Tedizolid: a novel treatment for Gram + infections and its potential role in clinical practice
|
|
|
- Nathan McKenzie
- 5 years ago
- Views:
Transcription

 Member of General Assembly")
 With approval of the Belgian Common Ethical Health Platform visa no.")
1 Tedizolid: a novel treatment for Gram + infections and its potential role in clinical practice Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain Drug Research Institute Catholic University of Louvain, Brussels, Belgium Co-founder and Past President of the International Society of Anti-infective Pharmacology (ISAP) Member of General Assembly (2006-) and of the Steering Committee ( ) of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) With approval of the Belgian Common Ethical Health Platform visa no. 16/V1/8979/
2 Financial support from Non-profit Institutions: Disclosures the Belgian Fonds de la Recherche Scientifique for basic research on pharmacology antibiotics and related topics The European Union for applied research on optimization of β-lactams treatments through on-line monitoring of free serum levels Université catholique de Louvain for past personal support Industry: AstraZeneca, GSK, Sanofi-Aventis, Bayer HealthCare, Cempra Pharmaceuticals, The Medicines Company, Northern Antibiotics, RibX, Cubist, Galapagos, Other relationships in relation to this talk Belgian Antibiotic Policy Coordination Committee, European Committee for Antibiotic Susceptibility Testing (EUCAST) European Medicines Agency (EMA) Slides: Lectures 2
3 The programme A short view of Belgium and of where I work What is tedizolid? discovery, main properties What are our problems with ABSSSI (in very sort) a view of the infection and of bacterial resistance pros and cons of currently available antibiotics How does tedizolid compares clinically to linezolid? registration studies potential roles in daily therapy Questions, objections, suggestions 3





4 Belgium 4
5 Belgium 10 millions inhabitants 10 Nobel prizes (10/850) for activities in Belgium Peace - Institute of International Law, Ghent (1904) - Auguste Beernaert (1909) - Henri Lafontaine (1913) - Father Dominique Pire (1958) Literature - Maurice Maeterlinck, Ghent (1911) Medicine - Jules Bordet, Brussels (1919) - Corneille Heymans, Ghent (1938) - Christian de Duve, Louvain (1974) - Albert Claude, Brussels (1974) Chemistry - Ilya Prigogyne, Brussels (1977) - Physics - François Englert, Brussels (2013) source: Last accessed: 10 May

6 The Catholic University of Louvain in brief (1 of 4) originally founded in 1425 in the city of Louvain (in French and English; known as Leuven in Flemish) 6

 The University in")
7 The Catholic University of Louvain in brief (2 of 4) Created in 1425, it was one of the major University of the so-called "Low Countries" in the period, with famous scholars and discoverers (Vesalius for anatomy, Erasmus for philosophy, ). Teaching was in Latin, Greek, and Hebrew (College of the 3 languages ) The University in the 1500's Erasmus Vesalius 7

 Professor C.")
8 The Catholic University of Louvain in brief (3 of 4) In the 19 th century, teaching was in French but in the early 1900's, a Flemishspeaking section was opened. Courses were given in both languages, attracting many students and celebrities Prof. G. Lemaitre, professor of Physics and Mathematics at the University who, in the 1930's, made the first suggestion of the continuous expansion of the Universe ( big bang ) (here in conversation with A. Einstein) Professor C. de Duve, Professor of Biochemistry, obtained the Nobel Prize (Physiology and Medicine) in 1974 for his work on intracellular organelles (lysosomes, peroxisomes ) (here in front of a centrifuge) in 1968, the University was divided into a French-speaking Université catholique de Louvain a Flemish-speaking Katholieke Universiteit Leuven 8
 Université")
9 The Catholic University of Louvain in brief (4 of 4) The Flemish-speaking Katholieke Universiteit Leuven has remained in Louvain (Leuven) and is named in English "Catholic Universiteit Leuven". The French-speaking Université catholique de Louvain has moved about 25 km South in a place called "Louvain-la-Neuve, with the "Health Sciences Sector" located in Brussels (Woluwé) Université catholique de Louvain 10 km Katholieke Universiteit Leuven Together, the two sister Universities have about 60,000 students 9

10 What do we do? Teaching of Pharmacology and Pharmacotherapy Post-graduate training on Drug Development Launching of Clinical Pharmacy in Europe Web-based courses on anti-infective Pharmacology 30 graduating students, doctoral fellows and post-graduate fellows working on antiinfective therapy (laboratory and clinical applications) Toxicity, medicinal chemistry, and improved schedules of aminoglycosides novel antibiotics beta-lactams (ceftaroline ) fluoroquinolones (delafloxacin * ) ketolides (solithromycin * ) oxazolidinones (tedizolid ) * in development re-assessment of older antibiotics Editorial board of AAC and IJAA Member of the General Committee of EUCAST (for ISC) and of its Steering committee ( ) Member of the Belgian Antibiotic Policy Coordination Committee Founder and Past President of the International Society of Antiinfective Pharmacology (ISAP) A partial view of our University Clinic (900 beds) and the Education and Research buildings (5,000 students), with the Institute (framed), located in then the outskirts of Brussels, Belgium 10



11 Why should a Belgian come to Jeddah to speak about tedizolid? and find the sun? to leave this? 11
12 We have been working on tedizolid since 2007 called "torezolid" or TR-700 at that time 12



13 But where does tedizolid come from? 13
14 The programme A short view of Belgium and of where I work What is tedizolid? discovery, main properties What are our problems with ABSSSI (in very sort) a view of the infection and of bacterial resistance pros and cons of currently available antibiotics How does tedizolid compares clinically to linezolid? registration studies potential roles in daily therapy Questions, objections, suggestions 14
15 From linezolid to tedizolid: the basics Linezolid (LZD) O O O N N H N O N N N N N F O N O OH acetamido vs. free -OH F Tedizolid (TR-700) additional methyltetrazolyl pyridinyl replacing the morpholinyl Substantial differences that DO impact on intrinsic activity (more potent) activity against LZD-resistant strains half-life (longer) 15
16 Tedizolid is more potent because of more interactions with the target PMID: tedizolid 16
17 Tedizolid is systematically 3-4-x more active than linezolid against LSD S strains O O N N O H N O F O N N N N N N O OH F potential role of the tetrazolyl moiety Lemaire et al. J Antimicrob Chemother 2009;64: PMID:
18 And also for a large-scale survey of different Gram-positive organisms from multiple US and European sites tedizolid linezolid S. aureus (n=4499) Coagulase (-) staphylococci (n=537) % of isolates at MC Enterococci (n=873) β-hemolytic streptococci (n=975) Sahm et al. Diagn Microbiol Infect Dis. 2015;81:112-8: PMID:
19 And also for a another large-scale survey of different Gram-positive organisms from Asia-Pacific, Eastern Europe, and Latin American Countries in 2014 Pfaller et al. Antimicrob Agents Chemother 2016;60:
20 And also for a another large-scale survey of different Gram-positive organisms from Asia-Pacific, Eastern Europe, and Latin American Countries in 2014 BSI: bloodstream infections PIHP: pneumonia in hospitalized patients SSSI: skin and skin structures infection Pfaller et al. Antimicrob Agents Chemother 2016;60:
21 And also for a another large-scale survey of different Gram-positive organisms from Asia-Pacific, Eastern Europe, and Latin American Countries in 2014 S. aureus (all; n=2382) 100 cumulative percentage tedizolid linezolid m g/l Pfaller et al. Antimicrob Agents Chemother 2016;60:
22 And also for a another large-scale survey of different Gram-positive organisms from Asia-Pacific, Eastern Europe, and Latin American Countries in 2014 E. faecalis (n=193) 100 cumulative percentage tedizolid linezolid m g/l Pfaller et al. Antimicrob Agents Chemother 2016;60:
23 Tedizolid is also active against linezolid-resistant isolates (cfr + ) O O N N O H N O F O N N N N N N O OH F Lemaire et al. J Antimicrob Chemother 2009;64: PMID:
24 Activity against Cfr + resistant strains (cfr + bacteria) Locke et al. Antimicrob Agents Chemother 2010;54: PMID:

25 Why is tedizolid active against LZD R strains (cfr)? O O N N O H N O F LZD O N N N N N N O OH F TR700 Locke et al. Antimicrob Agents Chemother 2010;54: PMID:

26 Why is tedizolid active against LZD R strains (cfr)? Locke et al. Antimicrob Agents Chemother 2010;54: PMID:
27 A summary at this point? Chemistry and microbiology Tedizolid is 3-4 x more potent than linezolid Tedizolid is active against cfr + linezolid-resistant strains 27
28 N N N N Tedizolid is presented as a prodrug to increase its solubility O N O O N P F NaO ONa TR-701 O TR-700 O N O N N N N N F OH Tedizolid phosphate (TR-701) is a water soluble phosphate prodrug of TR-700 (compound 11) Phosphatases rapidly cleave TR-701 in vivo to active moiety TR
29 Oral and IV tedizolid phosphate yield similar systemic conversion to tedizolid (high bioavailability) N N N N N F TR-701 O N O O NaO P O ONa N N N N N TR-700 F O N O OH Percentage bioavailability of tedizolid after oral tedizolid phosphate dosing: 91.5% Mean tedizolid plasma concentration after a single dose of IV or oral 200 mg tedizolid phosphate (log time scale; n=8). Flanagan et al. Pharmacotherapy 2014;34: PMID:


30 Tedizolid clinical presentations O N N N N N N O O P O F NaO ONa Tedizolid phosphate Active pharmaceutical ingredient: stable at room temp for >2 yrs 2 formulations: IV Lyophile: TR-701 FA Lyophilized Vial for Injection, 200 mg Oral Tablet: TR-701 FA Immediate Release Tablet, 200 mg Tablets can be crushed in water and tedizolid phosphate remains stable for at least 4h Kennedy et al. Drugs R D. 2015;15: PMID:
31 mg/l linezolid 600 mg day 1 day 21 Tedizolid has a longer half-life than linezolid once-daily dosing is possible 5 breakpoint time (h) tedizolid 200 mg Tedizolid : mean t 1/2 2 x that of linezolid 18h presence > breakpoint (0.5 mg/l) vs. 12h for linezolid (4 mg/l). mg/l day 1 day breakpoint time (h) Muñoz et al. ECCMID 2010 P1594 This allows for a once-a-day dosing 31
32 Tedizolid elimination is largely not through the kidney When using 14 C-labelled tedizolid phosphate, in humans, most of the radioactivity is excreted in feces Mean cumulative percentage of radioactive dose was recovered in urine and feces after single 204-mg (100-mCi) oral 14 C-tedizolid phosphate to healthy male subjects. (+/- SD) No need of adjustment for decreased renal function Ong et al. Drug Metab Dispos. 2014;42:
33 Impact of variations in excretory functions on tedizolid pharmacokinetics Mean (SD) Plasma Tedizolid Concentration (µg/ml) Tedizolid pharmacokinetics for patients with severe renal impairment (egfr < 30 ml/min/1.73 m 2 ) Tedizolid has been shown to have predictable PKs in the following patient groups: Severe renal impairment (egfr < 30 ml/min/1.73 m 2 ) Moderate hepatic impairment (Child- Pugh score 7-9) Severe hepatic impairment (Child- Pugh score 10-15) Elderly (age 66-78) Obese and morbidly obese Ethnic populations No exposure difference between fasted and fed conditions Flanagan et al Antimicrob Agents Chemother 2014;58: PMID Flanagan et al Pharmacotherapy 2014;34: PMID Flanagan et al Antmicrob Agents Chemother 2014;58: PMID Data on file, Bayer. Sivextro (tedizolid phosphate) [prescribing information]. Whitehouse Station, NJ: Merck & Co., Inc.;
 0 6 18 24 12")
34 PK parameters governing the activity of antibiotics Concentration C max C max / MIC f T > MIC AUC 24h / MIC f T > MIC MIC Time (h)


35 AUC 24h and activity tedizolid TZD activity depends on actual fauc 24h /MIC value, and is independent of the dosing schedule (in the limits investigated) Louie et al Antimicrob Agents Chemother 2011;55: PMID
36 Tedizolid breakpoints (200 mg/once daily) 36
37 Accumulation and activity of tedizolid in macrophages 37

38 Accumulation and activity of tedizolid in eukaryotic cells 38
39 Tedizolid is more active (3 4 x) than linezolid against intracellular S. aureus macrophages endothelial Concentration-dependent effects of linezolid (LZD) and torezolid (TR-700) towards S. aureus ATCC after phagocytosis by THP-1 macrophages or HUVECs (endothelial cells) Lemaire et al. JAC 2010; 64:
40 Tedizolid is active intracellularly against MRSA disregarding resistance phenotypes MSSA CA-MRSA HA-MRSA HA-MRSA HA-MRSA LZD R Concentration-dependent effects of torezolid (TR-700) towards S. aureus with different resistance phenotypes after phagocytosis by THP-1 macrophages Lemaire et al. JAC 2010; 64:
41 Tedizolid accumulates in lung macrophages (and fluid) of healthy adults volunteers (200 mg dose) alveolar macrophages epithelial lining fluid free serum concentration Housman et al. ICAAC 2011 A & AAC 2012; 56:

42 Tedizolid distributes equally in muscle and adipose tissue (microdialysis) compared to plasma Subjects administered a single oral dose of 600 mg tedizolid phosphate (prodrug) microdialysis probes into the subcutaneous adipose tissue and nto the muscle analysis by high-performance liquid chromatography with UV detection Sahre et al. Int J Antimicrob Agents. 2012;40: PMID

43 A summary for tedizolid at this point? Chemistry and microbiology 3-4 x more potent than linezolid active against cfr + linezolid-resistant strains Pharmacokinetics, breakpoints, tissue distribution longer half-life than linezolid once daily dosing No need of dose readjustment (renal or hepatic failure, weight ) 200 mg/day covers for MICs up to 0.5 mg/l (EU) or 1 mg/l (USA) accumulates and show activity in macrophages but what about safety? 43
44 Linezolid adverse effects Drug interactions: cytochrome P450: no special effect antibiotics: rifampin causes a 21 % in LZD serum levels Monoamine Oxidase Inhibition (reversible, nonselective inhibitor): adrenergic and serotonergic agents (PRECAUTIONS) Myelosuppression (including anemia, leukopenia, pancytopenia, and thrombocytopenia) (WARNING) Hypoglycemia Lactic acidosis (PRECAUTION Immediate medical attention) Peripheral and Optic Neuropathy (> 28 days) Convulsions 44
45 Monoamine Oxidase (MAO) Substrate Specificity * Consequences of MAO-A Inhibition * Linezolid inhibits both enzymes, causing increased concentration of these bioamines MAO-A MAO-B Serotonin Syndrome Hypertensive crisis Serotonin Noradrenaline Adrenaline Octopamine Dopamine Tyramine a Tryptamine Kynuramine 3-methoxytyramine a MAO-A is the predominant form for oxidation of tyramine Benzylamine Phenylethylamine N-phenylamine Octylamine N-acetylputrescine Milacemide N-methyl-4-phenyl- 1,2,3,6- tetrahydropyridine Elmer & Bertoni. Expert Opin Pharmacother. 2008;9: PMID:

46 Is serotonergic syndrome an important problem? Spectrum of Clinical Findings Manifestations of the serotonin syndrome range from mild to life-threatening. The vertical arrows suggest the approximate point at which clinical findings initially appear in the spectrum of the disease, but all findings may not be consistently present in a single patient with the serotonin syndrome. Severe signs may mask other clinical findings. For example, muscular hypertonicity can overwhelm tremor and hyperreflexia. Boyer & Shannon. N Engl J Med 2005;352: PMID:
47 5-HTP Mouse Head Twitch * (Model of Serotonergic Effects) * The head-twitch response (HTR) is a rapid side-to-side head movement that occurs in mice and rats after the serotonin 5-HT2A receptor is activated (Nakagawasai et al. Neurotoxicology. 2004;25: PMID: ) Flanagan et al. Antimicrob Agents Chemother. 2013;57: PMID:

48 Human data for blood pressure response to pseudoephedrine (60 mg) vs placebo in tedizolid-pretreated patients Flanagan et al. Antimicrob Agents Chemother. 2013;57: PMID:
![Linezolid vs tedizolid effects on platelets (21 days [phase I trials])](/docs-images/95/125399744/images/49-0.jpg "* Tedizolid 200 mg QD * treatment duration of tedizolid in phase III")

49 Linezolid vs tedizolid effects on platelets (21 days [phase I trials]) * Tedizolid 200 mg QD * treatment duration of tedizolid in phase III is limited to 6 days Prokocimer et al. ICAAC IDSA 2008; Poster F1-2069a. Lodise et al J Antimicrob Chemother 2016;71: PMID

50 Linezolid and tedizolid impairment of mitochondrial protein synthesis and human pharmacokinetics 1. Impairment of mitochondrial protein synthesis may explain linezolid-induced lactic acidosis and neuropathies 2. Both linezolid and tedizolid impair mitochondrial protein synthesis. but this is reversible 1 3. For linezolid, plasma concentrations of linezolid remain always > IC 50 permanent inhibition 2 4. For tedizolid, free through concentrations fall < IC50 partial daily recovery 2 25 Pharmacia and Upjohn Co Zyvox (linezolid) prescribing information.pfizer, Inc, New York, NY. 41 Flanagan et al. 2013;23d ECCMID - poster Milosevic et al. 55 th ICAAC & 25th ICC, 2015: poster 1008 (available from ) 2 Flanagan et al. Antimicrob Agents Chemother 2015; 59: PMID
51 A summary of tedizolid preclinical safety attributes Drug-Drug Interactions No inhibition or induction of human hepatic cytochrome P450 activities at high concentrations * No tyramine or noradrenergic "Pressor potentiation Effect" (vs significant effect for linezolid) (see previous slides) No serotonergic effect in head twitch model (see previous slides) Other potential pharmacological issues No effects in pivotal cardiovascular, neurobehavioral, respiratory, or gastrointestinal systems * No IKr or QTc signal with TR-700 at highest soluble dose * No non-clinical genetic toxicology signals: Ames, Chrom Ab, Micronucleus, UDS * No genotoxicity or reprotoxicity issues * No effect on spermatogenesis * * not shown here but see registration data (FDA / EMA) 51





52 So, what do we do now? erysipelas cellulitis surgical wound infection abscess Do you need to treat THESE? deep abscess traumatic wound infection 52
53 The programme A short view of Belgium and of where I work What is tedizolid? discovery, main properties What are our problems with ABSSSI (in very sort) a view of the infection and of bacterial resistance pros and cons of currently available antibiotics How does tedizolid compares clinically to linezolid? registration studies potential roles in daily therapy Questions, objections, suggestions 53
 100 80 60 40 20 0 65% 14% 22% Class I n=88 25% 39% 36% Class II n=56 39% 30% 30% Class III n=33 8% 0% 92%")

54 Patients May Be Over- or Under-treated Depending on the Severity of the Skin Infection N=205 patients in 1 centre; retrospective cohort study in UK Number of patients (%) % 14% 22% Class I n=88 25% 39% 36% Class II n=56 39% 30% 30% Class III n=33 8% 0% 92% Class IV n=12 Classes represent Eron/CREST classification system Appropriate Under-treated Over-treated Inappropriate treatment: under-treatment and over-treatment according to Eron/CREST classification guidance Adapted from: Marwick C, et al. J Antimicrob Chemother 2011;66:
55 Inappropriate Antibiotic Treatment in Patients with Surgical Site Infections Resulted in Worse Clinical Outcomes Mortality rate after hospital admission Hospital length of stay P< % of patients Number of days AB treatment: Appropriate Inappropriate 0.0 Appropriate Inappropriate Initial treatment failure: No Yes No Yes Initial treatment failure due to inappropriate antibiotic therapy was defined as those hospitalised patients who received a new antibiotic after >24h, or underwent drainage/debridement/amputation >72h after hospital admission. Berger A et al. Surg Infect 2013;14(3):
56 56

57 Worldwide prevalence of hospitalacquired methicillin-resistant Staphylococcus aureus. Xia J. et al, Biosc Tre
58 Saudi Arabia But what about MRSA in Saudi Arabia? Journal of Chemotherapy 2014; 2:

59 MRSA in Saudi Arabia 59
60 MRSA in Saudi Arabia 60
61 Inappropriate Antibiotic Treatment is Associated with Worse Outcomes in Patients with Hospitalised csstis Compared with successful therapy, inappropriate antibiotic treatment* is associated with: Mean length of stay (days) o o Longer duration of hospital stay, particularly in patients with HCA and MRSA infections Increased likelihood of unscheduled clinic visits, emergency department visits or hospital admission Odds Ratio: Overall, 1.79; MRSA + HCA, 6.92 Appropriate therapy Inappropriate therapy p= p= p= p= Overall HCA MRSA MRSA + HCA *Initial IV antibiotic treatment was considered inappropriate if the selected agents were not active against the identified pathogens based on in vitro susceptibility testing or usual spectrum of coverage or when they were not given within 24 h of hospital admission. HCA = healthcare associated MRSA = methicillin-resistant Staphylococcus aureus OR = odds ratio Lipsky B et al. Diagn Microbiol Infect Dis 2014;79: patients 61
62 Agent Dose Notes vancomycin linezolid 15 mg/kg every 12 h or continuous infusion 600 mg every 12 h IV OR PO long first choice for IV treatment of MRSA requires drug monitoring may cause nephrotoxicity beware of MICs 2 mg/l bacteriostatic allows for efficient IV PO switch toxicities daptomycin 4 6 mg/kg Q24h IV bactericidal doses may need to be increased possible myopathy ceftaroline 600 mg every 12 h IV bactericidal well tolerated but requires compliance IV only and twice daily oritavancin * dalbavancin * MRSA SSTI: Available treatments 1200 mg once 1000 mg mg at day 7 bactericidal (VISA and VRSA not susceptible) convenient use but long infusion time (3h) prolonged tissue accumulation (risk?) * approved after publication of the guidelines Adapted from the IDSA guidelines (Stevens DL, et al. Clin Infect Dis 2014;59:e10 52 PMID ) East Jeddah Hospital 62

63 Important limits of vancomycin: 1. MIC-related failures Relationship of MIC to treatment failures heteroresistance Moise-Broder et al Clin Infect Dis 2004;38: PMID

64 Vancomycin MIC >1 as a Predictor for Treatment Failure in MRSA Bloodstream Infections Van Hal SJ, et al. CID 2012;54:




65 Important limits of vancomycin: 2. poor tissue penetration Sternal bone 1 : 57% Heart valve 4 : 12% CNS: <10% Epithelial lining fluid 3 : 18% Lung tissue 2 : 17% 24% Vancomycin Penetration Bone 5 : 7% 13% Fat 4 : 14% Muscle 4 : 9% 1. Massias L, et al. Antimicrob Agents Chemother 1992;36: Cruciani M, et al. J Antimicrob Chemother 1996;38: Lamer C. et al. Antimicrob Agents Chemother 1993;37: Daschner FD et al. J Antimicrob Chemother 1987;19: Graziani AL, et al. Antimicrob Agents Chemother 1988;32:
66 Important limits of vancomycin: 3. unpredictable serum levels (at the level of individual patients and over time) Continuous infusion of vancomycin: target value: 27.5 mg/l 40 total vancomycin concentrations over time in all patients with > 3 measures at any time (n=91) it looks fine, but 30 mg/l hours Ampe et al Intern J Antimicrob Agents 2013;41: PMID
67 Important limits of vancomycin: 3. unpredictable serum levels (at the level of individual patients and over time) 50 Continuous infusion of vancomycin: target value: 27.5 mg/l sucessive vancomycin serum levels values in individual patients with > 3 determinations after the first 96h of treatment (n = 52) look at the individual values 40 mg/l patient no. Ampe et al Intern J Antimicrob Agents 2013;41: PMID
68 Important limits of vancomycin: 4. nephrotoxicity Incidence of nephrotoxicity as a function of the trough serum levels 50 Cano Lodise Kullar < >20 Vancomycin trough level categories (mg/l) Cano et al. Clin Therap 2012;34: Kullar et al. Pharmacotherapy 2012;32: Lodise et al. CID 2009;49:
69 The programme A short view of Belgium and of where I work What is tedizolid? discovery, main properties What are our current choices for treatment of ABSSSI a brief overview of the pros and cons of currently available antibiotics for treatment of ABSSSI (other than tedizolid) How does tedizolid compares clinically to linezolid? registration studies potential roles in daily therapy Questions, objections, suggestions 69


70 Tedizolid phase III studies Prokocimer et al. JAMA. 2013; 309: PMID: Moran et al. Lancet Infect Dis. 2014; 14: PMID:
71 FDA new clinical guidance (2013) Indication Prior Guidance (1998) New Guidance* (2013) csssi ABSSSI Infection Type Large Abscess, Wound, Cellulitis, DFI, Chronic Ulcer Large Abscess, Wound, Cellulitis min. 75 cm 2 Infection Severity Intermediate/Severe Severe Primary Endpoints Secondary Endpoints Subjective Clinicians Assessment at 7-14 Days After EOT Varied Low Potential for Differentiation Objective 20% reduction in lesion size at hours Primary Endpoint Sustained to EOT Clinician s Assessment at EOT Higher Potential for differentiation ABSSSI = acute bacterial skin and skin structure infections csssi = complicated skin and skin structure infections; including chronic ulcers, diabetic foot infections, and burns very different in nature, treated differently (polymicrobial) and chronic * The 2010 FDA Guidance primary endpoint: "Cessation of lesion spread & fever at h" was updated in 2013 * Guidance for Industry: Acute Bacterial Skin and Skin Structure Infections: Developing Drugs for Treatment (FDA - CDER -- October
72 FDA new clinical guidance Indication Prior Guidance (1998) New Guidance* (2013) csssi ABSSSI Infection Type Large Abscess, Wound, Cellulitis, DFI, Chronic Ulcer Large Abscess, Wound, Cellulitis min. 75 cm 2 Infection Severity Intermediate/Severe Severe Cellulitis/erysipelas Diffuse skin infection characterized by spreading of edema, Subjective Objective redness, and heat Primary Endpoints Clinicians 1,2 Assessment at % reduction in lesion size at May accompany Days lymphangitis After EOT and regional lymph node hours inflammation 2 Erysipelas may be differentiated Varied with raised Primary skin lesions Endpoint and Sustained to EOT clear demarcation line of affected and unaffected Clinician s areas Assessment 2 at EOT Wound Secondary infection Endpoints Purulent drainage with edema, redness, and/or induration of the surrounding Low wound Potential 1 Higher Potential for Differentiation Cutaneous abscess Involves the dermis and deeper skin tissues in the presence for differentiation of pus collections 1,2 1 see note * in the bottom of the slide 2 ABSSSI = acute bacterial skin and skin structure infections Stevens et al. Clin Infect Dis. 2005;41: PMID csssi = complicated skin and skin structure infections; including chronic ulcers, diabetic foot infections, and burns very different in nature, treated differently (polymicrobial) and chronic * The 2010 FDA Guidance primary endpoint: "Cessation of lesion spread & fever at h" was updated in 2013 * Guidance for Industry: Acute Bacterial Skin and Skin Structure Infections: Developing Drugs for Treatment (FDA - CDER -- October (last accessed: 8 March 2016) East Jeddah Hospital 72
 Abscess/wound margin to")

73 Measurement of Lesions Measurement for All Lesions Head-to-toe vs largest perpendicular width Additional Measurement for Abscesses and Wounds* (at screening only) Abscess/wound margin to perimeter of erythema, oedema, and/or induration/cellulitis *Erythema extending at least 5cm in the shortest distance from the peripheral margin of the abscess or wound Bien et al. Surg Infect 2014;15(2):

74 Two Methods to Measure the Lesion Size Ruler Technique (RT) and Digital Planimetry (DP) RT: the longest head-to-toe length and the greatest perpendicular width of a lesion; accurate for rectangular or square lesions DP: outline the edge of erythema with a surgical marker, then take photographic images of the lesions with digital camera. Bien et al. Surg Infect 2014;15(2):
75 Are these approaches in line with other clinical symptoms? Powers et al. Contemporary Clinical Trials 2016;50:

 the Visual Analog Scale or (B) Faces Rating Scale. Powers et al.")
76 Are these approaches in line with other clinical symptoms? Association of patient-reported pain withmedian ABSSSI lesion area in the Phase 3 trials, illustrating that pain decreases along with a reduction in lesion size, regardless of whether pain is measured by (A) the Visual Analog Scale or (B) Faces Rating Scale. Powers et al. Contemporary Clinical Trials 2016;50:
77 ESTABLISH-1 (PO) and -2 (IV/PO) Primary & Secondary Efficacy Endpoints ESTABLISH-1 (PO) ESTABLISH-2 (IV/PO) Primary Endpoint Cessation of spread and afebrile at hours after first dose of drug Primary Endpoint* 20% Reduction in lesion area at hours after first dose of drug Key Secondary Endpoint 20% Reduction in lesion area at hours after first dose of drug Programmatic clinical response at EOT Investigator s assessment of clinical response at PTE Key Secondary Endpoint Cessation of spread and afebrile at hours after first dose of drug Programmatic clinical response at EOT Investigator s assessment of clinical response at PTE EOT: end of therapy; PTE: post-treatment evaluation IV: intravenous; PO: oral Prokocimer et al. JAMA 2013;309(6): Moran et al. LID 2014;14(8):
: All oral N=667 ABSSSI patients 6 days, Oral Tedizolid QD 10 days, Oral Linezolid BID 4 days Placebo Post-treatment evaluations Post-treatment")
78 ESTABLISH-1 (PO) and -2 (IV/PO) Phase 3 Trial Design: combining FDA and EMA endpoints (double-blind, double-dummy) Day hours after initial dose End of Therapy Day 11 Post-Therapy Evaluation Day Late Follow-Up Day ESTABLISH-1 (112): All oral N=667 ABSSSI patients 6 days, Oral Tedizolid QD 10 days, Oral Linezolid BID 4 days Placebo Post-treatment evaluations Post-treatment evaluations ESTABLISH-2 (113): IV initiated with option of switching to oral N=666 ABSSSI patients 6 days IV/Oral Tedizolid QD 10 days, IV/Oral Linezolid BID 4 days Placebo Post-treatment evaluations Post-treatment evaluations Cessation of spread and absence of fever 20% decrease from baseline in lesion area FDA 1 endpoint Sustained clinical response FDA 2 endpoint Investigator s assessment of clinical response EMA 1 endpoint Sustained clinical success EMA 2 endpoint Prokocimer P, et al. JAMA 2013;309(6):
79 Baseline Key Demographics and Infection Types All randomised patients * ESTABLlSH-1 & ESTABLlSH-2 Tedizolid 200mg QD for 6 days %, ITT (n=664) Linezolid 600mg BID for 10 days %, ITT (n=669) Age (yrs), mean <65 years 65 years Male, % IV drug use Diabetes BMI (Range), kg/m Types of infection: Cellulitis/erysipelas Major abscess Wound infection Median Lesion Surface Area (cm 2 ) * Integrated data Geographical distribution of patients similar between the two treatment arms from US, Canada, Europe, South Africa and Pacific Rim Prokocimer et al. JAMA 2013;309(6): Moran et al. LID 2014;14(8): East Jeddah Hospital 79
80 Baseline Pathogen Distribution All randomised patients * ESTABLlSH-1 & ESTABLlSH-2 Tedizolid 200mg QD for 6 days %, ITT (n=664) Linezolid 600mg BID for 10 days %, ITT (n=669) No pathogen identified Any Gram-positive pathogen Staphylococcus aureus MRSA MSSA Streptococcus pyogenes S. anginosus-milleri group * Integrated data Prokocimer et al. JAMA 2013;309(6): Moran et al. LID 2014;14(8):

81 Establish-1 and Establish-2 Integrated Efficacy Data Can we do it? East Jeddah Hospital 81
82 ESTABLISH-1 and -2 Integrated Efficacy: All Efficacy Endpoints Achieved ITT Analysis Set* Patients with treatment response (%) (-2.0; 6.5) (-4.4; 2.7) -0.1 (-3.8; 3.6) hours Day 11 Days 7-14 post-eot Tedizolid N=664 Linezolid N=669 Early Clinical Response ( 20% lesion area Reduction) End of therapy (Programmatic clinical response) (Investigator assessed response) * Pooled data Prokocimer et al. JAMA 2013;309(6): Shorr et al. AAC 2015;59(2): Moran et al. LID 2014;14(8): East Jeddah Hospital 82
83 ESTABLISH-1 and -2 Integrated Efficacy: Non-inferiority Achieved in Each Infection Type Patients with treatment response (%) Early Clinical Response Rate at h. ITT Analysis Set* ( 5.4; 8.3) ( 8.6; 6.5) ( 1.2; 13.4) n=301 n=307 n=168 n=166 n=195 n=196 Tedizolid N=664 Linezolid N=669 0 Cellulitis/erysipelas Major cutaneous abscess Wound infection * Pooled data Prokocimer et al. JAMA 2013;309(6): Shorr et al. AAC 2015;59(2): Moran et al. LID 2014;14(8):
84 ESTABLISH-1 and -2 Integrated Efficacy Non-inferiority was Achieved at hours in All Subgroups ITT analysis set Tedizolid, % (n/n) Linezolid, % (n/n) Age Sex BMI Treatment difference (95% CI) <65 years 82.6 (489/592) 79.5 (485/610) 3.1 (-1.3; 7.6) 65 years 73.6 (53/72) 78.0 (46/59) -4.9 (-19.4; 10.1) Male 83.0 (356/429) 80.1 (330/412) 2.8 (-2.4; 8.1) Female 79.1 (186/235) 78.2 (201/257) 1.0 (-6.4; 8.2) <30 kg/m (389/464) 79.4 (347/437) 4.4 (-0.6; 9.5) 30 kg/m (153/200) 79.3 (184/232) -2.8 (-10.8; 5.0) IV drug use 82.5 (151/183) 79.6 (164/206) 2.9 (-5.0; 10.7) Diabetes 70.7 (41/58) 82.1 (55/67) (-26.1; 4.0) Bacteraemia at baseline 100 (11/11) a 69 (11/16) ND a Pathogens isolated included: Staphylococcus aureus (methicillin-resistant S. aureus, 2 patients; methicillin-sensitive S. aureus, 4 patients; eradication confirmed for all), Streptococcus pyogenes (2 patients), Streptococcus constellatus (1 patient), Staphylococcus hominis (1 patient), Streptococcus agalactiae (1 patient). BMI = body mass index; CI = confidence interval; ND = not done; ITT = intent to treat; IV = intravenous. Shorr et al. AAC 2015;59(2):
85 ESTABLISH-1 and -2 Integrated Efficacy (by relevant host and disease factors (A) and baseline severity measures (B) in the ITT population) Shorr et al. AAC 2015;59(2):
86 What about lesion localizations? Joseph et al. J Am Podiatr Med Assoc Aug 17. [Epub ahead of print] - PMID:


87 What about lesion localizations? Joseph et al. J Am Podiatr Med Assoc Aug 17. [Epub ahead of print] - PMID:
88 ESTABLISH-1 and -2 Integrated Per-pathogen Microbiological Response at PTE Patients with treatment response (%) ( 6.6; 10.9) 84.4 ITT Analysis Set* ( 7.4; 3.3) 93.9 Tedizolid N=664 Linezolid N=669 0 n=141 n=146 n=188 n=198 MRSA MSSA MRSA and MSSA eradication rates are equivalent for tedizolid 200 mg 6 days vs linezolid 600 mg 10 days * Pooled data Prokocimer et al. JAMA 2013;309(6): Moran et al. LID 2014;14(8):
89 ESTABLISH-1 and -2 Integrated Per-pathogen Microbiological Response at PTE ESTABLlSH-1 & ESTABLlSH-2 MITT Analysis Set Tedizolid 200mg QD for 6 days % (n) Linezolid 600mg BID for 10 days % (n) 95% CI Staphylococcus aureus 88.8 (292/329) 88.9 (304/342) -0.1 (-5.0; 4.7) MRSA 84.4 (119/141) 82.2 (120/146) 2.2 (-6.6; 10.9) MSSA 92.0 (173/188) 93.9 (186/198) -1.9 (-7.4; 3.3) Streptococcus pyogenes 90.9 (30/33) 95.0 (19/20) -4.1 (-19.8; 16.1) S. anginosus-milleri group 73.3 (22/30) 89.3 (25/28) (-35.4; 5.7) High potency against Gram + pathogens Prokocimer et al. JAMA 2013;309(6): Moran et al. LID 2014;14(8):

90 Establish-1 and Establish-2 Integrated Safety Data are we safe with our patients? East Jeddah Hospital 90
 Most Adverse Events Reported were Mild or Moderate in Severity Tedizolid N=662 Linezolid N=662 29% 29% 58% 11% 57% 12% 2% 2% Mild Moderate Severe None Mild Moderate Severe None Prokocimer et al.")
91 ESTABLISH-1 and -2 Integrated Safety: Overall Adverse Events Treatment-Emergent Adverse Event (TEAE) Tedizolid % (n=662) Linezolid % (n=662) Any TEAE 283 (42.7) 286 (43.2) Most Adverse Events Reported were Mild or Moderate in Severity Tedizolid N=662 Linezolid N=662 29% 29% 58% 11% 57% 12% 2% 2% Mild Moderate Severe None Mild Moderate Severe None Prokocimer et al. JAMA 2013;309(6): Moran et al. LID 2014;14(8): East Jeddah Hospital 91
92 ESTABLISH-1 and -2 Integrated Safety: Overall Adverse Events Treatment-Emergent Adverse Event (TEAE) Tedizolid % (n=662) Linezolid % (n=662) Drug-related TEAE 148 (22.4) 185 (27.9) TEAE leading to discontinuation of study drug 3 (0.5) 6 (0.9) Serious TEAE 12 (1.8) 13 (2.0) Drug-related serious TEAE 0 (0.0) 2 (0.3) Any TEAE leading to death* 2 (0.3) 1 (0.2) Overall TEAE rates were similar between tedizolid- and linezolid-treated patients * Not related to study drug Prokocimer et al. JAMA 2013;309(6): Shorr et al. AAC 2015;59(2): Moran et al. LID 2014;14(8): Fang et al. Respirology 2013;18(Suppl4):165. Poster
93 ESTABLISH-1 and -2 Integrated Safety: TEAEs 1% in "Preferred Terms" System Organ Class "Preferred Term" Gastrointestinal disorders Nausea Diarrhoea Vomiting Tedizolid % (n=662) 106 (16.0)* 54 (8.2)* 26 (3.9) 19 (2.9)* Linezolid % (n=662) 152 (23.0) 81 (12.2) 35 (5.3) 37 (5.6) General disorders and administration site conditions (IV site reactions <2% both groups) 36 (5.4) 39 (5.9) Infections and infestations Abscess Cellulitis 91 (13.7) 35 (5.3) 17 (2.6) 78 (11.8) 26 (3.9) 14 (2.1) *P<0.05 Lower incidence of gastrointestinal TEAEs in tedizolid- vs linezolid-treated patients Prokocimer et al. JAMA 2013;309(6): Shorr et al. AAC 2015;59(2): Moran et al. LID 2014;14(8): East Jeddah Hospital 93
94 Tedizolid- and linezolid associated GI Adverse Events: time of apparence GI = gastrointestinal. Shorr et al. AAC 2015;59(2): Tedizolid was associated with a significantly lower incidence of GI adverse events irrespective of duration of therapy East Jeddah Hospital 94
95 Tedizolid Use was Associated with Overall Reduced Risk of Myelosuppression Patients with reduced platelet counts during the entire study period LLN = lower limit of normal. Shorr et al. AAC 2015;59(2): Tedizolid was associated with a significantly lower risk of developing thrombocytopenia Tedizolid is not known to increase the risk of anemia, leukopenia, or pancytopenia 95
96 Summary clinical data * and perspectives Non-inferior to linezolid overall and in all infection types with a shorter duration of therapy ( 6 days vs 10 days) a lower daily dose (200 mg/day vs 1200 mg/day) a simplified schedule of administration (once daily) High eradication rates against Gram-positive pathogens Well tolerated with no serious AE occurring related to tedizolid Significantly lower incidence of gastrointestinal adverse events vs linezolid; irrespective of treatment duration Significantly lower risk of developing thrombocytopenia vs linezolid * as shown in this presentation East Jeddah Hospital 96
97 Summary clinical data and perspectives Non-inferior to linezolid overall and in all infection types with a shorter duration of therapy ( 6 days vs 10 days) a lower daily dose (200 mg/day vs 1200 mg/day) a simplified schedule of administration (once daily) High eradication rates against Gram-positive pathogens Well tolerated with no serious AE occurring related to tedizolid Significantly lower incidence of gastrointestinal adverse events vs linezolid; irrespective of treatment duration Significantly lower risk of developing thrombocytopenia vs linezolid Compare also with the other available antibiotics that we have surveyed * as shown in this presentation East Jeddah Hospital 97



98 A recent expert opinion "Tedizolid has demonstrated excellent activity against broad spectrum aerobic and facultative anaerobic gram-positive bacteria. Other advantages include the availability of both oral and intravenous routes of administration, the short course of therapy, the convenient dosing scheme, and the trend toward less hematological toxicity. Taken these advantages into consideration, tedizolid appears increasingly preferable to linezolid in ABSSSIs." Panagopoulos et al. Expert Opin Pharmacother. 2016;17: PMID:
99 Please, ask questions be critical, ask for facts! Vesalius - anatomy All slide are available on Lectures 99
100 Back up slides 100
101 Microbiology 101

102 And even with recent Chinese isolates ECCMID 2015 Poster P

103 Strains from Europe 592 non-duplicate, non-consecutive isolates of S. aureus collected between 2009 and 2013 from patients with skin infections from 19 European countries (Austria, Belgium, Czech Republic, Denmark, France, Germany, Greece, Hungary, Ireland, Italy, Netherlands, Poland, Portugal, Romania, Russia, Spain, Sweden, Turkey, and the United Kingdom) ECCMID 2015 Poster EP

104 Activity of tedizolid against staphylococci from difficult-to-treat infections Schmidt-Malan et al. Diagn Microbiol Infect Dis. 2016;85:77-9 PMID:

105 Tedizolid and Penicillin-resistant S. pneumoniae 106
106 Pharmacokinetics 107
107 Tedizolid human pharmacokinetics: ascending doses 108
108 Human pharmacokinetics: linearity over increasing doses: single and multiple doses Pharmacotherapy Aug 7. doi: /phar PMID:
109 Tedizolid: Impact of renal and hepatic dysfunction renal dysfunction hepatic dysfunction Flanagan et al. Antimicrob Agents Chemother : PMID:


110 1. renal dysfunction Tedizolid: Impact of renal (incl. dialysis and CCRT) and hepatic dysfunction Flanagan et al. Antimicrob Agents Chemother : PMID: Additional information: at conventional Continuous Renal Replacement Therapy (CRRT) rates, tedizolid transmembrane clearance appears modest relative to total body clearance and is unlikely to require dose adjustments. 2. hepatic dysfunction Lewis et al. Blood Purif. 2015;40: PMID: Flanagan et al. Antimicrob Agents Chemother : PMID:
111 Similar pharmacokinetics in adolescents vs. adults Route PK parameter Geometric mean Geometric mean ratio adolescents adults * adolescents / adults (90% CI) IV C max (mg/l) 3.66 (10) 2.55 (34) ( ) AUC 0- (µg x h/ml) (10) (33) ( ) oral C max (mg/l) 2.17 (10) 2.23 (37) ( ) AUC 0- (µg x h/ml) (10) 28.3 (32) ( ) * Historical data for adult PK parameters after IV dosing were pooled from studies TR and TR Oral dosing data for adults were obtained from study TR Flanagan et al. Pharmacotherapy 2014;34: PMID: Flanagan et al. Antimicrob Agents Chemother. 2014;58: PMID: Fang et al. ECCMID 2013 ( ) Bradley et al. Pediatr Infect Dis J Feb 23. [Epub] PMID:
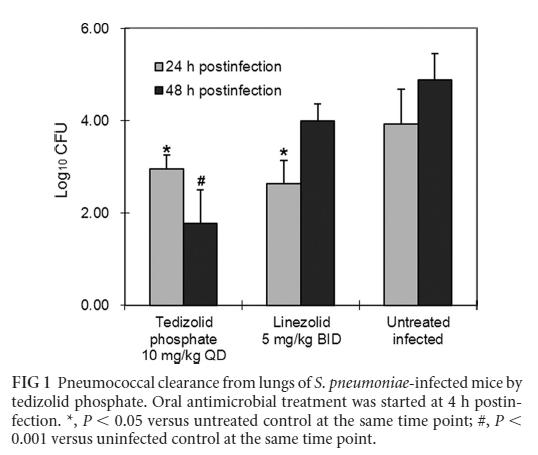
112 Tedizolid and cidal activity in vivo 113
113 Tedizolid is cidal in vivo Louie et al. AAC 2011; 55:

114 Tedizolid and granulocytes in vivo 115
115 Tedizolid cooperates with granulocytes in vivo Drusano et al. AAC 2011; Tedizolid becomes cidal at low doses (equivalent to human 200 mg dose) in the presence of PMN 116
116 Tedizolid and granulocytes cooperate in vivo upon each administration Killing progresses over time at each administration of tedizolid AUC 24 h = 20.1 (equivalent to humans for a dose of 200 mg) MIC = 0.5 mg/l Drusano et al. AAC 2011;
117 Tedizolid vs daptomycin in vivo Dose-Ranging Studies Linezolid Daptomycin 24 hr TR-701 Tedizolid has daptomycin-like in vivo bactericidal activity Linezolid at 160 mg/kg/day did not achieve stasis in this model Louie et al. Antimicrob Agents Chemother. 2011;;55:: (tedizolid) and data on file (daptomycin) 118
118 Pharmacodynamics and PK/PD breakpoint 119
119 How to determine which PK parameter is critical? If you fractionate the daily dose, you change C max without changing AUC 24h C max Concentration C max MIC AUC 24h = Dose 24h / Clearance AUC 24h is independent of the schedule Time (h)
120 How to determine which PK parameter is critical? If you increase the dose without change of schedule, you increase BOTH C max and AUC 24h C max Concentration C max MIC AUC 24h = Dose 24h / Clearance AUC 24h is proportional to the dose Time (h)
121 How do you do this with tedizolid? Louie et al. AAC 2011; 55:
122 What do you see? The correlation with f C max is not excellent The correlation with f T > MIC is worse! Louie et al. AAC 2011; 55:
123 Safety 125
124 Tyramine Sensitivity in humans Linezolid 1 Tedizolid 2 Mean (SD) Tyr 30 dose (mg) 136 (42) 339 (69) Mean; Max Tyramine Sensitivity Factor (TSF) Subjects with 2-fold TSF/total subjects 3.48; ; 2.1 8/10 1/7 TSF =Tyramine Sensitivity Factor = (Tyr 30 following Placebo or pretreatment)/(tyr 30 following TDZ or LZD). Note: 2-fold increase in TSF is threshold for clinically meaningful change in response to tyramine Antal, et al. J Clin Pharmacol 2001; 41: Study TR
125 Vasopressor (Pseudoephedrine) Interaction in humans Mean (SD) Maximum SBP and SBP Changes (mm Hg) Linezolid 3 Tedizolid 4 Pseudoephedrine alone/+ placebo Pseudoephedrine + drug Mean Maximum SBP Change Max SBP Value Mean Maximum SBP Change Max SBP Value 18 (9) 133 (17) 12 (6) 118 (10) 32 (10) 151 (15) 11 (5) 119 (9) Difference Hendershot, et al. J Clin Pharmacol 2001; 41: Study TR
126 Other antibiotics (competitors) 128
127 What are the problems with available anti-gram-positive antibiotics? 1. The emergence of MRSA what is the situation in your country? 129
128 What are the problems with available anti-gram-positive antibiotics? 1. The emergence of MRSA what is the situation in your country? 2. Vancomycin is an old and "difficult" drug IV only, at least twice daily, and 10 days or more monitoring is essential to avoid toxicity beware of MICs > 2 mg/l risk of failures! 130
129 What are the problems with available anti-gram-positive antibiotics? 1. The emergence of MRSA what is the situation in your country? 2. Vancomycin is an old and "difficult" drug IV only, at least twice daily, and 10 days or more monitoring is essential to avoid toxicity beware of MICs > 2 mg/l 3. Linezolid is fraught with toxicities risk of failures! drug interactions (MAO inhibition) myelosuppression, lactic acidosis more frequent than originally reported! 131
130 Clinical development 132
131 What do you wish to see for tedizolid clinically? What is the human safety profile? Phase I studies (ascending doses) What is the useful dose? PK/PD (infected animal) Phase II studies (patients) What are the efficacy and safety profiles against "standard of care" in a large meaningful population? Phase III studies 133

132 A short overview of phase I studies: impact of ascending doses (global) INCIDENCE OF ADVERSE EVENTS no dose effect up to 1200 mg/day presently proposed dosage Prokocimer et al. ICAAC 2011 P

133 A short overview of phase I studies: impact of ascending doses (details) ADVERSE EVENTS REPORTED BY AT LEAST 2 SUBJECTS IN TR-701 OVERALL There were no deaths, Serious AEs, or discontinuations due toaes. No clinically significant changes or findings were noted in clinical laboratory evaluations,vital sign measurements,12-lead ECGs, and physical examinations. There was no dose-response relationship to the number of AEs and, overall, changes in safety evaluations were unremarkable. Prokocimer et al. ICAAC 2011 P
134 Phase I: specific investigations: platelets (increasing doses) upper limit of normal values presently proposed dosage lower limit of normal values 136
 Phase II studies (patients) What are the efficacy and safety profiles against \"standard of care\" in a large meaningful population?")
135 What do you wish to see for tedizolid clinically? What is the human safety profile? Phase I studies (ascending doses) What is the useful dose? PK/PD (infected animal) Phase II studies (patients) What are the efficacy and safety profiles against "standard of care" in a large meaningful population? Phase III studies 137
136 Preclinical studies: definition of the "sufficient dose" in infected animals Drusano et al. AAC 2011; Tedizolid maximal effect is obtained at the equivalent of 200 mg (human dose) 138
137 Tedizolid phase II study 139
138 Tedizolid phase II study 140
139 Tedizolid phase II study 141
140 Tedizolid phase II study this IS the effective dose! 142
141 Tedizolid phase III studies: why two non-inferiority trials? 1. For most indications, both FDA and EMA usually require two independent studies demonstrating efficacy and safety It is preferred that two major (pivotal) studies of efficacy are performed for each clinical indication sought (EMA) Two adequate and well-controlled trials generally are recommended to provide evidence of effectiveness (FDA) General Considerations for Clinical Trials (EMEA - March CPMP/ICH/291/95) Evaluation of medicinal products indicated for treatment of bacterial infections - Adopted guideline (EMA CPMP/EWP/558/95 rev 2) Guidance for Industry: Acute Bacterial Skin and Skin Structure Infections: Developing Drugs for Treatment (FDA - CDER -- October
142 Tedizolid phase III studies: why two non-inferiority trials? 2. Appropriate comparators should be utilized and adequate numbers of subjects included to achieve the study objectives Comparisons may be made with placebo, no treatment, active controls or of different doses of the drug under investigation The choice of the comparator depends, among other things, on the objective of the trial The regimen selected [for comparison] should be considered one of the best available treatments based on one or more of previous studies, medical opinion, indication specific treatment guidelines and anticipated prevalence of resistance to the comparative agent at the investigative sites (EMA) For ABSSSI, there were no placebo-controlled trials reported in the historical literature (FDA) General Considerations for Clinical Trials (EMEA - March CPMP/ICH/291/95) Evaluation of medicinal products indicated for treatment of bacterial infections - Adopted guideline (EMA CPMP/EWP/558/95 rev 2) Guidance for Industry: Acute Bacterial Skin and Skin Structure Infections: Developing Drugs for Treatment (FDA - CDER -- October
143 Do we need antibiotics for ABSSSIs? 145



144 Some say that antibiotics are not needed for "minor skin infections" N Engl J Med 2016;374: one area of fluctuance (2 cm diameter, with tenderness, on the left anterior thigh Erythema up to 2 cm beyond the edges of the fluctuance. No spontaneous drainage and no associated lymphadenopathy. 146


145 Evidence-based medicine we do need antibiotics N Engl J Med 2016;374: PMID
NEW FORCES IN THE MANAGEMENT OF METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS (MRSA)
") EW FORCES I THE MAAGEMET OF METHICILLI-RESISTAT STAPHYLOCOCCUS AUREUS (MRSA) Paul M. Tulkens, MD, PhD Pharmacologie cellulaire et moléculaire Louvain Drug Research Institute, Université catholique de Louvain,
EW FORCES I THE MAAGEMET OF METHICILLI-RESISTAT STAPHYLOCOCCUS AUREUS (MRSA) Paul M. Tulkens, MD, PhD Pharmacologie cellulaire et moléculaire Louvain Drug Research Institute, Université catholique de Louvain,
New antimicrobial agents for the management of MRSA acute bacterial skin and skin structure infections (ABSSSI)
") New antimicrobial agents for the management of MRSA acute bacterial skin and skin structure infections (ABSSSI) Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy
New antimicrobial agents for the management of MRSA acute bacterial skin and skin structure infections (ABSSSI) Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens
 The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
New Antibiotics for MRSA
 New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
Advancing mrsa Management: A New Force for the Clinicians
 Advancing mrsa Management: A New Force for the Clinicians Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain Drug Research Institute Catholic University
Advancing mrsa Management: A New Force for the Clinicians Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain Drug Research Institute Catholic University
Novel therapies & the role of early switch and early discharge protocols for management of MRSA infections
 Novel therapies & the role of early switch and early discharge protocols for management of MRSA infections Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain
Novel therapies & the role of early switch and early discharge protocols for management of MRSA infections Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain
Class Review: Oxazolidinone Antibiotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Appropriate Antimicrobial Therapy for Treatment of
 Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Le infezioni di cute e tessuti molli
 Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections
 for the treatment of Acinetobacter baumannii infections") ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
Antibacterials. Recent data on linezolid and daptomycin
 Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Ceftaroline: a new antibiotic for your patients?
 Ceftaroline: a new antibiotic for your patients? Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology Louvain Drug Research Institute Université catholique de Louvain Brussels, Belgium 11 February
Ceftaroline: a new antibiotic for your patients? Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology Louvain Drug Research Institute Université catholique de Louvain Brussels, Belgium 11 February
Skin and Soft Tissue Infections Emerging Therapies and 5 things to know
 2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
The new antistaphylococcal drugs (tigecycline, daptomycin, telavancin, ): is the future (really) shining?
: is the future (really) shining?") S. aureus: what do we need to know (and to do) in 2007? The new antistaphylococcal drugs (tigecycline, daptomycin, telavancin, ): is the future (really) shining? Françoise Van Bambeke Unité de Pharmacologie
S. aureus: what do we need to know (and to do) in 2007? The new antistaphylococcal drugs (tigecycline, daptomycin, telavancin, ): is the future (really) shining? Françoise Van Bambeke Unité de Pharmacologie
ANTIBIOTICS USED FOR RESISTACE BACTERIA. 1. Vancomicin
 ANTIBIOTICS USED FOR RESISTACE BACTERIA 1. Vancomicin Vancomycin is used to treat infections caused by bacteria. It belongs to the family of medicines called antibiotics. Vancomycin works by killing bacteria
ANTIBIOTICS USED FOR RESISTACE BACTERIA 1. Vancomicin Vancomycin is used to treat infections caused by bacteria. It belongs to the family of medicines called antibiotics. Vancomycin works by killing bacteria
SIVEXTRO (tedizolid phosphate) oral tablet ZYVOX (linezolid) oral suspension and tablet
 oral tablet ZYVOX (linezolid) oral suspension and tablet") ZYVOX (linezolid) oral suspension and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
ZYVOX (linezolid) oral suspension and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Lefamulin: a novel pleuromutilin antibiotic class George Dimopoulos MD, PhD, FCCP, FCCM, FECMM
 : a novel pleuromutilin antibiotic class George Dimopoulos MD, PhD, FCCP, FCCM, FECMM Department of Critical Care, University Hospital ATTIKON National and Kapodistrian University of Athens, Medical School
: a novel pleuromutilin antibiotic class George Dimopoulos MD, PhD, FCCP, FCCM, FECMM Department of Critical Care, University Hospital ATTIKON National and Kapodistrian University of Athens, Medical School
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams
 DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
Staph Cases. Case #1
 Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Antimicrobials Update
 Antimicrobials Update Rosie Amini, PharmD. BCPS Antimicrobial Stewardship Program Coordinator Swedish Medical Center Disclosures: Dr. Amini has no significant financial interest in any of the products
Antimicrobials Update Rosie Amini, PharmD. BCPS Antimicrobial Stewardship Program Coordinator Swedish Medical Center Disclosures: Dr. Amini has no significant financial interest in any of the products
Scottish Medicines Consortium
 Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Université catholique de Louvain, Louvain Drug Research Institute, Brussels, Belgium. Bayer Santé SAS, Loos, France
 Communicating Comprehensive Safety Data Gained from Clinical Trials to the Scientific Community: Opportunities and Difficulties from an Example with Moxifloxacin P.M. Tulkens, 1 P. Arvis, 2 F. Kruesmann,
Communicating Comprehensive Safety Data Gained from Clinical Trials to the Scientific Community: Opportunities and Difficulties from an Example with Moxifloxacin P.M. Tulkens, 1 P. Arvis, 2 F. Kruesmann,
Introduction to Pharmacokinetics and Pharmacodynamics
 Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
A year in review in community-acquired respiratory tract infections
 A year in review in community-acquired respiratory tract infections Paul M. Tulkens, MD, PhD * Cellular and Molecular Pharmacology & Center for Clinical Pharmacy Louvain Drug Research Institute, Catholic
A year in review in community-acquired respiratory tract infections Paul M. Tulkens, MD, PhD * Cellular and Molecular Pharmacology & Center for Clinical Pharmacy Louvain Drug Research Institute, Catholic
The role of new antibiotics in the treatment of severe infections: Safety and efficacy features
 The role of new antibiotics in the treatment of severe infections Safety and efficacy features Christian Eckmann Hannover, Germany The role of new antibiotics in the treatment of severe infections: Safety
The role of new antibiotics in the treatment of severe infections Safety and efficacy features Christian Eckmann Hannover, Germany The role of new antibiotics in the treatment of severe infections: Safety
MRSA ventilatorassociated
 MRSA ventilatorassociated pneumonia Jean Chastre, M.D. www.reamedpitie.com Conflicts of interest Consulting or lecture fees: Medimmune/Astrazeneca, Bayer, Pfizer, Arsanis, Cubist/Merck, Basilea, Aridis,
MRSA ventilatorassociated pneumonia Jean Chastre, M.D. www.reamedpitie.com Conflicts of interest Consulting or lecture fees: Medimmune/Astrazeneca, Bayer, Pfizer, Arsanis, Cubist/Merck, Basilea, Aridis,
Therapeutic options: what s new in the pipeline?
 Therapeutic options: what s new in the pipeline? Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain Drug Research Institute, Université catholique de Louvain,
Therapeutic options: what s new in the pipeline? Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain Drug Research Institute, Université catholique de Louvain,
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate
 Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Product Safety and Quality: An act of social and ethical responsibility (a discussion about generic antibiotics)
") Product Safety and Quality: An act of social and ethical responsibility (a discussion about generic antibiotics) Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology Louvain Drug Research Institute
Product Safety and Quality: An act of social and ethical responsibility (a discussion about generic antibiotics) Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology Louvain Drug Research Institute
Future design of (comparative) clinical trials or how to bring antibiotics to the bed side
 clinical trials or how to bring antibiotics to the bed side") Future design of (comparative) clinical trials or how to bring antibiotics to the bed side Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology Louvain Drug Research Institute Université catholique
Future design of (comparative) clinical trials or how to bring antibiotics to the bed side Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology Louvain Drug Research Institute Université catholique
Period of study: 12 Nov 2002 to 08 Apr 2004 (first subject s first visit to last subject s last visit)
") Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Zyvox. Zyvox (linezolid) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.20 Subject: Zyvox Page: 1 of 7 Last Review Date: March 18, 2016 Zyvox Description Zyvox (linezolid)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.20 Subject: Zyvox Page: 1 of 7 Last Review Date: March 18, 2016 Zyvox Description Zyvox (linezolid)
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus
 Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
S aureus infections: outpatient treatment. Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium
 S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
The Medical Letter. on Drugs and Therapeutics. Objective Drug Reviews Since Volume 56 August 18, 2014
 The Medical Letter on Drugs and Therapeutics Objective Drug Reviews Since 1959 Volume 56 ISSUE ISSUE No. 1433 1449 Volume 56 IN THIS ISSUE Two New Drugs for Skin and Skin Structure Infections...p 73 Important
The Medical Letter on Drugs and Therapeutics Objective Drug Reviews Since 1959 Volume 56 ISSUE ISSUE No. 1433 1449 Volume 56 IN THIS ISSUE Two New Drugs for Skin and Skin Structure Infections...p 73 Important
Lefamulin Evaluation Against Pneumonia (LEAP 1) Phase 3 Topline Results. September 18, 2017
 Phase 3 Topline Results. September 18, 2017") Lefamulin Evaluation Against Pneumonia (LEAP 1) Phase 3 Topline Results September 18, 2017 Safe Harbor and Disclaimer Any statements in this presentation about future expectations, plans and prospects
Lefamulin Evaluation Against Pneumonia (LEAP 1) Phase 3 Topline Results September 18, 2017 Safe Harbor and Disclaimer Any statements in this presentation about future expectations, plans and prospects
Scottish Medicines Consortium
 Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Antimicrobial Cycling. Donald E Low University of Toronto
 Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Bacterial skin and soft tissues infections (SSTI) are one of the most common 1. infections among different age groups
 are one of the most common 1. infections among different age groups") Bacterial skin and soft tissues infections (SSTI) are one of the most common 1 infections among different age groups Gram-positive bacteria are the most frequently isolated pathogens from SSTI, with a
Bacterial skin and soft tissues infections (SSTI) are one of the most common 1 infections among different age groups Gram-positive bacteria are the most frequently isolated pathogens from SSTI, with a
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS. Medicinal product no longer authorised
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE VETERINARY MEDICINAL PRODUCT Zubrin 50 mg oral lyophilisates for dogs Zubrin 100 mg oral lyophilisates for dogs Zubrin 200 mg oral lyophilisates
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE VETERINARY MEDICINAL PRODUCT Zubrin 50 mg oral lyophilisates for dogs Zubrin 100 mg oral lyophilisates for dogs Zubrin 200 mg oral lyophilisates
Amoxicillin trihydrate. Amoxicillin trihydrate. Amoxicillin trihydrate. Amoxicillin trihydrate. Amoxicillin trihydrate. Amoxicillin trihydrate
 Annex I List of the names, pharmaceutical form, strength of the veterinary medicinal product, animal species, route of administration, applicant in the Member States Member State EU/EEA Applicant Name
Annex I List of the names, pharmaceutical form, strength of the veterinary medicinal product, animal species, route of administration, applicant in the Member States Member State EU/EEA Applicant Name
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Oxazolidinone Antibiotics Table of Contents Coverage Policy... 1 General Background... 3 Coding/Billing Information... 5 References... 5 Effective Date...
Cigna Drug and Biologic Coverage Policy Subject Oxazolidinone Antibiotics Table of Contents Coverage Policy... 1 General Background... 3 Coding/Billing Information... 5 References... 5 Effective Date...
Best Antimicrobials for Staphylococcus aureus Bacteremia
 Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Role of IV Therapy in Bone and Joint Infection
 Role of IV Therapy in Bone and Joint Infection Andrew Seaton ID Consultant, Queen Elizabeth University Hospital Lead Doctor Antimicrobial Management Team, NHS GGC @raseaton66 OPAT The IVnOAT Perspective
Role of IV Therapy in Bone and Joint Infection Andrew Seaton ID Consultant, Queen Elizabeth University Hospital Lead Doctor Antimicrobial Management Team, NHS GGC @raseaton66 OPAT The IVnOAT Perspective
Management of Native Valve
 Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
Management of Native Valve Infective Endocarditis 2005 AHA 2015 Baddour LM, et al. Circulation. 2015;132(15):1435-86 2009 ESC 2015 Habib G, et al. Eur Heart J. 2015;36(44):3075-128 ESC 2015: Endocarditis
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali. Lec 1
 Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Optimising treatment based on PK/PD principles
 Optimising treatment based on PK/PD principles Paul M. Tulkens Cellular and Molecular Pharmacology & Center for Clinical Pharmacy Louvain Drug Research Institute Catholic University of Louvain Brussels,
Optimising treatment based on PK/PD principles Paul M. Tulkens Cellular and Molecular Pharmacology & Center for Clinical Pharmacy Louvain Drug Research Institute Catholic University of Louvain Brussels,
DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY*
 44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE (CVMP) REVISED GUIDELINE ON THE SPC FOR ANTIMICROBIAL PRODUCTS
 REVISED GUIDELINE ON THE SPC FOR ANTIMICROBIAL PRODUCTS") European Medicines Agency Veterinary Medicines and Inspections London, 12 November 2007 EMEA/CVMP/SAGAM/383441/2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE (CVMP) REVISED GUIDELINE ON THE SPC
European Medicines Agency Veterinary Medicines and Inspections London, 12 November 2007 EMEA/CVMP/SAGAM/383441/2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE (CVMP) REVISED GUIDELINE ON THE SPC
USA Product Label CLINTABS TABLETS. Virbac. brand of clindamycin hydrochloride tablets. ANADA # , Approved by FDA DESCRIPTION
 VIRBAC CORPORATION USA Product Label http://www.vetdepot.com P.O. BOX 162059, FORT WORTH, TX, 76161 Telephone: 817-831-5030 Order Desk: 800-338-3659 Fax: 817-831-8327 Website: www.virbacvet.com CLINTABS
VIRBAC CORPORATION USA Product Label http://www.vetdepot.com P.O. BOX 162059, FORT WORTH, TX, 76161 Telephone: 817-831-5030 Order Desk: 800-338-3659 Fax: 817-831-8327 Website: www.virbacvet.com CLINTABS
COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE
 European Medicines Agency Veterinary Medicines and Inspections EMEA/CVMP/211249/2005-FINAL July 2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE DIHYDROSTREPTOMYCIN (Extrapolation to all ruminants)
European Medicines Agency Veterinary Medicines and Inspections EMEA/CVMP/211249/2005-FINAL July 2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE DIHYDROSTREPTOMYCIN (Extrapolation to all ruminants)
Evaluating the Role of MRSA Nasal Swabs
 Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Evaluating the Role of MRSA Nasal Swabs Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds February 28, 2017 2016 MFMER slide-1 Objectives Identify the pathophysiology of MRSA nasal colonization
Curricular Components for Infectious Diseases EPA
 Curricular Components for Infectious Diseases EPA 1. EPA Title Promoting antimicrobial stewardship based on microbiological principles 2. Description of the A key role for subspecialists is to utilize
Curricular Components for Infectious Diseases EPA 1. EPA Title Promoting antimicrobial stewardship based on microbiological principles 2. Description of the A key role for subspecialists is to utilize
Clinical Policy: Linezolid (Zyvox) Reference Number: CP.PMN.27 Effective Date: Last Review Date: Line of Business: HIM*, Medicaid
 Reference Number: CP.PMN.27 Effective Date: Last Review Date: Line of Business: HIM*, Medicaid") Clinical Policy: (Zyvox) Reference Number: CP.PMN.27 Effective Date: 09.01.06 Last Review Date: 02.19 Line of Business: HIM*, Medicaid Coding Implications Revision Log See Important Reminder at the end
Clinical Policy: (Zyvox) Reference Number: CP.PMN.27 Effective Date: 09.01.06 Last Review Date: 02.19 Line of Business: HIM*, Medicaid Coding Implications Revision Log See Important Reminder at the end
An Approach to Linezolid and Vancomycin against Methicillin Resistant Staphylococcus Aureus
 Article ID: WMC00590 ISSN 2046-1690 An Approach to Linezolid and Vancomycin against Methicillin Resistant Staphylococcus Aureus Author(s):Dr. K P Ranjan, Dr. D R Arora, Dr. Neelima Ranjan Corresponding
Article ID: WMC00590 ISSN 2046-1690 An Approach to Linezolid and Vancomycin against Methicillin Resistant Staphylococcus Aureus Author(s):Dr. K P Ranjan, Dr. D R Arora, Dr. Neelima Ranjan Corresponding
COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS
 The European Agency for the Evaluation of Medicinal Products Veterinary Medicines and Inspections EMEA/CVMP/627/01-FINAL COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS GUIDELINE FOR THE DEMONSTRATION OF EFFICACY
The European Agency for the Evaluation of Medicinal Products Veterinary Medicines and Inspections EMEA/CVMP/627/01-FINAL COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS GUIDELINE FOR THE DEMONSTRATION OF EFFICACY
Tel: Fax:
 CONCISE COMMUNICATION Bactericidal activity and synergy studies of BAL,a novel pyrrolidinone--ylidenemethyl cephem,tested against streptococci, enterococci and methicillin-resistant staphylococci L. M.
CONCISE COMMUNICATION Bactericidal activity and synergy studies of BAL,a novel pyrrolidinone--ylidenemethyl cephem,tested against streptococci, enterococci and methicillin-resistant staphylococci L. M.
Pharmacology Week 6 ANTIMICROBIAL AGENTS
 Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Pharmacology Week 6 ANTIMICROBIAL AGENTS Mechanisms of antimicrobial action Mechanisms of antimicrobial action Bacteriostatic - Slow or stop bacterial growth, needs an immune system to finish off the microbe
Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy
 Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy Leonardo Pagani MD Director Unit for Hospital Antimicrobial Chemotherapy
Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy Leonardo Pagani MD Director Unit for Hospital Antimicrobial Chemotherapy
ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE
 ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE Version 1.0 Date ratified June 2009 Review date June 2011 Ratified by Authors Consultation Nottingham Antibiotic Guidelines Committee
ANTIBIOTIC PRESCRIBING POLICY FOR DIABETIC FOOT DISEASE IN SECONDARY CARE Version 1.0 Date ratified June 2009 Review date June 2011 Ratified by Authors Consultation Nottingham Antibiotic Guidelines Committee
Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring. Janis Chan Pharmacist, UCH 2008
 and their Monitoring. Janis Chan Pharmacist, UCH 2008") Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring Janis Chan Pharmacist, UCH 25-4-2008 2008 Aminoglycosides (AG) 1. Gentamicin 2. Amikacin 3. Streptomycin 4. Neomycin
Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring Janis Chan Pharmacist, UCH 25-4-2008 2008 Aminoglycosides (AG) 1. Gentamicin 2. Amikacin 3. Streptomycin 4. Neomycin
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
Surgical prophylaxis for Gram +ve & Gram ve infection
 Surgical prophylaxis for Gram +ve & Gram ve infection Professor Mark Wilcox Clinical l Director of Microbiology & Pathology Leeds Teaching Hospitals & University of Leeds, UK Heath Protection Agency Surveillance
Surgical prophylaxis for Gram +ve & Gram ve infection Professor Mark Wilcox Clinical l Director of Microbiology & Pathology Leeds Teaching Hospitals & University of Leeds, UK Heath Protection Agency Surveillance
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering
 SMC No. (650/10) Bayer Schering") moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
MRSA What Are Our Treatment Options and How Do We Choose the Right One?
 MRSA What Are Our Treatment Options and How Do We Choose the Right One? Kristi Traugott, PharmD, BCPS Clinical Pharmacy Specialist Infectious Diseases University Health System San Antonio, TX October 25,
MRSA What Are Our Treatment Options and How Do We Choose the Right One? Kristi Traugott, PharmD, BCPS Clinical Pharmacy Specialist Infectious Diseases University Health System San Antonio, TX October 25,
ESCMID Online Lecture Library. by author
 Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Developing Well-Differentiated Antibiotics. June 2017 Mark Hahn Chief Financial Officer
 Developing Well-Differentiated Antibiotics June 2017 Mark Hahn Chief Financial Officer Forward Looking Statements This presentation contains forward-looking statements regarding future events. These statements
Developing Well-Differentiated Antibiotics June 2017 Mark Hahn Chief Financial Officer Forward Looking Statements This presentation contains forward-looking statements regarding future events. These statements
ETX0282, a Novel Oral Agent Against Multidrug-Resistant Enterobacteriaceae
 ETX0282, a Novel Oral Agent Against Multidrug-Resistant Enterobacteriaceae Thomas Durand-Réville 02 June 2017 - ASM Microbe 2017 (Session #113) Disclosures Thomas Durand-Réville: Full-time Employee; Self;
ETX0282, a Novel Oral Agent Against Multidrug-Resistant Enterobacteriaceae Thomas Durand-Réville 02 June 2017 - ASM Microbe 2017 (Session #113) Disclosures Thomas Durand-Réville: Full-time Employee; Self;
Patients. Excludes paediatrics, neonates.
 Full title of guideline Author Division & Speciality Scope Gentamicin Prescribing Guideline For Adult Patients Annette Clarkson, Specialist Clinical Pharmacist Antimicrobials and Infection Control All
Full title of guideline Author Division & Speciality Scope Gentamicin Prescribing Guideline For Adult Patients Annette Clarkson, Specialist Clinical Pharmacist Antimicrobials and Infection Control All
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections
 Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
Optimizing Antibiotic Treatment of Skin and Soft Tissue Infections 15th Annual Rocky Mountain Hospital Medicine Symposium November 6, 2017 Tim Jenkins, MD Director, Antibiotic Stewardship Program Denver
CF WELL Pharmacology: Microbiology & Antibiotics
 CF WELL Pharmacology: Microbiology & Antibiotics Bradley E. McCrory, PharmD, BCPS Clinical Pharmacy Specialist Pulmonary Medicine Cincinnati Children s Hospital Medical Center January 26, 2017 Disclosure
CF WELL Pharmacology: Microbiology & Antibiotics Bradley E. McCrory, PharmD, BCPS Clinical Pharmacy Specialist Pulmonary Medicine Cincinnati Children s Hospital Medical Center January 26, 2017 Disclosure
Animal models and PK/PD. Examples with selected antibiotics
 Animal models and PK/PD PD Examples with selected antibiotics Examples of animal models Amoxicillin Amoxicillin-clavulanate Macrolides Quinolones Andes D, Craig WA. AAC 199, :375 Amoxicillin in mouse thigh
Animal models and PK/PD PD Examples with selected antibiotics Examples of animal models Amoxicillin Amoxicillin-clavulanate Macrolides Quinolones Andes D, Craig WA. AAC 199, :375 Amoxicillin in mouse thigh
USA Product Label LINCOCIN. brand of lincomycin hydrochloride tablets. brand of lincomycin hydrochloride injection, USP. For Use in Animals Only
 USA Product Label http://www.vetdepot.com PHARMACIA & UPJOHN COMPANY Division of Pfizer Inc. Distributed by PFIZER INC. 235 E. 42ND ST., NEW YORK, NY, 10017 Telephone: 269-833-4000 Fax: 616-833-4077 Customer
USA Product Label http://www.vetdepot.com PHARMACIA & UPJOHN COMPANY Division of Pfizer Inc. Distributed by PFIZER INC. 235 E. 42ND ST., NEW YORK, NY, 10017 Telephone: 269-833-4000 Fax: 616-833-4077 Customer
Dalbavancin, Oritavancin, and Tedizolid for the Treatment of Skin and Soft Tissue Infections
 Dalbavancin, Oritavancin, and Tedizolid for the Treatment of Skin and Soft Tissue Infections Corresponding Author: Robert D. Beckett, PharmD, BCPS* + Director of the Drug Information Center Assistant Professor
Dalbavancin, Oritavancin, and Tedizolid for the Treatment of Skin and Soft Tissue Infections Corresponding Author: Robert D. Beckett, PharmD, BCPS* + Director of the Drug Information Center Assistant Professor
Antimicrobial Therapy
 Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Disclosure: Dr. Spach has no significant financial interest in any of the
Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Disclosure: Dr. Spach has no significant financial interest in any of the
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
TDM of antibiotics. Paul M. Tulkens, MD, PhD
 TDM of antibiotics (Laboratory testing guideline in the intensive care unit) Paul M. Tulkens, MD, PhD Pharmacologie cellulaire et moléculaire Louvain Drug Research Institute, Université catholique de Louvain,
TDM of antibiotics (Laboratory testing guideline in the intensive care unit) Paul M. Tulkens, MD, PhD Pharmacologie cellulaire et moléculaire Louvain Drug Research Institute, Université catholique de Louvain,
Reduce the risk of recurrence Clear bacterial infections fast and thoroughly
 Reduce the risk of recurrence Clear bacterial infections fast and thoroughly Clearly advanced 140916_Print-Detailer_Englisch_V2_BAH-05-01-14-003_RZ.indd 1 23.09.14 16:59 In bacterial infections, bacteriological
Reduce the risk of recurrence Clear bacterial infections fast and thoroughly Clearly advanced 140916_Print-Detailer_Englisch_V2_BAH-05-01-14-003_RZ.indd 1 23.09.14 16:59 In bacterial infections, bacteriological
Critical impact of antimicrobial resistance
 New Antibiotics Kurt B. Stevenson, MD, MPH Professor of Medicine and Epidemiology Division of Infectious Diseases Department of Internal Medicine The Ohio State University College of Medicine Critical
New Antibiotics Kurt B. Stevenson, MD, MPH Professor of Medicine and Epidemiology Division of Infectious Diseases Department of Internal Medicine The Ohio State University College of Medicine Critical
Prophylactic antibiotic timing and dosage. Dr. Sanjeev Singh AIMS, Kochi
 Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Antibiotic stewardship in long term care
 Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Summary of the latest data on antibiotic consumption in the European Union
 Summary of the latest data on antibiotic consumption in the European Union ESAC-Net surveillance data November 2016 Provision of reliable and comparable national antimicrobial consumption data is a prerequisite
Summary of the latest data on antibiotic consumption in the European Union ESAC-Net surveillance data November 2016 Provision of reliable and comparable national antimicrobial consumption data is a prerequisite
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Not All Fluoroquinolones Are Equal
 ot All Fluoroquinolones Are Equal Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology Louvain Drug Research Institute Université catholique de Louvain Brussels, Belgium Singapore With approval
ot All Fluoroquinolones Are Equal Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology Louvain Drug Research Institute Université catholique de Louvain Brussels, Belgium Singapore With approval
Durata Therapeutics Presents New Comprehensive Review of the Efficacy and Safety Data of Dalbavancin and New In Vitro Findings at IDWeek 2013
 October 2, 2013 Durata Therapeutics Presents New Comprehensive Review of the Efficacy and Safety Data of Dalbavancin and New In Vitro Findings at IDWeek 2013 SAN FRANCISCO, Oct. 2, 2013 (GLOBE NEWSWIRE)
October 2, 2013 Durata Therapeutics Presents New Comprehensive Review of the Efficacy and Safety Data of Dalbavancin and New In Vitro Findings at IDWeek 2013 SAN FRANCISCO, Oct. 2, 2013 (GLOBE NEWSWIRE)
 The Journal of Emergency Medicine, Vol. 44, No. 6, pp. e397 e412, 2013 Copyright Ó 2013 Elsevier Inc. Printed in the USA. Open access under CC BY-NC-ND license. 0736-4679 http://dx.doi.org/10.1016/j.jemermed.2012.11.050
The Journal of Emergency Medicine, Vol. 44, No. 6, pp. e397 e412, 2013 Copyright Ó 2013 Elsevier Inc. Printed in the USA. Open access under CC BY-NC-ND license. 0736-4679 http://dx.doi.org/10.1016/j.jemermed.2012.11.050
Proceedings of the 13th International Congress of the World Equine Veterinary Association WEVA
 www.ivis.org Proceedings of the 13th International Congress of the World Equine Veterinary Association WEVA October 3-5, 2013 Budapest, Hungary Reprinted in IVIS with the Permission of the WEVA Organizers
www.ivis.org Proceedings of the 13th International Congress of the World Equine Veterinary Association WEVA October 3-5, 2013 Budapest, Hungary Reprinted in IVIS with the Permission of the WEVA Organizers
ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective
 : The Belgian perspective") ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective Antwerpen 8 november 2002 Yvan Valcke MD PhD AZ Maria Middelares Sint-Niklaas ACUTE EXACERBATIONS of COPD (AE-COPD) Treatment of AECB Role
ACUTE EXACERBATIONS of COPD (AE-COPD) : The Belgian perspective Antwerpen 8 november 2002 Yvan Valcke MD PhD AZ Maria Middelares Sint-Niklaas ACUTE EXACERBATIONS of COPD (AE-COPD) Treatment of AECB Role
Other β-lactamase Inhibitor (BLI) Combinations: Focus on VNRX-5133, WCK 5222 and ETX2514SUL
 Combinations: Focus on VNRX-5133, WCK 5222 and ETX2514SUL") Other β-lactamase Inhibitor (BLI) Combinations: Focus on VNRX-5133, WCK 5222 and ETX2514SUL David P. Nicolau, PharmD, FCCP, FIDSA Director, Center for Anti-Infective Research and Development Hartford Hospital
Other β-lactamase Inhibitor (BLI) Combinations: Focus on VNRX-5133, WCK 5222 and ETX2514SUL David P. Nicolau, PharmD, FCCP, FIDSA Director, Center for Anti-Infective Research and Development Hartford Hospital