Guideline Updates Change is Inevitable Especially in Infectious Diseases!
|
|
|
- Stuart Roberts
- 5 years ago
- Views:
Transcription
1 Guideline Updates Change is Inevitable Especially in Infectious Diseases! Vicky Shah, PharmD, BCPS Assistant Professor of Pharmacy Practice Wilkes University Nesbitt School of Pharmacy 1

2 Vicky Shah has no potential or actual conflicts of interest to disclose. 2
3 Objectives Describe first line therapies for the treatment of Clostridium difficile Apply new pneumonia guidelines to your place of practice Evaluate antimicrobial stewardship at your institution 3
4 Clostridium Difficile Guidelines Update 2017/2018 4
5 The Infectious Diseases Society of America (IDSA) New 2017/2018 Guidelines The Society for Healthcare Epidemiology of America (SHEA) 5
6 Major Guideline Updates Inclusion of specific pediatric guidelines Discussion on laboratory guided diagnosis in adults Removal of metronidazole for 1 st line therapy in adults Discussion on fecal transplantation utilization Consideration of prophylaxis techniques 6
7 Clostridium difficile Gram-positive, anaerobic, spore-forming bacillus Infection is a result of a disturbance of the normal flora of the colon Responsible for development of antibiotic-associated diarrhea and colitis Incidence and severity of infection is increasing Leffler DA, Lamont JT. Treatment of Clostridium difficile-associated disease. Gastroenterology 2009;136(6): Hensgens MP, Goorhuis A, Dekkers OM, Kuijper EJ. Time interval of increased risk for Clostridium difficile infection after exposure to antibiotics. J Antimicrob Chemother 2012; 67:
8 Epidemiology Normal fecal flora 2% of healthy adults Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med 2015; 372:
9 How long will Clostridium difficile pathogens live on a dry surface? Mayfield JL, Leet T, Miller J, Mundy LM. Environmental control to reduce transmission of Clostridium difficile. Clin Infect Dis 2000; 31:
10 Pathophysiology Antibiotic Therapy Alteration of colonic microorganisms C. difficile exposure and colonization Release of Toxins A and B Binding to enterocyte receptors Colonic mucosal injury and acute inflammation Diarrhea and colitis Leffler DA, Lamont JT. Treatment of Clostridium difficile-associated disease. Gastroenterology 2009;136(6):
11 Symptoms Asymptomatic Colonization Diarrhea Abdominal Pain/Distension Fever Pseudomembranous Colitis Toxic Megacolon Death Leffler DA, Lamont JT. Treatment of Clostridium difficile-associated disease. Gastroenterology 2009;136(6): Cohen SH, Gerding DN, Johnson S, et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults: 2010 Update by the Society for Healthcare Epidemiology of America (SHEA) 11 and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol 2010;31(5):
12 Risk Factors Hospitalization Chronic Care Facility Antibiotics Age Surgery Chemotherapy Intestinal Obstruction PPIs Kuntz JL, Johnson ES, Raebel MA, et al. Predicting the risk of Clostridium difficile infection following an outpatient visit: development and external validation of a pragmatic, prognostic risk score. Clin Microbiol Infect 2015; 21: Chitnis AS, Holzbauer SM, Belflower RM, et al. Epidemiology of community-associated Clostridium difficile infection, 2009 through JAMA Intern Med 2013; 173: Leffler DA, Lamont JT. Treatment of Clostridium difficile-associated disease. Gastroenterology 2009;136(6): Negrón ME, Rezaie A, Barkema HW, et al. Ulcerative colitis patients with Clostridium difficile are at increased risk of death, colectomy, and postoperative complications: a population-based 12 inception cohort study. Am J Gastroenterol 2016; 111:
13 Antibiotic Related Risk High Risk Medium Risk Low Risk Clindamycin Macrolides Aminoglycosides Cephalosporins Tetracyclines Metronidazole Ampicillin/Amoxicillin Fluoroquinolones Anti-pseudomonas Penicillin Rifampin Vancomycin Hensgens MP, Goorhuis A, Dekkers OM, Kuijper EJ. Time interval of increased risk for Clostridium difficile infection after exposure to antibiotics. J Antimicrob Chemother 2012; 67:
14 14
15 Inclusion of Specific Pediatric Guidelines Major Update 15
16 Pediatric Additions Surveillance Diagnosis Treatment McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 16 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
17 Pediatric Surveillance Epidemiology of pediatric cases will be tracked and reported in the same manner as adult cases Patients under the age of 2 weeks will not be included in the surveillance McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 17 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
18 Pediatric Diagnosis Neonates or infants 12 months of age with diarrhea Testing is not recommended due to high prevalence of asymptomatic carriage Ages 1-2 Testing is not recommended UNLESS other infectious or noninfectious causes have been excluded Children 3 and older Testing is recommended for patients with prolonged or worsening diarrhea WITH risk factors (underlying inflammatory bowel disease, immunocompromising condition, recent contact with the healthcare system or recent antibiotic use) McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 18 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
19 Pediatric Treatment Clinical Definition Recommended Treatment Pediatric Dose Maximum Dose Non-severe (initial episode) Metronidazole PO x 10 days 7.5mg/kg/dose TID or QID 500mg TID or QID Vancomycin PO x 10 days 10mg/kg/dose QID 125mg QID Severe/Fulminant (initial episode) Non-severe (1 st recurrence) Second or subsequent recurrence Vancomycin PO x 10 days 10mg/kg/dose QID 500mg QID WITH OR WITHOUT Metronidazole IV x 10 days 10mg/kg/dose TID 500mg TID Metronidazole PO x 10 days 7.5mg/kg/dose TID or QID 500mg TID or QID Vancomycin PO x 10 days 10mg/kg/dose QID 125mg QID Vancomycin Taper/Pulse Dose 10mg/kg/dose QID 125mg QID Vancomycin PO x 10 days followed by Rifaximin PO x 20 days No pediatric dosing for Rifaximin Fecal Microbiota Transplantation Vancomycin 500mg QID Rifaximin 400mg TID McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 19 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
20 Discussion on Laboratory Guided Diagnosis in Adults Major Update 20
21 Diagnosis Past medical history of the patient Laboratory results Symptoms (number of unformed stools in a 24 hour period) McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 21 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
22 Diagnosis If the institution uses only specimens from patients who are not taking laxatives and have at least 3 or more unformed stools in a 24 hour period Glutamate dehydrogenase (GDH) followed by a stool toxin test Nucleic Acid Amplification Test (NAAT) alone is satisfactory! If GDH comes back negative, follow-up with the NAAT Stool toxin test may be recommended to confirm the diagnosis McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 22 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
23 Nonpharmacological Treatments Discontinue antibiotics Fluid and electrolyte replacement Isolation Avoid antimotility agents Fecal Microbiota Transplantations (FMT) 23 McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
24 Severity Classification Non-Severe WBC Count <15,000 Severe WBC Count >15,000 SCr > 1.5mg/dL Fulminant WBC Count >15,000 SCr > 1.5mg/dL Signs of Complications Hypotension/shock Ileus Toxic Megacolon McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 24 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
25 Removal of Metronidazole for 1 st Line Therapy in Adults Major Update 25
26 Treatment Clinical Definition Recommended Treatment Vancomycin PO 125mg QID x 10 days Non-severe (initial episode) Fidaxomicin 200mg BID x 10 days Metronidazole 500mg BID x 10 days (only if Vancomycin and Fidaxomicin are unavailable) Severe (initial episode) Vancomycin PO 125mg QID x 10 days Fidaxomicin 200mg BID x 10 days Vancomycin PO 500mg QID x 10 days Fulminant (initial episode) WITH Metronidazole IV 500mg TID x 10 days McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 26 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
27 Treatment Clinical Definition Recommended Treatment If Metronidazole used during 1 st episode Vancomycin PO 125mg QID x 10 days First recurrence If Vancomycin used during 1 st episode Vancomycin Taper/Pulse Dose If Vancomycin used during 1 st episode Fidaxomicin 200mg BID x 10 days Vancomycin Taper/Pulse Dose Second recurrence Vancomycin PO 125mg QID x 10 days following by Rifaximin 400mg TID x 20 days Fidaxomicin 200mg BID x 10 days Fecal Microbiota Transplantation McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 27 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
28 Discussion on Fecal Transplantation Utilization Major Update 28
29 Fecal Microbiota Transplantation (FMT) Previously not recommended in 2010 guidelines as not much data was available 77-94% efficacy rate for treating and reducing reoccurrences Recommended for patients with multiple recurrences with failure of appropriate antibiotic treatments Bakken JS, Borody T, Brandt LJ, Brill JV, Demarco DC, Franzos MA, Kelly C, Khoruts A, Louie T, Martinelli LP, Moore TA, Russell G, Surawicz C (December 2011). "Treating Clostridium difficile infection with fecal microbiota transplantation". Clinical Gastroenterology and Hepatology. 9 (12): doi: /j.cgh PMC PMID MacConnachie AA, Fox R, Kennedy DR, Seaton RA. Faecal transplant for recurrent Clostridium difficile-associated diarrhoea: a UK case series. QJM 2009; 02: Rubin TA, Gessert CE, Aas J, Bakken JS. Fecal microbiome transplantation for recurrent Clostridium difficile infection: report on a case series. Anaerobe 2013; 19:22 6.
30 What makes someone a good candidate to be a DONOR? 30
31 Donor Requirements Healthy individual No history of irritable bowel diseases, crohn s disease, gastrointestinal cancer, etc. No active autoimmune disorders No antibiotic use in the last 90 days Not an asymptomatic carrier of Clostridium difficile Best candidate is someone with a similar diet as the recipient Bakken JS, Borody T, Brandt LJ, Brill JV, Demarco DC, Franzos MA, Kelly C, Khoruts A, Louie T, Martinelli LP, Moore TA, Russell G, Surawicz C (December 2011). "Treating Clostridium difficile infection with fecal microbiota transplantation". Clinical Gastroenterology and Hepatology. 9 (12): doi: /j.cgh PMC PMID MacConnachie AA, Fox R, Kennedy DR, Seaton RA. Faecal transplant for recurrent Clostridium difficile-associated diarrhoea: a UK case series. QJM 2009; 02: Rubin TA, Gessert CE, Aas J, Bakken JS. Fecal microbiome transplantation for recurrent Clostridium difficile infection: report on a case series. Anaerobe 2013; 19:22 6.
32 Consideration of Prophylaxis Techniques Major Update 32
33 Prophylaxis Probiotics may be effective at preventing infections when given to patients on antibiotics who do not have a history of Clostridium difficile Probiotic use is NOT currently supported due to lack of significant results in controlled trials Lactobacillus and Saccharomyces boulardii have been associated with some reduction in recurrence McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 33 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
34 Prophylaxis Patients who complete appropriate treatment for Clostridium difficile requiring antibiotic therapy for other infections may be provided prophylaxis treatment with Vancomycin 125mg daily or Fidaxomicin 200mg daily. Treatment duration of their Clostridium difficile treatment may also be extended beyond 10 days until completion of their new antibiotic for other infections Guidelines do not fully support prophylaxis but initial studies have shown reduction in recurrences when prophylaxis or extended therapy is administered McDonald, L. Clifford, et al. "Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for 34 Healthcare Epidemiology of America (SHEA)." Clinical Infectious Diseases 66.7 (2018): e1-e48.
35 HAP/VAP Guidelines Update
36 Major Guideline Updates Removal of the concept of Health Care Associated Pneumonia (HCAP) Larger emphasis on local institutions collecting data and creating antibiogram Decrease the unnecessary use of dual gram-negative and empiric MRSA coverage Shorter duration of therapy 36
37 Removal of the Concept of Health Care Associated Pneumonia (HCAP) Major Update 37

 Pneumonia developing 48 hours after admission Ventilator Associated Pneumonia (VAP) Aspiration Pneumonia (AP) Pneumonia developing 48 hours after")
38 Type of Pneumonia Definition Community Acquired Pneumonia (CAP) Pneumonia developing in patients with no contact to a medical facility Types of Pneumonia Healthcare Associated Pneumonia (HCAP) Pneumonia developing in patients not in medical facility but two or more risk factors for multidrug resistant pathogens: Recent hospitalization 2 days within past 90 days Nursing home or long-term care patients Recent antibiotic use, IV therapy, wound care, or chemotherapy within past 30 days Hemodialysis patient within past 30 days Contact with family member who has multidrug resistant pathogen infection Hospital Acquired Pneumonia (HAP) Pneumonia developing 48 hours after admission Ventilator Associated Pneumonia (VAP) Aspiration Pneumonia (AP) Pneumonia developing 48 hours after intubation and mechanical ventilation Pneumonia developing in alcoholic patients or patients who 38 have trouble swallowing
39 Healthcare Associated Pneumonia New IDSA 2016 guidelines recommend treating HCAP similar to CAP Older guidelines treated closer to HAP/VAP but newer guidelines reduce resistance and overuse of antibiotics 39
40 Larger Emphasis on Local Institutions Collecting Data and Creating Antibiogram Major Update 40
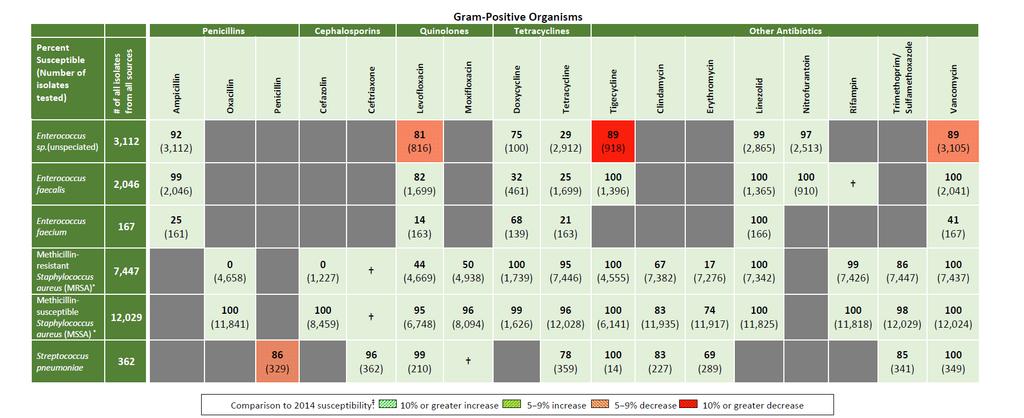
41 Antibiogram Example 41
42 Decrease the Unnecessary Use of Dual Gram-Negative and Empiric MRSA Coverage Major Update 42
43 Minimum Empiric Treatment for HAP/VAP Staphylococcus aureus MSSA coverage if MRSA negative Pseudomonas auroginosa coverage Single agent is appropriate 43 Kalil, Andre C., et al. "Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society." Clinical Infectious Diseases 63.5 (2016): e61-e111.
44 MRSA Treatment Greater than 10-20% MRSA in hospital Staphylococcus aureus isolates or unknown MRSA prevalence 44 Kalil, Andre C., et al. "Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society." Clinical Infectious Diseases 63.5 (2016): e61-e111.
45 Aggressive Anti-Pseudomonas Coverage HAP Ventilator support Septic shock Prior IV antibiotic use within 90days VAP Prior IV antibiotic use within 90days Septic Shock at time of VAP Acute Respiratory Distress Syndrome preceding VAP Five or more days of hospitalization prior to the occurrence of VAP Acute renal replacement therapy prior to VAP onset Structural Lung Disease >10% Pseudomonas Resistance Abundance of GNB on Gram Stain 45 Kalil, Andre C., et al. "Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society." Clinical Infectious Diseases 63.5 (2016): e61-e111.
46 Empiric Treatment 46 Kalil, Andre C., et al. "Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society." Clinical Infectious Diseases 63.5 (2016): e61-e111.
47 If dual pseudomonas coverage is needed, which of the following combinations would you recommend? A. Cefepime PLUS Zosyn B. Levofloxacin PLUS Zosyn C. Ceftriaxone PLUS Imipenem D. Cefepime PLUS Ertapenem 47
48 Not at high risk of mortality and no factors increasing likelihood of MRSA Zosyn OR Cefepime OR Levofloxacin OR Carbapenem Empiric Therapy Not at high risk of mortality but with factors increasing likelihood of MRSA Zosyn OR Cefepime or Ceftazidime OR Levofloxacin or Ciprofloxacin OR Carbapenem OR Aztreonam PLUS Vancomycin OR Linezolid High risk of mortality Zosyn OR Cefepime or Ceftazidime OR Carbapenem OR Aztreonam PLUS Levofloxacin or Ciprofloxacin OR Aminoglycoside PLUS Vancomycin OR Linezolid OR MSSA Coverage Kalil, Andre C., et al. "Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society." Clinical Infectious Diseases 63.5 (2016): e61-e
49 Shorter Duration of Therapy Major Update 49
50 Duration of Therapy 7 days 50 Kalil, Andre C., et al. "Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society." Clinical Infectious Diseases 63.5 (2016): e61-e111.
51 Role of Antibiotic Stewardship 51
52 Antibiotic Stewardship Minimize the frequency and duration of high risk antibiotic therapy and the number of antibiotic agents prescribed Implement an antibiotic stewardship program! Encourage in ALL IDSA/SHEA guidelines Target treatment based on local epidemiology and institution specific resistance rates. Restriction of fluoroquinolones, clindamycin and cephalosporin antibiotics may be considered (especially for Clostridium difficile risk patients) 52
53 What Questions Do You Have? 53
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Learning Objectives 6/1/18
 Gulf Coast Multidisciplinary Pharmacotherapy Conference Kelly R. Reveles, PharmD, PhD, BCPS College of Pharmacy, The University of Texas at Austin School of Medicine, UT Health San Antonio Email: kdaniels46@utexas.edu
Gulf Coast Multidisciplinary Pharmacotherapy Conference Kelly R. Reveles, PharmD, PhD, BCPS College of Pharmacy, The University of Texas at Austin School of Medicine, UT Health San Antonio Email: kdaniels46@utexas.edu
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship
 Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Overview of C. difficile infections. Kurt B. Stevenson, MD MPH Professor Division of Infectious Diseases
 Overview of C. difficile infections Kurt B. Stevenson, MD MPH Professor Division of Infectious Diseases Conflicts of Interest I have no financial conflicts of interest related to this topic and presentation.
Overview of C. difficile infections Kurt B. Stevenson, MD MPH Professor Division of Infectious Diseases Conflicts of Interest I have no financial conflicts of interest related to this topic and presentation.
Clostridium difficile Colitis
 Update on Clostridium difficile Colitis Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
Update on Clostridium difficile Colitis Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
11/2/2015. Update on the Treatment of Clostridium difficile Infections. Disclosure. Objectives
 Update on the Treatment of Clostridium difficile Infections Spencer H. Durham, Pharm.D.,BCPS (AQ-ID) Assistant Clinical Professor of Pharmacy Practice Auburn University Harrison School of Pharmacy Kurt
Update on the Treatment of Clostridium difficile Infections Spencer H. Durham, Pharm.D.,BCPS (AQ-ID) Assistant Clinical Professor of Pharmacy Practice Auburn University Harrison School of Pharmacy Kurt
Community-Associated C. difficile Infection: Think Outside the Hospital. Maria Bye, MPH Epidemiologist May 1, 2018
 Community-Associated C. difficile Infection: Think Outside the Hospital Maria Bye, MPH Epidemiologist Maria.Bye@state.mn.us 651-201-4085 May 1, 2018 Clostridium difficile Clostridium difficile Clostridium
Community-Associated C. difficile Infection: Think Outside the Hospital Maria Bye, MPH Epidemiologist Maria.Bye@state.mn.us 651-201-4085 May 1, 2018 Clostridium difficile Clostridium difficile Clostridium
Incidence of hospital-acquired Clostridium difficile infection in patients at risk
 Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 5-20-2016 Incidence of hospital-acquired Clostridium difficile infection in patients at risk Christine Ibarra
Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 5-20-2016 Incidence of hospital-acquired Clostridium difficile infection in patients at risk Christine Ibarra
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Clostridium Difficile Primer: Disease, Risk, & Mitigation
 Clostridium Difficile Primer: Disease, Risk, & Mitigation KALVIN YU, M.D. CHIEF INTEGRATION OFFICER, SCPMG/SCAL KAISER PERMANENTE ASSOCIATE PROFESSOR INFECTIOUS DISEASE, COLLEGE OF GLOBAL PUBLIC HEALTH,
Clostridium Difficile Primer: Disease, Risk, & Mitigation KALVIN YU, M.D. CHIEF INTEGRATION OFFICER, SCPMG/SCAL KAISER PERMANENTE ASSOCIATE PROFESSOR INFECTIOUS DISEASE, COLLEGE OF GLOBAL PUBLIC HEALTH,
Clostridium difficile Colitis
 1 Clostridium difficile Colitis William R. Sonnenberg, MD 2 Disclosure Dr. Sonnenberg has no conflict of interest, financial agreement, or working affiliation with any group or organization. 3 Learning
1 Clostridium difficile Colitis William R. Sonnenberg, MD 2 Disclosure Dr. Sonnenberg has no conflict of interest, financial agreement, or working affiliation with any group or organization. 3 Learning
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
Inappropriate Use of Antibiotics and Clostridium difficile Infection. Jocelyn Srigley, MD, FRCPC November 1, 2012
 Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Preventing Multi-Drug Resistant Organism (MDRO) Infections. For National Patient Safety Goal
 Infections. For National Patient Safety Goal") Preventing Multi-Drug Resistant Organism (MDRO) Infections For National Patient Safety Goal 07.03.01 2009 Methicillin Resistant Staphlococcus aureus (MRSA) About 3-8% of the population at large is a carrier
Preventing Multi-Drug Resistant Organism (MDRO) Infections For National Patient Safety Goal 07.03.01 2009 Methicillin Resistant Staphlococcus aureus (MRSA) About 3-8% of the population at large is a carrier
Clostridium difficile Surveillance Report 2016
 Clostridium difficile Surveillance Report 2016 EMERGING INFECTIONS PROGRAM Clostridium difficile Surveillance Report 2016 Minnesota Department of Health Emerging Infections Program PO Box 64882, St. Paul,
Clostridium difficile Surveillance Report 2016 EMERGING INFECTIONS PROGRAM Clostridium difficile Surveillance Report 2016 Minnesota Department of Health Emerging Infections Program PO Box 64882, St. Paul,
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017
 Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
Antimicrobial Stewardship 101
 Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
Antimicrobial stewardship in managing septic patients
 Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Clostridium difficile infection: The Present and the Future
 Clostridium difficile infection: The Present and the Future Carlos E. Figueroa Castro, MD Assistant Professor, Division of Infectious Diseases Medical College of Wisconsin November 2014 I have made this
Clostridium difficile infection: The Present and the Future Carlos E. Figueroa Castro, MD Assistant Professor, Division of Infectious Diseases Medical College of Wisconsin November 2014 I have made this
Clostridium difficile Infection: An Update on the Current State of Prevention
 Intermountain APIC and Qualis Health present I-APIC HAI Prevention Learning Network Webinar Series Clostridium difficile Infection An Update on the April 11, 2012 Ruth CarricoPhD RN FSHEA CIC Clostridium
Intermountain APIC and Qualis Health present I-APIC HAI Prevention Learning Network Webinar Series Clostridium difficile Infection An Update on the April 11, 2012 Ruth CarricoPhD RN FSHEA CIC Clostridium
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles
 Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Objectives. Review basic categories of intra-abdominal infection and their respective treatments. Community acquired intra-abdominal infection
 Objectives Review basic categories of intra-abdominal infection and their respective treatments Community acquired intra-abdominal infection Mild/Moderate Severe Acute biliary tract infections Nosocomial
Objectives Review basic categories of intra-abdominal infection and their respective treatments Community acquired intra-abdominal infection Mild/Moderate Severe Acute biliary tract infections Nosocomial
DATA COLLECTION SECTION BY FRONTLINE TEAM. Patient Identifier/ Medical Record number (for facility use only)
") Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
3/20/2011. Code 215 of Hammurabi: If a physician performed a major operation on
 The Good Antibiotics: the Good, the Bad and the Ugly John P. Cello, MD Professor of Medicine and Surgery, University of California, San Francisco Most organisms can be readily identified by culture, special
The Good Antibiotics: the Good, the Bad and the Ugly John P. Cello, MD Professor of Medicine and Surgery, University of California, San Francisco Most organisms can be readily identified by culture, special
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Preventing Clostridium difficile Infection (CDI)
") 1 Preventing Clostridium difficile Infection (CDI) All Hands on Deck to Reduce CDI Skill Nursing Facility Conference July 28, 2017 Idamae Kennedy, MPH,BSN,RN,CIC Liaison Infection Preventionist Healthcare
1 Preventing Clostridium difficile Infection (CDI) All Hands on Deck to Reduce CDI Skill Nursing Facility Conference July 28, 2017 Idamae Kennedy, MPH,BSN,RN,CIC Liaison Infection Preventionist Healthcare
Infectious Disease Update 2017
 Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Infectious Disease Update 2017 Greg Moran, MD, FACEP, FIDSA Professor of Clinical Emergency Medicine Geffen School of Medicine at UCLA Dept. of Emergency Medicine and Division of Infectious Diseases Olive
Antibiotic Stewardship Beyond Hospital Walls
 Antibiotic Stewardship Beyond Hospital Walls Katie Burenheide Foster, PharmD, MS, BCPS, FCCM Pharmacy Clinical Manager & PGY1 Pharmacy Residency Director OBJECTIVES 1. Review what Antibiotic Stewardship
Antibiotic Stewardship Beyond Hospital Walls Katie Burenheide Foster, PharmD, MS, BCPS, FCCM Pharmacy Clinical Manager & PGY1 Pharmacy Residency Director OBJECTIVES 1. Review what Antibiotic Stewardship
Healthcare-associated Infections Annual Report December 2018
 December 2018 Healthcare-associated Infections Annual Report 2011-2017 TABLE OF CONTENTS INTRODUCTION... 1 METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS INFECTIONS... 2 MRSA SURVEILLANCE... 3 CLOSTRIDIUM
December 2018 Healthcare-associated Infections Annual Report 2011-2017 TABLE OF CONTENTS INTRODUCTION... 1 METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS INFECTIONS... 2 MRSA SURVEILLANCE... 3 CLOSTRIDIUM
Section 10: Antimicrobial Stewardship and Clostridium difficile Infection: A Primer for the Infection Preventionist
 Section 10: Antimicrobial Stewardship and Clostridium difficile Infection: A Primer for the Infection Preventionist Antimicrobial stewardship may be a relatively new addition to the job responsibilities
Section 10: Antimicrobial Stewardship and Clostridium difficile Infection: A Primer for the Infection Preventionist Antimicrobial stewardship may be a relatively new addition to the job responsibilities
OBJECTIVES. Fast Facts 3/23/2017. Antibiotic Stewardship Beyond Hospital Walls. Antibiotics are a shared resource and becoming a scarce resource.
 Antibiotic Stewardship Beyond Hospital Walls Katie Burenheide Foster, PharmD, MS, BCPS, FCCM Pharmacy Clinical Manager & PGY1 Pharmacy Residency Director OBJECTIVES 1. Review what Antibiotic Stewardship
Antibiotic Stewardship Beyond Hospital Walls Katie Burenheide Foster, PharmD, MS, BCPS, FCCM Pharmacy Clinical Manager & PGY1 Pharmacy Residency Director OBJECTIVES 1. Review what Antibiotic Stewardship
8/17/2016 ABOUT US REDUCTION OF CLOSTRIDIUM DIFFICILE THROUGH THE USE OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM
 Mary Moore, MS CIC MT (ASCP) Infection Prevention Coordinator Great River Medical Center, West Burlington REDUCTION OF CLOSTRIDIUM DIFFICILE THROUGH THE USE OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM ABOUT
Mary Moore, MS CIC MT (ASCP) Infection Prevention Coordinator Great River Medical Center, West Burlington REDUCTION OF CLOSTRIDIUM DIFFICILE THROUGH THE USE OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM ABOUT
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Clostridium difficile may be found in 1% to 3% of all
 ORIGINAL ARTICLE Evaluating contemporary antibiotics as a risk factor for Clostridium difficile infection in surgical trauma patients Kruti Shah, PharmD, BCPS, Leigh Ann Pass, PharmD, BCPS, Mark Cox, PharmD,
ORIGINAL ARTICLE Evaluating contemporary antibiotics as a risk factor for Clostridium difficile infection in surgical trauma patients Kruti Shah, PharmD, BCPS, Leigh Ann Pass, PharmD, BCPS, Mark Cox, PharmD,
Clostridium difficile: Review of Treatment & Prevention through Antimicrobial Stewardship
 Clostridium difficile: Review of Treatment & Prevention through Antimicrobial Stewardship Kim Van Wyk, Pharm.D., BCPS Mountain-Pacific Quality Health Objectives Review epidemiology of Clostridium diffilcile
Clostridium difficile: Review of Treatment & Prevention through Antimicrobial Stewardship Kim Van Wyk, Pharm.D., BCPS Mountain-Pacific Quality Health Objectives Review epidemiology of Clostridium diffilcile
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Becker s Hospital Review
 Becker s Hospital Review Oct 2, 2014 Top 10 Best Practices for Antimicrobial Stewardship & Hospital Infection Prevention Presented in Cooperation with Today s Panelists: Stacy Pur, RN (Moderator) Vice
Becker s Hospital Review Oct 2, 2014 Top 10 Best Practices for Antimicrobial Stewardship & Hospital Infection Prevention Presented in Cooperation with Today s Panelists: Stacy Pur, RN (Moderator) Vice
Discussion Points. Decisions in Selecting Antibiotics
 Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Pharmacist Coordinated Antimicrobial Therapy: OPAT and Transitions of Care
 Pharmacist Coordinated Antimicrobial Therapy: OPAT and Transitions of Care Jennifer McCann, PharmD, BCCCP State Director of Clinical Pharmacy Services St. Vincent Health Indiana Conflicts of Interest No
Pharmacist Coordinated Antimicrobial Therapy: OPAT and Transitions of Care Jennifer McCann, PharmD, BCCCP State Director of Clinical Pharmacy Services St. Vincent Health Indiana Conflicts of Interest No
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Educational Module for Nursing Assistants in Long-term Care Facilities: Preventing and Managing Clostridium difficile Infections
 Educational Module for Nursing Assistants in Long-term Care Facilities: Preventing and Managing Clostridium difficile Infections Minnesota Department of Health Infectious Disease Epidemiology, Prevention,
Educational Module for Nursing Assistants in Long-term Care Facilities: Preventing and Managing Clostridium difficile Infections Minnesota Department of Health Infectious Disease Epidemiology, Prevention,
UPDATES IN INFECTIOUS DISEASES
 Disclosures UPDATES IN INFECTIOUS DISEASES Nothing to disclose Jacob Kesner, PharmD Lovelace Medical Center Albuquerque, NM 2018 NMSHP Balloon Fiesta Symposium Objectives Outline Pharmacist: 1. Recall
Disclosures UPDATES IN INFECTIOUS DISEASES Nothing to disclose Jacob Kesner, PharmD Lovelace Medical Center Albuquerque, NM 2018 NMSHP Balloon Fiesta Symposium Objectives Outline Pharmacist: 1. Recall
The Epidemiology Of Clostridium Difficile Infections Among Oncology Patients
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Public Health Theses School of Public Health January 2015 The Epidemiology Of Clostridium Difficile Infections Among Oncology
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Public Health Theses School of Public Health January 2015 The Epidemiology Of Clostridium Difficile Infections Among Oncology
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
FM - Male, 38YO. MRSA nasal swab (+) Due to positive MRSA nasal swab test, patient will be continued on Vancomycin 1500mg IV q12 for MRSA treatment...
 Due to positive MRSA nasal swab test, patient will be continued on Vancomycin 1500mg IV q12 for MRSA treatment...") Jillian O Keefe Doctor of Pharmacy Candidate 2016 September 15, 2015 FM - Male, 38YO HPI: Previously healthy male presents to ED febrile (102F) and in moderate distress ~2 weeks after getting a tattoo
Jillian O Keefe Doctor of Pharmacy Candidate 2016 September 15, 2015 FM - Male, 38YO HPI: Previously healthy male presents to ED febrile (102F) and in moderate distress ~2 weeks after getting a tattoo
Provincial Drugs & Therapeutics Committee Memorandum Version 2
 Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults
 Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
9/30/2016. Dr. Janell Mayer, Pharm.D., CGP, BCPS Dr. Lindsey Votaw, Pharm.D., CGP, BCPS
 Dr. Janell Mayer, Pharm.D., CGP, BCPS Dr. Lindsey Votaw, Pharm.D., CGP, BCPS 1 2 Untoward Effects of Antibiotics Antibiotic resistance Adverse drug events (ADEs) Hypersensitivity/allergy Drug side effects
Dr. Janell Mayer, Pharm.D., CGP, BCPS Dr. Lindsey Votaw, Pharm.D., CGP, BCPS 1 2 Untoward Effects of Antibiotics Antibiotic resistance Adverse drug events (ADEs) Hypersensitivity/allergy Drug side effects
Should we test Clostridium difficile for antimicrobial resistance? by author
 Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
UPDATES IN INFECTIOUS DISEASES
 UPDATES IN INFECTIOUS DISEASES Jacob Kesner, PharmD Lovelace Medical Center Albuquerque, NM 2018 NMSHP Balloon Fiesta Symposium Disclosures Nothing to disclose 1 Objectives Pharmacist: 1. Recall infectious
UPDATES IN INFECTIOUS DISEASES Jacob Kesner, PharmD Lovelace Medical Center Albuquerque, NM 2018 NMSHP Balloon Fiesta Symposium Disclosures Nothing to disclose 1 Objectives Pharmacist: 1. Recall infectious
Antimicrobial Stewardship
 Antimicrobial Stewardship Background Why Antimicrobial Stewardship 30-50% of antibiotic use in hospitals are unnecessary or inappropriate Appropriate antimicrobial use is a medication-safety and patient-safety
Antimicrobial Stewardship Background Why Antimicrobial Stewardship 30-50% of antibiotic use in hospitals are unnecessary or inappropriate Appropriate antimicrobial use is a medication-safety and patient-safety
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center
 Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center Case 1 60 yo healthy female admitted for fevers and dysuria.
Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center Case 1 60 yo healthy female admitted for fevers and dysuria.
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Super Bugs and Wonder Drugs: Protecting the One While Respecting the Many
 Super Bugs and Wonder Drugs: Protecting the One While Respecting the Many Vicki Stringfellow, MSN, CPNP-AC/PC Werner Division of Pediatric Critical Care University of Kentucky Lexington, KY Disclosure
Super Bugs and Wonder Drugs: Protecting the One While Respecting the Many Vicki Stringfellow, MSN, CPNP-AC/PC Werner Division of Pediatric Critical Care University of Kentucky Lexington, KY Disclosure
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Running head: CLOSTRIDIUM DIFFICILE 1
 Running head: CLOSTRIDIUM DIFFICILE 1 Clostridium difficile Infection Christy Lee Fenton Mountainland Applied Technology College CLOSTRIDIUM DIFFICILE 2 Clostridium difficile Infection Approximately 200,000
Running head: CLOSTRIDIUM DIFFICILE 1 Clostridium difficile Infection Christy Lee Fenton Mountainland Applied Technology College CLOSTRIDIUM DIFFICILE 2 Clostridium difficile Infection Approximately 200,000
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Best Practices: Goals of Antimicrobial Stewardship
 Best Practices: Goals of Antimicrobial Stewardship Gail Scully, M.D, M.P.H. and Elizabeth Radigan, PharmD, BCPS UMass Memorial Medical Center Division of Infectious Disease Department of Medicine September
Best Practices: Goals of Antimicrobial Stewardship Gail Scully, M.D, M.P.H. and Elizabeth Radigan, PharmD, BCPS UMass Memorial Medical Center Division of Infectious Disease Department of Medicine September
Antimicrobial Stewardship: The Premier Health Experience
 Antimicrobial Stewardship: The Premier Health Experience Steve Burdette, MD, FIDSA Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship Miami
Antimicrobial Stewardship: The Premier Health Experience Steve Burdette, MD, FIDSA Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship Miami
Head to Toe: Common infections in Hospital settings. Katya Calvo MD Medical Director of Antimicrobial Stewardship Division of Infectious Diseases
 Head to Toe: Common infections in Hospital settings Katya Calvo MD Medical Director of Antimicrobial Stewardship Division of Infectious Diseases Objectives To identify at least one common infection in
Head to Toe: Common infections in Hospital settings Katya Calvo MD Medical Director of Antimicrobial Stewardship Division of Infectious Diseases Objectives To identify at least one common infection in
Antibiotic stewardship in long term care
 Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Clostridium difficile
 Clostridium difficile A Challenge in Long-Term Care Andrew E. Simor, MD, FRCPC Sunnybrook Health Sciences Centre University of Toronto Hosted by Paul Webber paul@webbertraining.com Objectives to understand
Clostridium difficile A Challenge in Long-Term Care Andrew E. Simor, MD, FRCPC Sunnybrook Health Sciences Centre University of Toronto Hosted by Paul Webber paul@webbertraining.com Objectives to understand
Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report. July December 2013 Second and Third Quarters 2014
 Antimicrobial Stewardship Report. July December 2013 Second and Third Quarters 2014") H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report July December 213 Second and Third Quarters
H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report July December 213 Second and Third Quarters
Meropenem for all? Midge Asogan ICU Fellow (also ID AT)
") Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Antimicrobial Prescribing Advice for patients with Clostridium difficile Associated Diarrhoea
 For use in: By: For: Antimicrobial Prescribing Advice for patients with Clostridium difficile Division responsible for document: Key words: Names of document authors: Job titles of document authors: Name
For use in: By: For: Antimicrobial Prescribing Advice for patients with Clostridium difficile Division responsible for document: Key words: Names of document authors: Job titles of document authors: Name
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS
 PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
PIPERACILLIN- TAZOBACTAM INJECTION - SUPPLY PROBLEMS The current supply of piperacillin- tazobactam should be reserved f Microbiology / Infectious Diseases approval and f neutropenic sepsis, severe sepsis
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland
 Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
Management of Hospital-acquired Pneumonia
 Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
03/09/2014. Infection Prevention and Control A Foundation Course. Talk outline
 Infection Prevention and Control A Foundation Course 2014 What is healthcare-associated infection (HCAI), antimicrobial resistance (AMR) and multi-drug resistant organisms (MDROs)? Why we should be worried?
Infection Prevention and Control A Foundation Course 2014 What is healthcare-associated infection (HCAI), antimicrobial resistance (AMR) and multi-drug resistant organisms (MDROs)? Why we should be worried?
Healthcare-associated Infections Annual Report March 2015
 March 2015 Healthcare-associated Infections Annual Report 2009-2014 TABLE OF CONTENTS SUMMARY... 1 MRSA SURVEILLANCE RESULTS... 1 CDI SURVEILLANCE RESULTS... 1 INTRODUCTION... 2 METHICILLIN-RESISTANT
March 2015 Healthcare-associated Infections Annual Report 2009-2014 TABLE OF CONTENTS SUMMARY... 1 MRSA SURVEILLANCE RESULTS... 1 CDI SURVEILLANCE RESULTS... 1 INTRODUCTION... 2 METHICILLIN-RESISTANT
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP)
") IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
Optimize Durations of Antimicrobial Therapy
 Optimize Durations of Antimicrobial Therapy Evidence & Application Jill Cowper, Pharm.D. Division Infectious Diseases Pharmacist Parallon Supply Chain Solutions Richmond, VA P: 607 221 5101 jill.butterfield@parallon.com
Optimize Durations of Antimicrobial Therapy Evidence & Application Jill Cowper, Pharm.D. Division Infectious Diseases Pharmacist Parallon Supply Chain Solutions Richmond, VA P: 607 221 5101 jill.butterfield@parallon.com
SOFT Movement Survey of FMT Programs
 Appendix 1 (as supplied by the authors): Survey SOFT Movement Survey of FMT Programs Part 1: General Information about your Fecal Microbiota Transplant (FMT) Program 1) Please fill out the information
Appendix 1 (as supplied by the authors): Survey SOFT Movement Survey of FMT Programs Part 1: General Information about your Fecal Microbiota Transplant (FMT) Program 1) Please fill out the information
Clostridium difficile Infection Prevention. Basics of Infection Prevention 2-Day Mini-Course 2012
 Clostridium difficile Infection Prevention Basics of Infection Prevention 2-Day Mini-Course 2012 2 Objectives Describe the etiology and epidemiology of C. difficile infection (CDI) Review evidence-based
Clostridium difficile Infection Prevention Basics of Infection Prevention 2-Day Mini-Course 2012 2 Objectives Describe the etiology and epidemiology of C. difficile infection (CDI) Review evidence-based
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Clostridium Difficile Infection (CDI) Alistair McGregor Hobart Pathology Royal Hobart Hospital TIPCU
 Alistair McGregor Hobart Pathology Royal Hobart Hospital TIPCU") Clostridium Difficile Infection (CDI) Alistair McGregor Hobart Pathology Royal Hobart Hospital TIPCU Disclosures I am not Tom Riley The Fidaxomicin guys brought me dinner once Outline ASID/AICA position
Clostridium Difficile Infection (CDI) Alistair McGregor Hobart Pathology Royal Hobart Hospital TIPCU Disclosures I am not Tom Riley The Fidaxomicin guys brought me dinner once Outline ASID/AICA position
National Clinical Guideline Centre Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults
 National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
* gender factor (male=1, female=0.85)
") Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Usual Doses of Antimicrobials Typically Not Requiring Renal Adjustment Azithromycin 250 500 mg Q24 *Amphotericin B 1 3-5 mg/kg Q24 Clindamycin 600 900 mg Q8 Liposomal (Ambisome ) Doxycycline 100 mg Q12
Sepsis is the most common cause of death in
 ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
Source: Portland State University Population Research Center (
 Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Antibiotic Stewardship
 Antibiotic Stewardship Nick Zaksek Pharm D., BCPS AQ-ID Infectious Disease POMA 2019 1 Disclosures None 2 Objectives Practice good Antibiotic stewardship and foster the notion of antibiotic stewardship
Antibiotic Stewardship Nick Zaksek Pharm D., BCPS AQ-ID Infectious Disease POMA 2019 1 Disclosures None 2 Objectives Practice good Antibiotic stewardship and foster the notion of antibiotic stewardship
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Practical Pearls for Effective Sustainable Stewardship Programs
 Practical Pearls for Effective Sustainable Stewardship Programs Promoting Antimicrobial Stewardship Programs in Minnesota Oct. 24 th, 2013 MOA Bloomington, MN Susan Kline, MD, MPH Introduction Lead Physician
Practical Pearls for Effective Sustainable Stewardship Programs Promoting Antimicrobial Stewardship Programs in Minnesota Oct. 24 th, 2013 MOA Bloomington, MN Susan Kline, MD, MPH Introduction Lead Physician
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases
 The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Antimicrobial Stewardship Programs The Same, but Different. Sara Nausheen, MD Kevin Kern, PharmD
 Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS
 Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Reply to Fabre et. al
 Reply to Fabre et. al L. Clifford McDonald, 1 Stuart Johnson, 2,3 Johan S. Bakken, 4 Kevin W. Garey, 5 Ciaran Kelly, 6 Dale N. Gerding, 2 1 Centers for Disease Control and Prevention, Atlanta, Georgia;
Reply to Fabre et. al L. Clifford McDonald, 1 Stuart Johnson, 2,3 Johan S. Bakken, 4 Kevin W. Garey, 5 Ciaran Kelly, 6 Dale N. Gerding, 2 1 Centers for Disease Control and Prevention, Atlanta, Georgia;
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered