2016 Updates to the Hospital Acquired- and Ventilator Associated-Pneumonia Guidelines
|
|
|
- Ambrose Montgomery
- 6 years ago
- Views:
Transcription


1 2016 Updates to the Hospital Acquired- and Ventilator Associated-Pneumonia Guidelines Janessa M. Smith, PharmD, BCPS Clinical Pharmacy Specialist, Infectious Diseases The Johns Hopkins Hospital
2 Objectives List risk factors for development of pneumonia with multidrug resistant organisms Describe the role of an antibiogram in the empiric treatment of hospital acquired pneumonia (HAP) and ventilator associated pneumonia (VAP) Identify the role of pharmacokinetic and pharmacodynamic parameters in dose optimization Discuss the role of biomarkers in diagnosing and treating HAP and VAP
3 Epidemiology Pneumonia is the most common healthcare-associated infection (HAI) HAP and VAP account for 22% of HAI annually Up to 50% of patients with HAP develop serious complications Respiratory failure, pleural effusions, septic shock, renal failure and empyema All-cause mortality from VAP ranges from 20-50% and attributable mortality has been estimated at 13% Magill SSl. N Engl Med. 2014;370:2542; Sopena N. Chest. 2005;127:213; Melson WG. Lancet Infect Dis. 2013;13:665; Muscedere JG. Clin Infec Dis. 2010;51 (supp 1):S120; Kollef MH. Infec Control Hosp Epidemiol. 2012;33:250.
4 Impact on the Healthcare System VAP prolongs length of ventilation (7.6 to 11.5 days) and hospital stay (11.5 to 13.1 days) VAP estimated to result in excess health care costs of $40,000 per patient Limited data on the impact of HAP Magill SS, et al. N Engl Med. 2014;370:2542; Sopena N, et al., Chest. 2005;127:213; Melson WG, et al. Lancet Infect Dis. 2013;13:665; Muscedere JG, et al. Clin Infec Dis. 2010;51 (supp 1):S120; Kollef MH, et al. Infec Control Hosp Epidemiol.2012;33:250.
5 Definitions Pneumonia Presence of a new lung infiltrate plus clinical evidence of an infectious cause (fever, purulent sputum, leukocytosis and decline in oxygenation) VAP Pneumonia that develops >48 hours after endotracheal intubation HAP Pneumonia that develops >48 hours after hospital admission Am J Respir Crit Care Med. 2005;171:
6 Major Changes in the 2016 Update Recommend less invasive microbiologic methods for diagnosis Redefine risk factors for multidrug resistant organisms (MDRO) Emphasis on antibiograms to guide empiric therapy Emphasis on optimizing antimicrobial dosing based on pharmacokinetic (PK) and pharmacodynamic (PD) parameters Suggest duration of therapy of 7 days for all HAP/VAP treatment Kalil AC. Clin Infect Dis. 2016;63:1-51.
7 Microbiologic Methods to Diagnosis Recommendation Non-invasive sampling with semiquantitative cultures preferred Expectorated or induced sputum cultures Endonasotracheal cultures If invasive sampling methods used, should be quantitative and should be used to stop therapy if below diagnostic threshold: Bronchoalveolar lavage: <10 4 CFU/mL Protected brush specimen: <10 3 CFU/mL Rationale No evidence that invasive sampling impact clinical outcomes, including changes in antibiotics Non-invasive sampling can be done more rapidly and with fewer complications and resources Kalil AC. Clin Infect Dis. 2016;63:1-51.
8 Selecting Empiric Therapy Antibiotics should be started early and should target potential pathogens Potential pathogens determined by surveillance data and patient-specific risk factors Adequate early antibiotics Superfluous coverage Kalil AC. Clin Infect Dis. 2016;63:1-51.
9 Removal of HCAP Definition 2005 Guidelines HCAP: Healthcare-associated pneumonia Any patient who was hospitalized in an acute care hospital for > 48 hours within prior 90 days Residing in a nursing home or long-term care facility Received recent IV antibiotics, chemotherapy, or wound care in the prior 30 days Attended a hospital or hemodialysis clinic Role: to identify patients at risk for MDRO 2016 Guidelines Removed from guidelines Rationale: new evidence suggesting that many patients identified as HCAP did not have MDRO isolated as a cause of VAP or HAP Am J Respir Crit Care Med. 2005;171: ; Kalil AC. Clin Infect Dis. 2016;63:1-51.
10 Definition of MDRO Microorganisms that are resistant to one or more classes of antimicrobial agents E.g., MRSA, VRE, certain Gram-negative bacilli
11 MDRO Definition in Clinical Studies Reference Pneumonia Type Definition Gross (2014) HCAP/CAP MRSA, Pseudomonas aeruginosa, extended-spectrum beta-lactamase (ESBL)- producing Enterobacteriaceae, carbapenem-intermediate or -resistant Enterobacteriaceae (CIRE), Acinetobacter spp., and Stenotrophomonas maltophilia Chamlers (2014) HCAP/CAP MRSA, Gram-negative Enterobacteriaceae, and P. aeruginosa Valles (2014) HCAP MRSA, P. aeruginosa, S. maltophilia, A. baumannii, Klebsiella spp., and S. marcescens Depuydt (2008) VAP MRSA, ESBL, Acinetobacter spp., Pseudomonas spp., Stenotrophomonas spp. resistant to at least one of the following: ceftazidime, piperacillin, imipenem Giantsou (2005), Trouillet (1998), Martin-Loeches (2013) VAP P. aeruginosa, MRSA, A. baumannii, S. maltophilia Chamlers JD, et al. Clin Infec Dis. 2014;58:330.; Gross AE. Antimicrob Agents Chemother. 2014;58:5262.; Valles J.Intensive Care Med. 2014;40:572.; Depuydt P. Intensive Care Med.2008;34:675.; Giantsou E. Intensive Care Med. 2005;31:1488.; Trouillet JL. Am J Respir Crit Care Med. 1998; 157:531.Martin-Loeches I. Intensive Care Med.2013;39:672.
12 Trends in Antibiotic Use with HCAP 128 VA Hospitals evaluated trends in antibiotic prescribing and antibiotic resistance for pneumonia ,511 hospitalizations were included P-value Antibiotic Use Vancomycin 16% 31% <0.001 Piperacillin-tazobactam 16% 27% <0.001 Ceftriaxone 39% 33% <0.001 Azithromycin 39.5% 36% <0.001 MDRO Pathogens Isolated MRSA 2.5% 2% <0.001 P. aeruginosa 1.9% 2% 0.14 Acinetobacter spp. 0.2% 0.2% 0.17 Jones BE. Clin Infect Dis. 2015;61:
13 Sensitivity and Specificity of HCAP for Identifying MDRO HCAP more often associated with P. aeruginosa, S. aureus, Enterobacteriaceae but overall poor predictor of MDRO Meta-analysis of 24 studies comparing incidence of MDRO HCAP vs CAP found low sensitivity and specificity of HCAP definition Sensitivity Specificity All MDRO 53.7% 71.2% MRSA 69% 65.7% Enterobacteriaceae 42.9% 66.1% Pseudomonas aeruginosa 52.2% 67.7% Chamlers JD, et al. Clin Infec Dis. 2014;58:330.
14 Isolation of MDRO by HCAP Definition Retrospective review characterized the etiology of pneumonia and risk factors for MDRO CAP or HCAP Only 19% had an identifiable etiology Viral pneumonia was the most common cause, followed by S. pneumoniae Overall MDRO prevalence was 3.8% HCAP (n = 258) CAP (n = 263) Any MDRO 5.9% 1.9% MRSA 3.1% 1.1% P. aeruginosa 2.7% 0.8% MDRO independent predictors: Antibiotics in the last 90 days Duration of hospitalization in prior 90 and 180 days P. aeruginosa colonization/infection in the previous 12 months Gross AE. Antimicrob Agents Chemother. 2014;58:5262.
15 Risk Factors for Any MDRO Pneumonia MDRO-VAP vs non-mdro-vap Use of intravenous antibiotics in the past 90 days >5 days of hospitalization prior to VAP Acute respiratory distress syndrome before VAP Renal replacement therapy prior to VAP Septic shock at the time of VAP MDRO-HAP vs non-mdro-hap Use of intravenous antibiotics in the past 90 days
16 Risk factors for MRSA HAP/VAP More common in late-onset (>4 days of hospitalization) than early-onset Major risk factor for MRSA HAP/VAP is prior intravenous antibiotic exposure within 90 days Unclear which antibiotics put patients are higher risk as studies did not evaluate this The role of MRSA nasal surveillance is unclear
17 Case-Control Studies for MRSA HAP/VAP Reference Pneumonia Type Risk Factors OR (95% CI) Wooten (2013) Moreira (2008) Bouza (2012) MRSA vs MSSA pneumonia (all) MRSA vs MSSA VAP MRSA vs non-mrsa VAP Recent antibiotics (w/in 90 days) Tobacco use Illicit drug use Liver disease Previous antibiotic therapy Age >60 years Use of corticosteroids Antibiotic exposure Pleural effusion APACHE II score 7.01 ( ) 2.66 ( ) 3.52 ( ) 3.50 ( ) 5.93 ( ) 5.33 ( ) 5.79 ( ) 2.38 ( ) 2.74 ( ) 1.10 ( ) Wooten DA. Resp Med. 2013;107: ; Moreira MR. Braz J Infect Dis. 2008;12: ; Bouza E. J Hosp Infect. 2012;80:150-5.
18 MRSA Active Surveillance Screening of asymptomatic patients to identify carriers Swab of nares, oropharynx and/or perineum Identification of carriers for intervention to prevent spread of MRSA (e.g., contact precautions) Standard culture or PCR methods
19 Role of Surveillance in Empiric MRSA Treatment Concurrent or recent positive MRSA screen increases the likelihood of respiratory infection with MRSA Better negative predictive value (98%) vs positive predictive value (30%) May have a better role in deciding which patients do NOT need MRSA-active therapy About 30% of respiratory infections due to MRSA are in patients with positive MRSA surveillance studies Recent surveillance (<7 days) is more relevant as patients can acquire MRSA while hospitalized Robicsek A. J Clin Microbiol. 2008;46: Davis KA. Clin Infect Dis. 2004;39: Sarikonda KV. Crit Care Med. 2010;38:
20 Risk factors for MDR P. aeruginosa HAP/VAP Mechanical ventilation COPD Cystic fibrosis or bronchiectasis Prior antibiotic use Specifically carbapenems, broad spectrum cephalosporins and fluoroquinolones Montero M. Eur J Clin Microbiol Infect Dis. 2010;29:335-9.; Parker CM. J Crit Care. 2008;23:18-26.
21 Antibiogram Summary of antimicrobial susceptibilities of bacterial isolates within an institution over a defined period of time Used to track resistance rate over time and to inform clinicians about empiric antibiotic selection IDSA Guidelines on Implementing an Antimicrobial Stewardship Program recommend using a stratified antibiogram over a non-stratified antibiogram Stratified by location (e.g., ICU vs non-icu) or patient age Barlam TF. Clin Infect Dis. 2016;62:e51-77.
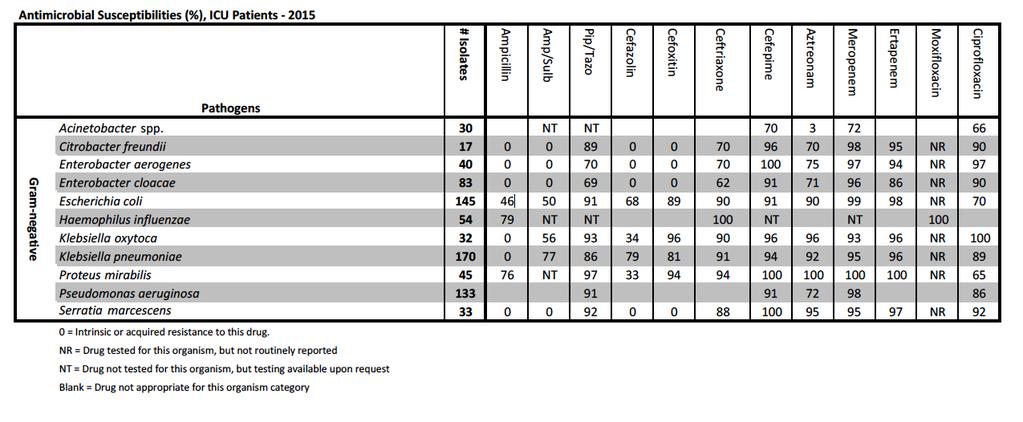
22 Example Antibiogram
23 Empiric Treatment of VAP Initial therapy for VAP should be based on local antibiogram, ideally ICU-specific In absence of local antibiogram data, clinicians should refer to large national and international surveys of organisms and resistance patterns Surveillance studies indicate the most common organisms: S. aureus (20-30%) P. aeruginosa (10-20%) Other enteric Gram-negative organisms (20-40%) A. baumanii (5-10%) Sievert DM. Infect Control Hosp Epidemiol. 2013;34:1-14.
24 Sievert DM. Infect Control Hosp Epidemiol. 2013;34:1-14.
25 Empiric Treatment of VAP S. aureus For empiric coverage, use an agent with activity against Gramnegative bacilli and MSSA Cefepime, piperacillin-tazobactam, levofloxacin, imipenem or meropenem Therapeutic regimen should include an agent targeted at MRSA if: Patient has been exposed to intravenous antibiotics within the prior 90 days Patient being treated in a unit with >10-20% of S. aureus isolates are MRSA or if the prevalence of MRSA is unknown Weak recommendation with low-quality evidence Empiric therapy targeted at MRSA should include Vancomycin or Linezolid


26 Targeted Therapy S. aureus MRSA MSSA Vancomycin Linezolid Oxacillin Nafcillin Cefazolin
27 MRSA Agents Vancomycin vs Linezolid Author Patient population Results Stevens et al. (2002) Kohno et al. (2007) Wunderink et al (2008) Wunderink et al (2012) NS, Not statistically significant Suspected MRSA infection (MRSA pneumonia, n = 64) Suspected MRSA infection (MRSA pneumonia, n = 54) VAP, MRSA (n = 146) HAP or HCAP, MRSA (n = 448) Clinical cure, MRSA pneumonia (NS): Linezolid 52.2% Vancomycin 53.8% Clinical cure, MRSA pneumonia (NS): Linezolid 60% Vancomycin 47.4% Clinical response (NS): Linezolid 66.7% Vancomycin 52.9% Clinical success (p = 0.042): Linezolid 57.6% Vancomycin 46.6% Stevens DL. Clin Infect Dis.2002;34: ; Kohno S. J Antimicrob Chemother. 2007;60: Wunderink RG. Chest. 2008;134: ; Wunderink RG. Clin Infect Dis. 2012;54:621-9.
28 Empiric Treatment of VAP Pseudomonas spp. Two agents targeted at Pseudomonas spp. should be used in the following situations: Patients with prior intravenous antibiotic exposure in the past 90 days Units where >10% of isolates are resistant to an agent being considered for monotherapy or resistance rates are unknown Patients with structural lung disease (e.g., bronchiectasis or cystic fibrosis) Weak recommendation with low-quality evidence Combination therapy increases the likelihood that at least one of the agents used will be active against the pathogen. Monotherapy should be used once an organism has been isolated and susceptibilities are known.
29 Empiric Treatment of VAP Pseudomonas spp. Avoid aminoglycosides and Colistin if alternative agents are available Given poor lung penetration, toxicities, and poorer clinical response Patients randomized to aminoglycoside-containing regimens had similar mortality rates but lower clinical response rates compared to aminoglycoside-free regimens
30 Empiric Treatment of HAP Bacterial etiologies of HAP Non-glucose fermenting Gram-negative bacilli: 19%, Pseudomonas spp. 13% and Acinetobacter spp. 4% Enteric Gram-negative organisms: 16% S. aureus: 16% MRSA 10%, MSSA 6% Kalil AC. Clin Infect Dis. 2016;63:1-51.
31 Empiric Treatment of HAP S. aureus For empiric coverage, use an agent with activity against Gramnegative bacilli and MSSA Cefepime, piperacillin-tazobactam, levofloxacin, imipenem or meropenem) Therapeutic regimen should include an agent targeted at MRSA if: Patient has been exposed to intravenous antibiotics within the prior 90 days Patient being treated in a unit with >20% of S. aureus isolates are MRSA or if the prevalence of MRSA is unknown Patients with high risk of mortality (e.g., patients requiring ventilatory support or with septic shock) Weak recommendation with low-quality evidence Empiric therapy targeted at MRSA should include Vancomycin or Linezolid
32 Empiric Treatment of HAP Pseudomonas spp. Two agents targeted at Pseudomonas spp. should be used in the following situations: Patients with prior intravenous antibiotic exposure in the past 90 days Patients with high risk of mortality (e.g., patients requiring ventilatory support or with septic shock) Patients with structural lung disease (e.g., bronchiectasis or cystic fibrosis) Weak recommendation with low-quality evidence Combination therapy increases the likelihood that at least one of the agents used will be active against the pathogen. Monotherapy should be used once an organism has been isolated and susceptibilities are known.
33 PK/PD Dose Optimization Antibiotic dosing should be determined using PK/PD data, rather than manufacturer s prescribing information Clinical studies have found that PK/PD-optimized dosing results in: Reduced mortality (12% vs 24%, RR 0.49) Reduced ICU length of stay (mean difference -2.48) Improved clinical cure rate (81% vs 64%, RR 1.40)


34 Antimicrobial Therapy PK/PD Pharmacokinetics (drug concentrations) What does the BODY do to the drug? Absorption Distribution Metabolism Elimination PK-PD Drug concentrations and effect Pharmacodynamics (antimicrobial effects) What does the drug do to the BUG? Bacteriostatic/Bactericidal Post-antibiotic effect Minimum inhibitory concentration Owens RC, et al. Am J Health-Syst Pharm 2009;66:S23-30.
35 Static vs Cidal Bacteriostatic Inhibits growth and replication of the organism Require the aid of host defenses to clear infecting microorganisms Agents that alter bacterial physiology such as inhibition of folate synthesis (e.g. sulfonamides) Bactericidal Directly cause cell death Agents that interfere with the development of the cell wall or membrane (e.g. beta-lactams, vancomycin) Agents that inhibit nucleic acid synthesis (e.g. fluoroquinolones) or protein synthesis (e.g. aminoglycosides) Levison ME, et al. Infect Dis Clin North Am 2009:23:
36 Minimum inhibitory concentration (MIC) The minimal concentration of antibiotic that inhibits bacterial growth The MIC usually represents attainable concentrations in serum Concentrations at the site of infection may be higher (e.g. urine) or lower (e.g. CSF) Antimicrobials have variable lung penetration March 27,
37 Interpreting MIC Values GREATER THAN 10,000 COLONIES PER ML. ESCHERICHIA COLI ANTIBIOTIC MIC (mcg/ml) INTERPRETATION Ampicillin <= Susceptible Amp/Sulbactam / Susceptible Piper/Tazo / Susceptible Cefazolin <= Susceptible Cefoxitin Susceptible Ceftriaxone <= Susceptible Cefepime <= Susceptible Aztreonam <= Susceptible Meropenem <= Susceptible Ertapenem <= Susceptible Trimeth/Sulfa <=0.5/ Susceptible Tetracycline Intermediate Gentamicin <= Susceptible Tobramycin <= Susceptible Amikacin <= Susceptible Ciprofloxacin > Resistant Nitrofurantoin <= Susceptible Susceptible: strain can be treated with antibiotic at recommended doses and schedules. Useful to know when treating an organism in an area that is difficult to penetrate (CSF, osteomyelitis) Intermediate:antibiotic level can usually be obtained in the tissue or blood, but response may be diminished Resistant: growth not inhibited by usually achievable concentrations at normal doses
38 PK-PD Principles of Antibiotics Time-Dependent ft>mic: The cumulative percentage of a 24 hour period that the drug exceeds the MIC E.g., β-lactams fauc/mic The ratio of the area under the curve to the MIC E.g., vancomycin, fluoroquinolones Concentration-Dependent fcmax/mic The ratio of maximal drug concentration to the MIC E.g., aminoglycosides Mandell, Douglas and Bennet s Principles and Practice of Infectious Diseases. 7th ed. 38
39 PK-PD Measures of Antibiotics Aminoglycosides fc max /MIC Drug Concentration Fluoroquinolones fauc/mic Beta-lactams ft>mic Time MIC Figure adapted from Amsden G et al. Pharmacokinetics and Pharmacodynamics of Anti-infectives. Mandell, Douglas and Bennett s Principles and Practice of Infectious Diseases. 7th ed Print. 39
40 PK-PD Targets of Beta-Lactams Drug Class Bacteriostatic %ft > MIC Bactericidal %ft > MIC Post-Antibiotic Effect Penicillins ~30% ~50% 0.1 hours for Gram-negatives hours for Gram-positives Cephalosporins 35-40% 60-70% None for Gram-negative hours for Gram-positives Carbapenems 20% 40% 0.9 for Gram-negatives hours for Gram-positive Post-Antibiotic Effect: time of growth suppression after drug exposure has fallen below MIC Drusano GL. Clin Inect Dis 2007;45:S Ambrose P. et al. Clin Infect. Dis 2007;44: George JM, et al. Pharmacotherapy 2012;32:
41 Administration Strategies for Antibiotics Time (hours)
42 PK/PD Optimization for Pneumonia Agent PK/PD Parameter Manufacturer Dosing Optimized Regimen Levofloxacin AUC/MIC >87 HAP/VAP: 750 mg once daily 750 mg once daily Ciprofloxacin AUC/MIC >125 Nosocomial pneumonia: 400 mg IV Q8H 400 mg Q8H Ceftazidime % T>MIC Uncomplicated pneumonia: 1 g Q8H Cefepime 100% T>MIC Pneumonia (P. aeruginosa): 2 g Q8H Meropenem 54% T>MIC, Cmin:MIC>5 OR 75% T>MIC Pneumonia (not P. aeruginosa): 1-2 g Q8-12H Not in labeling 2 g Q8H over 3 hour infusion 2 g Q8H over 3 hour infusion 1 g Q8H over 3 hour infusion
43 Cefepime Probability of varying regimens achieving >50% T>MIC With an MIC of 8 mcg/ml Standard infusion over 30- minutes 1 g Q12H: 50% 2 g Q12H: 75% 1 g Q8H: 70% 2 g Q8H: 85% Prolonged infusion over 3-hours 2 g Q8H: 95% Nicasio AM. Antimicrob Agents Chemother.2009;53:
44 Duration of Therapy Both HAP and VAP should be treated for 7 days, rather than a longer duration Strong recommendation, moderate quality evidence Short courses (7-8 days) are associated with: Increased 28-day antibiotic-free days (mean 4.02 days) Reduced recurrent VAP due to MDRO (42.1% vs 62.3%) No differences in mortality, recurrent pneumonia, treatment failure, hospital length of stay or duration of mechanical ventilation
45 De-escalation of Therapy De-escalation refers to changing from an empiric broad-spectrum antibiotic to a narrower antibiotic regimen Antibiotic therapy should be de-escalated, rather than fixed
46 Procalcitonin (PCT) Produced by parenchymal tissue throughout the body when stimulated by endotoxin and bacterial infection PCT should not be used to diagnosis HAP/VAP When combined with clinical criteria, it has a sensitivity of 67% and specificity of 83% PCT combined with clinical criteria can guide discontinuation of antibiotics Resulted in shorter duration of antibiotic therapy (9.1 vs 12.1 days; P <.00001) with no effect on clinical outcomes Kalil AC. Clin Infect Dis. 2016;63:1-51.; Stolz D. Eur Respir J. 2009;34: ; Bouadma L. Lancet. 2010;375:
47 strem-1 Member of immunoglobulin superfamily strongly expressed on neutrophils and monocytes infiltrating tissues invaded by bacteria and fungi Measured in BAL fluid, cutoff values have not been validated strem-1 should not be used to diagnose HAP/VAP Sensitivity of 84% and specificity of 49% as a diagnostic tool
48 Clinical Pulmonary Infection Score (CPIS) 0 Points 1 Point 2 Points Temperature (C) or 39 Peripheral WBC 4,000-11,000 <4,000 or >11,000, >50% bands: add 1 point Tracheal secretions None Non-purulent Purulent Chest x-ray No infiltrate Diffuse or patchy infiltrates Localized infiltrate Progression of infiltrate from prior radiographs None Culture of ET suction No growth/light growth Heavy growth, same bacteria on Gram stain: add 1 point Progression Oxygenation (PaO2/FiO2) >240 or ARDS 240 and no ARDS If CPIS 6, VAP unlikely. If CPIS remains 6 after 3 days, antibiotics can be stopped in most cases
49 CPIS Recommend clinical criteria alone to determine initiation and discontinuation of antibiotics CPIS should not be used to diagnose HAP or VAP Low diagnostic sensitivity (65%) and specificity (64%) for VAP
50 Summary Empiric antibiotic therapy for HAP and VAP should be based on patient-specific risk factors for MDRO Local, stratified antibiograms should be used to guide empiric treatment of HAP and VAP Antimicrobial dosing should be optimized based on PK/PD parameters, when feasible PCT levels, combined with clinical criteria, may be used to guide discontinuation of antibiotics
51 2016 Updates to the Hospital Acquired- and Ventilator Associated-Pneumonia Guidelines Janessa M. Smith, PharmD, BCPS Clinical Pharmacy Specialist, Infectious Diseases The Johns Hopkins Hospital
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
Management of Hospital-acquired Pneumonia
 Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship
 Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
NEW ATS/IDSA VAP-HAP GUIDELINES
 NEW ATS/IDSA VAP-HAP GUIDELINES MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the University
NEW ATS/IDSA VAP-HAP GUIDELINES MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the University
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases
 The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia. Po-Ren Hsueh. National Taiwan University Hospital
 Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Introduction to Pharmacokinetics and Pharmacodynamics
 Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Mono- versus Bitherapy for Management of HAP/VAP in the ICU
 Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Antimicrobial stewardship in managing septic patients
 Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Clinical Infectious Diseases IDSA GUIDELINE
 Clinical Infectious Clinical Diseases Infectious Diseases Advance Access published July 14, 2016 IDSA GUIDELINE Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical
Clinical Infectious Clinical Diseases Infectious Diseases Advance Access published July 14, 2016 IDSA GUIDELINE Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical
Sustaining an Antimicrobial Stewardship
 Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Understanding the Hospital Antibiogram
 Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Not for patients with immunosuppression.
 CID Sept 2016 (previous 2005). Littérature: jusque nov.2015. 18 experts dont un Espagnol ( J Carratalà), un Allemand (S Ewig) et un Australien (JA Roberts). ATS/IDSA/SHEA/SCCM 25 items; 50 pages Sept 2017
CID Sept 2016 (previous 2005). Littérature: jusque nov.2015. 18 experts dont un Espagnol ( J Carratalà), un Allemand (S Ewig) et un Australien (JA Roberts). ATS/IDSA/SHEA/SCCM 25 items; 50 pages Sept 2017
CF WELL Pharmacology: Microbiology & Antibiotics
 CF WELL Pharmacology: Microbiology & Antibiotics Bradley E. McCrory, PharmD, BCPS Clinical Pharmacy Specialist Pulmonary Medicine Cincinnati Children s Hospital Medical Center January 26, 2017 Disclosure
CF WELL Pharmacology: Microbiology & Antibiotics Bradley E. McCrory, PharmD, BCPS Clinical Pharmacy Specialist Pulmonary Medicine Cincinnati Children s Hospital Medical Center January 26, 2017 Disclosure
CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE)
") CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE) Bartsch SM et al. Potential economic burden of carbapenem-resistent Enterobacteriaceae (CRE) in the United States. Clin Microbiol Infect 2017;23(1):48e9-e16.
CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE) Bartsch SM et al. Potential economic burden of carbapenem-resistent Enterobacteriaceae (CRE) in the United States. Clin Microbiol Infect 2017;23(1):48e9-e16.
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY*
 44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
Fighting MDR Pathogens in the ICU
 Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Outline. Antimicrobial resistance. Antimicrobial resistance in gram negative bacilli. % susceptibility 7/11/2010
 Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Detection and Quantitation of the Etiologic Agents of Ventilator Associated Pneumonia in Endotracheal Tube Aspirates From Patients in Iran
 Letter to the Editor Detection and Quantitation of the Etiologic Agents of Ventilator Associated Pneumonia in Endotracheal Tube Aspirates From Patients in Iran Mohammad Rahbar, PhD; Massoud Hajia, PhD
Letter to the Editor Detection and Quantitation of the Etiologic Agents of Ventilator Associated Pneumonia in Endotracheal Tube Aspirates From Patients in Iran Mohammad Rahbar, PhD; Massoud Hajia, PhD
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Antimicrobial Susceptibility Testing: Advanced Course
 Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance
 Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
New Drugs for Bad Bugs- Statewide Antibiogram
 New Drugs for Bad Bugs- Statewide Antibiogram Felicia Matthews, Pharm.D., BCPS Senior Consultant, Pharmacy Specialty BE MedMined Services Disclosures Employee of BD Corporation MedMined Services Agenda
New Drugs for Bad Bugs- Statewide Antibiogram Felicia Matthews, Pharm.D., BCPS Senior Consultant, Pharmacy Specialty BE MedMined Services Disclosures Employee of BD Corporation MedMined Services Agenda
Sepsis is the most common cause of death in
 ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles
 Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Antibiotic treatment in the ICU 1. ICU Fellowship Training Radboudumc
 Antibiotic treatment in the ICU 1 ICU Fellowship Training Radboudumc Main issues Delayed identification of microorganisms Impact of critical illness on Pk/Pd High prevalence of antibiotic resistant strains
Antibiotic treatment in the ICU 1 ICU Fellowship Training Radboudumc Main issues Delayed identification of microorganisms Impact of critical illness on Pk/Pd High prevalence of antibiotic resistant strains
2012 ANTIBIOGRAM. Central Zone Former DTHR Sites. Department of Pathology and Laboratory Medicine
 2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Successful stewardship in hospital settings
 Successful stewardship in hospital settings Pr Charles-Edouard Luyt Service de Réanimation Institut de Cardiologie Groupe Hospitalier Pitié-Salpêtrière Université Pierre et Marie Curie, Paris 6 www.reamedpitie.com
Successful stewardship in hospital settings Pr Charles-Edouard Luyt Service de Réanimation Institut de Cardiologie Groupe Hospitalier Pitié-Salpêtrière Université Pierre et Marie Curie, Paris 6 www.reamedpitie.com
2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania
 2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania Day 1: Saturday 30 th September 2017 09:00 09:20 Registration
2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania Day 1: Saturday 30 th September 2017 09:00 09:20 Registration
Int.J.Curr.Microbiol.App.Sci (2017) 6(3):
 6(3):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
Management of hospital-acquired pneumonia and ventilator-associated pneumonia: an ERS/ESICM/ESCMID/ ALAT guideline
 ERS pocket guidelines Management of hospital-acquired pneumonia and ventilator-associated pneumonia: an ERS/ESICM/ESCMID/ ALAT guideline From the Task Force for the Management of Hospital-acquired Pneumonia
ERS pocket guidelines Management of hospital-acquired pneumonia and ventilator-associated pneumonia: an ERS/ESICM/ESCMID/ ALAT guideline From the Task Force for the Management of Hospital-acquired Pneumonia
FM - Male, 38YO. MRSA nasal swab (+) Due to positive MRSA nasal swab test, patient will be continued on Vancomycin 1500mg IV q12 for MRSA treatment...
 Due to positive MRSA nasal swab test, patient will be continued on Vancomycin 1500mg IV q12 for MRSA treatment...") Jillian O Keefe Doctor of Pharmacy Candidate 2016 September 15, 2015 FM - Male, 38YO HPI: Previously healthy male presents to ED febrile (102F) and in moderate distress ~2 weeks after getting a tattoo
Jillian O Keefe Doctor of Pharmacy Candidate 2016 September 15, 2015 FM - Male, 38YO HPI: Previously healthy male presents to ED febrile (102F) and in moderate distress ~2 weeks after getting a tattoo
ESISTONO LE HCAP? Francesco Blasi. Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano
 ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
Antimicrobial de-escalation in the ICU
 Antimicrobial de-escalation in the ICU A FOCUS ON EVIDENCE-BASED STRATEGIES Dave Leedahl, PharmD, BCPS-AQ ID, BCCCP Pharmacy Clinical Manager Sanford Health Fargo, ND, USA I have no conflicts of interest
Antimicrobial de-escalation in the ICU A FOCUS ON EVIDENCE-BASED STRATEGIES Dave Leedahl, PharmD, BCPS-AQ ID, BCCCP Pharmacy Clinical Manager Sanford Health Fargo, ND, USA I have no conflicts of interest
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate
 Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania
 2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania Day 1: Saturday 30 th September 2017 Time Topic/Activity
2017 Introduction to Infectious Diseases Clinical Seminar Saturday 30th September - Sunday 1st October 2017 Hotel Grand Chancellor Hobart, Tasmania Day 1: Saturday 30 th September 2017 Time Topic/Activity
Antimicrobial Cycling. Donald E Low University of Toronto
 Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIII NUMBER 1 July 2008 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell, SM (ASCP), Marti Roe SM (ASCP), Ann-Christine Nyquist MD, MSPH Are the bugs winning? The 2007
VOLUME XXIII NUMBER 1 July 2008 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell, SM (ASCP), Marti Roe SM (ASCP), Ann-Christine Nyquist MD, MSPH Are the bugs winning? The 2007
Community Acquired Pneumonia. Epidemiology: Acute Lower Respiratory Tract Infections. Community Acquired Pneumonia (CAP) Outline
 Outline") Community Acquired Pneumonia (CAP) Outline Lisa G. Winston, MD University of California, San Francisco Zuckerberg San Francisco General Epidemiology Diagnosis Microbiology Risk stratification Treatment
Community Acquired Pneumonia (CAP) Outline Lisa G. Winston, MD University of California, San Francisco Zuckerberg San Francisco General Epidemiology Diagnosis Microbiology Risk stratification Treatment
Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them?
 Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them? Roberta B. Carey, PhD Centers for Disease Control and Prevention Division of Healthcare Quality Promotion Why worry? MDROs Clinical
Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them? Roberta B. Carey, PhD Centers for Disease Control and Prevention Division of Healthcare Quality Promotion Why worry? MDROs Clinical
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Prevalence of Metallo-Beta-Lactamase Producing Pseudomonas aeruginosa and its antibiogram in a tertiary care centre
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 952-956 http://www.ijcmas.com Original Research Article Prevalence of Metallo-Beta-Lactamase
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 952-956 http://www.ijcmas.com Original Research Article Prevalence of Metallo-Beta-Lactamase
Nosocomial Infections: What Are the Unmet Needs
 Nosocomial Infections: What Are the Unmet Needs Jean Chastre, MD Service de Réanimation Médicale Hôpital Pitié-Salpêtrière, AP-HP, Université Pierre et Marie Curie, Paris 6, France www.reamedpitie.com
Nosocomial Infections: What Are the Unmet Needs Jean Chastre, MD Service de Réanimation Médicale Hôpital Pitié-Salpêtrière, AP-HP, Université Pierre et Marie Curie, Paris 6, France www.reamedpitie.com
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Best Practices: Goals of Antimicrobial Stewardship
 Best Practices: Goals of Antimicrobial Stewardship Gail Scully, M.D, M.P.H. and Elizabeth Radigan, PharmD, BCPS UMass Memorial Medical Center Division of Infectious Disease Department of Medicine September
Best Practices: Goals of Antimicrobial Stewardship Gail Scully, M.D, M.P.H. and Elizabeth Radigan, PharmD, BCPS UMass Memorial Medical Center Division of Infectious Disease Department of Medicine September
Antimicrobial Stewardship Strategy: Antibiograms
 Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Burton's Microbiology for the Health Sciences. Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents
 Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
Burton's Microbiology for the Health Sciences Chapter 9. Controlling Microbial Growth in Vivo Using Antimicrobial Agents Chapter 9 Outline Introduction Characteristics of an Ideal Antimicrobial Agent How
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland
 Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
Surveillance of Antimicrobial Resistance among Bacterial Pathogens Isolated from Hospitalized Patients at Chiang Mai University Hospital,
 Original Article Vol. 28 No. 1 Surveillance of Antimicrobial Resistance:- Chaiwarith R, et al. 3 Surveillance of Antimicrobial Resistance among Bacterial Pathogens Isolated from Hospitalized Patients at
Original Article Vol. 28 No. 1 Surveillance of Antimicrobial Resistance:- Chaiwarith R, et al. 3 Surveillance of Antimicrobial Resistance among Bacterial Pathogens Isolated from Hospitalized Patients at
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Learning Points. Raymond Blum, M.D. Antimicrobial resistance among gram-negative pathogens is increasing
 Raymond Blum, M.D. Learning Points Antimicrobial resistance among gram-negative pathogens is increasing Infection with antimicrobial-resistant pathogens is associated with increased mortality, length of
Raymond Blum, M.D. Learning Points Antimicrobial resistance among gram-negative pathogens is increasing Infection with antimicrobial-resistant pathogens is associated with increased mortality, length of
Bad Bugs. Pharmacist Learning Objectives. Antimicrobial Resistance. Patient Case. Pharmacy Technician Learning Objectives 4/8/2016
 Pharmacist Learning Objectives Antimicrobial Resistance Julie Giddens Pharm D, BCPS Infectious Disease Clinical Pharmacist OSF Saint Francis Medical Center Peoria, IL The speaker has no conflicts to disclose
Pharmacist Learning Objectives Antimicrobial Resistance Julie Giddens Pharm D, BCPS Infectious Disease Clinical Pharmacist OSF Saint Francis Medical Center Peoria, IL The speaker has no conflicts to disclose
Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy
 Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy Leonardo Pagani MD Director Unit for Hospital Antimicrobial Chemotherapy
Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy Leonardo Pagani MD Director Unit for Hospital Antimicrobial Chemotherapy
Pharmacokinetics and Pharmacodynamics of Antimicrobials in the Critically Ill Patient
 Pharmacokinetics and Pharmacodynamics of Antimicrobials in the Critically Ill Patient Rania El-Lababidi, Pharm.D., BCPS (AQ-ID), AAHIVP Manager, Pharmacy Education and Training Cleveland Clinic Abu Dhabi
Pharmacokinetics and Pharmacodynamics of Antimicrobials in the Critically Ill Patient Rania El-Lababidi, Pharm.D., BCPS (AQ-ID), AAHIVP Manager, Pharmacy Education and Training Cleveland Clinic Abu Dhabi
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Jerome J Schentag, Pharm D
 Clinical Pharmacy and Optimization of Antibiotic Usage: How to Use what you have Learned in Pharmacokinetics and Pharmacodynamics of Antibiotics Jerome J Schentag, Pharm D Presented at UCL on Thursday
Clinical Pharmacy and Optimization of Antibiotic Usage: How to Use what you have Learned in Pharmacokinetics and Pharmacodynamics of Antibiotics Jerome J Schentag, Pharm D Presented at UCL on Thursday
Combating Antimicrobial Resistance with Extended Infusion Beta-lactams. Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident
 Combating Antimicrobial Resistance with Extended Infusion Beta-lactams Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident Disclosure The presenter has no conflicts of interest to disclose with material
Combating Antimicrobial Resistance with Extended Infusion Beta-lactams Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident Disclosure The presenter has no conflicts of interest to disclose with material
Disclosure. Objectives. Combating Antimicrobial Resistance with Extended Infusion Beta-lactams
 Combating Antimicrobial Resistance with Extended Infusion Beta-lactams Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident Disclosure The presenter has no conflicts of interest to disclose with material
Combating Antimicrobial Resistance with Extended Infusion Beta-lactams Stephen Andrews, PharmD PGY-1 Pharmacy Practice Resident Disclosure The presenter has no conflicts of interest to disclose with material
Lack of Change in Susceptibility of Pseudomonas aeruginosa in a Pediatric Hospital Despite Marked Changes in Antibiotic Utilization
 Infect Dis Ther (2014) 3:55 59 DOI 10.1007/s40121-014-0028-8 BRIEF REPORT Lack of Change in Susceptibility of Pseudomonas aeruginosa in a Pediatric Hospital Despite Marked Changes in Antibiotic Utilization
Infect Dis Ther (2014) 3:55 59 DOI 10.1007/s40121-014-0028-8 BRIEF REPORT Lack of Change in Susceptibility of Pseudomonas aeruginosa in a Pediatric Hospital Despite Marked Changes in Antibiotic Utilization
BACTERIAL SUSCEPTIBILITY REPORT: 2016 (January 2016 December 2016)
") BACTERIAL SUSCEPTIBILITY REPORT: 2016 (January 2016 December 2016) VA Palo Alto Health Care System April 14, 2017 Trisha Nakasone, PharmD, Pharmacy Service Russell Ryono, PharmD, Public Health Surveillance
BACTERIAL SUSCEPTIBILITY REPORT: 2016 (January 2016 December 2016) VA Palo Alto Health Care System April 14, 2017 Trisha Nakasone, PharmD, Pharmacy Service Russell Ryono, PharmD, Public Health Surveillance
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Infectious Disease Update 2017
 Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Antimicrobial Stewardship/Statewide Antibiogram. Felicia Matthews Senior Consultant, Pharmacy Specialty BD MedMined Services
 Antimicrobial Stewardship/Statewide Antibiogram Felicia Matthews Senior Consultant, Pharmacy Specialty BD MedMined Services Disclosures Employee of BD Corporation MedMined Services Agenda CMS and JCAHO
Antimicrobial Stewardship/Statewide Antibiogram Felicia Matthews Senior Consultant, Pharmacy Specialty BD MedMined Services Disclosures Employee of BD Corporation MedMined Services Agenda CMS and JCAHO
Multi-drug resistant microorganisms
 Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Jump Starting Antimicrobial Stewardship
 Jump Starting Antimicrobial Stewardship Amanda C. Hansen, PharmD Pharmacy Operations Manager Carilion Roanoke Memorial Hospital Roanoke, Virginia March 16, 2011 Objectives Discuss guidelines for developing
Jump Starting Antimicrobial Stewardship Amanda C. Hansen, PharmD Pharmacy Operations Manager Carilion Roanoke Memorial Hospital Roanoke, Virginia March 16, 2011 Objectives Discuss guidelines for developing
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Optimize Durations of Antimicrobial Therapy
 Optimize Durations of Antimicrobial Therapy Evidence & Application Jill Cowper, Pharm.D. Division Infectious Diseases Pharmacist Parallon Supply Chain Solutions Richmond, VA P: 607 221 5101 jill.butterfield@parallon.com
Optimize Durations of Antimicrobial Therapy Evidence & Application Jill Cowper, Pharm.D. Division Infectious Diseases Pharmacist Parallon Supply Chain Solutions Richmond, VA P: 607 221 5101 jill.butterfield@parallon.com
These recommendations were approved for use by the Pharmaceutical and Therapeutics Committee, RCWMCH on 1 February 2017.
 Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS
 PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Pharmacodynamics as an Approach to Optimizing Therapy Against Problem Pathogens
 Pharmacodynamics as an Approach to Optimizing Therapy Against Problem Pathogens Jared L. Crandon, Pharm.D., BCPS Associate Director, Clinical and Experimental Pharmacology Center for Anti-Infective Research
Pharmacodynamics as an Approach to Optimizing Therapy Against Problem Pathogens Jared L. Crandon, Pharm.D., BCPS Associate Director, Clinical and Experimental Pharmacology Center for Anti-Infective Research
a. 379 laboratories provided quantitative results, e.g (DD method) to 35.4% (MIC method) of all participants; see Table 2.
 to 35.4% (MIC method) of all participants; see Table 2.") AND QUANTITATIVE PRECISION (SAMPLE UR-01, 2017) Background and Plan of Analysis Sample UR-01 (2017) was sent to API participants as a simulated urine culture for recognition of a significant pathogen colony
AND QUANTITATIVE PRECISION (SAMPLE UR-01, 2017) Background and Plan of Analysis Sample UR-01 (2017) was sent to API participants as a simulated urine culture for recognition of a significant pathogen colony
MAGNITUDE OF ANTIMICROBIAL USE. Antimicrobial Stewardship in Acute and Long Term Healthcare Facilities: Design, Implementation and Challenges
 Antimicrobial Stewardship in Acute and Long Term Healthcare Facilities: Design, Implementation and Challenges John A. Jernigan, MD, MS Division of Healthcare Quality Promotion Centers for Disease Control
Antimicrobial Stewardship in Acute and Long Term Healthcare Facilities: Design, Implementation and Challenges John A. Jernigan, MD, MS Division of Healthcare Quality Promotion Centers for Disease Control
Antibiotic Resistance in the Post-Acute and Long-Term Care Settings: Strategies for Stewardship
 Antibiotic Resistance in the Post-Acute and Long-Term Care Settings: Strategies for Stewardship J. Hudson Garrett Jr., PhD, MSN, MPH, FNP-BC, PLNC, CDONA, IP-BC, GDCN, CDP, CADDCT, CALN, VA-BC, AS-BC,
Antibiotic Resistance in the Post-Acute and Long-Term Care Settings: Strategies for Stewardship J. Hudson Garrett Jr., PhD, MSN, MPH, FNP-BC, PLNC, CDONA, IP-BC, GDCN, CDP, CADDCT, CALN, VA-BC, AS-BC,
Original Articles. K A M S W Gunarathne 1, M Akbar 2, K Karunarathne 3, JRS de Silva 4. Sri Lanka Journal of Child Health, 2011; 40(4):
:") Original Articles Analysis of blood/tracheal culture results to assess common pathogens and pattern of antibiotic resistance at medical intensive care unit, Lady Ridgeway Hospital for Children K A M S
Original Articles Analysis of blood/tracheal culture results to assess common pathogens and pattern of antibiotic resistance at medical intensive care unit, Lady Ridgeway Hospital for Children K A M S
2015 Antibiogram. Red Deer Regional Hospital. Central Zone. Alberta Health Services
 2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site