Overview of GRACE WP8 and. How long does it take for adults consulting with acute cough to get better, and are they helped by antibiotic treatment?
|
|
|
- Lynn Boyd
- 5 years ago
- Views:
Transcription
1 GRACE WP8 symposium, Warsaw, February 2010 The management of adults with acute cough in Europe - GRACE WP8 answers to key clinical questions Overview of GRACE WP8 and How long does it take for adults consulting with acute cough to get better, and are they helped by antibiotic treatment? Chris Butler, Theo Verheij, Paul Little, Herman Goossens and the GRACE-01 and GRACE-02 Study Teams


2 GRACE-01: Objectives To establish a collaboration of primary care research networks in Europe To describe current presentation, investigation, management and outcomes for patients with community-acquired LRTI in primary care across and within European Countries


3 Clinician beliefs on factors contributing GRACE-02 to variation in antibiotic use & resistance Objective: To achieve a micro-level understanding of the contextual factors that influence antibiotic prescription and other forms of management for Primary Care patients with LRTI Patient beliefs on factors contributing to variation in antibiotic use & resistance
4 GRACE 02 Methods Interviews conducted Network Clinician Patient Antwerp Balatonfüred Barcelona Cardiff 8 10 Lodz Milan Southampton 6 9 Tromsø 7 10 Utrecht TOTAL Framework approach (Ritchie & Spencer 1994)
5 Sample: GRACE 01: METHODS Enrolment of consecutive patients consulting with acute ( 28 days duration) cough as the main symptom. 2 recruitment periods of 1 month (Oct/06, Feb/07) Target 300 patients per network. ~4200 patients in total. Sample size based on requirements for within network analysis.
6 GRACE 01 METHODS Data capture: CRF (clinician completed) Demographics, history, presentation, clinical findings, usual investigations, management, referral, perceived expectations etc. One month diary (patient completed) Expectations, hopes & beliefs of antibiotics, reasons for consulting, daily symptoms, taking of medications, healthcare resource use. Data collection coordinated within each network, with data management via a secure online system
7 GRACE 01 METHODS Analysis Descriptive analysis corrected for clustering at the practice level Two level logistic regression modelling of antibiotic prescribing Three level ARMA modelling of patient outcome with time fitted as a cubic polynomial
8 GRACE 01: Participant Flow Chart Patients Recruited and Registered (n=3402) Excluded Patients (n=4) Reason: Patients did not meet eligibility criteria Case Record Form (CRF) (n=3368) 99% Patient Diary (n=2714) 80% CRF and Diary Returned N = 2690 (79%)
9 Patient Characteristics 37% Male Average age 46.0 (sd 16.40) 98% seen at the office/surgery Co morbidities 15% existing respiratory condition 8% heart related illness 4% diabetes Presenting symptoms (3 most common) Cough (100%) Generally unwell (80%) Phlegm production (77%) Average temperature 36.8ºC (se 0.72) Average of 7.6 symptoms per patient reported present, out of max of 14


10 Patient Characteristics Jonkoping has the highest average symptom scores Mataro, Milan & Barcelona have the lowest Symptom severity Median 31 (0 to 81)
11 Clinician Management Antibiotics prescribed 53% 12% advised delay (median duration 3 days) Median duration of course of antibiotics 7 days Patients were unwell for a median of 5 days before consulting with a clinician
12 Clinician Management Types of Antibiotic Prescribed Sulfonamide/Trimethopri m Other Phenoxymethyl Penicillin Quinolone Southampton Helsinki Utrecht Jonkoping Rotenburg Mataro Tromso Antwerp Barcelona Network Cephalosporin Tetracycline Co-Amoxiclav Macrolide/Lincosamide Amoxicillin Cardiff Lodz Milano Balatonfured Bratislava Percentagee
13 Clinician Management: antibiotic prescribing
14 Patient Outcome: Symptom trajectory over time Min Max Day 7 Day 7 Model Balatonfured Model Balatonfured 10.6 Cardiff 7.4 Mataro Model 3 Not prescribed 4.2 Balatonfured 7.3 Mataro Prescribed 4.3 Balatonfured 7.4 Mataro Adjusted for age, co morbidity and symptom severity
15 Survival modelling Models the time to symptom resolution (total symptom severity score of zero) controlling for casemix Naturally accounts for censoring Survival analysis equivalent of hierarchical modelling is frailty modelling
16
17 GRACE: WP8 Study Team GRACE Network Lucy Brookes-Howell Curt Brugman Chris Butler Jo Coast Samuel Coenen Lucy Cooper Dave Gillespie Herman Goosens Giles Greene Kerry Hood Mark Kelly Frank Leus Paul Little Jacqui Nuttall Richard Smith Robert Veen Theo Verheij Primary Care Networks Mel Davies Peter Edwards Mike Moore Tricia Worby Alicia Borras Antoni Torres Matteu Serra Jordi Almirall Iris Hering Tom Schaberg Judit Holczerné Zseraldina Arvai Bernadette Kovaks Kristien Dirven Maciek Godycki-Cwirko Magdalena Muras Paolo Tarsia Francesco Blasi Sigvard Molstad Chrisina Lannering Hasse Melbye Carol Pascoe Kristin Alise Jakobsen Ulla-Maija Rautakorpi Kirsi Valve Zuzana Bielicka Helena Hupkova
18 Discoloured sputum and feeling unwell does not predict benefit from antibiotic treatment for acute cough: a prospective study in 13 European countries Chris Butler (WP8) Mark Kelly (WP8) Kerenza Hood (WP8) Tom Schaberg (Rotenberg) Hasse Melbye (Tromso) Mateu Sierra-Prat Francesco Blasi (Milan) Paul Little (Southampton: WP10) Theo Verheij (Utrecht; WP9) Sigvard Mölstad (Jönköping) Maciek Godycki-Cwirko (Lodz) Peter Edwards (Cardiff) Jordi Almirall (Mataro) Antoni Torres (Barcelona) Ulla-Maija Rautakorpi (Helsinki) Jacqui Nuttall (WP8) Herman Goossens (WP1) Samuel Coenen (Antwerp; WP1)
19 Rapid response to the BMJ paper I am not surprised at these findings of the GRACE group. Antibiotics in the otherwise healthy are only needed if the patient feels unwell or has purulent phlegm.
20 Purulent sputum & feeling generally unwell 1. Do patients with discoloured sputum or feeling generally unwell receive more antibiotics? 2. Was antibiotic treatment associated with patient recovery for those with these symptoms?
21 Yellow Sputum Green Sputum Feeling Feeling % (n) % (n) moderately severely unwell unwell % (n) % (n) Cardiff 21.4 (37) 37.6 (65) 47.4 (82) 19.7 (34) Southampton 18.0 (25) 34.5 (48) 43.2 (60) 12.9 (18) Utrecht 20.6 (32) 25.8 (40) 35.5 (55) 7.7 (12) Barcelona 13.7 (21) 19.6 (30) 18.3 (28) 2.0 (3) Mataro 21.0 (34) 22.2 (36) 22.2 (36) 2.5 (4) Rotenburg 28.7 (49) 17.5 (30) 40.4 (69) 21.6 (37) Balatonfured 33.9(108) 6.9 (22) 39.5(126) 5.6 (18) Antwerpen 30.3 (37) 12.3 (15) 42.6 (52) 11.5 (14) Lodz 28.9 (63) 9.2 (20) 55.5(121) 17.0 (37) Milan 30.5 (43) 5.7 (8) 27.7 (39) 6.4 (9) Jönköping 36.1 (66) 15.3 (28) 49.2 (90) 27.3 (50) Tromsö 23.4 (32) 30.7 (42) 48.2 (66) 5.8 (8) Helsinki 34.9 (29) 24.1 (20) 32.5 (27) 3.6 (3) Bratislava 23.6 (62) 17.9 (47) 36.5 (96) 4.6 (12)
22 Analysis Analysis controlled for - clinician recorded symptoms - sputum colour - temperature - age - co-morbidities (cardiovascular, respiratory including COPD, and COPD on its own, and diabetes) - the number of days waited before presentation - smoking status - network
23 Results Those producing normal sputum (clear/white) were not more likely to be prescribed than those not producing sputum (OR: 0.95, 95% CI: [0.61,1.48]) Those producing discoloured sputum were more likely to be prescribed than those not producing sputum (OR: 3.2, 95% CI: [2.1, 5.0]) Those feeling generally unwell (mild, moderate or severe) were not prescribed more frequently than those without
24 Patient outcome results Those who the clinician recorded as feeling generally unwell (mild, moderate or severe) had higher self-reported symptom severity scores at baseline recovered marginally faster than those not feeling generally unwell Antibiotic prescription was not associated with recovery rate for those: feeling generally unwell (any level) yellow sputum green sputum yellow/green sputum and feeling generally unwell
25 Recovery trajectories for each subgroup
26 Conclusion Discoloured sputum does influence clinician prescribing. Feeling generally unwell does not. There was no association between antibiotic prescribing and patient recovery for any patient subgroup investigated
27 Antibiotic class is not associated with recovery from acute cough in adults presenting to primary care: results from the GRACE 13-country prospective study Chris Butler (WP8) Kerry Hood (WP8) Mark Kelly (WP8) Joseph Wood (WP8) Jacqui Nuttall (WP8) Samuel Coenen (Antwerp; WP1) Helena Hupkova (Balatonfured) Antoni Torres (Barcelona) Zuzana Bielicka (Bratislava) Peter Edwards (Cardiff) Ulla-Maja Rautakorpi (Helsinki) Sigvard Mölstad (Jönköping) Maciek Godycki-Cwirko (Lodz) Jordi Almirall (Mataro) Francesco Blasi (Milan) Tom Schaberg (Rotenberg) Paul Little (Southampton: WP10) Hasse Melbye (Tromso) Theo Verheij (Utrecht; WP9) Herman Goossen (WP1)
28 BMJ paper summary There is considerable variation in antibiotic prescribing throughout Europe Self-reported symptom scores are not Self-reported symptom scores are not meaningfully associated with antibiotic prescription after controlling for clinical presentation
29 Aim To investigate whether treatment with a particular antibiotic class is associated with either symptom resolution or time until patients report they felt recovered compared with no antibiotic treatment or treatment with any antibiotic
30 Antibiotic class British National Formulary Classification Tetracyclines Amoxicillin Cephalosporins Sulfonamides/Trimethoprim Macrolides/Lincosamides Quinolones Penicillin Co-amoxiclav Other
31 Diary responses
32 Comparing with no AB treatment Intercept Beta p-value Interaction with time Beta p-value Tetracyclines Penicillin Amoxicillin Co-amoxiclav Cephalosporins Sulfonamides/Trimethoprim Macrolides/Lincosamides Quinolones Other
33 Comparing with overall average AB treatment Coefficient Interaction with time Interaction with time squared Beta p-value Beta p-value Beta p-value Tetracyclines Penicillin Amoxicillin Co-amoxiclav Cephalosporins Sulfonamides/Trimethoprim Macrolides/Lincosamides Quinolones
34 Day Felt Recovered Analysis Patients were asked Overall, on what day did you feel recovered The analysis controlled for - clinician recorded symptoms - sputum type - temperature - age - co-morbidities (cardiovascular, respiratory & diabetes) - the number of days waited before presentation - smoking status - network
35 Comparison with no treatment
36 Comparison with any antibiotic treatment
37 Conclusion No meaningful differences in symptom severity scores between those prescribed different antibiotic classes No differences between day felt recovered between those prescribed different antibiotic classes
38 Compared with no antibiotic treatment Antibiotic class Days Lower 95% limit Upper 95% limit Tetracyclines Amoxicillin Cephalosporins Sulfonamides/Trimethopr im Macrolides/Lincosamides Quinolones Penicillin Co-amoxiclav Other
39 Compared with any antibiotic treatment Antibiotic class Days Lower 95% limit Upper 95% limit Tetracyclines Amoxicillin Cephalosporins Sulfonamides/Trimethopr im Macrolides/Lincosamides Quinolones Penicillin Co-amoxiclav
40 Work package 8: GRACE-01 Antibiotic prescribing congruence to European Respiratory Society guidelines for LRTI: An observational study in 13 countries Joe Wood and the GRACE-01 Study Team Department of Primary Care and Public Health Cardiff University
41 Aims Are the first choice antibiotics being prescribed? Are they being prescribed to the right patients? Is the antibiotic treatment received associated with recovery?
42 European Respiratory Society (ERS) Guidelines - Antibiotic Type Preferred Tetracycline Amoxicillin Alternatives Macrolides Co-amoxiclav Levofloxacin Moxifloxacin
43 European Respiratory Society (ERS) Guidelines - Antibiotic Treatment Suspected or definite pneumonia Exacerbation of COPD Aged over 75 years with fever Cardiac failure Insulin-dependent diabetes mellitus Serious neurological disorder
44 Modelling the guidelines Suspected or definite pneumonia (Must have an acute cough and one of; new focal chest sign, dyspnoea, tachypnoea, fever lasting 4 days) Acute Cough Cough 1.New Focal Chest Sign Diminished Vesicular Breathing Crackles Rhonchi 2.Dyspnoea Shortness of breath 3.Tachypnoea Respiratory rate (breaths per minute) > 20 4.Fever Lasting 4 days How many days were you unwell before you saw your GP or nurse for this cough? Temperature > 37.8 c ERS Guideline CRF Data
45 Modelling the guidelines Exacerbation of COPD (Must have COPD and all of; Increased dyspnoea; Increased sputum volume; And increased sputum purulence) COPD COPD -Increased dyspnoea Shortness of breath -Increased sputum volume Phlegm production -Increased sputum purulence If producing phlegm, what colour? (Yellow, Green, Bloodstained) Severe COPD Pulse Oximitery (% saturation) < 90 ERS Guideline CRF Data
46 Modelling the guidelines Aged 75 yrs and fever (Must have both; Aged over 75 yrs; And fever) Cardiac Failure Insulin-dependent diabetes mellitus (Must have both; Diabetes; And Insulin) Serious Neurological Disorder Aged over 75 yrs Age Fever Temperature > 37.8 c Cardiac Failure Heart Failure Insulin-dependent diabetes mellitus Diabetes Insulin Serious Neurological Disorder n/a ERS Guideline CRF Data
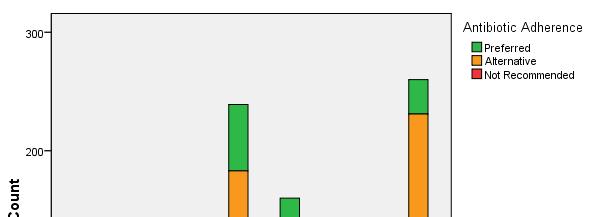
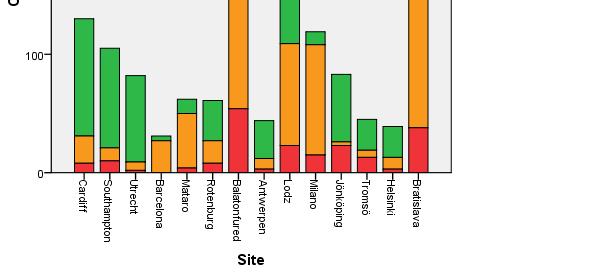
47 Results - Antibiotic Type A first choice antibiotic was prescribed in 41% (594) of antibiotic treatment cases 45% (662) patients prescribed an antibiotic received an alternative agent suggested by the ERS guidelines Not recommended antibiotics were prescribed in 14% (204) of cases Range of 1 st Choice: Utrecht 89% (73), Milan 9% (11) {CRF: n=3368, 43% (761) 1 st choice}
48 Results - Antibiotic Type
49 Results - Antibiotic Type Preferred (Amoxicillin and Tetracycline) Alternative (Macrolides, Co-amoxiclav, Levofloxacin and Moxifloxacin) Not Recommended (Others) Cardiff 76.2 (99) 17.7 (23) 6.2 (8) (130) Southampton 80.0 (84) 10.5 (11) 9.5 (10) (105) Utrecht 89.0 (73) 8.5 (7) 2.4 (2) (82) Barcelona 12.9 (4) 87.1 (27) 0.0 (0) (31) Mataro 19.4 (12) 74.2 (46) 6.5 (4) (62) Rotenburg 55.7 (34) 31.1 (19) 13.1 (8) (61) Balatonfured 23.4 (56) 54.0 (129) 22.6 (54) (239) Antwerpen 72.7 (32) 20.5 (9) 6.8 (3) (44) Lodz 31.9 (51) 53.8 (86) 14.4 (23) (160) Milano 9.2 (11) 78.2 (93) 12.6 (15) (119) Jönköping 68.7 (57) 3.6 (3) 27.7 (23) (83) Tromsö 57.8 (26) 13.3 (6) 28.9 (13) (45) Helsinki 66.7 (26) 25.6 (10) 7.7 (3) (39) Bratislava 11.2 (29) 74.2 (193) 14.6 (38) (260) Total 40.7 (594) 45.3 (662) 14.0 (204) (1460) Total
50 Results - Antibiotic Treatment Antibiotics prescribed to 54% (1464) of patients If the guidelines were strictly followed approximately 71% (1915) would have been prescribed 64% (1217/1915) of guideline indicated were actually prescribed antibiotics
51 Future Work - Outcomes Did those who received guideline congruent prescribing recover any faster? Hierarchical model Duration of illness based on symptom severity scores {Also looking into the working diagnosis given by clinicians}
52 Future Work - Outcomes What is the best reference category? Guideline Congruent Yes Guideline Incongruent Antibiotic? Partially Congruent No Guideline Congruent Guideline Incongruent
53 Summary One of the preferred or alternative agents is prescribed in most cases of antibiotic prescribing Current guidelines suggest antibiotics are possibly under prescribed There may be no association between congruent prescribing and recovery rate
54 Thank you, any questions?

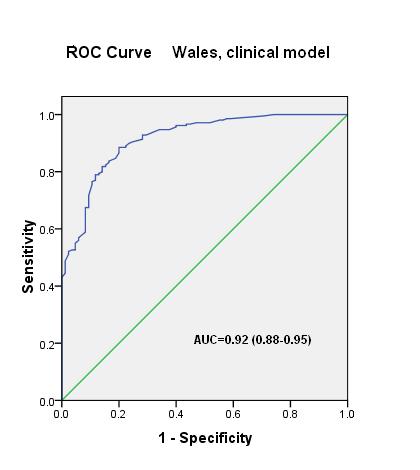
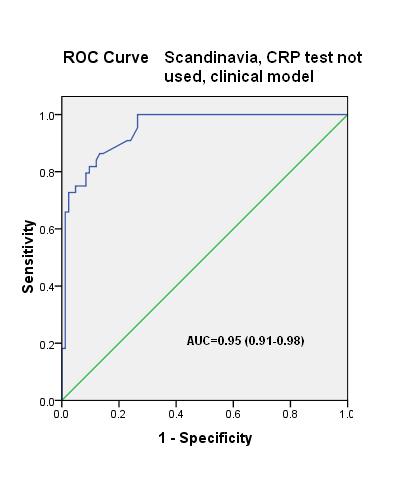
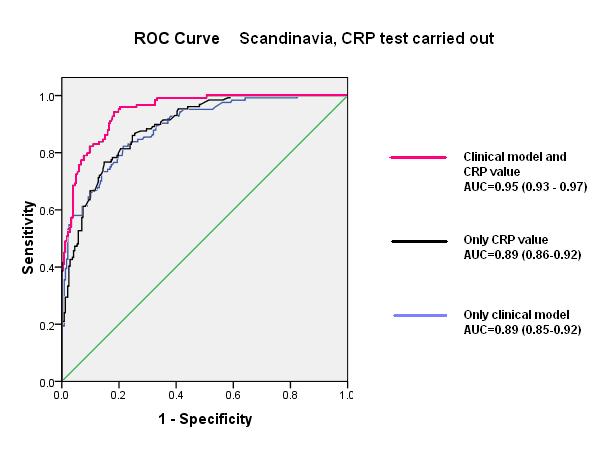
55 Influence of CRP testing and clinical findings on antibiotic prescribing in adults presenting with acute cough in primary care K A Jakobsen, H Melbye, M J Kelly, C Ceynova, S Mölstad, K Hood, C C Butler
56 Patients and CRP testing 503 Scandinavian patients and 300 Welsh patients were included The CRP test was used in all Scandinavian practices and 371 (74%) were tested
57 Sweden and Norway CRP taken (n=372) Sweden and Norway CRP not taken (n=131) Wales (n=300) Age 65 years 67 (18%) 17 (13%) 51 (17%) Any co-morbidity 102 (28%) 19 (14%)* 97 (32%) Any abnormal lung sound 168 (46%) 40 (30%)* 156 (52%) Perceived patient preference of antibiotics Patients treated with antibiotics 61(16%) 23 (18%) 164 (55%)** 129 (35%) 46 (36%) 209 (70%)**
58 When CRP test was used Antibiotics prescribed in % by CRP value % < CRP mg/l
59 Predictors for prescribing antibiotics Odds ratios (logistic regression) Sweden and Norway CRP taken (n=372) Sweden and Norway CRP not taken (n=131) Wales (n=300) Coloured phlegm 1.70 ( ) 3.41 ( ) 3.30 ( ) Crackles 9.51 ( ) ( ) ( ) CRP 50 mg/l ( ) Perceived patient preference of antibiotics ( ) ( ) 6.18 ( )
60
61 Conclusion Clinicians weight clinical findings differently in the decision whether or not to prescribe antibiotics for acute cough. When a CRP test is performed, the CRP result is strongly emphasized. The lower antibiotic prescribing rate in the Scandinavian countries suggests that evidence based CRP testing could usefully be extended to primary care settings outside Scandinavia.
62 Clinical and non-clinical determinants of prescribing


63 Interviews conducted Network Clinician Patient Antwerp Balatonfüred Barcelona Cardiff 8 10 Lodz Milan Southampton 6 9 Tromsø 7 10 Utrecht TOTAL
64 Clinician beliefs on factors contributing to variation in antibiotic use 1. Clinical factors 2. Non-clinical: Factors linked with particular network 3. Non-clinical: Factors linked to clinician characteristics
65 1. Clinical factors: Physical exam Theme Sub-theme Description Physical examination Chest examination Temperature Signs of URTI Cough General illness Vital signs Breathing Auscultation, percussion Throat, nose, ears, eyes Type of cough Heartbeat/rate, blood pressure, pulse Rapid breathing Chest exam: Above all, I would examine him by auscultationto check for rhonchus and crepitations, and according to this, I would make a diagnosis and prescribe a treatment (Barcelona, Clinician 17) Temperature: Temperaturethat s actually not a routine job for me...often I will only do it...when I see, they don t look too good after all (Antwerp, Clinician 119) General illness: By simply watchinga patient with a clinical look you can also see how ill a patient is. Of course, that is vague but you do get a better impression than when you do not see that patient of the extent of the illness (Utrecht, Clinician 100) Vital signs: And then, something I do almost routine, after all people expect that very often, is indeed check the pulse and take the blood pressure (Antwerp, Clinician 119)
66 Theme Patient s history The reason for prescribing is based upon Sub-theme combinations of signs and symptoms Description of current illness Medical history 1. Clinical factors: Patient s history Symptoms there is no individual cardinal symptom Illness course that says I will treat (Cardiff, Clinician 42) Comorbidity Cough, fever, mucus, breathlessness Duration, severity, deterioration, general illness, previous actions There take are Recurring into social account factors RTIs patient s you ll get case still, history, whether poorly this nourished the patient with any chronic illness, Age individuals who you may well especially give an respiratory antibiotic system to because illness, you feel whether Allergy that generally it may prevent healthy further to which problems. the infection Even happened if it s Medication not going completely to alter by this accident viral illness, (Lodz, that Clinician they Family are 50) at history risk of pieces CAP because of jigsaw, they are Smoking who they are building because up of their picture nourishment status or Alcohol use of whatever the diagnosis and so(cardiff, Clinician 28) that can have an impact (Cardiff, Clinician 42) Social history Living conditions Community Work environment
67 1. Clinical factors: Tests/investigations Theme Sub-theme Description Tests/ Investigations CRP (Tromsø) X-rays and CRP (all other networks) Near patient test, immediate impact on management, routine practice Combination of symptoms, severity, uncertainty, patient expectations, undesirable illness course CRP: There was just more of a struggle before. What has really changed though is CRP. That I can, there and then, get an answer, in context with the medical history and findings...so CRP has really made a difference (Tromsø, Clincian 193) X-rays/blood test: I would do that when I find discrepancy between two different findings of X-rays: I do not work with photos a lot. When I think someone is sick, then I give antibiotics the physical examination. So if I think he is sick, but I do not actually hear abnormalities when I and if I then receive a photo which shows that everything is clean, then I would still give them listen to the lungs, then I wonder whether I miss something. So then I would consider taking a antibiotics since he is sick. While if you receive a photo which shows a pneumonia then I would picture of the lungs...and maybe some blood test (Antwerp, Clinician 119) CRP: think If yes, you I already have a very knew ill that. patient So and the a consequence low CRP, you of should that photo trust the is not ill person that considerable and not the low (Utrecht, CRP. I Clincian regard that 44) mostly as beginners mistakes, so I hope I don t make mistakes like that (Tromsø, Clincian 193)
68 2. Non clinical factors network related Southampton Antwerp Tromsø Utrecht Cardiff Balatonfüred Lodz Barcelona Milan
69 3. Non-clinical factors - clinician related Professional ethos Self belief in decision making Attitude towards relationship with patient
70 3. Clinician characteristics: professional ethos Receptiveness: Old habits die hard [...] even when new guidelines are implemented I find it difficult to put these into practice. I am so used to the old ways (Utrecht, clinician 0072) School of thought: I came very much from the older school of thought, you know, irrespective of what the patient presents with and how well they are, antibiotics is always a good idea because it acts as a placebo if not as the cure (Cardiff, clinician 0098)
71 3. Clinician characteristics: self belief Confidence: I think there is accumulating evidence about the appropriateness of using antibiotics per se and I follow that. I think I struggle to an extent with my confidence at not giving antibiotics (Southampton, clinician 0029) Tolerating uncertainty: Defensive medicine is very common [ ] Scared to make decisions that turn out to be wrong. You could lose patients as well, in those areas where there is competition about the patients (Tromsø, clinician 0319)
72 3. Clinician characteristics: relationship with pt Emotional investment: At the beginning I had a greater enthusiasm in dissuading the patient in explaining him that the antibiotic is not necessary with relation to what I do now (Lodz, clinician 0078) Confrontation threshold: Sometimes I ll have that whole fight about not giving antibiotics and I feel sometimes practically I feel like crying cause they re so horrible that some days I just don t want that argument and I ll back out of it (Cardiff, clinician 0056) Sharing responsibility: The image of the doctor really has changed over time, hasn t it?! I can tell the patient what I think would be the correct treatment, but I can t force them The patient is the one who decides (Barcelona, clinician 0015)
73 Key messages: Clinician beliefs on factors contributing to variation in antibiotics Clinical factors consist of information from physical exam and information gathered on patient s medical history Most frequently mentioned clinical factor guiding management was auscultation CRP POCTs were routinely used in Tromsø and had an immediate impact on the management decision Clinicians across all networks talked about need to combine clinical findings and clinical factors have different weightings Non-clinical factors are widely reported across all networks and can be divided into: wider contextual factors unique to particular networks personal characteristics of groups of clinicians regardless of network
74 How do (GPs' perceptions of) patient expectations influence antibiotic prescribing? Samuel Coenen On behalf of the GRACE-01 Study Team
75 Objectives To assess the influence of (GPs perceptions of) patient expectations and satisfaction on the antibiotic prescribing decision. BMJ 2009;338:b2242
76 Methods The final BMJ* model predicting antibiotic prescribing controlling for Network presented in (14 networks) Co-morbidities (heart, respiratory, diabetes) Age in decades Clinical presentation (all clinician ratings) Sputum type (absent, normal, abnormal) Temperature (low, normal, high) + Patient expectation of antibiotics (yes, no) + Patient hope for antibiotics (yes, no) + Patient ask for antibiotics (yes, no) + Patient satisfaction with visit (very satisfied, -, -, dissatisfied) + GPs perception of patient expectation (strongly (dis)agree) + GPs perception of patient satisfaction (strongly (dis)agree) + GPs perception of benefit for patient (strongly (dis)agree) * BMJ 2009;338:b2242
77 Results OR (95% BI) Patient expectations yes 2.68 ( ) Patient hope yes 1.88 ( ) Patient ask yes 0.43 ( ) Patient satisfaction very satisfied 4.08 ( ) satisfied 2.26 ( ) neither nor 1 dissatisfied 0.36 ( ) p < 0.05
78 GPs perception of Results continued OR (95% BI) - Patient expectation strongly agree 8.74 ( ) agree 2.67 ( ) neither nor 1 disagree 0.45 ( ) strongly disagree 0.58 ( ) - Patient satisfaction strongly agree 2.21 ( ) agree 2.69 ( ) neither nor disagree ( ) - Benefit for patient strongly agree ( ) agree ( ) neither nor 1 disagree 0.02 ( ) p < 0.05 strongly disagree 0.01 ( )
79 Conclusions 1. Patient expectations (and hopes) and patient satisfaction influence the antibiotic prescribing decision; 2. GPs perceptions of patient expectations influence the antibiotic prescribing decision, as well as their perception of patient satisfaction and of patient benefit; 3. No match between GPs perceptions and patient expectations? 4. No network specific effect of (GPs perceptions of) patient expectations? To be taken into account when developing interventions to change antibiotic prescribing behaviour, i.e. in GRACE WP10b
80 Extra Table Percentage of patients expecting, hoping or asking antibiotics split by the GPs responses to the related perceptions question, and Wilcoxon effect size* This patient wanted me to prescribe antibiotics Strongly Agree Agree Neither agree nor disagree Disagree Strongly disagree Wilcoxon effect size % n % n % n % n % n Patient expecting Patient hoping Patient asking * A statistically valid way of formally assessing how related clinician s perceptions and patient views are. It compares GPs perception scores of those patients who answer positively to each of the three questions they were asked with those who answered negatively, and ranges between 0 and 1. If there is no difference between these groups, the Wilcoxon effect size would be 0.5. Values away from 0.5 indicate that these two groups are rated differently by the GPs.
81 What do patients understand by antibiotic resistance? Lucy Brookes-Howell, Glyn Elwyn, Kerry Hood, Lucy Cooper, Herman Goossens, Christopher C Butler
82 GRACE 02: Methods Design Multi-centre qualitative study using in-depth semi-structured interviews. Setting Primary care research networks based in nine European cities: Antwerp, Balatonfüred, Barcelona, Cardiff, Łódź, Milan, Southampton, Tromsø, and Utrecht. Participants 121 adult patients who had recently consulted a primary care clinician with symptoms of LRTI. Data collection and analysis Topic guide translated and back-translated, interviewers trained, recorded, transcribed, translated, sent to Cardiff, subject to framework analysis
83 Results 1: Body becomes immune to antibiotics 2: Bacteria become immune to antibiotics
84 1: The resistant body Commonest view across all 8 networks Body gets used to antibiotics If you take them too much then you get to the point where it doesn t work any more, because the body gets used to it. Then they don t have the desired effect (Barcelona 185)
85 1: Body gets used to it This form of immunity often led to the view that different antibiotics might be needed I think it s like everything if you take too much of it then your body is going to start building up a resistance against those antibiotics, it s thinking oh not more of the same things yes I m going to fight these sort of thing and your body ll build up resistance until you re put on something a different drug where your body thinks oh this is different [ ] I haven t had this one before (Cardiff 266)
86 1: Body becomes immune to antibiotics I am convinced that when you use too many antibiotics that when at a given time you really need them, your body has become so immune to them, that they will not really have an effect, but that you should keep them for when they are really needed (Antwerp 539)
87 1: Body develops tolerance as it does to a drug Well, I think that if you take antibiotics too much and when you don't really need them, then the body gets used to them and then later when you do actually need them they don't work or they're less effective, kind of like what happens with a heroine
88 1: The body resists antibiotics I do understand quite often when the GP will say there s no point in taking antibiotics it s not going to do any good, it s not going to work or your body may not accept them so, yes along those lines (Southampton 449)
89 1: Individual body becomes incompatible with antibiotics Resistant to antibiotics? [ ] Yes, all I know is that he is generally immune to antibiotics and they don t work in his case. [...] For example I am allergic to detreomicine and I can t use it (Lodz 316)
90 1: Antibiotics retards development of immunity Well it stops, your immune system stops building up and then like, to me your immune system stops building up and then when you take the antibiotic it doesn t work (Southampton 267)
91 2: The resistant bacterium Less than half the number who spoke of resistant body spoke of resistant bacteria: If it is taken too often then bacteria If it is taken too often then bacteria become stronger and the same medication won t work, I know that, but then they give a bigger dose (Balatonfured 160)
92 2: The resistant bacterium Let s say the microbes become immune somehow [...] all the bacteria and the elements which infect usually evolve to beat the element that attacks them. [...] in the end the bacteria also travel from some people and others and if reinforced bacteria come well the antibiotics, well (Barcelona 171).
93 Explanations are fluid: antibiotic lost potency, illness became too strong I think a resistance is that it that when you take it, that it can t do its work anymore. That the product has lost its strength or that the illness has become too strong. That the illness, well the bacteria or the viruses, have resisted. That the products are in fact no longer strong enough to root out the bacteria (Antwerp 497).
94 Conclusions Patients across Europe are generally aware of the problems of antibiotic resistance but have widely contrasting interpretations of the mechanisms The dominant interpretation of antibiotic resistance is one where a tolerance or immunity develops in the body ( Your body gets used to them ) This interpretation undermines the population-wide relevance of bacterial resistance to antimicrobials (resistance is transmitted between bacteria an people) There is a need for clear, consistent messages directed at increasing the understanding that we risk making bacteria impossible to treat if we over use antibiotics and that this is a problem for society in general.
95 WP8 Publication Policy Warsaw, Feb 10 Prof Chris Butler WP8 Leader, Cardiff University
96 Authorship criteria Authorship credit will be based only on substantial contribution to all the following criteria: conception and design, or analysis and interpretation of data drafting or critically revising the article for important intellectual content final approval of the version to be published.
97 Publication List Title of paper GRACE 01 Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: prospective study in 13 countries. Aim 1. Describe differences between networks in antibiotic prescribing, taking case mix into account. 2. Describe network differences in management - does it affect the outcome, taking case mix into account? Target journal/s BMJ Lead author (Writing Group) CCB (KH, TV PL HG JN, UMR, AT, HM, MK, SM) Status Published BMJ Are smokers with acute cough in Do GPs treat smokers differently ERJ NS (MGC, Published primary care prescribed (prescribing only)? KH, DG, ERJ MK, JN, antibiotics more often, and to CCB) what benefit? An observational study in 13 European countries Building an international network for primary care research: challenges and solutions in the set-up and delivery of a prospective observational study of acute cough in 13 European Countries to reflect on methodological considerations and challenges in developing a large-scale quantitative project. Biomed Central Family Practice JN, CCB, KH, PL, TV, CB, RV, HG Submitted to BMC Nov 09
98 Publication List Title of paper Aim Target journal/s Lead author (Writing Group) Status Discoloured sputum and feeling unwell does not predict benefit from antibiotic treatment for acute cough: a prospective study in 13 European countries NEJM KH (JC UMR MGC, CCB, TV, PL, HG, RO MMu) Analysis complete Submit Feb 10 Lancet Antibiotic class is not Lancet MM (KH, Analysis associated with recovery in MK, JN) complete adults presenting with acute Submit cough in primary care: results Mar 10 from the GRACE 13-country prospective study Congruence with European guidelines ERJ MGC, HM (UMR, KH, MK, JN) Analysis in progress Patient views on antibiotics, expectations and satisfaction with management of LRTI in Europe. To what extent do patient views on antibiotics, expectations and perceived expectation of an antibiotic mean the patient will be prescribed an antibiotic? BMJ / Lancet SC (CCB, PL, TV, HG, RS/JC? UMR MGC SM, KH) Analysis complete paper being written
99 Publication List Title of paper Aim Target journal/s Lead author (Writing Group) Status Use of investigations in LRTI across Europe. E.g. x-ray; targeted or blanket? Standardised across country or symptom specific (given specifically for certain patients?) Describe variation between countries KH, RS/JC UMR SM,AT MM,PL, CCB, HG, TV Analysis in progress Health service use in community LRTI in Europe Describe what do patients decide to do when they want to re-consult? KH JC UMR MGC, CCB, TV, PL, HG, RO Analysis in progress Receiving a delayed prescription and cashing it in Describing gaps between prescribed dispensed and taken. JN PL, MM, KH, KH Analysis in progress Assessing the Impact of Nonresponse in a 13-Country Prospective Study of Acute Cough in Primary Care DG, KH, MK, JN, CCB Analysis in progress Prediction of a complicated outcome in primary care patients with a lower respiratory tract infection: a prognostic study SVV, CCB, MK, KH, TV et al Analysis in progress
100 Publication List Title of paper Aim Target journal/s Lead author (Writing Group) Status Sickness certification in LRTI; variation across Europe. Describing the prevalence of issued sick certificates between Countries. Duration of certificate and reason given. Is there a trend for certain diagnoses/age/job? MGC, HM (UMR, KH, MK, JN) Self medication in LRTI; variation across Europe Describe how patients self medicate and use OTC medicine. KH (JC UMR MGC, CCB, TV, PL, HG, RO MMu) Taking temperature in LRTI Do GPs normally take temperature, variation between countries? Is there a relationship between whether GP would normally take temperature and diagnosis? MM (KH, MK, JN) Assessing recovery in LRTI Methodological paper describing differences between and utility of patient s report of day they felt better versus cut points on symptom score. Also, how do symptom scores relate to functional measures of EQ5D. Specialist journal MK (RS/JC? SC AT MM)
101 Publication List Title of paper Aim Target journal/s GRACE-01 Network Specific paper and ideas Helsinki Nordic CRP Study Lead author (Writing Group) UMR Status Tromso - The predictive value of CRP for prescribing of antibiotics in acute cough in Nordic countries How does the use of the CRP-test affect the emphasis laid by GPs on other predictors? KAJ (CP SM HM, MK, Kh, CCB, Analysis complete Mar 10 Norway/Poland sick certificate analysis based on Norwegian and Polish data only ( See No 10 lead on main paper and then focus on Country specific data) HM, MGC Analysis in progress
102 Publication List Title of paper Aim Target journal/s GRACE 02 The body gets used to them : patients interpretations of antibiotic resistance and the implications for improvement strategies Lancet Lead author (Writing Group) GE CCB (SC, LBH, FW, KH, LC, PL, TV) Non-clinical factors influencing variation in management Medical Journal (e.g. BMJ) (CCB SC, FW, KH, LC. PL, TV) LBH Status Analysis complete (Milan interviews) Clinical methods for managing overview of patterns of similarity and General LBH Re- LRTI differences in clinician beliefs across countries submission Mar 10 Draft paper written Point of care testing FW Analysis in progress
103 Publication List Title of paper Aim Target journal/s Lead author (Writing Group) Status An exploration of the factors which influence clinicians decisions about antibiotic type To provide an overview of the clinical and non-clinical factors which influence clinicians decisions about antibiotic type General Medical Journal (e.g. BMJ) LBH (CCB, LC) Analysis in progress Pathways of care for patients with LRTI in 13 European countries To describe the different routes through the healthcare system for a patient with symptoms of LRTI in 13 European countries (identifying variable factors e.g. finance, location etc.). Specialist Journal (e.g. JAC, Emerg Infect Dis) LBH (JC, LC, KH, CCB, BB) The process of capturing wider health context in multi-centre research: producing patient pathways A methodological paper reflecting on the need to capture wider health care context in cross-national health research and a practical overview of the process to do this. Health & Place, J Int Med Res LBH (BB, CCB, KH) Submitted awaiting response Methodological considerations in developing multi-centre, cross- European qualitative research in primary care to reflect on methodological considerations and challenges in developing a large-scale qualitative project. Specialist methodologi cal journal. Although ongoing discussion in BMJ LBH (SC) Presented at conference.
104 Publication List Title of paper Aim Target journal/s GRACE-02 Network specific Poland Demonstrating the value of qualitative research, using GRACE-02 as an illustration Lead author (Writing Group) MGC (LBH) Status Discussion in Milan Comparison of Clinician and Patient beliefs in Netherlands and Belgium SC A qualitative study of patients beliefs in respiratory tract infections in Spain. Local journal in Spain AB (LBH) The future of point-of-care testing in management of LRTI across Europe: Clinician and patient beliefs To explore beliefs about the use of POCTs in management of LRTI in Tromsø, where POCTs are routinely used, and other GRACE-02 networks KAJ (HM, LBH)
105 Publication List Title of paper Aim Target journal/s GRACE-03 LRTI definitions in LRTI; a modified Delphi study ERS Lead author (Writing Group) GG (UMR KH, CCB, PL, TV, HG) Status Draft paper written - to be circulated to wider group Feb. 10
106 Publication List Title of paper Aim Target journal/s Lead Status Network additional suggestions Milan comparison of outcome in patients prescribed antibiotics with or without atypical coverage? covered in antibiotic choice paper Clinical endopoints such as need for new antibiotic, re-consultation, or hospitalisation will be compared between those receiving and those not receiving an antibiotic. Among the former, clinical outcomes will be compared between antibiotics with or without atypical coverage. (PT FB) Norway - The impact of the duration of illness on symptoms presented when a GP is consulted for an acute cough/lrti. Which symptoms can be expected at certain durations of illness in uncomplicated LRTI. Untreated patients with uncomplicated courses of illness will be analysed separately (HM)
107 Publication List Title of paper Aim Target journal/s Lead author (Writing Group) Status Norway - Cough remedies in LRTI in European countries. I think a specific focus on cough treatment is a good idea. European and American guidelines have recently been published, and I think the real practice is quite different. (HM, KAJ) What predicts antibiotic What predicts antibiotic prescribing in SM prescribing in LRTI in those LRTI in those patients without patients without investigations investigations; patient expectations, time to consultation, illness score, country, etc. In patients with similar illness score - does results of investigations change prescribing of antibiotics.. SM
108 Publication List Health Economics papers Use of 01 data Use of 01, H/E and map data Use of 01, H/E and map data JAC QoLR BMJ RO (MK, JN,JC) RO (KH, MK, JC) RO (TV, KH, RS, JC) Use of 01 and 02 data 01 and 02 JC (LBH, CB)
Antibiotics and acute cough: a pan European study
 WONCA Europe 2007, Paris Antibiotics and acute cough: a pan European study Kerry Hood and the GRACE-01 Study Team Department of Primary Care and Public Health Cardiff University Conflict of Interest: None
WONCA Europe 2007, Paris Antibiotics and acute cough: a pan European study Kerry Hood and the GRACE-01 Study Team Department of Primary Care and Public Health Cardiff University Conflict of Interest: None
Antibiotic prescribing for adults with acute cough/lrti:
 ERJ Express. Published on January 13, 2011 as doi: 10.1183/09031936.00145810 Antibiotic prescribing for adults with acute cough/lrti: congruence with guidelines Joseph Wood South East Wales Trials Unit
ERJ Express. Published on January 13, 2011 as doi: 10.1183/09031936.00145810 Antibiotic prescribing for adults with acute cough/lrti: congruence with guidelines Joseph Wood South East Wales Trials Unit
RESEARCH. for acute cough in primary care in Europe and its impact on recovery, controlling for presentation.
 Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: prospective study in 13 countries C C Butler, professor, 1 K Hood, director, 2 T Verheij, professor,
Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: prospective study in 13 countries C C Butler, professor, 1 K Hood, director, 2 T Verheij, professor,
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Belgian National Antibiotic Awareness Campaigns
 Belgian National Antibiotic Awareness Campaigns Herman Goossens, Stijn De Corte, Samuel Coenen University of Antwerp and BAPCOC Joris Mateusen, Sarah Tulkens Absoluut Belgium Belgian National Antibiotic
Belgian National Antibiotic Awareness Campaigns Herman Goossens, Stijn De Corte, Samuel Coenen University of Antwerp and BAPCOC Joris Mateusen, Sarah Tulkens Absoluut Belgium Belgian National Antibiotic
Prepared: August Review: July Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide.
 Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
Prepared: August 2013 Review: July 2014 Common Infections. A Medicines Optimisation Antibiotic Prescribing Guide. Contents Page: Page No Why do we want to review antibiotics? 2 What do NICE say? 3 Acute
Implementing EBM: the case of antibiotics for sore throat
 Implementing EBM: the case of antibiotics for sore throat Mieke van Driel, Marc De Meyere, Jan De Maeseneer Department of General Practice, Ghent University, Belgium mieke.vandriel@ugent.be Supported by
Implementing EBM: the case of antibiotics for sore throat Mieke van Driel, Marc De Meyere, Jan De Maeseneer Department of General Practice, Ghent University, Belgium mieke.vandriel@ugent.be Supported by
Antimicrobial Update Stewardship in Primary Care. Clare Colligan Antimicrobial Pharmacist NHS Forth Valley
 Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
Antimicrobial Update Stewardship in Primary Care Clare Colligan Antimicrobial Pharmacist NHS Forth Valley Setting the Scene! Consequences of Antibiotic Use? Resistance For an individual patient with
CLINICAL PROTOCOL FOR COMMUNITY ACQUIRED PNEUMONIA. SCOPE: Western Australia. CORB score equal or above 1. All criteria must be met:
 CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
CLINICAL PROTOCOL F COMMUNITY ACQUIRED PNEUMONIA SCOPE: Western Australia All criteria must be met: Inclusion Criteria Exclusion Criteria CB score equal or above 1. Mild/moderate pneumonia confirmed by
Volume. December Infection. Notes. length of. cases as 90% 1 week. tonsillitis. First Line. sore throat / daily for 5 days. quinsy >4000.
 Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
Volume 8; Number 22 LINCOLNSHIRE GUIDELINES FOR THE TREATMENT OF COMMONLYY OCCURRING INFECTIONS IN PRIMARY CARE: WINTER 2014/15 In this issue of the PACE Bulletin we present an update of our Guidelines
Outpatient Antimicrobial Stewardship. Jeffrey S Gerber, MD, PhD Division of Infectious Diseases The Children s Hospital of Philadelphia
 Outpatient Antimicrobial Stewardship Jeffrey S Gerber, MD, PhD Division of Infectious Diseases The Children s Hospital of Philadelphia Overview The case for outpatient antimicrobial stewardship Interventions
Outpatient Antimicrobial Stewardship Jeffrey S Gerber, MD, PhD Division of Infectious Diseases The Children s Hospital of Philadelphia Overview The case for outpatient antimicrobial stewardship Interventions
Who is the Antimicrobial Steward?
 Who is the Antimicrobial Steward? J. Njeri Wainaina, MD FACP Assistant Professor of Medicine Division of Infectious Diseases and Section of Perioperative Medicine Disclosures None 1 Objectives Highlight
Who is the Antimicrobial Steward? J. Njeri Wainaina, MD FACP Assistant Professor of Medicine Division of Infectious Diseases and Section of Perioperative Medicine Disclosures None 1 Objectives Highlight
Volume 2; Number 16 October 2008
 Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Volume 2; Number 16 October 2008 What s new this month NHS Lincolnshire have launched a public information campaign designed to raise public awareness of the risks associated with the inappropriate use
Delayed Prescribing for Minor Infections Resource Pack for Prescribers
 Delayed Prescribing for Minor Infections Resource Pack for Prescribers Background: Antibiotic resistance is an alarming threat to modern healthcare, and infectious illness remains a major global threat
Delayed Prescribing for Minor Infections Resource Pack for Prescribers Background: Antibiotic resistance is an alarming threat to modern healthcare, and infectious illness remains a major global threat
Managing winter illnesses without antibiotics
 CLINICAL AUDIT Managing winter illnesses without antibiotics Valid to June 2023 bpac nz better medicin e Background Over the winter months, thousands of people across New Zealand will present to primary
CLINICAL AUDIT Managing winter illnesses without antibiotics Valid to June 2023 bpac nz better medicin e Background Over the winter months, thousands of people across New Zealand will present to primary
European Antibiotic Awareness Day
 Initiating a pan-european health campaign - experiences from setting up the European Antibiotic Awareness Day Dr Ülla-Karin Nurm Head of Public Health Development Section, Public Health Capacity and Communication
Initiating a pan-european health campaign - experiences from setting up the European Antibiotic Awareness Day Dr Ülla-Karin Nurm Head of Public Health Development Section, Public Health Capacity and Communication
Workshop on the use of antibiotics. Dr Rosemary Ikram FRCPA Consultant Clinical Microbiologist
 Workshop on the use of antibiotics. Dr Rosemary Ikram FRCPA Consultant Clinical Microbiologist Declaration of affiliations. Working with: BPAC, DHBSS laboratory schedule group, IANZ, Pharmacy Brands (UTI
Workshop on the use of antibiotics. Dr Rosemary Ikram FRCPA Consultant Clinical Microbiologist Declaration of affiliations. Working with: BPAC, DHBSS laboratory schedule group, IANZ, Pharmacy Brands (UTI
Volume 1; Number 7 November 2007
 Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Volume 1; Number 7 November 2007 CONTENTS Page 1 Page 3 Guidance on the Use of Antibacterial Drugs in Lincolnshire Primary Care: Winter 2007/8 NICE Clinical Guideline 54: Urinary Tract Infection in Children
Objective 1/20/2016. Expanding Antimicrobial Stewardship into the Outpatient Setting. Disclosure Statement of Financial Interest
 Expanding Antimicrobial Stewardship into the Outpatient Setting Michael E. Klepser, Pharm.D., FCCP Professor Pharmacy Practice Ferris State University College of Pharmacy Disclosure Statement of Financial
Expanding Antimicrobial Stewardship into the Outpatient Setting Michael E. Klepser, Pharm.D., FCCP Professor Pharmacy Practice Ferris State University College of Pharmacy Disclosure Statement of Financial
Building Rapid Interventions to reduce antimicrobial resistance and overprescribing of antibiotics (BRIT)
") Greater Manchester Connected Health City (GM CHC) Building Rapid Interventions to reduce antimicrobial resistance and overprescribing of antibiotics (BRIT) BRIT Dashboard Manual Users: General Practitioners
Greater Manchester Connected Health City (GM CHC) Building Rapid Interventions to reduce antimicrobial resistance and overprescribing of antibiotics (BRIT) BRIT Dashboard Manual Users: General Practitioners
Antimicrobial Stewardship
 Antimicrobial Stewardship Report: 11 th August 2016 Issue: As part of ensuring compliance with the National Safety and Quality Health Service Standards (NSQHS), Yea & District Memorial Hospital is required
Antimicrobial Stewardship Report: 11 th August 2016 Issue: As part of ensuring compliance with the National Safety and Quality Health Service Standards (NSQHS), Yea & District Memorial Hospital is required
Antimicrobial Resistance Update for Community Health Services
 Antimicrobial Resistance Update for Community Health Services Elizabeth Beech Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England October 2015 elizabeth.beech@nhs.net Superbugs
Antimicrobial Resistance Update for Community Health Services Elizabeth Beech Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England October 2015 elizabeth.beech@nhs.net Superbugs
ANTIMICROBIAL RESISTANCE and causes of non-prudent use of antibiotics in human medicine in the EU
 ANTIMICROBIAL RESISTANCE and causes of non-prudent use of antibiotics in human medicine in the EU Health and Food Safety John Paget (NIVEL) Dominique Lescure (NIVEL) Ann Versporten (University of Antwerp)
ANTIMICROBIAL RESISTANCE and causes of non-prudent use of antibiotics in human medicine in the EU Health and Food Safety John Paget (NIVEL) Dominique Lescure (NIVEL) Ann Versporten (University of Antwerp)
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository:
 This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/93229/ This is the author s version of a work that was submitted to / accepted
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/93229/ This is the author s version of a work that was submitted to / accepted
GP Small Group education April/May 2015 Antibiotics Resistance is futile
 GP Small Group education April/May 2015 Antibiotics Resistance is futile Acknowledgements This material was prepared by the Clinical Quality and Education team with help gratefully received from: Topic
GP Small Group education April/May 2015 Antibiotics Resistance is futile Acknowledgements This material was prepared by the Clinical Quality and Education team with help gratefully received from: Topic
ESISTONO LE HCAP? Francesco Blasi. Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano
 ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
4. The use of antibiotics without a prescription in seven EU Member States
 4. The use of antibiotics without a prescription in seven EU Member States Main findings The results are based upon telephone interviews in seven Member States (Cyprus, Estonia, Greece, Hungary, Italy,
4. The use of antibiotics without a prescription in seven EU Member States Main findings The results are based upon telephone interviews in seven Member States (Cyprus, Estonia, Greece, Hungary, Italy,
Owner Compliance. The Role of the Veterinary Nurse in Ensuring that the Patient is Properly Medicated
 Owner Compliance The Role of the Veterinary Nurse in Ensuring that the Patient is Properly Medicated 1 Compliance - definition The owner or person in charge administers The right medication At the correct
Owner Compliance The Role of the Veterinary Nurse in Ensuring that the Patient is Properly Medicated 1 Compliance - definition The owner or person in charge administers The right medication At the correct
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering
 SMC No. (650/10) Bayer Schering") moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
moxifloxacin intravenous, 400mg/250mL, solution for infusion (Avelox ) SMC No. (650/10) Bayer Schering 05 November 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
Nursing Home Online Training Sessions Session 2: Exploring Antibiotics and Their Role in Fighting Bacterial Infections
 National Nursing Home Quality Care Collaborative Nursing Home Online Training Sessions Session 2: Exploring Antibiotics and Their Role in Fighting Bacterial Infections Health Services Advisory Group (HSAG)
National Nursing Home Quality Care Collaborative Nursing Home Online Training Sessions Session 2: Exploring Antibiotics and Their Role in Fighting Bacterial Infections Health Services Advisory Group (HSAG)
Physician Rating: ( 23 Votes ) Rate This Article:
 Rate This Article:") From Medscape Infectious Diseases Conquering Antibiotic Overuse An Expert Interview With the CDC Laura A. Stokowski, RN, MS Authors and Disclosures Posted: 11/30/2010 Physician Rating: ( 23 Votes ) Rate
From Medscape Infectious Diseases Conquering Antibiotic Overuse An Expert Interview With the CDC Laura A. Stokowski, RN, MS Authors and Disclosures Posted: 11/30/2010 Physician Rating: ( 23 Votes ) Rate
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
10/9/2017. Evidence-Based Interventions to Reduce Inappropriate Prescription of Antibiotics. Prescribing for Respiratory Tract Infections
 Evidence-Based Interventions to Reduce Inappropriate Prescription of Antibiotics Ann Thomas, MD, MPH Oregon Public Health Division Prescribing for Respiratory Tract Infections Antibiotic use is primary
Evidence-Based Interventions to Reduce Inappropriate Prescription of Antibiotics Ann Thomas, MD, MPH Oregon Public Health Division Prescribing for Respiratory Tract Infections Antibiotic use is primary
BELIEFS AND PRACTICES OF PARENTS ON THE USE OF ANTIBIOTICS FOR THEIR CHILDREN WITH UPPER RESPIRATORY TRACT INFECTION
 PIDSP Journal 2009 Vol 10No.1 Copyright 2009 BELIEFS AND PRACTICES OF PARENTS ON THE USE OF ANTIBIOTICS FOR THEIR CHILDREN WITH UPPER RESPIRATORY TRACT INFECTION Micheline Joyce C. Salonga, MD* ABSTRACT
PIDSP Journal 2009 Vol 10No.1 Copyright 2009 BELIEFS AND PRACTICES OF PARENTS ON THE USE OF ANTIBIOTICS FOR THEIR CHILDREN WITH UPPER RESPIRATORY TRACT INFECTION Micheline Joyce C. Salonga, MD* ABSTRACT
Period of study: 12 Nov 2002 to 08 Apr 2004 (first subject s first visit to last subject s last visit)
") Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Study Synopsis This file is posted on the Bayer HealthCare Clinical Trials Registry and Results website and is provided for patients and healthcare professionals to increase the transparency of Bayer's
Knowledge, attitude, and behaviour toward antibiotics among Hong Kong people: local-born versus immigrants
 RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES Knowledge, attitude, and behaviour toward antibiotics among Hong Kong people: local-born versus immigrants TP Lam *, KF Lam, PL Ho, RWH Yung K e y M
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES Knowledge, attitude, and behaviour toward antibiotics among Hong Kong people: local-born versus immigrants TP Lam *, KF Lam, PL Ho, RWH Yung K e y M
ANTIMICROBIAL STEWARDSHIP FOR AMBULATORY CARE SETTINGS
 ANTIMICROBIAL STEWARDSHIP FOR AMBULATORY CARE SETTINGS Jeffrey S Gerber, MD, PhD Children s Hospital of Philadelphia University of Pennsylvania School of Medicine DISCLOSURE STATEMENT I have no conflicts
ANTIMICROBIAL STEWARDSHIP FOR AMBULATORY CARE SETTINGS Jeffrey S Gerber, MD, PhD Children s Hospital of Philadelphia University of Pennsylvania School of Medicine DISCLOSURE STATEMENT I have no conflicts
Geriatric Mental Health Partnership
 Geriatric Mental Health Partnership September 8, 2017 First, let s test your knowledge about antibiotics http://www.cdc.gov/getsmart/community/about/quiz.html 2 Get Smart Antibiotics Quiz Antibiotics fight
Geriatric Mental Health Partnership September 8, 2017 First, let s test your knowledge about antibiotics http://www.cdc.gov/getsmart/community/about/quiz.html 2 Get Smart Antibiotics Quiz Antibiotics fight
Community-Acquired Pneumonia: Severity scoring and compliance to BTS guidelines. Julie Harris Antibiotic Pharmacist Hywel Dda Healthboard
 Community-Acquired Pneumonia: Severity scoring and compliance to BTS guidelines Julie Harris Antibiotic Pharmacist Hywel Dda Healthboard Plan Background BTS guidelines Differences in opinion Measures introduced
Community-Acquired Pneumonia: Severity scoring and compliance to BTS guidelines Julie Harris Antibiotic Pharmacist Hywel Dda Healthboard Plan Background BTS guidelines Differences in opinion Measures introduced
Antimicrobial practice. Laboratory antibiotic susceptibility reporting and antibiotic prescribing in general practice
 Journal of Antimicrobial Chemotherapy (2003) 51, 379 384 DOI: 10.1093/jac/dkg032 Advance Access publication 6 January 2003 Antimicrobial practice Laboratory antibiotic susceptibility reporting and antibiotic
Journal of Antimicrobial Chemotherapy (2003) 51, 379 384 DOI: 10.1093/jac/dkg032 Advance Access publication 6 January 2003 Antimicrobial practice Laboratory antibiotic susceptibility reporting and antibiotic
ECHO: Management of URIs. Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018
 ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
Promoting Appropriate Antimicrobial Prescribing in Secondary Care
 Promoting Appropriate Antimicrobial Prescribing in Secondary Care Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2015 Introduction Background ESPAUR
Promoting Appropriate Antimicrobial Prescribing in Secondary Care Stuart Brown Healthcare Acquired Infection and Antimicrobial Resistance Project Lead NHS England March 2015 Introduction Background ESPAUR
SECTION 3A. Section 3A Criteria for Optional Special Authorization of Select Drug Products
 SECTION 3A Criteria for Optional Special Authorization of Select Drug Products Section 3A Criteria for Optional Special Authorization of Select Drug Products CRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION
SECTION 3A Criteria for Optional Special Authorization of Select Drug Products Section 3A Criteria for Optional Special Authorization of Select Drug Products CRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION
Discussion Paper: Antimicrobial Resistance Sept 2014
 Homeless Health Network Better healthcare for people who are homeless Discussion Paper: Antimicrobial Resistance Sept 2014 The Queen s Nursing Institute s Homeless Health Network shared their views on
Homeless Health Network Better healthcare for people who are homeless Discussion Paper: Antimicrobial Resistance Sept 2014 The Queen s Nursing Institute s Homeless Health Network shared their views on
SEASONAL TRENDS IN ANTIBIOTIC USAGE AMONG PAEDIATRIC OUTPATIENTS
 SEASONAL TRENDS IN ANTIBIOTIC USAGE AMONG PAEDIATRIC OUTPATIENTS Edita Alili-Idrizi, Msc Merita Dauti, Msc State University of Tetovo, Faculty of Medicine, Department of Pharmacy, Tetovo, R. of Macedonia
SEASONAL TRENDS IN ANTIBIOTIC USAGE AMONG PAEDIATRIC OUTPATIENTS Edita Alili-Idrizi, Msc Merita Dauti, Msc State University of Tetovo, Faculty of Medicine, Department of Pharmacy, Tetovo, R. of Macedonia
running head: SUPERBUGS Humphreys 1
 running head: SUPERBUGS Humphreys 1 Superbugs GCH 360 Term Paper Assignment Kelly Humphreys April 30, 2014 SUPERBUGS Humphreys 2 Introduction The World Health Organization (WHO) recognizes antibiotic resistance
running head: SUPERBUGS Humphreys 1 Superbugs GCH 360 Term Paper Assignment Kelly Humphreys April 30, 2014 SUPERBUGS Humphreys 2 Introduction The World Health Organization (WHO) recognizes antibiotic resistance
Suitability of Antibiotic Treatment for CAP (CAPTIME) The duration of antibiotic treatment in community acquired pneumonia (CAP)
 The duration of antibiotic treatment in community acquired pneumonia (CAP)") STUDY PROTOCOL Suitability of Antibiotic Treatment for CAP (CAPTIME) Purpose The duration of antibiotic treatment in community acquired pneumonia (CAP) lasts about 9 10 days, and is determined empirically.
STUDY PROTOCOL Suitability of Antibiotic Treatment for CAP (CAPTIME) Purpose The duration of antibiotic treatment in community acquired pneumonia (CAP) lasts about 9 10 days, and is determined empirically.
Antimicrobial use in humans
 Antimicrobial use in humans Ann Versporten Prof. Herman Goossens OIE Global Conference on the Responsible and Prudent Use of Antimicrobial Agents for Animals - 13 March 2013 - Ann.versporten@ua.ac.be Herman.goossens@uza.be
Antimicrobial use in humans Ann Versporten Prof. Herman Goossens OIE Global Conference on the Responsible and Prudent Use of Antimicrobial Agents for Animals - 13 March 2013 - Ann.versporten@ua.ac.be Herman.goossens@uza.be
Tandan, Meera; Duane, Sinead; Vellinga, Akke.
 Provided by the author(s) and NUI Galway in accordance with publisher policies. Please cite the published version when available. Title Do general practitioners prescribe more antimicrobials when the weekend
Provided by the author(s) and NUI Galway in accordance with publisher policies. Please cite the published version when available. Title Do general practitioners prescribe more antimicrobials when the weekend
5/15/17. Core Elements of Outpatient Antibiotic Stewardship: Implementing Antibiotic Stewardship Into Your Outpatient Practice.
 National Center for Emerging and Zoonotic Infectious Diseases Core Elements of Outpatient Antibiotic Stewardship: Implementing Antibiotic Stewardship Into Your Outpatient Practice Melinda Neuhauser, PharmD,
National Center for Emerging and Zoonotic Infectious Diseases Core Elements of Outpatient Antibiotic Stewardship: Implementing Antibiotic Stewardship Into Your Outpatient Practice Melinda Neuhauser, PharmD,
Let me clear my throat: empiric antibiotics in
 Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
Let me clear my throat: empiric antibiotics in respiratory tract infections Alexander John Langley, MD MS MPH Goals of this talk Overuse of antibiotics is a major issue, as a result many specialist medical
Antibiotics: Take a Time Out
 Antibiotics: Take a Time Out Christine LaRocca, MD Telligen April 27, 2018 This material was prepared by Telligen, the Medicare Quality Innovation Network Quality Improvement Organization, under contract
Antibiotics: Take a Time Out Christine LaRocca, MD Telligen April 27, 2018 This material was prepared by Telligen, the Medicare Quality Innovation Network Quality Improvement Organization, under contract
Core Elements of Outpatient Antibiotic Stewardship Implementing Antibiotic Stewardship Into Your Outpatient Practice
 National Center for Emerging and Zoonotic Infectious Diseases Core Elements of Outpatient Antibiotic Stewardship Implementing Antibiotic Stewardship Into Your Outpatient Practice Katherine Fleming-Dutra,
National Center for Emerging and Zoonotic Infectious Diseases Core Elements of Outpatient Antibiotic Stewardship Implementing Antibiotic Stewardship Into Your Outpatient Practice Katherine Fleming-Dutra,
Managing AMR at the Human-Animal Interface. OIE Contributions to the AMR Global Action Plan
 Managing AMR at the Human-Animal Interface OIE Contributions to the AMR Global Action Plan 6th Asia-Pacific Workshop on Multi-Sectoral Collaboration for the Prevention and Control of Zoonoses Dr Susan
Managing AMR at the Human-Animal Interface OIE Contributions to the AMR Global Action Plan 6th Asia-Pacific Workshop on Multi-Sectoral Collaboration for the Prevention and Control of Zoonoses Dr Susan
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days
 Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Treatment Duration for Uncomplicated Community-Acquired Pneumonia: The Evidence in Support of 5 Days Executive Summary National consensus guidelines created jointly by the Infectious Diseases Society of
Objectives 4/26/2017. Co-Investigators Sadie Giuliani, PharmD, BCPS Claude Tonnerre, MD Jayme Hartzell, PharmD, MS, BCPS
 IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings. Carlos Reyes Sacin, MD, AAHIVS
 Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Research & Reviews: Journal of Hospital and Clinical Pharmacy
 Research & Reviews: Journal of Hospital and Clinical Pharmacy Empiric Antibiotic Prescribing For Community Acquired Pneumonia and Patient Characteristics Associated with Broad Spectrum Antibiotic Use Mirza
Research & Reviews: Journal of Hospital and Clinical Pharmacy Empiric Antibiotic Prescribing For Community Acquired Pneumonia and Patient Characteristics Associated with Broad Spectrum Antibiotic Use Mirza
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES
 AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
AZITHROMYCIN, DOXYCYCLINE, AND FLUOROQUINOLONES Update in Medicine and Primary Care Whitney R. Buckel, PharmD, BCPS-AQ ID System Antimicrobial Stewardship Pharmacist Manager OBJECTIVES 1. List three antibiotics
ESAC s Surveillance by Point Prevalence Measurements. by author
 ESAC s Surveillance by Point Prevalence Measurements Herman Goossens, MD, PhD ESAC Co-ordinator VAXINFECTIO, Laboratory of Medical Microbiology University of Antwerp, Belgium Outline Background Point Prevalence
ESAC s Surveillance by Point Prevalence Measurements Herman Goossens, MD, PhD ESAC Co-ordinator VAXINFECTIO, Laboratory of Medical Microbiology University of Antwerp, Belgium Outline Background Point Prevalence
Is amoxicillin good for viral infections
 Is amoxicillin good for viral infections 19-6-2017 Is Amoxicillin Good For Throat Infection. They will not help sore throats caused by allergies or viral infections such as colds amoxicillin is. Reviews
Is amoxicillin good for viral infections 19-6-2017 Is Amoxicillin Good For Throat Infection. They will not help sore throats caused by allergies or viral infections such as colds amoxicillin is. Reviews
FIS Resistance Surveillance: The UK Landscape. Alasdair MacGowan Chair BSAC Working Party on Antimicrobial Resistance Surveillance
 FIS 2013 Resistance Surveillance: The UK Landscape Alasdair MacGowan Chair BSAC Working Party on Antimicrobial Resistance Surveillance A statement of the obvious Good quality surveillance data on resistant
FIS 2013 Resistance Surveillance: The UK Landscape Alasdair MacGowan Chair BSAC Working Party on Antimicrobial Resistance Surveillance A statement of the obvious Good quality surveillance data on resistant
Summary of the latest data on antibiotic consumption in the European Union
 Summary of the latest data on antibiotic consumption in the European Union ESAC-Net surveillance data November 2016 Provision of reliable and comparable national antimicrobial consumption data is a prerequisite
Summary of the latest data on antibiotic consumption in the European Union ESAC-Net surveillance data November 2016 Provision of reliable and comparable national antimicrobial consumption data is a prerequisite
Improving patient knowledge of antimicrobial resistance and appropriate antibiotic use in a Rutland county acute care center
 University of Vermont ScholarWorks @ UVM Family Medicine Clerkship Student Projects College of Medicine 2019 Improving patient knowledge of antimicrobial resistance and appropriate antibiotic use in a
University of Vermont ScholarWorks @ UVM Family Medicine Clerkship Student Projects College of Medicine 2019 Improving patient knowledge of antimicrobial resistance and appropriate antibiotic use in a
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC
 Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus
 Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children
 Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Prescribing Guidelines for Outpatient Antimicrobials in Otherwise Healthy Children Prescribing Antimicrobials for Common Illnesses When treating common illnesses such as ear infections and strep throat,
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities
 Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities Introduction As the problem of antibiotic resistance continues to worsen in all healthcare setting, we
Commonwealth of Kentucky Antibiotic Stewardship Practice Assessment For Long-Term Care Facilities Introduction As the problem of antibiotic resistance continues to worsen in all healthcare setting, we
Bacterial Resistance of Respiratory Pathogens. John C. Rotschafer, Pharm.D. University of Minnesota
 Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Community Acquired 1) Is it pneumonia? ie new symptoms and signs of a lower respiratory
Challenges and opportunities for rapidly advancing reporting and improving inpatient antibiotic use in the U.S.
 Challenges and opportunities for rapidly advancing reporting and improving inpatient antibiotic use in the U.S. Overview of benchmarking Antibiotic Use Scott Fridkin, MD, Senior Advisor for Antimicrobial
Challenges and opportunities for rapidly advancing reporting and improving inpatient antibiotic use in the U.S. Overview of benchmarking Antibiotic Use Scott Fridkin, MD, Senior Advisor for Antimicrobial
Antimicrobial Stewardship
 Antimicrobial Stewardship Preventing the Spread of Antibiotic Resistance and Improving Patient Care (Adapted from the Centers for Disease Control and Prevention) What is Stewardship? Antimicrobial stewardship
Antimicrobial Stewardship Preventing the Spread of Antibiotic Resistance and Improving Patient Care (Adapted from the Centers for Disease Control and Prevention) What is Stewardship? Antimicrobial stewardship
Supplementary Online Content
 Supplementary Online Content Gerber JS, Prasad PA, Fiks AG, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians:
Supplementary Online Content Gerber JS, Prasad PA, Fiks AG, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians:
Models for stewardship in Hospital - UK Models Philip Howard Consultant Antimicrobial Pharmacist
 Models for stewardship in Hospital - UK Models Philip Howard Consultant Antimicrobial Pharmacist philip.howard2@nhs.net Twitter: @AntibioticLeeds United Kingdom of England, Scotland, Wales & Northern Ireland
Models for stewardship in Hospital - UK Models Philip Howard Consultant Antimicrobial Pharmacist philip.howard2@nhs.net Twitter: @AntibioticLeeds United Kingdom of England, Scotland, Wales & Northern Ireland
Antimicrobial Resistance and Dentistry. LDC Officials Day 4 December 2015 Susie Sanderson
 Antimicrobial Resistance and Dentistry LDC Officials Day 4 December 2015 Susie Sanderson Who am I? Why are we interested in AMR? Where is the leadership? Who is taking action? What is the BDA doing? Is
Antimicrobial Resistance and Dentistry LDC Officials Day 4 December 2015 Susie Sanderson Who am I? Why are we interested in AMR? Where is the leadership? Who is taking action? What is the BDA doing? Is
Cellulitis. Assoc Prof Mark Thomas. Conference for General Practice Auckland Saturday 28 July 2018
 Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Cellulitis Assoc Prof Mark Thomas Conference for General Practice Auckland Saturday 28 July 2018 Summary Cellulitis Usual treatment flucloxacillin for 5 days Frequent recurrences consider penicillin 250mg
Antibiotic resistance and prescribing in Australia: current attitudes and practice of GPs
 CSIRO PUBLISHING Healthcare Infection, 2013, 18, 147 151 http://dx.doi.org/10.1071/hi13019 Antibiotic resistance and prescribing in Australia: current attitudes and practice of GPs Rachel Hardy-Holbrook
CSIRO PUBLISHING Healthcare Infection, 2013, 18, 147 151 http://dx.doi.org/10.1071/hi13019 Antibiotic resistance and prescribing in Australia: current attitudes and practice of GPs Rachel Hardy-Holbrook
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP)
") IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
IMPLEMENTATION AND ASSESSMENT OF A GUIDELINE-BASED TREATMENT ALGORITHM FOR COMMUNITY-ACQUIRED PNEUMONIA (CAP) Lucas Schonsberg, PharmD PGY-1 Pharmacy Practice Resident Providence St. Patrick Hospital Missoula,
What is Antibiotic Resistance. Antibiotic Resistance A Public Health Issue
 What is Antibiotic Resistance Antibiotic Resistance A Public Health Issue Antibiotic resistance is the ability of a bacteria, to stop an antibiotics from working against it. As a result, standard treatments
What is Antibiotic Resistance Antibiotic Resistance A Public Health Issue Antibiotic resistance is the ability of a bacteria, to stop an antibiotics from working against it. As a result, standard treatments
Dr Eleri Davies. Consultant Microbiologist and Infection Control Doctor, Public Health Wales NHS Trust
 Dr Eleri Davies Consultant Microbiologist and Infection Control Doctor, Public Health Wales NHS Trust Antimicrobial stewardship What is it? Why is it important? Treatment and management of catheter-associated
Dr Eleri Davies Consultant Microbiologist and Infection Control Doctor, Public Health Wales NHS Trust Antimicrobial stewardship What is it? Why is it important? Treatment and management of catheter-associated
Summary of the latest data on antibiotic consumption in the European Union
 Summary of the latest data on antibiotic consumption in the European Union November 2012 Highlights on antibiotic consumption Antibiotic use is one of the main factors responsible for the development and
Summary of the latest data on antibiotic consumption in the European Union November 2012 Highlights on antibiotic consumption Antibiotic use is one of the main factors responsible for the development and
Stewardship: Challenges & Opportunities in the Gulf Region
 Stewardship: Challenges & Opportunities in the Gulf Region Mushira Enani, MBBS, FRCPE, FACP,CIC Head- Infectious Disease Section King Fahad Medical City Outline Background of Healthcare system in GCC GCC
Stewardship: Challenges & Opportunities in the Gulf Region Mushira Enani, MBBS, FRCPE, FACP,CIC Head- Infectious Disease Section King Fahad Medical City Outline Background of Healthcare system in GCC GCC
TREAT Steward. Antimicrobial Stewardship software with personalized decision support
 TREAT Steward TM Antimicrobial Stewardship software with personalized decision support ANTIMICROBIAL STEWARDSHIP - Interdisciplinary actions to improve patient care Quality Assurance The aim of antimicrobial
TREAT Steward TM Antimicrobial Stewardship software with personalized decision support ANTIMICROBIAL STEWARDSHIP - Interdisciplinary actions to improve patient care Quality Assurance The aim of antimicrobial
ANTIBIOTIC RESISTANCE: MULTI-COUNTRY SURVEY
 ANTIBIOTIC RESISTANCE: MULTI-COUNTRY SURVEY November 2015 CONTENTS 1. Executive Summary Page 3 2. Introduction Page 5 3. Methodology Page 6 3.1 Country selection 3.2 Approach 3.3 Limitations 4. Results
ANTIBIOTIC RESISTANCE: MULTI-COUNTRY SURVEY November 2015 CONTENTS 1. Executive Summary Page 3 2. Introduction Page 5 3. Methodology Page 6 3.1 Country selection 3.2 Approach 3.3 Limitations 4. Results
Knowledge, attitudes and perceptions of antimicrobial resistance amongst private practice patients and primary care prescribers in South Africa
 Knowledge, attitudes and perceptions of antimicrobial resistance amongst private practice patients and primary care prescribers in South Africa Dena van den Bergh, Elise Farley, Annemie Stewart, Mary-Ann
Knowledge, attitudes and perceptions of antimicrobial resistance amongst private practice patients and primary care prescribers in South Africa Dena van den Bergh, Elise Farley, Annemie Stewart, Mary-Ann
REPORT FROM THE FIRST GLOBAL MILK QUALITY EXPERT FORUM
 REPORT FROM THE FIRST GLOBAL MILK QUALITY EXPERT FORUM CONTACT Charlotte Grime charlotte@mgcomms.co.uk +44 (0) 1488 657722 Chatham House rules report WHAT WILL MASTITIS MANAGEMENT LOOK LIKE IN 10 YEARS?
REPORT FROM THE FIRST GLOBAL MILK QUALITY EXPERT FORUM CONTACT Charlotte Grime charlotte@mgcomms.co.uk +44 (0) 1488 657722 Chatham House rules report WHAT WILL MASTITIS MANAGEMENT LOOK LIKE IN 10 YEARS?
Pharmacoeconomic analysis of selected antibiotics in lower respiratory tract infection Quenzer R W, Pettit K G, Arnold R J, Kaniecki D J
 Pharmacoeconomic analysis of selected antibiotics in lower respiratory tract infection Quenzer R W, Pettit K G, Arnold R J, Kaniecki D J Record Status This is a critical abstract of an economic evaluation
Pharmacoeconomic analysis of selected antibiotics in lower respiratory tract infection Quenzer R W, Pettit K G, Arnold R J, Kaniecki D J Record Status This is a critical abstract of an economic evaluation
IDENTIFICATION: PROCESS: Waging the War against C. difficile Radical Multidisciplinary Approaches From a Community Hospital
 Waging the War against C. difficile Radical Multidisciplinary Approaches From a Community Hospital Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Leigh Chapman RN,
Waging the War against C. difficile Radical Multidisciplinary Approaches From a Community Hospital Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Leigh Chapman RN,
Define evidence based practices for selection and duration of antibiotics to treat suspected or confirmed neonatal sepsis
 GLOBAL AIM: Antibiotic Stewardship Perinatal Quality Improvement Teams (PQITs) will share strategies and lessons learned to develop potentially better practices and employ QI methodologies to establish
GLOBAL AIM: Antibiotic Stewardship Perinatal Quality Improvement Teams (PQITs) will share strategies and lessons learned to develop potentially better practices and employ QI methodologies to establish
Quality and Safety Committee
 SUMMARY REPORT Quality and Safety Committee ABM University Health Board Meeting On 20 TH OCTOBER 2016 Subject Prepared by Approved & Presented by Purpose Big Fight Campaign AGENDA ITEM: 2.2 Debra Woolley
SUMMARY REPORT Quality and Safety Committee ABM University Health Board Meeting On 20 TH OCTOBER 2016 Subject Prepared by Approved & Presented by Purpose Big Fight Campaign AGENDA ITEM: 2.2 Debra Woolley
Antimicrobial Stewardship in the Outpatient Setting. ELAINE LADD, PHARMD, ABAAHP, FAARFM OCTOBER 28th, 2016
 Antimicrobial Stewardship in the Outpatient Setting ELAINE LADD, PHARMD, ABAAHP, FAARFM OCTOBER 28th, 2016 Abbreviations AMS - Antimicrobial Stewardship Program OP - Outpatient OPS - Outpatient Setting
Antimicrobial Stewardship in the Outpatient Setting ELAINE LADD, PHARMD, ABAAHP, FAARFM OCTOBER 28th, 2016 Abbreviations AMS - Antimicrobial Stewardship Program OP - Outpatient OPS - Outpatient Setting
Antibiotic Review Kit - Hospital
 The International Convention Centre (ICC), Birmingham 11 12 September 2017 Antibiotic Review Kit - Hospital (ARK-hospital) Elizabeth Cross Brighton and Sussex University Hospitals NHS Trust Brighton and
The International Convention Centre (ICC), Birmingham 11 12 September 2017 Antibiotic Review Kit - Hospital (ARK-hospital) Elizabeth Cross Brighton and Sussex University Hospitals NHS Trust Brighton and
What is the problem? Latest data on antibiotic resistance
 European Antibiotic Awareness Day 2009 What is the problem? Latest data on antibiotic resistance Zsuzsanna Jakab, ECDC Director Launch Seminar for EAAD Stockholm, 18 November 2009 Fluoroquinolone-resistant
European Antibiotic Awareness Day 2009 What is the problem? Latest data on antibiotic resistance Zsuzsanna Jakab, ECDC Director Launch Seminar for EAAD Stockholm, 18 November 2009 Fluoroquinolone-resistant
Symptom response to antibiotic prescribing strategies in acute sore throat in adults:
 Research Michael Moore, Beth Stuart, FD Richard Hobbs, Chris C Butler, Alastair D Hay, John Campbell, Brendan C Delaney, Sue Broomfield, Paula Barratt, Kerenza Hood, Hazel A Everitt, Mark Mullee, Ian Williamson,
Research Michael Moore, Beth Stuart, FD Richard Hobbs, Chris C Butler, Alastair D Hay, John Campbell, Brendan C Delaney, Sue Broomfield, Paula Barratt, Kerenza Hood, Hazel A Everitt, Mark Mullee, Ian Williamson,
Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings
 Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings Jasmanda H. Wu, Ph.D., 1 David H. Howard, Ph.D., 2 John E. McGowan, Jr.,
Compliance with antibiotic treatment guidelines in managed care patients with communityacquired pneumonia in ambulatory settings Jasmanda H. Wu, Ph.D., 1 David H. Howard, Ph.D., 2 John E. McGowan, Jr.,
ANTIMICROBIAL STEWARDSHIP IN PRIMARY CARE DR ROSEMARY IKRAM MBBS FRCPA CLINICAL MICROBIOLOGIST
 ANTIMICROBIAL STEWARDSHIP IN PRIMARY CARE DR ROSEMARY IKRAM MBBS FRCPA CLINICAL MICROBIOLOGIST CONFLICTS OF INTEREST NONE PRESENTATION OUTLINE. SETTING THE SCENE WORLD AND NEW ZEALAND. BARRIERS TO OVERCOME.
ANTIMICROBIAL STEWARDSHIP IN PRIMARY CARE DR ROSEMARY IKRAM MBBS FRCPA CLINICAL MICROBIOLOGIST CONFLICTS OF INTEREST NONE PRESENTATION OUTLINE. SETTING THE SCENE WORLD AND NEW ZEALAND. BARRIERS TO OVERCOME.
ANTIMICROBIAL STEWARDSHIP: THE ROLE OF THE CLINICIAN SAM GUREVITZ PHARM D, CGP BUTLER UNIVERSITY COLLEGE OF PHARMACY AND HEALTH SCIENCES
 ANTIMICROBIAL STEWARDSHIP: THE ROLE OF THE CLINICIAN SAM GUREVITZ PHARM D, CGP BUTLER UNIVERSITY COLLEGE OF PHARMACY AND HEALTH SCIENCES 1 Crisis: Antibiotic Resistance Success Strategy 2 OBJECTIVES Discuss
ANTIMICROBIAL STEWARDSHIP: THE ROLE OF THE CLINICIAN SAM GUREVITZ PHARM D, CGP BUTLER UNIVERSITY COLLEGE OF PHARMACY AND HEALTH SCIENCES 1 Crisis: Antibiotic Resistance Success Strategy 2 OBJECTIVES Discuss
Core Elements of Antibiotic Stewardship for Nursing Homes
 Core Elements of Antibiotic Stewardship for Nursing Homes Nimalie D. Stone, MD, MS Medical Epidemiologist for LTC Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Antimicrobial
Core Elements of Antibiotic Stewardship for Nursing Homes Nimalie D. Stone, MD, MS Medical Epidemiologist for LTC Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Antimicrobial
The Force Concept Inventory (FCI) is currently
 is currently") Common Concerns About the Force Concept Inventory Charles Henderson The Force Concept Inventory (FCI) is currently the most widely used assessment instrument of student understanding of mechanics. 1 This
Common Concerns About the Force Concept Inventory Charles Henderson The Force Concept Inventory (FCI) is currently the most widely used assessment instrument of student understanding of mechanics. 1 This