MANAGING ANTIBIOTIC THERAPY
|
|
|
- Phebe Gibson
- 5 years ago
- Views:
Transcription
1 MANAGING ANTIBIOTIC THERAPY ITS MORE THAN JUST ABOUT THE S AND THE R Larry M. Bush, MD, FACP Affiliated Professor of Biomedical Science Charles E. Schmidt College of Medicine Florida Atlantic University Affiliated Associate Professor of Medicine University of Miami-Miller School of Medicine
2 LETS FACE IT WE ARE OBSESSED WITH PRESCRIBNG ANTIBIOTICS IN FACT, THE CDC SAYS THAT APPROXIMATELY 50% OF HOSPITALIZED PATIENTS RECEIVE ONE ANTIBIOTIC OR ANOTHER SOMETIME DURING THEIR STAY AND.. EVEN THOUGH ABOUT 90% OF ALL RESPIRATORY OUTPATIENT INFECTIONS ARE CAUSED BY VIRUSES, ALMOST 70% OF PATIENTS ARE GIVEN AN ANTIBIOTIC, OFTEN BROAD SPECTRUM DRUGS i.e. fluoroquinolones
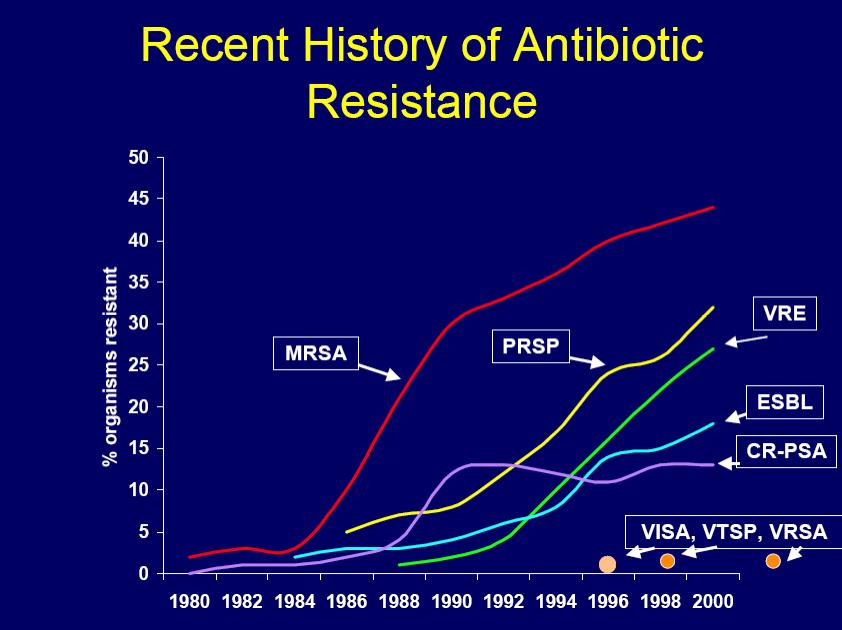
3 HOWEVER..THE CDC ALSO SAYS THAT ABOUT 50% OF THESE ANTIBIOTICS USED IN THE HOSPITAL ARE EITHER INCORRECTLY USED OR UNWARRANTED and FURTHERMORE.. The major instigating factors for the exponential rise in antimicrobial RESISTANCE is OUR OVER PRESCRIBING of this precious resource along with their use in animal feeds To the point that approximately 2 Million persons become ill every year with antibiotic-resistant infections, and about 23,000 die!
4
5 SO THEN. HOW DID WE GET TO THIS POINT. AND WHAT ARE WE (YOU) GOING TO DO TO CORRECT IT?
6 KEEP IN MIND. THE WORLD OF MEDICINE WAS CHANGED BY SANITATION & IMMUNIZATION
7 FIRST OFF LETS ALL BE TALKING APPLES to APPLES..does it fascinate you as it does me that when one considers that the human body is comprised of approx cells, and that located either within and/or on the surface of a human exists an estimated virions and bacteria (the indigenous microbiome)...it is astonishing yet comforting to realize that Clinical Infectious Disease is actually an INFREQUENT EVENT!..the question our patients should ask is..why have I not gotten more infections, rather than what we all hear.. HOW AND WHY did I get
8 LETS KEEP THE APPLE TERMS STRAIGHT INFECTION (COLONIZATION) A BUG WTIHIN OR ON A HOST, PERSISTENT OR TRANSIENT AND CAUSES NO HARM. INFECTIOUS DISEASE INTERACTION WITH THE BUG CAUSES HARM TO THE HOST, ALTERS PHYSIOLOGY AND LEADS TO SIGNS AND SYMPTOMS PATHOGEN A BUG THAT HAS THE CAPACITY TO CAUSE DISEASE. ALMOST ALWAYS FROM THE ENDOGENOUS MICRO-FLORA..so why the common question, how, why, and where did I get this infection from? VIRULENCE PROVIDES A QUANTITATIVE MEASURE OF A BUG S CAPACITY TO CAUSE DISEASE (i.e. Staph aureus, encapsulated Pneumococcus / Meningococcus, C dif toxins)
9 I CAN NOT STAND THE PHRASE PERCEPTION IS REALITY REALITY IS REALITY BUT WE ALL HAVE TO LIVE WITH OUR PATIENTS PERCEPTIONS EACH AND EVERY DAY JUST TELL ME I DON T HAVE MRSA, THEY TOLD ME YOU CAN NEVER GET RID OF IT OH NO, A POSITIVE TB SKIN TEST, I THOUGHT TUBERCULOSIS WAS ONLY IN THEM ZIKA, EBOLA WERE ALL DOOMED GIVE ME (OR HERE, TAKE) THE ANTIBIOTIC, JUST TO BE SAFE.. IT CAN T HURT
10 BUT THIS IS THE ONE MOST MISUNDERSTOOD BY PATIENTS, ADMINISTRATORS, HEALTH-CARE AGENCIES AND REGULATORY BODIES AND FRANKLY BY MANY OF OUR COLLEAGUES SEPSIS THANK GOODNESS I DON T HAVE SEPSIS, BUT JUST PNEUMONIA
11 SEPSIS - WHAT REALLY IS THIS CONDITION ANYWAY? EARLY 1980 S SEPSIS IS ENDOTOXEMIA, HOW DO YOU REALLY MEASURE THAT SEPTICEMIA THE ONGOING MISCONCEPTION OF BACTEREMIA And then in 1991, and for 25 years thereafter.. The almost religious adoption that sepsis was THE SYSTEMIC INFLAMMATORY RESPONSE SYNDROME (SIRS) 2 OR MORE OF: HR>90/MIN, RR>20/MIN, TEMP>100.4F or <96.8F, WBC>12,000 or <4,000 OR >10% Band forms
.")
12 BUT FINALLY IN FEBRUARY, 2016 (JAMA) WE GOT.an actual DEFINITION of what SEPSIS actually is..no longer clinical criteria alone LIFE THREATENING ORGAN DYSFUNCTION caused by a DYSREGULATED HOST RESPONSE to INFECTION (proven or suspected)..based on PATHOBIOLOGY Leads to prolonged ICU stays and a significant risk of dying,10% mortality
13 SEPSIS WHAT S IN and WHAT S OUT OUT.SIRS and SEVERE SEPSIS the reasons are 1- all based on clinical signs/symptoms,no definition 2- too sensitive, not specific enough 3-50% have appropriate adaptive response, not dying 4-1 in 8 missed organ failure and risk of death 5 all sepsis is severe (10% mortality), why separate term but lets remember that 1- since the incorporation of SIRS, less sepsis mortality?????? denominator increase

14 OUT NO MORE, TOSSED UNDER THE BUS
15 SEPSIS.WHAT S IN and WHAT S OUT IN NEW CLINICAL CRITERIA, INFECTION with ORGAN DYSFUNCTION Identified as an ACUTE CHANGE in total SOFA SCORE >2 CONSEQUENT TO INFECTION SOFA SEQUENTIAL (SEPSIS-RELATED) ORGAN FAILURE ASSESSMENT SCORE RESPIRATION, COAGULATION, LIVER, CARDIOVASCULAR CNS, RENAL ONLY validated for ICU PATIENTS and ALL BEGIN with SCORE = O unless known underlying abnormalities in parameters

16 NEW
17 QUICK SOFA..qSOFA EMERGENCY DEPARTMENT and GENERAL WARD BEDSIDE EVALUATION HAT. 1- HYPOTENSION SYSTOLIC BP <100 mm/hg 2- ALTERED MENTAL STATUS GLASGOW COMA SCORE <15 3- TACHYPNEA RESP RATE >22 / min >2 OF THE PARAMETERS SERVE AS QUALIFIERS AND ELIMINATE THE NEED FOR LABORATORY TESTING

18 HERE IS THE NEW ROAD MAP.
19 .and now SEPTIC SHOCK is...a SUBSET OF SEPSIS, in which UNDERLYING CIRCULATORY and CELLULAR / METABOLIC ABNORMALITIES are PROFOUND enough to SUBSTANTIALLY INCREASE MORTALITY (currently 42%). in other words BAD SEPSIS
20 ..and for SEPTIC SHOCK Having SEPSIS and 2 THINGS The Need for Vasopressor medications to Maintain a Mean Arterial Pressure(MAP) >65 mmhg Serum LACTATE level >2 mmol/l
21 THE ISSUES WITH SEPSIS-3 1- MAY BE TOO SENSITIVE AND LEAD TO UNWWARRANTED ANTIBIOTICS (or, so what else is new!!) 2- HOW TO MEASURE A DYSREGULATED HOST REPSONSE (or, when does this transition from regulated and helpful to dysregulated and and harmful??) 3- THE WHOLE CONCEPT IS PREDICATED ON INFECTION BEING THE TRIGGER (they could not define infection, but relied on any patient having cultures sent and given antibiotics how well has that worked out until now??) 4- REQUIRES CLINICAL PROMPTS FROM RNs, etc. (here comes code sepsis and more telephone random orders!)
22 AND IT IS STILL DEFINED AND CODED DIFFERENTLY BY: CDC JOINT COMMISION CMS HOSPITAL QUALITY MEASURES

23 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
24 Antibiotics We recommend that administration of IV antimicrobials be initiated as soon as possible after recognition and within 1 h for both sepsis and septic shock. (strong recommendation, moderate quality of evidence). We recommend empiric broad-spectrum therapy with one or more antimicrobials to cover all likely pathogens. (strong recommendation, moderate quality of evidence).
25 Antibiotics We suggest empiric combination therapy (using at least two antibiotics of different antimicrobial classes) aimed at the most likely bacterial pathogen(s) for the initial management of septic shock. (Weak recommendation; low quality of evidence)
26 Antibiotics We suggest that combination therapy not be routinely used for on-going treatment of most other serious infections, including bacteremia and sepsis without shock. (Weak recommendation; low quality of evidence). We recommend against combination therapy for the routine treatment of neutropenic sepsis/bacteremia. (Strong recommendation; moderate quality of evidence).

27 ..NOW TELL ME THIS IS NOT A COMMON EVERYDAY EVENT!
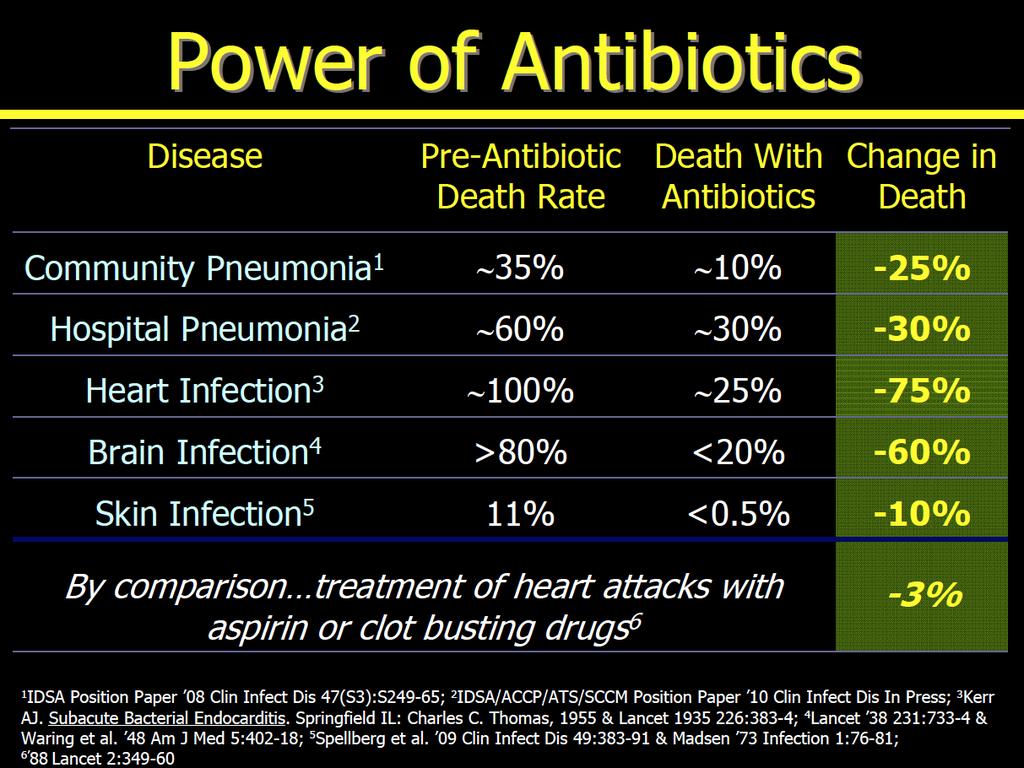
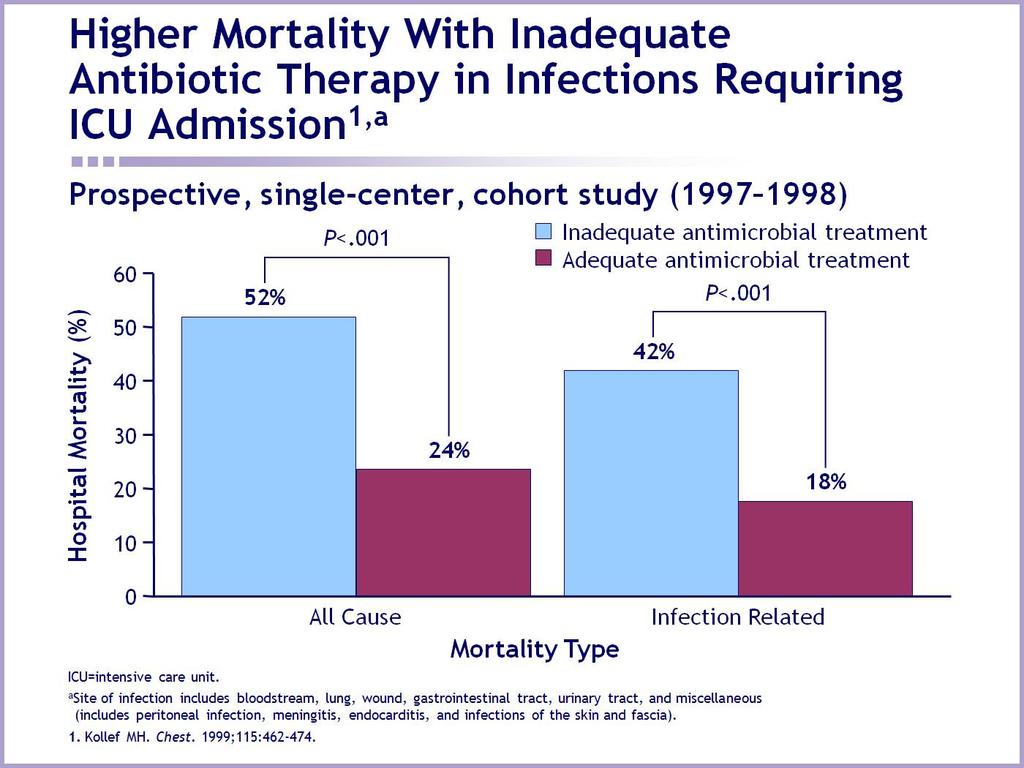
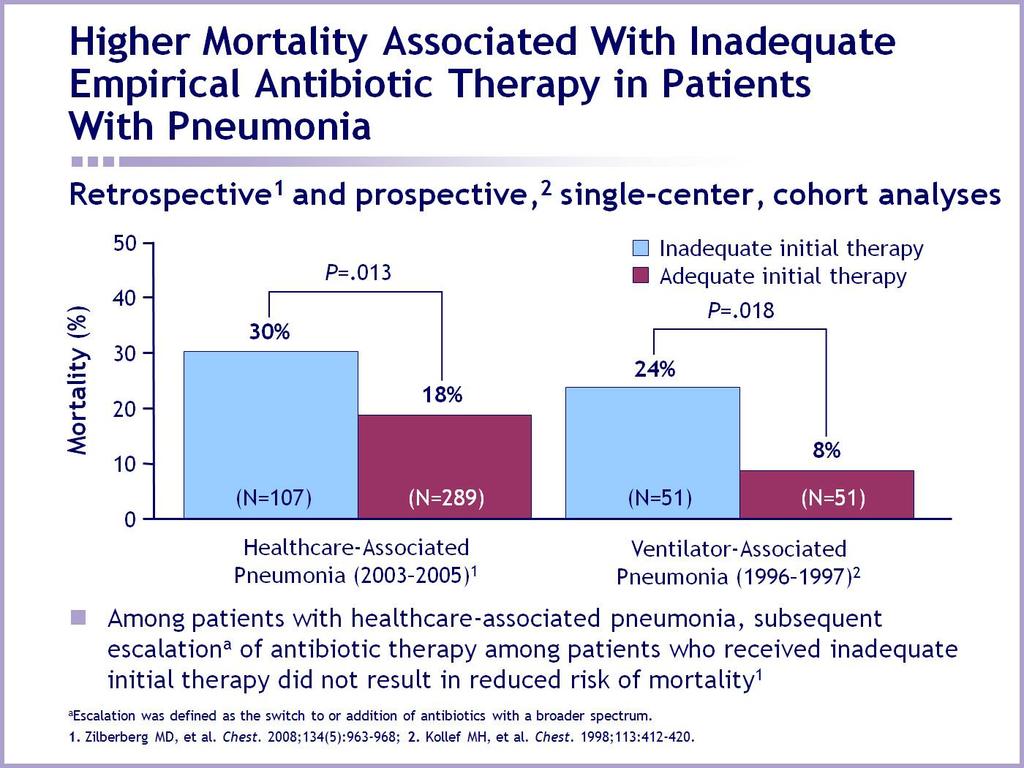
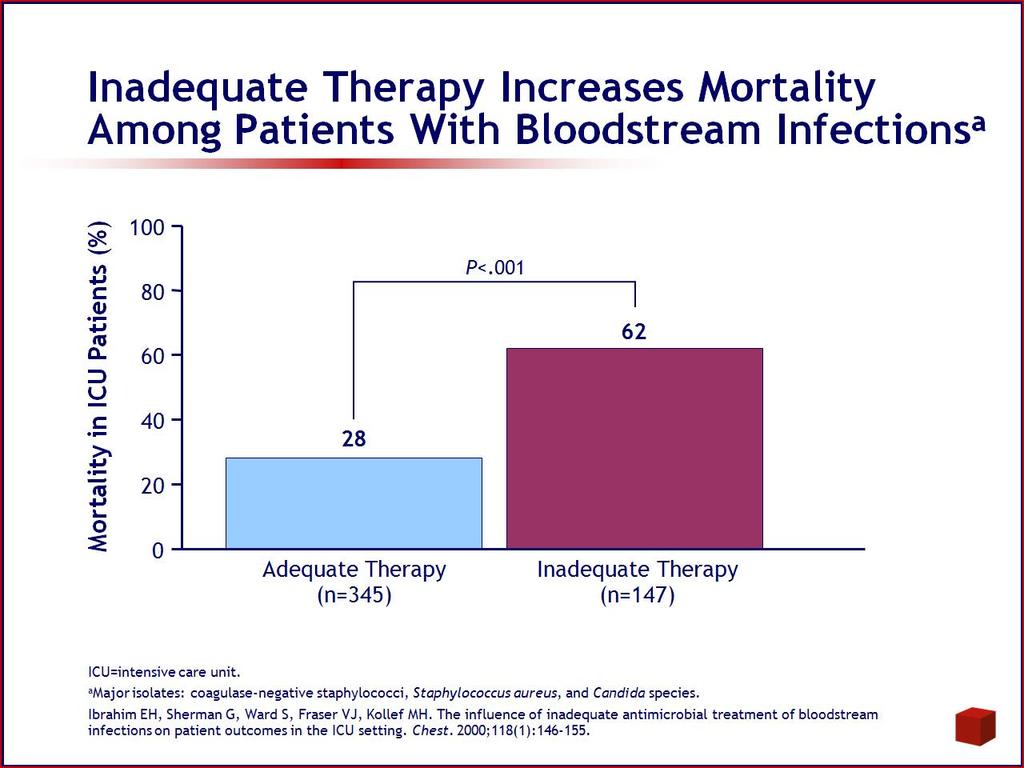
28 THE FACT IS.. THE ADMINISTRATION OF ADEQUATE ANTIBIOTICS HAS BEEN THE ONLY CLEARLY PROVEN BENEFICIAL INTERVENTION IN LOWERING MORTALITY IN SEPSIS AND SEPTIC SHOCK.
29 SO THEN HOW DO WE GET IT RIGHT?
30 The Origins of Antimicrobial Drugs Antibiotics ~ metabolic products of aerobic bacteria and fungi ~ reduce competition for nutrients and space Bacteria: Streptomyces,Acromyces and Bacillus Molds: Penicillium and Cephalosporium Antimicrobials Chemists have created new drugs by altering the structure of naturally occurring antibiotics

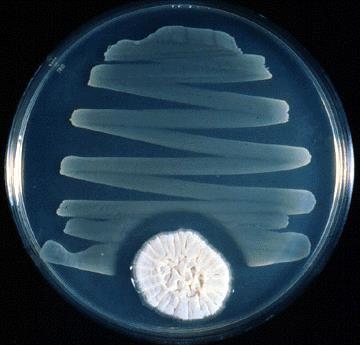
31 Flemming and Penicillin

32 Plate of Staphylococcus aureus inhibited by Penicillium notatum
33 Antibiotics Revolutionized Medicine Enable complicated surgery Enable cancer chemotherapy Enable critical care medicine Enable care for premature babies Enable organ transplantation Changed medicine from a diagnostic profession to a treatment profession
34
35
36
37 Antibiotics Are UNIQUE They are the only drugs that: lose efficacy over time & must be continually replaced need to be used sparingly to prolong their efficacy we actively discourage use of when they are approved
38
39
40
41
42
43

44
45 NONINFERIORITY TRIALS How do we claim the need for new antibiotics is based on the lack of efficacy of older agents in diseases, because of resistant pathogens, and then design the trial such as to show how much less effective a new drug might be compared with the older drug whose effectiveness is in doubt?
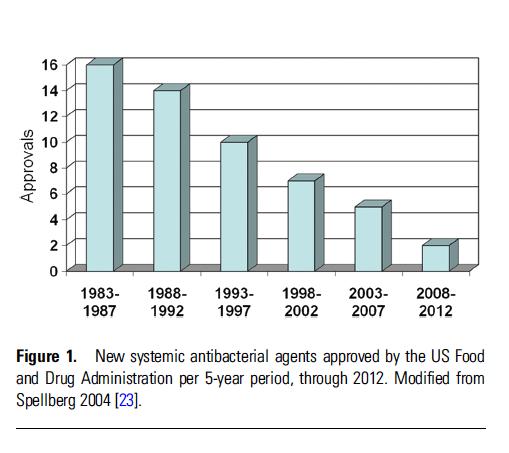
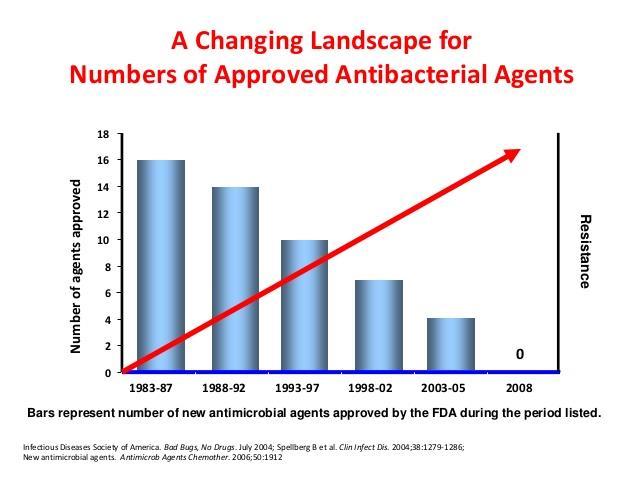
46 RECENTLY APPROVED NEW ANITIBACTERIAL AGENTS

47 ANTIBACTERIAL AGENTS IN CLINICAL DEVELOPMENT

48 ? SO WHY ALL THE RESISTANCE

49 Inappropriate Antimicrobial Use Prescription not taken correctly Antibiotics for viral infections Antibiotics sold without medical supervision Spread of resistant microbes in hospitals due to lack of hygiene
50
51
52
53
54 STRATEGIES TO REDUCE RESISTANCE (R) BLAST THEM antibiotic combinations never been shown to reduce emergence of R in routine bacteria FOOL THEM cycling drugs only temporarily changes R selection pressure STOP IRRITATING THEM Best Idea - 3 points Before Rx begins only treat true infection During avoid combos where single agents suffice Tail end only treat as long as needed to cure the infection
55 TERMS Modern Day Buzz Words Evidence Based Medicine Recommendations graded (strong-very weak) on Quality of Evidence (high-low) from studies Consensus of Expert Opinions Published Guidelines Experience, Anecdotal, Random What would seem to make Rational Scientific Sense


56 APPROPRIATE ANTIBIOTIC THERAPY THE USE OF ANTIBIOTICS WITH GOOD OR SUSCEPTIBLE IN-VITRO ACTIVITY AGAINST THE BACTERIA AT THE TISSUE SITE OF INFECTION i.e. just look for the S, I or R on the micro sheet


57 ADEQUATE ANTIMICROBIAL THERAPY INCLUDES APPROPRIATE PLUS DESCRIBES THE OPTIMAL THERAPY BASED UPON DOSAGE, PENETRATION TO THE SITE OF INFECTION, ROUTE OF ADMINISTRATION, COMBINATION THERAPY AND DURATION i.e. you need to really understand the drug and the infection
58 APPROPRIATE DOES NOT EQUAL ADEQUATE
59
60
61
62 SO THEN HOW DOES ONE CHOOSE AN ADEQUATE ANTIBIOTIC?
63 Many infections are self limited and lead to minimal morbidity and mortality in hosts with normal defense mechanisms I.E. They get better in spite of our correct or incorrect antibiotic choice and usage
64 In seriously ill patients, because of compromised immune function, anatomic abnormalities or infection with more virulent organisms, the outcome of the infection depends on early institution and correct use of APPROPRAITE AND ADEQUATE antimicrobial therapy
65 Empiric Antimicrobial Regimens are based on: History and Physical Likely site of infection Knowledge of pathogens commonly causing infection at that site Gram stain of appropriate specimen, modify regimen when pathogen(s) known


66 The role of antibacterials is to eradicate the causative organisms from the site of infection
67 The New Science : Pharmacokinetics and Pharmacodynamics Concept in Summary: Is there an antibiotic level in blood that predicts bacterial eradication and clinical success? If so, what is the optimal profile to maximize bacterial kill? Peak level of Abx = bacterial kill? Length of Time that Abx level exceeds the MIC = bacterial kill? Once PK/PD requirements are known, one can: Calculate appropriate doses of new or existing agents Compare antimicrobial activity of existing agents and utilize data in the development of guidelines Determine susceptibility of isolated pathogens
68 MIC: MINIMAL INHIBITORY CONCENTRATION Drug potency is measured by determining lowest concentration of an antimicrobial that results in the inhibition of visible growth of a microorganism after overnight exposure Known bacterial inoculum placed into each tube MIC = 4.0 µg/ml 0.25 µg/ml 0.5 µg/ml 1.0 µg/ml 2.0 µg/ml 4.0 µg/ml 8.0 µg/ml 16 µg/ml Increasing Antibiotic Concentration
69
70
71
72 TIME DEPENDENT ANTIBIOTICS TIME > MIC CORRELATES WITH CLINICAL ADEQUACY HOW MUCH TIME IS THAT? MORE IS NOT BETTER, JUST MORE
73 Pharmacokinetics and Pharmacodynamics: Required information Step 1: Determine MIC: How much antibiotic is required to inhibit further growth (stasis) in a test tube? Pathogen broth Antibiotic conc. (ug/ml) ABX Conc. (ug/ml) Step 2: Determine Dose: How much antibiotic is required in the blood to kill the pathogen at its site? (i.e. What is the correlation between the required serum level in the body and the MIC found in the lab?) MIC How high? (peak level vs MIC) How long? (time above MIC) How high for how long? (AUC vs MIC) Time
74 Predictors of Bacterial Eradication: Pharmacokinetic/Pharmacodynamic Profiles Time >MIC (time-dependent activity) AUC 24 /MIC (concentration-dependent activity) MIC MIC 40-50% Penicillins Cephalosporins Erythromycin Clarithromycin Optimal profile: Antibiotic level exceeds MIC for at least 40% of dosing interval Quinolones Aminoglycosides Azithromycin Optimal profile: AUC/MIC ratio at least: (Strep., other gram-positive) 125 (gram-negative bacilli) 1. Craig WA. Clin Infect Dis. 1998;26:1-12.
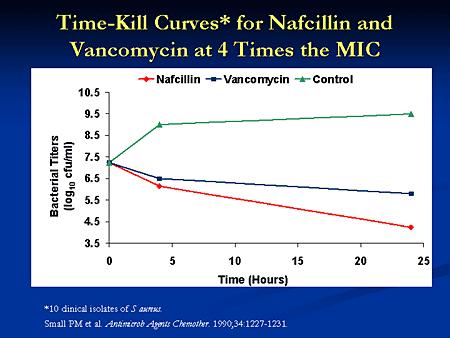
75 Bacteriological cure (%) The relationship between time above MIC 90 and bacteriological cure in S. pneumoniae (red) and H. influenzae (blue) in otitis media and sinusitis Otitis media Sinusitis Time Above MIC (% of dosing interval) Craig & Andes, Pediatr Infect Dis J 15;255,1996
76
77
78
79
80 CONCENTRATION DEPENDENT ANTIBIOTICS AUC / MIC CORRELATES WITH CLINICAL ADEQUACY MORE IS BETTER!
81 Concentration Pharmacokinetic/Pharmacodynamic Predictors of Efficacy 10 x C max (Peak) Parameters of Interest: AUC/MIC ratio 25: S. pneumoniae, Gram (+) 125: Gram (-) bacilli MIC B A C AUC D E F Time (hours) Craig W. Pharmacokinetic/Pharmacodynamic Parameters: Rationale for Antibacterial Dosing of Mice and Men. Clin Infect Dis. 1998; 26:1-12. G H I J K L M N O MIC= how much abx is required to inhibit growth in a test tube Area = length x width = conc. X time = mg/l x hr A+B+C+E+ = AUC
82 AUC:MIC ratio (area under the curve:mic ratio): Quinolones, Aminoglycosides and Azithromycin Concentration-dependent killing AUC 24 : MIC ratio = gm (+) 125 = gm (-) AUC Area Under the Curve MIC 0
83 Mortality (%) Relationship between Antibiotic concentration (24-Hr AUC/MIC) and Mortality in Immunocompetent Animals infected with S. pneumoniae using Fluoroquinolones Craig WA. Presented at ICAAC hr AUC/MIC
84
85
86
87
88
89
90
91
92
93
94
95

96
97
98
99
100
101

102 this HAS BEEN TAKING PLACE FOR YEARS. asking physicians to do a better job at prescribing antibiotics has and does not work and will require a behavior change. AREN T WE REALLY TALKING KNOWLEDGE AND UNDERSTANDING?
103
104
105 the risks of action are far less serious than those posed by comfortable status quo and inaction JFK..circa 1962
106 NOW, PERHAPS MORE THAN EVER TIME TO GET IT RIGHT! THANK YOU
Rational management of community acquired infections
 Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Rational management of community acquired infections Dr Tanu Singhal MD, MSc Consultant Pediatrics and Infectious Disease Kokilaben Dhirubhai Ambani Hospital, Mumbai Why is rational management needed?
Introduction to Pharmacokinetics and Pharmacodynamics
 Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
CHAPTER:1 THE RATIONAL USE OF ANTIBIOTICS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Antibiotics One of the most commonly used group of drugs In USA 23
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY*
 44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
44 DETERMINING CORRECT DOSING REGIMENS OF ANTIBIOTICS BASED ON THE THEIR BACTERICIDAL ACTIVITY* AUTHOR: Cecilia C. Maramba-Lazarte, MD, MScID University of the Philippines College of Medicine-Philippine
CHSPSC, LLC Antimicrobial Stewardship Education Series
 CHSPSC, LLC Antimicrobial Stewardship Education Series March 8, 2017 Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 1 Featured Speaker: Larry Danziger, Pharm.D. Professor of Pharmacy
CHSPSC, LLC Antimicrobial Stewardship Education Series March 8, 2017 Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 1 Featured Speaker: Larry Danziger, Pharm.D. Professor of Pharmacy
running head: SUPERBUGS Humphreys 1
 running head: SUPERBUGS Humphreys 1 Superbugs GCH 360 Term Paper Assignment Kelly Humphreys April 30, 2014 SUPERBUGS Humphreys 2 Introduction The World Health Organization (WHO) recognizes antibiotic resistance
running head: SUPERBUGS Humphreys 1 Superbugs GCH 360 Term Paper Assignment Kelly Humphreys April 30, 2014 SUPERBUGS Humphreys 2 Introduction The World Health Organization (WHO) recognizes antibiotic resistance
مادة االدوية المرحلة الثالثة م. غدير حاتم محمد
 م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
م. مادة االدوية المرحلة الثالثة م. غدير حاتم محمد 2017-2016 ANTIMICROBIAL DRUGS Antimicrobial drugs Lecture 1 Antimicrobial Drugs Chemotherapy: The use of drugs to treat a disease. Antimicrobial drugs:
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens
 The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
The pharmacological and microbiological basis of PK/PD : why did we need to invent PK/PD in the first place? Paul M. Tulkens Cellular and Molecular Pharmacology Unit Catholic University of Louvain, Brussels,
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali. Lec 1
 Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Principles of Anti-Microbial Therapy Assistant Professor Naza M. Ali Lec 1 28 Oct 2018 References Lippincott s IIIustrated Reviews / Pharmacology 6 th Edition Katzung and Trevor s Pharmacology / Examination
Pneumonia considerations Galia Rahav Infectious diseases unit Sheba medical center
 Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
Pneumonia considerations 2017 Galia Rahav Infectious diseases unit Sheba medical center Sir William Osler (1849 1919) "Father of modern medicine Pneumonia: The old man's friend The captain of the men of
COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS
 The European Agency for the Evaluation of Medicinal Products Veterinary Medicines and Inspections EMEA/CVMP/627/01-FINAL COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS GUIDELINE FOR THE DEMONSTRATION OF EFFICACY
The European Agency for the Evaluation of Medicinal Products Veterinary Medicines and Inspections EMEA/CVMP/627/01-FINAL COMMITTEE FOR VETERINARY MEDICINAL PRODUCTS GUIDELINE FOR THE DEMONSTRATION OF EFFICACY
Vaccination as a potential strategy to combat Antimicrobial Resistance in the elderly
 Vaccination as a potential strategy to combat Antimicrobial Resistance in the elderly Wilbur Chen, MD, MS 22-23 March 2017 WHO meeting on Immunization of the Elderly The Problem Increasing consumption
Vaccination as a potential strategy to combat Antimicrobial Resistance in the elderly Wilbur Chen, MD, MS 22-23 March 2017 WHO meeting on Immunization of the Elderly The Problem Increasing consumption
Meropenem for all? Midge Asogan ICU Fellow (also ID AT)
") Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Meropenem for all? Midge Asogan ICU Fellow (also ID AT) Infections Common reason for presentation to ICU Community acquired - vs nosocomial - new infection acquired within hospital environment Treatment
Why we perform susceptibility testing
 22 nd June 2015 Why we perform susceptibility testing Robin A Howe Antimicrobial use in Primary Care Why do we perform AST? Clinical Clinical Prediction Prediction of of Efficacy Efficacy Why do we perform
22 nd June 2015 Why we perform susceptibility testing Robin A Howe Antimicrobial use in Primary Care Why do we perform AST? Clinical Clinical Prediction Prediction of of Efficacy Efficacy Why do we perform
Antibiotic stewardship in long term care
 Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
Antibiotic stewardship in long term care Shira Doron, MD Associate Professor of Medicine Division of Geographic Medicine and Infectious Diseases Tufts Medical Center Boston, MA Consultant to Massachusetts
AND MISCONCEPTIONS IN THE MANAGEMENT OF SEPSIS
 MYTHS AND MISCONCEPTIONS IN THE MANAGEMENT OF SEPSIS SEPSISMADE EASY SURVIVINGSEPSIS COOKBOOK SEPSIS ISAPIE MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK DISCUSSION
MYTHS AND MISCONCEPTIONS IN THE MANAGEMENT OF SEPSIS SEPSISMADE EASY SURVIVINGSEPSIS COOKBOOK SEPSIS ISAPIE MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK DISCUSSION
Role of the general physician in the management of sepsis and antibiotic stewardship
 Role of the general physician in the management of sepsis and antibiotic stewardship Prof Martin Wiselka Dept of Infection and Tropical Medicine University Hospitals of Leicester Sepsis and antibiotic
Role of the general physician in the management of sepsis and antibiotic stewardship Prof Martin Wiselka Dept of Infection and Tropical Medicine University Hospitals of Leicester Sepsis and antibiotic
Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy
 Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy Leonardo Pagani MD Director Unit for Hospital Antimicrobial Chemotherapy
Building a Better Mousetrap for Nosocomial Drug-resistant Bacteria: use of available resources to optimize the antimicrobial strategy Leonardo Pagani MD Director Unit for Hospital Antimicrobial Chemotherapy
Introduction to Chemotherapeutic Agents. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018
 Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Introduction to Chemotherapeutic Agents Munir Gharaibeh MD, PhD, MHPE School of Medicine, The university of Jordan November 2018 Antimicrobial Agents Substances that kill bacteria without harming the host.
Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring. Janis Chan Pharmacist, UCH 2008
 and their Monitoring. Janis Chan Pharmacist, UCH 2008") Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring Janis Chan Pharmacist, UCH 25-4-2008 2008 Aminoglycosides (AG) 1. Gentamicin 2. Amikacin 3. Streptomycin 4. Neomycin
Pharmacokinetic & Pharmadynamic of Once Daily Aminoglycosides (ODA) and their Monitoring Janis Chan Pharmacist, UCH 25-4-2008 2008 Aminoglycosides (AG) 1. Gentamicin 2. Amikacin 3. Streptomycin 4. Neomycin
Principles of Antimicrobial therapy
 Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
Principles of Antimicrobial therapy Laith Mohammed Abbas Al-Huseini M.B.Ch.B., M.Sc, M.Res, Ph.D Department of Pharmacology and Therapeutics Antimicrobial agents are chemical substances that can kill or
3/1/2016. Antibiotics --When Less is More. Most Urgent Threats. Serious Threats
 Antibiotics --When Less is More Ralph Gonzales, MD, MSPH Associate Dean, Clinical Innovation School of Medicine VP, Clinical Innovation, UCSF Health Most Urgent Threats Serious Threats Multidrug-Resistant
Antibiotics --When Less is More Ralph Gonzales, MD, MSPH Associate Dean, Clinical Innovation School of Medicine VP, Clinical Innovation, UCSF Health Most Urgent Threats Serious Threats Multidrug-Resistant
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients
 Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Duke University Hospital Guideline for Empiric Inpatient Treatment of Cancer- Related Neutropenic Fever in Adult Patients PURPOSE Fever among neutropenic patients is common and a significant cause of morbidity
Bacterial Resistance of Respiratory Pathogens. John C. Rotschafer, Pharm.D. University of Minnesota
 Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
Bacterial Resistance of Respiratory Pathogens John C. Rotschafer, Pharm.D. University of Minnesota Antibiotic Misuse ~150 million courses of antibiotic prescribed by office based prescribers Estimated
General Approach to Infectious Diseases
 General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
General Approach to Infectious Diseases 2 The pharmacotherapy of infectious diseases is unique. To treat most diseases with drugs, we give drugs that have some desired pharmacologic action at some receptor
Antibiotic Resistance. Antibiotic Resistance: A Growing Concern. Antibiotic resistance is not new 3/21/2011
 Antibiotic Resistance Antibiotic Resistance: A Growing Concern Judy Ptak RN MSN Infection Prevention Practitioner Dartmouth-Hitchcock Medical Center Lebanon, NH Occurs when a microorganism fails to respond
Antibiotic Resistance Antibiotic Resistance: A Growing Concern Judy Ptak RN MSN Infection Prevention Practitioner Dartmouth-Hitchcock Medical Center Lebanon, NH Occurs when a microorganism fails to respond
DATA COLLECTION SECTION BY FRONTLINE TEAM. Patient Identifier/ Medical Record number (for facility use only)
") Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Assessment of Appropriateness of ICU Antibiotics (Patient Level Sheet) **Note this is intended for internal purposes only. Please do not return to PQC.** For this assessment, inappropriate antibiotic use
Geriatric Mental Health Partnership
 Geriatric Mental Health Partnership September 8, 2017 First, let s test your knowledge about antibiotics http://www.cdc.gov/getsmart/community/about/quiz.html 2 Get Smart Antibiotics Quiz Antibiotics fight
Geriatric Mental Health Partnership September 8, 2017 First, let s test your knowledge about antibiotics http://www.cdc.gov/getsmart/community/about/quiz.html 2 Get Smart Antibiotics Quiz Antibiotics fight
ECHO: Management of URIs. Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018
 ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
ECHO: Management of URIs Charles Krasner, M.D. Sierra NV Veterans Affairs Hospital University of NV, Reno School of Medicine October 16, 2018 Infectious causes of URIs change over time Most ARIs are viral
Antibiotics in vitro : Which properties do we need to consider for optimizing our therapeutic choice?
 Antibiotics in vitro : Which properties do we need to consider for optimizing our therapeutic choice? With the support of Wallonie-Bruxelles-International 1-1 In vitro evaluation of antibiotics : the antibiogram
Antibiotics in vitro : Which properties do we need to consider for optimizing our therapeutic choice? With the support of Wallonie-Bruxelles-International 1-1 In vitro evaluation of antibiotics : the antibiogram
Animal models and PK/PD. Examples with selected antibiotics
 Animal models and PK/PD PD Examples with selected antibiotics Examples of animal models Amoxicillin Amoxicillin-clavulanate Macrolides Quinolones Andes D, Craig WA. AAC 199, :375 Amoxicillin in mouse thigh
Animal models and PK/PD PD Examples with selected antibiotics Examples of animal models Amoxicillin Amoxicillin-clavulanate Macrolides Quinolones Andes D, Craig WA. AAC 199, :375 Amoxicillin in mouse thigh
Bai-Yi Chen MD. FCCP
 Treatment strategies for hospitalized versus nonhospitalized CAP patients: Asian perspective Bai-Yi Chen MD. FCCP Professor of Medicine Division of Infectious Disease, Infection Control Team The First
Treatment strategies for hospitalized versus nonhospitalized CAP patients: Asian perspective Bai-Yi Chen MD. FCCP Professor of Medicine Division of Infectious Disease, Infection Control Team The First
Objectives. Basic Microbiology. Patient related. Environment related. Organism related 10/12/2017
 Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
Basic Microbiology Vaneet Arora, MD MPH D(ABMM) FCCM Associate Director of Clinical Microbiology, UK HealthCare Assistant Professor, Department of Pathology and Laboratory Medicine University of Kentucky
Author - Dr. Josie Traub-Dargatz
 Author - Dr. Josie Traub-Dargatz Dr. Josie Traub-Dargatz is a professor of equine medicine at Colorado State University (CSU) College of Veterinary Medicine and Biomedical Sciences. She began her veterinary
Author - Dr. Josie Traub-Dargatz Dr. Josie Traub-Dargatz is a professor of equine medicine at Colorado State University (CSU) College of Veterinary Medicine and Biomedical Sciences. She began her veterinary
Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources
 Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources Andrew Hunter, PharmD, BCPS Infectious Diseases Clinical Pharmacy Specialist Michael E. DeBakey VA Medical Center Andrew.hunter@va.gov
Optimizing Antimicrobial Stewardship Activities Based on Institutional Resources Andrew Hunter, PharmD, BCPS Infectious Diseases Clinical Pharmacy Specialist Michael E. DeBakey VA Medical Center Andrew.hunter@va.gov
Antimicrobial stewardship in managing septic patients
 Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Antimicrobial Stewardship in Ambulatory Care
 Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Antimicrobial Stewardship in Ambulatory Care Nila Suntharam, M.D. May 5, 2017 Dr. Suntharam indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Combination vs Monotherapy for Gram Negative Septic Shock
 Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Combination vs Monotherapy for Gram Negative Septic Shock Critical Care Canada Forum November 8, 2018 Michael Klompas MD, MPH, FIDSA, FSHEA Professor, Harvard Medical School Hospital Epidemiologist, Brigham
Appropriate Management of Common Pediatric Infections. Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases
 Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Appropriate Management of Common Pediatric Infections Blaise L. Congeni M.D. Akron Children s Hospital Division of Pediatric Infectious Diseases It s all about the microorganism The common pathogens Viruses
Considerations in antimicrobial prescribing Perspective: drug resistance
 Considerations in antimicrobial prescribing Perspective: drug resistance Hasan MM When one compares the challenges clinicians faced a decade ago in prescribing antimicrobial agents with those of today,
Considerations in antimicrobial prescribing Perspective: drug resistance Hasan MM When one compares the challenges clinicians faced a decade ago in prescribing antimicrobial agents with those of today,
11/22/2016. Antimicrobial Stewardship Update Disclosures. Outline. No conflicts of interest to disclose
 Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Antimicrobial Stewardship Update 2016 APIC-CI Conference November 17 th, 2016 Jay R. McDonald, MD Chief, ID Section VA St. Louis Health Care System Assistant Professor of medicine Washington University
Critical Appraisal Topic. Antibiotic Duration in Acute Otitis Media in Children. Carissa Schatz, BSN, RN, FNP-s. University of Mary
 Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
Running head: ANTIBIOTIC DURATION IN AOM 1 Critical Appraisal Topic Antibiotic Duration in Acute Otitis Media in Children Carissa Schatz, BSN, RN, FNP-s University of Mary 2 Evidence-Based Practice: Critical
Antibiotic Kinetic and Dynamic Attributes for Community-Acquired Respiratory Tract Infections
 ...PRESENTATIONS... Antibiotic Kinetic and Dynamic Attributes for Community-Acquired Respiratory Tract Infections David P. Nicolau, PharmD Presentation Summary Factors, including the age of the treatment
...PRESENTATIONS... Antibiotic Kinetic and Dynamic Attributes for Community-Acquired Respiratory Tract Infections David P. Nicolau, PharmD Presentation Summary Factors, including the age of the treatment
Antibiotics in the future tense: The Application of Antibiotic Stewardship in Veterinary Medicine. Mike Apley Kansas State University
 Antibiotics in the future tense: The Application of Antibiotic Stewardship in Veterinary Medicine Mike Apley Kansas State University Changes in Food Animal Antibiotic Use How the uses of antibiotics in
Antibiotics in the future tense: The Application of Antibiotic Stewardship in Veterinary Medicine Mike Apley Kansas State University Changes in Food Animal Antibiotic Use How the uses of antibiotics in
Treatment of septic peritonitis
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Treatment of septic peritonitis Author : Andrew Linklater Categories : Companion animal, Vets Date : November 2, 2016 Septic
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017
 Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
Newsflash: Hospital Medicine JOHN C. CHRISTENSEN, MD FACP AMERICAN COLLEGE OF PHYSICIANS, UTAH CHAPTER SCIENTIFIC MEETING FEBRUARY 10, 2017 Newsflash: Fluoroquinolones Newsflash: Fluoroquinolones Don t
Antibiotic resistance: the rise of the superbugs
 Antibiotic resistance: the rise of the superbugs Allen Cheng Associate Professor of Infectious Diseases Epidemiology, Alfred Health; Monash University About me Specialist in infectious diseases Head, Infection
Antibiotic resistance: the rise of the superbugs Allen Cheng Associate Professor of Infectious Diseases Epidemiology, Alfred Health; Monash University About me Specialist in infectious diseases Head, Infection
Approach to pediatric Antibiotics
 Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
Approach to pediatric Antibiotics Gassem Gohal FAAP FRCPC Assistant professor of Pediatrics objectives To be familiar with common pediatric antibiotics o Classification o Action o Adverse effect To discus
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings?
 An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
An Approach to Appropriate Antibiotic Prescribing in Outpatient and LTC Settings? Dr. Andrew Morris Antimicrobial Stewardship ProgramMt. Sinai Hospital University Health Network amorris@mtsinai.on.ca andrew.morris@uhn.ca
Central Nervous System Infections
 Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Central Nervous System Infections Meningitis Treatment Bacterial meningitis is a MEDICAL EMERGENCY. ANTIBIOTICS SHOULD BE STARTED AS SOON AS THE POSSIBILITY OF BACTERIAL MENINGITIS BECOMES EVIDENT, IDEALLY
Percent Time Above MIC ( T MIC)
") 8 2007 Percent Time Above MIC ( T MIC) 18 8 25 18 12 18 MIC 1 1 T MIC 1 500 mg, 1 2 (500 mg 2) T MIC: 30 (TA30 ) 71.9 59.3 T MIC: 50 (TA50 ) 21.5, 0.1 1,000 mg 2 TA30 80.5, 68.7 TA50 53.2, 2.7 500 mg 3
8 2007 Percent Time Above MIC ( T MIC) 18 8 25 18 12 18 MIC 1 1 T MIC 1 500 mg, 1 2 (500 mg 2) T MIC: 30 (TA30 ) 71.9 59.3 T MIC: 50 (TA50 ) 21.5, 0.1 1,000 mg 2 TA30 80.5, 68.7 TA50 53.2, 2.7 500 mg 3
6/15/2017 PART 1: THE PROBLEM. Objectives. What is Antimicrobial Resistance? Conflicts of Interest Disclosure Statement
 Conflicts of Interest Disclosure Statement Getting a grasp on Antibiotic Use and Resistance: Principles of Antimicrobial Stewardship Speaker has nothing to disclose. Jacob M Kesner, PharmD UNMH PGY-2 Infectious
Conflicts of Interest Disclosure Statement Getting a grasp on Antibiotic Use and Resistance: Principles of Antimicrobial Stewardship Speaker has nothing to disclose. Jacob M Kesner, PharmD UNMH PGY-2 Infectious
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus
 Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Host, Syndrome, Bug, Drug: Introducing 2 Frameworks to Approach Infectious Diseases Cases with an Antimicrobial Stewardship Focus Montana ACP Meeting 2018 September 8, 2018 Staci Lee, MD, MEHP Billings
Does the Dose Matter?
 SUPPLEMENT ARTICLE Does the Dose Matter? William A. Craig Department of Medicine, University of Wisconsin, Madison, Wisconsin Pharmacokinetic/pharmacodynamic (PK/PD) parameters, such as the ratio of peak
SUPPLEMENT ARTICLE Does the Dose Matter? William A. Craig Department of Medicine, University of Wisconsin, Madison, Wisconsin Pharmacokinetic/pharmacodynamic (PK/PD) parameters, such as the ratio of peak
Barriers to Intravenous Penicillin Use for Treatment of Nonmeningitis
 JCM Accepts, published online ahead of print on 7 July 2010 J. Clin. Microbiol. doi:10.1128/jcm.01012-10 Copyright 2010, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
JCM Accepts, published online ahead of print on 7 July 2010 J. Clin. Microbiol. doi:10.1128/jcm.01012-10 Copyright 2010, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
Trea%ng Sepsis in 2016 Are the Big Guns Losing the War?
 Trea%ng Sepsis in 2016 Are the Big Guns Losing the War? ERIC HODGSON FCA (Crit Care) Inkosi Albert Luthuli Central Hospital & NELSON R MANDELA SCHOOL OF MEDICINE DURBAN, KZN Declaration Advisory boards
Trea%ng Sepsis in 2016 Are the Big Guns Losing the War? ERIC HODGSON FCA (Crit Care) Inkosi Albert Luthuli Central Hospital & NELSON R MANDELA SCHOOL OF MEDICINE DURBAN, KZN Declaration Advisory boards
Disclosures. Principles of Antimicrobial Therapy. Obtaining an Accurate Diagnosis Obtain specimens PRIOR to initiating antimicrobials
 Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Disclosures Principles of Antimicrobial Therapy None Lori A. Cox MSN, ACNP-BC, ACNPC, FCCM Penn State Hershey Medical Center Neuroscience Critical Care Unit Obtaining an Accurate Diagnosis Determine site
Comparative studies on pulse and continuous oral norfloxacin treatment in broilers and turkeys. Géza Sárközy
 Comparative studies on pulse and continuous oral norfloxacin treatment in broilers and turkeys Géza Sárközy Department of Pharmacology and Toxicology Faculty of Veterinary Science Szent István University
Comparative studies on pulse and continuous oral norfloxacin treatment in broilers and turkeys Géza Sárközy Department of Pharmacology and Toxicology Faculty of Veterinary Science Szent István University
P< cells/µl mg/dl P<0.01 P<0.01
 Technical Reports Judicious Use of s for Pediatric Infection Global Strategies to Prevent the Increase of Bacterial Resistance Kazunobu OUCHI Principle of antimicrobial therapy in children is to select
Technical Reports Judicious Use of s for Pediatric Infection Global Strategies to Prevent the Increase of Bacterial Resistance Kazunobu OUCHI Principle of antimicrobial therapy in children is to select
Curricular Components for Infectious Diseases EPA
 Curricular Components for Infectious Diseases EPA 1. EPA Title Promoting antimicrobial stewardship based on microbiological principles 2. Description of the A key role for subspecialists is to utilize
Curricular Components for Infectious Diseases EPA 1. EPA Title Promoting antimicrobial stewardship based on microbiological principles 2. Description of the A key role for subspecialists is to utilize
Antibiotic Stewardship in the LTC Setting
 Antibiotic Stewardship in the LTC Setting Joe Litsey, Director of Consulting Services Pharm.D., Board Certified Geriatric Pharmacist Thrifty White Pharmacy Objectives Describe the Antibiotic Stewardship
Antibiotic Stewardship in the LTC Setting Joe Litsey, Director of Consulting Services Pharm.D., Board Certified Geriatric Pharmacist Thrifty White Pharmacy Objectives Describe the Antibiotic Stewardship
3.0 Treatment of Infection
 3.0 Treatment of Infection Antibiotics and Medicine National Curriculum Link Key Stage 3 Sc1:1a - 1c. 2a 2p Sc2: 2n Unit of Study Unit 8: Microbes and Disease Unit 9B: Fit and Healthy Unit 20: 20 th Century
3.0 Treatment of Infection Antibiotics and Medicine National Curriculum Link Key Stage 3 Sc1:1a - 1c. 2a 2p Sc2: 2n Unit of Study Unit 8: Microbes and Disease Unit 9B: Fit and Healthy Unit 20: 20 th Century
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings. Carlos Reyes Sacin, MD, AAHIVS
 Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Antimicrobial Stewardship in the Long Term Care and Outpatient Settings Carlos Reyes Sacin, MD, AAHIVS Disclosure Speaker and consultant in HIV medicine for Gilead and Jansen Pharmaceuticals Objectives
Choosing an Antibiotic
 Principles of Antibiotic Use - The 6 Step Plan Robin J Green MBBCh, DCH, FC Paed, DTM&H, MMed, FCCP, PhD, Dip Allergy, FAAAAI Department of Paediatrics and Child Health 1 Choosing an Antibiotic Disease/Site
Principles of Antibiotic Use - The 6 Step Plan Robin J Green MBBCh, DCH, FC Paed, DTM&H, MMed, FCCP, PhD, Dip Allergy, FAAAAI Department of Paediatrics and Child Health 1 Choosing an Antibiotic Disease/Site
Antimicrobial therapy in critical care
 Antimicrobial therapy in critical care KARLEE JOHNSTON LEAD PHARMACIST DIVISION OF CRITICAL CARE CANBERRA HOSPITAL AND HEALTH SERVICE Outline 1. Let s talk about sepsis 2. PK/PD considerations 3. Selecting
Antimicrobial therapy in critical care KARLEE JOHNSTON LEAD PHARMACIST DIVISION OF CRITICAL CARE CANBERRA HOSPITAL AND HEALTH SERVICE Outline 1. Let s talk about sepsis 2. PK/PD considerations 3. Selecting
ESCMID Online Lecture Library. by author
 Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
Treatment of community-acquired meningitis including difficult to treat organisms like penicillinresistant pneumococci and guidelines (ID perspective) Stefan Zimmerli, MD Institute for Infectious Diseases
COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE (CVMP) REVISED GUIDELINE ON THE SPC FOR ANTIMICROBIAL PRODUCTS
 REVISED GUIDELINE ON THE SPC FOR ANTIMICROBIAL PRODUCTS") European Medicines Agency Veterinary Medicines and Inspections London, 12 November 2007 EMEA/CVMP/SAGAM/383441/2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE (CVMP) REVISED GUIDELINE ON THE SPC
European Medicines Agency Veterinary Medicines and Inspections London, 12 November 2007 EMEA/CVMP/SAGAM/383441/2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE (CVMP) REVISED GUIDELINE ON THE SPC
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance
 Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
Necrotizing Soft Tissue Infections: Emerging Bacterial Resistance Eileen M. Bulger, MD Professor of Surgery Harborview Medical Center University of Washington Objectives Review definition & diagnostic
ANTIMICROBIAL DOSING GUIDE 2013
 page 1 / 5 page 2 / 5 antimicrobial dosing guide 2013 pdf Stanford Hospital & Clinics Aminoglycoside Dosing Guidelines 2013 I. DETERMINING DOSE AND CREATININE CLEARANCE: 1. Use of ideal body weight (IBW)
page 1 / 5 page 2 / 5 antimicrobial dosing guide 2013 pdf Stanford Hospital & Clinics Aminoglycoside Dosing Guidelines 2013 I. DETERMINING DOSE AND CREATININE CLEARANCE: 1. Use of ideal body weight (IBW)
SESSION XVI NEW ANTIBIOTICS
 SESSION XVI NEW ANTIBIOTICS New Antibiotics to Treat Anaerobic Infections 2 Goldstein, E.J.C.;* Citron, D.M. Antibiotic Pharmacodynamics 3 Stein, G.E.* Targeting Selenium Metabolism in Stickland Fermentors:
SESSION XVI NEW ANTIBIOTICS New Antibiotics to Treat Anaerobic Infections 2 Goldstein, E.J.C.;* Citron, D.M. Antibiotic Pharmacodynamics 3 Stein, G.E.* Targeting Selenium Metabolism in Stickland Fermentors:
Antimicrobial Stewardship
 Antimicrobial Stewardship Preventing the Spread of Antibiotic Resistance and Improving Patient Care (Adapted from the Centers for Disease Control and Prevention) What is Stewardship? Antimicrobial stewardship
Antimicrobial Stewardship Preventing the Spread of Antibiotic Resistance and Improving Patient Care (Adapted from the Centers for Disease Control and Prevention) What is Stewardship? Antimicrobial stewardship
Challenges Emerging resistance Fewer new drugs MRSA and other resistant pathogens are major problems
 Micro 301 Antimicrobial Drugs 11/7/12 Significance of antimicrobial drugs Challenges Emerging resistance Fewer new drugs MRSA and other resistant pathogens are major problems Definitions Antibiotic Selective
Micro 301 Antimicrobial Drugs 11/7/12 Significance of antimicrobial drugs Challenges Emerging resistance Fewer new drugs MRSA and other resistant pathogens are major problems Definitions Antibiotic Selective
Collecting and Interpreting Stewardship Data: Breakout Session
 Collecting and Interpreting Stewardship Data: Breakout Session Michael S. Calderwood, MD, MPH Regional Hospital Epidemiologist, Dartmouth-Hitchcock Medical Center March 20, 2019 None Disclosures Outline
Collecting and Interpreting Stewardship Data: Breakout Session Michael S. Calderwood, MD, MPH Regional Hospital Epidemiologist, Dartmouth-Hitchcock Medical Center March 20, 2019 None Disclosures Outline
TREAT Steward. Antimicrobial Stewardship software with personalized decision support
 TREAT Steward TM Antimicrobial Stewardship software with personalized decision support ANTIMICROBIAL STEWARDSHIP - Interdisciplinary actions to improve patient care Quality Assurance The aim of antimicrobial
TREAT Steward TM Antimicrobial Stewardship software with personalized decision support ANTIMICROBIAL STEWARDSHIP - Interdisciplinary actions to improve patient care Quality Assurance The aim of antimicrobial
OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS
 HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
HTIDE CONFERENCE 2018 OPTIMIZATION OF PK/PD OF ANTIBIOTICS FOR RESISTANT GRAM-NEGATIVE ORGANISMS FEDERICO PEA INSTITUTE OF CLINICAL PHARMACOLOGY DEPARTMENT OF MEDICINE, UNIVERSITY OF UDINE, ITALY SANTA
Physician Rating: ( 23 Votes ) Rate This Article:
 Rate This Article:") From Medscape Infectious Diseases Conquering Antibiotic Overuse An Expert Interview With the CDC Laura A. Stokowski, RN, MS Authors and Disclosures Posted: 11/30/2010 Physician Rating: ( 23 Votes ) Rate
From Medscape Infectious Diseases Conquering Antibiotic Overuse An Expert Interview With the CDC Laura A. Stokowski, RN, MS Authors and Disclosures Posted: 11/30/2010 Physician Rating: ( 23 Votes ) Rate
Prophylactic antibiotic timing and dosage. Dr. Sanjeev Singh AIMS, Kochi
 Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Prophylactic antibiotic timing and dosage Dr. Sanjeev Singh AIMS, Kochi Meaning - Webster Medical Definition of prophylaxis plural pro phy lax es \-ˈlak-ˌsēz\play : measures designed to preserve health
Welcome! 10/26/2015 1
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
GUIDE TO INFECTION CONTROL IN THE HOSPITAL. Antibiotic Resistance
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 4: Antibiotic Resistance Author M.P. Stevens, MD, MPH S. Mehtar, MD R.P. Wenzel, MD, MSc Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 4: Antibiotic Resistance Author M.P. Stevens, MD, MPH S. Mehtar, MD R.P. Wenzel, MD, MSc Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
The Rise of Antibiotic Resistance: Is It Too Late?
 The Rise of Antibiotic Resistance: Is It Too Late? Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine None DISCLOSURES THE PROBLEM Antibiotic resistance is one of the
The Rise of Antibiotic Resistance: Is It Too Late? Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine None DISCLOSURES THE PROBLEM Antibiotic resistance is one of the
TITLE: Recognition and Diagnosis of Sepsis in Rural or Remote Areas: A Review of Clinical and Cost-Effectiveness and Guidelines
 TITLE: Recognition and Diagnosis of Sepsis in Rural or Remote Areas: A Review of Clinical and Cost-Effectiveness and Guidelines DATE: 11 August 2016 CONTEXT AND POLICY ISSUES Sepsis, defined in the 2016
TITLE: Recognition and Diagnosis of Sepsis in Rural or Remote Areas: A Review of Clinical and Cost-Effectiveness and Guidelines DATE: 11 August 2016 CONTEXT AND POLICY ISSUES Sepsis, defined in the 2016
Community-Associated C. difficile Infection: Think Outside the Hospital. Maria Bye, MPH Epidemiologist May 1, 2018
 Community-Associated C. difficile Infection: Think Outside the Hospital Maria Bye, MPH Epidemiologist Maria.Bye@state.mn.us 651-201-4085 May 1, 2018 Clostridium difficile Clostridium difficile Clostridium
Community-Associated C. difficile Infection: Think Outside the Hospital Maria Bye, MPH Epidemiologist Maria.Bye@state.mn.us 651-201-4085 May 1, 2018 Clostridium difficile Clostridium difficile Clostridium
Early Antibiotics for Sepsis and Septic Shock: A Gold Standard
 Early Antibiotics for Sepsis and Septic Shock: A Gold Standard Anand Kumar MD, FRCPC, FCCP, FCCM Professor of Medicine University of Manitoba Health Sciences Centre St. Boniface Hospital Winnipeg, Manitoba
Early Antibiotics for Sepsis and Septic Shock: A Gold Standard Anand Kumar MD, FRCPC, FCCP, FCCM Professor of Medicine University of Manitoba Health Sciences Centre St. Boniface Hospital Winnipeg, Manitoba
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani
 Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
Treatment of Respiratory Tract Infections Prof. Mohammad Alhumayyd Dr. Aliah Alshanwani 30-1-2018 1 Objectives of the lecture At the end of lecture, the students should be able to understand the following:
GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
 Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Version 3.1 GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS Date ratified June 2008 Updated March 2009 Review date June 2010 Ratified by Authors Consultation Evidence base Changes
Imagine. Multi-Drug Resistant Superbugs- What s the Big Deal? A World. Without Antibiotics. Where Simple Infections can be Life Threatening
 Multi-Drug Resistant Superbugs- What s the Big Deal? Toni Biasi, RN MSN MPH CIC Infection Prevention Indiana University Health Imagine A World Without Antibiotics A World Where Simple Infections can be
Multi-Drug Resistant Superbugs- What s the Big Deal? Toni Biasi, RN MSN MPH CIC Infection Prevention Indiana University Health Imagine A World Without Antibiotics A World Where Simple Infections can be
How is Ireland performing on antibiotic prescribing?
 European Antibiotic Awareness Campaign 2016 November Webinar Series on Antibiotic Prescribing How is Ireland performing on antibiotic prescribing? Dr Rob Cunney National Clinical Lead HCAI AMR Clinical
European Antibiotic Awareness Campaign 2016 November Webinar Series on Antibiotic Prescribing How is Ireland performing on antibiotic prescribing? Dr Rob Cunney National Clinical Lead HCAI AMR Clinical
Understanding the Hospital Antibiogram
 Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC
 Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Pneumonia Antibiotic Guidance for Adults PAGL Inclusion Approved at January 2017 PGC APPROVED BY: Policy and Guidelines Committee TRUST REFERENCE: B9/2009 AWP Ref: AWP61 Date (approved): July 2008 REVIEW
Control emergence of drug-resistant. Reduce costs
 ...PRESENTATIONS... Guidelines for the Management of Community-Acquired Pneumonia Richard E. Chaisson, MD Presentation Summary Guidelines for the treatment of community-acquired pneumonia (CAP) have been
...PRESENTATIONS... Guidelines for the Management of Community-Acquired Pneumonia Richard E. Chaisson, MD Presentation Summary Guidelines for the treatment of community-acquired pneumonia (CAP) have been
Antimicrobial Resistance and Papua New Guinea WHY is it important? HOW has the problem arisen? WHAT can we do?
 Antimicrobial Resistance and Papua New Guinea WHY is it important? HOW has the problem arisen? WHAT can we do? John Ferguson, John Hunter Hospital, University of Newcastle, NSW, Australia Infectious Diseases
Antimicrobial Resistance and Papua New Guinea WHY is it important? HOW has the problem arisen? WHAT can we do? John Ferguson, John Hunter Hospital, University of Newcastle, NSW, Australia Infectious Diseases
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults)
") Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
Guidelines for the Initiation of Empirical Antibiotic therapy in Respiratory Disease (Adults) Community Acquired Pneumonia Community Acquired Pneumonia 1) Is it pneumonia? ie new symptoms and signs of
parameters were enhanced to develop new antimicrobial formulations CONSIDERATIONS IN ANTIMICROBIAL SELECTION Using animal models and human data, PK an
 Overview of Newer Antimicrobial Formulations for Overcoming Pneumococcal Resistance William A Craig, MD The pharmacokinetic (PK) and pharmacodynamic (PD) profile of an antimicrobial agent provides important
Overview of Newer Antimicrobial Formulations for Overcoming Pneumococcal Resistance William A Craig, MD The pharmacokinetic (PK) and pharmacodynamic (PD) profile of an antimicrobial agent provides important
Antibiotics in the trenches: An ER Doc s Perspective
 Antibiotics in the trenches: An ER Doc s Perspective Peter Currie, MD Medical Director for Quality Emergency Physicians Professional Association (EPPA) Agenda Emergency Medicine Specific Disease Processes
Antibiotics in the trenches: An ER Doc s Perspective Peter Currie, MD Medical Director for Quality Emergency Physicians Professional Association (EPPA) Agenda Emergency Medicine Specific Disease Processes
Antibiotic Resistance
 Antibiotic Resistance ACVM information paper Background Within New Zealand and internationally, concerns have been raised about an association between antibiotics used routinely to protect the health of
Antibiotic Resistance ACVM information paper Background Within New Zealand and internationally, concerns have been raised about an association between antibiotics used routinely to protect the health of
Measure Information Form
 Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Release Notes: Measure Information Form Version 3.0b **NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE** Measure Set: Pneumonia (PN) Performance Measure Identifier: Measure Information Form
Dr. NAFRIALDI, PhD, SpPD, SpFK
 Dr. NAFRIALDI, PhD, SpPD, SpFK Lahir: Bukittinggi, 30 Oktober 1961. Pendidikan Dokter Umum: FKUI, 1986 S2 Farmakologi: Universite Claude Bernard, Lyon, Perancis, 1991 S3 Farmakologi: Universite Montpellier,
Dr. NAFRIALDI, PhD, SpPD, SpFK Lahir: Bukittinggi, 30 Oktober 1961. Pendidikan Dokter Umum: FKUI, 1986 S2 Farmakologi: Universite Claude Bernard, Lyon, Perancis, 1991 S3 Farmakologi: Universite Montpellier,