InPHARMation. Pharmacy and Therapeutics Committee Update May 23 rd, 2018 Meeting
|
|
|
- Owen Bates
- 5 years ago
- Views:
Transcription

1 VOLUME FOUR; ISSUE 5 May 23, 2018 Edited by: Gregory K. Perry, PharmD, BCPS-AQID
2 InPHARMation Pharmacy and Therapeutics Committee Update May 23 rd, 2018 Meeting The Pharmacy and Therapeutics Committee at Hendrick Medical Center is a Medical Staff Committee that meets the fourth Wednesday of each month with five physicians and one pharmacist serving as voting members. P and T is Medical Staff Committee. The current Chair of P and T is Charles W. Fuller, M.D. 1. Order Set Review: Beta-blocker/Calcium channel blocker overdose. A. Status: approved by P and T. The order set will be available in Apollo. If you would like a hard copy of this set please contact Greg Perry at gperry@hendrickhealth.org 2. Order Set Review: Multi-modal perioperative pain set for hip/knee replacement. A. Status: approved by the musculoskeletal section and P and T. The order set is specific to orthopedic surgeons. The order set will be available in Apollo. If you would like a hard copy of this set please contact Greg Perry at gperry@hendrickhealth.org 3. Formulary Delafloxacin (Baxdela) A. Status: P and T approved formulary addition with restrictions. Delafloxacin is a new fluoroquinolone that covers methicillin-resistant Stapylococcus aureus, Enterococcus faecalis, Pseuodomonas aeruginosa, enterics, anaerobes, and atypical pathogens such as Mycoplasama and Legionella. It is FDA indicated for acute bacterial skin and skin structure infections. It is available in both IV and oral presentations. B. Restrictions 1. Infectious Diseases only. 2. Documented polymicrobial infection (must have susceptible gram positive and negative pathogens) only day supply will be stocked in pharmacy. 4. Formulary Meropenem/vaborbactam (Vabomere) A. Status: P and T approved formulary addition with restrictions. Meropenem/vaborbactam is a combination of an existing carbapenem combined with a new beta-lactamase inhibitor. It covers all pathogens meropenem covers in addition to Enterobacteriaceae isolates, displaying carbapenem-resistant Enterobacteriaceae (CRE) and multidrug-resistant phenotypes. B. Restrictions 1. Infectious Diseases only. 2. Documented or history of CRE infection only day supply will be stocked in pharmacy. 5. Multidrug Resistant Infection Formulary all ID only. A. Ceftazidime/avibactam (Avycaz) specific for Pseudomonas aeruginosa infections suspected of expressing IMP and VIM resistance given with aztreonam. B. Meropenem/vaborbactam (Vabomere) specific for CRE as outlined above. 1
: $196,000.")

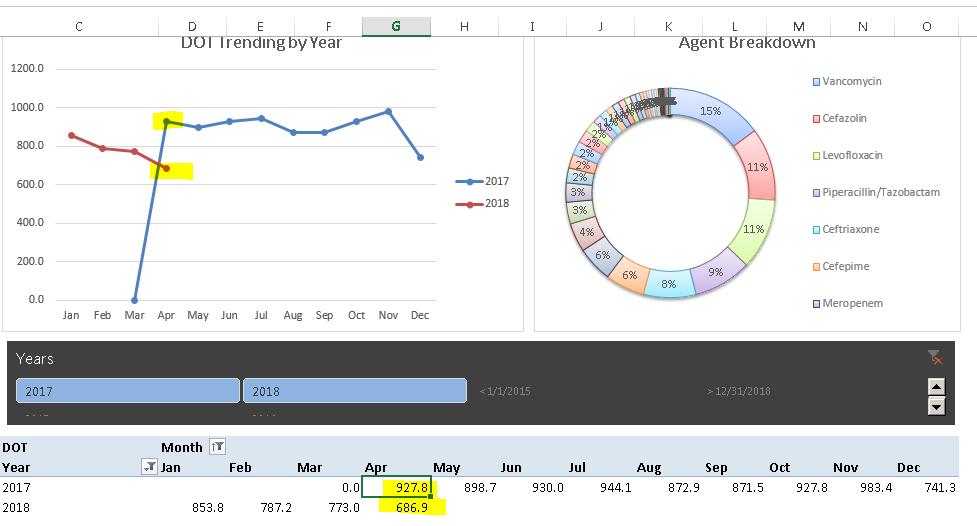
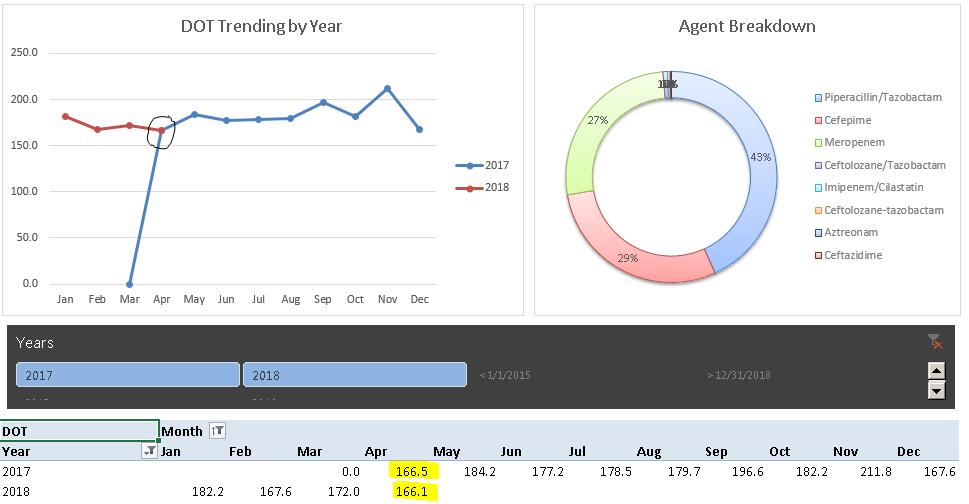
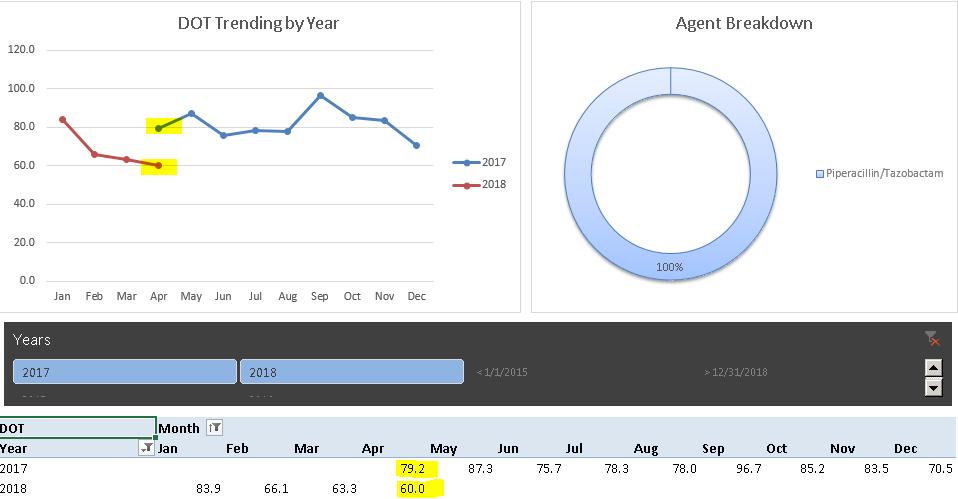
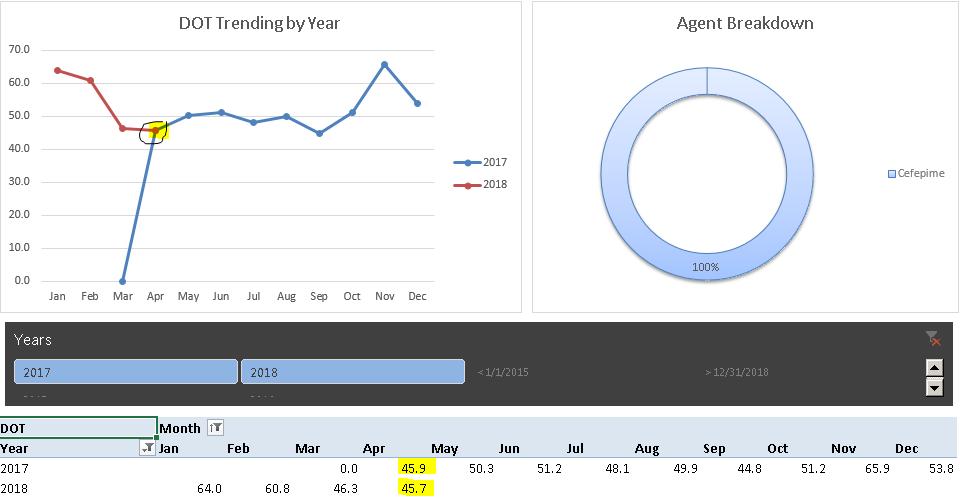
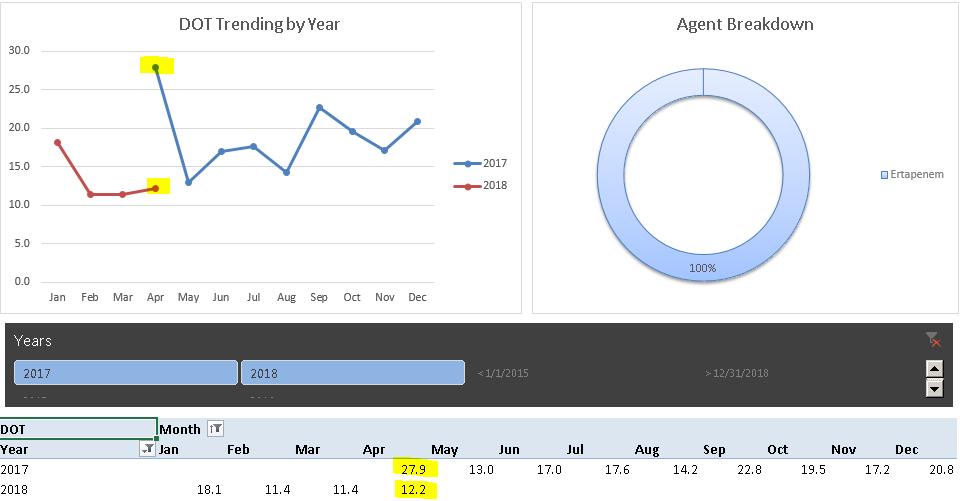
3 C. Ceftolozane/tazobactam (Zerbaxa) specific for Pseudomonas aeruginosa infection that are carbapenem resistant but not thought to be IMP or VIM expressing. 6. AMS Update: Year in Review April 2017 to April Utilization: 26% decrease. 2. Savings (actual hard cost acquisition): $196, Antimicrobial Stewardship Committee (AMS) Update: Utilization Reports through November 2017 CONGRATULATIONS: Antimicrobial use at HMC has decreased 26% compared to this time one year ago as it relates to Days of Therapy per 1000 patient days. Overall utilization of antimicrobials as defined by the CDC/NHSN indicates Hendrick Medical Center is potentially using to many antibiotics. The SAAR for April 2018 was for the system. The recommendation would be if you do not need therapy directed towards Pseudomonas aeruginosa then please avoid all anti-pseudomonal antibiotics if at all possible. The overall days of therapy per 1000 patient days represents a steady decline in antibiotic use over the past 12 months. If you would like to see a detailed report (Physician specific use, floor specific use, CDC specifics) please contact Greg Perry, PharmD, BCPS-AQID at gperry@hendrickhealth.org Always remember the premise of Antimicrobial Stewardship using the three R s. R = Right Drug. R = Right Dose. R = Right Duration of Therapy. 2

4 3


5 4
6 5


7 6
8 Antimicrobial Stewardship Education by Jacquelyn Glockner, PharmD, PGY1 Resident HMC Bites (animal and human) and which bacteria to cover Animal bites account for approximately 1% of emergency visits nationwide. The majority of animal bites are from dogs however, cat bites generally penetrate deeper layers of tissue. There are a number of common pathogens isolated from cat and dog bites including Pasteurella, Staphylococci, Bacteriodes tectum, Fusobacterium, Capnocytophaga, and Prophyromonas species. The decision for the route of antibiotic administration either oral (PO) or intravenous (IV) is dependent on the depth, severity, and time from initial injury. First-line treatment for patients include amoxicillin-clavulanate or ampicillin-sulbactam. If a penicillin allergy is a concern, alternatives include doxycycline, trimethoprim-sulfamethoxazole plus anaerobic coverage (clindamycin or metronidazole), a fluoroquinolone plus anaerobic coverage, or ertapenem. Antibiotics are generally recommended for 5 days however if the patient presents with an infected wound a day course is recommended. Human bites are generally more serious than animal bites and can result from a clenched fist injury where contact is made between the fist of one individual and the teeth of another, or an occlusive injury which is a more traditional bite of human skin. The common pathogens from a human bite include normal oral flora as well as normal skin flora including Streptococci, Staphylococci, Haemophilus, Eikenella corrodens, Fusobacterium nucleatum, Peptostreptococci, Prevontella, and Prophyromonas species. Firstline antibiotics are similar to animal bites and include amoxicillin-clavulanate or ampicillin-sulbactam. For patients with a penicillin allergy, doxycycline, trimethoprim-sulfamethoxazole plus anaerobic coverage, a fluoroquinolone plus anaerobic coverage, or ertapenem are recommended alternative treatments. Generally 5-10 days of antibiotic therapy is adequate for either a cellulitis or an abscess resulting from a human bite. 7 Antibiotic Route Adult Dosing Recommendations Amoxicillin-clavulanate (Augmentin ) PO mg PO q12h Ampicillin-sulbactam (Unasyn ) IV g IV q6h for human bites q6-8h for animal bites Ertapenem (Invanz ) IV 1 g IV daily Doxycycline (Vibramycin ) PO 100 mg PO BID Trimethoprim-sulfamethoxazole (Bactrim ) Clindamycin (Cleocin ) Metronidazole (Flagyl ) Levofloxacin (Levaquin ) Clindamycin (Cleocin ) Metronidazole (Flagyl ) Ciprofloxacin (Cipro ) Clindamycin (Cleocin ) Metronidazole (Flagyl ) PO IV or PO IV or PO Trimethoprim-sulfamethoxazole : mg PO BID Clindamycin: 300 mg PO TID Metronidazole: mg PO 4 times daily Levofloxacin (IV/PO): 750 mg PO daily Either: Clindamycin IV:600 mg IV q6-8h Clindamycin PO:300 mg PO TID Either: Metronidazole IV:500 mg IV q8h Metronidazole PO: mg PO 4 times daily Ciprofloxacin IV: 400 mg q12h Ciprofloxacin PO: mg BID Either: Clindamycin IV:600 mg IV q6-8h Clindamycin PO:300 mg PO TID Either: Metronidazole IV:500 mg IV q8h Metronidazole PO: mg PO 4 times daily References: 1. Stevens D, Bisno A, Chambers H, et al. Practice Guidelines for the Diagnosis and Management of Skin and Soft-Tissue Infections. CID. 2005;41(11):
9 2. Aziz H, Rhee, P, Pandit V, et al. The current concepts in management of animal (dog, cat, snake, scorpion) and human bite wounds. J Trauma Acute Care Surg. 2015; 78(3): Lexicomp Online, Therapeutically Speaking Test Your Knowledge: R.F., a 66-year-old man, presents to the ED with a 2-week history of low-grade fever, cough with putrid sputum, and night sweats. His physical examination is notable for gingivitis and decreased breath sounds on auscultation. His chest radiography reveals an irregularly shaped cavity with an air-fluid level in the upper left lobe surrounded by an infiltrate. His vital signs include temperature F (38 C), blood pressure 148/92 mm Hg, heart rate 88 beats/minute, respiratory rate 18 breaths/minute, and pain 2/10. His laboratory values include BUN 28 mg/dl, SCr 1.5 mg/dl, WBC 15 x 10 3 cells/mm 3, Hgb 12 g/dl, Hct 36%, and Plt 240,000 cells/mm 3. His medical history is significant for hypertension, dyslipidemia, depression, and chronic kidney disease. His current drugs include hydrochlorothiazide 25 mg/day, atorvastatin 20 mg/day, fluoxetine 40 mg/day, and duloxetine 60 mg/day. R.F. is given a diagnosis of a lung abscess and is admitted to the hospital for antibiotic administration. A nasal swab is negative for MRSA. 1. Which one of the following is the most likely cause of R.F. s lung abscess? A. Anaerobic bacteria and streptococci B. E. coli and K. pneumoniae C. M. tuberculosis and non-tubercular mycobacteria D. S. aureus and S. pneumoniae 2. Which one of the following is best to recommend as empiric therapy for R.F.? A. Clindamycin 600 mg intravenously every 8 hours B. Linezolid 600 mg orally every 12 hours C. Piperacillin/tazobactam 4.5 g intravenously every 6 hours D. Rifampin 600 mg orally daily plus isoniazid 300 mg orally daily plus pyrazinamide 1000 mg orally daily plus ethambutol 800 mg orally daily Test Your Knowledge Answer: Question 1: A if poor dentition then anaerobes. If dentition is good or the patient has no teeth then very little anaerobes so don t cover. Oral facultative Streptococci spp (anginosous) would be a concern. Note MRSA, Pseudomonas et al are not part of the differential in this case. The key is an aspiration event is not an aspiration pneumonia but seems to be treated as such many times. A negative CXR does not require treatment.just prevent future aspiration. In this case we have an obvious issue. Question 2: A You don t need MRSA coverage due to the negative predictive value of the MRSA nasal swab so linezolid is not a correct answer. Pseudomonas is not part of the differential so you don t need pip/tazo. TB is certainly not part of the equation so RIPE therapy is not indicated. Clindamycin would cover the oral strep pathogens and oral anaerobes. 8
April 25, 2018 Edited by: Gregory K. Perry, PharmD, BCPS-AQID
 VOLUME FOUR; ISSUE 4 April 25, 2018 Edited by: Gregory K. Perry, PharmD, BCPS-AQID InPHARMation Pharmacy and Therapeutics Committee Update April 25 th, 2018 Meeting The Pharmacy and Therapeutics Committee
VOLUME FOUR; ISSUE 4 April 25, 2018 Edited by: Gregory K. Perry, PharmD, BCPS-AQID InPHARMation Pharmacy and Therapeutics Committee Update April 25 th, 2018 Meeting The Pharmacy and Therapeutics Committee
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare
 Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Felipe N. Gutierrez MD, MPH Chief, Infectious Diseases Phoenix VA Healthcare 100% of all wounds will yield growth If you get a negative culture you something is wrong! Pseudomonas while ubiquitous does
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
11/10/2016. Skin and Soft Tissue Infections. Disclosures. Educational Need/Practice Gap. Objectives. Case #1
 Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Disclosures Selecting Antimicrobials for Common Infections in Children FMR-Contemporary Pediatrics 11/2016 Sean McTigue, MD Assistant Professor of Pediatrics, Pediatric Infectious Diseases Medical Director
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
LEARNING OBJECTIVES ANTIMICROBIAL USES AND ABUSES INFECTIOUS DISEASE SCARES
 LEARNING OBJECTIVES ANTIMICROBIAL USES AND ABUSES Goodbye to the Antibiotic Era? Glenn D. Bedsole, MD, FACP Infectious Disease Consultant 1. Be able to list 6 examples of resistant bacteria that present
LEARNING OBJECTIVES ANTIMICROBIAL USES AND ABUSES Goodbye to the Antibiotic Era? Glenn D. Bedsole, MD, FACP Infectious Disease Consultant 1. Be able to list 6 examples of resistant bacteria that present
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Copyright 2012 Diabetes In Control, Inc. For permission to reprint, please contact Heather Moran, Production Editor, at
 Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Malignant Otitis Externa Inflammation and damage at the base of the skull due to an untreated outer ear P. aeruginosa most common organism Yellow-green drainage from the ear Odor Fever Deep inner ear pain
Pinni Meedha Mojutho Ammanu Dengina Koduku Part 1 Kama Kathalu
 Search for: Search Search Does levaquin cover anaerobes Pinni Meedha Mojutho Ammanu Dengina Koduku Part 1 Kama Kathalu Levofloxacin, sold under the trade names Levaquin among others, is an antibiotic.
Search for: Search Search Does levaquin cover anaerobes Pinni Meedha Mojutho Ammanu Dengina Koduku Part 1 Kama Kathalu Levofloxacin, sold under the trade names Levaquin among others, is an antibiotic.
New Drugs for Bad Bugs- Statewide Antibiogram
 New Drugs for Bad Bugs- Statewide Antibiogram Felicia Matthews, Pharm.D., BCPS Senior Consultant, Pharmacy Specialty BE MedMined Services Disclosures Employee of BD Corporation MedMined Services Agenda
New Drugs for Bad Bugs- Statewide Antibiogram Felicia Matthews, Pharm.D., BCPS Senior Consultant, Pharmacy Specialty BE MedMined Services Disclosures Employee of BD Corporation MedMined Services Agenda
Interactive session: adapting to antibiogram. Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe
 Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Interactive session: adapting to antibiogram Thong Phe Heng Vengchhun Felix Leclerc Erika Vlieghe Case 1 63 y old woman Dx: urosepsis? After 2 d: intermediate result: Gram-negative bacilli Empiric antibiotic
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
Advanced Practice Education Associates. Antibiotics
 Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
Advanced Practice Education Associates Antibiotics Overview Difference between Gram Positive(+), Gram Negative(-) organisms Beta lactam ring, allergies Antimicrobial Spectra of Antibiotic Classes 78 Copyright
What s next in the antibiotic pipeline?
 What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally
![10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally](/thumbs/79/80222162.jpg "10/13/14. Low: not well absorbed. Good: [blood and tissue] < than if given IV. High: > 90% absorption orally") Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Low: not well absorbed PO agent not for serious infection nitrofurantoin Good: [blood and tissue] < than if given IV [Therapeutic] in excess of [effective] eg. cephalexin High: > 90% absorption orally
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Perichondritis: Source: UpToDate Ciprofloxacin 10 mg/kg/dose PO (max 500 mg/dose) BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV
 BID Inpatient: Ceftazidime 50 mg/kg/dose q8 hours IV") Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Empiric Antibiotics for Pediatric Infections Seen in ED NOTE: Choice of empiric antibiotic therapy must take into account local pathogen frequency and resistance patterns, individual patient characteristics,
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Bad Bugs. Pharmacist Learning Objectives. Antimicrobial Resistance. Patient Case. Pharmacy Technician Learning Objectives 4/8/2016
 Pharmacist Learning Objectives Antimicrobial Resistance Julie Giddens Pharm D, BCPS Infectious Disease Clinical Pharmacist OSF Saint Francis Medical Center Peoria, IL The speaker has no conflicts to disclose
Pharmacist Learning Objectives Antimicrobial Resistance Julie Giddens Pharm D, BCPS Infectious Disease Clinical Pharmacist OSF Saint Francis Medical Center Peoria, IL The speaker has no conflicts to disclose
Antimicrobial Stewardship Program
 Antimicrobial Stewardship Program David R. Woodard, MSc, FSHEA, CIC CDC: Antibiotic Resistance Threats in the United States, 2013 http://www.cdc.gov/drugresistance/threat-report-2013/pdf/ CDC Threat Levels
Antimicrobial Stewardship Program David R. Woodard, MSc, FSHEA, CIC CDC: Antibiotic Resistance Threats in the United States, 2013 http://www.cdc.gov/drugresistance/threat-report-2013/pdf/ CDC Threat Levels
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS
 Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
Give the Right Antibiotics in Trauma Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care Dell Seton Medical Center at the University of Texas and Seton Healthcare Family Clinical
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
CLINICAL USE OF BETA-LACTAMS
 CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
CLINICAL USE OF BETA-LACTAMS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu WHY IS INFECTIOUS DISEASE PHARMACOTHERAPY SO CONFUSING? Microbial
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Antimicrobial Susceptibility Testing: Advanced Course
 Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center
 Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center Case 1 60 yo healthy female admitted for fevers and dysuria.
Antibiotics: Selected Topics Steven Park, MD/PhD Director, Antimicrobial Stewardship Program Division of Infectious Diseases UCI Medical Center Case 1 60 yo healthy female admitted for fevers and dysuria.
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
2015 Antibiogram. Red Deer Regional Hospital. Central Zone. Alberta Health Services
 2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
Community Acquired Pneumonia: An Update on Guidelines
 Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Community Acquired Pneumonia: An Update on Guidelines Claudia Summa, BScPhm Pharmacy Resident September 12, 2006 Objectives To give a brief description of the pathophysiology of community acquired pneumonia
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles
 Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
Infectious Disease 101: Helping the Consultant Pharmacist with Stewardship Principles Conflicts of Interest None at this time May be discussing off-label indications KALIN M. CLIFFORD, PHARM.D., BCPS,
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Provincial Drugs & Therapeutics Committee Memorandum Version 2
 Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Provincial Drugs & Therapeutics Committee Memorandum Version 2 16 Garfield Street 16, rue Garfield PO Box 2000, Charlottetown C.P. 2000, Charlottetown Prince Edward Island Île-du-Prince-Édouard Canada
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults
 Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines for Sepsis Syndromes in Adults COMMUNITY-ACQUIRED PNEUMONIA HEALTHCARE-ASSOCIATED PNEUMONIA INTRA-ABDOMINAL INFECTION
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Super Bugs and Wonder Drugs: Protecting the One While Respecting the Many
 Super Bugs and Wonder Drugs: Protecting the One While Respecting the Many Vicki Stringfellow, MSN, CPNP-AC/PC Werner Division of Pediatric Critical Care University of Kentucky Lexington, KY Disclosure
Super Bugs and Wonder Drugs: Protecting the One While Respecting the Many Vicki Stringfellow, MSN, CPNP-AC/PC Werner Division of Pediatric Critical Care University of Kentucky Lexington, KY Disclosure
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Antibiotic stewardship in long term care
 Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
2016 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
National Clinical Guideline Centre Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults
 National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
Infection Prevention Highlights for the Medical Staff. Pamela Rohrbach MSN, RN, CIC Director of Infection Prevention
 Highlights for the Medical Staff Pamela Rohrbach MSN, RN, CIC Director of Infection Prevention Standard Precautions every patient every time a. Hand Hygiene b. Use of Personal Protective Equipment (PPE)
Highlights for the Medical Staff Pamela Rohrbach MSN, RN, CIC Director of Infection Prevention Standard Precautions every patient every time a. Hand Hygiene b. Use of Personal Protective Equipment (PPE)
General Infectious Disease Concepts/Resources
 General Infectious Disease Concepts/Resources Learning Objectives: 1. Distinguish between foundational infectious disease concepts including gram positive and negative bacteria, bacteriostatic and bactericidal
General Infectious Disease Concepts/Resources Learning Objectives: 1. Distinguish between foundational infectious disease concepts including gram positive and negative bacteria, bacteriostatic and bactericidal
Effectiv. q3) Purpose of Policy. Pharmacy: Antimicrobial subcommp&tittee of
 Purpose of Policy. Pharmacy: Antimicrobial subcommp&tittee of") Name ofpolicynupolicy:mber: Department: Approving Officer: Responsible Agent: Scope: Protected Antimicrobials 3364-133-106 Pharmacy: Antimicrobial subcommp&tittee of Chief Executive Officer Director of
Name ofpolicynupolicy:mber: Department: Approving Officer: Responsible Agent: Scope: Protected Antimicrobials 3364-133-106 Pharmacy: Antimicrobial subcommp&tittee of Chief Executive Officer Director of
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXXII NUMBER 6 September 2017 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Stacey Hamilton MT SM (ASCP), Samuel Dominguez MD PhD, Sarah Parker MD, and
VOLUME XXXII NUMBER 6 September 2017 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Stacey Hamilton MT SM (ASCP), Samuel Dominguez MD PhD, Sarah Parker MD, and
2017 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
New Antibiotics & New Insights into Old Antibiotics
 New Antibiotics & New Insights into Old Antibiotics Louisiana Chapter of the American Academy of Pediatrics August 18, 2018 Baton Rouge, Louisiana John Bradley MD Rady Children s Hospital San Diego University
New Antibiotics & New Insights into Old Antibiotics Louisiana Chapter of the American Academy of Pediatrics August 18, 2018 Baton Rouge, Louisiana John Bradley MD Rady Children s Hospital San Diego University
Antimicrobial Stewardship Programs The Same, but Different. Sara Nausheen, MD Kevin Kern, PharmD
 Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Antimicrobial Stewardship Programs The Same, but Different Sara Nausheen, MD Kevin Kern, PharmD Antimicrobial Stewardship Programs The Same, but Different Objectives: Outline the overall function of an
Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report. July December 2013 Second and Third Quarters 2014
 Antimicrobial Stewardship Report. July December 2013 Second and Third Quarters 2014") H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report July December 213 Second and Third Quarters
H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Misericordia Community Hospital (MCH) Antimicrobial Stewardship Report July December 213 Second and Third Quarters
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
THERAPY OF ANAEROBIC INFECTIONS LUNG ABSCESS BRAIN ABSCESS
 THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
THERAPY OF ANAEROBIC INFECTIONS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu LUNG ABSCESS A lung abscess is a localized pus cavity in
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Help with moving disc diffusion methods from BSAC to EUCAST. Media BSAC EUCAST
 Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Help with moving disc diffusion methods from BSAC to EUCAST This document sets out the main differences between the BSAC and EUCAST disc diffusion methods with specific emphasis on preparation prior to
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Clindamycin coverage streptococcus
 Clindamycin coverage streptococcus Oct 12, 2017. While clindamycin and erythromycin were at one time uniformly active against group B streptococci, resistance has been increasing. One large. We assessed
Clindamycin coverage streptococcus Oct 12, 2017. While clindamycin and erythromycin were at one time uniformly active against group B streptococci, resistance has been increasing. One large. We assessed
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Medicinal Chemistry 561P. 2 st hour Examination. May 6, 2013 NAME: KEY. Good Luck!
 Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Medicinal Chemistry 561P 2 st hour Examination May 6, 2013 NAME: KEY Good Luck! 2 MDCH 561P Exam 2 May 6, 2013 Name: KEY Grade: Fill in your scantron with the best choice for the questions below: 1. Which
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Antimicrobial Update. Alison MacDonald Area Antimicrobial Pharmacist NHS Highland April 2018
 Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Antimicrobial Update Alison MacDonald Area Antimicrobial Pharmacist NHS Highland alisonc.macdonald@nhs.net April 2018 Starter Questions Setting the scene... What if antibiotics were no longer effective?
Objectives 4/26/2017. Co-Investigators Sadie Giuliani, PharmD, BCPS Claude Tonnerre, MD Jayme Hartzell, PharmD, MS, BCPS
 IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
Clinical Practice Standard
 Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
Clinical Practice Standard 1-20-6-1-010 TITLE: INTRAVENOUS TO ORAL CONVERSION FOR ANTIMICROBIALS A printed copy of this document may not reflect the current, electronic version on OurNH. APPLICABILITY:
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES
 AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
Understanding the Hospital Antibiogram
 Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
Pharmacist-Driven ASP. Jessica Holt, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Coordinator October 24 th, 2013
 Infectious Diseases Pharmacy Coordinator October 24 th, 2013") Pharmacist-Driven ASP Jessica Holt, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Coordinator October 24 th, 2013 Abbott Northwestern Hospital Largest not-for-profit hospital in the Twin Cities area
Pharmacist-Driven ASP Jessica Holt, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Coordinator October 24 th, 2013 Abbott Northwestern Hospital Largest not-for-profit hospital in the Twin Cities area
Antimicrobial Stewardship 101
 Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
Antimicrobial Stewardship 101 Betty P. Lee, Pharm.D. Pediatric Infectious Disease/Antimicrobial Stewardship Pharmacist Lucile Packard Children s Hospital Stanford Disclosure I have no actual or potential
Antimicrobial susceptibility
 Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
Antimicrobial susceptibility PATTERNS Microbiology Department Canterbury ealth Laboratories and Clinical Pharmacology Department Canterbury District ealth Board March 2011 Contents Preface... Page 1 ANTIMICROBIAL
CLINICAL PROTOCOL FOR COMMUNITY ACQUIRED PNEUMONIA. SCOPE: Western Australia. CORB score equal or above 1. All criteria must be met:
 CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
The Nevada Adult Outpatient Empiric Prescribing Guidelines (2017)
") The Nevada Adult Outpatient Empiric Prescribing Guidelines (2017) Background These empiric prescriber guidelines were produced by the AntiMicrobial Stewardship Summit (AMSS) series led by the University
The Nevada Adult Outpatient Empiric Prescribing Guidelines (2017) Background These empiric prescriber guidelines were produced by the AntiMicrobial Stewardship Summit (AMSS) series led by the University
Bacterial Resistance of Respiratory Pathogens. John C. Rotschafer, Pharm.D. University of Minnesota
 Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Update on Fluoroquinolones. Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO
 Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
Update on Fluoroquinolones Charles Krasner, M.D. June 16, 2016 Antibiotic Stewardship Program -ECHO Potential fluoroquinolone side-effects Increased risk, greater than with most other antibiotics, for
New Opportunities for Microbiology Labs to Add Value to Antimicrobial Stewardship Programs
 New Opportunities for Microbiology Labs to Add Value to Antimicrobial Stewardship Programs Patrick R. Murray, PhD Senior Director, WW Scientific Affairs 2017 BD. BD, the BD Logo and all other trademarks
New Opportunities for Microbiology Labs to Add Value to Antimicrobial Stewardship Programs Patrick R. Murray, PhD Senior Director, WW Scientific Affairs 2017 BD. BD, the BD Logo and all other trademarks
Discussion Points. Decisions in Selecting Antibiotics
 Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Antibiotic Stewardship in the LTC Setting
 Antibiotic Stewardship in the LTC Setting Joe Litsey, Director of Consulting Services Pharm.D., Board Certified Geriatric Pharmacist Thrifty White Pharmacy Objectives Describe the Antibiotic Stewardship
Antibiotic Stewardship in the LTC Setting Joe Litsey, Director of Consulting Services Pharm.D., Board Certified Geriatric Pharmacist Thrifty White Pharmacy Objectives Describe the Antibiotic Stewardship
ß-lactams. Sub-families. Penicillins. Cephalosporins. Monobactams. Carbapenems
 β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
β-lactams ß-lactams Sub-families Penicillins Cephalosporins Monobactams Carbapenems ß-lactams Mode of action PBPs = Trans/Carboxy/Endo- peptidases PBP binding (Penicillin-Binding Proteins) activation of
Examples of Antimicrobial Stewardship Interventions: a couple of starter projects
 Examples of Antimicrobial Stewardship Interventions: a couple of starter projects Jennifer Ott, PharmD, BCPS Clinical Pharmacist Specialist Infectious Diseases Billings Clinic jott4@billingsclinic.org
Examples of Antimicrobial Stewardship Interventions: a couple of starter projects Jennifer Ott, PharmD, BCPS Clinical Pharmacist Specialist Infectious Diseases Billings Clinic jott4@billingsclinic.org
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Antimicrobial Chemotherapy
 2016 edition by Claudine El-Beyrouty, PharmD, BCPS Department of Pharmacy Thomas Jefferson University Hospital Brian Roslund, PharmD, BCPS, AQ-ID Department of Pharmacy Thomas Jefferson University Hospital
2016 edition by Claudine El-Beyrouty, PharmD, BCPS Department of Pharmacy Thomas Jefferson University Hospital Brian Roslund, PharmD, BCPS, AQ-ID Department of Pharmacy Thomas Jefferson University Hospital
Preserve the Power of Antibiotics
 PROVIDERInsight News for providers in Northeast Nebraska April 2016 Preserve the Power of Antibiotics Antimicrobial stewardship interventions have been proven to improve individual patient outcomes, reduce
PROVIDERInsight News for providers in Northeast Nebraska April 2016 Preserve the Power of Antibiotics Antimicrobial stewardship interventions have been proven to improve individual patient outcomes, reduce
3/23/2017. Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc. Kathryn G. Smith: Nothing to disclose
 Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
Kathryn G. Smith, PharmD PGY1 Pharmacy Resident Via Christi Hospitals Wichita, Inc Kathryn G. Smith: Nothing to disclose Describe the new updates and rationale for them Relay safety concerns with use of
Unasyn alternative if penicillin allergic
 Unasyn alternative if penicillin allergic The following guidelines have been developed to assist physicians with the appropriate selection of prophylactic and empiric antibiotic therapy for potential and.
Unasyn alternative if penicillin allergic The following guidelines have been developed to assist physicians with the appropriate selection of prophylactic and empiric antibiotic therapy for potential and.
INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS
 INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS 1 Research Associate, Drug Utilisation Research Unit, Nelson Mandela University 2 Human Sciences Research Council,
INCIDENCE OF BACTERIAL COLONISATION IN HOSPITALISED PATIENTS WITH DRUG-RESISTANT TUBERCULOSIS 1 Research Associate, Drug Utilisation Research Unit, Nelson Mandela University 2 Human Sciences Research Council,
Best Practices: Goals of Antimicrobial Stewardship
 Best Practices: Goals of Antimicrobial Stewardship Gail Scully, M.D, M.P.H. and Elizabeth Radigan, PharmD, BCPS UMass Memorial Medical Center Division of Infectious Disease Department of Medicine September
Best Practices: Goals of Antimicrobial Stewardship Gail Scully, M.D, M.P.H. and Elizabeth Radigan, PharmD, BCPS UMass Memorial Medical Center Division of Infectious Disease Department of Medicine September
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children
 Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Grey Nuns Community Hospital (GNCH) Antimicrobial Stewardship Report
 Antimicrobial Stewardship Report") H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Grey Nuns Community Hospital (GNCH) Antimicrobial Stewardship Report to 214 Table of Contents I. Introduction..
H e a l i n g t h e B o d y E n r i c h i n g t h e M i n d N u r t u r i n g t h e S o u l Grey Nuns Community Hospital (GNCH) Antimicrobial Stewardship Report to 214 Table of Contents I. Introduction..
number Done by Corrected by Doctor Dr.Malik
 number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
number 27 Done by Fatimah Farhan Corrected by Basil Al-Bakri Doctor Dr.Malik Note: anything in red is just extra info and you will not be asked about it in the exam. In this sheet we will continue talking
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of