Wounds: The ID/Microbiology Perspective. Max Bloomfield ID/micro registrar CCDHB 2018
|
|
|
- David Daniels
- 5 years ago
- Views:
Transcription

1 Wounds: The ID/Microbiology Perspective Max Bloomfield ID/micro registrar CCDHB 2018
2 Contents The lab perspective Colonisation vs infection Sampling of wounds Common bugs and which antibiotics to use Biofilms Antibiotic resistance/stewardship Cases
3 A sample arrives in the lab...

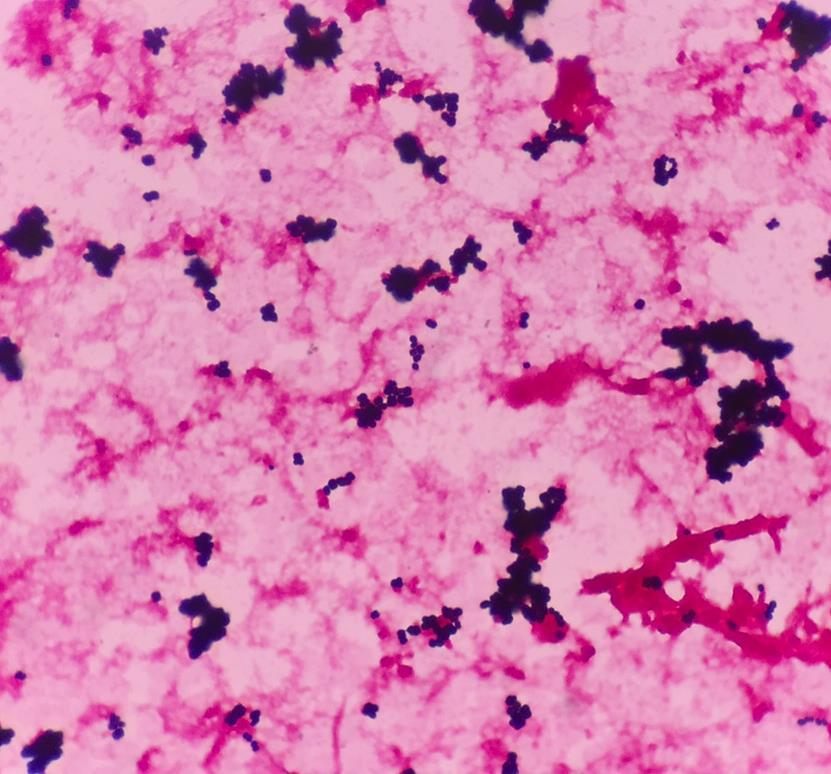
4 Step 1. Microscopy Part of sample is put onto a glass slide Gram stain (over 100 years old and still going strong)
5
6 Gram Stain Method 1. Crystal 2. Iodine 3. Alcohol wash 4. Safranin violet fixer decolourisation counterstain

7

8
9 Gram Stain First step in identification of bacteria Differentiates bacteria by cell wall properties Divided into Gram Positive and Gram Negative Shape of bacteria also identified: Round shaped cocci Rod shaped bacilli Can be performed rapidly Used to guide initial antibiotic choice

10 Gram stain Thick cell wall Thin cell wall Purple Pink Gram positive Gram negative

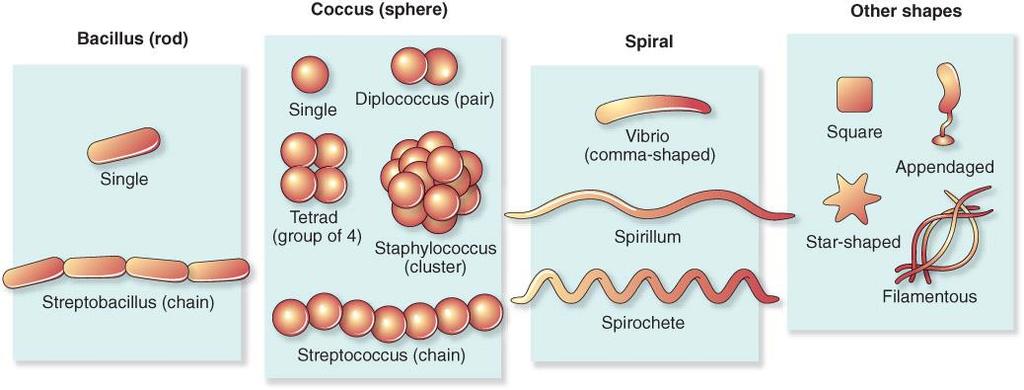

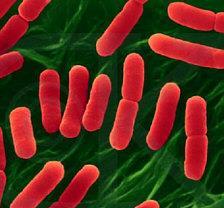
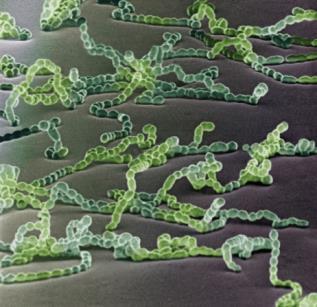
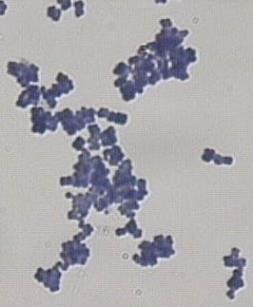

11 Cell wall shape
")
12 Step 1. Microscopy Gram stain (over 100 years old and still going strong) Microscopy can give initial clue as to bugs causing infection
13


14 Step 2. Culture Sample put onto different types of growth media Incubated to allow bugs to grow Usually takes 24-48h for growth Bugs that are grown are identified and reported
15
16 Step 3. Susceptibility testing Significant organisms selected for testing Tested against common antibiotics Grow the organism in the presence of different antibiotic discs Measure amount of growth around antibiotic disc to determine susceptibility/resistance Note: designed for planktonic bacteria, doesn t work well for bacteria in biofilms more to come on this
17
18 Step 4. Step 4. Result reporting Microbiologist reviews the results and clinical information Decides how to report the results onto the clinical information system May add interpretive comment

19 The REVIEWS problem with wound samples Glabella Alar crease External auditory canal Nare Manubrium Axillary vault Antecubital fossa Volar forearm Hypothenar palm Interdigital web space Inguinal crease Umbilicus Toe web space Actinobacteria Corynebacteriaceae Propionibacteriaceae Micrococciaceae Other Actinobacteria Bacteroidetes Cyanobacteria Firmicutes Other Firmicutes Staphylococcaceae Retroauricular crease Occiput Back Buttock Gluteal crease Popliteal fossa Plantar heel Proteobacteria Divisions contributing <1% Unclassified Sebaceous Moist Dry potential of gut microbiomes, revealing the increased energy harvesting potential of the obesity-associated gut microbiota 51. To date, WGS metagenomic analysis of skin microbiota has not been reported. Several factors delay this type of analysis of skin microbiota. One such factor is the lack of reference genome sequences for skin isolates; this is likely to be due to the difficulty in culturing some skin microorganisms such as the corynebacteria. Furthermore, obtaining the critical amount of starting material required for WGS metagenomic sequencing, free of contaminating host DNA, is challenging for skin. Before skin metagenomic sequencing is tractable on a large scale, robust methods need to be further developed to separate host DNA from microorganism DNA, followed by unbiased whole-genome amplification. Beyond the bacterial microbiome. Molecular approaches have been used to characterize eukaryotic species colonizing the skin, although these methods are not as well developed. The fungal phylogeny has been established using data from six genes: 18S rrna, 28S rrna, 5.8S rrna, elongation factor 1α and two RNA polymerase II subunits 52. When performing molecular surveys of fungal diversity, the most commonly analysed region is the internal transcribed spacer region that separates the small- and large-subunit rrna genes in eukaryotes 53. Most fungal organisms identified on the healthy skin by molecular typing resemble Malassezia spp., closely mirroring culture-based data In one study, Malassezia spp. were calculated to constitute 53 80% of the total skin fungal population, depending on the skin site, with the retroauricular crease harbouring the highest proportion 56. It still remains unclear which fungal species constitute the remainder of the population, and further investigation is warranted. Culture-based analysis suggests that Candida spp. rarely colonize human skin but can cause clinical infection especially in conditions of immune deficiency, diabetes or infection following antibiotic use 4,57. Other types of fungi that, according to culture-based analyses, are thought to grow on the skin,
20
21 Interpretation We know there are lots of bugs there anyway A WS cannot tell you the difference between infection and colonisation Why would we want to sample from a wound, and when should we do it?
22 All wounds are contaminated with bacteria Ulcers and Wounds Only sample wounds/ulcers if there is clinical evidence of infection Sampling from non-infected wounds/ulcers leads to unnecessary antibiotic treatment (Drs/nurses find it hard to ignore results)

23 Clinical Infectious Diseases 2012;54(12):
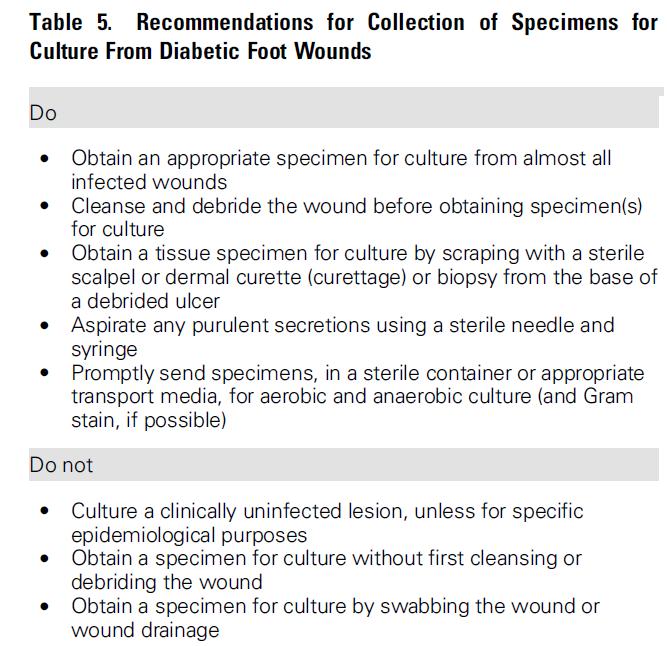
24 Sampling If we suspect an ulcer or wound is infected, we are NOT interested in the organisms on the surface of the wound, but rather the bacteria deep down in the tissues The best samples are actually: 1. Tissue / biopsy / aspirate 2. Wound fluid/pus 3. Swab properly collected The more of the contaminating surface bugs we can avoid the better
25
26 IDSA Guidelines recommend: Recomendations for collection of specimens for culture from diabetic foot wounds How to take a wound swab 1. Clean the surface of the wound of debris with sterile saline 2. Then express fresh pus if possible, and aspirate with needle/syringe a. If there s pus, send us the pus! (much better yield than a swab) 3. Avoid the peri-wound areas (edges) when swabbing 4. The Levine technique may be better than zig-zag technique Rotate the wound swab over a 1 cm 2 area of the central wound over an area of viable tissue (not necrotic), with sufficient pressure to express fluid from within the wound tissue

27 Why don t we like swabs?
28 Vac Wound Swabs We find these even more difficult to interpret! Tend to get overgrown with gram negative organisms, or others that are resistant to the antibiotics the patient is on We don t recommend taking swabs from these wounds (certainly not routinely)

29 Clinical Details Very important! The lab knows nothing about your patient Affects all stages of processing Whether a Gram stain is done Type of culture plates Which antibiotics are tested How the sample is reported onto the system wound swab vs facial cellulitis
30 Relevant Clinical Details for Wound Samples Animal/human bites (Pasteurella, Capnocytophaga, Eikenella, anaerobes etc) Travel (e.g. Pacific Islands -> C.diphtheriae) Environmental exposure (e.g. water -> Aeromonas, Vibrio, MVA -> Bacillus cereus, other environmental org.s, Soil/plant matter contamination -> fungi/other environmental bacteria) Burns (Gram negative organisms, Yeasts, other fungi) Immunosuppression/neutropenia (Gram negatives, fungi) Antibiotic allergies
31 Because wound swabs are often heavily contaminated with colonising organisms making them difficult to interpret, we often ignore the results Treatment generally aimed at most common organisms expected in a given scenario
32 THE USUAL SUSPECTS



33 The Main Offenders Picture of S.aureus and GAS culture + Gram stain Staphylococcus aureus Beta haemolytic streps (e.g. S.pyogenes/Grp A strep) Abx: Flucloxacillin Mild penicillin allergy: cefalexin
34 No. strains Amoxycillin Amoxycillin-clavulanate Amoxycillin-clavulanate: cystitis breakpoint Cephalexin Cefuroxime Co-trimoxazole Erythromycin Flucloxacillin Gentamicin Nitrofurantoin IV Penicillin Doxycycline Trimethoprim Amikacin Ceftazidime Ceftriaxone Clindamycin Ciprofloxacin Meropenem Piperacillin-tazobactam Vancomycin Flucloxacillin + Clindamycin Flucloxacillin + Gentamicin Amoxicillin + Gentamicin Amoxicillin + Gentamicin + Metronidazole Cefuroxime + Metronidazole Augmentin and Gentamicin Combined WDHB, HVDHB,CCDHB Hospitals Antibiogram 2016 Routinely Reported antibiotics Second line or restricted antibiotics Combinations Organism group Swabs, sputum Pseudomonas aeruginosa 424 IR IR IR IR IR IR IR IR IR IR Haemophilus influenzae IR Klebsiella spp all 650 IR IR Enterobacter spp 328 IR 0 IR IR IR Campylobacter spp IR NA NA NA NA Staphylococcus aureus Methicillin-resistant Staphylococcus aureus 891 IR 98 IR 94 IR 96 IR IR Streptococcus pyogenes IR Group B strep IR Streptococcus pneumoniae - meningitis breakpoint Streptococcus pneumoniae - noninvasive breakpoint Urine isolates Escherichia coli from urinary sources IR IR Klebsiella spp from urine 408 IR IR IR Bacteraemia all major pathogens associated with sepsis GNB GPC major pathogens Escherichia coli IR IR Klebsiella spp 37 IR IR IR Staphylococcus aureus NR NR Coagulase -ve staphylococci * one patient with CRE Notes: The testing results do not necessarily relate to treatment choice. For example gentamicin has activity against S. aureus, but it is not regarded as front line therapy. Campylobacter and pneumococcal numbers include community and hospital isolates There were only 2 episodes where S. pneumoniae was cultured from CSF: the numbers are too small to interpret.
35 MRSA Abx options: Co-trimoxazole Doxycycline Clindamycin Wound swab useful if MRSA detected
36 No. strains Amoxycillin Amoxycillin-clavulanate Amoxycillin-clavulanate: cystitis breakpoint Cephalexin Cefuroxime Co-trimoxazole Erythromycin Flucloxacillin Gentamicin Nitrofurantoin IV Penicillin Doxycycline Trimethoprim Amikacin Ceftazidime Ceftriaxone Clindamycin Ciprofloxacin Meropenem Piperacillin-tazobactam Vancomycin Flucloxacillin + Clindamycin Flucloxacillin + Gentamicin Amoxicillin + Gentamicin Amoxicillin + Gentamicin + Metronidazole Cefuroxime + Metronidazole Augmentin and Gentamicin Combined WDHB, HVDHB,CCDHB Hospitals Antibiogram 2016 Routinely Reported antibiotics Second line or restricted antibiotics Combinations Organism group Swabs, sputum Pseudomonas aeruginosa 424 IR IR IR IR IR IR IR IR IR IR Haemophilus influenzae IR Klebsiella spp all 650 IR IR Enterobacter spp 328 IR 0 IR IR IR Campylobacter spp IR NA NA NA NA Staphylococcus aureus Methicillin-resistant Staphylococcus aureus 891 IR 98 IR 94 IR 96 IR IR Streptococcus pyogenes IR Group B strep IR Streptococcus pneumoniae - meningitis breakpoint Streptococcus pneumoniae - noninvasive breakpoint Urine isolates Escherichia coli from urinary sources IR IR Klebsiella spp from urine 408 IR IR IR More common in Maori or Pacific Island Bacteraemia all major pathogens associated with sepsis GNB GPC major pathogens Escherichia coli IR IR Klebsiella spp 37 IR IR IR Staphylococcus aureus NR NR Coagulase -ve staphylococci * one patient with CRE Notes: The testing results do not necessarily relate to treatment choice. For example gentamicin has activity against S. aureus, but it is not regarded as front line therapy. Campylobacter and pneumococcal numbers include community and hospital isolates There were only 2 episodes where S. pneumoniae was cultured from CSF: the numbers are too small to interpret.
37 Diabetics Staph aureus Beta-haemolytic streptococci Anaerobes: Augmentin (good staph/strep cover) Metronidazole (no staph/strep cover)
38 Other Organisms Gram negative organisms e.g. Pseudomonas, Enterobacteriaceae e.g. E.coli, Klebsiella Not primary skin/soft tissue pathogens Don t tend to target these organisms with Abx treatment unless failing + found on culture, or certain situations: Burns Immunocompromised or debilitated patients Other specific situations e.g. wounds sustained in water, flooding victims, bites etc
39 A Common Question Swab of wound grows heavy growth of Pseudomonas aeruginosa What should we treat with?



40 Pseudomonas aeruginosa Opportunistic pathogen Environmental/aquatic organism Lives everywhere, including hospital taps Spa pool folliculitis Readily forms biofilm e.g. in taps Naturally resistant to many antibiotics Selected out in patients receiving antibiotics Unsurprisingly, finds its way into chronic ulcers/wounds!

 Resistance develops")
41 Pseudomonas aeruginosa Naturally resistant to many antibiotics Presents treatment difficulties Only one option for oral treatment: ciprofloxacin Side effects (FDA Boxed Warning) Resistance develops easily

42 A Common Question Swab of wound grows heavy growth of Pseudomonas aeruginosa What should we treat with?
43 BIOFILMS
44

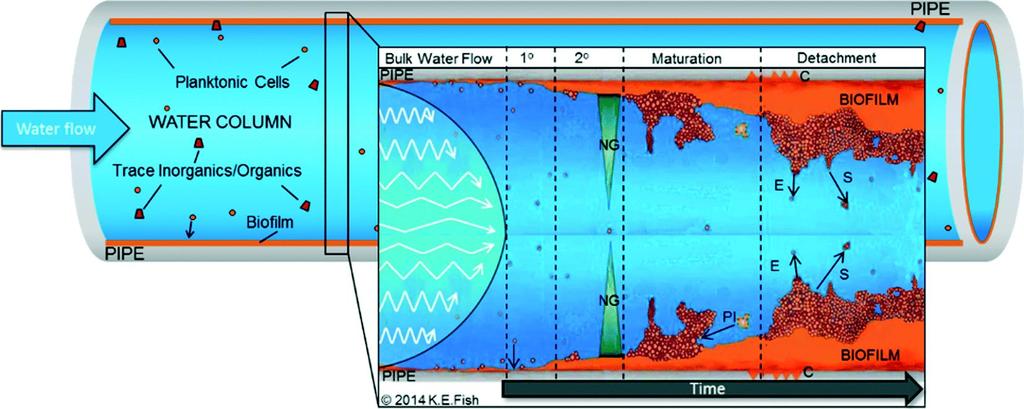
45 Complex community of bacteria bound in matrix Protects them from environmental and other stresses Interact in complex ways, bugs behave very differently in biofilm Biofilm bacteria x more tolerant to ABx: Abx can t penetrate the matrix very well Bugs share resistance enzymes and genes Bacteria less metabolically active Adverse conditions e.g. low ph Lab susceptibility testing designed for planktonic bacteria, NOT biofilms


46




47 Antibiotics not effective at eradicating biofilms Poor blood supply in chronic wounds (Abx don t get in) Also more likely to generate resistance Need to physically remove the biofilm Debridement/wound care
48 ANTIBIOTIC RESISTANCE & STEWARDSHIP

49

50 Figure 3. Annual per capita consumption of antimicrobials, by community-based patients in New Zealand, measured in DDDs/1000 population/day, between 2005 and 2012

51 Figure 4. Annual per capita consumption of antimicrobials by community-based patients, in various European countries 10 and in New Zealand, during 2010, measured in DDDs/1000 population/day
52


53 Date: 21 September 2016 Antimicrobial resistance United Nations high-level meeting on antimicrobial resistance Antimicrobial resistance summit to shape the international agenda
54 Topical Antibiotics NZ has very high fusidic acid resistance BPAC guidelines suggesting use Gene for fusidic acid resistance carried with gene for common NZ MRSA clone (AK3)
 Preference for other antimicrobial/antisepti c agents if required to reduce colonisation Less likely to drive resistance to")
55 Topical Antimicrobials Topical antibiotics not recommended in general (esp. if also available systemically) Preference for other antimicrobial/antisepti c agents if required to reduce colonisation Less likely to drive resistance to useful antibiotics
56 How Can We Help? Good wound care to decrease the risk of infection Good clinical assessment of whether wounds infected Don t give antibiotics for colonisation! Avoid topical antibiotics use of topical antiseptics/antimicrobials if required
57 How Can We Help? Don t send samples for micro unless there is clinical evidence of infection Sampling is often the first step along the path to an antibiotic prescription We know we will grow bugs someone will want to treat them if we show this on a lab report Appropriate, timely narrow spectrum Abx treatment for most, if clinical infection
58 Take Home Messages All wounds have bugs in them whether they re infected or not they will grow if sample is taken! We should only take samples if there is clinical evidence of infection They don t tell us if treatment is required or not, but act as a guide to what the best antibiotic might be Pus or tissue is much better than a swab Antibiotics don t work against biofilms need physical removal Staph aureus and beta-haemolytic streptococci are the most important bugs We try not to treat Pseudomonas and other gram negatives with antibiotics if possible
59 Thanks for your attention
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
2017 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Antimicrobial susceptibility
 Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
2015 Antibiogram. Red Deer Regional Hospital. Central Zone. Alberta Health Services
 2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
2016 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Diabetic Foot Infection. Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals
 Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Diabetic Foot Infection Dr David Orr Consultant Microbiologist Lancashire Teaching Hospitals History of previous amputation [odds ratio (OR)=19.9, P=.01], Peripheral vascular disease (OR=5.5, P=.007)
Cellulitis. Assoc Prof Mark Thomas. Conference for General Practice Auckland Saturday 28 July 2018
 Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Antimicrobial Susceptibility Testing: Advanced Course
 Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
2012 ANTIBIOGRAM. Central Zone Former DTHR Sites. Department of Pathology and Laboratory Medicine
 2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Treatment of Surgical Site Infection Meeting Quality Statement 6. Prof Peter Wilson University College London Hospitals
 Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
Treatment of Surgical Site Infection Meeting Quality Statement 6 Prof Peter Wilson University College London Hospitals TEG Quality Standard 6 Treatment and effective antibiotic prescribing: People with
CUMULATIVE ANTIBIOGRAM
 BC Children s Hospital and BC Women s Hospital & Health Centre CUMULATIVE ANTIBIOGRAM 2017 Division of Medical Microbiology Department of Pathology and Laboratory Medicine Page 1 of 5 GRAM-POSITIVE BACTERIA
BC Children s Hospital and BC Women s Hospital & Health Centre CUMULATIVE ANTIBIOGRAM 2017 Division of Medical Microbiology Department of Pathology and Laboratory Medicine Page 1 of 5 GRAM-POSITIVE BACTERIA
Objectives. Basic Microbiology. Patient related. Environment related. Organism related 10/12/2017
 Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
QUICK REFERENCE. Pseudomonas aeruginosa. (Pseudomonas sp. Xantomonas maltophilia, Acinetobacter sp. & Flavomonas sp.)
") Pseudomonas aeruginosa (Pseudomonas sp. Xantomonas maltophilia, Acinetobacter sp. & Flavomonas sp.) Description: Greenish gray colonies with some beta-hemolysis around each colony on blood agar (BAP),
Pseudomonas aeruginosa (Pseudomonas sp. Xantomonas maltophilia, Acinetobacter sp. & Flavomonas sp.) Description: Greenish gray colonies with some beta-hemolysis around each colony on blood agar (BAP),
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control as recommended by EUCAST Version 5.0, valid from 015-01-09 This document should be cited as "The
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIII NUMBER 1 July 2008 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell, SM (ASCP), Marti Roe SM (ASCP), Ann-Christine Nyquist MD, MSPH Are the bugs winning? The 2007
VOLUME XXIII NUMBER 1 July 2008 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell, SM (ASCP), Marti Roe SM (ASCP), Ann-Christine Nyquist MD, MSPH Are the bugs winning? The 2007
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Role of the nurse in diagnosing infection: The right sample, every time
 BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
BROUGHT TO YOU BY Role of the nurse in diagnosing infection: The right sample, every time The module has been written by Shanika Anne-Marie Crusz and Amelia Joseph Authors affiliation: Department of Clinical
Meropenem for all? Midge Asogan ICU Fellow (also ID AT)
") Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Routine internal quality control as recommended by EUCAST Version 3.1, valid from
 Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
Routine internal quality control as recommended by EUCAST Version.1, valid from 01-01-01 Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing
 Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Suggestions for appropriate agents to include in routine antimicrobial susceptibility testing These suggestions are intended to indicate minimum sets of agents to test routinely in a diagnostic laboratory
Help with moving disc diffusion methods from BSAC to EUCAST. Media BSAC EUCAST
 Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
2010 ANTIBIOGRAM. University of Alberta Hospital and the Stollery Children s Hospital
 2010 ANTIBIOGRAM University of Alberta Hospital and the Stollery Children s Hospital Medical Microbiology Department of Laboratory Medicine and Pathology Table of Contents Page Introduction..... 2 Antibiogram
2010 ANTIBIOGRAM University of Alberta Hospital and the Stollery Children s Hospital Medical Microbiology Department of Laboratory Medicine and Pathology Table of Contents Page Introduction..... 2 Antibiogram
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
European Committee on Antimicrobial Susceptibility Testing
 European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
European Committee on Antimicrobial Susceptibility Testing Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST Version 8.0, valid from 018-01-01
EUCAST recommended strains for internal quality control
 EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
EUCAST recommended strains for internal quality control Escherichia coli Pseudomonas aeruginosa Staphylococcus aureus Enterococcus faecalis Streptococcus pneumoniae Haemophilus influenzae ATCC 59 ATCC
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
2009 ANTIBIOGRAM. University of Alberta Hospital and the Stollery Childrens Hospital
 2009 ANTIBIOGRAM University of Alberta Hospital and the Stollery Childrens Hospital Division of Medical Microbiology Department of Laboratory Medicine and Pathology 2 Table of Contents Page Introduction.....
2009 ANTIBIOGRAM University of Alberta Hospital and the Stollery Childrens Hospital Division of Medical Microbiology Department of Laboratory Medicine and Pathology 2 Table of Contents Page Introduction.....
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
RCH antibiotic susceptibility data
 RCH antibiotic susceptibility data The following represent RCH antibiotic susceptibility data from 2008. This data is used to inform antibiotic guidelines used at RCH. The data includes all microbiological
RCH antibiotic susceptibility data The following represent RCH antibiotic susceptibility data from 2008. This data is used to inform antibiotic guidelines used at RCH. The data includes all microbiological
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Antibiotic Resistance. Antibiotic Resistance: A Growing Concern. Antibiotic resistance is not new 3/21/2011
 Antibiotic Resistance Antibiotic Resistance: A Growing Concern Judy Ptak RN MSN Infection Prevention Practitioner Dartmouth-Hitchcock Medical Center Lebanon, NH Occurs when a microorganism fails to respond
Antibiotic Resistance Antibiotic Resistance: A Growing Concern Judy Ptak RN MSN Infection Prevention Practitioner Dartmouth-Hitchcock Medical Center Lebanon, NH Occurs when a microorganism fails to respond
Introduction. Antimicrobial Usage ESPAUR 2014 Previous data validation Quality Premiums Draft tool CDDFT Experience.
 Secondary Care Data Validation: What do commissioners need to know? Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2014 Introduction Antimicrobial
Secondary Care Data Validation: What do commissioners need to know? Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2014 Introduction Antimicrobial
Cipro for gram positive cocci in urine
 Buscar... Cipro for gram positive cocci in urine 20-6-2017 Pneumonia can be generally defined as an infection of the lung parenchyma, in which consolidation of the affected part and a filling of the alveolar
Buscar... Cipro for gram positive cocci in urine 20-6-2017 Pneumonia can be generally defined as an infection of the lung parenchyma, in which consolidation of the affected part and a filling of the alveolar
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXXII NUMBER 6 September 2017 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Stacey Hamilton MT SM (ASCP), Samuel Dominguez MD PhD, Sarah Parker MD, and
VOLUME XXXII NUMBER 6 September 2017 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Stacey Hamilton MT SM (ASCP), Samuel Dominguez MD PhD, Sarah Parker MD, and
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
National Clinical Guideline Centre Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults
 National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
Lab Exercise: Antibiotics- Evaluation using Kirby Bauer method.
 Lab Exercise: Antibiotics- Evaluation using Kirby Bauer method. OBJECTIVES 1. Compare the antimicrobial capabilities of different antibiotics. 2. Compare effectiveness of with different types of bacteria.
Lab Exercise: Antibiotics- Evaluation using Kirby Bauer method. OBJECTIVES 1. Compare the antimicrobial capabilities of different antibiotics. 2. Compare effectiveness of with different types of bacteria.
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity.
 Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Similar to Penicillins: -Chemically. -Mechanism of action. -Toxicity. Cephalosporins are divided into Generations: -First generation have better activity against gram positive organisms. -Later compounds
Pharmacology Week 6 ANTIMICROBIAL AGENTS
 Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Antimicrobial Resistance Trends in the Province of British Columbia
 655 West 12th Avenue Vancouver, BC V5Z 4R4 Tel 604.707.2443 Fax 604.707.2441 www.bccdc.ca Antimicrobial Resistance Trends in the Province of British Columbia 2013 Prepared by the Do Bugs Need Drugs? Program
655 West 12th Avenue Vancouver, BC V5Z 4R4 Tel 604.707.2443 Fax 604.707.2441 www.bccdc.ca Antimicrobial Resistance Trends in the Province of British Columbia 2013 Prepared by the Do Bugs Need Drugs? Program
A retrospective analysis of urine culture results issued by the microbiology department, Teaching Hospital, Karapitiya
 A retrospective analysis of urine culture results issued by the microbiology department, Teaching Hospital, Karapitiya LU Edirisinghe 1, D Vidanagama 2 1 Senior Registrar in Medicine, 2 Consultant Microbiologist,
A retrospective analysis of urine culture results issued by the microbiology department, Teaching Hospital, Karapitiya LU Edirisinghe 1, D Vidanagama 2 1 Senior Registrar in Medicine, 2 Consultant Microbiologist,
What s new in EUCAST methods?
 What s new in EUCAST methods? Derek Brown EUCAST Scientific Secretary Interactive question 1 MIC determination MH-F broth for broth microdilution testing of fastidious microorganisms Gradient MIC tests
What s new in EUCAST methods? Derek Brown EUCAST Scientific Secretary Interactive question 1 MIC determination MH-F broth for broth microdilution testing of fastidious microorganisms Gradient MIC tests
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how?
 Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
Einheit für pädiatrische Infektiologie Antibiotics - what, why, when and how? Andrea Duppenthaler andrea.duppenthaler@insel.ch Limping patient local pain swelling tenderness warmth fever acute Osteomyelitis
جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی
 جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی ویرایش دوم بر اساس ed., 2017 CLSI M100 27 th تابستان ۶۹۳۱ تهیه
جداول میکروارگانیسم های بیماریزای اولویت دار و آنتی بیوتیک های تعیین شده برای آزمایش تعیین حساسیت ضد میکروبی در برنامه مهار مقاومت میکروبی ویرایش دوم بر اساس ed., 2017 CLSI M100 27 th تابستان ۶۹۳۱ تهیه
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings?
 An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE FOR HEALTHCARE ACQUIRED CEREBROSPINAL FLUID SHUNT ASSOCIATED INFECTIONS
 Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE FOR HEALTHCARE ACQUIRED CEREBROSPINAL FLUID SHUNT ASSOCIATED INFECTIONS FINAL November 29, 2017 Working Group: Joanne Langley (Chair),
Canadian Nosocomial Infection Surveillance Program 2018 SURVEILLANCE FOR HEALTHCARE ACQUIRED CEREBROSPINAL FLUID SHUNT ASSOCIATED INFECTIONS FINAL November 29, 2017 Working Group: Joanne Langley (Chair),
BactiReg3 Event Notes Module Page(s) 4-9 (TUL) Page 1 of 21
 4-9 (TUL) Page 1 of 21") www.wslhpt.org 2601 Agriculture Drive Madison, WI 53718 (800) 462-5261 (608) 265-1111 2015-BactiR Reg3 Shipment Date: September 14, 2015 Questions or comments should be directed to Amanda Weiss at 800-462-5261
www.wslhpt.org 2601 Agriculture Drive Madison, WI 53718 (800) 462-5261 (608) 265-1111 2015-BactiR Reg3 Shipment Date: September 14, 2015 Questions or comments should be directed to Amanda Weiss at 800-462-5261
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Introduction to Chemotherapeutic Agents. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018
 Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Study of Bacteriological Profile of Corneal Ulcers in Patients Attending VIMS, Ballari, India
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 7 (2016) pp. 200-205 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.507.020
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 7 (2016) pp. 200-205 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.507.020
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 1 Reviewing the organisms
 Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 1 Reviewing the organisms Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 1 Reviewing the organisms Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
21 st Expert Committee on Selection and Use of Essential Medicines Peer Review Report Antibiotics Review
 (1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
(1) Have all important studies/evidence of which you are aware been included in the application? Yes No Please provide brief comments on any relevant studies that have not been included: (2) For each of
INFECTIOUS DISEASES DIAGNOSTIC LABORATORY NEWSLETTER
 INFECTIOUS DISEASES DIAGNOSTIC LABORATORY NEWSLETTER University of Minnesota Health University of Minnesota Medical Center University of Minnesota Masonic Children s Hospital May 2017 Printed herein are
INFECTIOUS DISEASES DIAGNOSTIC LABORATORY NEWSLETTER University of Minnesota Health University of Minnesota Medical Center University of Minnesota Masonic Children s Hospital May 2017 Printed herein are
National Surveillance of Antimicrobial Resistance
 National Surveillance of Antimicrobial Resistance Report to Ministry of Health by Sri Lanka College of Microbiologists SLCM ARSP & NLBSA Technical Committees December 2014 National Surveillance of Antimicrobial
National Surveillance of Antimicrobial Resistance Report to Ministry of Health by Sri Lanka College of Microbiologists SLCM ARSP & NLBSA Technical Committees December 2014 National Surveillance of Antimicrobial
Gram-positive cocci Staphylococci and Streptococcia
 Medical microbiology Laboratory Lab 8 Gram-positive cocci Staphylococci and Streptococcia Lecturer Maysam A Mezher Gram positive cocci 1-Staphylococcus. 2-Streptococcus. 3-Micrococcus The medically important
Medical microbiology Laboratory Lab 8 Gram-positive cocci Staphylococci and Streptococcia Lecturer Maysam A Mezher Gram positive cocci 1-Staphylococcus. 2-Streptococcus. 3-Micrococcus The medically important
Antimicrobial Stewardship Strategy: Antibiograms
 Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Aerobic bacterial infections in a burns unit of Sassoon General Hospital, Pune
 Original article Aerobic bacterial infections in a burns unit of Sassoon General Hospital, Pune Patil P, Joshi S, Bharadwaj R. Department of Microbiology, B.J. Medical College, Pune, India. Corresponding
Original article Aerobic bacterial infections in a burns unit of Sassoon General Hospital, Pune Patil P, Joshi S, Bharadwaj R. Department of Microbiology, B.J. Medical College, Pune, India. Corresponding
Cell Wall Weakeners. Antimicrobials: Drugs that Weaken the Cell Wall. Bacterial Cell Wall. Bacterial Resistance to PCNs. PCN Classification
 Cell Wall Weakeners Antimicrobials: Drugs that Weaken the Cell Wall Beta Lactams Penicillins Cephalosporins Carbapenems Aztreonam Vancomycin Teicoplanin Bacterial Cell Wall Bacterial cytoplasm is hypertonic
Cell Wall Weakeners Antimicrobials: Drugs that Weaken the Cell Wall Beta Lactams Penicillins Cephalosporins Carbapenems Aztreonam Vancomycin Teicoplanin Bacterial Cell Wall Bacterial cytoplasm is hypertonic
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Understanding the Hospital Antibiogram
 Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
number Done by Corrected by Doctor Dr.Malik
 number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
C&W Three-Year Cumulative Antibiogram January 2013 December 2015
 C&W Three-Year Cumulative Antibiogram January 213 December 215 Division of Microbiology, Virology & Infection Control Department of Pathology & Laboratory Medicine Contents Comments and Limitations...
C&W Three-Year Cumulative Antibiogram January 213 December 215 Division of Microbiology, Virology & Infection Control Department of Pathology & Laboratory Medicine Contents Comments and Limitations...
number Done by Corrected by Doctor Dr Hamed Al-Zoubi
 number 8 Done by Corrected by Doctor Dr Hamed Al-Zoubi 25 10/10/2017 Antibacterial therapy 2 د. حامد الزعبي Dr Hamed Al-Zoubi Antibacterial therapy Figure 2/ Antibiotics target Inhibition of microbial
number 8 Done by Corrected by Doctor Dr Hamed Al-Zoubi 25 10/10/2017 Antibacterial therapy 2 د. حامد الزعبي Dr Hamed Al-Zoubi Antibacterial therapy Figure 2/ Antibiotics target Inhibition of microbial
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Liofilchem Chromatic Chromogenic culture media for microbial identification and for the screening of antimicrobial resistance mechanisms
 Liofilchem Chromatic Chromogenic culture media for microbial identification and for the screening of antimicrobial resistance mechanisms Microbiology Products since 1983 Liofilchem Chromatic ESBL Selective
Liofilchem Chromatic Chromogenic culture media for microbial identification and for the screening of antimicrobial resistance mechanisms Microbiology Products since 1983 Liofilchem Chromatic ESBL Selective
Prevalence of Metallo-Beta-Lactamase Producing Pseudomonas aeruginosa and its antibiogram in a tertiary care centre
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 952-956 http://www.ijcmas.com Original Research Article Prevalence of Metallo-Beta-Lactamase
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 952-956 http://www.ijcmas.com Original Research Article Prevalence of Metallo-Beta-Lactamase
Antibiotics in the future tense: The Application of Antibiotic Stewardship in Veterinary Medicine. Mike Apley Kansas State University
 Antibiotics in the future tense: The Application of Antibiotic Stewardship in Veterinary Medicine Mike Apley Kansas State University Changes in Food Animal Antibiotic Use How the uses of antibiotics in
Antibiotics in the future tense: The Application of Antibiotic Stewardship in Veterinary Medicine Mike Apley Kansas State University Changes in Food Animal Antibiotic Use How the uses of antibiotics in
Bacterial Pathogens in Urinary Tract Infection and Antibiotic Susceptibility Pattern from a Teaching Hospital, Bengaluru, India
 ISSN: 2319-7706 Volume 4 Number 11 (2015) pp. 731-736 http://www.ijcmas.com Original Research Article Bacterial Pathogens in Urinary Tract Infection and Antibiotic Susceptibility Pattern from a Teaching
ISSN: 2319-7706 Volume 4 Number 11 (2015) pp. 731-736 http://www.ijcmas.com Original Research Article Bacterial Pathogens in Urinary Tract Infection and Antibiotic Susceptibility Pattern from a Teaching
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Who should read this document? 2. Key practice points 2. Background/ Scope/ Definitions 2. What is new in this version? 3
 Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Neurosurgical infections (adult only) Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary
Microbiology : antimicrobial drugs. Sheet 11. Ali abualhija
 Microbiology : antimicrobial drugs Sheet 11 Ali abualhija return to our topic antimicrobial drugs, we have finished major group of antimicrobial drugs which associated with inhibition of protein synthesis
Microbiology : antimicrobial drugs Sheet 11 Ali abualhija return to our topic antimicrobial drugs, we have finished major group of antimicrobial drugs which associated with inhibition of protein synthesis
Florida Health Care Association District 2 January 13, 2015 A.C. Burke, MA, CIC
 Florida Health Care Association District 2 January 13, 2015 A.C. Burke, MA, CIC 11/20/2014 1 To describe carbapenem-resistant Enterobacteriaceae. To identify laboratory detection standards for carbapenem-resistant
Florida Health Care Association District 2 January 13, 2015 A.C. Burke, MA, CIC 11/20/2014 1 To describe carbapenem-resistant Enterobacteriaceae. To identify laboratory detection standards for carbapenem-resistant
Multi-Drug Resistant Organisms (MDRO)
") Multi-Drug Resistant Organisms (MDRO) 2016 What are MDROs? Multi-drug resistant organisms, or MDROs, are bacteria resistant to current antibiotic therapy and therefore difficult to treat. MDROs can cause
Multi-Drug Resistant Organisms (MDRO) 2016 What are MDROs? Multi-drug resistant organisms, or MDROs, are bacteria resistant to current antibiotic therapy and therefore difficult to treat. MDROs can cause
Burn Infection & Laboratory Diagnosis
 Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
Burn Infection & Laboratory Diagnosis Introduction Burns are one the most common forms of trauma. 2 million fires each years 1.2 million people with burn injuries 100000 hospitalization 5000 patients die
The Basics: Using CLSI Antimicrobial Susceptibility Testing Standards
 The Basics: Using CLSI Antimicrobial Susceptibility Testing Standards Janet A. Hindler, MCLS, MT(ASCP) UCLA Health System Los Angeles, California, USA jhindler@ucla.edu 1 Learning Objectives Describe information
The Basics: Using CLSI Antimicrobial Susceptibility Testing Standards Janet A. Hindler, MCLS, MT(ASCP) UCLA Health System Los Angeles, California, USA jhindler@ucla.edu 1 Learning Objectives Describe information
** the doctor start the lecture with revising some information from the last one:
 Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Page 1 of 7 ** the doctor start the lecture with revising some information from the last one: #penicillin G has a good susceptibility against gram(+ve), Neisseria (-ve) #mostly active against strep. (don
Antibacterial Resistance In Wales
 A Report from Public Health Wales Antimicrobial Resistance Programme Surveillance Unit: Antibacterial Resistance In Wales 2005-2012 Authors: Maggie Heginbothom Robin Howe & Catherine Thomas Version: 1
A Report from Public Health Wales Antimicrobial Resistance Programme Surveillance Unit: Antibacterial Resistance In Wales 2005-2012 Authors: Maggie Heginbothom Robin Howe & Catherine Thomas Version: 1
Leveraging the Lab and Microbiology Department to Optimize Stewardship
 Leveraging the Lab and Microbiology Department to Optimize Stewardship Presented by: Andrew Martinez MLS(ASCP), MT(AMT), MBA Alaska Native Medical Center Microbiology Supervisor Maniilaq Health Center
Leveraging the Lab and Microbiology Department to Optimize Stewardship Presented by: Andrew Martinez MLS(ASCP), MT(AMT), MBA Alaska Native Medical Center Microbiology Supervisor Maniilaq Health Center
Antimicrobial susceptibility testing challenges. Linda Joyce St Vincent s Hospital Melbourne
 Antimicrobial susceptibility testing challenges Linda Joyce St Vincent s Hospital Melbourne Bacteria/antimicrobials without breakpoints (B.A.W.B.S.) Enterobacteriacae Pseudomonas aeruginosa, Acinetobacter
Antimicrobial susceptibility testing challenges Linda Joyce St Vincent s Hospital Melbourne Bacteria/antimicrobials without breakpoints (B.A.W.B.S.) Enterobacteriacae Pseudomonas aeruginosa, Acinetobacter
The Rise of Antibiotic Resistance: Is It Too Late?
 The Rise of Antibiotic Resistance: Is It Too Late? Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine None DISCLOSURES THE PROBLEM Antibiotic resistance is one of the
The Rise of Antibiotic Resistance: Is It Too Late? Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine None DISCLOSURES THE PROBLEM Antibiotic resistance is one of the
Antibacterial Resistance In Wales
 A Report from Public Health Wales Antimicrobial Resistance Programme Surveillance Unit: Antibacterial Resistance In Wales 2005-2013 Authors: Maggie Heginbothom and Robin Howe Version: 1 Antibacterial Resistance
A Report from Public Health Wales Antimicrobial Resistance Programme Surveillance Unit: Antibacterial Resistance In Wales 2005-2013 Authors: Maggie Heginbothom and Robin Howe Version: 1 Antibacterial Resistance