication rate (54.5% vs. 28.1%, p = 0.04) were significantly higher in the combination therapy group than the monotherapy group. Park et al. BMC Infectious Diseases 2012, 12:308
58 Ps aeruginosa Bacteremia OR= %CI ; p = Hu Y et al International Journal Antimicrobial Agents 2013; 42:
59 Pseudomonas aeruginosa Definitive CT pts had nonsignificantly higher clinical cure (RR 1.36, 95% CI ). RR= 0.97, 95% CI Empirical CT pts had a significantly higher clinical cure rate (RR 1.23, 95% CI ). RR= 1.02, 95% CI Vardakas KZ et al International Journal Antimicrobial Agents 2013; 41:

60 Combination Antibiotics Pseudomonas aeruginosa Broaden the antimicrobial spectrum Synergism Drug Toxicity Decrease emergence of antimicrobial resistance Minimize superinfection Hu Y et al International Journal Antimicrobial Agents 2013; 42:

61 Acinetobacter baumannii > 50%
62 In vitro synergism Colistin Tigecycline Carbapenems Sulbactam Aminoglyc Rifampicin Others Colistin Pipt/tazo Tigecycline Carbapenems Sulbactam + Cefepime Fosfomycin Colistin + Tigecycline: better with Tigecycline 200 mg q12h Colistin + Carbapenem: In vitro synergy rates of 77% (95% CI: 64 to 87%) Meropenem was more synergistic than imipenem Carbapenem + Aminoglycoside: probably no better than carbapenem (imipenem) monotherapy Carbapenem + Rifampicin: no clinical benefit Triple combination therapy of meropenem,sulbactam and colistin has consistently shown very high levels of synergy.
 In-hospital mortality rate: 58% 30-days mortality rate: 49% Mortality: Carbapenem alone (58.3%) / Carbapenem and amikacin (50.")
63 Carbapenem-based regimens Retrospective study of 55 pts with MDR-AB bacteremia Combination therapy: n= 46 pts (83.6%) In-hospital mortality rate: 58% 30-days mortality rate: 49% Mortality: Carbapenem alone (58.3%) / Carbapenem and amikacin (50.0%) Kuo LC et al Clin Microbiol Infection 2007; 13:
64 Colistin plus Sulbactam n= 89 patients Colistin (58.4 %) vs. Colistin/sulbactam (41.6 %) Median APACHE II score was higher and diabetes mellitus was more common in the colistin/sulbactam Kalin G et al. Infection 2014; 42: 37 42
 or colistin (as above) plus rifampicin (600 mg q12 hours IV).")
65 Colistin plus Rifampicin Multicenter, parallel, randomized, open-label clinical trial 210 patients with life-threatening infections due to XDR A. baumannii Colistin alone (2 MU q8 h IV) or colistin (as above) plus rifampicin (600 mg q12 hours IV). Durante-Magoni E et al Clin Infect Dis 2013; 57:

66 Colistin plus Rifampicin Logistic Regression Analysis of Variables Related to Overall 30-Day Mortality At present, rifampicin should not be routinely combined with colistin in clinical practice. The increased rate of A. baumannii eradication with combination treatment could still imply a clinical benefit. Durante-Magoni E et al Clin Infect Dis 2013; 57:
67 Tigecycline-based regimens 386 patients with HAIs caused by MDRAB were retrospectively analyzed TG group (n=266): alone (n= 108) or in combination (n= 158) with ceftazidime, ceftriaxone, piperacillin/tazobactam, or a carbapenem. Non-TG group (n=120): treated with imipenem/cilastatin and sulbactam. Lee YT et al Eur J Clin Microbiol Infect Dis 2013; 32:
68 Tigecycline-based regimens Variable OR 95% CI p= Sepsis 1,737 1,078-2,798 0,023 TG alone 0,47 0,256-0,863 0,015 TG in combination 0,553 0,322-0,950 0,032 Switch to other antibiotics 0,468 0,294-0,746 0,001 Microbiological eradication 0,155 0,032-0,747 0,02 Multivariate analysis to identify risk factors influencing unfavorable clinical outcomes (stationary or deterioration) Although there were no significant differences in survival rates between the two groups, the rate of unfavorable outcome was significantly lower (p<0.05) among patients in the TG group than among patients in the non-tg group. The most significant predictors of favorable outcome were TG treatment and microbiological eradication. Lee YT et al Eur J Clin Microbiol Infect Dis 2013; 32:
69 Glycopeptide-colistin combination Retrospective study including episodes of VAP or bacteremia caused by carbapenem-resistant A. baumannii. 29 patients (group I) treated with colistin plus vancomycin (for at least 5 days) vs. 28 patients treated with colistin alone (group II). Baseline characteristics, clinical cure, microbiological eradication, and mortality were similar in both groups This combination significantly increases the risk of renal failure (55.2 vs. 28%; p = 0.04). Garnacho-Montero J et al Chemotherapy 2013; 59:
70 Glycopeptide-colistin combination Retrospective multicenter study of ICU patients 184 pts were treated with colistin and GNB infection was documented for 166 (MDR-Ab(59.6%), MDR Ps. aeruginosa (18.7%), and KPC-Kl. pneumoniae (14.5%)) 68 patients (40.9%) received CGC. Comparison of patients treated with and without CGC showed significant differences for respiratory failure (39.7% versus 58.2%), VAP (54.4% versus 71.4%), MDR-Ab infection (70.6% versus 52%), and GPB coinfection (41.2% versus 0%) No differences for nephrotoxicity (11.8% versus 13.3%) and 30-day mortality (33.8% versus 29.6%). Cox analysis for 30-day mortality performed on patients who survived for 5 days after treatment onset: Charlson index (HR 1.26; 95% CI: ; p= 0.001) MDR A. baumannii infection (HR 2.51; 95% CI: ; p= 0.01) Receiving CGC for 5 days was a protective factor (HR 0.42; 95% CI ; p= 0.03). Petrosillo N et al AAC 2014; 58:
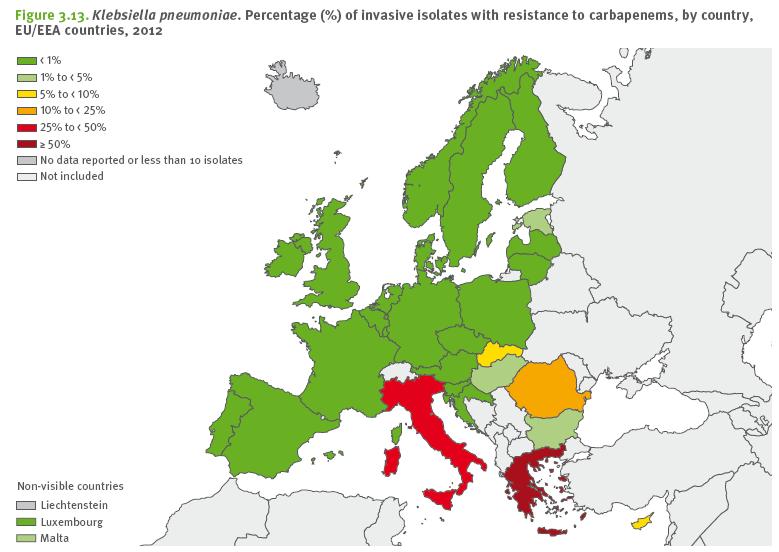
71 Carbapenemase-producing Kl. pneumoniae
72 Carbapenemase-producing Kl. pneumoniae KPC-Kl. pneumoniae has become a significant problem in terms of public health and clinical outcome. Not only able to hydrolyze carbapenems but they are often resistant to a variety of other antibiotics as well Small clinical studies have revealed high treatment failure rates and reported mortality rates range from 22% to 72% Treatment options are usually limited to colistin, gentamicin, and/or tigecycline, but the optimal regimen for infections caused by KPC-producing bacteria has yet to be defined. In vitro data demonstrated that combination therapies are often more effective than monotherapies Hirsch EB et al J Antimicrob Chemother 2010; 65: ; Carmeli Y et al Clin Microbiol Infect 2010; 16: Borer A et al Infect Control Hosp Epidemiol 2009; 30:972 6; Pournaras S et al Int J Antimicrob Agents 2011; 37:244 7.

73 Carbapenemase-producing Kl. pneumoniae n= 67 cases % Daikos GL et al AAC 2009; 53:
74 Carbapenemase-producing Kl. pneumoniae Qureshi ZA et al. AAC 2012; 56: The 28-day mortality was 13.3% in the CT vs. 57.8% in the M group (P = 0.01). In the multivariate analysis, definitive therapy with a combination regimen was independently associated with survival (OR 0.07 ;95% CI ; p = 0.02). Despite in vitro susceptibility, patients who received monotherapy with colistinpolymyxin B or tigecycline had a higher mortality of 66.7%. Colistin/Tigecycline + carbapenem: most common (mortality %). Zarkotou O et al. CMI 2011; 17: Overall mortality was 52.8% and infection mortality was 34% Appropriate antimicrobial therapy was administered to 35 patients (66%) In the appropriate group: mortality in CT was significantly lower than in M group ( 0% vs. 46,7%; p= 0.001) In univariate analysis, combinations of active antimicrobials (p 0.001) were significantly associated with survival.
75 Carbapenemase-producing Kl. pneumoniae n= 125 KPC-KP bacteremia episodes 60% of empirical antibiotics were classified as inadequate. Postantibiogram regimens used: monotherapy in 36.8% and 63.2% received 2 drugs with in vitro activity against the KPC-Kp isolate 30 day-mortality: 41,6% (mono - 54,3% vs. combination- 34,1%; p= 0.02) Lowest mortality rate with tigecycline+colistin+meropenem (12,5%) Tumbarello M et al Clinical Infect Dis 2012; 55:

76 Carbapenemase-producing Kl. pneumoniae To improve survival, combined treatment with 2 or more drugs with in vitro activity against the isolate, especially those also including a carbapenem, may be more effective than active monotherapy. Tumbarello M et al Clinical Infect Dis 2012; 55:

 activity against an already reduced, manageable All responded inoculum.")
77 Carbapenemase-producing pandrug-resistant Kl. pneumoniae Ertapenem + Doripenem In vitro and in vivo murine model enhanced efficacy of the combination regimens over that of the monotherapy regimens in both models Reduction in inoculum density by ertapenem acting as a suicide substrate Ertapenem and + thereby Doripenem/Meropenem permitting doripenem/meropenem to express 3 cases its (bacteremia, successful UTI) activity against an already reduced, manageable All responded inoculum. successfully without relapse at follow-up Ertapenem + Doripenem 5 cases (bacteremia) All had clinical and microbiologic cure Bulik CC et al AAC 2011; 55: ; Giamarellou H et al AAC 2013; 57: ; Nogid B, Nicolau DP. ACC Submitted


78 Conclusions The most common indication of combination of antibiotics is empiric treatment, when the goal is to cover all potential pathogens and when such a wide spectrum is impossible to guarantee with a single drug Combination therapy is not without risks, such as increased toxicity and cost. The host The source Local epidemiology
79 Conclusions Combination therapy is recommended in: Severe CAP, especially in shocked patients and bacteremic pneumococcal pneumonia, for 3-5 days Bacterial meningitis (if predisposing factors for Listeria) Enterococci infections (mainly endocarditis and meningitis) Infectious endocarditis by Staph aureus? If so, only 3 to 5 days Empiric treatment of nosocomial pneumonia with high suspicion for MDR pathogens (chosen according to local patterns and surveillance cultures and only until susceptibility available) Infections caused by XDR/PDR pathogens
80
Mono- versus Bitherapy for Management of HAP/VAP in the ICU
 Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Outline. Antimicrobial resistance. Antimicrobial resistance in gram negative bacilli. % susceptibility 7/11/2010
 Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Fighting MDR Pathogens in the ICU
 Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Successful stewardship in hospital settings
 Successful stewardship in hospital settings Pr Charles-Edouard Luyt Service de Réanimation Institut de Cardiologie Groupe Hospitalier Pitié-Salpêtrière Université Pierre et Marie Curie, Paris 6 www.reamedpitie.com
Successful stewardship in hospital settings Pr Charles-Edouard Luyt Service de Réanimation Institut de Cardiologie Groupe Hospitalier Pitié-Salpêtrière Université Pierre et Marie Curie, Paris 6 www.reamedpitie.com
Antimicrobial stewardship in managing septic patients
 Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia. Po-Ren Hsueh. National Taiwan University Hospital
 Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
High-Risk MDR clones news in treatment
 Ferrara, 20 giugno 2013 High-Risk MDR clones news in treatment Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Characteristics and determinants of outcome of hospital-acquired
Ferrara, 20 giugno 2013 High-Risk MDR clones news in treatment Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Characteristics and determinants of outcome of hospital-acquired
10 Golden rules of Antibiotic Stewardship in ICU. Jeroen Schouten, MD PhD intensivist, Nijmegen (Neth) Istanbul, Oct 6th 2017
 Istanbul, Oct 6th 2017") 10 Golden rules of Antibiotic Stewardship in ICU Jeroen Schouten, MD PhD intensivist, Nijmegen (Neth) Istanbul, Oct 6th 2017 10 golden rules of Antibiotic Stewardship in the ICU ID, Pharma & Micro advice
10 Golden rules of Antibiotic Stewardship in ICU Jeroen Schouten, MD PhD intensivist, Nijmegen (Neth) Istanbul, Oct 6th 2017 10 golden rules of Antibiotic Stewardship in the ICU ID, Pharma & Micro advice
Multi-drug resistant microorganisms
 Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
Antimicrobial Cycling. Donald E Low University of Toronto
 Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
ESCMID Online Lecture Library. by author
 Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections
 for the treatment of Acinetobacter baumannii infections") ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases
 The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
Summary of unmet need guidance and statistical challenges
 Summary of unmet need guidance and statistical challenges Daniel B. Rubin, PhD Statistical Reviewer Division of Biometrics IV Office of Biostatistics, CDER, FDA 1 Disclaimer This presentation reflects
Summary of unmet need guidance and statistical challenges Daniel B. Rubin, PhD Statistical Reviewer Division of Biometrics IV Office of Biostatistics, CDER, FDA 1 Disclaimer This presentation reflects
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Introduction to Pharmacokinetics and Pharmacodynamics
 Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
What does multiresistance actually mean? Yohei Doi, MD, PhD University of Pittsburgh
 What does multiresistance actually mean? Yohei Doi, MD, PhD University of Pittsburgh Disclosures Merck Research grant Clinical context of multiresistance Resistance to more classes of agents Less options
What does multiresistance actually mean? Yohei Doi, MD, PhD University of Pittsburgh Disclosures Merck Research grant Clinical context of multiresistance Resistance to more classes of agents Less options
Dr. Shaiful Azam Sazzad. MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College
 Critical Care Medicine Dhaka Medical College") Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
ESISTONO LE HCAP? Francesco Blasi. Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano
 ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
Konsequenzen für Bevölkerung und Gesundheitssysteme. Stephan Harbarth Infection Control Program
 Konsequenzen für Bevölkerung und Gesundheitssysteme Stephan Harbarth Infection Control Program University of Geneva Hospitals Outline Introduction What data sources are available? AMR-associated outcomes
Konsequenzen für Bevölkerung und Gesundheitssysteme Stephan Harbarth Infection Control Program University of Geneva Hospitals Outline Introduction What data sources are available? AMR-associated outcomes
Management of Hospital-acquired Pneumonia
 Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Antibacterials. Recent data on linezolid and daptomycin
 Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Measure Information Form
 Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other β-lactamase Inhibitor (BLI) Combinations: Focus on VNRX-5133, WCK 5222 and ETX2514SUL
 Combinations: Focus on VNRX-5133, WCK 5222 and ETX2514SUL") Other β-lactamase Inhibitor (BLI) Combinations: Focus on VNRX-5133, WCK 5222 and ETX2514SUL David P. Nicolau, PharmD, FCCP, FIDSA Director, Center for Anti-Infective Research and Development Hartford Hospital
Other β-lactamase Inhibitor (BLI) Combinations: Focus on VNRX-5133, WCK 5222 and ETX2514SUL David P. Nicolau, PharmD, FCCP, FIDSA Director, Center for Anti-Infective Research and Development Hartford Hospital
Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them?
 Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them? Roberta B. Carey, PhD Centers for Disease Control and Prevention Division of Healthcare Quality Promotion Why worry? MDROs Clinical
Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them? Roberta B. Carey, PhD Centers for Disease Control and Prevention Division of Healthcare Quality Promotion Why worry? MDROs Clinical
MDR Acinetobacter baumannii. Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta
 MDR Acinetobacter baumannii Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta 1 The Armageddon recipe Transmissible organism with prolonged environmental
MDR Acinetobacter baumannii Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta 1 The Armageddon recipe Transmissible organism with prolonged environmental
Management of Native Valve
 Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams
 DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
Duration of antibiotic therapy:
 Duration of antibiotic therapy: How low can you go? Thomas Holland, MD Hilton Head, SC July 2017 Disclosures Consulting: The Medicines Company, Basilea Pharmaceutica Adjudication committee: Achaogen Grant
Duration of antibiotic therapy: How low can you go? Thomas Holland, MD Hilton Head, SC July 2017 Disclosures Consulting: The Medicines Company, Basilea Pharmaceutica Adjudication committee: Achaogen Grant
Witchcraft for Gram negatives
 Witchcraft for Gram negatives Dr Subramanian S MD DNB MNAMS AB (Medicine, Infect Dis) Infectious Diseases Consultant Global Health City, Chennai www.asksubra.com Drug resistance follows the drug like a
Witchcraft for Gram negatives Dr Subramanian S MD DNB MNAMS AB (Medicine, Infect Dis) Infectious Diseases Consultant Global Health City, Chennai www.asksubra.com Drug resistance follows the drug like a
Scottish Medicines Consortium
 Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Pharmacokinetics and Pharmacodynamics of Antimicrobials in the Critically Ill Patient
 Pharmacokinetics and Pharmacodynamics of Antimicrobials in the Critically Ill Patient Rania El-Lababidi, Pharm.D., BCPS (AQ-ID), AAHIVP Manager, Pharmacy Education and Training Cleveland Clinic Abu Dhabi
Pharmacokinetics and Pharmacodynamics of Antimicrobials in the Critically Ill Patient Rania El-Lababidi, Pharm.D., BCPS (AQ-ID), AAHIVP Manager, Pharmacy Education and Training Cleveland Clinic Abu Dhabi
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
The role of carbapenems in the hospital
 The role of carbapenems in the hospital Matteo Bassetti, MD, PhD Infectious Diseases Division Santa Maria Misericordia University Hospital Udine, Italy Rationale for Antibiotic Optimizaton: Balancing The
The role of carbapenems in the hospital Matteo Bassetti, MD, PhD Infectious Diseases Division Santa Maria Misericordia University Hospital Udine, Italy Rationale for Antibiotic Optimizaton: Balancing The
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Nosocomial Infections: What Are the Unmet Needs
 Nosocomial Infections: What Are the Unmet Needs Jean Chastre, MD Service de Réanimation Médicale Hôpital Pitié-Salpêtrière, AP-HP, Université Pierre et Marie Curie, Paris 6, France www.reamedpitie.com
Nosocomial Infections: What Are the Unmet Needs Jean Chastre, MD Service de Réanimation Médicale Hôpital Pitié-Salpêtrière, AP-HP, Université Pierre et Marie Curie, Paris 6, France www.reamedpitie.com
Rational use of antibiotics
 Rational use of antibiotics Uga Dumpis MD, PhD,, DTM Stradins University Hospital Riga, Latvia ugadumpis@stradini.lv BALTICCARE CONFERENCE, PSKOV, 16-18.03, 18.03, 2006 Why to use antibiotics? Prophylaxis
Rational use of antibiotics Uga Dumpis MD, PhD,, DTM Stradins University Hospital Riga, Latvia ugadumpis@stradini.lv BALTICCARE CONFERENCE, PSKOV, 16-18.03, 18.03, 2006 Why to use antibiotics? Prophylaxis
Why should we care about multi-resistant bacteria? Clinical impact and
 Why should we care about multi-resistant bacteria? Clinical impact and public health implications Prof. Stephan Harbarth Infection Control Program Geneva, Switzerland and Ebola (in 2014/2015) Increased
Why should we care about multi-resistant bacteria? Clinical impact and public health implications Prof. Stephan Harbarth Infection Control Program Geneva, Switzerland and Ebola (in 2014/2015) Increased
Burton's Microbiology for the Health Sciences. Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents
 Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Sustaining an Antimicrobial Stewardship
 Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Int.J.Curr.Microbiol.App.Sci (2017) 6(3):
 6(3):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Learning Points. Raymond Blum, M.D. Antimicrobial resistance among gram-negative pathogens is increasing
 Raymond Blum, M.D. Learning Points Antimicrobial resistance among gram-negative pathogens is increasing Infection with antimicrobial-resistant pathogens is associated with increased mortality, length of
Raymond Blum, M.D. Learning Points Antimicrobial resistance among gram-negative pathogens is increasing Infection with antimicrobial-resistant pathogens is associated with increased mortality, length of
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE. Measure Information Form
 Last Updated: Version 3.2a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form Organization Set Measure ID#
Last Updated: Version 3.2a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form Organization Set Measure ID#
Appropriate Antimicrobial Therapy for Treatment of
 Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
UTILITY OF A COMBINATION ANTIBIOGRAM FOR TREATING PSEUDOMONAS AERUGINOSA
 American Journal of Infectious Diseases 10 (2): 88-94, 2014 ISSN: 1553-6203 2014 Science Publication doi:10.3844/ajidsp.2014.88.94 Published Online 10 (2) 2014 (http://www.thescipub.com/ajid.toc) UTILITY
American Journal of Infectious Diseases 10 (2): 88-94, 2014 ISSN: 1553-6203 2014 Science Publication doi:10.3844/ajidsp.2014.88.94 Published Online 10 (2) 2014 (http://www.thescipub.com/ajid.toc) UTILITY
Management of hospital-acquired acquired pneumonia in the Asian Pacific region
 Management of hospital-acquired acquired pneumonia in the Asian Pacific region Jae-Hoon Song, MD, PhD Samsung Medical Center Asian Network for Surveillance of Resistant Pathogens (ANSORP) Asian-Pacific
Management of hospital-acquired acquired pneumonia in the Asian Pacific region Jae-Hoon Song, MD, PhD Samsung Medical Center Asian Network for Surveillance of Resistant Pathogens (ANSORP) Asian-Pacific
Considerations for antibiotic therapy. Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen
 Considerations for antibiotic therapy Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen Infective Endocarditis There will never be a cure for this malignant disease! Sir
Considerations for antibiotic therapy Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen Infective Endocarditis There will never be a cure for this malignant disease! Sir
* gender factor (male=1, female=0.85)
") Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Early Antibiotics for Sepsis and Septic Shock: A Gold Standard
 Early Antibiotics for Sepsis and Septic Shock: A Gold Standard Anand Kumar MD, FRCPC, FCCP, FCCM Professor of Medicine University of Manitoba Health Sciences Centre St. Boniface Hospital Winnipeg, Manitoba
Early Antibiotics for Sepsis and Septic Shock: A Gold Standard Anand Kumar MD, FRCPC, FCCP, FCCM Professor of Medicine University of Manitoba Health Sciences Centre St. Boniface Hospital Winnipeg, Manitoba
EARS Net Report, Quarter
 EARS Net Report, Quarter 4 213 March 214 Key Points for 213* Escherichia coli: The proportion of patients with invasive infections caused by E. coli producing extended spectrum β lactamases (ESBLs) increased
EARS Net Report, Quarter 4 213 March 214 Key Points for 213* Escherichia coli: The proportion of patients with invasive infections caused by E. coli producing extended spectrum β lactamases (ESBLs) increased
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Sepsis is the most common cause of death in
 ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
Bacterial infections complicating cirrhosis
 PHC www.aphc.info Bacterial infections complicating cirrhosis P. Angeli, Dept. of Medicine, Unit of Internal Medicine and Hepatology (), University of Padova (Italy) pangeli@unipd.it Agenda Epidemiology
PHC www.aphc.info Bacterial infections complicating cirrhosis P. Angeli, Dept. of Medicine, Unit of Internal Medicine and Hepatology (), University of Padova (Italy) pangeli@unipd.it Agenda Epidemiology
Principles of Antimicrobial Therapy
 Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
What s next in the antibiotic pipeline?
 What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Pharmacodynamics as an Approach to Optimizing Therapy Against Problem Pathogens
 Pharmacodynamics as an Approach to Optimizing Therapy Against Problem Pathogens Jared L. Crandon, Pharm.D., BCPS Associate Director, Clinical and Experimental Pharmacology Center for Anti-Infective Research
Pharmacodynamics as an Approach to Optimizing Therapy Against Problem Pathogens Jared L. Crandon, Pharm.D., BCPS Associate Director, Clinical and Experimental Pharmacology Center for Anti-Infective Research
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali. Lec 1
 Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Principles of Antimicrobial therapy
 Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
Management of Infections with Multi-drug Resistance Bacteria การร กษาการต ดเช อแบคท เร ยด อยา
 Management of Infections with Multi-drug Resistance Bacteria การร กษาการต ดเช อแบคท เร ยด อยา รองศาสตราจารย แพทย หญ งศศ โสภ ณ เก ยรต บ รณก ล คณะแพทยศาสตร โรงพยาบาลรามาธ บด Sasisopin Kiertiburanakul, MD,
Management of Infections with Multi-drug Resistance Bacteria การร กษาการต ดเช อแบคท เร ยด อยา รองศาสตราจารย แพทย หญ งศศ โสภ ณ เก ยรต บ รณก ล คณะแพทยศาสตร โรงพยาบาลรามาธ บด Sasisopin Kiertiburanakul, MD,
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Antibacterial Resistance: Research Efforts. Henry F. Chambers, MD Professor of Medicine University of California San Francisco
 Antibacterial Resistance: Research Efforts Henry F. Chambers, MD Professor of Medicine University of California San Francisco Resistance Resistance Dose-Response Curve Antibiotic Exposure Anti-Resistance
Antibacterial Resistance: Research Efforts Henry F. Chambers, MD Professor of Medicine University of California San Francisco Resistance Resistance Dose-Response Curve Antibiotic Exposure Anti-Resistance
Rise of Resistance: From MRSA to CRE
 Rise of Resistance: From MRSA to CRE Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine SUPERBUGS (AKA MDROs) MRSA Methicillin-resistant S. aureus Evolution of Drug Resistance
Rise of Resistance: From MRSA to CRE Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine SUPERBUGS (AKA MDROs) MRSA Methicillin-resistant S. aureus Evolution of Drug Resistance
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
Original Articles. K A M S W Gunarathne 1, M Akbar 2, K Karunarathne 3, JRS de Silva 4. Sri Lanka Journal of Child Health, 2011; 40(4):
:") Original Articles Analysis of blood/tracheal culture results to assess common pathogens and pattern of antibiotic resistance at medical intensive care unit, Lady Ridgeway Hospital for Children K A M S
Original Articles Analysis of blood/tracheal culture results to assess common pathogens and pattern of antibiotic resistance at medical intensive care unit, Lady Ridgeway Hospital for Children K A M S
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
The Treatment of Resistant Bacterial Infection in Children
 The Treatment of Resistant Bacterial Infection in Children Andrew Whitelaw Division of Medical Microbiology, University of Stellenbosch & NHLS South African Antibiotic Stewardship Programme SAPA/SAAPS
The Treatment of Resistant Bacterial Infection in Children Andrew Whitelaw Division of Medical Microbiology, University of Stellenbosch & NHLS South African Antibiotic Stewardship Programme SAPA/SAAPS
Extremely Drug-resistant organisms: Synergy Testing
 Extremely Drug-resistant organisms: Synergy Testing Background Acinetobacter baumannii& Pseudomonas aeruginosa Emerging Gram-negative bacilli Part of the ESKAPE group of organisms 1 Enterococcus faecium
Extremely Drug-resistant organisms: Synergy Testing Background Acinetobacter baumannii& Pseudomonas aeruginosa Emerging Gram-negative bacilli Part of the ESKAPE group of organisms 1 Enterococcus faecium
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS
 PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
Antibiotics 201: Gramnegatives
 Antibiotics 201: Gramnegatives B. Joseph Guglielmo, Pharm.D. Professor and Dean School of Pharmacy University of California San Francisco Disclosures No potential conflicts of interest. 1 A 77 year old
Antibiotics 201: Gramnegatives B. Joseph Guglielmo, Pharm.D. Professor and Dean School of Pharmacy University of California San Francisco Disclosures No potential conflicts of interest. 1 A 77 year old
DOES TIMING OF ANTIBIOTICS IMPACT OUTCOME IN SEPSIS? Saravana Kumar MD HEAD,DEPT OF EM,DR MEHTA S HOSPITALS CHENNAI,INDIA
 DOES TIMING OF ANTIBIOTICS IMPACT OUTCOME IN SEPSIS? Saravana Kumar MD HEAD,DEPT OF EM,DR MEHTA S HOSPITALS CHENNAI,INDIA drsaravanakumar.ep@gmail.com JOINT SECRETARY RECOMMENDATIONS: INITIAL RESUSCITATION
DOES TIMING OF ANTIBIOTICS IMPACT OUTCOME IN SEPSIS? Saravana Kumar MD HEAD,DEPT OF EM,DR MEHTA S HOSPITALS CHENNAI,INDIA drsaravanakumar.ep@gmail.com JOINT SECRETARY RECOMMENDATIONS: INITIAL RESUSCITATION
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES:
These recommendations were approved for use by the Pharmaceutical and Therapeutics Committee, RCWMCH on 1 February 2017.
 Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Jump Starting Antimicrobial Stewardship
 Jump Starting Antimicrobial Stewardship Amanda C. Hansen, PharmD Pharmacy Operations Manager Carilion Roanoke Memorial Hospital Roanoke, Virginia March 16, 2011 Objectives Discuss guidelines for developing
Jump Starting Antimicrobial Stewardship Amanda C. Hansen, PharmD Pharmacy Operations Manager Carilion Roanoke Memorial Hospital Roanoke, Virginia March 16, 2011 Objectives Discuss guidelines for developing
The role of new antibiotics in the treatment of severe infections: Safety and efficacy features
 The role of new antibiotics in the treatment of severe infections Safety and efficacy features Christian Eckmann Hannover, Germany The role of new antibiotics in the treatment of severe infections: Safety
The role of new antibiotics in the treatment of severe infections Safety and efficacy features Christian Eckmann Hannover, Germany The role of new antibiotics in the treatment of severe infections: Safety
Does Early and Appropriate Antibiotic Administration Improve Mortality in Emergency Department Patients with Severe Sepsis or Septic Shock?
 References and Literature Grading Does Early and Appropriate Antibiotic Administration Improve Mortality in Emergency Department Patients with Severe Sepsis or Septic Shock? (9/6/2015) 1. Dellinger, R.P.,
References and Literature Grading Does Early and Appropriate Antibiotic Administration Improve Mortality in Emergency Department Patients with Severe Sepsis or Septic Shock? (9/6/2015) 1. Dellinger, R.P.,
48 th Annual Meeting. IDWeek and ICAAC: The Cliffs Notes Version. Skin and Soft Tissue Infections. Skin and Soft Tissue Infections.
 48 th Annual Meeting IDWeek and ICAAC: The Cliffs Notes Version Yanina Pasikhova Pharm.D., BCPS-AQ ID, AAHIVP Infectious Diseases Pharmacist Moffitt Cancer Center Navigating the Oceans of Opportunity Skin
48 th Annual Meeting IDWeek and ICAAC: The Cliffs Notes Version Yanina Pasikhova Pharm.D., BCPS-AQ ID, AAHIVP Infectious Diseases Pharmacist Moffitt Cancer Center Navigating the Oceans of Opportunity Skin
CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE)
") CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE) Bartsch SM et al. Potential economic burden of carbapenem-resistent Enterobacteriaceae (CRE) in the United States. Clin Microbiol Infect 2017;23(1):48e9-e16.
CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE) Bartsch SM et al. Potential economic burden of carbapenem-resistent Enterobacteriaceae (CRE) in the United States. Clin Microbiol Infect 2017;23(1):48e9-e16.
NEW ATS/IDSA VAP-HAP GUIDELINES
 NEW ATS/IDSA VAP-HAP GUIDELINES MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the University
NEW ATS/IDSA VAP-HAP GUIDELINES MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the University
Vaccination as a potential strategy to combat Antimicrobial Resistance in the elderly
 Vaccination as a potential strategy to combat Antimicrobial Resistance in the elderly Wilbur Chen, MD, MS 22-23 March 2017 WHO meeting on Immunization of the Elderly The Problem Increasing consumption
Vaccination as a potential strategy to combat Antimicrobial Resistance in the elderly Wilbur Chen, MD, MS 22-23 March 2017 WHO meeting on Immunization of the Elderly The Problem Increasing consumption
Antibiotic usage in nosocomial infections in hospitals. Dr. Birgit Ross Hospital Hygiene University Hospital Essen
 Antibiotic usage in nosocomial infections in hospitals Dr. Birgit Ross Hospital Hygiene University Hospital Essen Infection control in healthcare settings - Isolation - Hand Hygiene - Environmental Hygiene
Antibiotic usage in nosocomial infections in hospitals Dr. Birgit Ross Hospital Hygiene University Hospital Essen Infection control in healthcare settings - Isolation - Hand Hygiene - Environmental Hygiene
Tel: Fax:
 CONCISE COMMUNICATION Bactericidal activity and synergy studies of BAL,a novel pyrrolidinone--ylidenemethyl cephem,tested against streptococci, enterococci and methicillin-resistant staphylococci L. M.
CONCISE COMMUNICATION Bactericidal activity and synergy studies of BAL,a novel pyrrolidinone--ylidenemethyl cephem,tested against streptococci, enterococci and methicillin-resistant staphylococci L. M.
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship
 Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases