Electronic Record Exchange: The New Normal
|
|
|
- Derrick Newton
- 6 years ago
- Views:
Transcription

1 Electronic Record Exchange: The New Normal
2 Target Audience: Pharmacists ACPE#: L04-P Activity Type: Application-based
3 Disclosures Suzanne Higginbotham no conflicts to disclose Amina Abubakar no conflicts to disclose The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
4 Learning Objectives 1. Describe the legal requirements for maintaining accurate, perpetual patient care records for all patient care services. 2. Explain the concepts and application of Systemized Nomenclature of Medicine Clinical Terms and its relationship to standardized documentation, exchange, and reporting of patient care services. 3. Develop accurate and concise patient care documentation using a patient case example for both initial Target and follow-up Audience: care. 4. Describe methods for electronic exchange of information, including DIRECT and the use of health information exchanges ACPE#: 5. Explain the functionality of the Pharmacist ecare Plan and the system functionality being built by pharmacy management system vendors to enable pharmacists to create and exchange patient Activity care information. Type: 6. List the components of the Pharmacy Care Note template and identify appropriate information to include in each section.
5 1. Assessment Question Pharmacists are required to maintain patient health records that A. Are retained for five years B. Are stored physically on site C. Accessible to patients D. Include only medications and information related to the medication use
6 2. Assessment Question SNOWMED CT coding is a required form of documentation in which platform? A. JCCP Pharmacists Patient Care Process B. Diabetes self management education (DSME) sessions C. Tobacco cessation group facilitation sessions D. Pharmacist ecare Plan
7 3. Assessment Question Which of the following is a component of the assessment section in a clinical soap note A. Patient blood pressure is 132/88 B. Uncontrolled on current therapy of HCTZ 25mg once daily C. Initiate lisinopril 25mg once daily D. Patient reports eating foods high in sodium
8 4. Assessment Question Which of the following is not a core section of the Pharmacist ecare Plan? A. Goals B. Vital Signs C. Interventions D. Payer
9 5. Assessment Question Which of the following acts as an intermediary on behalf of an information exchange participant? A. HISP B. TITRS C. MIPS D. ACO
10 6. Assessment Question Pharmacy management systems have evolved to allow for this type of functionality as community pharmacists are offering more clinical services. A. Ability to create actions and tasks B. Utilization of care templates C. Ability to collect labs D. All of the above


11 Introduction Evolution of Healthcare Data Exchange Care Coordination Preparation for Provider Status Graphic retrieved from on January 8, 2018.
12 Describe the legal requirements for maintaining accurate, perpetual patient care records for all patient care services Suzanne Higginbotham
13 Purpose of Documentation Serves as a record of what has been done Efforts to achieve desired patient outcomes Evaluates patient progress Legal requirement Compliance with laws & regulations of patient records Billing purposes
14 Purpose of Documentation Form of communication among health care professionals Enhances continuity of care Standardized systematic process of care Demonstrates value of pharmacist-provided MTM services Clinical, economic and humanistic outcomes
15 Documentation and the Pharmacists Patient Care Process Foundational component of the Pharmacists Patient Care Process Led by Joint Commission of Pharmacy Practitioners (JCPP) Provides a consistent process for pharmacist-delivered care Applicable to any practice setting and any patient service where pharmacists provide care

16 The Pharmacists Patient Care Process
17 Legal Requirements Pharmacists are required to maintain medical records that are Complete Accurate Accessible Stored appropriately Retained



18 Patient Health Records Complete and Accurate Information Legible Promptly completed
19 Patient Health Records Should include at a minimum Patient identification Pertinent medical history and results of physical examination Allergies and known drug reactions Patient consent Notes by authorized staff members and individuals who have been granted clinical privileges Written recommendations/instructions given to the patient Significant medical advice given to a patient by telephone AHIMA EHR Practice Council. "Developing a Legal Health Record Policy: Appendix A." Journal of AHIMA 78, no. 9 (Oct. 2007): Web extra. Available online in the AHIMA Body of Knowledge at Accessed January 2, 2018
20 Patient Health Records Accessible To patients or patient designees Given access or as a copy To other HCP Given access to necessary information for intended purposes
21 Patient Health Records Medical records should be stored to provide protection from loss, damage or unauthorized access Under HIPAA, covered entities must Have safeguards to protect private information Limit use and sharing to the minimum necessary to accomplish intended purpose Establish agreements with service providers to perform functions or activities on their behalf Establish policies and procedures outlining who can access patient health information accessed January 2, 2018
22 Patient Health Records Retention of information is controlled by Federal legislation Provincial standards of practice Health Information Act
23 Health Records Electronic patient health records should be maintained for a minimum of Six years under HIPAA law 45CFR (j)(2) By the governing state board of pharmacy Whichever notes the longer period of time
24 Explain the concepts and application of Systemized Nomenclature of Medicine Clinical Terms and its relationship to standardized documentation, exchange, and reporting of patient care services Suzanne Higginbotham
25 Systemized Nomenclature of Medicine Clinical Terms (SNOWMED CT) A standardized, multilingual vocabulary of terminology Used by healthcare professionals for the electronic exchange of clinical health information Owned and maintained by the International Health Terminology Standards Development Organization (IHTSDO) Can be mapped to other coding systems, such as ICD-10, which helps to facilitate semantic interoperability Codes are searchable and available for free from the National Library of Medicine (NLM) accessed January 2, 2018 SKH1
26 Slide 25 SKH1 Suzanne Higginbotham, 1/16/2018
27 Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) Used for documenting and communicating diagnoses, procedures, and clinical information A pharmacy progress note is mapped as numbers backed to clinical terms or concepts Data must be codified into discrete data points that can be shared between providers and healthcare settings Standardization is key to interoperability Contains 300,000+ codes within value sets to streamline documentation Implementing SNOMED CT in Practice: A Beginner s Guide, Pharmacy Health Information Technology Collaborative, retrieved from accessed December 12, 2016.
28 Pharmacists and Documentation Pharmacists document in a variety of practice settings Progress notes are utilized to note patient assessments and findings Capture and measure the value of the care provided SNOMED CT codes allow pharmacists documentation to become more standardized Efficient and precise billing for services Effective communication of medication-related problems, medication history, and associated service activities with other care team members
29 Standardized Framework for Cross Walking MTM Services to SNOMED CT Codes Consensus document developed by a broad array of pharmacy stakeholders SNOMED CT codes are mapped to medication-related terms and definitions Codes can be incorporated into healthcare software to facilitate electronic documentation of patient care services In August 2017, The Pharmacy HIT Collaborative announced an updated release of SNOWMED CT value sets (originally published 2016) Over 20 pharmacy software vendors have adopted Medicare Part D Enhanced MTM model and Pharmacist ecare Plan project both require SNOMED CT codes for documentation Standardized Framework for Cross-Walking Medication Therapy Management (MTM) Services to SNOMED CT Codes, Joint Commission of Pharmacy Practitioners Workgroup, retrieved from accessed December 12, 2016.
30 SNOMED CT Examples SNOMED CT Concept SNOMED CT ID Referred by primary care physician Patient unable to obtain medication Medication dose too low Hypertension medication review Rheumatologic disorder education Recommendation to increase dose Medication reconciliation by pharmacist Hemoglobin A1c <7% Adverse reaction to drug UMLS SNOMED CT Browser. National Library of Medicine, National Institute of Health
31 SOAP Note Documentation with SNOMED CT Codes Embedded Electronically HIE Documentation Sample
32 S: PH is a 64 y.o. female, reported to the XYZ Pharmacy for a follow-up MTM session. CC: Patient sprained her left knee on Sunday (pain reported 8/10) PMH: Gout and HTN SH/FH: no changes since last visit HPI: No s/sx of gout noted after d/c of colchicine. Patient stated last uric acid lab was WNL. Preventive Care: Up to date on vaccines (PNU 2013, Zoster 2013, Flu 2016, Tdap 2015) DXA 2015 Medication: Glucosamine 500 mg, take 3 capsules three times daily Aspirin 81 mg daily Losartan 50 mg daily Atenolol 50 mg every 12 hours KlorCon Tablet 10 meq daily Furosemide 20 mg every morning Calcium Carbonate 600 mg + D 400 IU at bedtime Fluticasone NS twice daily during winter Loratadine 10 mg every night Aleve every 12 hours Adherence: Pt reports adherence with all meds except Atenolol only been taking morning doses b/c out of refills and trying to save pills O: Height: 64.5 in, Weight = lbs, BMI = 44.7, BP = 174/90 mmhg, Pulse = 83, Pulse Ox = 98% A/P: 1. Hypertension Uncontrolled on current therapy (goal < 150/90, JNC VIII). Advised patient to take Atenolol twice daily and Atenolol refilled at pharmacy. Pharmacist will follow up with patient in 1 week with BP check. If BP is still elevated, pharmacist will contact Dr. Johnson to adjust hypertensive regimen. 2. Pain Uncontrolled on current therapy and inappropriate therapy. Received cortisone injection Friday and sprained left knee on Sunday. Recommend to Dr. Levin to reinitiate Meloxicam 7.5 mg daily and d/c Aleve. If pain is not controlled by Meloxicam 7.5 mg after two weeks, consider increasing doage to Meloxicam 15 mg daily (per American College of Rheumatology Osteoarthritis guidelines). Patient is a candidate for PPI therapy while on NSAIDs (medium risk d/t hypertension + ASA use). Recommend Omeprazole 20 mg daily while on Meloxicam therapy.
33 S: PH is a 64 y.o. female, reported to the XYZ Pharmacy for a follow-up MTM session. CC: Patient sprained her left knee on Sunday (pain reported 8/10) PMH: Gout and HTN SH/FH: no changes since last visit HPI: No s/sx of gout noted after d/c of colchicine. Patient stated last uric acid lab was WNL. Preventive Care: Up to date on vaccines (PNU 2013, Zoster 2013, Flu 2016, Tdap 2015) DXA 2015 Medication: Glucosamine 500 mg, take 3 capsules three times daily Aspirin 81 mg daily Losartan 50 mg daily Atenolol 50 mg every 12 hours KlorCon Tablet 10 meq daily Furosemide 20 mg every morning Calcium Carbonate 600 mg + D 400 IU at bedtime Fluticasone NS twice daily during winter Loratadine 10 mg every night Aleve every 12 hours Adherence: Pt reports adherence with all meds except Atenolol only been taking morning doses b/c out of refills and trying to save pills O: Height: 64.5 in, Weight = lbs, BMI = 44.7, BP = 174/90 mmhg, Pulse = 83, Pulse Ox = 98% A/P: 1. Hypertension Uncontrolled on current therapy (goal < 150/90, JNC VIII). Advised patient to take Atenolol twice daily and Atenolol refilled at pharmacy. Pharmacist will follow up with patient in 1 week with BP check. If BP is still elevated, pharmacist will contact Dr. Johnson to adjust hypertensive regimen. 2. Pain Uncontrolled on current therapy and inappropriate therapy. Received cortisone injection Friday and sprained left knee on Sunday. Recommend to Dr. Levin to reinitiate Meloxicam 7.5 mg daily and d/c Aleve. If pain is not controlled by Meloxicam 7.5 mg after two weeks, consider increasing doage to Meloxicam 15 mg daily (per American College of Rheumatology Osteoarthritis guidelines). Patient is a candidate for PPI therapy while on NSAIDs (medium risk d/t hypertension + ASA use). Recommend Omeprazole 20 mg daily while on Meloxicam therapy.
34 S: PH is a 64 y.o. female, reported to the XYZ Pharmacy for a follow-up MTM session. CC: Patient sprained her left knee on Sunday (pain reported 8/10) PMH: Gout and HTN SH/FH: no changes since last visit HPI: No s/sx of gout noted after d/c of colchicine. Patient stated last uric acid lab was WNL. Preventive Care: Up to date on vaccines (PNU 2013, Zoster 2013, Flu 2016, Tdap 2015) DXA 2015 Medication: Glucosamine 500 mg, take 3 capsules three times daily Aspirin 81 mg daily Losartan 50 mg daily Atenolol 50 mg every 12 hours KlorCon Tablet 10 meq daily Furosemide 20 mg every morning Calcium Carbonate 600 mg + D 400 IU at bedtime Fluticasone NS twice daily during winter Loratadine 10 mg every night Aleve every 12 hours Adherence: Pt reports adherence with all meds except Atenolol only been taking morning doses b/c out of refills and trying to save pills O: Height: 64.5 in, Weight = lbs, BMI = 44.7, BP = 174/90 mmhg, Pulse = 83, Pulse Ox = 98% A/P: 1. Hypertension Uncontrolled on current therapy (goal < 150/90, JNC VIII). Advised patient to take Atenolol twice daily and Atenolol refilled at pharmacy. Pharmacist will follow up with patient in 1 week with BP check. If BP is still elevated, pharmacist will contact Dr. Johnson to adjust hypertensive regimen. 2. Pain Uncontrolled on current therapy and inappropriate therapy. Received cortisone injection Friday and sprained left knee on Sunday. Recommend to Dr. Levin to reinitiate Meloxicam 7.5 mg daily and d/c Aleve. If pain is not controlled by Meloxicam 7.5 mg after two weeks, consider increasing doage to Meloxicam 15 mg daily (per American College of Rheumatology Osteoarthritis guidelines). Patient is a candidate for PPI therapy while on NSAIDs (medium risk d/t hypertension + ASA use). Recommend Omeprazole 20 mg daily while on Meloxicam therapy.
35 S: PH is a 64 y.o. female, reported to the XYZ Pharmacy for a follow-up MTM session. CC: Patient sprained her left knee on Sunday (pain reported 8/10) PMH: Gout and HTN SH/FH: no changes since last visit HPI: No s/sx of gout noted after d/c of colchicine. Patient stated last uric acid lab was WNL. Preventive Care: Up to date on vaccines (PNU 2013, Zoster 2013, Flu 2016, Tdap 2015) DXA 2015 Medication: Glucosamine 500 mg, take 3 capsules three times daily Aspirin 81 mg daily Losartan 50 mg daily Atenolol 50 mg every 12 hours KlorCon Tablet 10 meq daily Furosemide 20 mg every morning Calcium Carbonate 600 mg + D 400 IU at bedtime Fluticasone NS twice daily during winter Loratadine 10 mg every night Aleve every 12 hours Adherence: Pt reports adherence with all meds except Atenolol only been taking morning doses b/c out of refills and trying to save pills O: Height: 64.5 in, Weight = lbs, BMI = 44.7, BP = 174/90 mmhg, Pulse = 83, Pulse Ox = 98% A/P: 1. Hypertension Uncontrolled on current therapy (goal < 150/90, JNC VIII). Advised patient to take Atenolol twice daily and Atenolol refilled at pharmacy. Pharmacist will follow up with patient in 1 week with BP check. If BP is still elevated, pharmacist will contact Dr. Johnson to adjust hypertensive regimen. 2. Pain Uncontrolled on current therapy and inappropriate therapy. Received cortisone injection Friday and sprained left knee on Sunday. Recommend to Dr. Levin to reinitiate Meloxicam 7.5 mg daily and d/c Aleve. If pain is not controlled by Meloxicam 7.5 mg after two weeks, consider increasing doage to Meloxicam 15 mg daily (per American College of Rheumatology Osteoarthritis guidelines). Patient is a candidate for PPI therapy while on NSAIDs (medium risk d/t hypertension + ASA use). Recommend Omeprazole 20 mg daily while on Meloxicam therapy.
36 S: PH is a 64 y.o. female, reported to the XYZ Pharmacy for a follow-up MTM session. CC: Patient sprained her left knee on Sunday (pain reported 8/10) PMH: Gout and HTN SH/FH: no changes since last visit HPI: No s/sx of gout noted after d/c of colchicine. Patient stated last uric acid lab was WNL. Preventive Care: Up to date on vaccines (PNU 2013, Zoster 2013, Flu 2016, Tdap 2015) DXA 2015 Medication: Glucosamine 500 mg, take 3 capsules three times daily Aspirin 81 mg daily Losartan 50 mg daily Atenolol 50 mg every 12 hours KlorCon Tablet 10 meq daily Furosemide 20 mg every morning Calcium Carbonate 600 mg + D 400 IU at bedtime Fluticasone NS twice daily during winter Loratadine 10 mg every night Aleve every 12 hours Adherence: Pt reports adherence with all meds except Atenolol only been taking morning doses b/c out of refills and trying to save pills O: Height: 64.5 in, Weight = lbs, BMI = 44.7, BP = 174/90 mmhg, Pulse = 83, Pulse Ox = 98% A/P: 1. Hypertension Uncontrolled on current therapy (goal < 150/90, JNC VIII). Advised patient to take Atenolol twice daily and Atenolol refilled at pharmacy. Pharmacist will follow up with patient in 1 week with BP check. If BP is still elevated, pharmacist will contact Dr. Johnson to adjust hypertensive regimen. 2. Pain Uncontrolled on current therapy and inappropriate therapy. Received cortisone injection Friday and sprained left knee on Sunday. Recommend to Dr. Levin to reinitiate Meloxicam 7.5 mg daily and d/c Aleve. If pain is not controlled by Meloxicam 7.5 mg after two weeks, consider increasing doage to Meloxicam 15 mg daily (per American College of Rheumatology Osteoarthritis guidelines). Patient is a candidate for PPI therapy while on NSAIDs (medium risk d/t hypertension + ASA use). Recommend Omeprazole 20 mg daily while on Meloxicam therapy.
37 S: PH is a 64 y.o. female, reported to the XYZ Pharmacy for a follow-up MTM session. CC: Patient sprained her left knee on Sunday (pain reported 8/10) PMH: Gout and HTN SH/FH: no changes since last visit HPI: No s/sx of gout noted after d/c of colchicine. Patient stated last uric acid lab was WNL. Preventive Care: Up to date on vaccines (PNU 2013, Zoster 2013, Flu 2016, Tdap 2015) DXA 2015 Medication: Glucosamine 500 mg, take 3 capsules three times daily Aspirin 81 mg daily Losartan 50 mg daily Atenolol 50 mg every 12 hours KlorCon Tablet 10 meq daily Furosemide 20 mg every morning Calcium Carbonate 600 mg + D 400 IU at bedtime Fluticasone NS twice daily during winter Loratadine 10 mg every night Aleve every 12 hours Adherence: Pt reports adherence with all meds except Atenolol only been taking morning doses b/c out of refills and trying to save pills O: Height: 64.5 in, Weight = lbs, BMI = 44.7, BP = 174/90 mmhg, Pulse = 83, Pulse Ox = 98% A/P: 1. Hypertension Uncontrolled on current therapy (goal < 150/90, JNC VIII). Advised patient to take Atenolol twice daily and Atenolol refilled at pharmacy. Pharmacist will follow up with patient in 1 week with BP check. If BP is still elevated, pharmacist will contact Dr. Johnson to adjust hypertensive regimen. 2. Pain Uncontrolled on current therapy and inappropriate therapy. Received cortisone injection Friday and sprained left knee on Sunday. Recommend to Dr. Levin to reinitiate Meloxicam 7.5 mg daily and d/c Aleve. If pain is not controlled by Meloxicam 7.5 mg after two weeks, consider increasing doage to Meloxicam 15 mg daily (per American College of Rheumatology Osteoarthritis guidelines). Patient is a candidate for PPI therapy while on NSAIDs (medium risk d/t hypertension + ASA use). Recommend Omeprazole 20 mg daily while on Meloxicam therapy.
38 S: PH is a 64 y.o. female, reported to the XYZ Pharmacy for a follow-up MTM session. CC: Patient sprained her left knee on Sunday (pain reported 8/10) PMH: Gout and HTN SH/FH: no changes since last visit HPI: No s/sx of gout noted after d/c of colchicine. Patient stated last uric acid lab was WNL. Preventive Care: Up to date on vaccines (PNU 2013, Zoster 2013, Flu 2016, Tdap 2015) DXA 2015 Medication: Glucosamine 500 mg, take 3 capsules three times daily Aspirin 81 mg daily Losartan 50 mg daily Atenolol 50 mg every 12 hours KlorCon Tablet 10 meq daily Furosemide 20 mg every morning Calcium Carbonate 600 mg + D 400 IU at bedtime Fluticasone NS twice daily during winter Loratadine 10 mg every night Aleve every 12 hours Adherence: Pt reports adherence with all meds except Atenolol only been taking morning doses b/c out of refills and trying to save pills O: Height: 64.5 in, Weight = lbs, BMI = 44.7, BP = 174/90 mmhg, Pulse = 83, Pulse Ox = 98% A/P: 1. Hypertension Uncontrolled on current therapy (goal < 150/90, JNC VIII). Advised patient to take Atenolol twice daily and Atenolol refilled at pharmacy. Pharmacist will follow up with patient in 1 week with BP check. If BP is still elevated, pharmacist will contact Dr. Johnson to adjust hypertensive regimen. 2. Pain Uncontrolled on current therapy and inappropriate therapy. Received cortisone injection Friday and sprained left knee on Sunday. Recommend to Dr. Levin to reinitiate Meloxicam 7.5 mg daily and d/c Aleve. If pain is not controlled by Meloxicam 7.5 mg after two weeks, consider increasing doage to Meloxicam 15 mg daily (per American College of Rheumatology Osteoarthritis guidelines). Patient is a candidate for PPI therapy while on NSAIDs (medium risk d/t hypertension + ASA use). Recommend Omeprazole 20 mg daily while on Meloxicam therapy.
39 S: PH is a 64 y.o. female, reported to the XYZ Pharmacy for a follow-up MTM session. CC: Patient sprained her left knee on Sunday (pain reported 8/10) PMH: Gout and HTN SH/FH: no changes since last visit HPI: No s/sx of gout noted after d/c of colchicine. Patient stated last uric acid lab was WNL. Preventive Care: Up to date on vaccines (PNU 2013, Zoster 2013, Flu 2016, Tdap 2015) DXA 2015 Medication: Glucosamine 500 mg, take 3 capsules three times daily Aspirin 81 mg daily Losartan 50 mg daily Atenolol 50 mg every 12 hours KlorCon Tablet 10 meq daily Furosemide 20 mg every morning Calcium Carbonate 600 mg + D 400 IU at bedtime Fluticasone NS twice daily during winter Loratadine 10 mg every night Aleve every 12 hours Adherence: Pt reports adherence with all meds except Atenolol only been taking morning doses b/c out of refills and trying to save pills O: Height: 64.5 in, Weight = lbs, BMI = 44.7, BP = 174/90 mmhg, Pulse = 83, Pulse Ox = 98% A/P: 1. Hypertension Uncontrolled on current therapy (goal < 150/90, JNC VIII). Advised patient to take Atenolol twice daily and Atenolol refilled at pharmacy. Pharmacist will follow up with patient in 1 week with BP check. If BP is still elevated, pharmacist will contact Dr. Johnson to adjust hypertensive regimen. 2. Pain Uncontrolled on current therapy and inappropriate therapy. Received cortisone injection Friday and sprained left knee on Sunday. Recommend to Dr. Levin to reinitiate Meloxicam 7.5 mg daily and d/c Aleve. If pain is not controlled by Meloxicam 7.5 mg after two weeks, consider increasing dosage to Meloxicam 15 mg daily (per American College of Rheumatology Osteoarthritis guidelines). Patient is a candidate for PPI therapy while on NSAIDs (medium risk d/t hypertension + ASA use). Recommend Omeprazole 20 mg daily while on Meloxicam therapy.
40 S: PH is a 64 y.o. female, reported to the XYZ Pharmacy for a follow-up MTM session. CC: Patient sprained her left knee on Sunday (pain reported 8/10) PMH: Gout and HTN SH/FH: no changes since last visit HPI: No s/sx of gout noted after d/c of colchicine. Patient stated last uric acid lab was WNL. Preventive Care: Up to date on vaccines (PNU 2013, Zoster 2013, Flu 2016, Tdap 2015) DXA 2015 Medication: Glucosamine 500 mg, take 3 capsules three times daily Aspirin 81 mg daily Losartan 50 mg daily Atenolol 50 mg every 12 hours KlorCon Tablet 10 meq daily Furosemide 20 mg every morning Calcium Carbonate 600 mg + D 400 IU at bedtime Fluticasone NS twice daily during winter Loratadine 10 mg every night Aleve every 12 hours Adherence: Pt reports adherence with all meds except Atenolol only been taking morning doses b/c out of refills and trying to save pills O: Height: 64.5 in, Weight = lbs, BMI = 44.7, BP = 174/90 mmhg, Pulse = 83, Pulse Ox = 98% A/P: 1. Hypertension Uncontrolled on current therapy (goal < 150/90, JNC VIII). Advised patient to take Atenolol twice daily and Atenolol refilled at pharmacy. Pharmacist will follow up with patient in 1 week with BP check. If BP is still elevated, pharmacist will contact Dr. Johnson to adjust hypertensive regimen. 2. Pain Uncontrolled on current therapy and inappropriate therapy. Received cortisone injection Friday and sprained left knee on Sunday. Recommend to Dr. Levin to reinitiate Meloxicam 7.5 mg daily and d/c Aleve. If pain is not controlled by Meloxicam 7.5 mg after two weeks, consider increasing dosage to Meloxicam 15 mg daily (per American College of Rheumatology Osteoarthritis guidelines). Patient is a candidate for PPI therapy while on NSAIDs (medium risk d/t hypertension + ASA use). Recommend Omeprazole 20 mg daily while on Meloxicam therapy.
41 Develop accurate and concise patient care documentation using a patient case example for both initial and follow-up care Suzanne Higginbotham

42 Documentation If it isn t documented, it isn t done!
43 Parts of a Documentation Note-Subjective Information from patient perspective Chief complaint (CC) History of present illness (HPI) Past medical history (PMH) Medication use and history Allergies Social or family history (SH or FH) Review of systems (ROS) Lauster CD, Srivastava SB. Fundamental Skills for Patient Care in Pharmacy Practice. Burlington, MA: Jones and Martlett Learning; 2013
44 Subjective vs. Objective Current list of medications From patient interview or pharmacy system Adherence Adverse effects REMEMBER OTC, immunizations, and complementary/alternative medicines and supplements Lauster CD, Srivastava SB. Fundamental Skills for Patient Care in Pharmacy Practice. Burlington, MA: Jones and Martlett Learning; 2013
45 Parts of a Documentation Note-Objective Data that can be measured objectively Vital signs Blood pressure, heart rate, respiratory rate, temperature, weight, height Screening results Risk assessment Laboratory test results CBC, CHEM-7, Lipid panel, INR, serum drug concentration Findings from other tests Lauster CD, Srivastava SB. Fundamental Skills for Patient Care in Pharmacy Practice. Burlington, MA: Jones and Martlett Learning; 2013
46 Parts of a Documentation Note-Assessment and Plan Summarizes the pharmacist s evaluation Current status of patient Based on subjective & objective data Provides rationale for plan Goals set utilizing evidence based medicine (and referenced) Lauster CD, Srivastava SB. Fundamental Skills for Patient Care in Pharmacy Practice. Burlington, MA: Jones and Martlett Learning; 2013
47 How Much Data to Include Include only pertinent data Patient background information Control of disease state Identification of potential/actual ADE Assessment of medication use List form vs paragraph Actionable steps of assessment and plan Monitoring steps and follow up Prescription template
48 Patient Case Example Steven Jones is a 60-year-old white man with a 10-year history of T2DM. He reports to your ambulatory care center today for help managing his diabetes. He tests his blood glucose before meals and at bedtime. There have been no substantial changes in diet, stress, or illness within past 3 months. Please create a care plan based on the information below. Current Medications Metformin extended release (XR) 2 g daily Novolog 2 units with each meal Lantus 20 units at bedtime Amlodipine 5mg each morning Citalopram 40mg once daily
49 Glucose Log 7:00 a.m. 12:00 p.m. 5:00 p.m. 10:00 p.m. Monday Tuesday Wednesday Thursday Friday Saturday Sunday
50 Labs (taken 2 days ago) Hemoglobin A1c: 8.2 Microalbumin: 13.4 Gluc BUN Creat NA K CL CO CHOL TG HDL LDL LDL/HDL /3
51 Vitals and Vaccine History BP:132/80 Height:72 Weight:310 lbs Vaccine History IIV4 on 9/14/201 Td on 4/1/2010 * Up to date on all childhood vaccines
52 Let s Practice Documenting!
53 Describe methods for electronic exchange of information, including DIRECT and the use of Health Information Exchanges Amina Abubakar
54 Health Information Exchange (HIE) Allows healthcare providers and patients to appropriately access and securely share information electronically Reduces the need for the patient to transport or relay health information Improves speed, quality, safety, and cost of patient care What is HIE?, retrieved from accessed December 5, 2016.
55 Nationwide HIE Strategy Provider participation motivation Meaningful use requirements New payment approaches (ACOs, bundled payment options, PCMHs) MACRA & MIPS Congress allocated $548 million to states under the State HIE Cooperative Agreement Program in 2010 Administered by the Office of the National Coordinator for Health Information Technology (ONC) 2016 Report To Congress on Health IT Progress, The Office of the National Coordinator for Health Information Technology (ONC) Office of the Secretary, United States Department of Health and Human Services, retrieved from accessed December 13, 2016.
56 Forms of HIE DIRECTED Exchange Ability to send and receive secure information electronically between care providers to support coordinated care QUERY-BASED Exchange Ability for providers to find and/or request information on a patient from other providers, often used for unplanned care CONSUMER MEDIATED Exchange Ability for patients to aggregate and control the use of their health information among providers What is HIE?, retrieved from accessed December 5, 2016.
57 Health Information Services Provider (HISP) Private service provider offering information exchange capabilities Manages security and transport of health information Acts as an intermediary on behalf of exchange participant Functions: Issue security certificates Issue Direct addresses DIRECT Project, retrieved from accessed December 12, 2016.
58 The DIRECT Project Enables simple, secure electronic transport of health information Encrypted messaging to ensure safety and security of exchanged information Available through EHR vendors, State HIE entities, regional/local HIE entities, and HISPs Push messaging with known and trusted Direct addresses Allow information exchange between multiple vendors Recipient s Direct address and public certificate required to exchange DIRECT Project, retrieved from accessed December 12, 2016.

, retrieved from https://www.healthit.")
59 EHR message EHR HISP/HIE DIRECT EHR Affiliated HISP/HIE Understanding and Leveraging MU2 Optional Transports, The Office of the National Coordinator for Health Information Technology (ONC), retrieved from accessed December 12, 2016.
60 Role of HIE in Community Pharmacy Example Rx Clinic Pharmacy Partnered with local primary care providers to offer Chronic Care Management (CCM) Goals: improve patient outcomes through pharmacy engagement
61 Community Pharmacy CCM Integration Chronic Care Eligible Patient identified All eligible patients tagged in Pharmacy Management System Community pharmacy clinical services provided Service billed monthly for tasks completed in the pharmacy Platform shares ecare Plan with medical providers though HIE Services documented in platform in ecare Plan
62 Ambulatory Care CCM Integration Chronic Care Management eligible patients identified Clinical pharmacist completes required activities in clinic Clinical pharmacist documents activity in vendor platform Service billed monthly for tasks completed by the clinical pharmacist Vendor platform shares information with EHR via ecareplan and HIE Vendor platform tracks time spent and activities accomplished with patient
63 Barriers of HIE Implementation in the Community Data Governance Agreements Patient Consent Technical Difficulties Physician Communication Burden of Documentation Cost and Sustainability
64 Explain the functionality of the Pharmacist ecare Plan and the system functionality being built by pharmacy management system vendors to enable pharmacists to create and exchange patient care information. Amina Abubakar
65 Pharmacist ecare Plan Clinically-minded pharmacists utilizing their medication expertise to craft a comprehensive care plan Serves as the foundation for longitudinal coordination of care Template used to exchange information between patients and their care team to optimize medication-related decision support Goal: Create a comprehensive, multi-disciplinary longitudinal care plan that promotes interoperability Pharmacist ecare Plan: Guidance on the Use of the HL7 CDA Consolidated Templates for Clinical Notes R2.1 Care Plan (Version 1.0), National Council for Prescription Drug Programs (NCPDP), retrieved from accessed December 5, 2016.
66 The Role of ecare Plans Community Pharmacists are the most accessible providers Trusted relationships Access to social determinants of health that can be valuable to care team Maximizing documentation for services that pharmacists have been providing for decades Networks are seeing the value Additional layer to coordination of care Improved communication of valuable health information
67
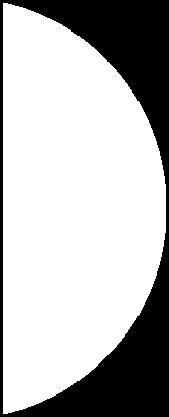
68 Documenting Encounter with Patient Patient report Counseling points Goals both clinician-guided and personal SMART Goals Specific Measurable Achievable Realistic Timely
69
70 The Role of Pharmacy Management Systems Systems are evolving to accommodate the changing role of community pharmacists Collect labs Create actions Utilize care templates Integrate with MTM platforms Partnerships with other programs when functionality is lacking
71 Use in Practice Enhanced Services Network Transitions of Care Chronic Care Management Medication Therapy Management
72 List the components of the Pharmacy Care Note template and identify appropriate information to include in each section Amina Abubakar
73 Community Pharmacy in Care Management MTM ecare Plans Steady State Model
74
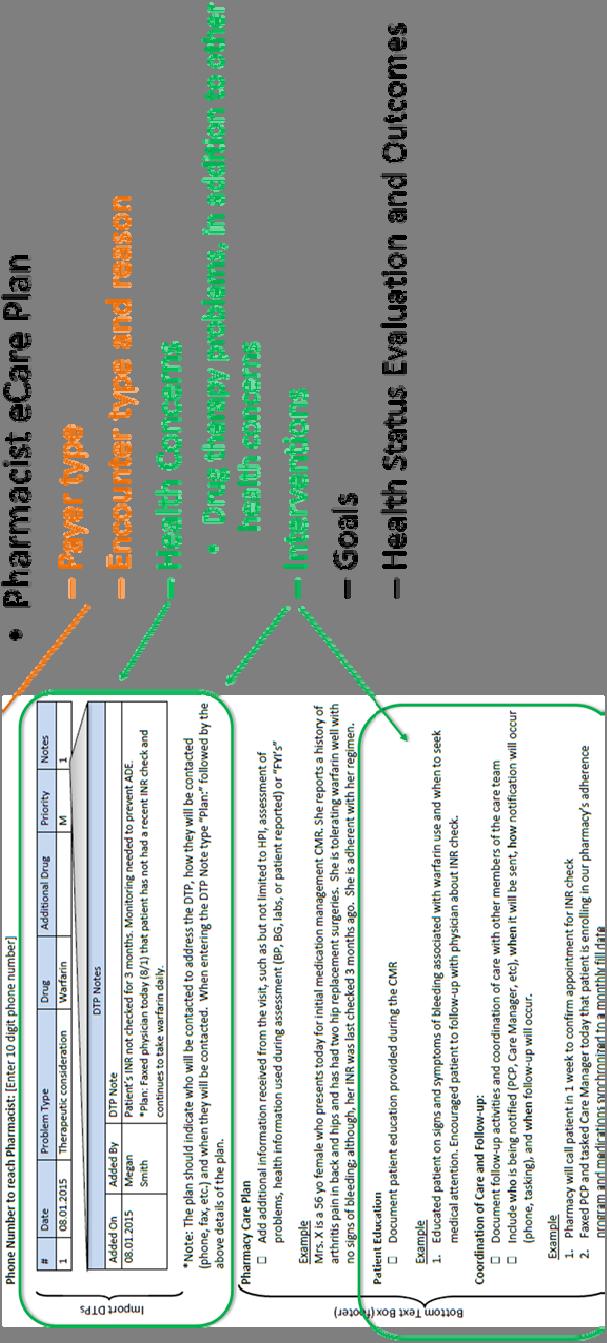
75 Comparison of Care Plans for Other Health Care Professionals Traditional Care Plan Pharmacist Care Plan Health Concerns Identified health or risk concerns such as problems, allergies, or social issue, etc Interventions Includes active medication list, medications administered, and planned medications Goals Health Status Evaluation and Outcomes Health Concerns (Pharmacist Care Plan) In addition to traditional care plan will include documentation of medication therapy problems. Interventions (Pharmacist Care Plan) In addition to traditional care plan will include medication history. Goals (Pharmacist Care Plan) Payer Health Status Evaluation and Outcomes (Pharmacist Care Plan)
76 Subjective and Objective Information Encounter Type and Reason Demographics History of Allergies and Adverse Effects Medication Reconciliation Fill History Patient Goals
77 Assessment Pharmacist assesses collected information Analysis of clinical effects of therapy Identification and prioritizing of problems Goal of Optimal Care
78 Plan Identification of Drug Therapy Problems Personalized Education and Interventions Coordination of Care
79 Follow-Up Identification of New Drug Therapy Problems and Resolution of Previously Identified Drug Therapy Problems Updates of Personal Goals Ongoing Assessment

80 The New Normal EHRs that communicate Connectivity and alerting Standardized documentation Complete with clinical coding Pharmacist integration in clinical services Ability to increase patient impact
81 Helpful Resources C-CDA Pharmacist Care Plan Implementation Guide emplates_and_supporting.pdf FHIR Pharmacist Care Plan Implementation Guide
82 1. Assessment Question Pharmacists are required to maintain patient health records that A. Are retained for five years B. Are stored physically on site C. Accessible to patients D. Include only medications and information related to the medication use
83 2. Assessment Question SNOWMED CT coding is a required form of documentation in which platform? A. JCCP Pharmacists Patient Care Process B. Diabetes self management education (DSME) sessions C. Tobacco cessation group facilitation sessions D. Pharmacist ecare Plan
84 3. Assessment Question Which of the following is a component of the assessment section in a clinical soap note A. Patient blood pressure is 132/88 B. Uncontrolled on current therapy of HCTZ 25mg once daily C. Initiate lisinopril 25mg once daily D. Patient reports eating foods high in sodium
85 4. Assessment Question Which of the following is not a core section of the Pharmacist ecare Plan? A. Goals B. Vital Signs C. Interventions D. Payer
86 5. Assessment Question Which of the following acts as an intermediary on behalf of an information exchange participant? A. HISP B. TITRS C. MIPS D. ACO
87 6. Assessment Question Pharmacy management systems have evolved to allow for this type of functionality as community pharmacists are offering more clinical services. A. Ability to create actions and tasks B. Utilization of care templates C. Ability to collect labs D. All of the above
Digital Strategies for Documenting and Sharing Patient Information Suzanne Higginbotham, PharmD, BCACP Olivia Bentley, PharmD, CFts, AAHIVP
 Digital Strategies for Documenting and Sharing Patient Information Suzanne Higginbotham, PharmD, BCACP Olivia Bentley, PharmD, CFts, AAHIVP Annual Meeting & Exposition Seattle, Washington March 22 25 Disclosures
Digital Strategies for Documenting and Sharing Patient Information Suzanne Higginbotham, PharmD, BCACP Olivia Bentley, PharmD, CFts, AAHIVP Annual Meeting & Exposition Seattle, Washington March 22 25 Disclosures
Antibiotic Stewardship and Critical Access Hospitals. Robert White, BA, PT, CPHQ Program Manager TMF Quality Innovation Network
 Antibiotic Stewardship and Critical Access Hospitals Robert White, BA, PT, CPHQ Program Manager TMF Quality Innovation Network Antibiotic-Resistant Bacteria A serious threat to public health and the economy
Antibiotic Stewardship and Critical Access Hospitals Robert White, BA, PT, CPHQ Program Manager TMF Quality Innovation Network Antibiotic-Resistant Bacteria A serious threat to public health and the economy
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings. Carlos Reyes Sacin, MD, AAHIVS
 Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
MHA/OHA HIIN Antibiotic Stewardship/MDRO Collaborative
 MHA/OHA HIIN Antibiotic Stewardship/MDRO Collaborative Place picture here Nov. 14, 2017 Reminders For best sound quality, dial in at 1-800-791-2345 and enter code 11076 Please use the chat box to ask questions!
MHA/OHA HIIN Antibiotic Stewardship/MDRO Collaborative Place picture here Nov. 14, 2017 Reminders For best sound quality, dial in at 1-800-791-2345 and enter code 11076 Please use the chat box to ask questions!
11/22/2016. Antimicrobial Stewardship Update Disclosures. Outline. No conflicts of interest to disclose
 Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Strategy 2020 Final Report March 2017
 Strategy 2020 Final Report March 2017 THE COLLEGE OF VETERINARIANS OF ONTARIO Introduction This document outlines the current strategic platform of the College of Veterinarians of Ontario for the period
Strategy 2020 Final Report March 2017 THE COLLEGE OF VETERINARIANS OF ONTARIO Introduction This document outlines the current strategic platform of the College of Veterinarians of Ontario for the period
Core Elements of Antibiotic Stewardship for Nursing Homes
 Core Elements of Antibiotic Stewardship for Nursing Homes Nimalie D. Stone, MD, MS Medical Epidemiologist for LTC Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Antimicrobial
Core Elements of Antibiotic Stewardship for Nursing Homes Nimalie D. Stone, MD, MS Medical Epidemiologist for LTC Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Antimicrobial
UPDATE ON ANTIMICROBIAL STEWARDSHIP REGULATIONS AND IMPLEMENTATION OF AN AMS PROGRAM
 UPDATE ON ANTIMICROBIAL STEWARDSHIP REGULATIONS AND IMPLEMENTATION OF AN AMS PROGRAM Diane Rhee, Pharm.D. Associate Professor of Pharmacy Practice Roseman University of Health Sciences Chair, Valley Health
UPDATE ON ANTIMICROBIAL STEWARDSHIP REGULATIONS AND IMPLEMENTATION OF AN AMS PROGRAM Diane Rhee, Pharm.D. Associate Professor of Pharmacy Practice Roseman University of Health Sciences Chair, Valley Health
Objective 1/20/2016. Expanding Antimicrobial Stewardship into the Outpatient Setting. Disclosure Statement of Financial Interest
 Expanding Antimicrobial Stewardship into the Outpatient Setting Michael E. Klepser, Pharm.D., FCCP Professor Pharmacy Practice Ferris State University College of Pharmacy Disclosure Statement of Financial
Expanding Antimicrobial Stewardship into the Outpatient Setting Michael E. Klepser, Pharm.D., FCCP Professor Pharmacy Practice Ferris State University College of Pharmacy Disclosure Statement of Financial
Complying with California Senate Bill 27 Livestock: Use of Antimicrobial Drugs
 Complying with California Senate Bill 27 Livestock: Use of Antimicrobial Drugs Annette Jones, DVM State Veterinarian and Director Animal Health and Food Safety Services California Department of Food And
Complying with California Senate Bill 27 Livestock: Use of Antimicrobial Drugs Annette Jones, DVM State Veterinarian and Director Animal Health and Food Safety Services California Department of Food And
Antimicrobial Stewardship in the Outpatient Setting. ELAINE LADD, PHARMD, ABAAHP, FAARFM OCTOBER 28th, 2016
 Antimicrobial Stewardship in the Outpatient Setting ELAINE LADD, PHARMD, ABAAHP, FAARFM OCTOBER 28th, 2016 Abbreviations AMS - Antimicrobial Stewardship Program OP - Outpatient OPS - Outpatient Setting
Antimicrobial Stewardship in the Outpatient Setting ELAINE LADD, PHARMD, ABAAHP, FAARFM OCTOBER 28th, 2016 Abbreviations AMS - Antimicrobial Stewardship Program OP - Outpatient OPS - Outpatient Setting
Define evidence based practices for selection and duration of antibiotics to treat suspected or confirmed neonatal sepsis
 GLOBAL AIM: Antibiotic Stewardship Perinatal Quality Improvement Teams (PQITs) will share strategies and lessons learned to develop potentially better practices and employ QI methodologies to establish
GLOBAL AIM: Antibiotic Stewardship Perinatal Quality Improvement Teams (PQITs) will share strategies and lessons learned to develop potentially better practices and employ QI methodologies to establish
Jump Start Stewardship
 Jump Start Stewardship Webinar 2: Building your Stewardship Team and Selecting Interventions and Targets for your Implementation Welcome Thank you for your time today This webinar will be recorded for
Jump Start Stewardship Webinar 2: Building your Stewardship Team and Selecting Interventions and Targets for your Implementation Welcome Thank you for your time today This webinar will be recorded for
TREAT Steward. Antimicrobial Stewardship software with personalized decision support
 TREAT Steward TM Antimicrobial Stewardship software with personalized decision support ANTIMICROBIAL STEWARDSHIP - Interdisciplinary actions to improve patient care Quality Assurance The aim of antimicrobial
TREAT Steward TM Antimicrobial Stewardship software with personalized decision support ANTIMICROBIAL STEWARDSHIP - Interdisciplinary actions to improve patient care Quality Assurance The aim of antimicrobial
OIE Regional Commission for Europe Regional Work Plan Framework Version adopted during the 85 th OIE General Session (Paris, May 2017)
") OIE Regional Commission for Europe Regional Work Plan Framework 2017-2020 Version adopted during the 85 th OIE General Session (Paris, May 2017) Chapter 1 - Regional Directions 1.1. Introduction The slogan
OIE Regional Commission for Europe Regional Work Plan Framework 2017-2020 Version adopted during the 85 th OIE General Session (Paris, May 2017) Chapter 1 - Regional Directions 1.1. Introduction The slogan
Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources
 Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources Andrew Hunter, PharmD, BCPS Infectious Diseases Clinical Pharmacy Specialist Michael E. DeBakey VA Medical Center Andrew.hunter@va.gov
Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources Andrew Hunter, PharmD, BCPS Infectious Diseases Clinical Pharmacy Specialist Michael E. DeBakey VA Medical Center Andrew.hunter@va.gov
Antimicrobial Stewardship-way forward. Dr. Sonal Saxena Professor Lady Hardinge Medical College New Delhi
 Antimicrobial Stewardship-way forward Dr. Sonal Saxena Professor Lady Hardinge Medical College New Delhi Lets save what we have! What is Antibiotic stewardship? Optimal selection, dose and duration of
Antimicrobial Stewardship-way forward Dr. Sonal Saxena Professor Lady Hardinge Medical College New Delhi Lets save what we have! What is Antibiotic stewardship? Optimal selection, dose and duration of
What is an Antibiotic Stewardship Program?
 What is an Antibiotic Stewardship Program? Jane Rogers, R.N. Anne Messer, MPH Learning Session #4 August 15, 2017 National Nursing Home Quality Care Collaborative Change Package Change Bundle: To prevent
What is an Antibiotic Stewardship Program? Jane Rogers, R.N. Anne Messer, MPH Learning Session #4 August 15, 2017 National Nursing Home Quality Care Collaborative Change Package Change Bundle: To prevent
California Senate Bill 27 Livestock: Use of Antimicrobial Drugs (An Interesting Journey)
") California Senate Bill 27 Livestock: Use of Antimicrobial Drugs (An Interesting Journey) Annette Jones, DVM State Veterinarian and Director Animal Health and Food Safety Services California Department
California Senate Bill 27 Livestock: Use of Antimicrobial Drugs (An Interesting Journey) Annette Jones, DVM State Veterinarian and Director Animal Health and Food Safety Services California Department
Welcome to Texas. What is this? 2018 American Society of Health-System Pharmacists Page 1 of 13
 Clinical Integration: Strengthening Patient Care Services with a Systems Approach Brett D. Stauffer, MD, MHS, FHM Chief Quality Officer Baylor Scott & White Health Welcome to Texas What is this? A. Baby
Clinical Integration: Strengthening Patient Care Services with a Systems Approach Brett D. Stauffer, MD, MHS, FHM Chief Quality Officer Baylor Scott & White Health Welcome to Texas What is this? A. Baby
international news RECOMMENDATIONS
 The Third OIE Global Conference on Veterinary Education and the Role of the Veterinary Statutory Body was held in Foz do Iguaçu (Brazil) from 4 to 6 December 2013. The Conference addressed the need for
The Third OIE Global Conference on Veterinary Education and the Role of the Veterinary Statutory Body was held in Foz do Iguaçu (Brazil) from 4 to 6 December 2013. The Conference addressed the need for
Draft ESVAC Vision and Strategy
 1 2 3 7 April 2016 EMA/326299/2015 Veterinary Medicines Division 4 5 6 Draft Agreed by the ESVAC network 29 March 2016 Adopted by ESVAC 31 March 2016 Start of public consultation 7 April 2016 End of consultation
1 2 3 7 April 2016 EMA/326299/2015 Veterinary Medicines Division 4 5 6 Draft Agreed by the ESVAC network 29 March 2016 Adopted by ESVAC 31 March 2016 Start of public consultation 7 April 2016 End of consultation
June 2009 (website); September 2009 (Update) consent, informed consent, owner consent, risk, prognosis, communication, documentation, treatment
; September 2009 (Update) consent, informed consent, owner consent, risk, prognosis, communication, documentation, treatment") GUIDELINES Informed Owner Consent Approved by Council: June 10, 2009 Publication Date: June 2009 (website); September 2009 (Update) To Be Reviewed by: June 2014 Key Words: Related Topics: Legislative References:
GUIDELINES Informed Owner Consent Approved by Council: June 10, 2009 Publication Date: June 2009 (website); September 2009 (Update) To Be Reviewed by: June 2014 Key Words: Related Topics: Legislative References:
A General Overview of New York State Law Governing Recordkeeping By Veterinarians for Animal Care and Frequently Asked Questions for the Veterinarian
 A General Overview of New York State Law Governing Recordkeeping By Veterinarians for Animal Care and Frequently Asked Questions for the Veterinarian A. MAINTAINING ANIMAL PATIENT CARE RECORDS What information
A General Overview of New York State Law Governing Recordkeeping By Veterinarians for Animal Care and Frequently Asked Questions for the Veterinarian A. MAINTAINING ANIMAL PATIENT CARE RECORDS What information
Resolution adopted by the General Assembly on 5 October [without reference to a Main Committee (A/71/L.2)]
![Resolution adopted by the General Assembly on 5 October [without reference to a Main Committee (A/71/L.2)]](/thumbs/93/113861770.jpg "Resolution adopted by the General Assembly on 5 October [without reference to a Main Committee (A/71/L.2)]") United Nations A/RES/71/3 General Assembly Distr.: General 19 October 2016 Seventy-first session Agenda item 127 Resolution adopted by the General Assembly on 5 October 2016 [without reference to a Main
United Nations A/RES/71/3 General Assembly Distr.: General 19 October 2016 Seventy-first session Agenda item 127 Resolution adopted by the General Assembly on 5 October 2016 [without reference to a Main
Overview of the OIE PVS Pathway
 Overview of the OIE PVS Pathway Regional Seminar for OIE National Focal Points for Animal Production Food Safety Hanoi, Vietnam, 24-26 June 2014 Dr Agnes Poirier OIE Sub-Regional Representation for South-East
Overview of the OIE PVS Pathway Regional Seminar for OIE National Focal Points for Animal Production Food Safety Hanoi, Vietnam, 24-26 June 2014 Dr Agnes Poirier OIE Sub-Regional Representation for South-East
Geriatric Mental Health Partnership
 Geriatric Mental Health Partnership September 8, 2017 First, let s test your knowledge about antibiotics http://www.cdc.gov/getsmart/community/about/quiz.html 2 Get Smart Antibiotics Quiz Antibiotics fight
Geriatric Mental Health Partnership September 8, 2017 First, let s test your knowledge about antibiotics http://www.cdc.gov/getsmart/community/about/quiz.html 2 Get Smart Antibiotics Quiz Antibiotics fight
Hot Topics in Antimicrobial Stewardship. Meghan Brett, MD Medical Director, Antimicrobial Stewardship University of New Mexico Hospital
 Hot Topics in Antimicrobial Stewardship Meghan Brett, MD Medical Director, Antimicrobial Stewardship University of New Mexico Hospital Antimicrobial Stewardship Goals Primary Goal Optimize clinical outcomes
Hot Topics in Antimicrobial Stewardship Meghan Brett, MD Medical Director, Antimicrobial Stewardship University of New Mexico Hospital Antimicrobial Stewardship Goals Primary Goal Optimize clinical outcomes
Stewardship: Challenges & Opportunities in the Gulf Region
 Stewardship: Challenges & Opportunities in the Gulf Region Mushira Enani, MBBS, FRCPE, FACP,CIC Head- Infectious Disease Section King Fahad Medical City Outline Background of Healthcare system in GCC GCC
Stewardship: Challenges & Opportunities in the Gulf Region Mushira Enani, MBBS, FRCPE, FACP,CIC Head- Infectious Disease Section King Fahad Medical City Outline Background of Healthcare system in GCC GCC
CMS Antibiotic Stewardship Initiative
 CMS Antibiotic Stewardship Initiative Mary Fermazin, MD, MPA Chief Medical Officer Vice President, Health Policy and Quality Measurement Health Services Advisory Group (HSAG) March 11, 2017 Disclosure
CMS Antibiotic Stewardship Initiative Mary Fermazin, MD, MPA Chief Medical Officer Vice President, Health Policy and Quality Measurement Health Services Advisory Group (HSAG) March 11, 2017 Disclosure
Drive More Efficient Clinical Action by Streamlining the Interpretation of Test Results
 White Paper: Templated Report Comments Drive More Efficient Clinical Action by Streamlining the Interpretation of Test Results Background The availability of rapid, multiplexed technologies for the comprehensive
White Paper: Templated Report Comments Drive More Efficient Clinical Action by Streamlining the Interpretation of Test Results Background The availability of rapid, multiplexed technologies for the comprehensive
Comments from The Pew Charitable Trusts re: Consultation on a draft global action plan to address antimicrobial resistance September 1, 2014
 Comments from The Pew Charitable Trusts re: Consultation on a draft global action plan to address antimicrobial resistance September 1, 2014 The Pew Charitable Trusts is an independent, nonprofit organization
Comments from The Pew Charitable Trusts re: Consultation on a draft global action plan to address antimicrobial resistance September 1, 2014 The Pew Charitable Trusts is an independent, nonprofit organization
European Regional Verification Commission for Measles and Rubella Elimination (RVC) TERMS OF REFERENCE. 6 December 2011
 TERMS OF REFERENCE. 6 December 2011") European Regional Verification Commission for Measles and Rubella Elimination (RVC) TERMS OF REFERENCE 6 December 2011 Address requests about publications of the WHO Regional Office for Europe to: Publications
European Regional Verification Commission for Measles and Rubella Elimination (RVC) TERMS OF REFERENCE 6 December 2011 Address requests about publications of the WHO Regional Office for Europe to: Publications
WENDY WILLIAMS, MT(AMT) MSAH DIRECTOR LABORATORY AND PATHOLOGY SERVICES. Appalachian Regional Healthcare System apprhs.org
 MSAH DIRECTOR LABORATORY AND PATHOLOGY SERVICES. Appalachian Regional Healthcare System apprhs.org") Incorporating Automation and Rapid Diagnostic Technologies into the Micro Lab's Lean Workflow to Boost Productivity, Shorten Length of Stay, and Improve Antibiotic Utilization WENDY WILLIAMS, MT(AMT) MSAH
Incorporating Automation and Rapid Diagnostic Technologies into the Micro Lab's Lean Workflow to Boost Productivity, Shorten Length of Stay, and Improve Antibiotic Utilization WENDY WILLIAMS, MT(AMT) MSAH
Antimicrobial Stewardship 201: It s Time to Act. Michael E. Klepser, Pharm.D., FCCP, FIDP Professor Ferris State University College of Pharmacy
 Antimicrobial Stewardship 201: It s Time to Act Michael E. Klepser, Pharm.D., FCCP, FIDP Professor Ferris State University College of Pharmacy Target Audience: Pharmacists ACPE#: 0202-0000-18-006-L04-P
Antimicrobial Stewardship 201: It s Time to Act Michael E. Klepser, Pharm.D., FCCP, FIDP Professor Ferris State University College of Pharmacy Target Audience: Pharmacists ACPE#: 0202-0000-18-006-L04-P
PROFESSIONAL PRACTICE STANDARD
 PROFESSIONAL PRACTICE STANDARD Dispensing Drugs TBD Introduction Under the Veterinarians Act and Regulations, veterinarians licensed by the College of Veterinarians of Ontario are authorized to engage
PROFESSIONAL PRACTICE STANDARD Dispensing Drugs TBD Introduction Under the Veterinarians Act and Regulations, veterinarians licensed by the College of Veterinarians of Ontario are authorized to engage
Government Initiatives to Combat Antimicrobial Resistance (AMR)
") Government Initiatives to Combat Antimicrobial Resistance (AMR) in the Philippines Ma. Virginia G. Ala, MD, MPH, CESO III Director IV and Program Manager National Center for Pharmaceutical Access and Management,
Government Initiatives to Combat Antimicrobial Resistance (AMR) in the Philippines Ma. Virginia G. Ala, MD, MPH, CESO III Director IV and Program Manager National Center for Pharmaceutical Access and Management,
Promoting One Health : the international perspective OIE
 Promoting One Health : the international perspective OIE Integrating Animal Health & Public Health: Antimicrobial Resistance SADC SPS Training Workshop (Animal Health) 29-31 January 2014 Gaborone, Botwana
Promoting One Health : the international perspective OIE Integrating Animal Health & Public Health: Antimicrobial Resistance SADC SPS Training Workshop (Animal Health) 29-31 January 2014 Gaborone, Botwana
Using Data to Track Antibiotic Use and Outcomes
 Using Data to Track Antibiotic Use and Outcomes Michelle Nemec, PharmD Thrifty White Drug Pharmacy Objectives Describe the Antibiotic Stewardship Core Element of tracking and the specific interventions
Using Data to Track Antibiotic Use and Outcomes Michelle Nemec, PharmD Thrifty White Drug Pharmacy Objectives Describe the Antibiotic Stewardship Core Element of tracking and the specific interventions
Implementing Antibiotic Stewardship in Rural and Critical Access Hospitals
 National Center for Emerging and Zoonotic Infectious Diseases Implementing Antibiotic Stewardship in Rural and Critical Access Hospitals Denise Cardo, MD Director, Division of Healthcare Quality Promotion,
National Center for Emerging and Zoonotic Infectious Diseases Implementing Antibiotic Stewardship in Rural and Critical Access Hospitals Denise Cardo, MD Director, Division of Healthcare Quality Promotion,
National Action Plan development support tools
 National Action Plan development support tools Sample Checklist This checklist was developed to be used by multidisciplinary teams in countries to assist with the development of their national action plan
National Action Plan development support tools Sample Checklist This checklist was developed to be used by multidisciplinary teams in countries to assist with the development of their national action plan
Nurse Prescribing: Key Principles and Developments. Elissa Ladd, PhD, FNP-BC MGH Institute of Health Professions Boston, Massachusetts USA
 Nurse Prescribing: Key Principles and Developments Elissa Ladd, PhD, FNP-BC MGH Institute of Health Professions Boston, Massachusetts USA No disclosures to report Objectives: 1) To provide an overview
Nurse Prescribing: Key Principles and Developments Elissa Ladd, PhD, FNP-BC MGH Institute of Health Professions Boston, Massachusetts USA No disclosures to report Objectives: 1) To provide an overview
Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities
 Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities Introduction As the problem of antibiotic resistance continues to worsen in all healthcare setting, we
Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities Introduction As the problem of antibiotic resistance continues to worsen in all healthcare setting, we
Canada s Activities in Combatting Antimicrobial Resistance. Presentation to the JPIAMR Management Board March 29, 2017
 Canada s Activities in Combatting Antimicrobial Resistance Presentation to the JPIAMR Management Board March 29, 2017 AMR in Canada Surveillance data indicates that rates of infection for some resistant
Canada s Activities in Combatting Antimicrobial Resistance Presentation to the JPIAMR Management Board March 29, 2017 AMR in Canada Surveillance data indicates that rates of infection for some resistant
ANTIMICROBIAL RESISTANCE and causes of non-prudent use of antibiotics in human medicine in the EU
 ANTIMICROBIAL RESISTANCE and causes of non-prudent use of antibiotics in human medicine in the EU Health and Food Safety John Paget (NIVEL) Dominique Lescure (NIVEL) Ann Versporten (University of Antwerp)
ANTIMICROBIAL RESISTANCE and causes of non-prudent use of antibiotics in human medicine in the EU Health and Food Safety John Paget (NIVEL) Dominique Lescure (NIVEL) Ann Versporten (University of Antwerp)
Primary Care & Chronic Disease Management. Education for Health Care Professionals. Alberta Healthy Living Program
 Alberta Healthy Living Program Primary Care & Chronic Disease Management Education for Health Care Professionals Edmonton Zone Fall 2018 / Winter 2019 Guide Current as of 24 JULY 2018 Workshops are free.
Alberta Healthy Living Program Primary Care & Chronic Disease Management Education for Health Care Professionals Edmonton Zone Fall 2018 / Winter 2019 Guide Current as of 24 JULY 2018 Workshops are free.
Antibiotic Stewardship: The Facility Role and Implementation. Tim Cozad, LPN, Lead LTC Health Facilities Surveyor
 Antibiotic Stewardship: The Facility Role and Implementation Tim Cozad, LPN, Lead LTC Health Facilities Surveyor Phase II CMS Regulatory Changes Current information available includes: New Survey Process
Antibiotic Stewardship: The Facility Role and Implementation Tim Cozad, LPN, Lead LTC Health Facilities Surveyor Phase II CMS Regulatory Changes Current information available includes: New Survey Process
COMMISSION OF THE EUROPEAN COMMUNITIES
 COMMISSION OF THE EUROPEAN COMMUNITIES Brussels, 22 December 2005 COM (2005) 0684 REPORT FROM THE COMMISSION TO THE COUNCIL ON THE BASIS OF MEMBER STATES REPORTS ON THE IMPLEMENTATION OF THE COUNCIL RECOMMENDATION
COMMISSION OF THE EUROPEAN COMMUNITIES Brussels, 22 December 2005 COM (2005) 0684 REPORT FROM THE COMMISSION TO THE COUNCIL ON THE BASIS OF MEMBER STATES REPORTS ON THE IMPLEMENTATION OF THE COUNCIL RECOMMENDATION
OIE STANDARDS ON VETERINARY SERVICES ( ), COMMUNICATION (3.3), & LEGISLATION (3.4)
, COMMUNICATION (3.3), & LEGISLATION (3.4)") OIE STANDARDS ON VETERINARY SERVICES (3.1-3.2), COMMUNICATION (3.3), & LEGISLATION (3.4) Ronello Abila Sub-Regional Representative for South-East Asia 1 2 CHAPTER 3.1 VETERINARY SERVICES The Veterinary
OIE STANDARDS ON VETERINARY SERVICES (3.1-3.2), COMMUNICATION (3.3), & LEGISLATION (3.4) Ronello Abila Sub-Regional Representative for South-East Asia 1 2 CHAPTER 3.1 VETERINARY SERVICES The Veterinary
Antimicrobial Stewardship
 Antimicrobial Stewardship Report: 11 th August 2016 Issue: As part of ensuring compliance with the National Safety and Quality Health Service Standards (NSQHS), Yea & District Memorial Hospital is required
Antimicrobial Stewardship Report: 11 th August 2016 Issue: As part of ensuring compliance with the National Safety and Quality Health Service Standards (NSQHS), Yea & District Memorial Hospital is required
Speaking notes submitted by Dr. Duane Landals. on behalf of the Canadian Veterinary Medical Association (CVMA)
") 339, rue Booth Street Ottawa (Ontario) K1R 7K1 t (800) 567-2862 f (613) 236-9681 admin@cvma-acmv.org Speaking notes submitted by Dr. Duane Landals on behalf of the Canadian Veterinary Medical Association
339, rue Booth Street Ottawa (Ontario) K1R 7K1 t (800) 567-2862 f (613) 236-9681 admin@cvma-acmv.org Speaking notes submitted by Dr. Duane Landals on behalf of the Canadian Veterinary Medical Association
Antimicrobial Stewardship: Stopping the Spread of Antibiotic Resistance
 Antimicrobial Stewardship: Stopping the Spread of Antibiotic Resistance Natalie Weber, PharmD PGY2 Critical Care Pharmacy Resident September 22, 2016 The speaker has no actual or potential conflicts of
Antimicrobial Stewardship: Stopping the Spread of Antibiotic Resistance Natalie Weber, PharmD PGY2 Critical Care Pharmacy Resident September 22, 2016 The speaker has no actual or potential conflicts of
Surveillance. Mariano Ramos Chargé de Mission OIE Programmes Department
 Mariano Ramos Chargé de Mission OIE Programmes Department Surveillance Regional Table Top Exercise for Countries of Middle East and North Africa Tunisia; 11 13 July 2017 Agenda Key definitions and criteria
Mariano Ramos Chargé de Mission OIE Programmes Department Surveillance Regional Table Top Exercise for Countries of Middle East and North Africa Tunisia; 11 13 July 2017 Agenda Key definitions and criteria
Embracing the Open Pet Pharmaceutical Transition
 Embracing the Open Pet Pharmaceutical Transition The Shifting Pet Pharmacy Revenue In March 2015, leading animal health industry consultancy, Brakke Consulting, Inc., in collaboration with the leading
Embracing the Open Pet Pharmaceutical Transition The Shifting Pet Pharmacy Revenue In March 2015, leading animal health industry consultancy, Brakke Consulting, Inc., in collaboration with the leading
Antibiotic Stewardship Beyond Hospital Walls
 Antibiotic Stewardship Beyond Hospital Walls Katie Burenheide Foster, PharmD, MS, BCPS, FCCM Pharmacy Clinical Manager & PGY1 Pharmacy Residency Director OBJECTIVES 1. Review what Antibiotic Stewardship
Antibiotic Stewardship Beyond Hospital Walls Katie Burenheide Foster, PharmD, MS, BCPS, FCCM Pharmacy Clinical Manager & PGY1 Pharmacy Residency Director OBJECTIVES 1. Review what Antibiotic Stewardship
Challenges and opportunities for rapidly advancing reporting and improving inpatient antibiotic use in the U.S.
 Challenges and opportunities for rapidly advancing reporting and improving inpatient antibiotic use in the U.S. Overview of benchmarking Antibiotic Use Scott Fridkin, MD, Senior Advisor for Antimicrobial
Challenges and opportunities for rapidly advancing reporting and improving inpatient antibiotic use in the U.S. Overview of benchmarking Antibiotic Use Scott Fridkin, MD, Senior Advisor for Antimicrobial
Nursing Home Online Training Sessions Session 2: Exploring Antibiotics and Their Role in Fighting Bacterial Infections
 National Nursing Home Quality Care Collaborative Nursing Home Online Training Sessions Session 2: Exploring Antibiotics and Their Role in Fighting Bacterial Infections Health Services Advisory Group (HSAG)
National Nursing Home Quality Care Collaborative Nursing Home Online Training Sessions Session 2: Exploring Antibiotics and Their Role in Fighting Bacterial Infections Health Services Advisory Group (HSAG)
Highlights on Hong Kong Strategy and Action Plan on Antimicrobial Resistance ( ) (Action Plan)
 (Action Plan)") 香港藥學會 The Pharmaceutical Society of Hong Kong Kowloon G.P.O. Box 73552, Yau Ma Tei, Kowloon, Hong Kong Society s Fax: (852) 2376-3091 E-mail: pharmacist@pshk.hk Websites: http://pshk.hk Highlights on Hong
香港藥學會 The Pharmaceutical Society of Hong Kong Kowloon G.P.O. Box 73552, Yau Ma Tei, Kowloon, Hong Kong Society s Fax: (852) 2376-3091 E-mail: pharmacist@pshk.hk Websites: http://pshk.hk Highlights on Hong
Antibiotic Stewardship in Nursing Homes SAM GUREVITZ PHARM D, CGP ASSOCIATE PROFESSOR BUTLER UNIVERSITY COLLEGE OF PHARMACY AND HEALTH SCIENCE
 Antibiotic Stewardship in Nursing Homes SAM GUREVITZ PHARM D, CGP ASSOCIATE PROFESSOR BUTLER UNIVERSITY COLLEGE OF PHARMACY AND HEALTH SCIENCE Crisis: Antibiotic Resistance Success Strategy WWW.optimistic-care.org
Antibiotic Stewardship in Nursing Homes SAM GUREVITZ PHARM D, CGP ASSOCIATE PROFESSOR BUTLER UNIVERSITY COLLEGE OF PHARMACY AND HEALTH SCIENCE Crisis: Antibiotic Resistance Success Strategy WWW.optimistic-care.org
Communicating about AR: It s complicated but not impossible! Mary Beth Wenger Health Communications Specialist New York State Department of Health
 Communicating about AR: It s complicated but not impossible! Mary Beth Wenger Health Communications Specialist New York State Department of Health So, why are antibiotics inappropriately prescribed? 2
Communicating about AR: It s complicated but not impossible! Mary Beth Wenger Health Communications Specialist New York State Department of Health So, why are antibiotics inappropriately prescribed? 2
American Association of Equine Practitioners White Paper on Telehealth July 2018
 American Association of Equine Practitioners White Paper on Telehealth July 2018 Introduction Telehealth, by definition, encompasses all uses of technology designed to remotely deliver health information
American Association of Equine Practitioners White Paper on Telehealth July 2018 Introduction Telehealth, by definition, encompasses all uses of technology designed to remotely deliver health information
Multisector Collaboration One Health Approach to Addressing Antibiotic Resistance Nov. 5, 2015
 Multisector Collaboration One Health Approach to Addressing Antibiotic Resistance Nov. 5, 2015 The One Health concept recognizes that the health of humans is connected to the health of animals and the
Multisector Collaboration One Health Approach to Addressing Antibiotic Resistance Nov. 5, 2015 The One Health concept recognizes that the health of humans is connected to the health of animals and the
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus
 Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
4/4/2018. Pathway Health 1. Antibiotics - Are they OVERUSED?? Best Practice Approach to Antibiotic Stewardship: Essential Strategies for Compliance
 Best Practice Approach to Antibiotic Stewardship: Essential Strategies for Compliance Laura Chambers, RN, MSN, RAC-CT, CIMT Pathway Health Objectives Upon completion of this presentation, attendees should
Best Practice Approach to Antibiotic Stewardship: Essential Strategies for Compliance Laura Chambers, RN, MSN, RAC-CT, CIMT Pathway Health Objectives Upon completion of this presentation, attendees should
Antimicrobial Stewardship: Setting minimum expectations for optimizing antimicrobial use and addressing resistance
 Antimicrobial Stewardship: Setting minimum expectations for optimizing antimicrobial use and addressing resistance Loria Pollack, MD, MPH Centers for Disease Control and Prevention Division of Healthcare
Antimicrobial Stewardship: Setting minimum expectations for optimizing antimicrobial use and addressing resistance Loria Pollack, MD, MPH Centers for Disease Control and Prevention Division of Healthcare
Development and improvement of diagnostics to improve use of antibiotics and alternatives to antibiotics
 Priority Topic B Diagnostics Development and improvement of diagnostics to improve use of antibiotics and alternatives to antibiotics The overarching goal of this priority topic is to stimulate the design,
Priority Topic B Diagnostics Development and improvement of diagnostics to improve use of antibiotics and alternatives to antibiotics The overarching goal of this priority topic is to stimulate the design,
Telligen Outpatient Antibiotic Stewardship Initiative. The Renal Network March 1, 2017
 Telligen Outpatient Antibiotic Stewardship Initiative The Renal Network March 1, 2017 Who is Telligen? What is the QIN-QIO Program? Telligen: The Medicare Quality Innovation Network (QIN)-Quality Improvement
Telligen Outpatient Antibiotic Stewardship Initiative The Renal Network March 1, 2017 Who is Telligen? What is the QIN-QIO Program? Telligen: The Medicare Quality Innovation Network (QIN)-Quality Improvement
Best Practices for Humane Care & High Live Release Programming
 Florida Animal Control Association & The Florida Association of Animal Welfare Organizations Best Practices for Humane Care & High Live Release Programming About FACA and FAAWO The Florida Animal Control
Florida Animal Control Association & The Florida Association of Animal Welfare Organizations Best Practices for Humane Care & High Live Release Programming About FACA and FAAWO The Florida Animal Control
Understand the application of Antibiotic Stewardship regulations in LTC. Understand past barriers to antibiotic management concepts
 Objectives Understand the application of Antibiotic Stewardship regulations in LTC Understand past barriers to antibiotic management concepts Understand benefits of adoption of antibiotic stewardship regulations
Objectives Understand the application of Antibiotic Stewardship regulations in LTC Understand past barriers to antibiotic management concepts Understand benefits of adoption of antibiotic stewardship regulations
Vice President of Development Denver, CO
 Vice President of Development Denver, CO A Nonprofit Community-Based Animal Welfare Organization Committed to Ending Pet Homelessness and Animal Suffering The Dumb Friends League Mission For over 100 years,
Vice President of Development Denver, CO A Nonprofit Community-Based Animal Welfare Organization Committed to Ending Pet Homelessness and Animal Suffering The Dumb Friends League Mission For over 100 years,
Internship/Seasonal Employment Opportunities 2018
 Internship/Seasonal Employment Opportunities 2018 Goals: The goals of the Internship/Seasonal Employment program at DuPage County Animal Care & Control are threefold. The first is to provide an experiential
Internship/Seasonal Employment Opportunities 2018 Goals: The goals of the Internship/Seasonal Employment program at DuPage County Animal Care & Control are threefold. The first is to provide an experiential
Dr. Gérard Moulin AFSSA/ANMV OIE Collaborating Centre on Veterinary medicinal products BP FOUGERES CEDEX, FRANCE
 Dr. Gérard Moulin AFSSA/ANMV OIE Collaborating Centre on Veterinary medicinal products BP 90203-35302 FOUGERES CEDEX, FRANCE gerard.moulin@anses.fr Introduction to the working sessions Need for a good
Dr. Gérard Moulin AFSSA/ANMV OIE Collaborating Centre on Veterinary medicinal products BP 90203-35302 FOUGERES CEDEX, FRANCE gerard.moulin@anses.fr Introduction to the working sessions Need for a good
of Conferences of OIE Regional Commissions organised since 1 June 2013 endorsed by the Assembly of the OIE on 29 May 2014
 of Conferences of OIE Regional Commissions organised since 1 June 2013 endorsed by the Assembly of the OIE on 29 May 2014 2 12 th Conference of the OIE Regional Commission for the Middle East Amman (Jordan),
of Conferences of OIE Regional Commissions organised since 1 June 2013 endorsed by the Assembly of the OIE on 29 May 2014 2 12 th Conference of the OIE Regional Commission for the Middle East Amman (Jordan),
Antimicrobial Stewardship in Food Animals in Canada AMU/AMR WG Update Forum 2016
 Antimicrobial Stewardship in Food Animals in Canada AMU/AMR WG Update Forum 2016 What is Antimicrobial Stewardship? Conserving the effectiveness of existing treatments through infection prevention and
Antimicrobial Stewardship in Food Animals in Canada AMU/AMR WG Update Forum 2016 What is Antimicrobial Stewardship? Conserving the effectiveness of existing treatments through infection prevention and
OBJECTIVES. Fast Facts 3/23/2017. Antibiotic Stewardship Beyond Hospital Walls. Antibiotics are a shared resource and becoming a scarce resource.
 Antibiotic Stewardship Beyond Hospital Walls Katie Burenheide Foster, PharmD, MS, BCPS, FCCM Pharmacy Clinical Manager & PGY1 Pharmacy Residency Director OBJECTIVES 1. Review what Antibiotic Stewardship
Antibiotic Stewardship Beyond Hospital Walls Katie Burenheide Foster, PharmD, MS, BCPS, FCCM Pharmacy Clinical Manager & PGY1 Pharmacy Residency Director OBJECTIVES 1. Review what Antibiotic Stewardship
Service Dog Application
 Thank you for requesting a service dog from the Dog Alliance. To qualify for a service dog under this program you need to have been discharged from the military with an honorable or medical discharge or
Thank you for requesting a service dog from the Dog Alliance. To qualify for a service dog under this program you need to have been discharged from the military with an honorable or medical discharge or
SECOND REPORT FROM THE COMMISSION TO THE COUNCIL
 SECOND REPORT FROM THE COMMISSION TO THE COUNCIL ON THE BASIS OF MEMBER STATES REPORTS ON THE IMPLEMENTATION OF THE COUNCIL RECOMMENDATION (2002/77/EC) ON THE PRUDENT USE OF ANTIMICROBIAL AGENTS IN HUMAN
SECOND REPORT FROM THE COMMISSION TO THE COUNCIL ON THE BASIS OF MEMBER STATES REPORTS ON THE IMPLEMENTATION OF THE COUNCIL RECOMMENDATION (2002/77/EC) ON THE PRUDENT USE OF ANTIMICROBIAL AGENTS IN HUMAN
POSITION DESCRIPTION. Organisational Context: Important Functional Relationships: Page 1. Job Title: Reports To: Direct Reports: Position Purpose:
 Page 1 POSITION DESCRIPTION Job Title: Reports To: Direct Reports: Position Purpose: Keeper Level One, Two and /Animal Care Manager Nil A Zoo Keeper is responsible for providing quality animal husbandry
Page 1 POSITION DESCRIPTION Job Title: Reports To: Direct Reports: Position Purpose: Keeper Level One, Two and /Animal Care Manager Nil A Zoo Keeper is responsible for providing quality animal husbandry
Better Training for Safer Food
 Better Training for Safer Food Initiative Susanne Münstermann Better Training for Safer Food is an initiative of the European Commission aimed at organising an EU training strategy in the areas of food
Better Training for Safer Food Initiative Susanne Münstermann Better Training for Safer Food is an initiative of the European Commission aimed at organising an EU training strategy in the areas of food
Dear Sir/Madam, Re: Inquiry into the Agricultural and Veterinary Chemicals Legislation Amendment (Removing
 18 April 2014 Committee Secretary Senate Standing Committees on Rural and Regional Affairs and Transport PO Box 6100 Parliament House Canberra ACT 2600 By email: rrat.sen@aph.gov.au Dear Sir/Madam, Re:
18 April 2014 Committee Secretary Senate Standing Committees on Rural and Regional Affairs and Transport PO Box 6100 Parliament House Canberra ACT 2600 By email: rrat.sen@aph.gov.au Dear Sir/Madam, Re:
ANTIMICROBIALS PRESCRIBING STRATEGY
 Directorate of Operations Clinical Support Services Diagnostic Services Pharmacy ANTIMICROBIALS PRESCRIBING STRATEGY Reference: DCM021 Version: 2.0 This version issued: 25/04/16 Result of last review:
Directorate of Operations Clinical Support Services Diagnostic Services Pharmacy ANTIMICROBIALS PRESCRIBING STRATEGY Reference: DCM021 Version: 2.0 This version issued: 25/04/16 Result of last review:
A New Approach for Managing Bovine Tuberculosis: Veterinary Services Proposed Action Plan
 University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Michigan Bovine Tuberculosis Bibliography and Database Wildlife Disease and Zoonotics 7-2009 A New Approach for Managing
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Michigan Bovine Tuberculosis Bibliography and Database Wildlife Disease and Zoonotics 7-2009 A New Approach for Managing
Office Managers Meeting
 Office Managers Meeting Watertown, MA and by Live Stream March 26, 2019 Discussion Topics Product Overviews Plan Identification Provider Resource Center Provider Website Navigation Online Tools for Providers
Office Managers Meeting Watertown, MA and by Live Stream March 26, 2019 Discussion Topics Product Overviews Plan Identification Provider Resource Center Provider Website Navigation Online Tools for Providers
VetPrescriber: The Forefront of Digital Prescribing for Veterinarians
 VetPrescriber: The Forefront of Digital Prescribing for Veterinarians SUMMARY Electronic prescribing also referred to as e-prescribing, digital prescribing, and occasionally e-rx uses hospital/clinic/office
VetPrescriber: The Forefront of Digital Prescribing for Veterinarians SUMMARY Electronic prescribing also referred to as e-prescribing, digital prescribing, and occasionally e-rx uses hospital/clinic/office
Global Strategies to Address AMR Carmem Lúcia Pessoa-Silva, MD, PhD Antimicrobial Resistance Secretariat
 Global Strategies to Address AMR Carmem Lúcia Pessoa-Silva, MD, PhD Antimicrobial Resistance Secretariat EMA Working Parties with Patients and Consumers Organisations (PCWP) and Healthcare Professionals
Global Strategies to Address AMR Carmem Lúcia Pessoa-Silva, MD, PhD Antimicrobial Resistance Secretariat EMA Working Parties with Patients and Consumers Organisations (PCWP) and Healthcare Professionals
Healthcare Facilities and Healthcare Professionals. Public
 Document Title: DOH Guidelines for Antimicrobial Stewardship Programs Document Ref. Number: DOH/ASP/GL/1.0 Version: 1.0 Approval Date: 13/12/2017 Effective Date: 14/12/2017 Document Owner: Applies to:
Document Title: DOH Guidelines for Antimicrobial Stewardship Programs Document Ref. Number: DOH/ASP/GL/1.0 Version: 1.0 Approval Date: 13/12/2017 Effective Date: 14/12/2017 Document Owner: Applies to:
Guidance Document. Veterinary Operating Instructions. Guidance re: Requirements for Authorising Veterinarians Notice.
 Guidance Document Veterinary Operating Instructions Guidance re: Requirements for Authorising Veterinarians Notice 28 August 2015 A guidance document issued by the Ministry for Primary Industries Title
Guidance Document Veterinary Operating Instructions Guidance re: Requirements for Authorising Veterinarians Notice 28 August 2015 A guidance document issued by the Ministry for Primary Industries Title
Overview of Canada's Federal Actions to Address Antimicrobial Resistance and Antibiotic Stewardship
 Overview of Canada's Federal Actions to Address Antimicrobial Resistance and Antibiotic Stewardship Jacqueline Arthur, RN, BScN Centre for Communicable Diseases and Infection Control Commonwealth Laboratory
Overview of Canada's Federal Actions to Address Antimicrobial Resistance and Antibiotic Stewardship Jacqueline Arthur, RN, BScN Centre for Communicable Diseases and Infection Control Commonwealth Laboratory
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process High Priority
 MEASURE TYPE: Process High Priority") Quality ID #464 (NQF 0657): Otitis Media with Effusion: Systemic Antimicrobials - Avoidance of Inappropriate Use National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Appropriate
Quality ID #464 (NQF 0657): Otitis Media with Effusion: Systemic Antimicrobials - Avoidance of Inappropriate Use National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Appropriate
OIE capacity-building activities
 OIE capacity-building activities OIE Regional Seminar for Recently Appointed OIE Delegates Tokyo (Japan) 7-8 February 2012 Dr Mara Gonzalez Ortiz OIE Regional Activities Department OIE Fifth Strategic
OIE capacity-building activities OIE Regional Seminar for Recently Appointed OIE Delegates Tokyo (Japan) 7-8 February 2012 Dr Mara Gonzalez Ortiz OIE Regional Activities Department OIE Fifth Strategic
V E T E R I N A R Y C O U N C I L O F I R E L A N D ETHICAL VETERINARY PRACTICE
 V E T E R I N A R Y C O U N C I L O F I R E L A N D ETHICAL VETERINARY PRACTICE ETHICAL VETERINARY PRACTICE The term Ethical Veterinary Practice is a wide ranging one, implying as it does, compliance with
V E T E R I N A R Y C O U N C I L O F I R E L A N D ETHICAL VETERINARY PRACTICE ETHICAL VETERINARY PRACTICE The term Ethical Veterinary Practice is a wide ranging one, implying as it does, compliance with
ASCENSION TEXAS Antimicrobial Stewardship: Practical Implementation Strategies
 ASCENSION TEXAS Antimicrobial Stewardship: Practical Implementation Strategies Theresa Jaso, PharmD, BCPS (AQ-ID) Network Clinical Pharmacy Specialist Infectious Diseases Seton Healthcare Family Ascension
ASCENSION TEXAS Antimicrobial Stewardship: Practical Implementation Strategies Theresa Jaso, PharmD, BCPS (AQ-ID) Network Clinical Pharmacy Specialist Infectious Diseases Seton Healthcare Family Ascension
ANTIMICROBIAL RESISTANCE
 Session 4: How to join efforts for improving communication, education and training Prescription by general practitioners/family physicians ANTIMICROBIAL RESISTANCE Walter Marrocco EFPC September 19 th
Session 4: How to join efforts for improving communication, education and training Prescription by general practitioners/family physicians ANTIMICROBIAL RESISTANCE Walter Marrocco EFPC September 19 th
Antimicrobial Stewardship:
 Antimicrobial Stewardship: Inpatient and Outpatient Elements Angela Perhac, PharmD afperhac@carilionclinic.org Disclosure I have no relevant finances to disclose. Objectives Review the core elements of
Antimicrobial Stewardship: Inpatient and Outpatient Elements Angela Perhac, PharmD afperhac@carilionclinic.org Disclosure I have no relevant finances to disclose. Objectives Review the core elements of
Identifying Medicine Use Problems Using Indicator-Based Studies in Health Facilities
 Identifying Medicine Use Problems Using Indicator-Based Studies in Health Facilities Review of the Cesarean-section Antibiotic Prophylaxis Program in Jordan and Workshop on Rational Medicine Use and Infection
Identifying Medicine Use Problems Using Indicator-Based Studies in Health Facilities Review of the Cesarean-section Antibiotic Prophylaxis Program in Jordan and Workshop on Rational Medicine Use and Infection
Dr René A. Carlson President, World Veterinary Association. The Current and Future Role of the WVA in Continuing Education for Veterinarians
 Dr René A. Carlson President, World Veterinary Association The Current and Future Role of the WVA in Continuing Education for Veterinarians CONTENT Introduction of the World Veterinary Association WVA
Dr René A. Carlson President, World Veterinary Association The Current and Future Role of the WVA in Continuing Education for Veterinarians CONTENT Introduction of the World Veterinary Association WVA
Submission for Reclassification
 Submission for Reclassification Fucithalmic (Fusidic Acid 1% Eye Drops) From Prescription Medicine to Restricted Medicine (Pharmacist Only Medicine) CSL Biotherapies (NZ) Limited 666 Great South Road Penrose
Submission for Reclassification Fucithalmic (Fusidic Acid 1% Eye Drops) From Prescription Medicine to Restricted Medicine (Pharmacist Only Medicine) CSL Biotherapies (NZ) Limited 666 Great South Road Penrose
RESPONSIBLE ANTIMICROBIAL USE
 RESPONSIBLE ANTIMICROBIAL USE IN THE CANADIAN CHICKEN AND TURKEY SECTORS VERSION 2.0 brought to you by: ANIMAL NUTRITION ASSOCIATION OF CANADA CANADIAN HATCHERY FEDERATION CANADIAN HATCHING EGG PRODUCERS
RESPONSIBLE ANTIMICROBIAL USE IN THE CANADIAN CHICKEN AND TURKEY SECTORS VERSION 2.0 brought to you by: ANIMAL NUTRITION ASSOCIATION OF CANADA CANADIAN HATCHERY FEDERATION CANADIAN HATCHING EGG PRODUCERS
THIS ARTICLE IS SPONSORED BY THE MINNESOTA DAIRY HEALTH CONFERENCE.
 THIS ARTICLE IS SPONSORED BY THE MINNESOTA DAIRY HEALTH CONFERENCE. ST. PAUL, MINNESOTA UNITED STATES OF MINNESOTA Responsible Drug Use: Has the Regulatory Cloud Been Lifted? M. Gatz Riddell, Jr. Auburn
THIS ARTICLE IS SPONSORED BY THE MINNESOTA DAIRY HEALTH CONFERENCE. ST. PAUL, MINNESOTA UNITED STATES OF MINNESOTA Responsible Drug Use: Has the Regulatory Cloud Been Lifted? M. Gatz Riddell, Jr. Auburn
Interdisciplinary Communication in Antimicrobial Stewardship. Jennifer Liao, PharmD September 29, 2017 Patient Safety Academy
 Interdisciplinary Communication in Antimicrobial Stewardship Jennifer Liao, PharmD September 29, 2017 Patient Safety Academy Objectives 1. Define antimicrobial stewardship (AMS) teams across various settings
Interdisciplinary Communication in Antimicrobial Stewardship Jennifer Liao, PharmD September 29, 2017 Patient Safety Academy Objectives 1. Define antimicrobial stewardship (AMS) teams across various settings