Managing serious Gram positive infection 2018 Matthew Dryden MD Director of Infection Royal Hampshire County Hospital, Winchester University of
|
|
|
- Donald Gordon
- 5 years ago
- Views:
Transcription


1 Managing serious Gram positive infection 2018 Matthew Dryden MD Director of Infection Royal Hampshire County Hospital, Winchester University of Southampton
2 Disclosures Consulting or lecture honoraria from Bayer, Wyeth, Janssen-Cilag, Pfizer, Astra Zeneca, Cubist, Merk, Motif Bio, Matoke Investigator on antibiotic trials for Bayer, Pfizer, Basilea, Wyeth, Astra Zeneca Recent General Secretary of British Society of Antimicrobial Chemotherapy



3 Post operative suppuration necessary to healing or a complication? My delight may be conceived when there were revealed to me beautiful tangles, tufts and chains of round organisms in great numbers, which stood out clear and distinct among the pus cells and debris... Alexander Ogston 1880
4 What Gram positives are we concerned about? MRSA, hvisa, VRSA Coagulase negative staphylococci Strep pneumoniae Other streptococci Enterococci, VRE
5 Problems with health care infections driven by antibiotic selection Community acquired. MRSA, hvisa, VRSA, cmrsa Coagulase negative staphylococci Strep pneumoniae Other streptococci Enterococci, VRE

6 MRSA as % of invasive S. aureus isolates


7 2014 invasive isolates VRE Macrolide res Strep. pneumonia


8 Variability in MRSA infections and pathogenicity Number of death certificates mentioning Staphylococcus aureus: by methicillin resistance, England and Wales, Number of PVL SA strains identified by the HPA s Staphylococcus Reference Unit2 Patients becoming more complex, vulnerable and harder to predict likely microbial aetiology3 HPA, Health Protection Agency; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible Staphylococcus aureus; PVL, Panton-Valentine leucocidin; SA, Staphylococcus aureus. 1.Office for National Statistics, Deaths involving MRSA: 2008 to Available at: Accessed March 2018; 2. The National Archives. Heath Protection Report 2011;5(7). Available at: Accessed February 2018; 3. Dryden, M. Personal opinion.


9 Intercontinental Exchanges of CA-MRSA Clones ST8, ST59, ST80, ST30 DeLeo FR, et al. Lancet 2010; 375:


10 Antimicrobial resistance in community acquired staphylococcal soft tissue infection Kearns A on behalf of the Community Skin Infection (CSI) study group Public Health England, Colindale, London, NW9 5EQ, UK

11 Clinical issues with invasive staphylococcal infection Which antibiotic? One drug or two? Duration of treatment Source control Test of cure
12 Staphylococcal bacteraemia Most patients should have TTE Consider imaging bone and back pain Failure to identify vertebral osteomyelitis or epidural abscess or BE can lead to catastrophic consequences Repeat BC on day 3
13 When might a TTE be avoided? Nosocomial or health care-associated acquisition of bacteremia Sterile follow-up blood cultures within four days after the initial positive culture No permanent intracardiac device No hemodialysis dependence No clinical signs of endocarditis or secondary foci of infection Removable focus of infection removed promptly, if present Defervescence within 72 hours of initial positive blood culture
14 Dual therapy? Rifampicin 700 adults with S. aureus bacteremia randomized to treatment with standard therapy plus rifampin (600 or 900 mg per day, orally or intravenously) or placebo, no significant difference in mortality or bacteriologic failure was observed after 12 weeks (17 versus 18 percent; hazard ratio 0.96, CI ). Lancet. 2018;391(10121):668. Gentamicin 48 patients with MSSA native valve endocarditis. Although patients who received nafcillin plus gentamicin for the first two weeks of therapy had more rapid clearing of bacteremia than those who received nafcillin alone, cure rates were comparable and combination nafcillin and gentamicin therapy was associated with a higher incidence of renal dysfunction. Ann Intern Med. 1982;97(4):496 Toxin related Gram positive infections staph PVL or GAS Role of contact tracing Decolonisation
15 PVL (MSSA or MRSA) Panton-Valentine Leukocidin (PVL) is a toxin produced by some strains of Staphylococcus aureus. The toxin can destroy white blood cells and cause extensive tissue necrosis and severe infection. PVL infections remain uncommon in the UK but are likely to become more common in the future PVL infection can cause recurrent deep, painful abscesses It should be considered when the severity and extent of lesions is greater than expected, when close contacts have similar lesions, if frequent relapses occur and if there is poor response to antibiotics Pets have been implicated in transmission PVL is not identified by most laboratories Treatment is with drainage + antibiotics eg a two - four week course of flucloxacillin + clindamycin or linezolid, plus five days of chlorhexidine wash and nasal mupirocin to clear the lesions completely.
16 Amount of PVL Effect of antibiotics on staphylococcal PVL production Dumitrescu O, et al. Antimicrobial Agents And Chemotherapy. 2007,
 for MRSA and 27% (58/214) for MSSA Wylie et al BMJ. 2006 Aug 5; 333(7562): 281. doi: 10.")
17 Odds of death after bacteraemia 441 cases of S aureus bacteraemia, 130 (29%) patients died within 30 days. The death rate was 34% (76/227) for MRSA and 27% (58/214) for MSSA Wylie et al BMJ Aug 5; 333(7562): 281. doi: /bmj F
18 Duration of treatment for uncomplicated bacteraemia 14 days from last positive BC Infective endocarditis has been excluded via echocardiography. No indwelling devices (such as prosthetic heart valves or vascular grafts) are present. Follow-up blood cultures drawn two to four days after initiating intravenous antistaphylococcal therapy and removing the presumed focus of infection (if present) are negative. The patient defervesced within 48 to 72 hours after initiating intravenous antistaphylococcal therapy and removal of the presumed focus of infection (such as debridement of soft tissue infection or intravascular catheter removal). There is no evidence of metastatic staphylococcal infection on physical examination.
19 Longer treatment required for: Infective endocarditis Cardiac device infection Osteomyelitis Prosthetic joint infection Septic arthritis Meningitis Pneumonia
20 Vanc Teic
 for MRSA and 45 had a higher MIC (>1.5 mg/l) for MRSA % of patients P<0.001 P=0.022 MIC 1.5 µg/ml vs >1.5 µg/ml influences clinical outcome determined by E-test; OR: 5.024 (1.913-13.192; P=0.")
21 Higher Teicoplanin MIC is Associated With Unfavourable Outcome and Increased Mortality In a retrospective cohort study of 101 bacteraemia patients, 56 had a lower teicoplanin MIC ( 1.5 mg/l) for MRSA and 45 had a higher MIC (>1.5 mg/l) for MRSA % of patients P<0.001 P=0.022 MIC 1.5 µg/ml vs >1.5 µg/ml influences clinical outcome determined by E-test; OR: ( ; P=0.001) * Clinical cure or improvement; Unfavourable outcome: clinical failure = inadequate response to teicoplanin therapy (e.g. resistance to teicoplanin, worsening, recurrence or new onset of signs and symptoms requiring change of antibiotic; positive MRSA blood culture at EOT Chang HJ, et al. JAC 2012;67:
22 Retrospective 30-day in-hospital mortality rate in methicillinsusceptible Staphylococcus aureus bacteraemia Treatment regimen Number of patients Mortality naf/cef only 38 3% (1/38) vanc plus naf/cef 135 7% (10/135) vanc only 94 20% (19/94) (chi-square test for trend p<0.01) Association Adjusted hazard ratio and 95% Confidence Interval Receipt of nafcillin or cefazolin vs. vancomycin alone 0.21 (0.09, 0.47) Switch from vancomycin to nafcillin or cefazolin vs. remaining on vancomycin alone 0.31 (0.10, 0.95) Schweizer et al. BMC Infectious Diseases 2011; 11:279.
23 Vancomycin vs. β-lactams for MSSA bacteraemia: Cohort, 7 years all cases No. cases No. deaths Deaths, % p Vanco β-lactam Case control matched for underlying status Vanco β-lactam <0.001 Kim et al. AAC 2008;52:192 7
24 Antibiotic Company Iclaprim Motifbio Delafloxacin Melinta Year Approved 2019? 2017 Indication Drug Class Spectrum Advantages Disadvantages dihydrofolate Gram +& Alternative class Rapidly bactericidal Not approved yet! ABSSI/CAP reductase inhibitor Gram - Gram + & IV /oral Favourable MICs Tendonitis etc fluoroquinolone ABSSSI Gram Dalbavancin Actavis 2014 ABSSSI lipoglycopeptide Gram + Single dose intravenous therapy Red man syndrome Renal adj Oritavancin Medicines Company 2014 ABSSSI lipoglycopeptide Gram + Single dose intravenous therapy Artificially prolong aptt, infusionrelated reactions?same as linezolid Tedizolid Merck 2014 ABSSSI oxazolidinone Gram + Telavancin Theravance 2013 ABSSSI and lipoglycopeptide Gram + cephalosporin Gram + & HABP / VABP Ceftaroline Pfizer (AZ) 2010 ABSSSI/CABP GramTigecycline Pfizer 2005/6 csssi IAI glycylcycline Gram + & Once a day oral formulation; 6 day treatment for ABSSSI Dual mechanism of action, inhibiting cell wall synthesis and cell membrane function, active against VISA and hvisa Potent activity against MRSA and Streptococci pneumoniae isolates, including drug resistant strains QTc prolongation, potential birth defects Mortality with chr renal failure Same as B lactams Once daily Efficacy v MDR Concerns in bacteraemia Familiarity - 14 years of clinical experience; generic pricing Familiarity - 17 years of clinical experience; oral formulation available; generic pricing Decreased efficacy with moderate renal impairment GramDaptomycin Merck (Cubist) 2003 csssi, S. aureus bacteremia cyclic lipopeptide Gram + Linezolid Pfizer 2000 csssi, CAP, HABP, VRE oxazolidinone Gram + Vancomycin Eli Lilly 1958 csssi lipoglycopeptide Gram + Familiarity - 59 years of clinical experience; generic Serotonin syndrome; adverse events in renal impairment; hypoglycemia if coadministered with insulin/oral hypoglycemics Nephrotoxicity risk with higher doses; ototoxic
25 A case for a b-lactam? Ceftaroline Effective Bactericidal Well tolerated low toxicity No levels required Easy to administer Standard of care vs. MSSA infections Broader cover Vulnerable patients with co-morbidities Early therapeutic response
26 Designed to be different from other cephalosporins 26 Zhanel GG et al. Drugs. 2009;69:
27 Competition assays with ceftaroline for PBP2a of MRSA Moisan et al. JAC 2010;65:
28 Ceftaroline Indications:1 Acute bacterial skin and skin structure infections (ABSSSI) Community-acquired bacterial pneumonia* Efficacy: Bactericidal activity against MRSA, multidrug-resistant Streptococcus pneumonia and some Gram-negative organisms (broad-spectrum)2 Clinical cure in csssi3 Ceftaroline 91.1% vs vancomycin/aztreonam 93.3% (MRSA csssi: 95.1% vs 95.2%) Resistance:4 Ceftaroline-resistant MRSA isolates have been identified in Europe and Asia with MICs between 4 and 8 µg/ml Safety:1 Serious hypersensitivity reactions have been reported In pooled phase 3 trials, direct Coombs test seroconversion occurred in 10.8% of ceftarolinetreated patients vs 4.4% of comparator drugs * Ceftaroline is not indicated for treatment of CAP caused by MRSA 1. TEFLARO Prescribing Information. Forest Laboratories, 2013; 2. Girish C, et al. J Pharmacol Pharmacother 2011;2: ; 3. Corey GR, et al. J Antimicrob Chemother 2010;65(Suppl 4):iv41-51; 4. Long SW, et al. Antimicrob Agents Chemother 2014; 58:
29 Ceftaroline 600 q12h dosing is optimised for time-dependent pharmacodynamics Mean free drug serum concentration-time profile1 Ceftaroline free drug concentration, mg/l S. aureus MIC90 1 µg/ml2 1.0 S. pneumoniae MIC mg/l Keel RA et al. Antimicrob Agents Chemother. 2011;55: Flamm RK et al. Clin Microbiol Infect. 2012;18(suppl S3): Farrell DJ et al. Clin Microbiol Infect. 2012;18(suppl S3): Time, h
30 CANVAS 1 and 2: pooled comorbidity data DM PVD Ceftaroline fosamil No. of patients cured/total no. of patients Difference, % (95% CI) PP-ZFO-EUR-0031 Date of preparation: March (%) of patients (%) of patients Integrated analysis: clinical cure rates by underlying comorbidity (CE population at TOC visit) 96/ / (-12.2 to 5.0) Vancomycin plus aztreonam No. of patients cured/total no. of patients Difference, % (95% CI) 80/90 75/ (-10.0 to 9.7) CANVAS, Ceftaroline versus Vancomycin in Skin and Skin-Structure Infection; CE, clinically evaluable; CI, confidence interval; cssti, complicated skin and soft tissue infection; DM, diabetes mellitus; PVD, peripheral vascular disease; TOC, test of cure. Corey R, et al. Clin Infect Dis 2010;51:
31 Early response data: overall response Clinical responders at Day 4 (%) FOCUS 1 and 2 Early clinical response at Day 4 in the EmMITT population 100 (N=309) FOCUS 1 Ceftaroline 600 mg FOCUS 2 FOCUS 1&2 Integrated Ceftriaxone 1 g FOCUS 1 responder* FOCUS 2 responder* FOCUS 1 and 2 responder* Ceftaroline (600 mg), n/n (%) 49/69 (71.0) 58/85 (68.2) 107/154 (69.5) Ceftriaxone (1 g), n/n (%) 41/72 (56.9) 51/83 (61.4) 92/155 (59.4) Neither FOCUS trial established that ceftaroline was statistically superior to ceftriaxone in terms of clinical response rates at Day 4 The suggestion of benefit seen with ceftaroline at Day 4 does not imply an improved overall end outcome *Responder defined by clinical stability and improvement of symptoms. EmMITT, exploratory microbiological modified intent-to-treat; FOCUS, Ceftaroline Community-Acquired Pneumonia Trial Versus Ceftriaxone in Hospitalized Patients. Eckburg PB, et al. Infect Dis Clin Pract 2012;20:
, n/n (%) 54/74 (73.0) 14/24 (58.3) 16/21 (76.2) 14/18 (77.8) 4/12 (33.3) Ceftriaxone (1 g), n/n (%) 42/75 (56.0) 17/31 (54.8) 20/28 (71.4) 7/12 (58.3) 7/13 (53.")
32 Early response data: by pathogen FOCUS 1 and 2 Early clinical response by pathogen at Day 4 in the EmMITT population (N=309) S. pneumoniae MSSA H. influenzae K. pneumoniae E. coli Ceftaroline (600 mg), n/n (%) 54/74 (73.0) 14/24 (58.3) 16/21 (76.2) 14/18 (77.8) 4/12 (33.3) Ceftriaxone (1 g), n/n (%) 42/75 (56.0) 17/31 (54.8) 20/28 (71.4) 7/12 (58.3) 7/13 (53.8) There was a high rate of early response, irrespective of pathogen The suggested benefit at Day 4 does not imply an improved overall end outcome EmMITT, exploratory microbiological modified intent-to-treat; MSSA, methicillin-sensitive Staphylococcus aureus. Eckburg PB, et al. Infect Dis Clin Pract 2012;20:
33 CAPTURE Registry: real-world data in patients with cssti and comorbidities Initial 1-year results (data collected from August 2011 to August 2012) reported on 647 patients treated for cssti High clinical success rates were observed for ceftaroline fosamil overall (85%) and across patient groups, including patients with comorbidities 100 Pathogens All pathogens MRSA MSSA Clinical success rate (%) Clinical success rate (%) Comorbidities DM PVD Obesity CAPTURE, Ceftaroline Assessment Program and Teflaro Utilization Registry; cssti, complicated skin and soft tissue infection; DM, diabetes mellitus; PVD, peripheral vascular disease; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible Staphylococcus aureus. Santos PD, et al. J Chemother 2013;25:341 6.
34 CAPTURE Registry: real-world data in patients with CAP and comorbidities Initial 18-month results (data collected from August 2011 to February 2013) reported on 398 patients treated for CAP High clinical success rates were observed for ceftaroline fosamil overall (79%) and across patient subgroups (those with comorbidities and different pathogen types) Clinical success rates were highest in patients with Streptococcus pneumoniae infections and CAP patients with structural lung disease or congestive heart failure Comorbidities and pathogen types Clinical success rate (%) All Structural CongestiveStroke All patients lung heart failure S. aureus disease MRSA MSSA All S. pneumoniae NOTE: There are no clinical data to support the use of ceftaroline fosamil for MRSA in CAP caution is advised when treating such patients (Zinforo SmPC, 2017). Clinical success is defined as the following: clinical cure with no further need for antibiotic therapy or clinical improvement with switch to oral agents at the end of ceftaroline fosamil treatment. CAP, community-acquired pneumonia; CAPTURE, Ceftaroline Assessment Program and Teflaro Utilization Registry; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillinsusceptible Staphylococcus aureus. Ramani A, et al. J Chemother 2014;26:
35 Emergence of High-level Ceftaroline Resistance in MRSA Isolates in the USA Caused by PBP2a Mutations Natural history of 6 MRSA clinical isolates collected from the blood and respiratory tract of a 20-year-old cystic fibrosis patient over 154 days with their PBP2a active-site amino acid mutations and ceftaroline MICs Site Sputum Sputum Sputum Sputum Blood Sputum Isolate no PBP2a amino acid changes Y446N E447K Y446N Y446N E447K E239K Y446N E447K MIC (mg/l) > >32 >32 Days post initial admission High-level ceftaroline-resistance (MIC >32 mg/l) in MRSA was detected in isolates collected from a cystic fibrosis patient in the USA Two amino acid-altering mutations (Y446N and E447K) uniquely present in the ceftaroline-binding pocket of PBP2a were found to be responsible for ceftaroline resistance Long SW et al. Antimicrob Agent Chemother 2014;58:
36 Combination treatment Ceftaroline restores daptomycin activity against daptomycinnonsusceptible vancomycin-resistant Enterococcus faecium. Sakoulas G, Rose W, Nonejuie P, et al. Antimicrob Agents Chemother 2014; 58:1494.

37
38 Use off licensed indications CNS Orthopaedic Endocarditis
39 Oxazolidinones Linezolid Tedizolid
40 Oxazolidinones Wide experience now: IV and oral Reduction in IV lines and duration of hospital stay Patient mobilisation Clinical role: oral and prolonged treatment;?superior in pneumonia and MRSA cssti Other indications? Caveat: Bone marrow suppression and neuropathy for linezolid Tedizolid advantages over linezolid: pk, lower dose, safer, short course

41 Tedizolid Linezolid Tedizolid Has Increased Binding Activity versus Linezolid Greater interactions of tedizolid translates into higher potency Locke JB, et al. AAC 2010;54:

42 Tedizolid Use was Associated with Overall Reduced Risk of Myelosuppression Patients with low platelet counts (%) Patients with reduced platelet counts during the entire study period P= Tedizolid 200 mg, 6 days Linezolid 600 mg, 10 days P= Tedizolid was associated with a significantly lower risk of developing thrombocytopenia Tedizolid is not known to increase the risk of anemia, leukopenia, or pancytopenia LLN = lower limit of normal; N1 = any post-baseline observation through last dose of active drug. Prokocimer P, et al. JAMA 2013;309(6): Shorr EF, et al. AAC 2014; doi: /aac Moran G, et al. LID 2014;14(8):

43 Iclaprim Iclaprim Motifbio 2019? ABSSI/CAP dihydrofolate Gram +& reductase Gram - Alternative class Rapidly bactericidal Not approved yet! inhibitor Huang D et al. A Pooled Analysis of the Phase 3 REVIVE Trials: Randomized, Double-blind Studies to EValuate the Safety and Efficacy of Iclaprim Versus Vancomycin for treatment of Acute Bacterial Skin and Skin Structure Infections IJAA
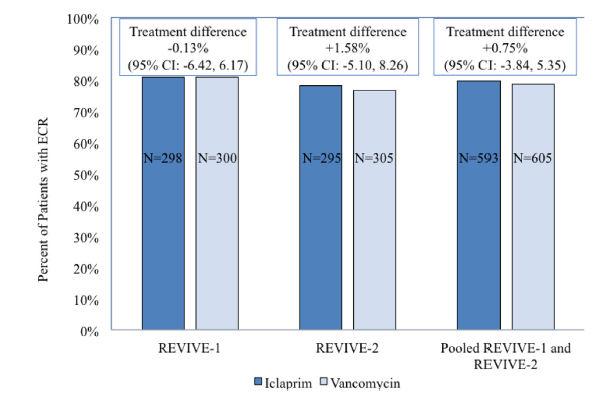
44 Iclaprim
:653. csssi, S.")
45 Daptomycin Daptomycin Merck (Cubist) 2003 Dapto non-inferior to anti-staph pen + gent or vanc + gent for staph bacteraemia. Fowler VG et al N Engl J Med. 2006;355(7):653. csssi, S. aureus bacteremia cyclic lipopeptide Gram + Familiarity - 14 years of clinical experience; generic pricing Decreased efficacy with moderate renal impairment
46 Trend for Lower Microbiological Success for Daptomycin vs Comparators for MRSA SSTIs Microbiological success rate for daptomycin was slightly lower vs comparator drugs* (3 RCTs, n=203; OR 0.91, 95% CI 0.77 to 1.06; p=0.10) *Vancomycin, semisynthetic penicillins, teicoplanin Fowler VG et al N Engl J Med. 2006;355(7):653. Wang SZ et al. BMJ Open 2014;4:e
47 Significantly Higher Creatinine Phosphokinase Elevation for Daptomycin vs Comparators in SSTI Patients Creatinine phosphokinase elevations were significantly more common for daptomycin vs comparator agents* in patients with SSTIs (5 RCTs, n=1521; OR=1.95, 95% CI 1.04 to 3.65, p=0.04) Incidence of treatment-emergent adverse events (AEs) was comparable or daptomycin vs comparators (5 RCTs, n=1521; OR=1.06, 95% CI 0.71 to 1.59, p=0.76) No significant differences were observed for discontinuation due to AEs and all-cause mortality between the daptomycin and comparator groups (6 RCTs, n=1710; OR=0.76, 95% CI 0.46 to 1.10, p=0.12) *Vancomycin, semisynthetic penicillins, teicoplanin Fowler VG et al N Engl J Med. 2006;355(7):653. Wang SZ et al. BMJ Open 2014;4:e
48 VRE infections: There are limited options for treatment of serious VRE infections. Monotherapy with daptomycin or tigecycline or linezolid may be sufficient in some cases All strains (60) were susceptible to LZD and DPT (MIC(90), 4 and 2μg/ml, respectively) and only a single strain presented intermediate susceptibility to tigecycline (MIC(90), 0.25μg/ml). 30% of strains were resistant to Q-D (MIC(90), 4μg/ml), and CFT was constantly inactive (MIC(90), 64μg/ml). Finally, TLV showed low-level MICs (MIC(90), 0.5μg/ml) against vanb-positive isolates but not against vana-positive isolates (MIC(90), 8μg/ml). Med Mal Infect 2011; 41:405.
49 VRE infections Combination therapy is often indicated for severe or complicated infections such as endocarditis. Several antibiotic combinations have been used in isolated case reports with some efficacy, including the following: high-dose ampicillin with an aminoglycoside, ampicillin with ceftriaxone or imipenem, high-dose daptomycin with ampicillin and gentamicin or with gentamicin and rifampin daptomycin with tigecycline quinupristin-dalfopristin with high-dose ampicillin doxycycline and rifampin linezolid with tigecycline limited efficacy, limited susceptibility, and extensive toxicities with many of these agents and combinations present barriers to effective treatment. oritavancin has been shown to have in vitro activity against some isolates of VRE prolonged course of oritavancin in the treatment of a serious VRE infection, prosthetic valve endocarditis. Ceftaroline restores daptomycin activity against daptomycin-nonsusceptible vancomycinresistant Enterococcus faecium. Sakoulas G, Rose W, Nonejuie P, et al. Antimicrob Agents Chemother 2014; 58:1494.
50 Dalbavancin / Oritavancin Dalbavancin Actavis 2014 ABSSSI lipoglycopeptide Gram + Oritavancin Medicines Company 2014 ABSSSI lipoglycopeptide Gram + Single dose intravenous therapy Single dose intravenous therapy Suitable for outpatient ID offices? Non-compliant patients Saves in patient days Oritavancin is a novel lipoglycopeptide with activity against Gram-positive organisms including streptococci, methicillin-resistant Staphylococcus aureus, vancomycin-resistant S aureus (VRSA), and vancomycin-resistant enterococci (VRE) Red man syndrome Renal adj Artificially prolong aptt, infusionrelated reactions
51 Dalbavancin +/- beta lactams a. - hvisa, b.- hvisa DNS, c.- VISA DNS, d.- VISA DNS Xhemali et al JAC 2018 in press

52 Delafloxacin a novel anionic fluoroquinolone Enhanced antimicrobial activity against both gram-positives, gram-negatives, atypicals and anaerobic bacteria Active against MSSA and MRSA Available as IV and oral formulation Improved safety profile 52
53 In vitro activity of delafloxacin against FQs-resistant S. aureus Almer et al., 2004: 71 strains. Origin: US Nilius et al., 2003: 19 strains. Origin: US Compound MIC50 (µg/ml) MIC90 (µg/ml) Compound MIC50 (µg/ml) MIC90 (µg/ml) Delafloxacin Delafloxacin Trovafloxacin 1 2 Levofloxacin Levofloxacin 8 16 Trovafloxacin 2 8 Ciprofloxacin Ciprofloxacin Moxifloxacin 4 8 Gatifloxacin 8 16 Gemifloxacin
54 Cardiac Safety Some FQs can precipitate episodes of Torsades de Pointes (TdP), a life threatening or even fatal episodes of ventricular arrhythmia. Some FQs prolong the QT interval by blocking voltage-gated potassium channels, especially the rapid component of the delayed rectifier potassium current IKr, expressed by herg. Concerns over the potential for proarrhythmia have prompted the withdrawal of grepafloxacin from the market. According to the available case reports and clinical studies, moxifloxacin carries the greatest risk of QT prolongation and should be used with caution in patients with predisposing factors for TdP. Although gemifloxacin, levofloxacin, and ofloxacin are associated with a lower risk of QT prolongation compared with moxifloxacin, they should also be used with caution in patients at risk for QT prolongation. Unlike other FQs, delafloxacin did not affect QT/QTc interval 54
55 Delafloxacin Clinical Development Program 2658 subjects exposed to delafloxacin 30 studies 23 Phase I studies 7 Phase II/III studies N=1158 N= PK studies N=881 1 photosens.study Oral Delafloxacin N=52 Phase II 2 studies in ABSSSI N=406 Phase II 2 studies other indications (CAP* and ABECB**) N= studies renal &hepatic impairment N=83 1 DDI study N=22 1 QT interval study Oral delafloxacin N=68 1 TQTc interval study IV delafloxacin N=52 Phase III 2 studies in ABSSSI N=1510 Phase III 1 study other indication (uncomplicated gonhorrea) N=460 *Community-acquired pneumonia; ** Acute bacterial exacerbation of chronic bronchititis 55
56 Summary Epidemiology of Gram positive infection is changing Patients with invasive staphylococcal disease need careful assessment and management Pathogenic strains eg PVL are emerging Wide variety of new antimicrobial agents (unlike for Gram negatives). All non inferior to comparators in registration trials All of these are welcome and have a clinical role to play.
57 Thank you
Appropriate Antimicrobial Therapy for Treatment of
 Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Appropriate Antimicrobial Therapy for Treatment of Staphylococcus aureus infections ( MRSA ) By : A. Bojdi MD Assistant Professor Inf. Dis. Dep. Imam Reza Hosp. MUMS Antibiotics Still Miracle Drugs Paul
Staph Cases. Case #1
 Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Staph Cases Lisa Winston University of California, San Francisco San Francisco General Hospital Case #1 A 60 y.o. man with well controlled HIV and DM presents to clinic with ten days of redness and swelling
Best Antimicrobials for Staphylococcus aureus Bacteremia
 Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Best Antimicrobials for Staphylococcus aureus Bacteremia I. Methicillin Susceptible Staph aureus (MSSA) A. In vitro - Anti-Staphylococcal β-lactams (Oxacillin, Nafcillin, Cefazolin) are more active B.
Le infezioni di cute e tessuti molli
 Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Le infezioni di cute e tessuti molli SCELTE e STRATEGIE TERAPEUTICHE Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi Treatment of complicated skin and skin structure infections
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibacterials. Recent data on linezolid and daptomycin
 Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
Antibacterials Recent data on linezolid and daptomycin Patricia Muñoz, MD. Ph.D. (pmunoz@micro.hggm.es) Hospital General Universitario Gregorio Marañón Universidad Complutense de Madrid. 1 GESITRA Reasons
New Antibiotics for MRSA
 New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
LINEE GUIDA: VALORI E LIMITI
 Ferrara 28 novembre 2014 LINEE GUIDA: VALORI E LIMITI Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi EVIDENCE BIASED GERIATRIC MEDICINE Older patients with comorbid conditions
Ferrara 28 novembre 2014 LINEE GUIDA: VALORI E LIMITI Pierluigi Viale Clinica di Malattie Infettive Policlinico S. Orsola Malpighi EVIDENCE BIASED GERIATRIC MEDICINE Older patients with comorbid conditions
Antimicrobial Therapy
 Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Disclosure: Dr. Spach has no significant financial interest in any of the
Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Disclosure: Dr. Spach has no significant financial interest in any of the
ANTIBIOTICS USED FOR RESISTACE BACTERIA. 1. Vancomicin
 ANTIBIOTICS USED FOR RESISTACE BACTERIA 1. Vancomicin Vancomycin is used to treat infections caused by bacteria. It belongs to the family of medicines called antibiotics. Vancomycin works by killing bacteria
ANTIBIOTICS USED FOR RESISTACE BACTERIA 1. Vancomicin Vancomycin is used to treat infections caused by bacteria. It belongs to the family of medicines called antibiotics. Vancomycin works by killing bacteria
Skin and Soft Tissue Infections Emerging Therapies and 5 things to know
 2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
2011 MFMER slide-1 Skin and Soft Tissue Infections Emerging Therapies and 5 things to know Aaron Tande, MD Assistant Professor of Medicine October 27, 2017 Division of INFECTIOUS DISEASES 2011 MFMER slide-2
Antimicrobials Update
 Antimicrobials Update Rosie Amini, PharmD. BCPS Antimicrobial Stewardship Program Coordinator Swedish Medical Center Disclosures: Dr. Amini has no significant financial interest in any of the products
Antimicrobials Update Rosie Amini, PharmD. BCPS Antimicrobial Stewardship Program Coordinator Swedish Medical Center Disclosures: Dr. Amini has no significant financial interest in any of the products
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
MRSA What Are Our Treatment Options and How Do We Choose the Right One?
 MRSA What Are Our Treatment Options and How Do We Choose the Right One? Kristi Traugott, PharmD, BCPS Clinical Pharmacy Specialist Infectious Diseases University Health System San Antonio, TX October 25,
MRSA What Are Our Treatment Options and How Do We Choose the Right One? Kristi Traugott, PharmD, BCPS Clinical Pharmacy Specialist Infectious Diseases University Health System San Antonio, TX October 25,
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate
 Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Cefazolin vs. Antistaphyloccal Penicillins: The Great Debate Annie Heble, PharmD PGY2 Pediatric Pharmacy Resident Children s Hospital Colorado Microbiology Rounds March 22, 2017 Image Source: Buck cartoons
Scottish Medicines Consortium
 Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium tigecycline 50mg vial of powder for intravenous infusion (Tygacil ) (277/06) Wyeth 9 June 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium
 Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Scottish Medicines Consortium daptomycin 350mg powder for concentrate for solution for infusion (Cubicin ) Chiron Corporation Limited No. (248/06) 10 March 2006 The Scottish Medicines Consortium (SMC)
Considerations for antibiotic therapy. Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen
 Considerations for antibiotic therapy Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen Infective Endocarditis There will never be a cure for this malignant disease! Sir
Considerations for antibiotic therapy Christoph K. Naber Interventional Cardiology Heartcenter - Elisabeth Hospital Essen Infective Endocarditis There will never be a cure for this malignant disease! Sir
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
The new antistaphylococcal drugs (tigecycline, daptomycin, telavancin, ): is the future (really) shining?
: is the future (really) shining?") S. aureus: what do we need to know (and to do) in 2007? The new antistaphylococcal drugs (tigecycline, daptomycin, telavancin, ): is the future (really) shining? Françoise Van Bambeke Unité de Pharmacologie
S. aureus: what do we need to know (and to do) in 2007? The new antistaphylococcal drugs (tigecycline, daptomycin, telavancin, ): is the future (really) shining? Françoise Van Bambeke Unité de Pharmacologie
The role of new antibiotics in the treatment of severe infections: Safety and efficacy features
 The role of new antibiotics in the treatment of severe infections Safety and efficacy features Christian Eckmann Hannover, Germany The role of new antibiotics in the treatment of severe infections: Safety
The role of new antibiotics in the treatment of severe infections Safety and efficacy features Christian Eckmann Hannover, Germany The role of new antibiotics in the treatment of severe infections: Safety
MRSA across roads: new antibiotic options
 MRSA across roads: new antibiotic options Javier Garau, MD, PhD University of Barcelona 18th Infection and Sepsis Symposium, BUGS, MUGS AND DRUGS, Porto, 27th February 2013 DISCLOSURES I have accepted
MRSA across roads: new antibiotic options Javier Garau, MD, PhD University of Barcelona 18th Infection and Sepsis Symposium, BUGS, MUGS AND DRUGS, Porto, 27th February 2013 DISCLOSURES I have accepted
Empiric therapy for severe suspected Staphylococcus aureus infection
 Empiric therapy for severe suspected Staphylococcus aureus infection Salman Qureshi, MD McGill University Faculty of Medicine Department of Critical Care Medicine McGill University Health Centre Relevant
Empiric therapy for severe suspected Staphylococcus aureus infection Salman Qureshi, MD McGill University Faculty of Medicine Department of Critical Care Medicine McGill University Health Centre Relevant
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections
 for the treatment of Acinetobacter baumannii infections") ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust
 PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
PVL Staph aureusjust a skin/soft tissue problem? Layla Mohammadi Lead Pharmacist, Antimicrobials Lewisham Healthcare NHS Trust Neonatal Case History Neonate born at 26 +2 gestation Spontaneous onset of
Source: Portland State University Population Research Center (
 Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Methicillin Resistant Staphylococcus aureus (MRSA) Surveillance Report 2010 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Health Authority Updated:
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Background and Plan of Analysis
 ENTEROCOCCI Background and Plan of Analysis UR-11 (2017) was sent to API participants as a simulated urine culture for recognition of a significant pathogen colony count, to perform the identification
ENTEROCOCCI Background and Plan of Analysis UR-11 (2017) was sent to API participants as a simulated urine culture for recognition of a significant pathogen colony count, to perform the identification
Choose Your Own Antibiotic/Adventure Gram-Positive Style
 Disclosures Consultant for Cubist Pharmaceuticals, Inc Research support from Forest Laboratories Choose Your Own Antibiotic/Adventure Gram-Positive Style I have never seen Star Wars (But I m a big fan
Disclosures Consultant for Cubist Pharmaceuticals, Inc Research support from Forest Laboratories Choose Your Own Antibiotic/Adventure Gram-Positive Style I have never seen Star Wars (But I m a big fan
MRSA ventilatorassociated
 MRSA ventilatorassociated pneumonia Jean Chastre, M.D. www.reamedpitie.com Conflicts of interest Consulting or lecture fees: Medimmune/Astrazeneca, Bayer, Pfizer, Arsanis, Cubist/Merck, Basilea, Aridis,
MRSA ventilatorassociated pneumonia Jean Chastre, M.D. www.reamedpitie.com Conflicts of interest Consulting or lecture fees: Medimmune/Astrazeneca, Bayer, Pfizer, Arsanis, Cubist/Merck, Basilea, Aridis,
Duration of antibiotic therapy:
 Duration of antibiotic therapy: How low can you go? Thomas Holland, MD Hilton Head, SC July 2017 Disclosures Consulting: The Medicines Company, Basilea Pharmaceutica Adjudication committee: Achaogen Grant
Duration of antibiotic therapy: How low can you go? Thomas Holland, MD Hilton Head, SC July 2017 Disclosures Consulting: The Medicines Company, Basilea Pharmaceutica Adjudication committee: Achaogen Grant
Burden of disease of antibiotic resistance The example of MRSA. Eva Melander Clinical Microbiology, Lund University Hospital
 Burden of disease of antibiotic resistance The example of MRSA Eva Melander Clinical Microbiology, Lund University Hospital Discovery of antibiotics Enormous medical gains Significantly reduced morbidity
Burden of disease of antibiotic resistance The example of MRSA Eva Melander Clinical Microbiology, Lund University Hospital Discovery of antibiotics Enormous medical gains Significantly reduced morbidity
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Critical impact of antimicrobial resistance
 New Antibiotics Kurt B. Stevenson, MD, MPH Professor of Medicine and Epidemiology Division of Infectious Diseases Department of Internal Medicine The Ohio State University College of Medicine Critical
New Antibiotics Kurt B. Stevenson, MD, MPH Professor of Medicine and Epidemiology Division of Infectious Diseases Department of Internal Medicine The Ohio State University College of Medicine Critical
Is Cefazolin Inferior to Nafcillin for Treatment of Methicillin-Susceptible Staphylococcus aureus Bacteremia?
 ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Nov. 2011, p. 5122 5126 Vol. 55, No. 11 0066-4804/11/$12.00 doi:10.1128/aac.00485-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Is Cefazolin
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Nov. 2011, p. 5122 5126 Vol. 55, No. 11 0066-4804/11/$12.00 doi:10.1128/aac.00485-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Is Cefazolin
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16
 Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
Northwestern Medicine Central DuPage Hospital Antimicrobial Criteria Updated 11/16/16 These criteria are based on national and local susceptibility data as well as Infectious Disease Society of America
SIVEXTRO (tedizolid phosphate) oral tablet ZYVOX (linezolid) oral suspension and tablet
 oral tablet ZYVOX (linezolid) oral suspension and tablet") ZYVOX (linezolid) oral suspension and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
ZYVOX (linezolid) oral suspension and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
Zyvox. Zyvox (linezolid) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.20 Subject: Zyvox Page: 1 of 7 Last Review Date: March 18, 2016 Zyvox Description Zyvox (linezolid)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.20 Subject: Zyvox Page: 1 of 7 Last Review Date: March 18, 2016 Zyvox Description Zyvox (linezolid)
RESISTANT PATHOGENS. John E. Mazuski, MD, PhD Professor of Surgery
 RESISTANT PATHOGENS John E. Mazuski, MD, PhD Professor of Surgery Disclosures Contracted Research: AstraZeneca, Bayer, Merck. Advisory Boards/Consultant: Allergan (Actavis, Forest Laboratories), AstraZeneca,
RESISTANT PATHOGENS John E. Mazuski, MD, PhD Professor of Surgery Disclosures Contracted Research: AstraZeneca, Bayer, Merck. Advisory Boards/Consultant: Allergan (Actavis, Forest Laboratories), AstraZeneca,
Cellulitis. Assoc Prof Mark Thomas. Conference for General Practice Auckland Saturday 28 July 2018
 Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
What s next in the antibiotic pipeline?
 What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process High Priority
 MEASURE TYPE: Process High Priority") Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Healthcare Associated
Quality ID #407: Appropriate Treatment of Methicillin-Susceptible Staphylococcus Aureus (MSSA) Bacteremia National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Healthcare Associated
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Principles of Antimicrobial Therapy
 Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
Principles of Antimicrobial Therapy Doo Ryeon Chung, MD, PhD Professor of Medicine, Division of Infectious Diseases Director, Infection Control Office SUNGKYUNKWAN UNIVERSITY SCHOOL OF MEDICINE CASE 1
The role of Ceftaroline for the treatment of CAP (Community acquired pneumonia)
") The role of Ceftaroline for the treatment of CAP (Community acquired pneumonia) S t e l i o s A s s i m a k o p o u l o s Assistant Professor of Internal Medicine Dept. of Medicine, School of Health Sciences
The role of Ceftaroline for the treatment of CAP (Community acquired pneumonia) S t e l i o s A s s i m a k o p o u l o s Assistant Professor of Internal Medicine Dept. of Medicine, School of Health Sciences
Does Screening for MRSA Colonization Have A Role In Healthcare-Associated Infection Prevention Programs?
 Does Screening for MRSA Colonization Have A Role In Healthcare-Associated Infection Prevention Programs? John A. Jernigan, MD, MS Division of Healthcare Quality Promotion Centers for Disease Control and
Does Screening for MRSA Colonization Have A Role In Healthcare-Associated Infection Prevention Programs? John A. Jernigan, MD, MS Division of Healthcare Quality Promotion Centers for Disease Control and
Class Review: Oxazolidinone Antibiotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Novel therapies & the role of early switch and early discharge protocols for management of MRSA infections
 Novel therapies & the role of early switch and early discharge protocols for management of MRSA infections Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain
Novel therapies & the role of early switch and early discharge protocols for management of MRSA infections Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Discussion Points. Decisions in Selecting Antibiotics
 Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Antibiotics in Acute Care Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
One-Hit Wonders: A New Era of Antibiotics?
 One-Hit Wonders: A New Era of Antibiotics? Patrick Wieruszewski, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds November 1, 2016 2016 MFMER slide-1 Objectives Identify advantages and disadvantages
One-Hit Wonders: A New Era of Antibiotics? Patrick Wieruszewski, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds November 1, 2016 2016 MFMER slide-1 Objectives Identify advantages and disadvantages
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering
 SMC No. (650/10) Bayer Schering") moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
ESCMID Online Lecture Library. by author
 Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Tel: Fax:
 CONCISE COMMUNICATION Bactericidal activity and synergy studies of BAL,a novel pyrrolidinone--ylidenemethyl cephem,tested against streptococci, enterococci and methicillin-resistant staphylococci L. M.
CONCISE COMMUNICATION Bactericidal activity and synergy studies of BAL,a novel pyrrolidinone--ylidenemethyl cephem,tested against streptococci, enterococci and methicillin-resistant staphylococci L. M.
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Safety of an Out-Patient Intravenous Antibiotics Programme
 Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Safety of an Out-Patient Intravenous Antibiotics Programme Chan VL, Tang ESK, Leung WS, Wong L, Cheung PS, Chu CM Department of Medicine & Geriatrics United Christian Hospital Outpatient Parental Antimicrobial
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Therapeutic options: what s new in the pipeline?
 Therapeutic options: what s new in the pipeline? Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain Drug Research Institute, Université catholique de Louvain,
Therapeutic options: what s new in the pipeline? Paul M. Tulkens, MD, PhD Cellular and Molecular Pharmacology & Centre for Clinical Pharmacy Louvain Drug Research Institute, Université catholique de Louvain,
Introduction to Pharmacokinetics and Pharmacodynamics
 Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
CEFTAROLINE FOSAMIL (ZINFORO )
") Page 1 London New Drugs Group APC/DTC Briefing Document CEFTAROLINE FOSAMIL (ZINFORO ) Contents Summary 1 Background 3 Ceftaroline 4 Clinical efficacy 6 FOCUS 1 and 2 6 CANVAS 1 and 2 9 Health economics
Page 1 London New Drugs Group APC/DTC Briefing Document CEFTAROLINE FOSAMIL (ZINFORO ) Contents Summary 1 Background 3 Ceftaroline 4 Clinical efficacy 6 FOCUS 1 and 2 6 CANVAS 1 and 2 9 Health economics
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES
 AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
The Impact of meca Gene Testing and Infectious Diseases Pharmacists. Intervention on the Time to Optimal Antimicrobial Therapy for ACCEPTED
 JCM Accepts, published online ahead of print on 7 May 2008 J. Clin. Microbiol. doi:10.1128/jcm.00801-08 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
JCM Accepts, published online ahead of print on 7 May 2008 J. Clin. Microbiol. doi:10.1128/jcm.00801-08 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland
 Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
Recommendations for Implementation of Antimicrobial Stewardship Restrictive Interventions in Acute Hospitals in Ireland A report by the Hospital Antimicrobial Stewardship Working Group, a subgroup of the
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
Lefamulin: a novel pleuromutilin antibiotic class George Dimopoulos MD, PhD, FCCP, FCCM, FECMM
 : a novel pleuromutilin antibiotic class George Dimopoulos MD, PhD, FCCP, FCCM, FECMM Department of Critical Care, University Hospital ATTIKON National and Kapodistrian University of Athens, Medical School
: a novel pleuromutilin antibiotic class George Dimopoulos MD, PhD, FCCP, FCCM, FECMM Department of Critical Care, University Hospital ATTIKON National and Kapodistrian University of Athens, Medical School
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
National Clinical Guideline Centre Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults
 National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
National Clinical Guideline Centre Antibiotic classifications Pneumonia Diagnosis and management of community- and hospital-acquired pneumonia in adults Clinical guideline 191 Appendix N 3 December 2014
ECHO: Management of URIs. Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018
 ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
STAPHYLOCOCCI: KEY AST CHALLENGES
 Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
Romney Humphries, PhD D(ABMM) Section Chief, UCLA Clinical Microbiology Los Angeles CA rhumphries@mednet.ucla.edu STAPHYLOCOCCI: KEY AST CHALLENGES THE CHALLENGES detection of penicillin resistance detection
Antibiotic Prophylaxis Update
 Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
Antibiotic Prophylaxis Update Choosing Surgical Antimicrobial Prophylaxis Peri-Procedural Administration Surgical Prophylaxis and AMS at Epworth HealthCare Mr Glenn Valoppi Dr Trisha Peel Dr Joseph Doyle
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens
 The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance
 Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
Initial Management of Infections in the Era of Enhanced Antimicrobial Resistance Robert C Welliver Sr, MD Hobbs-Recknagel Endowed Chair in Pediatrics Chief, Pediatric infectious Diseases Children s Hospital
New Antibiotics & New Insights into Old Antibiotics
 New Antibiotics & New Insights into Old Antibiotics Louisiana Chapter of the American Academy of Pediatrics August 18, 2018 Baton Rouge, Louisiana John Bradley MD Rady Children s Hospital San Diego University
New Antibiotics & New Insights into Old Antibiotics Louisiana Chapter of the American Academy of Pediatrics August 18, 2018 Baton Rouge, Louisiana John Bradley MD Rady Children s Hospital San Diego University
Fluoroquinolones in 2007: the Angels, the Devils, and What Should the Clinician Do?
 Fluoroquinolones in 2007: the Angels, the Devils, and What Should the Clinician Do? David C. Hooper, M.D. Division of Infectious Diseases Infection Control Unit Massachusetts General Hospital Harvard Medical
Fluoroquinolones in 2007: the Angels, the Devils, and What Should the Clinician Do? David C. Hooper, M.D. Division of Infectious Diseases Infection Control Unit Massachusetts General Hospital Harvard Medical
MRSA. ( Staphylococcus aureus; S. aureus ) ( community-associated )
 ( community-associated )") 005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
005 16 190-194 ( Staphylococcus aureus; S. aureus ) ( community-associated ) ( -susceptible Staphylococcus auerus; MSSA ) ( -resistant Staphylococcus auerus; ) ( ) ( -lactam ) ( glycopeptide ) ( Staphylococcus
Rise of Resistance: From MRSA to CRE
 Rise of Resistance: From MRSA to CRE Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine SUPERBUGS (AKA MDROs) MRSA Methicillin-resistant S. aureus Evolution of Drug Resistance
Rise of Resistance: From MRSA to CRE Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine SUPERBUGS (AKA MDROs) MRSA Methicillin-resistant S. aureus Evolution of Drug Resistance
Period of study: 12 Nov 2002 to 08 Apr 2004 (first subject s first visit to last subject s last visit)
") Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Ca-MRSA Update- Hand Infections. Washington Hand Society September 19, 2007
 Ca-MRSA Update- Hand Infections Washington Hand Society September 19, 2007 Resistant Staph. Aureus Late 1940 s -50% S.Aureus resistant to PCN 1957-80/81 strain- of S.A. highly virulent and easily transmissible
Ca-MRSA Update- Hand Infections Washington Hand Society September 19, 2007 Resistant Staph. Aureus Late 1940 s -50% S.Aureus resistant to PCN 1957-80/81 strain- of S.A. highly virulent and easily transmissible
Consequences of Antimicrobial Resistant Bacteria. Antimicrobial Resistance. Molecular Genetics of Antimicrobial Resistance. Topics to be Covered
 Antimicrobial Resistance Consequences of Antimicrobial Resistant Bacteria Change in the approach to the administration of empiric antimicrobial therapy Increased number of hospitalizations Increased length
Antimicrobial Resistance Consequences of Antimicrobial Resistant Bacteria Change in the approach to the administration of empiric antimicrobial therapy Increased number of hospitalizations Increased length
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali. Lec 1
 Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Role of IV Therapy in Bone and Joint Infection
 Role of IV Therapy in Bone and Joint Infection Andrew Seaton ID Consultant, Queen Elizabeth University Hospital Lead Doctor Antimicrobial Management Team, NHS GGC @raseaton66 OPAT The IVnOAT Perspective
Role of IV Therapy in Bone and Joint Infection Andrew Seaton ID Consultant, Queen Elizabeth University Hospital Lead Doctor Antimicrobial Management Team, NHS GGC @raseaton66 OPAT The IVnOAT Perspective
Mono- versus Bitherapy for Management of HAP/VAP in the ICU
 Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
MICHAEL J. RYBAK,* ELLIE HERSHBERGER, TABITHA MOLDOVAN, AND RICHARD G. GRUCZ
 ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Apr. 2000, p. 1062 1066 Vol. 44, No. 4 0066-4804/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. In Vitro Activities of Daptomycin,
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Apr. 2000, p. 1062 1066 Vol. 44, No. 4 0066-4804/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. In Vitro Activities of Daptomycin,
ANTIMICROBIAL SUSCEPTIBILITY CHARACTERIZING SUSCEPTIBILITY PATTERNS OF MSSA ASSOCIATED WITH SURGICAL WOUND INFECTIONS
 ASSOCIATED WITH SURGICAL WOUND INFECTIONS Specimen ES-02 was designated as a "surgical wound culture" to be identified to the species level and tested for antimicrobial susceptibility. 1-4 The culture
ASSOCIATED WITH SURGICAL WOUND INFECTIONS Specimen ES-02 was designated as a "surgical wound culture" to be identified to the species level and tested for antimicrobial susceptibility. 1-4 The culture
S aureus infections: outpatient treatment. Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium
 S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
S aureus infections: outpatient treatment Dirk Vogelaers Dept of Infectious Diseases University Hospital Gent Belgium Intern Med J. 2005 Feb;36(2):142-3 Intern Med J. 2005 Feb;36(2):142-3 Treatment of
GUIDE TO INFECTION CONTROL IN THE HOSPITAL
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 43: Staphylococcus Aureus Authors J. Pierce, MD M. Edmond, MD, MPH, MPA M.P. Stevens, MD, MPH Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key