Antibiotic use before chlamydia and gonorrhea genital. and extragenital screening in the STI clinic setting
|
|
|
- Brice Todd
- 5 years ago
- Views:
Transcription
1 AAC Accepts, published online ahead of print on 13 October 2014 Antimicrob. Agents Chemother. doi: /aac Copyright 2014, American Society for Microbiology. All Rights Reserved. 1 2 Antibiotic use before chlamydia and gonorrhea genital and extragenital screening in the STI clinic setting Nicole HTM Dukers-Muijrers* 1,2, Genevieve AFS van Liere 1,2 Petra FG Wolffs 2 Casper Den Heijer 1, Marita ILS Werner 1, Christian JPA Hoebe 1,2 1 Department of Sexual Health, Infectious Diseases and Environmental Health, South Limburg Public Health Service, Geleen, the Netherlands 2 Department of Medical Microbiology, School of Public Health and Primary Care (CAPHRI), Maastricht University Medical Centre (MUMC+) Maastricht, the Netherlands Running Head: Antibiotics preceding STI care practice *Address correspondence to Nicole Dukers-Muijrers, Nicole.dukers@ggdzl.nl 1
2 ABSTRACT Background antibiotic use (i.e. administration of antibiotics not directly related to Chlamydia trachomatis (Ct) or Neisseria gonorrhoea (GC)) infections has been associated with a lower prevalence of genital Ct infection in a clinical setting. Associations with specific antibiotic types or with GC are lacking. Here, we assess the prevalence of antibiotic use, the different classes and agents used and their association with a subsequent STI clinic Ct and GC test result. At our STI clinic, we systematically registered whether antibiotics were used in the past month (in 29% of the cases, the specific antibiotic agent was named). Patients were screened for urogenital Ct and Ng; a third of them were also screened for anorectal and oropharyngeal Ct and GC. The proportion of antibiotics used and their association with Ct and GC prevalence was assessed for heterosexual men, men who have sex with men (MSM) and women. During clinic consultations, antibiotic use was reported by 12.2% (95% CI: 95% CI: 11.7%-12.7%), i.e. 14.8% of women, 8.6% of heterosexual men and 11.6% of MSM. Tthe most reported antibiotics were penicillins, tetracyclines and macrolides, respectively. The prevalence was 11.0% (95%CI: 10.3%-11.3%) for Ct and 1.9% (95% CI: 1.7%-2.1%) for GC. Only tetracycline use was associated with a lower Ct prevalence (3%). Overall antibiotic use was associated with lower anorectal Ct prevalence in MSM only (odds ratio: 0.4, 95% CI: ). STI clinic visitors commonly report recent antibiotic use. Even in a country with low antibiotic consumption, tetracycline use impacted Ct prevalence, while there was a notable absence of association with azithromycin. 2
3 INTRODUCTION It is a continuous challenge to control the spread of sexually transmitted infections (STIs). Many cases are hidden to care and remain untested and untreated, for example cases of Chlamydia trachomatis (Ct) and Neisseria gonorrhoea (GC) [1,2]. Furthermore, control of GC is hampered by growing antimicrobial resistance [3-5]. Ct and GC are among the most common bacterial STIs If not adequately treated, they may result in serious complications such as epididymitis in men and pelvic inflammatory disease, infertility and ectopic pregnancy in women [6]. Ct infection can be treated by several classes of antibiotics: macrolides (i.e. azithromycin) and tetracyclines (i.e. doxycycline) are the recommended options. Alternatively, fluoroquinolones and quinolones (i.e. ofloxacin) can be prescribed [7,8,9]. GC can be treated with ceftriaxone or with ciprofloxacin when ceftriaxone is contraindicated and strains show no ciprofloxacin resistance [7,8,9]. Treatment of GC is complicated by increasing rates of resistance to quinolones, tetracyclines and penicillins and a decreasing susceptibility to cephalosporins [3-5]. Australian research has postulated that Ct may be incidentally treated in countries with a relatively high background antibiotic consumption [10,11], as the overall annual number of antibiotic prescriptions generally outweighs the frequency of Ct testing. The volume of outpatient systemic antibiotic use increased in most European countries between 1997 and 2003, while consumption remained stable between 2007 and 2011: a median consumption of 19.5 Defined Daily Doses (DDD) per 1000 inhabitants per day [12,13]. An ecological analysis of studies from 12 European countries demonstrated an inverse correlation between tetracycline and macrolide use in the year 2002 and genital Ct prevalence in all countries except for the Netherlands [12]. Tetracyclines and macrolides belong to the most commonly prescribed group of systemic antibacterial antibiotics after penicillins [13]. The Netherlands has historically had the lowest prescription rate of all European countries, although an increase has been noted (reaching a DDD of 11.4 per 1000 inhabitants per day in 2011) [13]. The Ct test rate in the Netherlands has been estimated to be 3 per 1000 persons in the community [14]. While background antibiotic use may impact the transmission of STIs on a population level, it may also 3
4 impact clinical practices since it affects the outcome of an STI diagnostic test and may interact with subsequent treatment. Studies among men and young women receiving antenatal, general practitioner or sexual health care in Australia demonstrated that recent antibiotic use was associated with a lower prevalence and incidence of genital Ct [1,15,16,17]. However, the specific antibiotic agents were not studied. Such reports are lacking for Ng, yet a similar phenomenon may be observed. The consumption of antibiotics may lead to increasing rates of resistance in the population, so overall antibiotic use may impact the clinical practice of STI testing. The number of incidentally treated GC infections is probably minimal as GC is more symptomatic and is therefore more likely to be identified and treated promptly. In this study, conducted in a country with low per capita antibiotic consumption (i.e. The Netherlands), we assessed the proportion of systemic antibiotic use before Ct and GC genital and extragenital (anorectal and oropharyngeal) screening in women and men visiting an STI clinic. Further, we tested the association between overall systemic antibiotic use and the specific agent, and the result of subsequent Ct and GC tests. MATERIALS AND METHODS Procedures and study population The outpatient STI clinic of the South Limburg Public Health Service offers free-of-charge examination and treatment for STIs. The clinic has four fixed testing sites in South Limburg (population 630,000). The study population includes surveillance data from all patients 18 years and older who visited our STI clinic between August 2010 and October 2013 (n=14945). At every new consultation, patients were tested urogenitally for Ct and GC on first void urine (men) or self-swab (women) and some of the patients (38%; n=5691) were also tested anorectally by self-swab (men and women) and/or oropharyngeally by nurse-taken swab (men and women). Testing was done by commercially available NAAT (SDA, Becton Dickinson ProbeTec ET system, Maryland, USA, or PCR, Roche Cobas Amplicor, 4
5 California, USA, or Roche Cobas 4800, California, USA; positive GC tests were confirmed by an inhouse PCR). In accordance with national guidelines, patients who tested positive were asked to return for treatment with azithromycin or doxycycline (in case of Ct) or with ceftriaxone (in case of Ng). From August 2010, we systematically registered (by self-report) whether patients had used antibiotics in the month preceding the screening test. An additional open question was asked about the type of regimen used: patients filled in their prescribed course and/or their indication for use. Variables and statistical analyses We assessed the prevalence of systemic antibiotic use and its association with Ct or GC diagnoses. To reduce confounding by indication (thereby excluding people who were recently treated for an STI), we removed certain consultations from the data: those that occurred within 45 days after a previous STI clinic consultation (n=100) or consultations in which a client reported a Ct or GC diagnosis in the past month (n=70). This resulted in consultations in our analyses. Of all the people who answered yes for antibiotic use (n=1994), 132 reported using medication other than systemic antibacterial treatment (e.g. painkillers, non-systemic (e.g. topical) antibiotics, anti-fungals, inhalation medication, antihistamines) and an additional 61 reported no systemic antibiotic agent but an indication that was not likely for systemic antibiotic use (i.e. fungal infection, herpes, eye infection, parasitic worms, hay fever, impetigo). In our analyses, we considered the patients in these 193 consultations to not have used systemic antibiotics. Of the 1801 remaining consultations in which antibiotic use was reported, named agents were given in 541 and no agents were named in the remaining We constructed several variables on antibiotic use (yes/no) by agent based on the reported antibiotic agent that was recommended against Ct or Ng: doxycycline, azithromycin, ofloxacin, erythromycin, amoxicillin, ceftriaxone and ciprofloxacin. Other variables were constructed on the combined classes of reported agents: tetracyclines, macrolides, fluorquinolones and quinolones, penicillins, cephalosporins, nitrofurantion/fosfomycin/trimethoprim and other (i.e. mainly metronidazole). 5
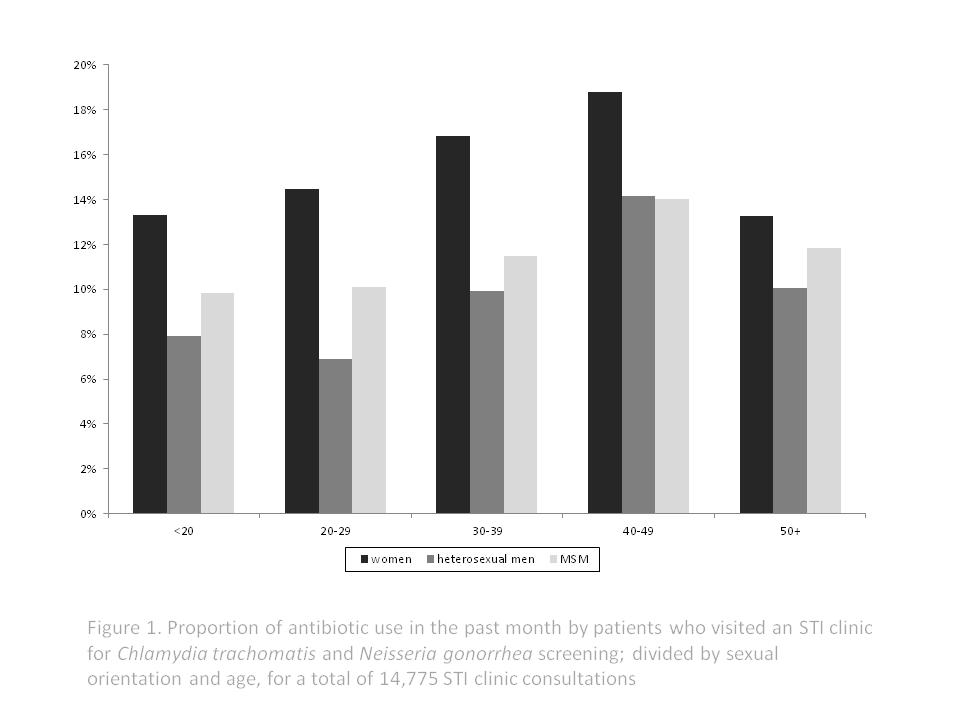
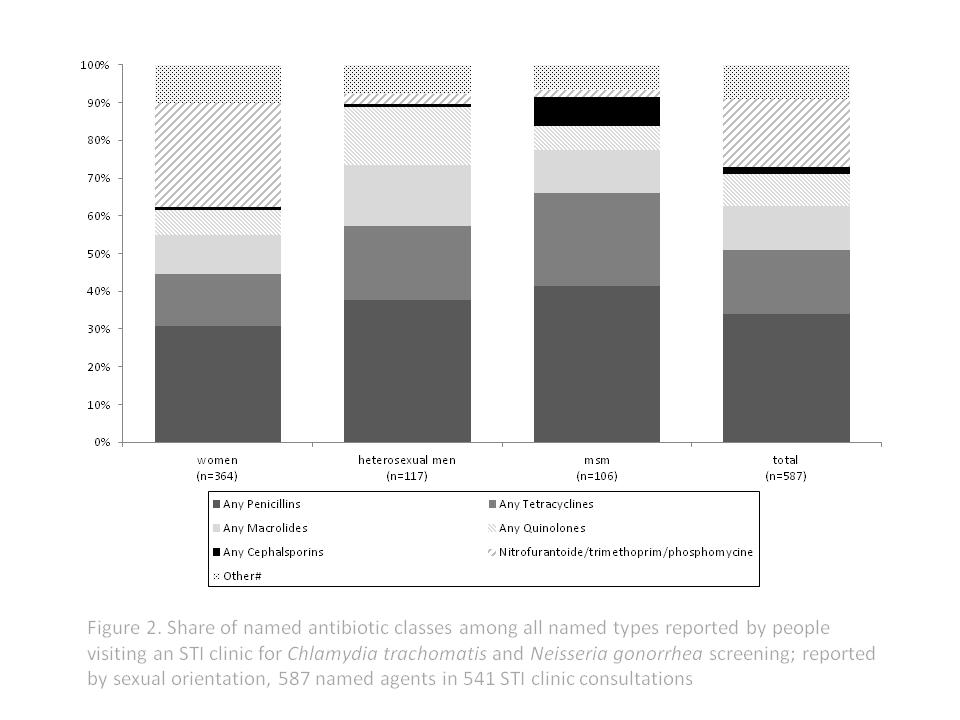
6 First, we used chi-square analyses to compare characteristics of the study population, including antibiotic use, between women, heterosexual men and men who have sex with men (MSM). Second, we used chi-square tests to make associations between overall antibiotic use and age, gender, sexual orientation and HIV positivity in the total group of consultations. Third, we used univariate and multivariable logistic regression analyses, accounting for repeated measures, to assess overall antibiotic use, antibiotic use by agent, gender, sexual orientation, HIV status and age (and their interaction), as determinants for Ct and for GC positivity. In analyses evaluating antibiotic use by specific agent, we excluded consultations in which antibiotics were reported but no specific agent was named (n=1260; resulting in n=13515 used in analyses). Overall Ct and GC (at any site) was used as the outcome, but we also performed analyses stratified by anatomic site. We noted differences between anatomic sites and considered a p value <0.05 to be statistically significant. Analyses were performed using the SPSS package version 20 (IBM Inc. Somers, New York, USA). Ethical approval The medical ethical committee of Maastricht University approved the study (no ). RESULTS Antibiotic use before STI testing During STI clinic testing consultations, 12.2% (n=1801) (95% CI: 11.7%-12.7%) of clinic patients reported recent antibiotic use. Women had higher rates of antibiotic use than heterosexual men or MSM, and antibiotic use increased with age (all p<0.001; Figure 1). Antibiotic use was also higher for those who were HIV positive (18.6% versus 12.1% of HIV negatives; p=0.004). Antibiotics were used for various reasons (e.g. for urinary tract infections (UTI) and respiratory tract infections (RTI)) yet, in the majority of cases (63%), data about the indication of antibiotic usage was absent. The specific agent(s) were named in 541 (30.0%) of the consultations where patients reported antibiotic use. The reported frequencies of use are displayed in Table 1 and the share of use in Figure 2. Of the named agents, 26.2% (n=142) contained any of the following: doxycycline, azithromycin, 6
7 ofloxacin or erythromycin. Another 6.3% (n=34) consisted of ceftriaxone or ciprofloxacin. In 46 consultations, patients reported using a combination of two different agents. The antibiotics used varied by gender and sexual orientation (Table 1). Penicillins were most frequently reported, followed by nitrofurantoin/trimethoprim/fosfomycin (commonly used for UTI) in women and tetracyclines and macrolides in both men and women (Figure 2). Prevalence of Ct and association with antibiotic use The overall prevalence of Ct was 10.8% (95% CI: 10.3%-11.3%) (Table 1) and recent antibiotic use was reported by 10.8% (173/1597) of patients who received Ct diagnoses. The association between antibiotic use and Ct differed between women, heterosexual men and MSM (overall P interaction-term 0.019). In univariate analyses, any recent antibiotic use was associated with a lower Ct prevalence in heterosexual men and in MSM but not in women (Table 2). When adjusting for age and HIV status, the risk estimate for heterosexual men attenuated somewhat and became non-statistically significant; however, the risk remained for MSM (Table 2). After stratifying analyses in MSM by anatomic site, it appeared that the inverse association between antibiotic use and Ct was only observed for anorectal Ct in MSM (OR adjusted for HIV and age: 0.42, 95% CI: ) and not for genital Ct in MSM (adjusted OR: 0.58, 95% CI: ) or oral Ct in MSM (adjusted OR: 1.10, 95% CI: ). We also evaluated associations with specific agents, thereby excluding from our analyses the consultations with patients who reported antibiotic use but failed to name the agent used (Table 3). Additional analyses demonstrated that whether or not a specific antibiotic agent was reported, was not associated with Ct (or with Ng) nor was the reason for antibiotic use (UTI, RTI or other; data not shown). As no interactions were observed between the evaluated agents and sexual orientation (all p>0.20), this paper presents overall models assessing Ct and GC (rather than separate models for women, heterosexual men and MSM). In both univariate and multivariate analyses, tetracycline use was inversely associated with Ct (Table 3). Further analyses showed the associations between tetracycline use and specific anatomic sites: for genital Ct (OR adjusted for gender, sexual orientation, age, and HIV status: 0.25, 95% 7
8 CI: ) and for anorectal Ct (adjusted OR: 0.26, 95% CI: ). Oropharyngeal Ct was not evaluated due to small numbers Prevalence of GC and association with antibiotic use The overall prevalence of GC was 1.9% (95% CI: 1.7%-2.1%) (Table 1) and recent antibiotic use was reported by 13.1% (37/282) of patients who received GC diagnoses. Overall antibiotic use was not associated with Ng, even when assessing associations for genital, anorectal or oral GC (data not shown) or by sexual orientation (Table 2). In univariate analyses, quinolone use was positively associated with Ng, while the risk estimate attenuated somewhat and became non-statistically significant in multivariate analyses (Table 3). DISCUSSION This is the first study to systematically assess the recent consumption of different antibiotic agents before STI testing and the impact of background antibiotic use on a Ct and GC diagnostic test result in a clinical setting. One out of eight clinic patients reported recent antibiotic use, of which only a minority were first-line treatments for Ct or GC. Tetracyclines were the only agents found to be associated with a lower Ct prevalence. In MSM, overall antibiotic use was associated with a lower anorectal Ct prevalence. Prior antibiotic use was not associated with GC. The observed recent antibiotic consumption rate (12%) may be higher than expected (5.5%, based on the background antibiotic consumption in the Netherlands of 11.4 DDD per 1000 persons per day, considering a typical course of five days with a daily dose in each course that equals DDD, depending on distribution of courses among individuals) [11,13]. It is possible that the symptoms that led some patients to visit the STI clinic may have also prompted earlier health care visits (e.g. to their GP). It also has been not uncommon in some communities globally to use antibiotics for prophylactic reasons prior to screening tests [18]. The share of the classes named were in line with reported rates from surveillance networks, with penicillins being most commonly used [13]. Tetracyclines (comprised mostly of 8
9 doxycycline) were associated with a lower Ct prevalence, confirming the ecological correlation found in other European countries between tetracyclines and a lower Ct prevalence [11]. While the consumption of macrolides per capita also correlated significantly with a lower chlamydia prevalence in Europe, the absence of an association between macrolides (azithromycin in particular) and Ct prevalence in our current study was notable. Azithromycin is commonly applied by using 500 mg daily for three to five days in non-ct infections (e.g. in RTIs); in Ct infections, the recommended dosage is higher but the duration is shorter (one 1000 mg dose). This difference in regimens may explain the absence of an association between background azithromycin use and Ct. Still, differences in regime were also present for doxycycline and other macrolides (e.g. the recommended dose for non-ct sinusitis is lower but of an equal duration as that in Ct infections). Although azithromycin is the most commonly used treatment for Ct in many countries, its efficacy is currently under heavy debate and several studies have demonstrated substantial post-treatment Ct detection [19,20]. While Ct DNA may remain detectable in up to 40% of patients after three weeks of treatment with azithromycin, it is unknown whether detection indicates a persisting Ct infection and whether detection rates differ between azithromycin and doxycycline [19,20]. There is no comparison data from other studies as no agent-specific associations at an individual level have yet been reported [15-17]. We could not confirm earlier Australian observations of an inverse association between overall antibiotic use and Ct prevalence, except for MSM. This may be due to differences in the study populations; the people in current study are higher risk- STI clinic attendees who potentially are more prone to acquiring a new STI after recent antibiotic use but before screening, attenuating associations in STI clinic populations. However, STI clinics tend to not test individuals with recent STI exposure (patients are asked to come back after a certain window phase) and therefore, such possible effect is likely to be minimal. Are more likely explanation is that, lower shares of consumption of anti-ct classes in the Netherlands compared to Australia may explain the discrepancy. MSM in our study reported higher shares of tetracycline use than did heterosexual men or women; the latter group reported relatively high rates of use of nitrofurantoin, trimethoprim or fosfomycin (i.e. agents not considered effective against Ct). 9
10 To our knowledge, this is the first report on the association between recent antibiotic use and GC. We observed no association between recent antibiotic use and GC. The implications for antibiotic use are broad and range from the contribution to antibiotic resistance, the utility of screening and their impact on transmission and the epidemiology of infection. The impact of our results on clinical practice should be considered in the light of superfluous testing (of incidentally treated cases) or unwanted effects of subsequent treatments (i.e. treatment interactions or induction of treatment-resistant GC isolates). For Ng, superfluous testing is likely not a problem as ceftriaxon (first-line GC treatment) is infrequently used, hence its impact on incidentally treated GC cases is probably limited. For Ct, one may argue that patients who had been treated recently (e.g. with azithromycin or doxycycline) should not be screened again for Ct as they could be assumed to have been cured (treated) or to have acquired their infection very recently (after antibiotic use). In both cases they would not be eligible for screening. However, macrolide (or azithromycin) use was not associated with a lower Ct prevalence and, in those patients who had used tetracyclines, the Ct prevalence was low (3%) but not completely zero. As noted before, it is yet unknown whether detected Ct DNA really indicates a persistent infection in treated cases, since no laboratory tests that can test this exist. Antimicrobial resistance and overuse of antimicrobials are considered serious threats, especially to the treatment of GC [5]. In 2011, the European Gonococcal Antimicrobial Surveillance Programme (Euro-GASP) found that 7.6% of isolates were resistant to cefotaxime (2.3% in the Netherlands; RIVM, GRAS, 2013). Euro-GASP also detected isolates with decreased susceptibility to ceftriaxone for the first time [21,22]. Penicillin-, tetracycline-, quinolone- and fluorquinolone-resistant GC isolates are now disseminated globally. Of all the diagnosed GC cases in our study, 13% reported recent antibiotic use. Potential induced resistance to first-line GC treatment (ceftriaxone) does not (or not yet) seem to be an important factor in current clinical treatment of GC. However, GC seems to retain resistance to several classes of antimicrobials, even when the antimicrobials in question are discontinued. Hence, resistance to other antimicrobials may still be a point of concern. 10
11 The prevalence of GC and Ct in patients who used quinolones was higher than in those who did not use quinolones. This finding should be interpreted with caution due to relatively low numbers. Nevertheless, it may reflect the possibility that symptoms related to Ct and GC have caused patients to use quinolones before visiting the STI clinic for further testing. On the other hand, it could be hypothesized that the marginally positive association may reflect possible increased susceptibility due to its effect on protective alternative microbiota [23]. Finally, the possible interaction (antagonistic or synergic) effects between treatments should always be carefully considered in clinical practice for persons who are currently using antibiotics. Altogether, the impact of background antibiotic use on STI clinic practice seems relatively limited so far, although this may change with increasing antibiotic consumption and it may be different in countries with a higher background antibiotic consumption. This study has several limitations. First, the information on antibiotic use was based on selfreport, which is subject to both under-and over-reporting bias. Second, the specific antibiotic agent could not be identified in two-thirds of consultations. The reported indications were not attributed to a specific agent as the first-line regimens and their use in practice did not refer to a single agent or class of antibiotics. This limited our analyses to some extent, especially by largely underestimating the prevalence of use of specific agents in the total population and possibly attenuating observed associations with STI prevalence. We have no reason to assume that potential reporting bias may have affected the share of reported agents (as displayed in Figure 2). While this study is the only study to date to report on specific agents of background antibiotic use at an individual level in a clinic setting, numbers for some agents were small, limiting statistical analyses for detecting associations. Third, no information was available about the exact dosage, start date and duration. There was also no information about whether a client currently used antibiotics or had stopped more than a week ago. In clinical practice, it would be useful to know whether treatment was current or less recent. When designing future studies, these issues need to be taken into account, for example by prospective systematic assessment of antibiotic consumption by a trained interviewer. When available, review of prescribing records would limit the flaws introduced by self-reports. Fourth, it is likely that non genital infections were missed as anorectal or oropharyngeal Ct 11
12 and GC were not tested in all individuals possible attenuating associations with antibiotic use. However, potential underestimation of risk estimates is likely minimal as restricting the data to people tested at all anatomic sites revealed highly similar results (i.e. for women OR:0.86, 95%CI: (total group OR:1.09, for heterosexual men OR:0.86, 95%CI: (total group OR: 0.74), and for MSM OR:0.42, 95%CI: (total group OR: 0.49). In conclusion, recent antibiotic use is common: one of eight clinic patients reported it before being screened for STI. Tetracyclines are associated with a lower Ct prevalence, while there is a notable absence of an association between Ct and azithromycin. Some patients who tested positive for Ct and GC had very recently been treated with antibiotics, so possible interactions with current clinic treatments need to be carefully considered. Still, a large part of the reported antibiotics are not first-line treatments against Ct or GC. The impact of background antibiotic use on STI clinic practice seems relatively limited, although that may be different in countries with a higher background antibiotic consumption. Downloaded from on July 17, 2018 by guest 12
13 Acknowledgements The authors thank the staff of the STI clinic and Helen Sijstermans (Health Service South Limburg), and Kevin Theunissen (Health Service South Limburg) for assistance in retrieving the data Key messages 1. One in eight clinic patients reported recent antibiotic use before they were screened for chlamydia and gonorrhea. 2. A large part of the reported antibiotics are not first-line treatments against chlamydia or gonorrhea. 3. Tetracyclines are associated with a lower chlamydia prevalence in screening, while there is a notable absence of an association with macrolides (i.e. azithromycin). 4. Background antibiotic use is not associated with gonorrhea prevalence. 5. The impact of background antibiotic use on STI clinic practice seems relatively limited, although it may be different when per capita consumption increases or in countries with a higher background antibiotic consumption. 13
14 References 1. Turner CF, Rogers SM, Miller HG, Miller WC, Gribble JN, Chromy JR, Leone PA, Cooley PC, Quinn TC, Zenilman JM Untreated gonococcal and chlamydial Infection in a probability sample of adults. JAMA. 287: doi: / jama Senior K Chlamydia: a much underestimated STI. Lancet Infect Dis. 12(7): Davies SC, Fowler T, Watson J, Livermore DM, Walker D Annual Report of the Chief Medical Officer: infection and the rise of antimicrobial resistance. Lancet. 381: World Health Organization Global action plan to control the spread and impact of antimicrobial resistance in Neisseria gonorrhoeae Geneva: World Health Organization. 5. Low N, Unemo M, Skov Jensen J, Breuer J, Stephenson J Molecular Diagnostics for Gonorrhoea: Implications for Antimicrobial Resistance and the Threat of Untreatable Gonorrhoea. PLoS Med. 11(2): e Published online Feb 4, doi: /journal.pmed Price MJ, Ades AE, De Angelis D, Welton NJ, Macleod J, Soldan K, Simms I, Turner K, Horner PJ Risk of pelvic inflammatory disease following Chlamydia trachomatis infection: analysis of prospective studies with a multistate model. Am J Epidemiol. 1;178(3): doi: /aje/kws583. Epub 2013 Jun Centers for Disease Control and Prevention (CDC) STD Treatment Guidelines. MMWR Recomm Rep 59: British Association for Sexual Health and HIV (BASHH) Chlamydia trachomatis UK Testing Guidelines. Clinical Effectiveness Group. Update to Chlamydia testing. Available: and 9. Westrom L Incidence, prevalence, and trends of acute pelvic inflammatory disease and its consequences in industrialized countries. Am J Obstet Gynecol. 138(7 Pt 2): O Rourke KM, Fairley CK, Samaranayake A, Collignon P, Hocking JS Trends in Chlamydia positivity over time among women in Melbourne Australia, 2003 to 2007.STD. 36(12):
15 Ginige S, Chen MY, Hocking JS, Read TR, Fairley CK Antibiotic consumption and chlamydia prevalence in international studies. Sex Health. 3(4): Ferech M, Coenen S, Malhotra-Kumar S, Dvorakova K, Hendrickx E, Suetens C, Goossens H ESAC ProjeCt Group. European Surveillance of Antimicrobial Consumption (ESAC): outpatient antibiotic use in Europe. J Antimicrob Chemother. 58(2): Epub 2006 May European Centre for Disease Prevention and Control Surveillance of antimicrobial consumption in Europe Stockholm: ECDC; Land JA, Van Bergen JE, Morré SA, Postma MJ Epidemiology of Chlamydia trachomatis infection in women and the cost-effectiveness of screening. Hum Reprod Update. 16(2): doi: /humupd/dmp035. Epub 2009 Oct Walker J, Tabrizi SN, Fairley CK, Chen MY, Bradshaw CS, Twin J, Taylor N, Donovan B, Kaldor JM, McNamee K, Urban E, Walker S, Currie M, Birden H, Bowden F, Gunn J, Pirotta M, Gurrin L, Harindra V, Garland SM, Hocking JS Chlamydia trachomatis incidence and reinfection among young women--behavioural and microbiological characteristics. PLoS One. 7(5):e doi: /journal.pone Epub 2012 May Chen MY, Fairley CK, De Guingand D, Hocking J, Tabrizi S, Wallace EM, Grover S, Gurrin L, Carter R, Pirotta M, Garland S Screening pregnant women for chlamydia: what are the predictors of infection? Sex Transm Infect. 85(1):31-5. doi: /sti Epub 2008 Aug Chen MY, Rohrsheim R, Donovan B The differing profiles of symptomatic and asymptomatic Chlamydia trachomatis-infected men in a clinical setting. Int J STD AIDS. 18: Klausner JD, Aplasca MR, Mesola VP, Bolan G, Whittington WL, Holmes KK. Correlates of gonococcal infection and of antimicrobial-resistant Neisseria gonorrhoeae among female sex workers, Republic of the Philippines, J Infect Dis Mar;179(3): Dukers-Muijrers NH, Speksnijder AG, Morre SA, Wolffs PF, van der Sande MA, Brink AA, van den Broek IV, Werner MI, Hoebe CJ Detection of anorectal and cervicovaginal Chlamydia trachomatis infections following azithromycin treatment: prospective cohort study with multiple time- 15
16 sequential measures of rrna, DNA, quantitative load and symptoms. PLoS One.14(11):e doi: /journal.pone Hathorn E, Opie C, Goold P What is the appropriate treatment for the management of rectal Chlamydia trachomatis in men and women? Sex Transm Infect. 88: 352e354 doi: /sextrans European Centre for Disease Prevention and Control Response plan to control and manage the threat of multidrug-resistant gonorrhoea in Europe. Stockholm: ECDC; National Institute For Public Health and the Environment (RIVM) Sexually transmitted infections, including HIV, in The Netherlands, Bilthoven, The Netherlands. Report number / Stokholm J, Schjørring S, Eskildsen CE, Pedersen L, Bischoff AL, Følsgaard N, Carson CG, Chawes BL, Bønnelykke K, Mølgaard A, Jacobsson B, Krogfelt KA, Bisgaard H Antibiotic use during pregnancy alters the commensal vaginal microbiota. Clin Microbiol Infect. Oct 1. doi: /
17 Conflict of interest statement There are no conflicts of interest. The corresponding author has had full access to all the data in the study and had final responsibility for the decision to submit for publication Funding Investigator initiated Contributions of the authors Contributions: ND analyzed the data and wrote the manuscript; all authors contributed to the final draft of the manuscript. Word count Abstract: 259 words Article: 3379 words (text only) 17
18 APPENDIXES Figure 1. Proportion of antibiotic use in the past month by patients who visited an STI clinic for Chlamydia trachomatis and Neisseria gonorrhea screening; divided by sexual orientation and age, for a total of 14,775 STI clinic consultations Figure 2. Share of named antibiotic classes among all named types reported by people visiting an STI clinic for Chlamydia trachomatis and Neisseria gonorrhea screening; reported by sexual orientation, 587 named agents in 541 STI clinic consultations Table 1: Characteristics of the study population and self-reported antibiotic use in the past month; divided by sexual orientation, for a total of STI clinic consultations Table 2: Proportion of Chlamydia trachomatis (Ct) and Neisseria gonorrhea (Ng) positive screening diagnoses and association with preceding use of antibiotics; for a total of STI clinic consultations Table 3: Proportion of Ct and GC positive screening diagnoses and association with preceding use of specific agents of antibiotics; for a total of STI clinic consultations 18
19 Table 1: Characteristics of the study population and self-reported antibiotic use in the past month; divided by sexual orientation, for a total of STI clinic consultations Women Heterosexual men MSM Total N=7419 N=5007 N=2349 N=14775 % (n) % (n) % (n) P~ % (n) Age (median; interquartile range) 23 (20-30) 25 (22-36) 37 (25-48) ** 24 (21-37) Ct diagnosis (any site)$ 10.6 (788) 11.8 (593) 9.2 (216) ** 10.8 (1597) Genital Ct diagnosis& 10.2 (757) 11.7 (588) 3.2 (76) ** 9.6 (1421) Anorectal Ct diagnosis& 6.5 (136) 0.9 (7) 7.3 (162) ** 6.0 (305) Oropharyngeal Ct diagnosis& 1.4 (22) 0.2 (2) 0.7 (16) ** 0.8 (40) Ng diagnosis (any site)$ 1.1 (82) 1.0 (50) 6.4 (150) ** 1.9 (282) Genital Ng diagnosis& 0.6 (45) 0.6 (30) 1.4 (32) ** 0.7 (107) Anorectal Ng diagnosis& 0.7 (15) 0.4 (3) 4.0 (88) ** 2.1 (106) Oropharyngeal Ng diagnosis& 2.7 (43) 2.2 (19) 3.4 (79) 3.0 (141) HIV positive~ 0.2 (13) 0.1 (7) 9.2 (216) 1.6 (236) Overall antibiotic use (past month) 14.8 (1099) 8.5 (428) 11.7 (274) ** 12.2 (1801) Antibiotic use per named indication Urinary tract infections (UTI) 3.1 (229) 0.2 (12) 0.3 (6) ** 1.7 (247) Respiratory tract infections (RTI) 1.4 (105) 1.1 (57) 1.5 (35) ** 1.3 (197) Other (non-sti) indications> 1.4 (102) 1.4 (71) 1.5 (36) 1.4 (209) Unknown indication> 8.9 (663) 5.8 (288) 8.4 (197) ** 7.8 (1148) Any antibiotic agent reported 4.5 (331) 2.2 (109) 4.3 (101) ** 3.7 (541) Antibiotic use per named agent/class@ Doxycycline 0.6 (39) 0.4 (20) 0.8 (18) 0.5 (77) Azitromycine 0.4 (28) 0.4 (17) 0.6 (12) 0.4 (57) Ofloxacin 0.1 (4) 0.1 (4) 0 (0) 0.1 (8) Amoxicillin 1.1 (76) 0.7 (31) 1.5 (33) ** 1.0 (140) Erythromycin 0.1 (4) 0 (0) 0 (0) 0 (4) Ceftriaxon 0 (1) 0 (1) 0.2 (5) ** 0.1 (7) Ciprofloxacin 0.2 (12) 0.2 (9) 0.3 (6) 0.2 (27)
20 Any Tetracyclines 0.8 (50) 0.5 (23) 1.2 (26) ** 0.7 (99) Any Macrolides 0.6 (38) 0.4 (19) 0.6 (12) 0.5 (69) Any Quinolones 0.4 (24) 0.4 (18) 0.3 (7) 0.3 (49) Any Cephalsporins 0 (3) 0 (1) 0.4 (8) ** 0.1 (12) Any Penicillins 1.7 (112) 0.9 (44) 2.0 (44) ** 1.5 (200) Nitrofurantoin/trimethoprim/fosfomycin 1.5 (100) 0.1 (3) 0.1 (2) ** 0.8 (105) Other# 0.6 (37) 0.2 (9) 0.3 (7) * 0.4 (53) *p<0.05;**p<0.01 indicates Chi-square test on the difference between women, heterosexual men and MSM (for age; nonparametric test) $ including genital, anorectal and/or oral diagnosis at current consultation & denominator includes only the tested individuals ~HIV diagnosed at current consultation or known HIV more than 1 agent could be named during a consultation # mainly metronidazole and (some) clindamycin Downloaded from on July 17, 2018 by guest
21 Table 2: Proportion of Chlamydia trachomatis (Ct) and Neisseria gonorrhea (Ng) positive screening diagnoses and association with preceding use of antibiotics; for a total of STI clinic consultations Ct Univariate OR^ Adj.$ OR^ Ng Univariate OR^ Adj.$ OR^ % (n) 95% CI 95% CI % (n) 95% CI 95% CI WOMEN No antibiotic use (n=6320) 10.6 (667) (67) 1 1 Antibiotic use (n=1099) 11.0 (121) 1.05 ( ) 1.09 ( ) 1.4 (15) 1.29 ( ) 1.23 ( ) HETEROSEXUAL MEN No antibiotic use (n=4579) 12.1 (556) (48) 1 1 Antibiotic use (n=428) 8.6 (37) 0.69 ( )* 0.76 ( ) 0.9 (4) 0.93 ( ) 0.83 ( ) MSM No antibiotic use (n=2075) 9.7 (201) (132) 1 1 Antibiotic use (n=274) 5.5 (15) 0.54 ( )* 0.49 ( )* 6.6 (18) 1.04 ( ) 0.91 ( ) *P<0.05 $ adjusted for age and HIV status ^ risk estimates for the total group were not presented since Ct estimates significantly differed between women and heterosexual men (p interaction=0.039) and between women and MSM (p interaction 0.024). For Ng the risk estimates did not differ between sexual orientation groups and the overall univariate OR: 1.09, 95% CI: Analyses accounted for repeated measurements.
22 Table 3: Proportion of Ct and Ng positive screening diagnoses and association with preceding use of specific agents of antibiotics; for a total of STI clinic consultations Ct Univariate OR^ Adj.$ OR^ Ng Univariate OR^ Adj.$ OR^ % (n) 95% CI 95% CI % (n) 95% CI 95% CI Doxycycline No (n=13438) 10.9 (1467) (254) 1 1 Yes (n=77) 3.9 (3) 0.33 ( )# 0.37 ( ) 3.9 (3) 2.10 ( ) 1.19 ( ) Azythromycin No (n=13458) 10.9 (1461) (256) 1 1 Yes (n=57) 15.8 (9) 1.54 ( ) 1.62 ( ) 1.8 (1) 0.92 ( ) 0.69 ( ) Amoxicillin No (n=13375) 10.9 (1458) (255) 1 1 Yes (n=140) 8.6 (12) 0.77 ( ) 0.81 ( ) 1.4 (2) 0.75 ( ) 0.54 ( ) Any Tetracyclines No (n=13416) 10.9 (1467) (254) 1 1 Yes (n=99) 3.0 (3) 0.26 ( )* 0.29 ( )* 3.0 (3) 1.62 ( ) 0.95 ( ) Any Macrolides No (n=13446) 10.9 (1461) (256) 1 1 Yes (n=69) 13.0 (9)) 1.23 ( ) 1.29 ( ) 1.4 (1) 0.76 ( ) 0.63 ( ) Any Quinolones
23 No (n=13466) 10.8 (1461) (254)) 1 1 Yes (n=49) 18.4 (9) 1.85 ( ) 2.11 ( )* 6.1 (3) 3.39 ( )* 3.16 ( ) Any Cephalsporins No (n=13503) 10.9 (1469) (257) na na Yes (n=12) 8.3 (1) 0.75 ( ) 0.68 ( ) 0 (0) Any Penicillins No (n=13315) 10.9 (1455) (254) 1 1 Yes (n=200) 7.0 (15) 0.66 ( ) 0.70 ( ) 1.5 (3) 0.78 ( ) 0.64 ( ) Nitrofurantoin/trimethoprim/fosfomycin No (n=13410) 10.9 (1460) (255) 1 1 Yes (n=105) 9.5 (10) 0.86 ( ) 1.91 ( ) 1.9 (2) 1.00 ( ) 1.71 ( ) #p<0.10; *p<0.05 $ adjusted for age, HIV status, gender and sexual orientation ^ risk estimates for the total group were presented as estimates; they did not significantly differ between women, heterosexual men and MSM (p interaction > 0.05). Analyses accounted for repeated measurements.
24
25
The Threat of Multidrug Resistant Neisseria gonorrhoeae
 The Threat of Multidrug Resistant Neisseria gonorrhoeae Peel Public Health Symposium Sex, Drugs, and. Vanessa Allen, MD MPH October 16, 2012 The threat of multidrug resistant gonorrhea "We're sitting on
The Threat of Multidrug Resistant Neisseria gonorrhoeae Peel Public Health Symposium Sex, Drugs, and. Vanessa Allen, MD MPH October 16, 2012 The threat of multidrug resistant gonorrhea "We're sitting on
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007
 Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Updated recommended treatment regimens for gonococcal infections and associated conditions United States, April 2007 1 Ongoing data from CDC 's Gonococcal Isolate Surveillance Project (GISP), including
Does flagyl treat gonorrhea and chlamydia
 Does flagyl treat gonorrhea and chlamydia The Borg System is 100 % Does flagyl treat gonorrhea and chlamydia Mild Chlamydia infection, limited to the cervix, can be treated with a single dose of an antibiotic
Does flagyl treat gonorrhea and chlamydia The Borg System is 100 % Does flagyl treat gonorrhea and chlamydia Mild Chlamydia infection, limited to the cervix, can be treated with a single dose of an antibiotic
Monitoring gonococcal antimicrobial susceptibility
 Monitoring gonococcal antimicrobial susceptibility The rapidly changing antimicrobial susceptibility of Neisseria gonorrhoeae has created an important public health problem. Because of widespread resistance
Monitoring gonococcal antimicrobial susceptibility The rapidly changing antimicrobial susceptibility of Neisseria gonorrhoeae has created an important public health problem. Because of widespread resistance
Sexually Transmitted Disease Surveillance 2012:
 Sexually Transmitted Disease Surveillance 212: Gonococcal Isolate Surveillance Project (GISP) Supplement & Profiles Division of STD Prevention February 214 U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Sexually Transmitted Disease Surveillance 212: Gonococcal Isolate Surveillance Project (GISP) Supplement & Profiles Division of STD Prevention February 214 U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Tandan, Meera; Duane, Sinead; Vellinga, Akke.
 Provided by the author(s) and NUI Galway in accordance with publisher policies. Please cite the published version when available. Title Do general practitioners prescribe more antimicrobials when the weekend
Provided by the author(s) and NUI Galway in accordance with publisher policies. Please cite the published version when available. Title Do general practitioners prescribe more antimicrobials when the weekend
ESAC s Surveillance by Point Prevalence Measurements. by author
 ESAC s Surveillance by Point Prevalence Measurements Herman Goossens, MD, PhD ESAC Co-ordinator VAXINFECTIO, Laboratory of Medical Microbiology University of Antwerp, Belgium Outline Background Point Prevalence
ESAC s Surveillance by Point Prevalence Measurements Herman Goossens, MD, PhD ESAC Co-ordinator VAXINFECTIO, Laboratory of Medical Microbiology University of Antwerp, Belgium Outline Background Point Prevalence
Tubo-ovarian abscess in OPAT
 Tubo-ovarian abscess in OPAT James Hatcher Consultant in Infectious Diseases and Medical Microbiology OUTLINE What is a tubo-ovarian abscess Current recommendations Our experience and challenges How to
Tubo-ovarian abscess in OPAT James Hatcher Consultant in Infectious Diseases and Medical Microbiology OUTLINE What is a tubo-ovarian abscess Current recommendations Our experience and challenges How to
Women s Antimicrobial Guidelines Summary
 Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
Women s Antimicrobial Guidelines Summary 1. Introduction and Who Guideline applies to This guideline has been developed to deliver safe and appropriate empirical use of antibiotics for patients at University
European Antibiotic Awareness Day
 Initiating a pan-european health campaign - experiences from setting up the European Antibiotic Awareness Day Dr Ülla-Karin Nurm Head of Public Health Development Section, Public Health Capacity and Communication
Initiating a pan-european health campaign - experiences from setting up the European Antibiotic Awareness Day Dr Ülla-Karin Nurm Head of Public Health Development Section, Public Health Capacity and Communication
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings?
 An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
SEASONAL TRENDS IN ANTIBIOTIC USAGE AMONG PAEDIATRIC OUTPATIENTS
 SEASONAL TRENDS IN ANTIBIOTIC USAGE AMONG PAEDIATRIC OUTPATIENTS Edita Alili-Idrizi, Msc Merita Dauti, Msc State University of Tetovo, Faculty of Medicine, Department of Pharmacy, Tetovo, R. of Macedonia
SEASONAL TRENDS IN ANTIBIOTIC USAGE AMONG PAEDIATRIC OUTPATIENTS Edita Alili-Idrizi, Msc Merita Dauti, Msc State University of Tetovo, Faculty of Medicine, Department of Pharmacy, Tetovo, R. of Macedonia
Summary of the latest data on antibiotic consumption in the European Union
 Summary of the latest data on antibiotic consumption in the European Union ESAC-Net surveillance data November 2016 Provision of reliable and comparable national antimicrobial consumption data is a prerequisite
Summary of the latest data on antibiotic consumption in the European Union ESAC-Net surveillance data November 2016 Provision of reliable and comparable national antimicrobial consumption data is a prerequisite
Amoxicillin dosage for chlamydia
 Amoxicillin dosage for chlamydia Search 6-3-2018 Detailed Amoxicillin dosage information for adults and TEENren. Includes dosages for Urinary Tract Infection, Sinusitis, Bronchitis and more; plus renal.
Amoxicillin dosage for chlamydia Search 6-3-2018 Detailed Amoxicillin dosage information for adults and TEENren. Includes dosages for Urinary Tract Infection, Sinusitis, Bronchitis and more; plus renal.
Cephalosporins, Quinolones and Co-amoxiclav Prescribing Audit
 Cephalosporins, Quinolones and Co-amoxiclav Prescribing Audit Executive Summary Background Antibiotic resistance poses a significant threat to public health, as antibiotics underpin routine medical practice.
Cephalosporins, Quinolones and Co-amoxiclav Prescribing Audit Executive Summary Background Antibiotic resistance poses a significant threat to public health, as antibiotics underpin routine medical practice.
How is Ireland performing on antibiotic prescribing?
 European Antibiotic Awareness Campaign 2016 November Webinar Series on Antibiotic Prescribing How is Ireland performing on antibiotic prescribing? Dr Rob Cunney National Clinical Lead HCAI AMR Clinical
European Antibiotic Awareness Campaign 2016 November Webinar Series on Antibiotic Prescribing How is Ireland performing on antibiotic prescribing? Dr Rob Cunney National Clinical Lead HCAI AMR Clinical
Summary of the latest data on antibiotic consumption in the European Union
 Summary of the latest data on antibiotic consumption in the European Union November 2012 Highlights on antibiotic consumption Antibiotic use is one of the main factors responsible for the development and
Summary of the latest data on antibiotic consumption in the European Union November 2012 Highlights on antibiotic consumption Antibiotic use is one of the main factors responsible for the development and
Neisseria gonorrhoeae: Situation of antibiotic resistance
 Neisseria gonorrhoeae: Situation of antibiotic resistance Susanne Buder, Peter K. Kohl Konsiliarlaboratorium für Gonokokken Klinik für Dermatologie und Venerologie Vivantes Klinikum Neukölln, Berlin +
Neisseria gonorrhoeae: Situation of antibiotic resistance Susanne Buder, Peter K. Kohl Konsiliarlaboratorium für Gonokokken Klinik für Dermatologie und Venerologie Vivantes Klinikum Neukölln, Berlin +
Belgian National Antibiotic Awareness Campaigns
 Belgian National Antibiotic Awareness Campaigns Herman Goossens, Stijn De Corte, Samuel Coenen University of Antwerp and BAPCOC Joris Mateusen, Sarah Tulkens Absoluut Belgium Belgian National Antibiotic
Belgian National Antibiotic Awareness Campaigns Herman Goossens, Stijn De Corte, Samuel Coenen University of Antwerp and BAPCOC Joris Mateusen, Sarah Tulkens Absoluut Belgium Belgian National Antibiotic
MANAGEMENT OF PELVIC INFLAMMATORY DISEASE
 GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
GYNAECOLOGY SERVICES NORTH CUMBRIA MANAGEMENT OF PELVIC INFLAMMATORY DISEASE Author/Contact DOCUMENT CONTROL Lufti Shamsuddin, ST4 Obs & Gynae Trainee / Nalini Munjuluri, Consultant Gynaecology Tel: 01228
Best Practice Guidelines for Treatment of Uncomplicated UTIs in Women While Decreasing Risk of Antibiotic Resistance
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Antimicrobial use in humans
 Antimicrobial use in humans Ann Versporten Prof. Herman Goossens OIE Global Conference on the Responsible and Prudent Use of Antimicrobial Agents for Animals - 13 March 2013 - Ann.versporten@ua.ac.be Herman.goossens@uza.be
Antimicrobial use in humans Ann Versporten Prof. Herman Goossens OIE Global Conference on the Responsible and Prudent Use of Antimicrobial Agents for Animals - 13 March 2013 - Ann.versporten@ua.ac.be Herman.goossens@uza.be
Emerging cephalosporin and multidrug-resistant gonorrhoea in Europe
 Surveillance and outbreak reports Emerging cephalosporin and multidrug-resistant gonorrhoea in Europe M J Cole (michelle.cole@phe.gov.uk) 1, G Spiteri 2, S A Chisholm 2, S Hoffmann 3, C A Ison 1, M Unemo
Surveillance and outbreak reports Emerging cephalosporin and multidrug-resistant gonorrhoea in Europe M J Cole (michelle.cole@phe.gov.uk) 1, G Spiteri 2, S A Chisholm 2, S Hoffmann 3, C A Ison 1, M Unemo
Antibiotic Reference Laboratory, Institute of Environmental Science and Research Limited (ESR); August 2017
; August 2017") Antimicrobial susceptibility of Shigella, 2015 and 2016 Helen Heffernan and Rosemary Woodhouse Antibiotic Reference Laboratory, Institute of Environmental Science and Research Limited (ESR); August 2017
Antimicrobial susceptibility of Shigella, 2015 and 2016 Helen Heffernan and Rosemary Woodhouse Antibiotic Reference Laboratory, Institute of Environmental Science and Research Limited (ESR); August 2017
Troubling treatment failure against an emerging sexually transmitted infection
 CATIE-News CATIE s bite-sized HIV and hepatitis C news bulletins. Troubling treatment failure against an emerging sexually transmitted infection 10 October 2013 The bacterium Mycoplasma genitalium (MG)
CATIE-News CATIE s bite-sized HIV and hepatitis C news bulletins. Troubling treatment failure against an emerging sexually transmitted infection 10 October 2013 The bacterium Mycoplasma genitalium (MG)
The UK 5-year AMR Strategy - a brief overview - Dr Berit Muller-Pebody National Infection Service Public Health England
 The UK 5-year AMR Strategy - a brief overview - Dr Berit Muller-Pebody National Infection Service Public Health England Chief Medical Officer - Annual Report 2013 Antimicrobial resistance poses catastrophic
The UK 5-year AMR Strategy - a brief overview - Dr Berit Muller-Pebody National Infection Service Public Health England Chief Medical Officer - Annual Report 2013 Antimicrobial resistance poses catastrophic
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Received: Accepted: Access this article online Website: Quick Response Code:
 Indian Journal of Drugs, 2016, 4(3), 69-74 ISSN: 2348-1684 STUDY ON UTILIZATION PATTERN OF ANTIBIOTICS AT A PRIVATE CORPORATE HOSPITAL B. Chitra Department of Pharmacy Practice, College of Pharmacy, Sri
Indian Journal of Drugs, 2016, 4(3), 69-74 ISSN: 2348-1684 STUDY ON UTILIZATION PATTERN OF ANTIBIOTICS AT A PRIVATE CORPORATE HOSPITAL B. Chitra Department of Pharmacy Practice, College of Pharmacy, Sri
Volume 1; Number 7 November 2007
 Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Prior antibiotics and risk of antibiotic-resistant community-acquired urinary tract infection: a case control study
 Journal of Antimicrobial Chemotherapy (2007) 60, 92 99 doi:10.1093/jac/dkm141 Advance Access publication 30 May 2007 Prior antibiotics and risk of antibiotic-resistant community-acquired urinary tract
Journal of Antimicrobial Chemotherapy (2007) 60, 92 99 doi:10.1093/jac/dkm141 Advance Access publication 30 May 2007 Prior antibiotics and risk of antibiotic-resistant community-acquired urinary tract
Antimicrobial practice. Laboratory antibiotic susceptibility reporting and antibiotic prescribing in general practice
 Journal of Antimicrobial Chemotherapy (2003) 51, 379 384 DOI: 10.1093/jac/dkg032 Advance Access publication 6 January 2003 Antimicrobial practice Laboratory antibiotic susceptibility reporting and antibiotic
Journal of Antimicrobial Chemotherapy (2003) 51, 379 384 DOI: 10.1093/jac/dkg032 Advance Access publication 6 January 2003 Antimicrobial practice Laboratory antibiotic susceptibility reporting and antibiotic
What is the problem? Latest data on antibiotic resistance
 European Antibiotic Awareness Day 2009 What is the problem? Latest data on antibiotic resistance Zsuzsanna Jakab, ECDC Director Launch Seminar for EAAD Stockholm, 18 November 2009 Fluoroquinolone-resistant
European Antibiotic Awareness Day 2009 What is the problem? Latest data on antibiotic resistance Zsuzsanna Jakab, ECDC Director Launch Seminar for EAAD Stockholm, 18 November 2009 Fluoroquinolone-resistant
ANTIBIOTIC USE GUIDELINES FOR URINARY TRACT AND RESPIRATORY DISEASE
 ANTIBIOTIC USE GUIDELINES FOR URINARY TRACT AND RESPIRATORY DISEASE Jane Sykes, BVSc(Hons), PhD, DACVIM (SAIM) School of Veterinary Medicine Dept. of Medicine & Epidemiology University of California Davis,
ANTIBIOTIC USE GUIDELINES FOR URINARY TRACT AND RESPIRATORY DISEASE Jane Sykes, BVSc(Hons), PhD, DACVIM (SAIM) School of Veterinary Medicine Dept. of Medicine & Epidemiology University of California Davis,
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Stewardship in Ambulatory Care
 Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Executive Summary: A Point Prevalence Survey of Antimicrobial Use: Benchmarking and Patterns of Use to Support Antimicrobial Stewardship Efforts
 Executive Summary: A Point Prevalence Survey of Antimicrobial Use: Benchmarking and Patterns of Use to Support Antimicrobial Stewardship Efforts Investigational Team: Diane Brideau-Laughlin BSc(Pharm),
Executive Summary: A Point Prevalence Survey of Antimicrobial Use: Benchmarking and Patterns of Use to Support Antimicrobial Stewardship Efforts Investigational Team: Diane Brideau-Laughlin BSc(Pharm),
running head: SUPERBUGS Humphreys 1
 running head: SUPERBUGS Humphreys 1 Superbugs GCH 360 Term Paper Assignment Kelly Humphreys April 30, 2014 SUPERBUGS Humphreys 2 Introduction The World Health Organization (WHO) recognizes antibiotic resistance
running head: SUPERBUGS Humphreys 1 Superbugs GCH 360 Term Paper Assignment Kelly Humphreys April 30, 2014 SUPERBUGS Humphreys 2 Introduction The World Health Organization (WHO) recognizes antibiotic resistance
Quelle politique antibiotique pour l Europe? Dominique L. Monnet
 Quelle politique antibiotique pour l Europe? Dominique L. Monnet National Center for Antimicrobials & Infection Control Statens Serum Institut, Copenhagen, Denmark Opinion of the Section for Protection
Quelle politique antibiotique pour l Europe? Dominique L. Monnet National Center for Antimicrobials & Infection Control Statens Serum Institut, Copenhagen, Denmark Opinion of the Section for Protection
Clinical and Economic Impact of Urinary Tract Infections Caused by Escherichia coli Resistant Isolates
 Clinical and Economic Impact of Urinary Tract Infections Caused by Escherichia coli Resistant Isolates Katia A. ISKANDAR Pharm.D, MHS, AMES, PhD candidate Disclosure Katia A. ISKANDAR declare to meeting
Clinical and Economic Impact of Urinary Tract Infections Caused by Escherichia coli Resistant Isolates Katia A. ISKANDAR Pharm.D, MHS, AMES, PhD candidate Disclosure Katia A. ISKANDAR declare to meeting
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Table 2.01 Overview of Surveillance programs in the Netherlands. available since. GP, laboratories Decentral Hospital,
 2 Extensive summary In the Netherlands, several surveillance programs have been developed to monitor antimicrobial resistance in important pathogens in different settings (SERIN, SIRIN, ISIS- AR). In addition,
2 Extensive summary In the Netherlands, several surveillance programs have been developed to monitor antimicrobial resistance in important pathogens in different settings (SERIN, SIRIN, ISIS- AR). In addition,
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
9/30/2016. Dr. Janell Mayer, Pharm.D., CGP, BCPS Dr. Lindsey Votaw, Pharm.D., CGP, BCPS
 Dr. Janell Mayer, Pharm.D., CGP, BCPS Dr. Lindsey Votaw, Pharm.D., CGP, BCPS 1 2 Untoward Effects of Antibiotics Antibiotic resistance Adverse drug events (ADEs) Hypersensitivity/allergy Drug side effects
Dr. Janell Mayer, Pharm.D., CGP, BCPS Dr. Lindsey Votaw, Pharm.D., CGP, BCPS 1 2 Untoward Effects of Antibiotics Antibiotic resistance Adverse drug events (ADEs) Hypersensitivity/allergy Drug side effects
Chris R. Kenyon 1,2, Irith De Baetselier 1, Tania Crucitti 1
 RESEARCH ARTICLE Does gonorrhoea screening intensity play a role in the early selection of antimicrobial resistance in men who have sex with men (MSM)? A comparative study of Belgium and the United Kingdom
RESEARCH ARTICLE Does gonorrhoea screening intensity play a role in the early selection of antimicrobial resistance in men who have sex with men (MSM)? A comparative study of Belgium and the United Kingdom
Quality indicators and outcomes in the devolved nations Scotland
 Quality indicators and outcomes in the devolved nations Scotland Dr Jacqueline Sneddon, MRPharmS Project Lead, Scottish Antimicrobial Prescribing Group Federation of Infection Societies Conference Birmingham,
Quality indicators and outcomes in the devolved nations Scotland Dr Jacqueline Sneddon, MRPharmS Project Lead, Scottish Antimicrobial Prescribing Group Federation of Infection Societies Conference Birmingham,
Practical application of antibiotic use data. Uga Dumpis MD PhD Pauls Stradins Clinical University Hospital University of Latvia
 Practical application of antibiotic use data Uga Dumpis MD PhD Pauls Stradins Clinical University Hospital University of Latvia No conflict of interest Questions for the ACASEM Survey Question 1. Antimicrobial
Practical application of antibiotic use data Uga Dumpis MD PhD Pauls Stradins Clinical University Hospital University of Latvia No conflict of interest Questions for the ACASEM Survey Question 1. Antimicrobial
Overview of C. difficile infections. Kurt B. Stevenson, MD MPH Professor Division of Infectious Diseases
 Overview of C. difficile infections Kurt B. Stevenson, MD MPH Professor Division of Infectious Diseases Conflicts of Interest I have no financial conflicts of interest related to this topic and presentation.
Overview of C. difficile infections Kurt B. Stevenson, MD MPH Professor Division of Infectious Diseases Conflicts of Interest I have no financial conflicts of interest related to this topic and presentation.
Update on Fluoroquinolones. Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO
 Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Swedish strategies and methods to combat antibiotic resistance
 Swedish strategies and methods to combat antibiotic resistance Stephan Stenmark MD, PhD, County Medical Officer Västerbotten County Council, Sweden Head of Department for communicable disease control and
Swedish strategies and methods to combat antibiotic resistance Stephan Stenmark MD, PhD, County Medical Officer Västerbotten County Council, Sweden Head of Department for communicable disease control and
The Australian Gonococcal Surveillance Programme
 The Australian Gonococcal Surveillance Programme 1979 2017 Monica M Lahra A,B,F, CR Robert George A,C and David M Whiley D,E A WHO Collaborating Centre for STD, Microbiology Department, New South Wales
The Australian Gonococcal Surveillance Programme 1979 2017 Monica M Lahra A,B,F, CR Robert George A,C and David M Whiley D,E A WHO Collaborating Centre for STD, Microbiology Department, New South Wales
Protocol for Surveillance of Antimicrobial Resistance in Urinary Isolates in Scotland
 Protocol for Surveillance of Antimicrobial Resistance in Urinary Isolates in Scotland Version 1.0 23 December 2011 General enquiries and contact details This is the first version (1.0) of the Protocol
Protocol for Surveillance of Antimicrobial Resistance in Urinary Isolates in Scotland Version 1.0 23 December 2011 General enquiries and contact details This is the first version (1.0) of the Protocol
Lyme disease: diagnosis and management
 National Institute for Health and Care Excellence Final Lyme disease: diagnosis and management [D] Evidence review for the management of erythema migrans NICE guideline 95 Evidence review April 2018 Final
National Institute for Health and Care Excellence Final Lyme disease: diagnosis and management [D] Evidence review for the management of erythema migrans NICE guideline 95 Evidence review April 2018 Final
Cork and Kerry SARI Newsletter; Vol. 2 (2), December 2006
, December 2006") Cork and SARI Newsletter; Vol. 2 (2), December 6 Item Type Newsletter Authors Murray, Deirdre;O'Connor, Nuala;Condon, Rosalind Download date 31/1/18 15:27:31 Link to Item http://hdl.handle.net/1147/67296
Cork and SARI Newsletter; Vol. 2 (2), December 6 Item Type Newsletter Authors Murray, Deirdre;O'Connor, Nuala;Condon, Rosalind Download date 31/1/18 15:27:31 Link to Item http://hdl.handle.net/1147/67296
WORKSHOP 6 Towards European consensus indications for major antibiotic classes: an exercise with the macrolides. Objectives
 Objectives To establish the basic pharmacokinetic properties and safety profile of predefined macrolides. To make an inventory of the intrinsic susceptibilities of pathogenic organisms towards macrolides
Objectives To establish the basic pharmacokinetic properties and safety profile of predefined macrolides. To make an inventory of the intrinsic susceptibilities of pathogenic organisms towards macrolides
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process High Priority
 MEASURE TYPE: Process High Priority") Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction Meaningful Measure Area: Appropriate
Quality ID #65 (NQF 0069): Appropriate Treatment for Children with Upper Respiratory Infection (URI) National Quality Strategy Domain: Efficiency and Cost Reduction Meaningful Measure Area: Appropriate
Measure Information Form
 Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Antimicrobial Stewardship Programs The Same, but Different. Sara Nausheen, MD Kevin Kern, PharmD
 Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
$100 $200 $300 $400 $500
 Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Skin is In Runny Noses Got to go! Hear no evil It s in the Lungs $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500 Double Jeopardy
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
ANTIMICROBIAL STEWARDSHIP IN PRIMARY HEALTH CARE WESTERN CAPE GOVERNMENT: HEALTH METRO DISTRICT FINDINGS 6 MONTHS AFTER INITIATION
 ANTIMICROBIAL STEWARDSHIP IN PRIMARY HEALTH CARE WESTERN CAPE GOVERNMENT: HEALTH METRO DISTRICT FINDINGS 6 MONTHS AFTER INITIATION 2018 IHI Africa Forum for Quality and Safety in Healthcare Bart Willems,
ANTIMICROBIAL STEWARDSHIP IN PRIMARY HEALTH CARE WESTERN CAPE GOVERNMENT: HEALTH METRO DISTRICT FINDINGS 6 MONTHS AFTER INITIATION 2018 IHI Africa Forum for Quality and Safety in Healthcare Bart Willems,
Marc Decramer 3. Respiratory Division, University Hospitals Leuven, Leuven, Belgium
 AAC Accepts, published online ahead of print on April 0 Antimicrob. Agents Chemother. doi:./aac.0001- Copyright 0, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.
AAC Accepts, published online ahead of print on April 0 Antimicrob. Agents Chemother. doi:./aac.0001- Copyright 0, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.
Barriers to Intravenous Penicillin Use for Treatment of Nonmeningitis
 JCM Accepts, published online ahead of print on 7 July 2010 J. Clin. Microbiol. doi:10.1128/jcm.01012-10 Copyright 2010, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
JCM Accepts, published online ahead of print on 7 July 2010 J. Clin. Microbiol. doi:10.1128/jcm.01012-10 Copyright 2010, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
Inappropriate Use of Antibiotics and Clostridium difficile Infection. Jocelyn Srigley, MD, FRCPC November 1, 2012
 Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Inappropriate Use of Antibiotics and Clostridium difficile Infection Jocelyn Srigley, MD, FRCPC November 1, 2012 Financial Disclosures } No conflicts of interest } The study was supported by a Hamilton
Preventing and Responding to Antibiotic Resistant Infections in New Hampshire
 Preventing and Responding to Antibiotic Resistant Infections in New Hampshire Benjamin P. Chan, MD, MPH NH Dept. of Health & Human Services Division of Public Health Services May 23, 2017 To bring a greater
Preventing and Responding to Antibiotic Resistant Infections in New Hampshire Benjamin P. Chan, MD, MPH NH Dept. of Health & Human Services Division of Public Health Services May 23, 2017 To bring a greater
POINT PREVALENCE SURVEY A tool for antibiotic stewardship in hospitals. Koen Magerman Working group Hospital Medicine
 POINT PREVALENCE SURVEY A tool for antibiotic stewardship in hospitals Koen Magerman Working group Hospital Medicine Background Strategic plan By means of a point prevalence survey and internal audits
POINT PREVALENCE SURVEY A tool for antibiotic stewardship in hospitals Koen Magerman Working group Hospital Medicine Background Strategic plan By means of a point prevalence survey and internal audits
A Point Prevalence Survey of Antibiotic Prescriptions and Infection in Sanandaj Hospitals, Prospects for Antibiotic Stewardship
 A Point Prevalence Survey of Antibiotic Prescriptions and Infection in Sanandaj Hospitals, Prospects for Antibiotic Stewardship Jafar Soltani* Ann Versporten**, Behzad Mohsenpour*, Herman Goossen**, Soheila
A Point Prevalence Survey of Antibiotic Prescriptions and Infection in Sanandaj Hospitals, Prospects for Antibiotic Stewardship Jafar Soltani* Ann Versporten**, Behzad Mohsenpour*, Herman Goossen**, Soheila
Local Action from Integrated Data: Presentation of Laboratory Test Result Data for Informed Management of Sexually Transmitted Infections
 Local Action from Integrated Data: Presentation of Laboratory Test Result Data for Informed Management of Sexually Transmitted Infections LabWare CEC Conference May 22, 2014 Lost Pines, Texas Jim Tom,
Local Action from Integrated Data: Presentation of Laboratory Test Result Data for Informed Management of Sexually Transmitted Infections LabWare CEC Conference May 22, 2014 Lost Pines, Texas Jim Tom,
Urinary Tract Infection Workshop
 Urinary Tract Infection Workshop Diagnosis, sampling, antibiotic selection, recurrence, prophylaxis Nick Francis, Robin Howe, Harry Ahmed Outline Diagnosis and sampling Nick 10 min Choice of antibiotic
Urinary Tract Infection Workshop Diagnosis, sampling, antibiotic selection, recurrence, prophylaxis Nick Francis, Robin Howe, Harry Ahmed Outline Diagnosis and sampling Nick 10 min Choice of antibiotic
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Antibiotic resistance and prescribing in Australia: current attitudes and practice of GPs
 CSIRO PUBLISHING Healthcare Infection, 2013, 18, 147 151 http://dx.doi.org/10.1071/hi13019 Antibiotic resistance and prescribing in Australia: current attitudes and practice of GPs Rachel Hardy-Holbrook
CSIRO PUBLISHING Healthcare Infection, 2013, 18, 147 151 http://dx.doi.org/10.1071/hi13019 Antibiotic resistance and prescribing in Australia: current attitudes and practice of GPs Rachel Hardy-Holbrook
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Dr Eleri Davies. Consultant Microbiologist and Infection Control Doctor, Public Health Wales NHS Trust
 Dr Eleri Davies Consultant Microbiologist and Infection Control Doctor, Public Health Wales NHS Trust Antimicrobial stewardship What is it? Why is it important? Treatment and management of catheter-associated
Dr Eleri Davies Consultant Microbiologist and Infection Control Doctor, Public Health Wales NHS Trust Antimicrobial stewardship What is it? Why is it important? Treatment and management of catheter-associated
Responsible use of antibiotics
 Responsible use of antibiotics Uga Dumpis MD, PhD Department of Infectious Diseases and Infection Control Pauls Stradiņs Clinical University Hospital Challenges in the hospitals Antibiotics are still effective
Responsible use of antibiotics Uga Dumpis MD, PhD Department of Infectious Diseases and Infection Control Pauls Stradiņs Clinical University Hospital Challenges in the hospitals Antibiotics are still effective
Sommer. Memorial. Lectures
 When do the costs of using antibiotics outweigh the benefits? Lecture: May 11 2018 Established risks of antibiotic use Source: CDC British Journal of Experimental Pathology 1929;79:780. J Clin Invest
When do the costs of using antibiotics outweigh the benefits? Lecture: May 11 2018 Established risks of antibiotic use Source: CDC British Journal of Experimental Pathology 1929;79:780. J Clin Invest
HSE - Health Protection Surveillance Centre Surveillance of Antimicrobial Consumption in Ireland
 Surveillance of Antimicrobial Consumption in Ireland Ajay Oza A European Study on the Relationship between Antimicrobial Use and Antimicrobial Resistance (1998-1999) Bronzwaer et al 2002 Emerging Infectious
Surveillance of Antimicrobial Consumption in Ireland Ajay Oza A European Study on the Relationship between Antimicrobial Use and Antimicrobial Resistance (1998-1999) Bronzwaer et al 2002 Emerging Infectious
REPORT ON POINT PREVALENCE SURVEY OF ANTIMICROBIAL PRESCRIPTION IN EUROPEAN NURSING HOMES, November 2009
 REPORT ON POINT PREVALENCE SURVEY OF ANTIMICROBIAL PRESCRIPTION IN EUROPEAN NURSING HOMES, November 29 ESAC-3: Nursing Home Subproject Group Broex E, Jans B, Latour K, Goossens H and the ESAC management
REPORT ON POINT PREVALENCE SURVEY OF ANTIMICROBIAL PRESCRIPTION IN EUROPEAN NURSING HOMES, November 29 ESAC-3: Nursing Home Subproject Group Broex E, Jans B, Latour K, Goossens H and the ESAC management
Can i take diflucan with antibiotics
 Can i take diflucan with antibiotics Search Taking Diflucan while on antibiotics. If you re taking the antibiotics to cure a urinary tract infection then there s no reason to take them for a UTI. You can.
Can i take diflucan with antibiotics Search Taking Diflucan while on antibiotics. If you re taking the antibiotics to cure a urinary tract infection then there s no reason to take them for a UTI. You can.
Treatment of Sexually Transmitted Infections. Wolverton Centre Guidelines
 Treatment of Sexually Transmitted Infections Wolverton Centre Guidelines Updated Jan 2018 Please ensure that you have the latest version. V: Department Folder/Standard Operating Guides/Clinical Governance/Treatment
Treatment of Sexually Transmitted Infections Wolverton Centre Guidelines Updated Jan 2018 Please ensure that you have the latest version. V: Department Folder/Standard Operating Guides/Clinical Governance/Treatment
English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR)
") English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Berit Muller-Pebody HCAI & AMR Department, Centre for Infectious Disease Surveillance and Control Chief Medical Officer
English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Berit Muller-Pebody HCAI & AMR Department, Centre for Infectious Disease Surveillance and Control Chief Medical Officer
Antibiotic Stewardship in the LTC Setting
 Antibiotic Stewardship in the LTC Setting Joe Litsey, Director of Consulting Services Pharm.D., Board Certified Geriatric Pharmacist Thrifty White Pharmacy Objectives Describe the Antibiotic Stewardship
Antibiotic Stewardship in the LTC Setting Joe Litsey, Director of Consulting Services Pharm.D., Board Certified Geriatric Pharmacist Thrifty White Pharmacy Objectives Describe the Antibiotic Stewardship
TRENDS IN ANTI-INFECTIVE DRUGS USE DURING PREGNANCY
 TRENDS IN ANTI-INFECTIVE DRUGS USE DURING PREGNANCY Fabiano Santos 1,2, Odile Sheehy 2, Sylvie Perreault 1, Ema Ferreira 1,2, Anick Bérard 1,2 1 Faculty of Pharmacy, University of Montreal, Montreal, Quebec,
TRENDS IN ANTI-INFECTIVE DRUGS USE DURING PREGNANCY Fabiano Santos 1,2, Odile Sheehy 2, Sylvie Perreault 1, Ema Ferreira 1,2, Anick Bérard 1,2 1 Faculty of Pharmacy, University of Montreal, Montreal, Quebec,
Antimicrobial Resistance Update for Community Health Services
 Antimicrobial Resistance Update for Community Health Services Elizabeth Beech Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England October 2015 elizabeth.beech@nhs.net Superbugs
Antimicrobial Resistance Update for Community Health Services Elizabeth Beech Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England October 2015 elizabeth.beech@nhs.net Superbugs
OBSTETRICS & GYNAECOLOGY. Penicillin G 5 million units IV ; followed by 2.5 million units 4hourly upto delivery
 OBSTETRICS & GYNAECOLOGY A.OBSTETRICS Infection/Condition/likely organism Intrapartum Group B Streptococcal (GBS) infection; positive mothers Suggested treatment Preferred Penicillin G 5 million units
OBSTETRICS & GYNAECOLOGY A.OBSTETRICS Infection/Condition/likely organism Intrapartum Group B Streptococcal (GBS) infection; positive mothers Suggested treatment Preferred Penicillin G 5 million units
Antimicrobial Resistance (2013)
") Antimicrobial Resistance (2013) In the second half of 2013, the NIHR issued a call for research into the evaluation of public health measures, health care interventions and health services to reduce the
Antimicrobial Resistance (2013) In the second half of 2013, the NIHR issued a call for research into the evaluation of public health measures, health care interventions and health services to reduce the
Lack of Change in Susceptibility of Pseudomonas aeruginosa in a Pediatric Hospital Despite Marked Changes in Antibiotic Utilization
 Infect Dis Ther (2014) 3:55 59 DOI 10.1007/s40121-014-0028-8 BRIEF REPORT Lack of Change in Susceptibility of Pseudomonas aeruginosa in a Pediatric Hospital Despite Marked Changes in Antibiotic Utilization
Infect Dis Ther (2014) 3:55 59 DOI 10.1007/s40121-014-0028-8 BRIEF REPORT Lack of Change in Susceptibility of Pseudomonas aeruginosa in a Pediatric Hospital Despite Marked Changes in Antibiotic Utilization
UTI Dr S Mathijs Department of Pharmacology
 UTI Dr S Mathijs Department of Pharmacology Introduction Responsible for > 7 million consultations annually 15% of all antibiotic prescriptions 40% of all hospital acquired infections Significant burden
UTI Dr S Mathijs Department of Pharmacology Introduction Responsible for > 7 million consultations annually 15% of all antibiotic prescriptions 40% of all hospital acquired infections Significant burden
The Perils of Mixing Warfarin & Antibiotics: A Potentially Deadly Combination
 The Perils of Mixing Warfarin & Antibiotics: A Potentially Deadly Combination Lynn McNicoll, MD, FRCPC, AGSF Associate Professor of Medicine, Department of Medicine Warren Alpert Medical School of Brown
The Perils of Mixing Warfarin & Antibiotics: A Potentially Deadly Combination Lynn McNicoll, MD, FRCPC, AGSF Associate Professor of Medicine, Department of Medicine Warren Alpert Medical School of Brown
Antimicrobial Susceptibility Patterns of Salmonella Typhi From Kigali,
 In the name of God Shiraz E-Medical Journal Vol. 11, No. 3, July 2010 http://semj.sums.ac.ir/vol11/jul2010/88030.htm Antimicrobial Susceptibility Patterns of Salmonella Typhi From Kigali, Rwanda. Ashok
In the name of God Shiraz E-Medical Journal Vol. 11, No. 3, July 2010 http://semj.sums.ac.ir/vol11/jul2010/88030.htm Antimicrobial Susceptibility Patterns of Salmonella Typhi From Kigali, Rwanda. Ashok
Antimicrobial consumption
 Antimicrobial consumption Annual Epidemiological Report for 2017 Key facts Twenty-seven countries, comprising 25 EU Member States and two EEA countries (Iceland and Norway) reported data on antimicrobial
Antimicrobial consumption Annual Epidemiological Report for 2017 Key facts Twenty-seven countries, comprising 25 EU Member States and two EEA countries (Iceland and Norway) reported data on antimicrobial
Study Protocol. Funding: German Center for Infection Research (TTU-HAARBI, Research Clinical Unit)
") Effectiveness of antibiotic stewardship interventions in reducing the rate of colonization and infections due to antibiotic resistant bacteria and Clostridium difficile in hospital patients a systematic
Effectiveness of antibiotic stewardship interventions in reducing the rate of colonization and infections due to antibiotic resistant bacteria and Clostridium difficile in hospital patients a systematic
Vaccine Evaluation Center, BC Children s Hospital Research Institute, 950 West 28 th Ave,
 Manuscript Click here to view linked References Age-specific trends in antibiotic resistance in Escherichia coli infections in Oxford, United Kingdom 2013-2014 Rebecca C Robey a, Simon B Drysdale b,c,
Manuscript Click here to view linked References Age-specific trends in antibiotic resistance in Escherichia coli infections in Oxford, United Kingdom 2013-2014 Rebecca C Robey a, Simon B Drysdale b,c,
ANTHRAX. INHALATION, INTESTINAL and CUTANEOUS ANTHRAX
 INHALATION, INTESTINAL and CUTANEOUS ANTHRAX CPMP/4048/01, rev. 3 1/7 General points on treatment Anthrax is an acute infectious disease caused by Bacillus anthracis, that may be infecting man via cutaneous
INHALATION, INTESTINAL and CUTANEOUS ANTHRAX CPMP/4048/01, rev. 3 1/7 General points on treatment Anthrax is an acute infectious disease caused by Bacillus anthracis, that may be infecting man via cutaneous
Antibiotic usage in the British sheep industry. Dr Peers Davies
 Antibiotic usage in the British sheep industry Dr Peers Davies 40% of all livestock biomass in the UK (ESVAC report 2016) Current Estimates and Data Sources No published, quantitative estimates of antimicrobial
Antibiotic usage in the British sheep industry Dr Peers Davies 40% of all livestock biomass in the UK (ESVAC report 2016) Current Estimates and Data Sources No published, quantitative estimates of antimicrobial
Introduction. Antimicrobial Usage ESPAUR 2014 Previous data validation Quality Premiums Draft tool CDDFT Experience.
 Secondary Care Data Validation: What do commissioners need to know? Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2014 Introduction Antimicrobial
Secondary Care Data Validation: What do commissioners need to know? Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2014 Introduction Antimicrobial
Scholars Research Library. Investigation of antibiotic usage pattern: A prospective drug utilization review
 Available online at www.scholarsresearchlibrary.com Scholars Research Library Der Pharmacia Lettre, 2011: 3 (5) 301-306 (http://scholarsresearchlibrary.com/archive.html) ISSN 0974-248X USA CODEN: DPLEB4
Available online at www.scholarsresearchlibrary.com Scholars Research Library Der Pharmacia Lettre, 2011: 3 (5) 301-306 (http://scholarsresearchlibrary.com/archive.html) ISSN 0974-248X USA CODEN: DPLEB4
Objective 1/20/2016. Expanding Antimicrobial Stewardship into the Outpatient Setting. Disclosure Statement of Financial Interest
 Expanding Antimicrobial Stewardship into the Outpatient Setting Michael E. Klepser, Pharm.D., FCCP Professor Pharmacy Practice Ferris State University College of Pharmacy Disclosure Statement of Financial
Expanding Antimicrobial Stewardship into the Outpatient Setting Michael E. Klepser, Pharm.D., FCCP Professor Pharmacy Practice Ferris State University College of Pharmacy Disclosure Statement of Financial
3/23/2017. Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc. Kathryn G. Smith: Nothing to disclose
 Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
Should we test Clostridium difficile for antimicrobial resistance? by author
 Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
Should we test Clostridium difficile for antimicrobial resistance? Paola Mastrantonio Department of Infectious Diseases Istituto Superiore di Sanità, Rome,Italy Clostridium difficile infection (CDI) (first
Volume 2; Number 16 October 2008
 Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use