AND MISCONCEPTIONS IN THE MANAGEMENT OF SEPSIS
|
|
|
- Tracy O’Neal’
- 5 years ago
- Views:
Transcription

1 MYTHS AND MISCONCEPTIONS IN THE MANAGEMENT OF SEPSIS SEPSISMADE EASY SURVIVINGSEPSIS COOKBOOK SEPSIS ISAPIE MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK
2 DISCUSSION POINTS.. Guidelines should be slavishly followed One size fits all Every hour of antibiotic delay kills How long should a course of antibiotics last? Sepsis mortality is improving Why do people die of sepsis?
3 DISCUSSION POINTS.. Guidelines should be slavishly followed One size fits all Every hour of antibiotic delay kills How long should a course of antibiotics last? Sepsis mortality is improving Why do people die of sepsis?
4 INDIVIDUALS VERSUS POPULATION
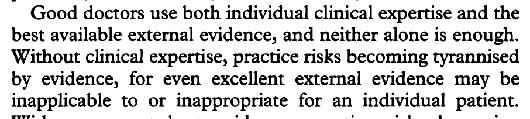
5 INDIVIDUALS VERSUS POPULATION Patients do NOT necessarily follow the rule book MUST tailor therapy to the individual Guidelines should NOT be used as rigid protocols/rules of stone Clinical expertise is VITAL


6 INDIVIDUALS VERSUS POPULATION Patients do NOT necessarily follow the rule book MUST tailor therapy to the individual Guidelines should NOT be used as rigid protocols/rules of stone Clinical expertise is VITAL.. not my words, but David Sackett s
7
8
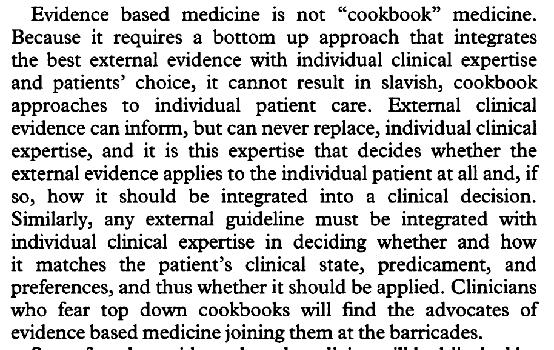
9 QUALITY - OR LACK - OF EVIDENC


10 QUALITY - OR LACK - OF EVIDENC Overall evidence base for sepsis is - sadly - rather weak Only a few awarded high quality (but generally do nots rather than do s )
11 DOGMA SHOULDN T RULE Need decent evidence to confirm need to change For example, Rivers showed EGDT was beneficial in but why?

12 DOGMA SHOULDN T RULE Need decent evidence to confirm need to change For example, Rivers showed EGDT was beneficial in but why?
13 DOGMA SHOULDN T RULE Need decent evidence to confirm need to change For example, Rivers showed EGDT was beneficial in but why?
14 DOGMA SHOULDN T RULE Need decent evidence to confirm need to change For example, Rivers showed EGDT was beneficial in but why?
15 DOGMA SHOULDN T RULE Need decent evidence to confirm need to change For example, Rivers showed EGDT was beneficial in but why?
16
17



18
19 TAKE-HOME MESSAGE Identify patient early Treat promptly and appropriately.. but the specific Rivers protocol doesn t seem to offer any overall added benefit
20 LOWEST COMMON DENOMINATOR? good performing hospitals not-so-good performing hospitals Standardised mortality ratio
21 LOWEST COMMON DENOMINATOR? good performing hospitals Standardised mortality ratio? rigid protocol application not-so-good performing hospitals
22 LOWEST COMMON DENOMINATOR? good performing hospitals Standardised mortality ratio? rigid protocol application? rigid protocol application not-so-good performing hospitals


23 LOWEST COMMON DENOMINATOR? good performing hospitals Standardised mortality ratio? rigid protocol application? rigid protocol application not-so-good performing hospitals
24 BUT. Guidelines are often taken too literally by: clinical zealots institutions governments


25 BUT. Guidelines are often taken too literally by: clinical zealots institutions governments.. with financial penalties or name-and-shame for non-compliance

26 TAKE-HOME MESSAGE Use guidelines/protocols as an aide memoire.. but not rules of stone Don t be afraid to deviate.. but be able to justify why
27 DISCUSSION POINTS.. Guidelines should be slavishly followed One size fits all Every hour of antibiotic delay kills How long should a course of antibiotics last? Sepsis mortality is improving Why do people die of sepsis?

28 THE INTERVENTION.. OR TARGETED ENDPOIN.. MUST BE RATIONAL FOR EVERYONE
29

30
31
32


33 S O W H Y TA R G E T A P O P U L AT I O N, AND NOT AN INDIVIDUAL!!!!!
34
35
36
37
38 TAKE-HOME MESSAGE
39 TAKE-HOME MESSAGE Titrate to the individual e.g. what BP suits them? MAP or 75-80?
40 TAKE-HOME MESSAGE Titrate to the individual e.g. what BP suits them? MAP or 75-80? Titrate to a goal if a patient needs fluid (if hypovolaemia -> hypoperfusion), give fluid if not hypovolaemic and hypoperfused, don t give fluid
, give fluid if not hypovolaemic and hypoperfused, don t give fluid Avoid")
41 TAKE-HOME MESSAGE Titrate to the individual e.g. what BP suits them? MAP or 75-80? Titrate to a goal if a patient needs fluid (if hypovolaemia -> hypoperfusion), give fluid if not hypovolaemic and hypoperfused, don t give fluid Avoid excess - too much fluid, too much oxygen, too much catecholamine
42 DISCUSSION POINTS.. Guidelines should be slavishly followed One size fits all Every hour of antibiotic delay kills How long should a course of antibiotics last? Sepsis mortality is improving Why do people die of sepsis?
43 INTERESTING FACTS - 1
44 INTERESTING FACTS - 1 Multiple papers - including EVERY prospective study I m aware of do NOT show a correlation between a short-term delay in administering antibiotics and mortality
45 INTERESTING FACTS - 2
46 INTERESTING FACTS - 2 Studies claiming every hour counts are all based on retrospective analyses of databases collected for other reasons (usually administrative), but lacking vital data e.g. antibiotic sensitivities
47 INTERESTING FACTS - 2 Studies claiming every hour counts are all based on retrospective analyses of databases collected for other reasons (usually administrative), but lacking vital data e.g. antibiotic sensitivities.. and use complex adjustments to find a mortality difference
48 INTERESTING FACTS - 2 Studies claiming every hour counts are all based on retrospective analyses of databases collected for other reasons (usually administrative), but lacking vital data e.g. antibiotic sensitivities.. and use complex adjustments to find a mortality difference.. and often incorporate very delayed treatment (>6h) into the analysis
49 INTERESTING FACTS - 2 Studies claiming every hour counts are all based on retrospective analyses of databases collected for other reasons (usually administrative), but lacking vital data e.g. antibiotic sensitivities.. and use complex adjustments to find a mortality difference.. and often incorporate very delayed treatment (>6h) into the analysis.. and often lack biological plausibility
50 INTERESTING FACTS - 2 Studies claiming every hour counts are all based on retrospective analyses of databases collected for other reasons (usually administrative), but lacking vital data e.g. antibiotic sensitivities.. and use complex adjustments to find a mortality difference.. and often incorporate very delayed treatment (>6h) into the analysis.. and often lack biological plausibility.. and cannot explain why there was a delay in treatment in some
51 Survival time following hypotension (hours)
52 Survival 7.6% decrease in survival per hour of delay time following hypotension (hours)
53 Survival 7.6% decrease in survival per hour of delay time following hypotension (hours)
54 Survival time following hypotension (hours)
55 Survival time following hypotension (hours)
56 Survival time following hypotension (hours)
57 Survival time following hypotension (hours)

58 Survival time following hypotension (hours)
59 Survival time following hypotension (hours)
60 Survival n=2154 time following hypotension (hours)
61 Survival n=2154 time following hypotension (hours)

62 Survival n=558 n=2154 time following hypotension (hours)
63
64

65
66
67 ED Ward ICU Mortality (%) Time to antibiotic (hr) >6
68 ED Ward ICU Mortality (%) Time to antibiotic (hr) >6
69 ED Ward ICU Mortality (%) Time to antibiotic (hr) >6
70 ED Ward ICU Mortality (%) Time to antibiotic (hr) >6
71 ED Ward ICU Mortality (%) Time to antibiotic (hr) >6
72 ED Ward ICU Mortality (%) Time to antibiotic (hr) >6
73
74 1373 ICU patients between coded as septic/septic shock
75 1373 ICU patients between coded as septic/septic shock
76 1373 ICU patients between coded as septic/septic shock

77 1373 ICU patients between coded as septic/septic shock
78
79
80
81
82
83
84
85
86
87
88
89
90 and no data on antibiotic sensitivities, adequacy of dosing, source control, etc..
91
 had septic")
92 .. yet 45% of patients (early and late treated) had septic shock!!
93
94
95 82.5% of pts 2% of pts
96 23.6% 22.6% 82.5% of pts 2% of pts
97 82.5% of pts 15.5% of pts 2% of pts
98 82.5% of pts 15.5% of pts 2% of pts
99 82.5% of pts 15.5% of pts 2% of pts

100 82.5% of pts 15.5% of pts 2% of pts
101 PROSPECTIVE STUDIES SHOW NO DIFFERENC
102 PROSPECTIVE STUDIES SHOW NO DIFFERENC Often designed to specifically look at impact of antibiotics on outcomes None show an each-hour-delay-kills signal Puskarich, CCM 2011 septic shock (ED) Hranjec, Lancet Infect Dis 2012 sepsis/septic shock (ICU) Kaasch, Infection 2013 S aureus bacteraemia (Ward/ICU) Bloos, Crit Care 2014 sepsis/septic shock (ICU) De Groot, Crit Care 2015 ED sepsis/septic shock (ED) Fitzpatrick, Clin Microbiol Infect 2016 Gm -tive bacteraemia (Ward) Alan, Lancet Respir Dis 2018 sepsis (pre-hospital ED)
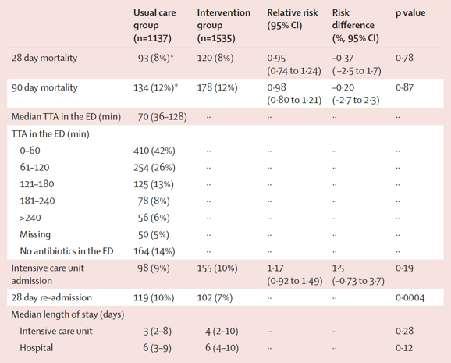
103 prospective observational study in 3 Dutch EDs hospitalized ED patients requiring iv antibiotics stratified by illness severity (low, intermediate, high) time to antibiotics <1 hour vs 1-3 hours v >3 hours 1168 patients enrolled - overall mortality 10% 85% received antibiotics within 3 hours, 95% within 6 hours
 antibiotics associated with more surviving days outside hospital (HR 1.46 (95%CI 1.")
104 No association between time to a/b and surviving days outside hospital or mortality In low illness severity group, delayed (>3h) antibiotics associated with more surviving days outside hospital (HR 1.46 (95%CI )
105
106 2672 patients randomised to receive pre-hospital antibiotics (ceftriaxone 2g) from paramedics on suspicion of sepsis OR start antibiotics in ED Mean 96 minute difference in time to administration of antibiotics
107
108
109
110

111
112 TAKE-HOME MESSAGE

113 TAKE-HOME MESSAGE Every second doesn t count.. but reasonable/rational to treat sepsis and septic shock promptly Rather than simply throwing antibiotics at the patient, apply some thought, seek advice, and think source control
114 DISCUSSION POINTS.. Guidelines should be slavishly followed One size fits all Every hour of antibiotic delay kills How long should a course of antibiotics last? Sepsis mortality is improving Why do people die of sepsis?
115
116
117

118
119
120
121

122
123
124 6 month audit in University hospital medical-surgical ICU
125 6 month audit in University hospital medical-surgical ICU 113 bacteraemia episodes in 87 patients
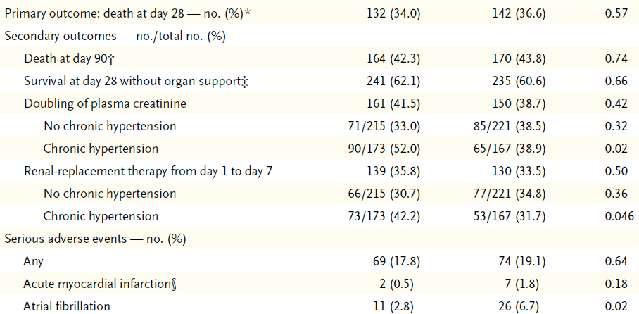
126 6 month audit in University hospital medical-surgical ICU 113 bacteraemia episodes in 87 patients Short-course monotherapy (4-5 days) used in 65.7%
127 6 month audit in University hospital medical-surgical ICU 113 bacteraemia episodes in 87 patients Short-course monotherapy (4-5 days) used in 65.7% Low rates of bacteraemia breakthrough/relapse
128 6 month audit in University hospital medical-surgical ICU 113 bacteraemia episodes in 87 patients Short-course monotherapy (4-5 days) used in 65.7% Low rates of bacteraemia breakthrough/relapse Very low incidence of antimicrobial resistance or fungaemia
129 6 month audit in University hospital medical-surgical ICU 113 bacteraemia episodes in 87 patients Short-course monotherapy (4-5 days) used in 65.7% Low rates of bacteraemia breakthrough/relapse Very low incidence of antimicrobial resistance or fungaemia Less ICU-acquired MRSA, MDR Gram -tives, VRE and fluconazole-resistant candidaemia c/f similar audit in 2000
130
131
132
133 fluconazole-resistant
134 fluconazole-resistant methicillin -resistant
135 fluconazole-resistant methicillin -resistant VRE
136 fluconazole-resistant methicillin -resistant VRE MDR
137 fluconazole-resistant methicillin -resistant VRE MDR no fluconazole-resistance
138 fluconazole-resistant methicillin -resistant VRE MDR 1 VRE no fluconazole-resistance
139 fluconazole-resistant methicillin -resistant VRE MDR no MRSA 1 VRE no fluconazole-resistance

140 fluconazole-resistant methicillin -resistant VRE no MRSA 1 VRE no MDR MDR no fluconazole-resistance
141
142
143 4 vs 8 days
144 DISCUSSION POINTS.. Guidelines should be slavishly followed One size fits all Every hour of antibiotic delay kills How long should a course of antibiotics last? Sepsis mortality is improving Why do people die of sepsis?
145
146

147
148
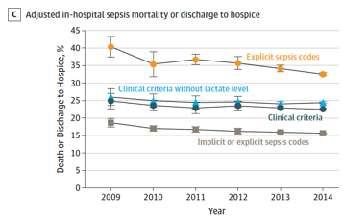
149 781, ,270
150 781, , , ,124
151 781, , , ,124


152 781,725??? under-reported 118,676??? over-reported 300, ,124
153
154





155
156

157
158 DISCUSSION POINTS.. Guidelines should be slavishly followed One size fits all Every hour of antibiotic delay kills How long should a course of antibiotics last? Sepsis mortality is improving Why do people die of sepsis?
159
160



161
162 MAINTAINING A SENSE OF PROPORTION
163 MAINTAINING A SENSE OF PROPORTION 34 million antibiotic prescriptions by English GPs in
164 MAINTAINING A SENSE OF PROPORTION 34 million antibiotic prescriptions by English GPs in million hospital patient episodes with a sepsis/infection code in England p.a.
165 MAINTAINING A SENSE OF PROPORTION 34 million antibiotic prescriptions by English GPs in million hospital patient episodes with a sepsis/infection code in England p.a... with 32,300 in-hospital deaths = 2.5% mortality rate

166 MAINTAINING A SENSE OF PROPORTION 34 million antibiotic prescriptions by English GPs in million hospital patient episodes with a sepsis/infection code in England p.a... with 32,300 in-hospital deaths = 2.5% mortality rate BUT only 11,000 cases of sepsis had an ICU admission
167 DO ALL SEPTIC PATIENTS WARRANT LIFE-PROLONGING TREATMENT???

168 DO ALL SEPTIC PATIENTS WARRANT LIFE-PROLONGING TREATMENT??? Pneumonia is the old man s friend - Sir William Osler Patients may be allowed to die from sepsis due to the severity of their underlying comorbidity - terminal cancer, severe stroke, end-stage chronic organ failure, severe dementia
169 N SUSPICIONOF SEPSIS HOSPITALADMISSIONS IN ENGLAND Age
170 SUSPICIONOF SEPSIS HOSPITALADMISSIONS IN ENGLAND N Age SUSPICIONOF SEPSIS MORTALITY Mortality (%) Age 90+
171 SUSPICIONOF SEPSIS HOSPITALADMISSIONS IN ENGLAND N Age SUSPICIONOF SEPSIS MORTALITY Mortality (%) 77.5% OF DEATHS Age 90+
172 SUSPICIONOF SEPSIS HOSPITALADMISSIONS IN ENGLAND N Age 20 8% OF DEATHS SUSPICIONOF SEPSIS MORTALITY Mortality (%) 77.5% OF DEATHS Age 90+
173
174
175 Dementia? Stroke? Other severe disability?
176 Dementia? Stroke? Other severe disability?
177 CONCLUSION
178 CONCLUSION Apply physiology to patient management
179 CONCLUSION Apply physiology to patient management Personalization not rigid protocolization
180 CONCLUSION Apply physiology to patient management Personalization not rigid protocolization Challenge dogma based on weak/contrived evidence
181 CONCLUSION Apply physiology to patient management Personalization not rigid protocolization Challenge dogma based on weak/contrived evidence Sepsis only constitutes a small proportion of infection but should be identified and acted upon promptly.. but with some thought applied


182 CONCLUSION Apply physiology to patient management Personalization not rigid protocolization Challenge dogma based on weak/contrived evidence Sepsis only constitutes a small proportion of infection but should be identified and acted upon promptly.. but with some thought applied
ESISTONO LE HCAP? Francesco Blasi. Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano
 ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
DOES TIMING OF ANTIBIOTICS IMPACT OUTCOME IN SEPSIS? Saravana Kumar MD HEAD,DEPT OF EM,DR MEHTA S HOSPITALS CHENNAI,INDIA
 DOES TIMING OF ANTIBIOTICS IMPACT OUTCOME IN SEPSIS? Saravana Kumar MD HEAD,DEPT OF EM,DR MEHTA S HOSPITALS CHENNAI,INDIA drsaravanakumar.ep@gmail.com JOINT SECRETARY RECOMMENDATIONS: INITIAL RESUSCITATION
DOES TIMING OF ANTIBIOTICS IMPACT OUTCOME IN SEPSIS? Saravana Kumar MD HEAD,DEPT OF EM,DR MEHTA S HOSPITALS CHENNAI,INDIA drsaravanakumar.ep@gmail.com JOINT SECRETARY RECOMMENDATIONS: INITIAL RESUSCITATION
Early Antibiotics for Sepsis and Septic Shock: A Gold Standard
 Early Antibiotics for Sepsis and Septic Shock: A Gold Standard Anand Kumar MD, FRCPC, FCCP, FCCM Professor of Medicine University of Manitoba Health Sciences Centre St. Boniface Hospital Winnipeg, Manitoba
Early Antibiotics for Sepsis and Septic Shock: A Gold Standard Anand Kumar MD, FRCPC, FCCP, FCCM Professor of Medicine University of Manitoba Health Sciences Centre St. Boniface Hospital Winnipeg, Manitoba
Sepsis. ...striking a balance. Dr Ron Daniels.
 Sepsis...striking a balance Dr Ron Daniels Fellow: NHS Improvement Faculty Chair: United Kingdom Sepsis Group, Sepsis Trust & UK SSC Sepsis as a Global Emergency Committee, Global Sepsis Alliance Midland
Sepsis...striking a balance Dr Ron Daniels Fellow: NHS Improvement Faculty Chair: United Kingdom Sepsis Group, Sepsis Trust & UK SSC Sepsis as a Global Emergency Committee, Global Sepsis Alliance Midland
Antimicrobial Resistance Update for Community Health Services
 Antimicrobial Resistance Update for Community Health Services Elizabeth Beech Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England October 2015 elizabeth.beech@nhs.net Superbugs
Antimicrobial Resistance Update for Community Health Services Elizabeth Beech Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England October 2015 elizabeth.beech@nhs.net Superbugs
Role of the general physician in the management of sepsis and antibiotic stewardship
 Role of the general physician in the management of sepsis and antibiotic stewardship Prof Martin Wiselka Dept of Infection and Tropical Medicine University Hospitals of Leicester Sepsis and antibiotic
Role of the general physician in the management of sepsis and antibiotic stewardship Prof Martin Wiselka Dept of Infection and Tropical Medicine University Hospitals of Leicester Sepsis and antibiotic
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Does Early and Appropriate Antibiotic Administration Improve Mortality in Emergency Department Patients with Severe Sepsis or Septic Shock?
 References and Literature Grading Does Early and Appropriate Antibiotic Administration Improve Mortality in Emergency Department Patients with Severe Sepsis or Septic Shock? (9/6/2015) 1. Dellinger, R.P.,
References and Literature Grading Does Early and Appropriate Antibiotic Administration Improve Mortality in Emergency Department Patients with Severe Sepsis or Septic Shock? (9/6/2015) 1. Dellinger, R.P.,
NUOVE IPOTESI e MODELLI di STEWARDSHIP
 Esperienze di successo di antimicrobial stewardship Bologna, 18 novembre 2014 NUOVE IPOTESI e MODELLI di STEWARDSHIP Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Interventions
Esperienze di successo di antimicrobial stewardship Bologna, 18 novembre 2014 NUOVE IPOTESI e MODELLI di STEWARDSHIP Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Interventions
Antibiotic treatment in the ICU 1. ICU Fellowship Training Radboudumc
 Antibiotic treatment in the ICU 1 ICU Fellowship Training Radboudumc Main issues Delayed identification of microorganisms Impact of critical illness on Pk/Pd High prevalence of antibiotic resistant strains
Antibiotic treatment in the ICU 1 ICU Fellowship Training Radboudumc Main issues Delayed identification of microorganisms Impact of critical illness on Pk/Pd High prevalence of antibiotic resistant strains
Why should we care about multi-resistant bacteria? Clinical impact and
 Why should we care about multi-resistant bacteria? Clinical impact and public health implications Prof. Stephan Harbarth Infection Control Program Geneva, Switzerland and Ebola (in 2014/2015) Increased
Why should we care about multi-resistant bacteria? Clinical impact and public health implications Prof. Stephan Harbarth Infection Control Program Geneva, Switzerland and Ebola (in 2014/2015) Increased
Guidance Notes on the Antimicrobial Companion Audit Tool for the Antimicrobial Prescribing Quality Indicators 2017/18
 Guidance tes on the Antimicrobial Companion Audit Tool for the Antimicrobial Prescribing Quality Indicators 2017/18 Summary of the indicators The 2017/18 hospital antimicrobial prescribing quality indicators
Guidance tes on the Antimicrobial Companion Audit Tool for the Antimicrobial Prescribing Quality Indicators 2017/18 Summary of the indicators The 2017/18 hospital antimicrobial prescribing quality indicators
Burden of disease of antibiotic resistance The example of MRSA. Eva Melander Clinical Microbiology, Lund University Hospital
 Burden of disease of antibiotic resistance The example of MRSA Eva Melander Clinical Microbiology, Lund University Hospital Discovery of antibiotics Enormous medical gains Significantly reduced morbidity
Burden of disease of antibiotic resistance The example of MRSA Eva Melander Clinical Microbiology, Lund University Hospital Discovery of antibiotics Enormous medical gains Significantly reduced morbidity
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases
 The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
8/17/2016 ABOUT US REDUCTION OF CLOSTRIDIUM DIFFICILE THROUGH THE USE OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM
 Mary Moore, MS CIC MT (ASCP) Infection Prevention Coordinator Great River Medical Center, West Burlington REDUCTION OF CLOSTRIDIUM DIFFICILE THROUGH THE USE OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM ABOUT
Mary Moore, MS CIC MT (ASCP) Infection Prevention Coordinator Great River Medical Center, West Burlington REDUCTION OF CLOSTRIDIUM DIFFICILE THROUGH THE USE OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM ABOUT
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship
 Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Active Bacterial Core Surveillance Site and Epidemiologic Classification, United States, 2005a. Copyright restrictions may apply.
 Impact of routine surgical ward and intensive care unit admission surveillance cultures on hospital-wide nosocomial methicillin-resistant Staphylococcus aureus infections in a university hospital: an interrupted
Impact of routine surgical ward and intensive care unit admission surveillance cultures on hospital-wide nosocomial methicillin-resistant Staphylococcus aureus infections in a university hospital: an interrupted
Antimicrobial therapy in critical care
 Antimicrobial therapy in critical care KARLEE JOHNSTON LEAD PHARMACIST DIVISION OF CRITICAL CARE CANBERRA HOSPITAL AND HEALTH SERVICE Outline 1. Let s talk about sepsis 2. PK/PD considerations 3. Selecting
Antimicrobial therapy in critical care KARLEE JOHNSTON LEAD PHARMACIST DIVISION OF CRITICAL CARE CANBERRA HOSPITAL AND HEALTH SERVICE Outline 1. Let s talk about sepsis 2. PK/PD considerations 3. Selecting
Collecting and Interpreting Stewardship Data: Breakout Session
 Collecting and Interpreting Stewardship Data: Breakout Session Michael S. Calderwood, MD, MPH Regional Hospital Epidemiologist, Dartmouth-Hitchcock Medical Center March 20, 2019 None Disclosures Outline
Collecting and Interpreting Stewardship Data: Breakout Session Michael S. Calderwood, MD, MPH Regional Hospital Epidemiologist, Dartmouth-Hitchcock Medical Center March 20, 2019 None Disclosures Outline
Welcome! 10/26/2015 1
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
The CARI Guidelines Caring for Australians with Renal Impairment. 8. Prophylactic antibiotics for insertion of peritoneal dialysis catheter
 8. Prophylactic antibiotics for insertion of peritoneal dialysis catheter Date written: February 2003 Final submission: May 2004 Guidelines (Include recommendations based on level I or II evidence) Antibiotic
8. Prophylactic antibiotics for insertion of peritoneal dialysis catheter Date written: February 2003 Final submission: May 2004 Guidelines (Include recommendations based on level I or II evidence) Antibiotic
Le infezioni di cute e tessuti molli
 Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
10 Golden rules of Antibiotic Stewardship in ICU. Jeroen Schouten, MD PhD intensivist, Nijmegen (Neth) Istanbul, Oct 6th 2017
 Istanbul, Oct 6th 2017") 10 Golden rules of Antibiotic Stewardship in ICU Jeroen Schouten, MD PhD intensivist, Nijmegen (Neth) Istanbul, Oct 6th 2017 10 golden rules of Antibiotic Stewardship in the ICU ID, Pharma & Micro advice
10 Golden rules of Antibiotic Stewardship in ICU Jeroen Schouten, MD PhD intensivist, Nijmegen (Neth) Istanbul, Oct 6th 2017 10 golden rules of Antibiotic Stewardship in the ICU ID, Pharma & Micro advice
MDR Acinetobacter baumannii. Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta
 MDR Acinetobacter baumannii Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta 1 The Armageddon recipe Transmissible organism with prolonged environmental
MDR Acinetobacter baumannii Has the post antibiotic era arrived? Dr. Michael A. Borg Infection Control Dept Mater Dei Hospital Malta 1 The Armageddon recipe Transmissible organism with prolonged environmental
Surveillance of AMR in PHE: a multidisciplinary,
 Surveillance of AMR in PHE: a multidisciplinary, integrated approach Professor Neil Woodford Antimicrobial Resistance & Healthcare Associated Infections (AMRHAI) Reference Unit Crown copyright International
Surveillance of AMR in PHE: a multidisciplinary, integrated approach Professor Neil Woodford Antimicrobial Resistance & Healthcare Associated Infections (AMRHAI) Reference Unit Crown copyright International
Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings
 Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings Jasmanda H. Wu, Ph.D., 1 David H. Howard, Ph.D., 2 John E. McGowan, Jr.,
Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings Jasmanda H. Wu, Ph.D., 1 David H. Howard, Ph.D., 2 John E. McGowan, Jr.,
Jump Starting Antimicrobial Stewardship
 Jump Starting Antimicrobial Stewardship Amanda C. Hansen, PharmD Pharmacy Operations Manager Carilion Roanoke Memorial Hospital Roanoke, Virginia March 16, 2011 Objectives Discuss guidelines for developing
Jump Starting Antimicrobial Stewardship Amanda C. Hansen, PharmD Pharmacy Operations Manager Carilion Roanoke Memorial Hospital Roanoke, Virginia March 16, 2011 Objectives Discuss guidelines for developing
The Core Elements of Antibiotic Stewardship for Nursing Homes
 The Core Elements of Antibiotic Stewardship for Nursing Homes APPENDIX B: Measures of Antibiotic Prescribing, Use and Outcomes National Center for Emerging and Zoonotic Infectious Diseases Division of
The Core Elements of Antibiotic Stewardship for Nursing Homes APPENDIX B: Measures of Antibiotic Prescribing, Use and Outcomes National Center for Emerging and Zoonotic Infectious Diseases Division of
UPDATE ON ANTIMICROBIAL STEWARDSHIP REGULATIONS AND IMPLEMENTATION OF AN AMS PROGRAM
 UPDATE ON ANTIMICROBIAL STEWARDSHIP REGULATIONS AND IMPLEMENTATION OF AN AMS PROGRAM Diane Rhee, Pharm.D. Associate Professor of Pharmacy Practice Roseman University of Health Sciences Chair, Valley Health
UPDATE ON ANTIMICROBIAL STEWARDSHIP REGULATIONS AND IMPLEMENTATION OF AN AMS PROGRAM Diane Rhee, Pharm.D. Associate Professor of Pharmacy Practice Roseman University of Health Sciences Chair, Valley Health
Bacterial infections complicating cirrhosis
 PHC www.aphc.info Bacterial infections complicating cirrhosis P. Angeli, Dept. of Medicine, Unit of Internal Medicine and Hepatology (), University of Padova (Italy) pangeli@unipd.it Agenda Epidemiology
PHC www.aphc.info Bacterial infections complicating cirrhosis P. Angeli, Dept. of Medicine, Unit of Internal Medicine and Hepatology (), University of Padova (Italy) pangeli@unipd.it Agenda Epidemiology
Original Date: 02/2010 Purpose: To maximize antibiotic stewardship for intraabdominal infection in the Precedes: 4/2013
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Antibiotic Therapy: Intra-Abdominal Infections Clinical Practice Algorithm Original Date: 02/2010 Purpose: To maximize
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Antibiotic Therapy: Intra-Abdominal Infections Clinical Practice Algorithm Original Date: 02/2010 Purpose: To maximize
Screening programmes for Hospital Acquired Infections
 Screening programmes for Hospital Acquired Infections European Diagnostic Manufacturers Association In Vitro Diagnostics Making a real difference in health & life quality June 2007 HAI Facts Every year,
Screening programmes for Hospital Acquired Infections European Diagnostic Manufacturers Association In Vitro Diagnostics Making a real difference in health & life quality June 2007 HAI Facts Every year,
POTENTIAL STRUCTURE INDICATORS FOR EVALUATING ANTIMICROBIAL STEWARDSHIP PROGRAMMES IN EUROPEAN HOSPITALS
 POTENTIAL STRUCTURE INDICATORS FOR EVALUATING ANTIMICROBIAL STEWARDSHIP PROGRAMMES IN EUROPEAN HOSPITALS Dirk VOGELAERS Department of General Internal Medicine, Infectious Diseases and Psychosomatic Medicine
POTENTIAL STRUCTURE INDICATORS FOR EVALUATING ANTIMICROBIAL STEWARDSHIP PROGRAMMES IN EUROPEAN HOSPITALS Dirk VOGELAERS Department of General Internal Medicine, Infectious Diseases and Psychosomatic Medicine
Why we perform susceptibility testing
 22 nd June 2015 Why we perform susceptibility testing Robin A Howe Antimicrobial use in Primary Care Why do we perform AST? Clinical Clinical Prediction Prediction of of Efficacy Efficacy Why do we perform
22 nd June 2015 Why we perform susceptibility testing Robin A Howe Antimicrobial use in Primary Care Why do we perform AST? Clinical Clinical Prediction Prediction of of Efficacy Efficacy Why do we perform
Optimize Durations of Antimicrobial Therapy
 Optimize Durations of Antimicrobial Therapy Evidence & Application Jill Cowper, Pharm.D. Division Infectious Diseases Pharmacist Parallon Supply Chain Solutions Richmond, VA P: 607 221 5101 jill.butterfield@parallon.com
Optimize Durations of Antimicrobial Therapy Evidence & Application Jill Cowper, Pharm.D. Division Infectious Diseases Pharmacist Parallon Supply Chain Solutions Richmond, VA P: 607 221 5101 jill.butterfield@parallon.com
POINT PREVALENCE SURVEY A tool for antibiotic stewardship in hospitals. Koen Magerman Working group Hospital Medicine
 POINT PREVALENCE SURVEY A tool for antibiotic stewardship in hospitals Koen Magerman Working group Hospital Medicine Background Strategic plan By means of a point prevalence survey and internal audits
POINT PREVALENCE SURVEY A tool for antibiotic stewardship in hospitals Koen Magerman Working group Hospital Medicine Background Strategic plan By means of a point prevalence survey and internal audits
Antibacterials. Recent data on linezolid and daptomycin
 Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Hot Topics in Antimicrobial Stewardship. Meghan Brett, MD Medical Director, Antimicrobial Stewardship University of New Mexico Hospital
 Hot Topics in Antimicrobial Stewardship Meghan Brett, MD Medical Director, Antimicrobial Stewardship University of New Mexico Hospital Antimicrobial Stewardship Goals Primary Goal Optimize clinical outcomes
Hot Topics in Antimicrobial Stewardship Meghan Brett, MD Medical Director, Antimicrobial Stewardship University of New Mexico Hospital Antimicrobial Stewardship Goals Primary Goal Optimize clinical outcomes
Study Protocol. Funding: German Center for Infection Research (TTU-HAARBI, Research Clinical Unit)
") Effectiveness of antibiotic stewardship interventions in reducing the rate of colonization and infections due to antibiotic resistant bacteria and Clostridium difficile in hospital patients a systematic
Effectiveness of antibiotic stewardship interventions in reducing the rate of colonization and infections due to antibiotic resistant bacteria and Clostridium difficile in hospital patients a systematic
Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources
 Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources Andrew Hunter, PharmD, BCPS Infectious Diseases Clinical Pharmacy Specialist Michael E. DeBakey VA Medical Center Andrew.hunter@va.gov
Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources Andrew Hunter, PharmD, BCPS Infectious Diseases Clinical Pharmacy Specialist Michael E. DeBakey VA Medical Center Andrew.hunter@va.gov
Measurement of Antimicrobial Drug Use. Elizabeth Dodds Ashley, PharmD, MHS, FCCP, BCPS DASON Liaison Pharmacist
 Measurement of Antimicrobial Drug Use Elizabeth Dodds Ashley, PharmD, MHS, FCCP, BCPS DASON Liaison Pharmacist Defined Daily Dose Target Audience: Administrators and Epidemiologists Standardized definition
Measurement of Antimicrobial Drug Use Elizabeth Dodds Ashley, PharmD, MHS, FCCP, BCPS DASON Liaison Pharmacist Defined Daily Dose Target Audience: Administrators and Epidemiologists Standardized definition
Surgical prophylaxis for Gram +ve & Gram ve infection
 Surgical prophylaxis for Gram +ve & Gram ve infection Professor Mark Wilcox Clinical l Director of Microbiology & Pathology Leeds Teaching Hospitals & University of Leeds, UK Heath Protection Agency Surveillance
Surgical prophylaxis for Gram +ve & Gram ve infection Professor Mark Wilcox Clinical l Director of Microbiology & Pathology Leeds Teaching Hospitals & University of Leeds, UK Heath Protection Agency Surveillance
Promoting Appropriate Antimicrobial Prescribing in Secondary Care
 Promoting Appropriate Antimicrobial Prescribing in Secondary Care Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2015 Introduction Background ESPAUR
Promoting Appropriate Antimicrobial Prescribing in Secondary Care Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2015 Introduction Background ESPAUR
Appropriate Antibiotic Administration in Critically Ill Patients with Pneumonia
 Research Paper Appropriate Antibiotic Administration in Critically Ill Patients with Pneumonia R. A. KHAN, M. M. BAKRY 1 AND F. ISLAHUDIN 1 * Hospital SgBuloh, Jalan Hospital, 47000 SgBuloh, Selangor,
Research Paper Appropriate Antibiotic Administration in Critically Ill Patients with Pneumonia R. A. KHAN, M. M. BAKRY 1 AND F. ISLAHUDIN 1 * Hospital SgBuloh, Jalan Hospital, 47000 SgBuloh, Selangor,
Core Elements of Antibiotic Stewardship for Nursing Homes
 Core Elements of Antibiotic Stewardship for Nursing Homes Nimalie D. Stone, MD, MS Medical Epidemiologist for LTC Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Antimicrobial
Core Elements of Antibiotic Stewardship for Nursing Homes Nimalie D. Stone, MD, MS Medical Epidemiologist for LTC Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Antimicrobial
Konsequenzen für Bevölkerung und Gesundheitssysteme. Stephan Harbarth Infection Control Program
 Konsequenzen für Bevölkerung und Gesundheitssysteme Stephan Harbarth Infection Control Program University of Geneva Hospitals Outline Introduction What data sources are available? AMR-associated outcomes
Konsequenzen für Bevölkerung und Gesundheitssysteme Stephan Harbarth Infection Control Program University of Geneva Hospitals Outline Introduction What data sources are available? AMR-associated outcomes
Quality indicators and outcomes in the devolved nations Scotland
 Quality indicators and outcomes in the devolved nations Scotland Dr Jacqueline Sneddon, MRPharmS Project Lead, Scottish Antimicrobial Prescribing Group Federation of Infection Societies Conference Birmingham,
Quality indicators and outcomes in the devolved nations Scotland Dr Jacqueline Sneddon, MRPharmS Project Lead, Scottish Antimicrobial Prescribing Group Federation of Infection Societies Conference Birmingham,
Challenges and opportunities for rapidly advancing reporting and improving inpatient antibiotic use in the U.S.
 Challenges and opportunities for rapidly advancing reporting and improving inpatient antibiotic use in the U.S. Overview of benchmarking Antibiotic Use Scott Fridkin, MD, Senior Advisor for Antimicrobial
Challenges and opportunities for rapidly advancing reporting and improving inpatient antibiotic use in the U.S. Overview of benchmarking Antibiotic Use Scott Fridkin, MD, Senior Advisor for Antimicrobial
Epidemiology of early-onset bloodstream infection and implications for treatment
 Epidemiology of early-onset bloodstream infection and implications for treatment Richard S. Johannes, MD, MS Marlborough, Massachusetts Health care-associated infections: For over 35 years, infections
Epidemiology of early-onset bloodstream infection and implications for treatment Richard S. Johannes, MD, MS Marlborough, Massachusetts Health care-associated infections: For over 35 years, infections
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Clinical Guideline. District Infectious Diseases Management. Go to Guideline. District Infectious Diseases Management CG 18_24
 Clinical Guideline District Infectious Diseases Management Sites where Clinical Guideline applies All facilities This Clinical Guideline applies to: 1. Adults Yes 2. Children up to 16 years Yes 3. Neonates
Clinical Guideline District Infectious Diseases Management Sites where Clinical Guideline applies All facilities This Clinical Guideline applies to: 1. Adults Yes 2. Children up to 16 years Yes 3. Neonates
Multi-drug resistant microorganisms
 Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
Hospital Acquired Infections in the Era of Antimicrobial Resistance
 Hospital Acquired Infections in the Era of Antimicrobial Resistance Datuk Dr Christopher KC Lee Infectious Diseases Unit Department of Medicine Sungai Buloh Hospital Patient Story 23 Year old female admitted
Hospital Acquired Infections in the Era of Antimicrobial Resistance Datuk Dr Christopher KC Lee Infectious Diseases Unit Department of Medicine Sungai Buloh Hospital Patient Story 23 Year old female admitted
Mono- versus Bitherapy for Management of HAP/VAP in the ICU
 Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Reducing the Burden of Severe Sepsis and Infections in Indian ICUs
 Reducing the Burden of Severe Sepsis and Infections in Indian ICUs J.V. Divatia Professor & Head Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai India Infections in the ICU
Reducing the Burden of Severe Sepsis and Infections in Indian ICUs J.V. Divatia Professor & Head Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai India Infections in the ICU
Adequacy of Early Empiric Antibiotic Treatment and Survival in Severe Sepsis: Experience from the MONARCS Trial
 BRIEF REPORT Adequacy of Early Empiric Antibiotic Treatment and Survival in Severe Sepsis: Experience from the MONARCS Trial Rodger D. MacArthur, 1 Mark Miller, 2 Timothy Albertson, 3 Edward Panacek, 3
BRIEF REPORT Adequacy of Early Empiric Antibiotic Treatment and Survival in Severe Sepsis: Experience from the MONARCS Trial Rodger D. MacArthur, 1 Mark Miller, 2 Timothy Albertson, 3 Edward Panacek, 3
La sepsi Il ruolo dell antibiotico terapia
 Congresso Nazionale AcEMC Fermo 11-12 Maggio 2017 La sepsi Il ruolo dell antibiotico terapia Michele Bartoletti Infectious Disease Unit - Sant Orsola Hospital, Bologna, Italy Disclosures: none Epidemiology
Congresso Nazionale AcEMC Fermo 11-12 Maggio 2017 La sepsi Il ruolo dell antibiotico terapia Michele Bartoletti Infectious Disease Unit - Sant Orsola Hospital, Bologna, Italy Disclosures: none Epidemiology
ANTIMICROBIALS PRESCRIBING STRATEGY
 Directorate of Operations Clinical Support Services Diagnostic Services Pharmacy ANTIMICROBIALS PRESCRIBING STRATEGY Reference: DCM021 Version: 2.0 This version issued: 25/04/16 Result of last review:
Directorate of Operations Clinical Support Services Diagnostic Services Pharmacy ANTIMICROBIALS PRESCRIBING STRATEGY Reference: DCM021 Version: 2.0 This version issued: 25/04/16 Result of last review:
Ithas been estimated that one
 Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department David F. Gaieski, MD; Jesse M. Pines,
Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department David F. Gaieski, MD; Jesse M. Pines,
Inappropriate Use of Antibiotics and Clostridium difficile Infection. Jocelyn Srigley, MD, FRCPC November 1, 2012
 Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
3/1/2016. Antibiotics --When Less is More. Most Urgent Threats. Serious Threats
 Antibiotics --When Less is More Ralph Gonzales, MD, MSPH Associate Dean, Clinical Innovation School of Medicine VP, Clinical Innovation, UCSF Health Most Urgent Threats Serious Threats Multidrug-Resistant
Antibiotics --When Less is More Ralph Gonzales, MD, MSPH Associate Dean, Clinical Innovation School of Medicine VP, Clinical Innovation, UCSF Health Most Urgent Threats Serious Threats Multidrug-Resistant
Antimicrobial stewardship in managing septic patients
 Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Fighting MDR Pathogens in the ICU
 Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Antibiotic Stewardship in the Hospital Setting
 Antibiotic Stewardship in the Hospital Setting G. Evans, MD FRCPC Medical Director, Infection Prevention & Control Kingston General Hospital & Hotel Dieu Hospital EOPIC September 26, 2012 Stewardship stew-ard-ship
Antibiotic Stewardship in the Hospital Setting G. Evans, MD FRCPC Medical Director, Infection Prevention & Control Kingston General Hospital & Hotel Dieu Hospital EOPIC September 26, 2012 Stewardship stew-ard-ship
Susan Becker DNP, RN, CNS, CCRN, CCNS Marymount University, Arlington, VA
 Susan Becker DNP, RN, CNS, CCRN, CCNS Marymount University, Arlington, VA Disclosures Study and presentation has no commercial bias or interests No financial relationship with a commercial interest, products,
Susan Becker DNP, RN, CNS, CCRN, CCNS Marymount University, Arlington, VA Disclosures Study and presentation has no commercial bias or interests No financial relationship with a commercial interest, products,
NIH Public Access Author Manuscript Crit Care Med. Author manuscript; available in PMC 2012 September 1.
 NIH Public Access Author Manuscript Published in final edited form as: Crit Care Med. 2011 September ; 39(9): 2066 2071. doi:10.1097/ccm.0b013e31821e87ab. Association Between Timing of Antibiotic Administration
NIH Public Access Author Manuscript Published in final edited form as: Crit Care Med. 2011 September ; 39(9): 2066 2071. doi:10.1097/ccm.0b013e31821e87ab. Association Between Timing of Antibiotic Administration
Gram negative bacteraemia
 Gram negative bacteraemia David Enoch Consultant Medical Microbiologist PHE Cambridge Cambridge University Hospitals NHS FT Overview Gram negative bacteraemia Changing epidemiology in England Epidemiology
Gram negative bacteraemia David Enoch Consultant Medical Microbiologist PHE Cambridge Cambridge University Hospitals NHS FT Overview Gram negative bacteraemia Changing epidemiology in England Epidemiology
ANTIBIOTIC STEWARDSHIP
 ANTIBIOTIC STEWARDSHIP Adrie Bekker - Kenya 2018 Department of Pediatric and Child Health, Division of Neonatology University of Stellenbosch, Tygerberg Hospital DEFINITION OF ANTIMICROBIAL STEWARDSHIP
ANTIBIOTIC STEWARDSHIP Adrie Bekker - Kenya 2018 Department of Pediatric and Child Health, Division of Neonatology University of Stellenbosch, Tygerberg Hospital DEFINITION OF ANTIMICROBIAL STEWARDSHIP
Summary of unmet need guidance and statistical challenges
 Summary of unmet need guidance and statistical challenges Daniel B. Rubin, PhD Statistical Reviewer Division of Biometrics IV Office of Biostatistics, CDER, FDA 1 Disclaimer This presentation reflects
Summary of unmet need guidance and statistical challenges Daniel B. Rubin, PhD Statistical Reviewer Division of Biometrics IV Office of Biostatistics, CDER, FDA 1 Disclaimer This presentation reflects
Taiwan Crit. Care Med.2009;10: %
 2008 30% 2008 2008 2004 813 386 07-346-8339 E-mail srwann@vghks.gov.tw 66 30% 2008 1 2008 2008 Intensive Care Med (2008)34:17-60 67 2 3 C activated protein C 4 5,6 65% JAMA 1995;273(2):117-23 Circulation,
2008 30% 2008 2008 2004 813 386 07-346-8339 E-mail srwann@vghks.gov.tw 66 30% 2008 1 2008 2008 Intensive Care Med (2008)34:17-60 67 2 3 C activated protein C 4 5,6 65% JAMA 1995;273(2):117-23 Circulation,
11/22/2016. Antimicrobial Stewardship Update Disclosures. Outline. No conflicts of interest to disclose
 Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
EVIDENCE BASED MEDICINE: ANTIBIOTIC RESISTANCE IN THE ELDERLY CHETHANA KAMATH GERIATRIC MEDICINE WEEK
 EVIDENCE BASED MEDICINE: ANTIBIOTIC RESISTANCE IN THE ELDERLY CHETHANA KAMATH GERIATRIC MEDICINE WEEK EPIDEMIOLOGY AND BACKGROUND Every year, more than 2 million people in the United States acquire antibiotic-resistant
EVIDENCE BASED MEDICINE: ANTIBIOTIC RESISTANCE IN THE ELDERLY CHETHANA KAMATH GERIATRIC MEDICINE WEEK EPIDEMIOLOGY AND BACKGROUND Every year, more than 2 million people in the United States acquire antibiotic-resistant
Antimicrobial Stewardship Advisory Committee Meeting
 Antimicrobial Stewardship Advisory Committee Meeting August 25, 2016 3:00 PM-4:30 PM Washington State Dept of Health Room A42 1610 NE 150th St Shoreline, WA 98155 Call in: (571) 317-3116 Access Code: 211-449-029
Antimicrobial Stewardship Advisory Committee Meeting August 25, 2016 3:00 PM-4:30 PM Washington State Dept of Health Room A42 1610 NE 150th St Shoreline, WA 98155 Call in: (571) 317-3116 Access Code: 211-449-029
A Point Prevalence Survey of Antibiotic Prescriptions and Infection in Sanandaj Hospitals, Prospects for Antibiotic Stewardship
 A Point Prevalence Survey of Antibiotic Prescriptions and Infection in Sanandaj Hospitals, Prospects for Antibiotic Stewardship Jafar Soltani* Ann Versporten**, Behzad Mohsenpour*, Herman Goossen**, Soheila
A Point Prevalence Survey of Antibiotic Prescriptions and Infection in Sanandaj Hospitals, Prospects for Antibiotic Stewardship Jafar Soltani* Ann Versporten**, Behzad Mohsenpour*, Herman Goossen**, Soheila
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Antibiotic resistance: the rise of the superbugs
 Antibiotic resistance: the rise of the superbugs Allen Cheng Associate Professor of Infectious Diseases Epidemiology, Alfred Health; Monash University About me Specialist in infectious diseases Head, Infection
Antibiotic resistance: the rise of the superbugs Allen Cheng Associate Professor of Infectious Diseases Epidemiology, Alfred Health; Monash University About me Specialist in infectious diseases Head, Infection
Meropenem for all? Midge Asogan ICU Fellow (also ID AT)
") Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Nosocomial Infections: What Are the Unmet Needs
 Nosocomial Infections: What Are the Unmet Needs Jean Chastre, MD Service de Réanimation Médicale Hôpital Pitié-Salpêtrière, AP-HP, Université Pierre et Marie Curie, Paris 6, France www.reamedpitie.com
Nosocomial Infections: What Are the Unmet Needs Jean Chastre, MD Service de Réanimation Médicale Hôpital Pitié-Salpêtrière, AP-HP, Université Pierre et Marie Curie, Paris 6, France www.reamedpitie.com
Treatment of septic peritonitis
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
RESISTANCE, USE, INTERVENTIONS. Hugh Webb
 RESISTANCE, USE, INTERVENTIONS Hugh Webb EU Initiatives: EARSS and ESAC. Antimicrobial Use and Resistance The Relationship. Bias and confounding in published studies. Mathematical modelling of resistance
RESISTANCE, USE, INTERVENTIONS Hugh Webb EU Initiatives: EARSS and ESAC. Antimicrobial Use and Resistance The Relationship. Bias and confounding in published studies. Mathematical modelling of resistance
Antibiotic usage in nosocomial infections in hospitals. Dr. Birgit Ross Hospital Hygiene University Hospital Essen
 Antibiotic usage in nosocomial infections in hospitals Dr. Birgit Ross Hospital Hygiene University Hospital Essen Infection control in healthcare settings - Isolation - Hand Hygiene - Environmental Hygiene
Antibiotic usage in nosocomial infections in hospitals Dr. Birgit Ross Hospital Hygiene University Hospital Essen Infection control in healthcare settings - Isolation - Hand Hygiene - Environmental Hygiene
Development of Drugs for HAP-VAP. Robert Fromtling, MD
 Development of Drugs for HAP-VAP Robert Fromtling, MD Hospital-Acquired & Ventilator- Associated Pneumonia (HAP-VAP) The EMA 2015 roadmap recognizes the need for new antibiotics New drugs for HAP-VAP are
Development of Drugs for HAP-VAP Robert Fromtling, MD Hospital-Acquired & Ventilator- Associated Pneumonia (HAP-VAP) The EMA 2015 roadmap recognizes the need for new antibiotics New drugs for HAP-VAP are
Lindsay E. Nicolle University of Manitoba Winnipeg, CANADA
 Lindsay E. Nicolle University of Manitoba Winnipeg, CANADA Long Term Care Facilities: Spectrum low acuity assisted living mobile independent Not LTAC high acuity complete functional disability dialysis
Lindsay E. Nicolle University of Manitoba Winnipeg, CANADA Long Term Care Facilities: Spectrum low acuity assisted living mobile independent Not LTAC high acuity complete functional disability dialysis
Advances in Antimicrobial Stewardship (AMS) at University Hospital Southampton
 at University Hospital Southampton") Advances in Antimicrobial Stewardship (AMS) at University Hospital Southampton Dr Julian Sutton Consultant in Infectious Diseases & Medical Microbiology Federation of Infection Societies 1 st December,
Advances in Antimicrobial Stewardship (AMS) at University Hospital Southampton Dr Julian Sutton Consultant in Infectious Diseases & Medical Microbiology Federation of Infection Societies 1 st December,
Antimicrobial Cycling. Donald E Low University of Toronto
 Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Antimicrobial Resistance and Papua New Guinea WHY is it important? HOW has the problem arisen? WHAT can we do?
 Antimicrobial Resistance and Papua New Guinea WHY is it important? HOW has the problem arisen? WHAT can we do? John Ferguson, John Hunter Hospital, University of Newcastle, NSW, Australia Infectious Diseases
Antimicrobial Resistance and Papua New Guinea WHY is it important? HOW has the problem arisen? WHAT can we do? John Ferguson, John Hunter Hospital, University of Newcastle, NSW, Australia Infectious Diseases
M.L. Avent* 1,2, E.Waddell 1, K.Daveson 1 and K. Hajkowicz 1 1. Queensland Statewide Antimicrobial Stewardship 2. UQCCR, The University of Queensland
 @MinyonAvent #ruralhealthconf M.L. Avent* 1,2, E.Waddell 1, K.Daveson 1 and K. Hajkowicz 1 1. Queensland Statewide Antimicrobial Stewardship 2. UQCCR, The University of Queensland Queensland State- Wide
@MinyonAvent #ruralhealthconf M.L. Avent* 1,2, E.Waddell 1, K.Daveson 1 and K. Hajkowicz 1 1. Queensland Statewide Antimicrobial Stewardship 2. UQCCR, The University of Queensland Queensland State- Wide
Assessment of empirical antibiotic therapy in a tertiary-care hospital: An observational descriptive study
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 9 Ver. VI (September). 2016), PP 118-124 www.iosrjournals.org Assessment of empirical antibiotic
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 9 Ver. VI (September). 2016), PP 118-124 www.iosrjournals.org Assessment of empirical antibiotic
Impact of Antimicrobial Resistance on Human Health. Robert Cunney HSE HCAI/AMR Programme and Temple Street Children s University Hospital
 Impact of Antimicrobial Resistance on Human Health Robert Cunney HSE HCAI/AMR Programme and Temple Street Children s University Hospital AMR in Foodchain Conference, UCD, Dec 2014 Sir Patrick Dun s Hospital
Impact of Antimicrobial Resistance on Human Health Robert Cunney HSE HCAI/AMR Programme and Temple Street Children s University Hospital AMR in Foodchain Conference, UCD, Dec 2014 Sir Patrick Dun s Hospital
Antibiotic Guideline: Empirical Treatment of Bone and Joint Infection in Adults
 Antibiotic Guideline: Empirical Treatment of Bone and Joint Infection in Adults Document type: Prescribing guideline Version: 5.0 Author (name and designation) Samim Patel, Antimicrobial Lead Pharmacist
Antibiotic Guideline: Empirical Treatment of Bone and Joint Infection in Adults Document type: Prescribing guideline Version: 5.0 Author (name and designation) Samim Patel, Antimicrobial Lead Pharmacist
Health Informatics Centre, Division of Community Health Sciences, Dundee, UK
 REVIEW Appropriate vs. inappropriate antimicrobial therapy P. G. Davey and C. Marwick Health Informatics Centre, Division of Community Health Sciences, Dundee, UK ABSTRACT Inappropriate antimicrobial treatment
REVIEW Appropriate vs. inappropriate antimicrobial therapy P. G. Davey and C. Marwick Health Informatics Centre, Division of Community Health Sciences, Dundee, UK ABSTRACT Inappropriate antimicrobial treatment
MRSA in the United Kingdom status quo and future developments
 MRSA in the United Kingdom status quo and future developments Dietrich Mack Chair of Medical Microbiology and Infectious Diseases The School of Medicine - University of Wales Swansea P R I F Y S G O L
MRSA in the United Kingdom status quo and future developments Dietrich Mack Chair of Medical Microbiology and Infectious Diseases The School of Medicine - University of Wales Swansea P R I F Y S G O L
Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report. July December 2013 Second and Third Quarters 2014
 Antimicrobial Stewardship Report. July December 2013 Second and Third Quarters 2014") H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report July December 213 Second and Third Quarters
H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report July December 213 Second and Third Quarters
These recommendations were approved for use by the Pharmaceutical and Therapeutics Committee, RCWMCH on 1 February 2017.
 Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Antibiotic regimens for suspected hospital-acquired infection (HAI) outside the Paediatric Intensive Care Unit at Red Cross War Memorial Children s Hospital (RCWMCH) Lead author: Brian Eley Contributing
Antimicrobial Stewardship. October 2012
 Antimicrobial Stewardship October 2012 Rising Antimicrobial Resistance Methicillin resistant staphylococcus aureus (MRSA) Vancomycin resistant enterococci (VRE) MDR and extremely drug resistant (XDR TB)
Antimicrobial Stewardship October 2012 Rising Antimicrobial Resistance Methicillin resistant staphylococcus aureus (MRSA) Vancomycin resistant enterococci (VRE) MDR and extremely drug resistant (XDR TB)
Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities
 Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities Introduction As the problem of antibiotic resistance continues to worsen in all healthcare setting, we
Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities Introduction As the problem of antibiotic resistance continues to worsen in all healthcare setting, we